OITE & ABOS Orthopedic Board Exam MCQs: Spine, Trauma, Knee - Part 142

Key Takeaway
This page presents Part 142 of a comprehensive orthopedic board review series, featuring 100 verified, high-yield multiple-choice questions. Modeled after OITE and AAOS exams, it is designed for orthopedic residents and surgeons seeking rigorous preparation for their board certification assessments.
About This Board Review Set
This is Part 142 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 142
This module focuses heavily on: Deformity, Fracture, Knee, Spine, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: Pedicle subtraction osteotomies (PSO) are commonly performed in the lumbar spine to treat sagittal imbalance. What is the most common complication following a PSO in the lumbar spine? Review Topic...
Sample Question 2: Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The find...
Sample Question 3: A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?...
Sample Question 4: A 41-year-old woman has medial-sided knee pain and varus deformity. Her radiographic findings are consistent with isolated medial compartment osteoarthritis. Her pain persists despite nonsurgical therapy. A medial-sided, opening-wedge osteo...
Sample Question 5: Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Pedicle subtraction osteotomies (PSO) are commonly performed in the lumbar spine to treat sagittal imbalance. What is the most common complication following a PSO in the lumbar spine? Review Topic
Explanation
Question 2
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of
Explanation
REFERENCES: Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516.
Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228.
Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Beaty JH, Austin SM, Warner WC, et al: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop
1994;14:178-183.
Question 3
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Explanation
REFERENCES: van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437.
Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 4
A 41-year-old woman has medial-sided knee pain and varus deformity. Her radiographic findings are consistent with isolated medial compartment osteoarthritis. Her pain persists despite nonsurgical therapy. A medial-sided, opening-wedge osteotomy with locking plate fixation is performed. What factor is most associated with delayed union or nonunion of the osteotomy?
Explanation
Many factors can lead to delayed union or nonunion after medial opening-wedge high tibial osteotomy; the factor most associated with delayed union or nonunion is smoking. Other factors include obesity and unstable lateral hinge fractures, but to a lesser extent. An accelerated weight-bearing protocol has no effect on union. The use of locking screws should increase construct stability and is not associated with osteotomy delayed union or nonunion.

Question 5
Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?
Explanation
The influence of sagittal balance on outcomes following fusion-based procedures for degenerative conditions of the lumbar spine has only recently been appreciated. Restoration of sagittal spinal balance improves low-back-pain outcomes and quality of life. Sagittal spinal balance has not been shown to relieve neurogenic claudication attributable to spinal stenosis.
RECOMMENDED READINGS
Li Y, Hresko MT. Radiographic analysis of spondylolisthesis and sagittal spinopelvic deformity. J Am Acad Orthop Surg. 2012 Apr;20(4):194-205. doi: 10.5435/JAAOS-20-04-194. Review. PubMed PMID: 22474089. View Abstract at PubMed
Korovessis P, Repantis T, Papazisis Z, Iliopoulos P. Effect of sagittal spinal balance, levels of posterior instrumentation, and length of follow-up on low back pain in patients undergoing posterior decompression and instrumented fusion for degenerative lumbar spine disease: a multifactorial analysis. Spine (Phila Pa 1976). 2010 Apr 15;35(8):898-905. doi: 10.1097/BRS.0b013e3181d51e84. PubMed PMID: 20354466. View Abstract at PubMed
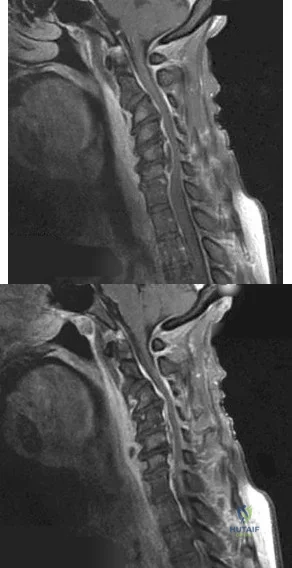
CLINICAL SITUATION FOR QUESTIONS 99 AND 100
Figures 99a and 99b are MR images of a 59-year-old man with a history of intravenous (IV) drug abuse who arrives at the emergency department with malaise and fever. Upon admission, the patient's temperature is 38.9°C, his white blood cell count is 17000/µL (reference range [rr], 4500-11000/µL), his erythrocyte sedimentation rate is 98 mm/h (rr, 0-20 mm/h), and his C-reactive protein level is 45 mg/L (rr, 0.08-3.1 mg/L). He is admitted to the medical service to evaluate the source of his fevers. On hospital day 1, the patient reports weakness in his left arm and leg. Blood cultures are positive for methicillin-resistant Staphylococcus aureus.
A B
Question 6
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 7
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
REFERENCES: Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 8
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 43.
Question 9
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
REFERENCES: Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496.
Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 10
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 11
A 24-year-old man sustained a bilateral C5-6 facet dislocation in a car accident and was intubated at the scene. He remains sedated in the intensive care unit
Explanation
Question 12
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group? Review Topic

Explanation
Question 13
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?
Explanation
REFERENCES: Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Paiement GD: Prevention and treatment of venous thromboembolic disease complications in primary hip arthroplasty patients, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 331-335.
Question 14
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
REFERENCES: Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
Mann RA, Mann JA: Keratotic disorders of the plantar skin. Instr Course Lect 2004;53:287-302.
Question 15
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?
Explanation
REFERENCES: Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101.
McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk?
J Bone Joint Surg Br 2000;82:200-203.
Keating JF, Orfaly R, O’Brien PJ: Knee pain after tibial nailing. J Orthop Trauma
1997;11:10-13.
Question 16
A 70-year-old healthy man had total knee arthroplasty 18 years ago, and it now is painful. Radiographs reveal aseptic loosening and the range of motion before surgery is 15 to 85 degrees. The strongest indication for performing a tibial tubercle osteotomy to aid in exposure in his knee would be
Explanation

Question 17
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
specific to this pathology.
Question 18
An active 66-year-old man who underwent total shoulder arthroplasty 3 years ago now reports pain. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein. Intraoperative frozen section reveals greater than 10 white blood cells per high power field on two slides and the Gram stain reveals gram-positive cocci in clusters. What is the most appropriate surgical treatment to eradicate the infection and maintain function? Review Topic
Explanation
Question 19
A 7-year-old male is struck by a motor vehicle while crossing the street and suffers an open tibia fracture with a crush injury of the ipsilateral foot. After multiple attempts at limb salvage, the family and treating surgeon elect to proceed with a knee disarticulation. What complication of pediatric amputations is avoided with a knee disarticulation as opposed to a transtibial amputation?

Explanation
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
Question 20
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 21
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
REFERENCES: Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45.
Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369.
McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Brundage SI, McGhan R, Jurkovich GJ, et al: Timing of femur fracture fixation: Effect on outcome in patients with thoracic and head injuries. J Trauma 2002;52:299-307.
Question 22
What is the most common turf toe mechanism of injury?
Explanation
Turf toe, or capsuloligamentous injury to the first MTP joint, most commonly is caused by an axial load being applied to a fixed, dorsiflexed great toe with the heel off the ground. The external force causes further dorsiflexion of the great toe, leading to injury to the capsuloligamentous complex. A less common mechanism of turf toe is hyperplantarflexion of the great toe with valgus stress, which is seen in beach volleyball players.
RECOMMENDED READINGS
Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. View Abstract at PubMed
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
Question 23
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 24
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Hollingshead WH: Anatomy for Surgeons: The Back and Limbs, ed 2. Hagerstown, MD, Harper & Row, 1969, pp 607-609.
Question 25
A 78-year-old woman has had activity-limiting cervical pain and occipital headaches for the past 4 years. Management consisting of injections, analgesics, and part-time collar wear has provided temporary relief. Examination reveals that her neck pain seems to be primarily located immediately below the skull and is aggravated by long periods of sitting and rotation of her head. Plain radiographs are shown in Figures 36a through 36c. What is the best course of action?
Explanation
REFERENCES: Ghanayem AJ, Leventhal M, Bohlman HH: Osteoarthrosis of the atlanto-axial joints: Long-term follow-up after treatment with arthrodesis. J Bone Joint Surg Am 1996;78:1300-1307.
Star MJ, Curd JG, Thorne RP: Atlantoaxial lateral mass osteoarthritis: A frequently overlooked cause of severe occipitocervical pain. Spine 1992;17:S71-S76.
Question 26
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 27
An athletic 55-year-old man reports a painless mass in the anterior aspect of the thigh that appeared 3 weeks ago and has not changed in size. The patient denies any history of trauma. Examination reveals a firm, well-defined nontender mass in the anterior thigh and no inguinal adenopathy or cutaneous changes. Plain radiographs are unremarkable. T1- and T2-weighted MRI scans are shown in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 28
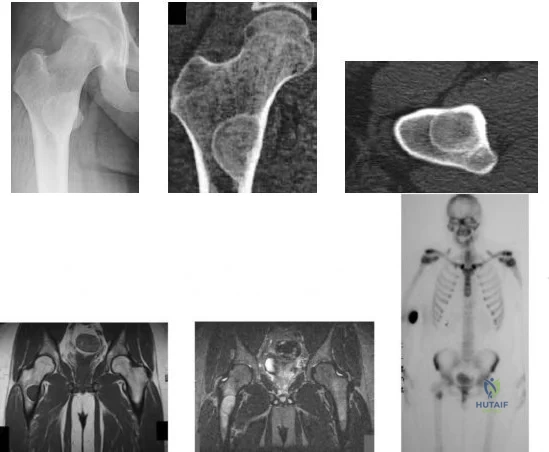
-Figures a through f are the radiograph, CT scan, MRI scan, and bone scan of a 28-year-old woman with a newly diagnosed breast carcinoma who underwent a bone scan for staging. She has no hip pain but a lesion is noted. What is the best next treatment step?
Explanation
Question 29
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 30
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal
Explanation
REFERENCES: Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Habernek H, Weinstabl R, Kdolsky R, et al: Volar lunate fracture-dislocations of the wrist: Case report for two patients treated with external frame and internal open reduction. J Trauma 1998;45:975-978.
Question 31
- Which of the following nerves supply the muscles on each side of internervous plane identified when performing the anterior (Smith-Petersen) approach to the hip?
Explanation
Question 32
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure 2. What is the most appropriate management at this time?
Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 33
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of
Explanation
REFERENCES: Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Cavolo DJ, Sherwood GF: Dupuytren’s disease of the plantar fascia. J Foot Surg 1982;21:12-15.
Question 34
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 35
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 36
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
Explanation
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
Question 37
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
Explanation
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Question 38
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
REFERENCES: McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 39
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
REFERENCE: Parvizi J, Sullivan TA, Trousdale RT, Lewallen DG: Thirty-day mortality after total knee arthroplasty. J Bone Joint Surg Am 2001;83:1157-1161.
Question 40
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 41
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Explanation
back to this question next question
Question 42
A 60-year-old woman sustains the injury shown in Figure 75. Prior to her injury, she lived independently and was a community ambulator without need for any assistive devices. What treatment will give her the greatest long-term painless hip function with the lowest reoperation rate?

Explanation
Question 43
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.
Question 44
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
REFERENCES: Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
Teitz CC, Hu SS, Arendt EA: The female athlete: Evaluation and treatment of sports-related problems. J Am Acad Orthop Surg 1997;5:87-96.
Question 45
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury? Review Topic

Explanation
Question 46
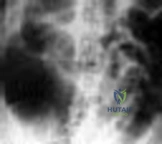
Figure below shows the abdominal radiograph obtained from a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 47
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to
Explanation
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 48
- Radiographs of a 20-year-old college athlete who sustained an injury to the ankle reveal no fractures or widening of the ankle mortise. Examination shows swelling at the ankle region and pain with medial lateral compression of the distal tibiofibular joint. Which of the following studies would best help in confirming a diagnosis?
Explanation
2 and 3 are occasionally utilized when there is questionable involvement of surrounding bone or tendons. 4 rarely indicated for acute ankle sprain but can help in the diagnosis of RSD following ankle injury.
Question 49
What portion of the pitching phase creates forces approaching the tensile limit of the medial ulnar collateral ligament of the elbow? Review Topic
Explanation
Fleisig et al. were among the first to elucidate the elbow and shoulder kinetics in healthy adult pitchers using high-speed motion capture analysis. Inability to generate sufficient elbow varus torque may result in medial tension, lateral compression, or posteromedial impingement injury.
According to Lynch et al. the late cocking phase of the overhand throw places a marked valgus moment across the medial elbow. This repetitive force reaches the tensile limits of the medial collateral ligament, subjecting it to microtraumatic injury and attenuation. The anterior bundle of the medial collateral ligament has been identified as the primary restraint to valgus load and is the focus of reconstruction.
Incorrect Responses:
1,4,5: The medial elbow forces are less during these phases. 4: Ball release is not one of the 5 phases of throwing and marks the end of the acceleration and beginning of deceleration phase.
Question 50
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
Question 51
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
REFERENCES: Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Henry R, Goletz B, Williamson C: Lateral release in patello-femoral subluxation. Am J Sports Med 1986;14:121.
Question 52
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
REFERENCES: Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Eilber FC, Rosen G, Nelson SE, et al: High-grade extremity soft tissue sarcomas: Factors predictive of local recurrence and its effect on morbidity and mortality.
Ann Surg 2003;237:218-226.
Question 53
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
REFERENCES: Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
Whitesides TE Jr, Heckman MM: Acute compartment syndrome: Update on diagnosis and treatment. J Am Acad Orthop Surg 1996;4:209-218.
Question 54
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
REFERENCE: Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 55
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
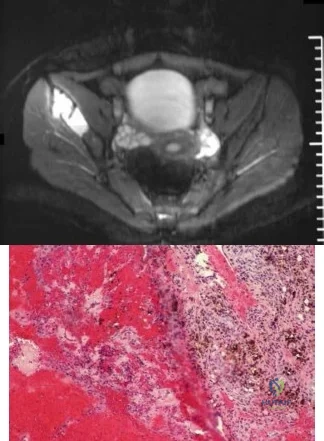
Question 56
Figures 25a through 25c are the axial T1 and postcontrast MRI scans and biopsy specimen of a 35-yearold man with a painless right thigh mass. He noticed the mass about 2 weeks ago and is unsure if it has changed in size. Which translocation most commonly is associated with this type of tumor?
Explanation
Question 57
A 23-year-old man has had heel pain and fullness for the past several months. He reports that initially the pain was present only with activity, but more recently the pain has become constant. Figures 53a through 53d show a radiograph, a bone scan, and T2-weighted and gadolinium MRI scans. What is the most likely diagnosis?
Explanation
bone cyst.
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Dorfman HD, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1998, pp 855-879.
Question 58
Which of the following nutraceuticals has been associated with perioperative bleeding?
Explanation
REFERENCES: Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776.
Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Bebbington A, Kulkarni R, Roberts P: Ginkgo biloba: Persistent bleeding after total hip arthroplasty caused by herbal self-medication. J Arthroplasty 2005;20:125-126.
Question 59
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 60
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 61
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 62
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by Review Topic
Explanation
Question 63
Moderate distance running has what effect on knee articular cartilage in asymptomatic distance runners?
Explanation
Question 64
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 65
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
REFERENCES: Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears.
Am J Sports Med 2005;33:1405-1417.
Fukuda H: The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br 2003;85:3-11.
Question 66
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
REFERENCE: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 67
Figures 15a and 15b are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared to traditional arthroscopic techniques when evaluating which outcome?
Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the 2 techniques.

CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 17
Figure 16 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop," and then he needed help walking off the field. His knee is visibly swollen.
Question 68
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Explanation
have been performed to offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
Question 69
A 25-year-old patent underwent anterior cruciate reconstruction (ACL) surgery 6 months ago. He returns to clinic with persistent instability. Physical examination reveals full range of motion of the knee. Additional tests show a 1A Lachman, 2+ pivot shift, negative external rotation dial, negative reverse pivot shift and negative McMurray. His radiographs are shown in Figure A. What is the likely cause of his persistent symptoms? Review Topic

Explanation
An anterior cruciate reconstruction (ACL) surgery with vertically placed grafts will result in persistent knee instability. Complaints will be mainly related to activities that require twisting or cutting movements. Physical examination will likely reveal a positive pivot shift exam due to the failure to reconstruct the posterolateral bundle of the ACL. Current standards for anatomic ACL reconstruction stress the importance of more horizontal graft placement (for example, 10:30 in a right knee vs 1:30 in the left knee). This allows for more rotational stability, while maintaining anterior stability. Improper femoral graft placement is one of the most common reasons for ACL revision surgery.
Noyes et al. looked at patients undergoing revision ACL surgery with the use of patellar bone-tendon-bone (BTB) autograft. They showed the rate of graft failure to be three times higher than their reported failure rate after primary ACL reconstructions.
Driscoll et al. performed a biomechanical study comparing 2 femoral tunnel locations in anatomic single-bundle anterior cruciate ligament reconstruction. They found that a femoral tunnel positioned in the anatomic center of the femoral origin of the ACL, as opposed to the anteromedial position, provides the greatest amount of rotatory and anterior stability.
Figure A shows AP and lateral radiographs of the knee. Note there is a autograft ACL reconstruction with vertical placement of the femoral and tibial tunnel.
Incorrect Answers:
Question 70
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
REFERENCES: Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388.
Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
Mills WJ, Tejwani N: Heterotopic ossification after knee dislocation: The predictive value of the injury severity score. J Orthop Trauma 2003;17:338-345.
Question 71
A 15-year-old male jumps off a 6 foot ramp and lands awkwardly. His knee swells up immediately and he is taken to the emergency room. Figures A is a sagittal CT scan image. In the next 3 hours, he complains of increasing leg pain. This is likely because of injury to which of the following structures? Review Topic

Explanation
Tibial tubercle fractures usually occur during aggressive quadriceps contraction during sports. The Ogden classification classifies this by site of fracture (Type I, through the tubercle; Type II, at the level of the tibial physis; Type III, extending through the anterior tibial epiphysis). Other complications include extensive soft tissue damage, periosteal stripping, vascular compromise and intra-articular damage.
Pandya et al. reviewed 41 tibial tubercle fractures. They found compartment syndrome or vascular compromise in nearly 10%. They found that the degree of injury was underestimated 50% of the time when classified using lateral radiographs alone. They recommend CT scan or MRI as an adjunct. If intra-articular involvement is seen, arthroscopy or open arthrotomy should be performed.
Pape et al. describe 2 case reports of anterior compartment syndrome after tibial tubercle fracture. The compartment syndrome occurs as a result of proximity of the tibial tubercle physis to the anterior tibial recurrent artery.
Figure A shows the sagittal reconstruction CT image showing intraarticular involvement. Illustrations A and B are axial and coronal CT images in the subchondral region showing the fracture line traversing the zone between fused and unfused physis (see Illustration C for physeal closure pattern). Illustration C shows the direction of closure of the proximal tibial physis. In the sagittal plane, the proximal tibial physis closes from posterior to anterior, then to the tubercle apophysis which closes from proximal to distal also. In the coronal plane, the physis closes from medial to lateral. In the axial plane, the physis closes from posteromedial to anterolateral. Illustration D shows the anterior tibial recurrent artery.
Incorrect Answers:
Question 72
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 73
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.

Question 74
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Explanation
REFERENCES: Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: Review of a series of 25 cases. J Pediatr Orthop 1987;7:444-449.
Question 75
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
REFERENCES: Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880.
Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
Hadjipavlou AG, Mader JT, Necessary JT, et al: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000;25:1668-1679.
Question 76
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
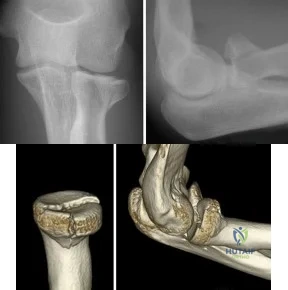
Explanation
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
>= 3 fragments.
Question 77
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 78
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 79
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
Question 80
A 16-year-old boy with spastic quadriplegic cerebral palsy has been referred for evaluation and management of scoliosis. His parents report increasing problems with sitting balance, positioning, and hygiene because of the deformity. The radiograph shown in Figure 46 reveals a lordoscoliosis of 105° with marked pelvic obliquity. Attempts at correcting the pelvic obliquity on supine bending radiographs show significant rigidity. Management should consist of
Explanation
REFERENCES: Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 977-997.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 447-459.
Question 81
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
neck pain.
REFERENCES: Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
Zdeblick TA, Ducker TB: The use of freeze-dried allograft bone for anterior cervical fusions. Spine 1991;16:726-729.
Question 82
Placing the starting point for an antegrade femoral nail too anterior to the axis of the medullary canal can lead to what intraoperative complication?

Explanation
Question 83
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 84
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 85
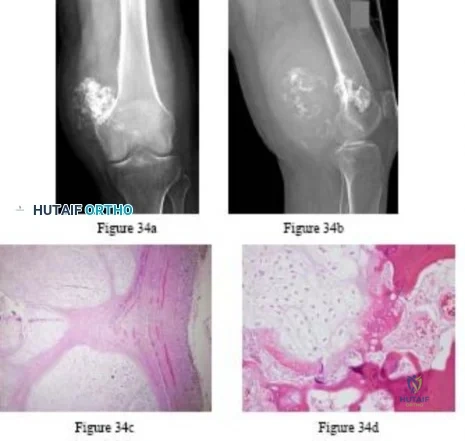
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?

Explanation

Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
Question 86
A 6-year-old girl sustains an ankle injury after falling on roller blades. An AP radiograph is shown in Figure 68. Treatment should consist of which of the following?
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 87
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
REFERENCES: Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.
Question 88
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 89
A 12-year-old boy is emergently transported to the emergency department following a motor vehicle accident. He was restrained in the back seat with a lap belt. On a physical exam bruising is noted across his abdomen as shown in Figure A. Lateral radiographs are shown in Figure B. Which of the following injuries are most frequently associated with this injury pattern? Review Topic

Explanation
A Chance fracture injury is a flexion-distraction injury of the spine. The anterior column (vertebral body) collapses under compression and the posterior elements fail under tension (rupture of the interspinous ligaments or avulsion fracture of the spinous process). A common mechanism is a MVA where the child is wearing a seatbelt, leading to a "seatbelt sign". In the presence of a "seatbelt" sign, on should have a high suspicion for a bowel injury.
Reid et al. reported seven cases of pediatric patients with Chance fractures. All had associated intraabdominal bowel injury.
Holland et al. retrospectively reviewed 28 pediatric patients with Chance fractures, 71% sustained following road trauma. Eleven percent had associated small bowel injury, but all patients had abnormal abdominal CT scans.
Figure A is a clinical photo of a 'seatbelt sign' following a motor vehicle accident. Figure B exhibits a "bony" Chance fracture where the spinous process has been avulsed. Illustration A depict the failure of the anterior column under compression and failure of the posterior column under tension.
Incorrect answers:
(SBQ12SP.32) A 48-year-old man is involved in a motor vehicle accident and is taken to an outside hospital where he undergoes CT imaging, displayed in Figures A-B. Approximately 36 hours later he is transferred to your hospital for further evaluation and management. On exam, he has tenderness over his upper cervical spine and is neurologically intact with no myelopathic signs. What is the most appropriate treatment method for this patient and why? Review Topic

Soft cervical orthosis because his gender puts him at a low risk of nonunion.
Halo vest immobilization because the degree of fracture displacement puts him at a low risk of nonunion.
Anterior screw fixation because his delayed time to treatment puts him at an high risk of nonunion.
Posterior C1-C2 fusion with rigid instrumentation because his age puts him at a high risk of nonunion.
Posterior C1-C2 fusion with sublaminar wiring because the degree of fracture angulation puts him at a high risk of nonunion.
The patient has a type II odontoid fracture and should be managed with halo vest immobilization as he has minimal fracture displacement (< 5mm) and no other risk factors for nonunion.
Type II odontoid fractures comprise 35% of all C2 fractures and have the highest nonunion rate. Commonly cited risk factors for nonunion include posterior displacement, posterior angulation, delayed initiation of treatment, fracture comminution and advanced age. Patients without these risk factors can often be successfully managed with halo vest immobilization. Elderly patients are frequently unable to tolerate halo vest immobilization and can be placed in a rigid cervical orthosis. Patients at high risk for nonunion are generally managed surgically with either anterior screw fixation, posterior rigid fixation (C1-C2 transarticular screw construct versus C1 lateral mass screw + C2 pedicle screw construct), or posterior C1-C2 sublaminar wiring.
Greene et al found that type II odonotoid fractures that were displaced >/= 6mm had a nonunion rate of 86% compared to 18% in patients with < 6mm displacement. This was statistically significant regardless of direction of displacement. Age was not significantly associated with nonunion.
Koivikko et al performed a retrospective review of conservatively treated type II odontoid fractures and identified risk factors for nonunion. Fracture gap > 1mm, posterior displacement > 5mm, posterior angulation > 20°, delayed start of treatment
> 4 days and posterior redisplacement > 2mm were all correlated with nonunion. In this study, anterior displacement, gender and age were unrelated to nonunion.
Figures A and B are coronal and sagittal CT scans of the cervical spine, respectively, demonstrating a noncomminuted type II odontoid fracture with minimal posterior displacement and angulation.
Incorrect
Responses:
Question 90
What is an example of cognitive rest after concussion? Review Topic
Explanation
Question 91
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 92
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 93
The additional risk of complications in organ transplant patients receiving a total joint arthroplasty is attributed to
Explanation
REFERENCE: Tannenbaum DA, Matthews LS, Grady-Benson JC: Infection around joint replacements in patients who have a renal or liver transplantation. J Bone Joint Surg Am 1997;79:36-43.
Question 94
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
Question 95
Figures 1a through 1c are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury, she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?

Explanation
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized. Intralesional steroid injections have a role in the treatment of simple bone cysts; however, this treatment is not recommended for enchondromas. Immediate curettage alone is not the best treatment because it does not include bone graft (either autograft or allograft) or bone graft substitute. Also, it would be best to allow the fracture to heal prior to curettage to prevent fracture displacement. An enchondroma this size necessitates a graft because of high risk for refracture if curettage alone is performed. Many surgeons believe it is best if a fracture heals prior to curettage and grafting because this allows better graft containment and eliminates concern about fracture displacement. Recent data suggest early surgery using injectable calcium sulfate cement in the fracture setting can achieve satisfactory results. Splint
immobilization would allow fracture healing, and then curettage with bone graft can be performed after healing occurs.
RECOMMENDED READINGS
Jacobson ME, Ruff ME. Solitary enchondroma of the phalanx. J Hand Surg Am. 2011 Nov;36(11):1845-7. doi: 10.1016/j.jhsa.2011.05.002. Epub 2011 Jun 11. Review. PubMed PMID: 21658859.
Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am. 2012 Jun;37(6):1229-34. doi: 10.1016/j.jhsa.2012.03.019. Epub 2012 Apr 27. PubMed PMID: 22542061.
CLINICAL SITUATION FOR QUESTIONS 2 THROUGH 5
A 45-year-old man injured his arm when it was forcibly extended while he was flexing his elbow. He notes swelling in the antecubital fossa and arm weakness. The physician suspects a distal biceps rupture.
Question 96
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 97
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 98
A year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 08 to 1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
ERGUIDE MCQ 401-450
ORTHOPEDICS HYPERGUIDE MCQ 351-400
ORTHOPEDICS HYPERGUIDE MCQ 301-350
ORTHOPEDICS HYPERGUIDE MCQ 251-300
ORTHOPEDICS HYPERGUIDE MCQ 201-250
ORTHOPEDICS HYPERGUIDE MCQ 151-200
ORTHOPEDICS HYPERGUIDE MCQ 101-150
FREE Orthopedics MCQS 2022 51-100
Orthopedics Hyperguide MCQ 1-50
Question 99
A 24-year-old professional male soccer player has lower abdominal pain on exertion. He has pain with resisted hip adduction and with sit-ups. There is no palpable inguinal hernia with a Valsalva maneuver. Nonsurgical management has failed to provide relief. After ruling out malignancies, what is the next most appropriate step in management?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Biedert RM, Wamke K, Meyer S: Symphysis syndrome in athletes: Surgical treatment for chronic lower abdominal, groin, and adductor pain in athletes. Clin J Sport Med 2003;13:278-284.
Question 100
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
