Orthopedic Board Review MCQs: Elbow & Fracture Surgery | Part 144

Key Takeaway
This page provides Part 144 of a comprehensive OITE/ABOS Orthopedic Surgery Board Review. Featuring 100 high-yield, verified MCQs, it's meticulously modeled after actual board examinations. Designed for orthopedic residents and surgeons, this interactive quiz aids effective preparation for certification.
About This Board Review Set
This is Part 144 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 144
This module focuses heavily on: Elbow, Fracture.
Sample Questions from This Set
Sample Question 1: Autosomal dominant...
Sample Question 2: Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis...
Sample Question 3: Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population? Review Topic...
Sample Question 4: During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?...
Sample Question 5: Figures 38a and 38b...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 2
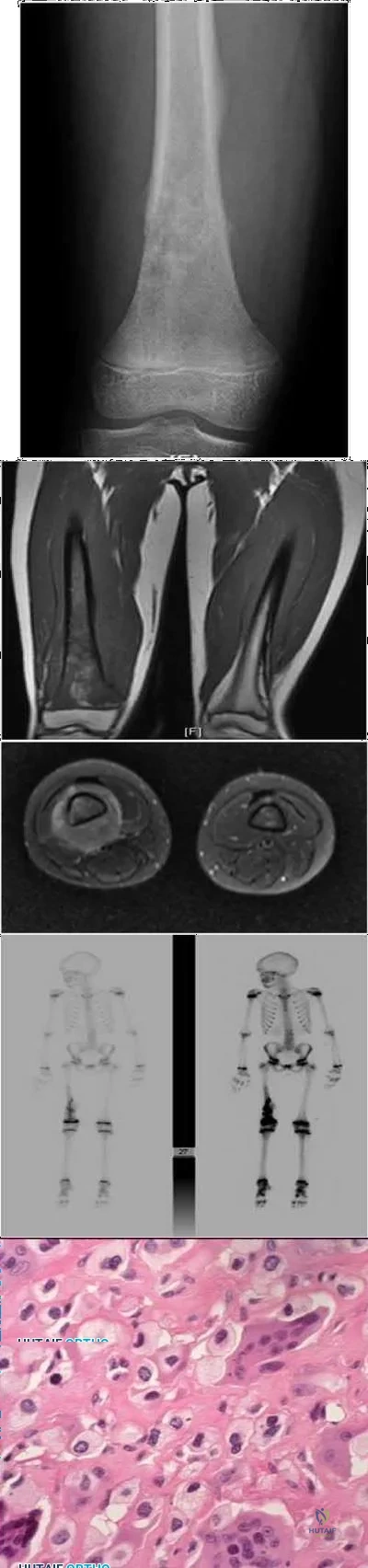
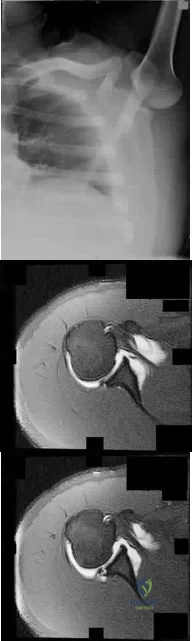
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 3
Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population? Review Topic
Explanation
Question 4
During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?
Explanation
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary bone healing and secondary bone healing takes place at tissue strain of 2-10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40% or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
Question 5
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 6
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?
Explanation
REFERENCES: Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Mealy K, Brennan H, Fenelon GC: Early mobilization of acute whiplash injuries. Br Med J 1986;292:656-657.
Question 7
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 8
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 9
A 17-year-old football player continues to have discomfort after sustaining a blow to his midthigh during a game 8 weeks ago. A plain radiograph is shown in Figure 13. What is the most appropriate management?
Explanation
REFERENCES: Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4:111-120.
Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Ryan JB, Wheeler JH, Hopkins WJ, et al: Quadriceps contusions: West Point update. Am J Sports Med 1991;19:299-304.
Question 10
What is the optimal biomechanical screw placement position to treat a waist-level scaphoid fracture?
Explanation
Dodds and associates looked at short (compared to long) scaphoid screws placed down the central axis in cadavers. A long screw placed along the central axis was significantly more stable when tested in all planes of motion about the wrist. McCallister and associates examined central placement and eccentric placement in a cadaver model. Central positioning produced 43% more stiffness and 113% more load (P < .01).
RECOMMENDED READINGS
Bedi A, Jebson PJ, Hayden RJ, Jacobson JA, Martus JE. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am. 2007 Mar;32(3):326-33. PubMed PMID: 17336838.View Abstract at PubMed
Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734. View Abstract at PubMed
McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am.2003 Jan;85-A(1):72-7.PubMed: 12533575.View Abstract at PubMed
RESPONSES FOR QUESTIONS 72 THROUGH 75

The figures listed above depict the scenarios described below. Please match the appropriate scenarios and figures.
Question 11
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
REFERENCES: Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Morrey BF: Difficult complications after hip joint replacement: Dislocation. Clin Orthop 1997;344:179-187.
Question 12
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 13
A 47-year-old man has left-sided motor weakness in the extensor digitorum longus and extensor hallucis longus, sensory loss in the lateral calf and dorsal foot, and no discernible reflex loss.
Explanation
Figures 72a and 72b are the T1-weighted MR images of a disk bulge. Disk bulges are common in asymptomatic people and are not predictive of pathology. Figures 72c and 72d show T1 MR images of a far lateral disk herniation at the L4-L5 level. This would affect the exiting or L4 nerve root. Radicular symptoms would occur at the L4 level. Figures 72e and 72f show an annular tear at the L4-L5 level. This pathology is associated with discogenic low-back pain. Figures 72g and 72h show the T1 MR images of a central lateral disk herniation at the L4-L5 level. This would affect the traversing or L5 nerve root. Radicular symptoms would occur at the L5 level.
RECOMMENDED READINGS
Jarvik JG, Hollingworth W, Heagerty PJ, Haynor DR, Boyko EJ, Deyo RA. Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine (Phila Pa 1976). 2005 Jul 1;30(13):1541-8; discussion 1549. PubMed PMID: 15990670.View Abstract at PubMed
Hoppenfeld S. Physical Exam of the Spine and Extremities. Stamford, CT: Appleton and Lange; 1995.
Madigan L, Vaccaro AR, Spector LR, Milam RA. Management of symptomatic lumbar degenerative disk disease. J Am Acad Orthop Surg. 2009 Feb;17(2):102-11. Review. PubMed PMID: 19202123.View Abstract at PubMed
Question 14
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 15
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
REFERENCES: Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 16
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
REFERENCES: Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 17
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?

Explanation
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. View Abstract at PubMed
Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. View Abstract at PubMed
Question 18
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 19
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 20
-A 75-year-old woman fell at home and sustained the injury seen in Figures 249a through 249c. What is the most appropriate treatment option?
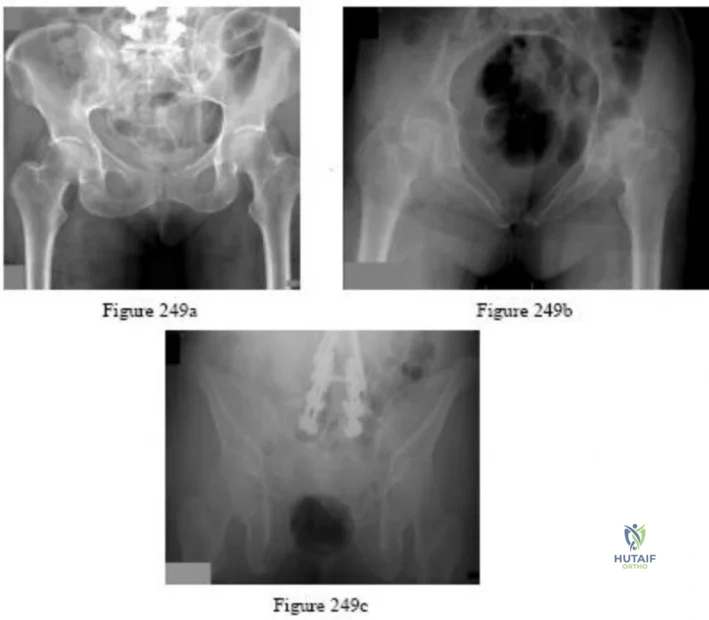
Explanation

Question 21
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 22
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
REFERENCES: Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Kasser JR (ed): Orthopedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 389-426.
Question 23
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Explanation
REFERENCES: Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
Dwars BJ,van den Broek TA, Rauwerda JA, et al: Criteria for reliable selection of the lowest level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
Question 24
A patient has persistent instability symptoms one year after ACL reconstruction. Radiographs and MRI show an intact graft with a femoral tunnel that enters the notch at the 12 o'clock position. These clinical findings have been associated with which of the following? Review Topic
Explanation
Early arthroscopic single-incision transtibial ACL reconstruction often resulted in femoral tunnels which were at the top of the notch (12 o:clock position), rather than at the anatomic origin on the wall. The resulting vertical graft often improved anteroposterior laxity (as tested with the Lachman) but was less able to provide rotational stability (as tested with the Pivot shift).
Lee et al. found a significant association between vertically positioned grafts and residual (postoperative) positive pivot shift tests. They also found patients with a vertically positioned graft had lower Lysholm satisfaction scores. They conclude more oblique positioning of the graft may have advantages in rotational stability, which in turn increase subjective patient satisfaction.
Yasuda et al. noted that vertical non-anatomic tunnel placement cannot completely restore normal rotatory stability in laboratory studies.
Incorrect
Question 25
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 26
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?
Explanation
REFERENCES: O’Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118.
Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
McDaniel WJ Jr, Dameron TB Jr: The untreated anterior cruciate ligament rupture. Clin Orthop 1983;172:158-163.
Question 27
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 28
A nonambulatory verbal 6-year-old child with spastic quadriplegic cerebral palsy has progressive bilateral hip subluxation of more than 50%. There is no pain with range of motion, but abduction is limited to 20 degrees maximum. An AP radiograph is seen in Figure 34. Management should consist of
Explanation
REFERENCES: Presedo A, Oh CW, Dabney KY, et al: Soft-tissue releases to treat spastic hip subluxation in children with cerebral palsy. J Bone Joint Surg Am 2005;87:832-841.
Miller F, Bagg MR: Age and migration percentage as risk factors for progression in spastic hip disease. Dev Med Child Neurol 1995;37:449-455.
Question 29
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Riley LH III, Frassica DA, Kostuik JP, Frassica FJ: Metastatic disease to the spine: Diagnosis and treatment. Instr Course Lect 2000;49:471-477.
Question 30
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of
recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 31
Figures below represent the radiographs obtained from a 37-year-old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?

Explanation
This patient has severe, uncorrectable varus deformity and pain from end-stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is
not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
Question 32
A 68-year-old woman stepped on a needle while walking barefoot 10 days ago. She is not certain but thinks it is imbedded in her foot, and she notes local tenderness at the puncture site and drainage. Her primary care physician has been treating her with oral antibiotics. A plain radiograph is shown in Figure 38. What is the best course of action?
Explanation
REFERENCES: Combs AH, Kernek CB, Heck DA: Orthopedic grand rounds: Retained wooden foreign body in the foot detected by computed tomography. Orthopedics 1986;9:1434-1435.
Markiewitz AD, Karns DJ, Brooks PJ: Late infections of the foot due to incomplete removal of foreign bodies: A report of two cases. Foot Ankle Int 1994;15:52-55.
Question 33
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?
Explanation
REFERENCES: Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
Vince KG: Why knees fail. J Arthroplasty 2003;18:39-44.
Question 34
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 35
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?
Explanation
5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority.
REFERENCES: Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 36
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 37
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?
Explanation
REFERENCES: Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Wascher DC, Dvirnak PC, DeCoster TA: Knee dislocation: Initial assessment and implications for treatment. J Orthop Trauma 1997;11:525-529.
Question 38
Which of the following cohorts of patients is at highest risk of a future anterior cruciate ligament (ACL) tear? Review Topic
Explanation
Question 39
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment? Review Topic

Explanation
option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform.
Question 40
After reduction and pinning, the radial pulse is absent by both palpation and Doppler. Capillary refill in the fingers appears normal. What is the most likely explanation?
Explanation
This is a classic extension-type supracondylar elbow fracture typically caused by a fall on an outstretched hand. The medial comminution of this fracture renders it predictably unstable and susceptible to varus malunion. Extra attention with fixation is required. In general, use of lateral-entry pins alone is effective for most supracondylar humeral fractures. The best technique for fixation with lateral-entry pins only involves maximization of pin separation at the fracture site, engaging sufficient bone in both the proximal segment and the distal fragment and using more than 2 lateral entry pins (if needed) for stability. In the presence of medial comminution, medial fixation also may be necessary.
Brachial artery spasm is the usual cause of absence of radial pulse if capillary refill is normal. Close postsurgical monitoring is warranted after reduction and pinning.
Question 41
Which of the following tumors have characteristic chromosomal translocations?
Explanation
REFERENCES: Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 42
Which of the following patients requires preoperative noninvasive cardiac testing?
Explanation
REFERENCES: Bushnell BD, Horton JK, McDonald MF, et al: Perioperative medical comorbidities in the orthopaedic patient. J Am Acad Orthop Surg 2008;16:216-227.
Auerback A, Goldman L: Assessing and reducing the cardiac risk of noncardiac surgery. Circulation 2006;113:1361-1376.
Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 105-113.

Question 43
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
REFERENCES: Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 165-201.
Question 44
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 45
A 61-year-old man reports right shoulder pain and loss of external rotation since having a seizure 5 months ago. MRI scans are shown in Figures 82a and 82b. What is the most appropriate treatment? Review Topic
Explanation
Question 46
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Explanation
flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb.
REFERENCES: Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 47
Figure 8a shows the clinical photograph of an 83-year-old woman who has an enlarging left forearm mass. MRI scans are shown in Figures 8b and 8c. What is the next most appropriate step in management?
Explanation
REFERENCES: Damron TA, Beauchamp CP, Rougraff BT, et al: Soft-tissue lumps and bumps. Instr Course Lect 2004;53:625-637.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 48
What is the most common complication after distal biceps tendon repair at the elbow?
Explanation
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
Question 49
A 25-year-old male is involved in an high-speed motor vehicle collision and sustains a closed femoral shaft fracture. During further evaluation, a CT scan of the chest/abdomen/pelvis reveals a non-displaced ipsilateral femoral neck fracture. Which of the following treatment options will most likely achieve anatomic healing of both fractures, mobilize the patient, and minimize the risk of complications?

Explanation
Question 50
A surgeon contemplates performing a hemiarthroplasty (HA) or total hip arthroplasty (THA) for an active, community ambulating 70-year-old female with a displaced femoral neck fracture. Which of the following is true for these options?
Explanation
There are a few differences between THA and HA performed in the setting of displaced FNF. THA has a higher dislocation rate, greater blood loss, requires a larger exposure than HA, and the operation is longer. HA often requires reoperation because of progressive acetabular erosion. Patient outcomes and function are greater following THA than HA.
Florschultz et al. reviewed current management of FNF. They concluded that CRIF / ORIF is indicated for displaced femoral neck fractures in younger individuals, select active elderly, and medically unfit patients. HA is indicated for lower demand ambulatory older patients. THA is indicated for the active elderly and those with preexisting acetabular disease.
Avery et al. reviewed 7-10 year results of an RCT comparing THA with HA. More HA patients had died during follow-up. All surviving patients had polyethylene wear (THA) and acetabular erosion (HA). They concluded that there was lower mortality and a trend towards superior function in patients with a THA in the medium term.
Hedbeck et al. performed a RCT comparing HA and THA. At 4 years, there was improved function and quality of life with THA. They recommend THA in elderly, lucid patients with a displaced FNF.
Incorrect Answers:
Question 51
Which stress fracture location is reported most frequently among ballet dancers?
Explanation
Stress fractures are a frequent overuse injury among professional ballet dancers. The most common location is at the proximal metaphyseal-diaphyseal junction of the second metatarsal. Repetitive stress injuries and fractures of the tibial sesamoid, tarsal navicular, and base of the fifth metatarsal occur among other athletes.
RECOMMENDED READINGS
O'Malley MJ, Hamilton WG, Munyak J, DeFranco MJ. Stress fractures at the base of the second metatarsal in ballet dancers. Foot Ankle Int. 1996 Feb;17(2):89-94. PubMed PMID: 8919407. View Abstract at PubMed
Micheli LJ, Sohn RS, Solomon R. Stress fractures of the second metatarsal involving Lisfranc's joint in ballet dancers. A new overuse injury of the foot. J Bone Joint Surg Am. 1985 Dec;67(9):1372-5. PubMed PMID: 4077907. View Abstract at PubMed
Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int. 2006 Sep;27(9):750-7. Review. PubMed PMID: 17038292. View Abstract at PubMed
Question 52
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999,
pp 247-263.
Question 53
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 54
Dislocation following primary total hip arthroplasty is more likely to occur in which of the following situations?
Explanation
REFERENCE: Berry DJ: Dislocation, in Steinberg ME (ed): Revision Total Hip Arthroplasty. Philadelphia, PA, 1999, pp 463-482.
Question 55
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
REFERENCES: Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Lemos MJ, Albert J, Simon T, et al: Radiographic analysis of femoral interference screw placement during ACL reconstruction: Endoscopic versus open technique. Arthroscopy 1993;9:154-158.
Question 56
What malignant disease most commonly develops in conjunction with chronic osteomyelitis?
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 57
A 26-year-old man is involved in a high-speed motorcycle accident. He sustains a grade IIIB open tibia fracture. Examination reveals a large soft-tissue defect and an insensate foot. What is the expected outcome in this scenario? Review Topic
Explanation
Question 58
If the quality of the tendon is poor at the lateral attachment of a partial articular side rotator cuff tear (more than 6 mm of footprint exposure or greater than 50% thickness), what should the surgeon do? Review Topic
Explanation
Question 59
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
REFERENCE: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 458.
Question 60
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 61
Figures 6a and 6b are the radiographs of a thin 23-year-old man who sustained a closed injury to his left arm in a fall. He has no other injuries and his

Explanation
Question 62
A 43-year-old man who works as a plumber has a painful stiff elbow in his dominant arm. He notes that while he recalls no single event of injury, he thinks the many years of pulling wrenches and soldering pipes have resulted in his problem. He reports that he has pain with any motion in bending his arm and can no longer straighten his elbow. Examination reveals generalized swelling of the elbow, both medial and lateral with a range of motion that lacks 45 degrees of extension and flexes only to 110 degrees. Pronation and supination are also limited to 45 degrees. Audible crepitus is perceived but there is no instability. Radiographs reveal advanced osteoarthritis at the radiocapitellar and ulnohumeral joints with complete loss of articular cartilage. What is the most appropriate initial treatment option? Review Topic
Explanation
must respect the physical demands of the patient while trying to preserve joint motion and function with tolerable symptoms. Osteophyte resection and capsular release have offered many patients significant improvement in their symptoms while allowing them to return to most activities. The osteophyte resection and releases can be done effectively by an open or arthroscopic approach. Whereas total elbow arthroplasty would likely result in better and more thorough pain relief, it would not tolerate the occupational demands of this individual. There is no role for physical therapy initially in the face of advanced, painful arthritis associated with long-standing fixed joint contractures. Elbow fusion results in severe loss of function and its indication is rare and usually considered in the face of unmanageable sepsis. Radial head resection may improve symptoms related to the radial capitellar arthritis but would not improve range of motion or end range impingement pain. Also, radial head resection should be avoided in heavy laborers with elbow arthritis because it would lead to increased loads across the arthritic ulnohumeral joint.
Question 63
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 64
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 65
A patient is seen in the emergency department after a motor vehicle accident. He reports right hip pain and chest pain. Initial hypotension has responded to a fluid bolus. Radiographs reveal a posterior hip dislocation with a small posterior acetabular wall fracture. You are called at home and informed of the findings. What is the next most appropriate step in management? Review Topic
Explanation
Question 66
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation

Question 67
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 68
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 69
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
Explanation
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
Question 70
Which of the following is a recognized consequence of hip fusion?
Explanation
REFERENCES: Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Sponseller PD, McBeath AA, Perpich M: Hip arthrodesis in young patients: A long-term follow-up study. J Bone Joint Surg Am 1984;66:853-859.
Question 71
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 72
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 73
A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?
Explanation
REFERENCES: Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.
Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.
Question 74
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of
Explanation
REFERENCES: Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine
1992;17:1137-1143.
Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Farey ID, McAfee PC, Davis RF, Long DM: Pseudarthrosis of the cervical spine after anterior arthrodesis: Treatment by posterior nerve root decompression, stabilization, and arthrodesis.
J Bone Joint Surgery Am 1990;72:1171-1177.
Question 75
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and
Explanation
Question 76
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 77
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma.
REFERENCES: Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033.
Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Dormans JP, Rang M: Fractures of the olecranon and radial neck in children. Orthop Clin North Am 1990;21:257-268.
Question 78
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 79
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 80
Ewing’s sarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Wold LA, et al: Ewing’s Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 81
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
REFERENCES: Fukuda K, Craig EV, An KN, et al: Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-439.
Bosworth B: Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-225.
Question 82
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 83
A 10-year-old boy has 2 months of right knee pain that started at summer camp. The patient denies constitutional symptoms. There is no lymphadenopathy present. CT of the chest shows no signs of metastatic disease. Imaging studies and biopsy results are shown in Figures A-E. What is the most likely diagnosis?
Explanation
Treatment for osteosarcoma includes neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy.
Question 84
Figures 1 and 2 are the clinical photographs of a 36-year-old woman who cannot fully extend the metacarpophalangeal (MP) joints of her long and ring fingers 9 months after the removal of a plate from the proximal radius via a dorsal approach. What is the most likely cause of this problem?

Explanation
Plating of the proximal radius from a dorsal or Thompson approach (between the extensor carpi radialis brevis and extensor digitorum communis) allows complete visualization of the PIN through the supinator. Going through the same incision from proximal to distal produces a scar-filled proximal approach, and it is not uncommon to drift ulnarly and injure an individual nerve to the extensor digitorum communis muscle, resulting in the deformity seen in Figures 1 and 2.Postsurgical tendon adhesions rarely involve only 2 tendons. Complete tendon lacerations are rare at this level in the proximal forearm, as is a complete laceration of the PIN. Neuropraxias are common but usually resolve after 3 months. The gossamer-thin branch of the PIN to the EDC can be easily damaged in scar tissue, resulting in an inability to fully extend the MP joints of the long and ring fingers. The proprius tendons allow the patient to fully extend the index and little finger MP joints. Connecting the EDC of the long finger to the extensor indicis proprius and the EDC of the ring finger to the extensor digiti quinti proprius can correct the deformity. To avoid the problem, the surgeon should start the incision distally in normal anatomy, and the interval between the mobile wad and the digital extensors will be more easily found.
Question 85
A 47-year-old male with a history of a Putti-Platt procedure 20 years ago presents with right shoulder pain with decreased range-of-motion. Radiograph is shown in Figure A. What is the most accurate diagnosis? Review Topic

Explanation
Post-stabilization procedure arthritis is thought to occur due to changes in contact loading in the shoulder joint due to fixing the joint in an incongruent posistion. It can be severe and debilitating, and lead to arthroplasty as a salvage procedure. The Putti-Platt procedure involves a division of the subscapularis tendon and anterior capsule, and realignment of the lateral tendon stump and capsule sewn into the anterior glenoid neck capsular insertion. The "pants-over-vest" style of repair is then finished by sewing the medial tendon stump into the tuberosity, so that external rotation is significantly limited by the soft tissue imbrication. There is no coracoid transfer for this stabilization procedure.
Bigliani et al. reported on a series of similar patients who developed arthritis following surgery for recurrent glenohumeral dislocation. Authors have theorized that instability repair may excessively tighten the joint in one direction and cause a fixed subluxation in the direction opposite from the side of repair, leading to severe degenerative arthritis due to inappropriate contact loading. 77% of patients following arthroplasty after post-capsulorrhaphy arthropathy had an excellent or satisfactory outcome, with improved pain and range of motion.
Figure A demonstrates severe osteoarthrosis of the affected shoulder, with significant joint space narrowing, periarticular osteophyte formation, and subchondral sclerosis.
Incorrect Answers:
performed for traumatic dislocation, but the best answer choice for this stem is Answer 2.
Question 86
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?
Explanation
REFERENCES: Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Resnick D, Walter RD, Crudale AS: Bilateral dysplasia of the scapular neck. Am J Roentgenol 1982;139:387-390.
Question 87
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
REFERENCE: Hayes WC, Myers ER: Biomechanical considerations of hip and spine fractures in osteoporotic bone, in Springfield D (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 431-438.
Question 88
Figures 111a and 111b show axial MRI scans of a 24-year-old man who injured his right shoulder several years ago and now reports continued difficulty with the shoulder and has pain with activity. He reports that when the injury occurred, he felt that his shoulder "popped" but he never required closed reduction. He wore a
Explanation
Question 89
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 90
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
Explanation
Question 91
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 92
What is the most common bone tumor in the hand?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Kuur E, Hansen SL, Lindequist S: Treatment of solitary enchondromas in fingers. J Hand Surg Br 1989;14:109-112.
Question 93
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 94
A 30-year-old man has had leg pain for 6 months. A lesion is identified in the proximal femur and biopsy it taken. Histology is shown in Figure A and is consistent with a low-grade intramedullary osteogenic sarcoma. Additional imaging studies confirm that this is an isolated lesion with no metastasis. What is the standard treatment for this type of lesion?
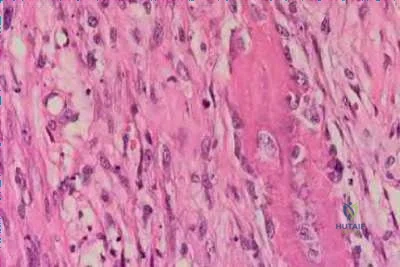
Explanation
Choong et al. reviewed the long term follow-up of 20 patients diagnosed with low grade osteogenic sarcoma and found the 5 year survival rate was 90% and at 10 years was 85%. Local recurrence is a key feature in most cases and is typically the result of inadequate surgical margins frequently arising from initial misdiagnosis. Although amputation generally is successful for primary and recurrent tumors, limb salvage surgery is a definite option.
Kurt et al reviewed 80 well-differentiated osteosarcomas. They found local excision was almost always associated with recurrence. Wide excision was
almost never followed by recurrence. The recurrent tumor was a high-grade, conventional osteosarcoma in 15% of the patients, and this was associated with a poor prognosis. They recommend wide excision as the treatment of choice for this very rare variant of osteosarcoma.
A 32-year-old male sustains a the injury shown in Figure A after a high-speed motor vehicle collision. Which factor has been found to have the highest direct correlation with severe heterotopic ossification after traumatic knee dislocation?

Injury Severity Score (ISS )
Glascow Coma Scale (GCS )
Timing of knee reconstruction
Number of ligaments reconstructed
Open ligament reconstruction
Figure A shows a knee dislocation with cruciate ligament avulsion injuries. Development of significant heterotopic ossification (HO) formation has been shown to be most directly correlated to the ISS score.
Mills and Tejwani looked at multiple variables including injury severity score
( ISS), Glascow coma scale (GCS), closed head injury (CHI), timing of surgery (> or < 3 weeks) and type of surgery (open vs. arthroscopic, number of ligaments reconstructed) in its relation to the formation of HO following knee dislocation. In the final group the sensitivity and specificity of the ISS in relation to HO formation was 100%, while presence of CHI had a specificity of 97 %. Timing, type of surgery and approach did not influence HO formation.
A 52-year-old male presents with 6 months of swelling and pain in his leg. He states the lesion has not changed in size for several months and doesn't bother him. He is otherwise healthy and has no other complaints. Representative photograph and MRI are shown in Figures A through C. What is the best initial step in his management?
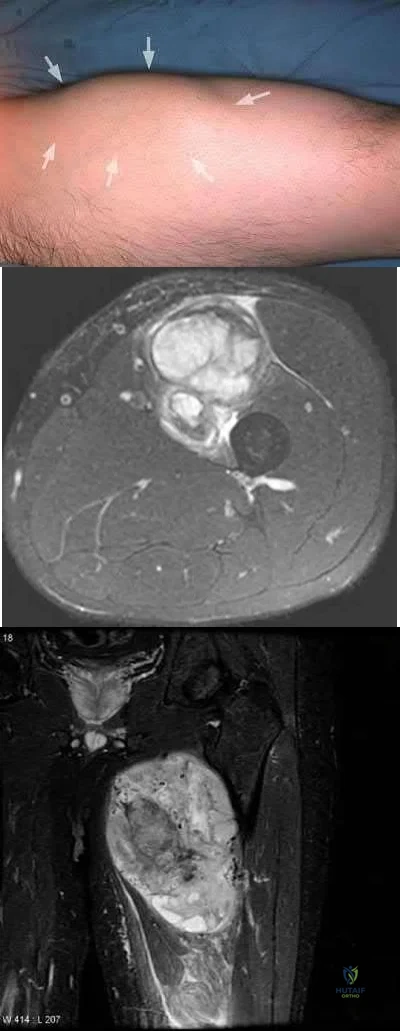
Follow-up in 6 months with repeat radiographs
Biopsy
Marginal excision
Radiation therapy
Neoadjuvant chemotherapy and wide excision
The initial step in management of a patient presenting with a large soft tissue mass deep to the fascia is to obtain a tissue diagnosis, via biopsy. Initiation of treatment prior to tissue diagnosis is inappropriate and can result in significant patient morbidity and potential mortality. While some soft tissue sarcomas may benefit from chemotherapy, this cannot be initiated prior to diagnosis.
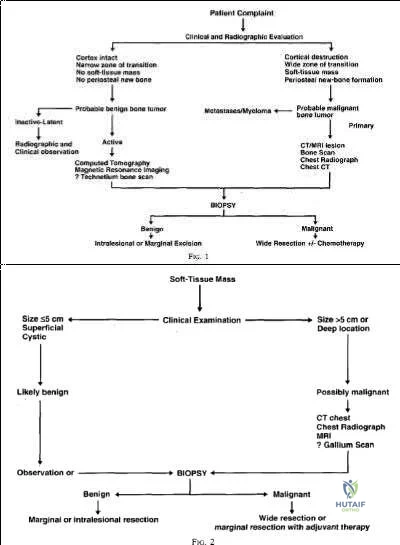
Radiation therapy is used in the treatment of soft tissue sarcoma, but again, only after tissue diagnosis. Peabody et al review the appropriate evaluation and staging for musculoskeletal neoplasms and present flow-charts useful in the work-up of bone (Illustration A) and soft tissue (Illustration B) neoplasms. Skrzynski et al performed a comparison of outpatient core-needle biopsy with open surgical biopsy for musculoskeletal tumors. They found the diagnostic accuracy of core-needle biopsy was only 84% with many samples yielding no or different histological samples when compared to final resected specimens. They conclude that while core-needle biopsy is significantly less expensive
than surgical biopsy ($1106 vs. $7234), there is higher concern for sampling error or general diagnostic inaccuracy associated with a core-needle biopsy compared to open biopsy, the "gold standard".
What is the appropriate treatment for a 10-year-old boy with Ewing's sarcoma isolated to the proximal femur?
Neoadjuvant chemotherapy and surgical excision
Neoadjuvant chemotherapy, surgical excision, and radiation therapy
Neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy
Neoadjuvant radiation therapy and surgical excision
Surgical excision and hormonal therapy
Ewing's sarcoma is a malignant small round blue cell neoplasm which has a predilection for long tubular bones, pelvis, and ribs. The radiographic appearance of "onion-skinning" seen in illustrations A and B is due to the body's periosteal reaction. Illustration C shows the large soft tissue extraosseous mass characteristic for Ewing's sarcoma. Finally, Illustration D shows the histology where the multiple small round blue neoplastic cells are seen.
Ewing's sarcoma is most commonly treated with neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy - in particular for tumors located in bones which can be easily resected and reconstructed. For large tumors in areas which either cannot be completely excised or where excision is associated with significant morbidity, some centers consider chemotherapy and radiation therapy without surgical excision. There is a current trend towards surgical resection and away from irradiation for Ewing's sarcoma even though it is radiosensitive, because of the risk of secondary malignancy and growth disturbance due to radiation.
Pierz et al review many of the common bone tumors including Ewing's sarcoma and discuss the relevant diagnostic factors as well as specific treatment protocols for each tumor.

A 30-year-old female presents with a painful posterior knee mass. The mass gets larger and more painful with activity. Examination reveals a boggy soft tissue mass about her knee. Radiograph and MRI are shown in Figures A and B. What is the most likely diagnosis?
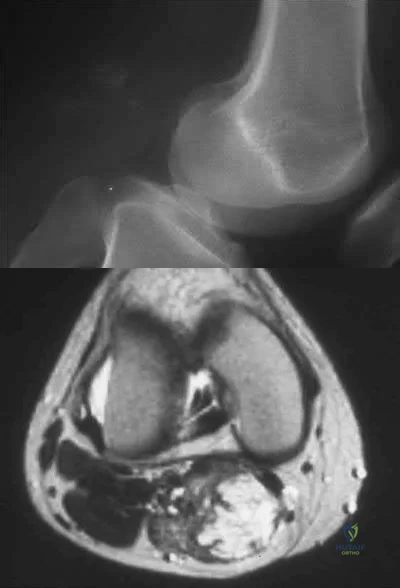
Synovial sarcoma
Hemangioma
Lipoma
Parosteal osteosarcoma
Pigmented villonodular synovitis (PVNS )
This patients history, physical exam, and imaging studies are suggestive of a hemangioma. Pain in hemangiomas is thought to occur due to vascular engorgement secondary to activity and increased blood flow to the lesion. The calcification on the plain radiograph and the fat of the T1 MRI are diagnostic for hemangioma. Current treatment for symptomatic hemangiomas includes some combination of sclerotherapy or vascular coiling, with surgical excision
reserved for few cases. The two attached reviews by Gilbert et al and Damron et al review the history, diagnosis, treatment, and controversial issues in soft tissue sarcomas and benign sarcoma like conditions such as hemangiomas.
Current treatment for soft tissue sarcomas includes radiotherapy and surgical excision. While many centers in the world use chemotherapy for soft tissue sarcomas, the data supporting its use is quite limited and likely too controversial to be tested. With regard to the other answer choices, synovial sarcoma and lipoma can show calcification on radiographs, but they are usually not painful and image differently on T1 MRI. Parosteal osteosarcoma typically occurs in this location (posterior distal femur) but occurs as a lesion stuck on the bone. PVNS can have a similar appearance on imaging, but doesn't cause this type of pain.
Question 95
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 96
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 97
-A 15-year-old boy underwent open reduction and internal fixation for a tibial tubercle fracture. The next morning he had dramatically increased pain, hypotension, ascending rash, and fever to 103°F. What is the most appropriate course of action?
Explanation

Question 98
Which of the following factors has been shown to be the strongest predictor of screw cutout of a dynamic compression hip screw used for an intertrochanteric femur fracture?

Explanation
Baumgaertner et al reported that he had no screws cut out if the tip-apex distance was less than 25mm. Tip-apex distance was the strongest predictor of cutout. Increasing age of the patient, poor reduction, use of a high angle sideplate, and unstable fracture were weaker predictors of cutout.
Kyle et al demonstrated that obtaining an anatomic reduction when using a sliding hip screw with intertrochanteric fractures leads to the best radiographic and clinical outcomes.
Question 99
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 100
-Figure 235 is the radiograph of a 75-year-old woman who is seen in the emergency department following a low-energy fall. What is the most appropriate treatment based on her radiographic findings?
Explanation

