Orthopedic Board Prep MCQs: Arthroplasty, Trauma, Hip, Peripheral Nerve & Tendon – Part 138

Key Takeaway
This page offers Part 138 of a comprehensive OITE & ABOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs on topics like arthroplasty and fracture, designed for orthopedic residents and surgeons. Utilize interactive study or exam modes with clinical explanations to confidently prepare for your board certification exams.
About This Board Review Set
This is Part 138 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 138
This module focuses heavily on: Arthroplasty, Fracture, Hip, Nerve, Tendon.
Sample Questions from This Set
Sample Question 1: The stiffness of a 16-mm femoral stem is mostly influenced by the...
Sample Question 2: A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?...
Sample Question 3: In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic...
Sample Question 4: Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implantis shown in Figure 181). He now has increasing hip pain. Radiographs...
Sample Question 5: A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
REFERENCE: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 458.
Question 2
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 3
In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic
Explanation
Question 4
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 5
A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern and paperwork is completed per institutional protocol. She is then brought back to the operating room. Which of the following is true regarding the pre-surgical timeout?
Explanation
The WHO pre-surgical safety checklist involves assessment at three points during an operative procedure: before induction of anesthesia, before skin incision, and before the patient leaves the operating room. Some components of the checklist include
confirming IV access and allergies, administration of antibiotic prophylaxis, and surgical site verification. The surgeon has been shown to be the most effective team member at reducing complications when using the checklist.
Haynes et al. evaluated the effects of the WHO pre-surgical checklist on perioperative complication rates at eight international sites. They found a significant reduction in rates of complications and death in patients over the age of 16 undergoing noncardiac procedures after implementation of the checklist.
Illustration A shows the WHO pre-surgical checklist Incorrect Answers:
present for the timeout. Answer 2: The implant representative is not necessary for the timeout. Answer 4: The attending surgeon needs to be present in the same OR for the timeout. Answer 5: The timeout has been shown to decrease rates of complication and death.
Question 6
MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
Explanation
A. Pain with elbow extension in forearm pronation
B. Mechanical symptoms when rising from a chair
C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
Question 7
Which component position is associated with poor patellar tracking during total knee arthroplasty (TKA)?
Explanation
Internal malrotation of the femoral or tibial component is associated with lateral tracking of the patella in TKA. Lateral placement of the femoral component and medial placement of the patella component can aid in preventing lateral tracking of the patella. Varus alignment of the proximal tibia has not been associated with patella maltracking.







RESPONSES FOR QUESTIONS 106 THROUGH 109
Immobilization/nonsurgical management
Irrigation and debridement
stage reimplantation total knee arthroplasty (TKA)
Increased constraint/polyethylene exchange
Revision of the femoral component only
Revision of the tibial component only
Revision of both components
Revision of the patellar component
Select the treatment listed above that most appropriately addresses each scenario described below.
Question 8
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
Question 9
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126.
Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, p 158.
Question 10
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?
Explanation
REFERENCES: Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 812-817.
MacDonald BD, Wertheimer SJ: Bilateral os peroneum fractures: Comparison of conservative and surgical treatment and outcomes. J Foot Ankle Surg 1997;36:220-225.
Question 11
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 12
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?
Explanation
REFERENCES: Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Resnick D, Walter RD, Crudale AS: Bilateral dysplasia of the scapular neck. Am J Roentgenol 1982;139:387-390.
Question 13
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
REFERENCES: Willis R, Blokker C, Stall TM, et al: Long-term follow-up of anterior
eminence fractures. J Pediatr Orthop 1993;13:361-364.
Smith JB: Knee instability after fracture of the intercondylar eminence of the tibia.
J Pediatr Orthop 1984;4:462-464.
Question 14
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
REFERENCE: Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 15
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
REFERENCE: O’Driscoll SW, Jaloszynski R, Morrey BF: Origin of the medial ulnar collateral ligament. J Hand Surg Am 1992;17:164-168.
Question 16
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 17
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 18
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 19
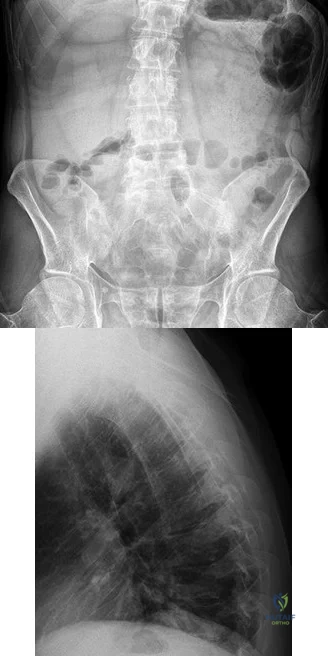
Figure 81 is a lateral thoracic spine radiograph of a 76-year-old man with a history of ankylosing spondylitis who falls and strikes his back. He has moderate thoracic discomfort. An initial examination does not reveal neurologic deficits. He is discharged home that day, but returns 3 days later with profound weakness in his legs. Which imaging study should have been obtained at his initial presentation?
Explanation
Patients with ankylosing spondylitis are at high risk for occult vertebral fractures that are not readily detectable on radiographs. The treating surgeon must have a high suspicion for fractures in these patients and pursue further imaging of the spine with CT and (often) MRI. Even among patients who are neurologically intact, fracture displacement and neurologic deterioration can occur if fractures are not recognized early and appropriately stabilized. Fractures in patients with ankylosing spondylitis are extremely unstable and are associated with high risk for delayed neurological deterioration. Although plain film imaging of the entire spine should be considered, occult fractures can easily be missed. Imaging of the sacroiliac joints can be helpful to establish the diagnosis of ankylosing spondylitis but would not identify an occult fracture of the vertebra in this patient.
RECOMMENDED READINGS
Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. View Abstract at PubMed Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. View Abstract at PubMed
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. View Abstract at PubMed
Question 20
Figure 1 is the MR image of a 43-year-old man who has left shoulder pain and weakness after a fall. An examination reveals active forward elevation at 120° and positive Yergason and lift-off test examination findings. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?

Explanation
Question 21
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 22
Following insertion of a cementless femoral component into the total hip arthroplasty construct, the amount of femoral stress shielding is most associated with
Explanation
Although material modulus, characteristics of surface, and extent of coating all contribute to stress shielding, poor bone quality is the most important factor associated with stress shielding.
Question 23
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intraoperatively, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation
Question 24
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Question 25
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?
Explanation
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 26
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Rockwood CA Jr, Thomas SC, Matsen FA III: Subluxations and dislocations about the glenohumeral joint, in Rockwood CA Jr, Green DP, Bucholz RW (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, vol 1, pp 1058-1065.
Question 27
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 28
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of 3.4, osteoarthritis had an OR of 2.4, and tobacco use had an OR of 1.9.
Question 29
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 30
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 31
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 32
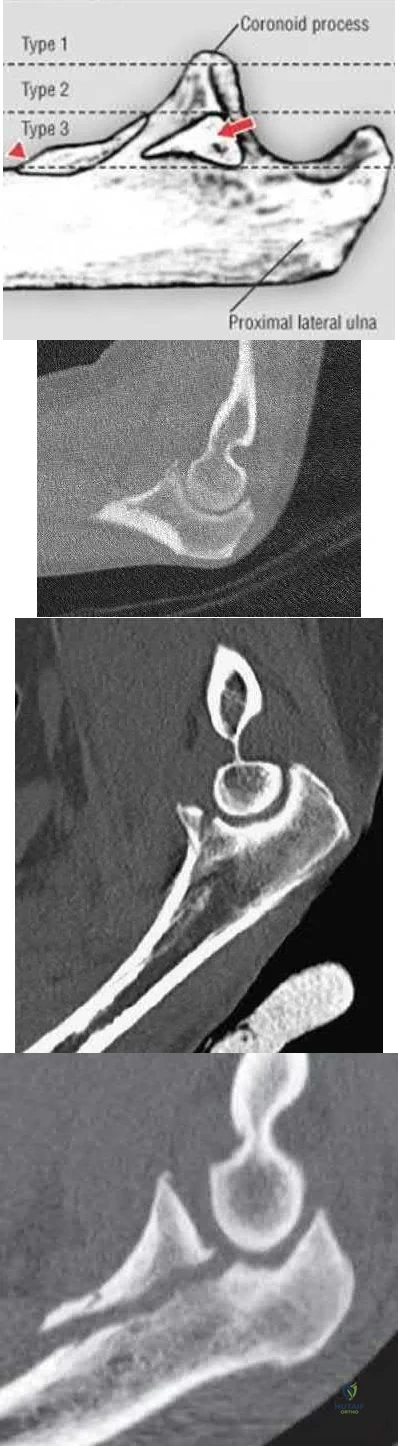
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 33
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Explanation
REFERENCES: Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 34
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic

Explanation
Question 35
below depicts the radiograph obtained from a year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 36
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis? Review Topic

Explanation
Question 37
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
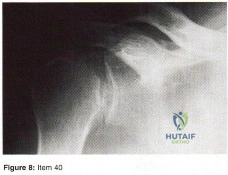
Question 38
Item Deleted by AAOS Question 40 - Figure 8 shows the AP radiograph of a 38-yea-old woman who has constant pain in her shoulder as the results of a motor vehicle accident. Examination reveals marked restriction in external rotation. Which of the following studies should be ordered to aid in making a diagnosis?
Explanation
Question 39
- A right-handed, 53 year old man reports pain in the left shoulder following a fall on an abducted externally rotated shoulder 3 months ago. Examination reveals pain on elevation and tenderness localized to the anterior aspect of the shoulder. Results of the lift-off test are inconclusive due to limited internal rotation. Figure 2 shows the T1-weighted axial image from an MRI-arthrogram. Treatment should include
Explanation
Question 40
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
REFERENCES: Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Question 41
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1009-1149.
Question 42
When performing a gastrocnemius recession, what structure should be protected?
Explanation
REFERENCES: Pinney SJ, Sangeorzan BJ, Hanen ST Jr: Surgical anatomy of the gastrocnemius resection (Strayer procedure). Foot Ankle Int 2004;25:247-250.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 415-417.
Question 43
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
REFERENCES: Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259.
Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 44
A B Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
Explanation
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. View Abstract at PubMed
Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. View Abstract at PubMed
Question 45
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of
recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 46
An 8-year-old boy reports progressive difficulty with walking. Examination reveals muscle weakness, with proximal groups more affected than distal muscles. Deep tendon reflexes are within normal limits. Laboratory studies show a creatine kinase level of 7,200 IU. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Sussman MD: Muscular dystrophy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1573-1583.
Thompson GH, Berenson FR: Other neuromuscular disorders, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, vol 1, pp 633-676.
Question 47
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Garcia JA, Mykula R, Stanley D: Complex fractures of the distal humerus in the elderly: The role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84:812-816.
Question 48
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 49
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 50
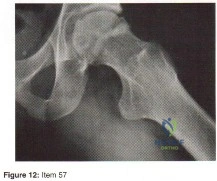
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
Explanation
Question 51
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
REFERENCES: Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978. JAMA 1979;241:1477-1479.
Question 52
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 53
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 54
Which of the following findings is more suggestive of neurogenic rather than vascular claudication in the differential diagnosis of leg pain?
Explanation
Question 55
A 14-year-old gymnast presents after a fall from the balance beam with a hyperextension injury to her left knee. She could ambulate with pain but was unable to continue exercise due to pain. On examination she has a swollen knee with painful

Explanation
Tibial eminence fractures are rare but occur more often in pediatric populations, often in the setting of sports-related injuries. Debate continues over operative vs nonoperative treatment, as well as fixation type (screw vs suture) for openly treated fractures. Past evidence suggested closed treatment was adequate but there has been an increase in operative management. Closed treatment is suggested for minimally displaced fractures (Type I and reducible Type II) and open treatment for completely displaced fractures (non-reducible Type II and Type III).
Wilfinger et al provide the results of a closed reduction protocol at their institution including 38 patients with long term followup. All patients underwent aspiration and closed reduction in the OR under fluoroscopic guidance followed by long leg casting in hyperextension and graduated weight bearing over weeks. No patients complained of persistent pain, swelling, giving way, or disability at follow up.
However, Edmonds et al in a retrospective review compare open reduction internal fixation (ORIF), arthroscopic-assisted internal fixation (AAIF), and closed reduction with casting (CRC) for pediatric patients with displaced tibial spine fractures. They report improved reduction but also increased arthrofibrosis in ORIF and AAIF groups
compared to CRC, but of the 24% of patients with long term followup results, there was no difference in functional outcomes across all 3 groups. There was a 17% rate of later operation for the CRC group patients. They suggest closed treatment for fractures with <5mm displacement, otherwise ORIF or AAIF.
Gans et al conducted a systematic review focused on the questions of open vs closed reduction, and screw vs suture fixation. The 26-article review found insufficient evidence to have any clear recommendations. They did find reduced laxity and improved range of motion for minimally displaced fractures that had an open reduction, and that completely displaced fractures treated nonoperative had higher rates of nonunion.
Figures A and B are AP and lateral knee radiographs demonstrating a moderately displaced (Meyers and McKeever Type II) tibial spine fracture in a skeletally immature patient.
Incorrect Responses
Question 56
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 57
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 58
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 59
Split posterior tibial tendon transfer is used in the treatment of children with cerebral palsy. Which of the following patients is considered the most appropriate candidate for this procedure?
Explanation
REFERENCES: Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in spastic cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 2, pp 1142-1152.
Question 60
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment?

Explanation
Question 61
Figures A and B are axial and coronal MRI images of a 21-year-old male athlete. He injured his left leg during a hurdling race approximately 1 week ago. What would be the next best step in the management of this injury? Review Topic
Explanation
Athletes participating in sports that require sprinting, jumping, acceleration and deceleration are at increased risk of sustaining a proximal hamstring tendon avulsion. The greatest predictor of this injury is prior hamstring injury. Other risk factors include increasing age, high training demand, increased body mass index and tight hip flexor muscles. MRI is the gold standard imaging to identify these images. Open hamstring tendon repair is recommended in athletes when all of the hamstring tendons have avulsed off their origin or 2 tendons have avulsed and retracted more than 2 cm.
Cohen et al. wrote a JAAOS article on acute proximal hamstring rupture. They point out that testing the peroneal branch of the sciatic nerve function is important in the physical examination, as injury to this branch will cause weakness of the short head of the biceps femoris and may slow potential postoperative rehabilitation.
Lefevre et al. reviewed the return to sports after surgical repair of acute proximal hamstring ruptures. They performed a prospective observational study that included 34 patients. Patients returned to sports within a mean 5.7 ± 1.6 months, at the same level in 27 patients (79.4 %) and at a lower level in 7 patients (20.6 %). They conclude that surgical repair of acute proximal hamstring ruptures has the potential to significantly improve the functional prognosis of patients with these injuries.
Figures A and B shows a significant amount of swelling and hematoma around the hamstring tendon. The whole ischial tuberosity is denuded of tendon, which is consistent with a complete rupture. Illustration A shows a large posterior thigh ecchymosis commonly seen with this injury. The ecchymosis presents approximately 1 week following injury, which is know as latent ecchymosis. Illustration B shows a
schematic and intraoperative image of the open tendon repair of an acute injury.
Incorrect
Question 62
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 63
Internal impingement is characterized by which of the following anatomic lesions? Review Topic
Explanation
Question 64
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Deyo RA, Diehl AK, Rosenthal M: How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med 1986;315:1064-1070.
Question 65
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 66
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
Explanation
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.
REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.
Question 67
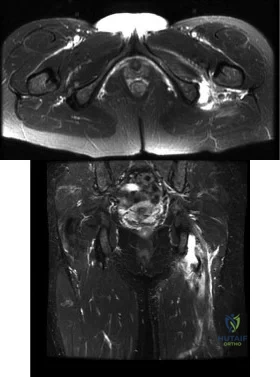
Figures 150a through 150d are the radiographs and MR images of a 37-year-old woman who has a 3-month history of severe right hip pain. She does not recall any trauma prior to the pain onset and denies any past steroid exposure. She has 3 children and is not currently pregnant. The pain is located in her groin and the onset was sudden. The pain is refractory to anti-inflammatory medications. What is the most appropriate treatment?
Explanation
The patient’s MR images are consistent with transient hip osteoporosis. No signs suggest avascular necrosis. She has no joint narrowing. Transient osteoporosis of the hip is characterized by bone marrow edema in the femoral head and neck. This condition affects more men than women and is sometimes seen in the third trimester of pregnancy but can be seen in women who are not pregnant as well. This is a self-limiting condition, and the treatment is limited weight-bearing activity until the symptoms resolve. Core decompression is rarely used in these cases. There is no indication for arthroplasty or osteotomy in this scenario.
Question 68
A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 69
A 75-year-old man presents with worsening low back and bilateral leg pain. The pain worsens with ambulation and improves with sitting. On exam, he has strong DP and PT pulses. Straight leg raise is negative. A MRI of the lumbar spine is performed and is pictured in Figure A. On further questioning, which of the following is the patient also likely to report? Review Topic

Explanation
Lumbar spinal stenosis often results from degenerative changes of the intervertebral disc and facet joints which ultimately narrows the space available for the thecal sac and exiting nerve roots. Patients can present with neurogenic claudication, reported as worsening leg and/or back pain with ambulation and diminished walking capacity. MRI may demonstrate disc degeneration/bulging, hypertrophy of the ligamentum flavum and facet capsule, and narrowing of the central canal. Nonoperative management includes NSAIDs, PT and epidural steroid injections (ESI). Surgery is reserved for patients who have failed nonoperative measures and includes decompressive laminectomy with or without fusion depending on presence of instability.
Issack et al reviewed degenerative lumbar spinal stenosis. Unlike patients with vascular claudication, patients with neurogenic claudication are able to improve walking tolerance with postural changes, specifically with flexed-forward posture (such as leaning forward on a shopping cart). They are unable to improve their symptoms simply by cessation of walking. Patients with neurogenic claudication tend to lack the trophic changes of the skin on the legs/feet as well as diminished pulses characteristic of vascular disease.
Young et al reviewed the utilization of lumbar ESI for low back and leg pain. The authors concluded that lumbar ESI are a reasonable nonsurgical option to provide temporary symptomatic relief. Fluoroscopic guidance facilitates accurate placement of the injection into the epidural space, while its nonuse may lead to higher percentage of technical failures. Lastly, the transforaminal approach is more selective
than the interlaminar approach and can provide diagnostic information as well as symptom relief.
Figures A and B are T1 sagittal and T2 axial MR images, respectively, of the lumbar spine demonstrating significant central canal stenosis most notable at L4-L5 with broad disc protrusion, facet degeneration and infolding of the ligamentum flavum.
Incorrect
Responses:
Question 70
The posterior approach to the proximal radius uses what intermuscular interval?
Explanation
REFERENCES: Spinner M: Injuries to the Major Branches of Peripheral Nerves of the Forearm, ed 2. Philadelphia, PA, WB Saunders, 1978, pp 66-77.
Henry AK: Extensile Exposure, ed 3. New York, NY, Churchill Livingstone, 1995.
Question 71
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 72
A coach of 3 football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on 1 team are different from those on the other teams?
Explanation
Data collected in research studies fall into 1 of 2 categories—continuous or discrete. Continuous data can be displayed on a curve. Examples include height, weight, and time recorded in a 40-yard dash. Discrete data represent data that fall into specific categories such as gender or the presence or absence of a risk factor.
ANOVA is used to determine statistical significance in mean values of continuous data when there are more than 2 independent samples. The 2-sample t test compares mean values of continuous data between 2 independent groups. The Chi-square test and Fisher's exact tests are tests used to analyze discrete data.
RESPONSES FOR QUESTIONS 58 THROUGH 61
Paresthesias in the fourth and fifth digits
Numbness on the lateral side of the forearm
Heterotopic ossification
Posterolateral rotatory instability of the elbow
Medial antebrachial cutaneous neuroma
For each surgical case described below, match the most likely related complication listed above.
Question 73
The patient undergoes hip arthroscopy and the image of the right hip is shown in Figure 39. Repair of the injured structure would be expected to improve
Explanation
The radiographic studies reveal both acetabular dysplasia and cam-type femoroacetabular impingement. The MR image shows an acetabular labral tear. Structural abnormalities of the hip, including femoroacetabular impingement, have commonly been identified in association with labral tears. Disruption of the ligamentum teres is not associated with impingement conditions in the absence of trauma.
The patient has acetabular dysplasia with a decreased lateral center-edge angle and also has visible cam-type femoroacetabular impingement. The common pathway for joint degeneration in hips with cam-type femoral head anatomy includes the development of cartilage damage in the anterior or superolateral aspects of the acetabular cartilage. Paralabral cysts may be seen more commonly in association with acetabular dysplasia, although the patient’s radiographs did not demonstrate substantial cystic changes. Osteochondral loose bodies and ligamentum teres ruptures can be seen at arthroscopy in a small number of cases.
There are several proposed roles of the acetabular labrum. It can increase the depth of the acetabular socket by as much as 21% to 28%. Roles of the acetabular labrum include joint lubrication, shock absorption, and pressure distribution. Recent studies assessing the effects of loading on joint stability for both normal and dysplastic hips did not demonstrate a substantial role of the labrum in differences in loading. Although joint stability might be improved following surgical repair, acetabular dysplasia is not likely to be resolved with acetabular labral repair alone.
RECOMMENDED READINGS
Tibor LM, Leunig M. The pathoanatomy and arthroscopic management of femoroacetabular impingement. Bone Joint Res. 2012 Oct 1;1(10):245-57. doi: 10.1302/2046-3758.110.2000105.PubMed: 23610655. View Abstract at PubMed
Peelle MW, Della Rocca GJ, Maloney WJ, Curry MC, Clohisy JC. Acetabular and femoral radiographic abnormalities associated with labral tears. Clin Orthop Relat Res. 2005 Dec;441:327-33. PubMed PMID: 16331022. View Abstract at PubMed
Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011 Jul;39 Suppl:72S-8S. doi: 10.1177/0363546511412320.
PubMed PMID: 21709035. View Abstract at PubMed
James SL, Ali K, Malara F, Young D, O'Donnell J, Connell DA. MRI findings of 37
femoroacetabular impingement. AJR Am J Roentgenol. 2006 Dec;187(6):1412-9. PubMed PMID: 17114529. View Abstract at PubMed
Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17. doi: 10.1007/s12178-009-9052-9. Epub 2009 Apr 7. PubMed PMID: 19468871. View Abstract at PubMed
Henak CR, Ellis BJ, Harris MD, Anderson AE, Peters CL, Weiss JA. Role of the acetabular labrum in load support across the hip joint. J Biomech. 2011 Aug 11;44(12):2201-6. doi: 10.1016/j.jbiomech.2011.06.011. Epub 2011 Jul 14. PubMed PMID: 21757198. View Abstract at PubMed
Question 74
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. Assuming her workup is negative for any other causes, what is the best treatment option?

Explanation
Question 75
A patient competing in a professional motocross race sustained a direct blow to the knee after falling off his bike at high speed. He sustained several lacerations as shown in Figure 60. He is able to actively extend his knee painlessly and his Lachman examination is negative. What is the most likely injury? Review Topic

Explanation
Question 76
At the level of the midcalf, the plantaris tendon is found at which of the following locations?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 475.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 491.
Question 77
03 Figure 72 shows the radiograph of a 4 y/o girl who has a painless right Trendelenburg limp. Management should consist of
Explanation
(unlike their bilateral counterparts which generally do not need to be reduced). Open reduction is used to obtain absolute concentric reduction. In the dislocated hip reduced at age 15 mths or older, there is usually enough associated bony deformity, either femoral, acetabular, or both to require stabilizing osteotomy to maintain the concentric reduction. Femoral shortening is often necessary to relax soft tissues before a perfect reduction is possible in children > 2 y/o.
back to this question next question
Question 78
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, Figure 7-53, p 346.
Callaghan JJ, Rosenberg AG, Rubash HE: The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, p 705.
Question 79
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
REFERENCES: Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Petilon J, Carr DR, Sekiya JK, et al: Pectoralis major muscle injuries: Evaluation and management. J Am Acad Orthop Surg 2005;13:59-68.
Question 80
A 40-year-old man sustains a fall while mountain biking and presents with a posterior elbow fracture-dislocation. The elbow is reduced in the ER and noted to be grossly unstable with varus and valgus stress. Imaging demonstrates a two part radial head fracture involving 40% of the articular surface and a fracture involving less than 10% of the coronoid tip. He is taken to the OR for surgical reconstruction. After fixation of the radial head and repair of the LCL complex, the elbow is fluoroscopically examined and noted to be unstable with valgus stress. The elbow is ranged and dislocates at less than 45 degrees of flexion with the forearm in full supination. What is the next best step in management?
Explanation
OrthoCash 2020
Question 81
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 82
Figures 51a and 51b show the radiographs of a 12-year-old boy obtained after an attempted closed reduction of an elbow injury in the emergency department. His motor examination is intact but he reports decreased sensation along the palmar aspect of his ring and little finger. What is the best treatment plan? Review Topic

Explanation
(SBQ13PE.97) A 3-year-old boy presents to your office for evaluation. On physical examination, the patient has large calves and uses his hands to assist in rising from the floor. Laboratory results from the pediatrician reports notably high creatinine kinase of 43000 IU/L. What is the most likely inheritance pattern? Review Topic
Autosomal recessive
Autosomal dominant
X-linked recessive
X-linked dominant
Mitochondrial inheritance
Duchenne's muscular dystrophy (DMD) has an X-linked recessive inheritance pattern.
Duchenne's muscular dystrophy is characterized by a lack of dystrophin on muscle biopsy. Gower's sign is a typical physical exam finding (child uses hands to assist in rising from sitting), along with pseudohypertrophy of the calves. Notable laboratory values include elevated creatinine kinase (CK), typically above 25,000 IU/L.
Sussman et al. provide a comprehensive review of DMD, highlighting characteristic findings, including pseudohypertrophy of the calves (due to replacement of skeletal muscle with adipose tissue), Gower's sign, as well as CK levels typically above 25,000 IU/L. CK levels can aid in distinguishing between Becker's dystrophy which has levels less than 25,000 IU/L.
Figure A exhibits a muscle biopsy (calf) at low power of DMD; note the replacement of muscle with adipose tissue.
Incorrect answers:
(SBQ13PE.47) Figure A shows an ultrasound of a 2 week old infant being evaluated for developmental dysplasia of the hip. Which of the labels depict the alpha angle, and what anatomic landmarks define this angle? Review Topic
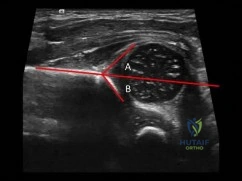
Angle A, ilium and cartilaginous acetabulum
Angle A, ilium and bony acetabulum
Angle B, ilium and cartilaginous acetabulum
Angle B, ilium and bony acetabulum
Angle B, bony acetabulum and acetabular labrum
The alpha angle is subtended by (1) a line drawn down the ilium to a point where it intersects with the bony and cartilaginous confluence of the acetabulum and (2) a line drawn along the roof of the bony acetabulum.
The coronal flexion view (as depicted in figure A) of the infant hip is perhaps more familiar if rotated 90 degrees to view as one would view an anterior posterior radiograph of the pelvis. Acetabular development is evaluated primarily by the alpha angle, indicating the morphology of the developing acetabulum, and the percentage of the femoral head that is covered by the bony acetabulum. These are each readily apparent on ultrasound. Normal hips should have an alpha angle of at least 60 degrees by 6-8 weeks of age.
Harcke et al. provide a current concepts review on the state of ultrasound in the diagnosis and management of developmental dysplasia of the hip (as of 1991). They report, since that time, ultrasound has become the mainstay for diagnostic confirmation and management of DDH.
LeBa et al. performed a study to look at whether ultrasound screening would increase in effectiveness if targeted toward infants with established risk factors for developmental dysplasia of the hip and normal findings on physical examination. They found dynamic ultrasound evaluation showed developmental dysplasia in 7.8% of patients who had normal physical exams and led to a change in treatment in 8%. They conclude selective ultrasound screening in infants with risk factors and normal
findings on physical examination is effective and leads to more effective treatment.
Figure A shows an ultrasound exam of a 2 week old infant. The alpha angle is labeled 'B'. The beta angle is lableled 'A'. Illustration A is a diagram from Tachdjian's illustrating diagrammatically the elements of these angles.
Incorrect answers.
Question 83
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Kohles SS, Kohles JD, Karp AP, et al: Time-dependent surgical outcomes following cauda equina syndrome diagnosis: Comments on meta-analysis. Spine 2004;29:1281-1287.
Question 84
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?
Explanation
Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents.
The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve.
REFERENCES: Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Salter RB, Harris WR: Injuries involving the epiphyseal plate. J Bone Joint Surg Am 1963;45:587-622.
Question 85
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following? Review Topic
Explanation
Question 86
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
Explanation
Question 87
1 shows the radiograph obtained from a year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 4 ng/mL, compared with a normal level of less than 3 ng/mL, and a cobalt level of 8 ng/mL, compared with a normal level less than 7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in What is the most appropriate management at this time?
Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 88
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
REFERENCES: Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
David TS, Drez DJ Jr: Electrothermally-assisted capsular shift. IEEE Eng Med Biol Mag 1998;17:102-104.
Question 89
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:

Explanation
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 90
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 91
- A 6-year-old boy sustained a fracture of the medial malleolus as a result of twisting his ankle. The fracture line extends from the joint surface proximally and medially to include a small fragment of the metaphysis, with a displacement of 3 mm. Management should consist of
Explanation
The authors felt that “anatomical reduction” must include closure of the physeal gap and restoration of rotational alignment of the fracture fragment. They recommended that these fractures be treated with ORIF, consisting of small, smooth Kirschner wires from one epiphyseal fragment to the other. The pins should diverge or converge to prevent any slippage or rotation. They do not recommend crossing the physis with fixation devices, for this may lead to further injury.
Question 92
Heat transfer from the skin to the environment when the ambient temperature exceeds 35°C primarily is attributable to
Explanation
Heat transfer from the skin to the environment occurs through conduction, convection, evaporation, and radiation. Evaporation of sweat is the primary mechanism by which core body temperature is regulated when the ambient temperature exceeds 35°C. High humidity can inhibit the evaporation of sweat, placing athletes at increased risk for heat-related illness, which is defined as a core temperature above 40°C. Symptoms include dizziness, confusion, irritability, hyperventilation, nausea, vomiting, fatigue, and collapse. Initial treatment involves rapid cooling through immersion in cold or ice water to prevent end-stage organ failure.
Question 93
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mmP3P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of Review Topic
Explanation
(SBQ12SP.92) A 36-year-old man presents to the emergency department after being involved in a motor vehicle collision. He is complaining of back pain and imaging shows the findings in Figure A. On neurological examination, he does not have any deficits. MRI shows approximately 25% canal encroachment and no evidence of injury to the posterior ligamentous complex. Which of the following is the most appropriate course in management? Review Topic

Strict bedrest for six weeks then progressive weightbearing
Ambulation as tolerated with or without a TLSO
Surgical decompression and anterior stabilization
Surgical decompression and posterior stabilization
Surgical decompression and combined anterior/posterior stabilization
The patient has a L1 burst fracture with minimal retropulsion of bony fragments in the spinal canal. In the absence of neurological deficits and injury to the PLC, the most appropriate treatment is ambulation as tolerated with or without a thoracolumbrosacral orthosis (TLSO).
Thoracolumbar burst fractures are typically caused by an axial load with flexion and commonly found in this location due to increased motion at these segments. With an intact posterior ligamentous complex (PLC) and no neural compromise, TLSO is the mainstay of treatment. If there is evidence of neurological deficit and/or PLC injury, decompression and fusion are indicated. The degree of acceptable kyphosis is controversial. The choice of anterior versus posterior approach is based on ease of decompression.
Vaccaro et al. introduced a new classification system for thoracolumbar injuries, TLICS, based on morphological appearance, integrity of the posterior ligamentous complex, and neurological status. They advocate use of the system for nonoperative versus operative decision making and communication between surgeons.
Bailey et al. completed a randomized, nonblinded controlled trial to determine the
efficacy of bracing for AO type A0-A3 thoracolumbar burst fractures. Both groups were encouraged to ambulate as tolerated and the no brace group had bending restrictions for 8 weeks. They found no difference in the Roland Morris Disability Questionnaire (RMDQ) score at 3 months after injury.
Figure A is sagittal CT scan of the lumbar spine showing a burst fracture of L1 with minimal retropulsion. Illustration A is the TLICS classification with score of 4 being the branch point for nonoperative versus operative management.
Incorrect Answers:
Question 94
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of
Explanation
REFERENCES: Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44.
Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov’s device. J Pediatr Orthop 1997;17:675-684.
Anderson DJ, Schoenecker PL, Sheridan JJ, Rich MM: Use of an intramedullary rod for the treatment of congenital pseudarthrosis of the tibia. J Bone Joint Surg Am 1992;74:161-168.
Question 95
Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when
Explanation
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
Question 96
Figures 3a and 3b show the inversion stress radiographs of a patient’s ankle. What is the most likely ligament injury pattern?
Explanation
REFERENCES: Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Question 97
Patients with patellar clunk syndrome are best managed by which of the following methods?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329.
Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Question 98
A study is proposed in which 50 patients with osteonecrosis of the knee are compared with 23 patients without osteonecrosis in terms of their alcohol consumption levels. This is an example of what type of study?
Explanation
Question 99
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be
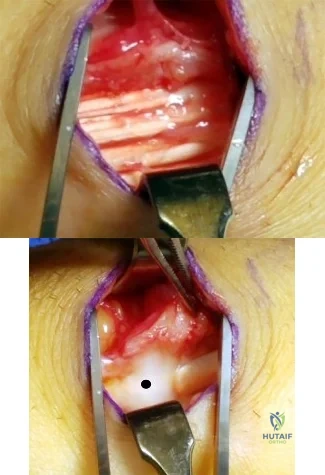
Explanation
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
Question 100
Which of the following activities can improve posterior capsular contractures?
Explanation
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
