Orthopedic Board Review MCQs: Arthroplasty, Trauma & Infection | Part 146
Key Takeaway
This page offers Part 146 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. Featuring 100 verified, high-yield MCQs, it's designed for orthopedic surgeons and residents preparing for certification exams. Utilize interactive study and exam modes to master topics like Arthroplasty, Hip, and Trauma with detailed explanations.
About This Board Review Set
This is Part 146 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 146
This module focuses heavily on: Arthroplasty, Elbow, Hip, Infection, Trauma.
Sample Questions from This Set
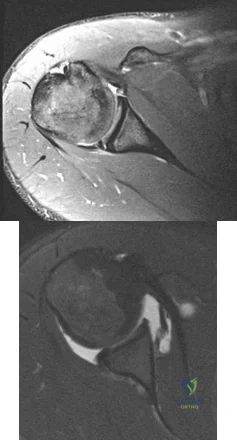
Sample Question 1: A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figur...
Sample Question 2: When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?...
Sample Question 3: A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?...
Sample Question 4: Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?...
Sample Question 5: A patient who has recalcitrant medial plantar heel pain and pain directly over the medial side of the heel undergoes open release of the plantar fascia. After releasing a portion of the plantar fascia, the deep fascia of the abductor halluc...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 2
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 3
A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?
Explanation
Sever disease, or calcaneal apophysitis, is best treated with activity modification that includes rest, restriction from sports and running, and Achilles tendon stretching exercises. The diagnosis is clinical (rendering MRI study unnecessary) and the course is usually self-limited, obviating the need for surgery. Occasionally, children with severe symptoms may benefit from a short period of cast or fracture brace immobilization.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Question 4
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 5
A patient who has recalcitrant medial plantar heel pain and pain directly over the medial side of the heel undergoes open release of the plantar fascia. After releasing a portion of the plantar fascia, the deep fascia of the abductor hallucis muscle is released to relieve pressure on which of the following structures?
Explanation
REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
Davies MS, Weiss GA, Saxby TS: Plantar fasciitis: How successful is surgical intervention? Foot Ankle Int 1999;20:803-807.
Question 6
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of
Explanation
REFERENCES: Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995,
pp 107-123.
Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 7
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?
Explanation
REFERENCES: Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
Hanna SL, Fletcher BD, Kaste SC, Fairclough DL, Parham DM: Increased confidence of diagnosis of Ewing sarcoma using T2-weighted MR images. Magn Reson Imaging 1994;12:559-568.
Question 8
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Explanation
REFERENCES: Sitler DF, Amendola A, Bailey CS, et al: Posterior ankle arthroscopy:
An anatomic study. J Bone Joint Surg Am 2002;84:763-769.
Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 361.
Question 9
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?
Explanation
REFERENCES: Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Jenter M, Lipton GE, Miller F: Operative treatment for hallux valgus in children with cerebral palsy. Foot Ankle Int 1998;19:830-835.
Question 10
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413.
Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 11
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 12
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?
Explanation
REFERENCE: Springfield DS, Rosenberg AE, Mankin HJ, et al: Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop 1994;309:234-244.
Question 13
View Abstract at PubMed Figures 87a and 87b are sagittal and coronal MR images of the affected elbow of a 36-year-old man who has a history of painful mechanical symptoms in his dominant arm when extending his elbow in full supination. What is the most likely cause of his painful snapping? A B

Explanation
The MRI studies show a radiocapitellar plica. This anomalous structure has been associated with symptomatic snapping. Lacertus fibrosis contracture will not cause painful snapping. An intra-articular pathology such as loose bodies is not present on these imaging studies. Olecranon fossa impingement causes posterior pain in extension and is not shown in the images.
RECOMMENDED READINGS
Antuna SA, O'Driscoll SW. Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy. 2001 May;17(5):491-5. PubMed 11337715. View Abstract at PubMed
Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006 May-Jun;15(3):367-70. PubMed PMID: 16679240. View Abstract at PubMed
Question 14
Figures 1 and 2 are the MR arthrogram images of a 20-year-old right-hand dominant collegiate basketball player who sustained an initial shoulder dislocation 1 year ago. In the month prior to presentation, he dislocated his shoulder two more times. Each time it occurred when going up for a rebound and an opponent grabbed the ball from behind him, hyperextending his shoulder. Physical examination demonstrates full range of motion, absence of atrophy, a positive apprehension sign and relocation test, and a positive Kim test. What is the best next step?
Explanation
physical examination and advanced imaging in these patients are crucial in directing appropriate treatment.
Question 15
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
Question 16
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
REFERENCES: Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 17
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
Question 18
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
REFERENCES: Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
Heydarian K, Akbarnia BA, Jabalameli M, Tabador K: Posterior capsulotomy for the treatment of severe flexion contractures of the knee. J Pediatr Orthop 1984;4:700-704.
Question 19
Communication breakdown is the leading cause of which of the following?
Explanation
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Question 20
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 21
Figures 20a and 20b show the radiographs of an obese 15-year-old boy who has severe left groin pain and is unable to bear weight following a minor injury. Treatment should consist of
Explanation
REFERENCES: Aronson DD, Loder RT: Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop 1996;322:99-110.
Karol LA, Doane RM, Cornicelli SF, Zak PA, Haut RC, Manoli A II: Single versus double screw fixation for treatment of slipped capital femoral epiphysis: A biomechanical analysis. J Pediatr Orthop 1992;12:741-745.
Stanitski CL: Acute slipped capital femoral epiphysis: Treatment alternatives. J Am Acad Orthop Surg 1994;2:96-106.
Question 22
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?

Explanation
Question 23
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a “lump” at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 1078-1079.
Rockwood CA, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 24
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled “A” in Figure 45?
Explanation
REFERENCES: Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Sobel M, Levy ME, Bohne WH: Congenital variations of the peroneus quartus muscle: An anatomic study. Foot Ankle 1990;11:81-89.
Question 25
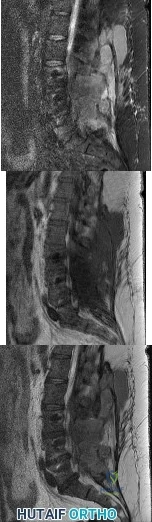
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 26
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;108:15-18.
Question 27
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Lucas DR, Nascimento AG, Sim FH: Clear cell sarcoma of soft tissues: Mayo Clinic experience with 35 cases. Am J Surg Pathol 1992;16:1197-1204.
Question 28
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted? Review Topic

Explanation
Question 29
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
Question 30
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?
Explanation
REFERENCES: Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.
Question 31
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 32
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
REFERENCE: Windsor RE: Knee arthrodesis, in Insall JN, Windsor R, Kelly M, et al (eds): Surgery of the Knee. New York, NY, Churchill Livingstone, 1993, pp 1103-1116.
Question 33
Which of the following is considered the most accurate test to determine the amount of limb-length discrepancy in a patient with a knee flexion contracture of 35°?
Explanation
REFERENCES: Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Tachdjian MO: Pediatric Orthopedics. Philadelphia, Pa, WB Saunders, 1990, pp 2867-2870.
Question 34
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 35
Which of the following is a recognized consequence of hip fusion?
Explanation
REFERENCES: Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Sponseller PD, McBeath AA, Perpich M: Hip arthrodesis in young patients: A long-term follow-up study. J Bone Joint Surg Am 1984;66:853-859.
Question 36
The initiating cellular event in development of posttraumatic osteoarthritis is attributed to which of the following?
Explanation
Question 37
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 68-72.
Question 38
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. View Abstract at PubMed
Question 39
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 40
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
Explanation
Plantar distal phalanges to medial navicular
Medial navicular to dorsal lateral cuneiform
Plantar 1st metatarsal to dorsal lateral cuneiform
5th metatarsal base to dorsal medial cuneiform
Plantar distal phalanx of the hallux to dorsal distal phalanx of hallux
Dynamic tendon transfer to restore active dorsiflexion of the foot involves transferring the posterior tibial tendon (PTT) insertion on the medial navicular to the dorsal lateral cuneiform.
Common peroneal nerve (CPN) injuries following traumatic knee dislocation are common, with an incidence of 25-40%. CPN palsy is characterized by foot drop due to loss of ankle dorsiflexors with a steppage gait and eventual development of a supinated equinovarus foot secondary to the unopposed pull of the PTT. Nonsurgical management involves use of an ankle-foot orthosis and physical therapy. Surgical
options include acute primary repair, nerve grafting with either autologous sural nerve or nerve conduits and dynamic tendon transfer. The PTT is harvested from its insertion at the navicular, passed through the interosseous membrane (IOM) and anchored to the lateral cuneiform (see Illustration A). The classic bridle procedure involves concomitant anastamosis of the PTT to the tibialis anterior (TA) and peroneus longus (PL) tendons.
Garozzo et al reported a case series of 62 patients with post-traumatic CPN palsy who underwent a one-stage procedure consisting of nerve repair and PTT transfer. Nerve repair combined with PTT transfer improved postoperative outcomes compared to nerve repair alone. At 2-year follow up, neural regeneration was demonstrated in 90% of patients. The authors hypothesized that poor outcomes following nerve repair alone are due to force imbalance between the functioning flexors and paralyzed extensors, which is somewhat equalized by performing a PTT transfer at time of repair.
Niall et al reviewed 55 patients with traumatic knee dislocation and reported a 41% incidence of CPN injury, exclusively associated with dislocations involving disruption of the posterior cruciate ligament (PCL) and posterolateral corner (PLC). Complete neurologic recovery was found in only 21% of patients. The best prognosis was found with lesions in continuity, less than 7cm of nerve involvement, and short conduction block and muscle activity on nerve conduction and EMG studies.
Vigasio et al described a dynamic tendon transfer technique for traumatic complete CPN injury, involving transfer of the PTT to the TA rerouted to a new origin at the lateral cuneiform to restore ankle dorsiflexion and flexor digitorum longus (FDL) to the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) to restore digit dorsiflexion. Rerouting the TA towards the transferred PTT ensures the PTT harvest length is sufficient. This avoids excessive tensioning of the PTT, which may limit tendon excursion and result in a static tenodesis rather than dynamic function, as well as the need for PTT lengthening which may decrease strength of the transfer
Illustration A is a series of intraoperative photographs demonstrating PTT transfer from Garg et al. An incision is made distal to the medial malleolus and the PTT is harvested subperiosteally (A). The PTT is delivered through a second incision ~15cm proximal to the medial malleolus (B-C). The PTT is then passed through the interosseous membrane and out a third incision over the anterior fibula (D). Lastly, the PTT is passed through a fourth incision over the dorsal midfoot and anchored to the lateral cuneiform (E).
Incorrect Responses:
nerve and therefore would not be functional. Answer 5: Transferring the flexor hallucis longus (FHL; insertion = plantar distal phalanx of the hallux) to the insertion of the EHL (dorsal distal phalanx of hallux) is recommended for correction of claw toe deformity and would not help restore foot dorsiflexion in this patient.
Question 41
Figure 131 is the abdominal radiograph of a 70-year-old man who experiences nausea and abdominal tightness 48 hours after undergoing left total knee arthroplasty. An examination reveals severe abdominal distension and markedly decreased bowel sounds. Insertion of a nasogastric tube does not relieve abdominal tightness. What is the best next step?
Explanation
The abdominal radiograph reveals an acute colonic pseudo-obstruction. It is associated with parenteral narcotic use and hypokalemia. Initial treatment is insertion of a nasograstric tube, discontinuation of parenteral narcotics, and correction of electrolyte imbalances. If a pseudo-obstruction is not relieved, colonoscopy should be performed.
Question 42
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 43
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 44
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Explanation
Question 45
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 46
A 3-year-old girl has had pain and swelling in her left thigh for the past 3 weeks. Her mother states she has had a temperature as high as 100.4 degrees F (38 degrees C) and a weight loss of 5 pounds. A CBC shows a WBC count of 11,000/mm3, an erythrocyte sedimentation rate of 13 mm/h, and a C-reactive protein of 0.3. A radiograph is shown in Figure 2. What is the next step in management?
Explanation
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
AL-Madena Copy
Question 47
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 48
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
Question 49
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 50
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 51
Sudden cardiac death in the young athlete is most frequently caused by
Explanation
REFERENCES: Burke AP, Farb A, Virmani R, Goodin J, Smialek JE: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991;121:568-575.
Maron BJ, Sharani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA
1996;276:199-204.
Question 52
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty? Review Topic
Explanation
Question 53
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10° to 55°, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
REFERENCE: Mauerhan DR, Mokris JG, Ly A, Kiebzak GM: Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty 1998;13:896-900.
Question 54
A 63-year-woman has an elbow flexion contracture. History reveals that she underwent three previous surgeries to remove a malignant fibrous histiocytoma of the forearm. An MRI scan reveals a locally recurrent tumor at the site of the previous surgery. Which of the following is considered the most predictive factor for local recurrence?
Explanation
REFERENCES: Bell RS, O’Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375.
Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J: Preoperative radiation, surgical margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;52:223-230.
Wilson AN, Davis A, Bell RS, et al: Local control of soft tissue sarcoma of the extremity: The experience of a multidisciplinary sarcoma group with definitive surgery and radiotherapy. Eur J Cancer 1994;30:746-751.
Question 55
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
Question 56
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 57
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure 2. Which interposed structure is preventing reduction?

Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
Question 58
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
Explanation
REFERENCES: Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
Question 59
A 27-year-old man has recurrent right shoulder instability. He first dislocated his shoulder in college while playing rugby and was treated nonsurgically. Since then, he has sustained nearly 1 dozen dislocations and says that his shoulder always feels “loose.” The shoulder recently dislocated in his sleep and while he was putting on clothes. Which factor is a contraindication to an arthroscopic soft-tissue repair?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Although some studies suggest that open stabilization may result in lower recurrence rates in contact athletes, this approach is now under scrutiny. Extensive labral involvement (posterior labral involvement in this scenario) is likely more accessible via arthroscopic methods. Although HAGL lesions may be more easily accessible via an open approach (particularly for inexperienced arthroscopists), numerous authors describe successful repair via arthroscopic techniques. Among these responses, the strongest indication for an open approach, including possible bony transfer, is high-grade glenoid bone loss. Although the critical amount of bone loss is a topic of debate, most surgeons and authors suggest a cutoff of 20% to 25%.

CLINICAL SITUATION FOR QUESTIONS 90 THROUGH 92
Figure 90 is the radiograph of a 14-year-old pitcher who plays in a year-round baseball program and has vague pain in his dominant shoulder. The pain occurs with throwing, and it has been worsening for 2 months. Pain typically occurs during the late cocking phase of throwing. He has no tenderness of the rotator cuff and 5/5 rotator cuff strength. His arc of motion is symmetric between his dominant and nondominant arms. The sulcus sign is negative.
Question 60
A 22-year-old male soccer player reports left hip and groin pain. He states that symptoms began before a preseason tournament but have worsened steadily for the past 2 weeks. He denies any recent fever or sickness and is otherwise healthy. Examination reveals tenderness over the symphysis pubis and pain with resisted rectus abdominus testing. Radiographs are negative. What is the next step in the proper management of this patient? Review Topic
Explanation
Question 61
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 2-49.
Question 62
What is the structure indicated by the letter “A” in Figure A? Review Topic
Explanation
Question 63
A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
Explanation
glenoid bone grafting may be considered for glenoid retroversion >15°.
Question 64
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel’s sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 530-531.
Question 65
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 66
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Henry R, Goletz B, Williamson C: Lateral release in patello-femoral subluxation. Am J Sports Med 1986;14:121.
Question 67
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 68
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF, Askew LJ, Chao EY: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-877.
Question 69
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 70
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic

Explanation
Question 71
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 72
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
REFERENCES: Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Sarhadi NS, Korday SN, Bainbridge LC: Radial tunnel syndrome: Diagnosis and management. J Hand Surg Br 1998;23:617-619.
Question 73
What is the primary mechanism of injury for the fracture shown in Figures 33a and 33b?
Explanation
REFERENCES: Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 267-272.
Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65:438-444.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 74
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology? Review Topic
Explanation
Question 75
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?
Explanation
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory

drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Question 76
What zone of the physis is widened in rickets?
Explanation
REFERENCES: Hunziker EB, Schenk RK, Cruz-Orive LM: Quantitation of chondrocyte performance in growth-plate cartilage during longitudinal bone growth. J Bone Joint Surg Am 1987;69:162-173.
Iannotti JP: Growth plate physiology and pathology. Orthop Clin North Am 1990;21:1-17.
Question 77
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Lynch NM, Cofield RH, Silbert PL, Hermann RC: Neurologic complications after total shoulder arthroplasty. J Shoulder Elbow Surg 1996;5:53-61.
Question 78
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 79
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
REFERENCES: DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.
Question 80
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis? Review Topic

Explanation
Question 81
Which of the following occurs frequently after nonsurgical management of displaced intra-articular fractures of the calcaneus?
Explanation
Question 82
Four weeks after undergoing elective THA, an 80-year-old man is in the emergency department with sudden-onset right hip pain and an inability to bear weight after bending over in his garden.
Explanation
In Question 138, pain and swelling following a metal-on-metal large-head THA represent a classic presentation for a pseudotumor from metallosis secondary to either articular metal wear or trunnionosis. For this patient, infection should be ruled out with laboratory studies (erythrocyte sedimentation rate and C-reactive protein) and joint aspiration. Metal ion levels and metal artifact reduction sequence MR imaging or ultrasound would be helpful to confirm the diagnosis of pseudotumor. In Question 139, chronic hip pain following elective THA with an antecedent postsurgical wound constitutes a typical presentation for chronic periprosthetic infection. Aseptic loosening could be considered although the timeline is short; bloodwork and joint aspiration would be appropriate investigations. In Question 140, giving way of the knee suggests quadriceps muscle dysfunction likely related to prolonged pressure on the femoral nerve from retractors during a long revision case. The pattern of weakness does not fit a sciatic nerve palsy. In Question 141, the presentation is typical of a prosthetic dislocation, most of which occur during the early postsurgical period following THA.

Question 83
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 84
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent
Explanation
Question 85
What defect in collagen synthesis is caused by a lack of vitamin C?
Explanation
Question 86
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves Review Topic
Explanation
Question 87
A 47-year-old man who works as a carpenter reports a 12-month history of painful mechanical locking of his dominant elbow in the mid range of movement. He also has progressive pain at terminal extension that has not responded to medication, rest, and intra-articular cortisone injection. Active range of movement is from 35 degrees to 130 degrees, and he has full pronation and supination. The ulnar nerve is stable, and he has no subjective or objective neurologic dysfunction in the hand. Radiographs are shown in Figures 22a and 22b. What is the most appropriate treatment? Review Topic

Explanation
Question 88
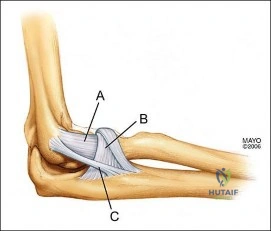
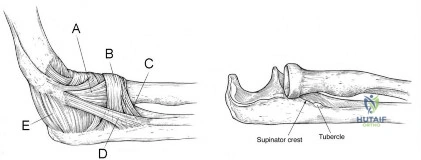
A 25-year-old athlete presents with symptoms attributed to injury to ligament D in Figure A. Which of the following symptoms and signs is characteristic of this injury? Review Topic
Explanation
PLRI can be diagnosed using the lateral pivot shift or posterolateral drawer. According to O’Driscoll, the elbow dislocates in 3 stages from lateral to medial (circle of Horii). Stage 1 involves disruption of the LUCL and partial/total disruption of the LCL complex (creating PLRI). Patients have pain with varus stress. Stage 2 includes disruption of the anterior capsule from incomplete elbow posterolateral dislocation. Stage 3 is divided into:
(a) Disruption of all soft tissues surrounding/ including the posterior MCL except for the anterior bundle. This bundle forms the pivot around which the elbow dislocates in a posterior direction by way of a posterolateral rotatory mechanism; and (b) complete disruption of the MCL.
O'Driscoll et al. describe PLRI diagnosed in 5 patients who had elbow dislocation using the posterolateral rotatory instability test, which they describe as being analogous to the test for lateral rotatory instability of the knee after ACL rupture. They believed the condition was laxity of the LUCL, which allowed transient rotatory subluxation of the ulnohumeral joint and secondary dislocation of the radiohumeral joint, without radio-ulnar joint dislocation. They recommended repair of the LUCL to eliminate PLRI.
Sanchez-Sotelo et al. retrospectively described 12 cases of direct repair and 33 ligamentous reconstructions for PLRI. 86% were satisfied with the procedure. Better results were obtained with patients with post-traumatic etiology, instability at presentation, and those with augmented reconstruction with tendon graft (compared with ligament repair alone).
Figure A shows structures on the lateral side of the elbow. The corresponding labels are seen in Illustration A. Illustration B shows the lateral pivot shift (also known as the posterolateral rotatory instability test).
Incorrect Answers:
Question 89
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result? Review Topic

Explanation
Question 90
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Explanation
sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH (“athlete’s heart”) from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm).
REFERENCES: Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436.
Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Pelliccia A, Culasso F, Di Paolo FM, et al: Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23-31.
Question 91
Denosumab, a monoclonal antibody used to treat osteoporosis, works through inhibition of
Explanation
Question 92
A 54-year-old woman sustained an elbow injury 3 months ago that was treated with open reduction and internal fixation. She now reports pain and limited elbow motion. Radiographs are shown in Figures 10a and 10b. Treatment should now consist of
Explanation
REFERENCE: Horii E, Nakamura R, Koh S, et al: Surgical treatment for chronic radial head dislocation. J Bone Joint Surg Am 2002;84:1183-1188.
Question 93
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 94
During surgical treatment of the most common variation of distal femoral "Hoffa" fractures, which of the following orientations for screw fixation should be used?

Explanation
Hoffa fractures are coronally oriented fractures of the femoral condyles, with most occurring in the lateral condyle. They are commonly associated with high-energy fractures of the distal femur and can often be overlooked during the assessment and treatment of distal femur fractures. Hoffa fractures are best evaluated using CT scans.
Nork et al. studied the association of supracondylar-intercondylar distal femoral fractures and coronal plane fractures. Of 202 supracondylar-intercondylar distal femoral fractures, they found coronal plane fractures were diagnosed in 38%. A coronal fracture of the lateral femoral condyle was involved more frequently than the medial condyle. Eighty-five percent of these coronal fractures involved a single lateral femoral condyle.
Holmes et al. looked at five cases of coronal fractures of the femoral condyle. All cases received open reduction and internal fixation with lag screws through a formal parapatellar approach. They reported good results with all fractures healing within 12 weeks without complications with final range of motion at least 0 degrees to 115 degrees.
Question 95
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
REFERENCES: Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 96
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 97
A 50-year-old patient underwent multiple debridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
A. clinical examination.
B. invasive pressure measurement.
C. arterial Doppler study.
D. MRI.
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow,
and an abnormality would be a late finding. 41
MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
45- Figures 1 and 2 show the MRI studies of a 35-year-old manual laborer with persistent wrist pain despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes of the midcarpal joint are noted. What is the most appropriate procedure for this condition?
A. Local vascularized bone graft
B. Proximal row carpectomy
C. Midcarpal fusion
D. Total wrist arthroplasty
The T1-weighted MRI reveals decreased signal that is consistent with avascular necrosis (AVN) of the capitate. Figure 2 demonstrates increased signal of the capitate consistent with edema. The etiology of AVN of the capitate may be related to trauma, abnormal interosseous vascular supply, and hypermobility. Surgical treatment is considered for patients who have had persistent symptoms despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes would be treated most appropriately with a salvage procedure. A midcarpal fusion is a motion-preserving salvage procedure and is the most appropriate option given to address the pain associated with the midcarpal arthritic changes. The alternative options are not appropriate for this patient. Local vascularized bone grafts are considered for situations in which no evidence of capitate collapse or arthritis is observed.
Question 98
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 99
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 100
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
REFERENCES: Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 47-55.
