Orthopedic Board Prep MCQs: Spine, Arthroplasty, & Trauma | Part 134

Key Takeaway
This page offers Part 134 of a comprehensive orthopedic surgery board review quiz, specifically designed for residents and surgeons preparing for OITE and AAOS exams. It contains 100 high-yield, verified MCQs, replicating exam format. Enhance your board certification readiness through interactive study or exam modes covering key topics.
About This Board Review Set
This is Part 134 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 134
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Infection, Knee, Scoliosis, Tendon.
Sample Questions from This Set
Sample Question 1: Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?...
Sample Question 2: A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?...
Sample Question 3: They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union....
Sample Question 4: A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 deg...
Sample Question 5: A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 2
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 3
They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Explanation
A 76-year old patient underwent partial foot amputation through the talonavicular and calcaneocuboid joints. Besides Achilles tendon lengthening, what additional procedure(s) may be required to prevent the most common post-operative deformity?
Posterior capsule release
Anterior tibialis transfer to the talar neck
Anterior tibialis transfer to cuboid
Flexor hallucis longus transfer to calcaneus
Peroneus brevis transfer to calcaneus Corrent answer: 2
Achilles tendon lengthening AND anterior tibialis transfer to the talar neck would be required to prevent equinovarus deformity.
Partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. Chopart amputation alone is known to result in significant equinovarus deformity. This deformity results in excessive pressure on the anterior wound during gait, causing pain and wound complications. Transfer of the tibialis anterior tendon to talar neck will provide force, and muscle tone, that promotes ankle dorsiflexion. Lengthening of the Achilles tendon will also reduce the equinus moment force across the ankle joint.
Dillion et al. examined the gait patterns of partial foot amputees. They found that amputations proximal to the metatarsal heads compromised the normal propulsive function of the foot and ankle. The ideal level of amputation to maintain normal propulsive function was distal to the metatarsal heads (i.e., disarticulating the metatarsophalangeal (MTP) joint).
Illustration A is a lateral radiograph showing a Chopart amputation. Incorrect Answers:
prevent the equinovarus deformity.

OrthoCash 2020
A 32-year-old male is involved in a motor vehicle collision and sustains the injury seen in Figure A. What is the most common urological injury associated with this injury pattern?

Testicular torsion
Posterior urethral tear
Bladder denervation
Testicular rupture
Renal hematoma
The figure shows an anteroposterior pelvic ring injury. The most common urological injury with pelvic ring injuries remains the posterior urethral tear, followed by bladder rupture.
Watnik et al notes lower urinary tract (bladder to end of urethra) injuries in up to 25% of patients with this injury. He reports that when contaminated urine communicates with the anterior arch, the possibility of infection exists, and early repair of bladder disruptions with simultaneous anterior arch plating minimizes this risk.
Routt et al notes that even with simultaneous treatment of these injuries, complications are common (late stricture in 44%, impotence in 16%, delayed incontinence in 20% of females, anterior deep pelvic infection in 4%). Despite this, they report that early urological repairs are easily performed at the time of anterior pelvic open reduction and internal fixation.
OrthoCash 2020
A 26-year-old women, 31-weeks pregnant, presents to the emergency department with the injury shown in Figure A. She states the injury occurred while lifting a heavy vacuum five days ago. She suffers from chronic headaches and sleep disturbances. On inspection, there are multiple dorsal and volar bruising over her wrist and upper arm. She is neurologically intact. After closed reduction and immobilizing the arm, what would be the next best step in management of this patient?

Diagnostic wrist arthroscopy
Urgent MRI wrist
Skeletal survey radiographs
Request a consultation with social worker in the hospital
Urgent open reduction internal fixation Corrent answer: 4
This patient presents with classic features of domestic violence. The most appropriate next step would be consultation with a social worker at the hospital, assess for child and patient safety, and encouraging the patient to seek self-protection.
Factors suggestive of domestic violence in the patient include pregnancy, delayed presentation after injury, inconsistent history, multiple bruises and complaints of chronic headache/sleep disturbances. Victims frequently miss days of work and as a result are at risk for losing their jobs. Victims are also more likely to engage in high-risk behavior with sex, drugs, alcohol, smoking, and eating.
The AAOS published a document outlining the Orthopaedic Surgeon’s responsibilities in domestic and family violence. Musculoskeletal injuries that should raise a suspicion of a problem include (1) Multiple injuries/fractures; (2) Unusual patterns of injury/fracture; (3) Injuries/fractures of varying ages; (4)
Injuries/fractures inconsistent with or disproportional to the history; (5) Multiple injuries treated in different hospital emergency departments or by different providers.
Incorrect Answers:
OrthoCash 2020
A 45-year-old man undergoes open reduction and internal fixation for a comminuted intra-articular humerus fracture . An olecranon osteotomy is performed and subsequently fixed with an intramedullary cancellous screw. Which of the following options in the table shown in Figure A best describes the characteristics of this osteotomy?
Question 4
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
Explanation
flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant.
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Fehring TK, Odum S, Griffin WL, et al: Early failures in total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 5
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively? Review Topic
Explanation
function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis.
Question 6
A year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in below. To avoid increasing this patient’s combined offset while maintaining her leg length, what is the most appropriate surgical plan?
Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 7
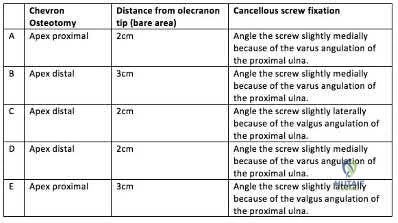
A 45-year-old male laborer injured his right elbow trying to catch a heavy object. He has antecubital pain and forearm ecchymosis. MRI scans are shown in Figures 4a and 4b. Nonsurgical management of this injury is most associated with the loss of Review Topic
Explanation
Question 8
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
REFERENCES: Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 1831-1835.
Question 9
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 10
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
REFERENCE: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 11
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degrees left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of
Explanation
REFERENCES: Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Pettine KA, Klassen RA: Osteoid-osteoma and osteoblastoma of the spine. J Bone Joint Surg Am 1986;68:354-361.
Question 12
Figure 20 shows the plain radiograph of a 70-year-old woman who has shoulder pain and is unable to reach above chest level as a result of a fall 3 months ago. An MRI scan of the shoulder shows a large rotator cuff tear. Examination reveals atrophy of the infraspinatus muscle, active forward elevation of 40 degrees, active external rotation of 30 degrees, passive forward elevation of 150 degrees, and passive external rotation of 60 degrees. The patient has no external rotation strength against resistance. Treatment should include
Explanation
Question 13
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 14
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?
Explanation
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
Question 15
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128.
Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184.
Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Hendel D, Aner A: Entrapment of the flexor digitorum profundus of the ring finger at the site of an ulnar fracture: A case report. Ital J Orthop Traumatol 1992;18:417-419.
Question 16
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 17
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10° of hip abduction on the left and 30° on the right with the hips and knees extended. The Thomas test shows 20° of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0° on the left and -10° on the right. The neck shaft angles are 170° bilaterally. Which of the following procedures would offer the best results?
Explanation
REFERENCES: Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Brunner R, Baumann JU: Long-term effects of intertrochanteric varus-derotation osteotomy on femur and acetabulum in spastic cerebral palsy: An 11- to 18-year follow-up study. J Pediatr Orthop 1997;17:585-591.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 18
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?
Explanation
REFERENCES: Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Daenen B, Preidler KW, Padmanabhan S, et al: Symptomatic herniation pits of the femoral neck: Anatomic and clinical study. Am J Roentgenol 1997;168:149-153.
Question 19
What percentage of bone weight is collagen?
Explanation
Question 20
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 21
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of Review Topic

Explanation
Question 22
03 An 18 year old female Olympic basketball player is seeking advice on how to prevent future ACL injury. What recommendations can be made based on available scientific data?
Explanation
In researching this answer I searched Ovid, looked in sports texts and looked online for “derotation brace.” Every article mentioned “derotation brace” with “the ACL-deficient knee.” I could not find any mention of prophylactic ACL injury prevention with derotation brace.
Prophylactic surgery and oral contraceptive prescription would never be correct answers. As with “derotation brace”, they are buzzwordsin the femaleACL injury literature and you could pick them as an answer if you didn’t have enough knowledge of the subject. It’s hypothesized that estrogen levels may have a role in when females injure there ACLs.
Finally, notchplasty relates to resecting part of the lateral femoral condyle during ACL reconstruction for both visualization of graft placement and to prevent impingement on the graft.
back to this question next question Figure 7 shows the clinical photograph of the knee of a chronic
Question 23
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure? Review Topic
Explanation
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include high-strength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, single-row configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 12-15mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing.
Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Question 24
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of
Explanation
REFERENCES: Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Kaplan H, Kiral A, Kuskucu M, et al: Report of eight cases of humeral fracture following the throwing of hand grenades. Arch Orthop Trauma Surg 1998;117:50-52.
Question 25
Which of the following structures runs through the site indicated by the arrow in Figure 11?
Explanation
REFERENCES: Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Hasan M, Shukla S, Siddiqui MS, et al: Posterolateral tunnels and ponticuli in human atlas vertebrae. J Anat 2001;199:339-343.
Question 26
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 27
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
REFERENCE: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 28
Figure 45 shows the current radiograph of an 11-year-old girl who sustained a simple nondisplaced fracture of the distal radius 4 weeks ago. Management at the time of injury consisted of application of a short arm cast but no manipulation. What is the major concern at this time?
Explanation
REFERENCES: Peterson HA: Physeal fractures: Part 2. Two previously unclassified types. J Pediatr Orthop 1994;14:431-438.
Peterson HA: Physeal and apophyseal injuries, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 108-109.
Question 29
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Explanation
REFERENCES: Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 513-536.
Question 30
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?
Explanation
REFERENCES: Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics 1996;19:383-388.
Mosier-LaClair S, Pomeroy G, Manoli A II: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:95-119.
Question 31
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
REFERENCES: Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98.
Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 32
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of
Explanation
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.

Question 33
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
REFERENCES: Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751.
Glassman SD, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
Raney EM, Bennett JT: Pediatric Chance fracture. Spine 1992;17:1522-1524.
Question 34
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 241.
Question 35
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?

Explanation
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block the UCL with this type of injury.
Question 36
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 37
Which of the following statements is correct regarding Vitamin D?
Explanation
Vitamin D is paramount to proper calcium homeostasis and has important clinical implications in the orthopaedic patient. Vitamin D3 is synthesized in the skin and is converted to 25-hydroxycholecalciferol in the liver. 25-hydroxycholecalciferol is then converted in the kidney into 1,25-dihydroxycholecalciferol, the active form of vitamin
D. The best test to determine Vitamin D deficiency is the measurement of 25-hydroxycholecalciferol, as it has a longer half-life and circulating levels are 1,000x more than 1,25-dihydrocholecalciferol.
Patton et al. review the importance of Vitamin D in the orthopaedic patient. They discuss the implications of Vitamin D deficiency, and urge orthopaedic surgeons to be proficient in both the diagnosis and treatment of the condition.
Bogunovic et al. measured the levels of 25-hydroxycholecalciferol in 723 patients who were to undergo orthopaedic surgery. 40% of these patients were noted to be deficient in Vitamin D, with the highest rates in patients scheduled to undergo trauma and sports surgery.
Illustration A reviews Vitamin D metabolism. 24,25-dihydroxycholecalciferol is referred to as pre-Vitamin D.
Incorrect Answers:
Question 38
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
REFERENCES: Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br
2001;83:954-962.
Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 39
A 19-year-old collegiate middistance runner has a 4-year history of bilateral leg pain. Pain begins within 10 minutes after starting to run and is described as a “tightness and cramping in the front of the legs.” Symptoms resolve within 15 to 20 minutes of running cessation. A presumptive diagnosis of exercise-induced compartment syndrome (EICS) is made, and the patient elects to undergo compartmental pressure testing. What is the strongest indication for elective fasciotomy of the anterior compartment?
Explanation
This clinical scenario describes a patient with EICS, marked by a nonphysiologic rise in muscle compartment pressure during exercise. Pressure testing is the best currently accepted method of diagnosis. Most physicians use the following criteria for diagnosis: resting pressure higher than 15 mm Hg, 1-minute postexercise pressure higher than 30 mm Hg, or 5-minute postexercise pressure higher than 20 mm Hg. Only 1-minute postexercise anterior compartment pressure of 42 mm Hg meets these criteria. Neurologic symptoms in the plantar foot would imply involvement of the posterior compartments and would not support the diagnosis of anterior compartment involvement.
Question 40
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 41
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 42
A fracture in the following location is most commonly associated with procurvatum and valgus malalignment?
Explanation
Proximal third tibial shaft fractures are often difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. Many different techniques have been devised to overcome the deforming forces. These include (1) Poller blocking screws posterior and lateral to the intramedullary nail (IMN), (2) utilizing a semiextended knee position during IMN of proximal tibia fractures (3) use of a suprapatellar approach for IMN, (4) usage of a slightly more lateral starting point during conventional IMN, and (5) application of unicortical plate.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibia. Post-operatively, all patients in their series had less than 5 degrees of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Illustration A shows intra-operative sagittal radiographs of the proximal tibia. Note the use of Poller blocking screws in the posterior and lateral aspects of the proximal tibia.
Incorrect Answers:
Question 43
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 44
7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Explanation
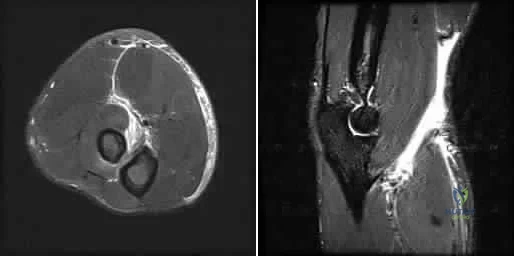
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
Longer operative times
Increased deep surgical infection rates
Unacceptably high malunion/nonunion rates
Slower early return to function
Longer hospital stays Corrent answer: 3
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
OrthoCash 2020
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?

Posterior approach
Anterior approach
Anterolateral approach
Use of a bipolar implant
Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?

Exchange humeral nailing
Augmentative plating
Nail removal with open reduction compression plating
Smoking cessation and medical optimization
Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
OrthoCash 2020
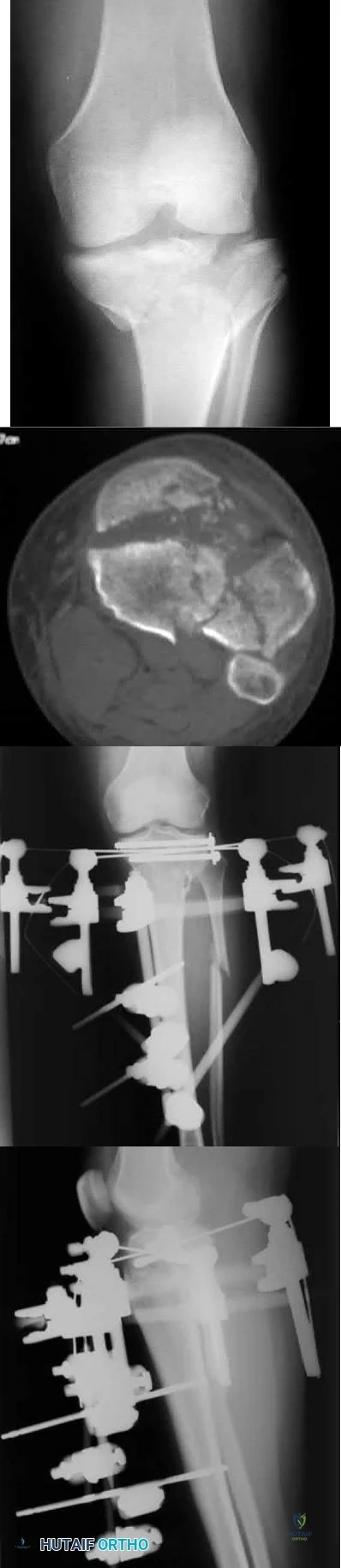
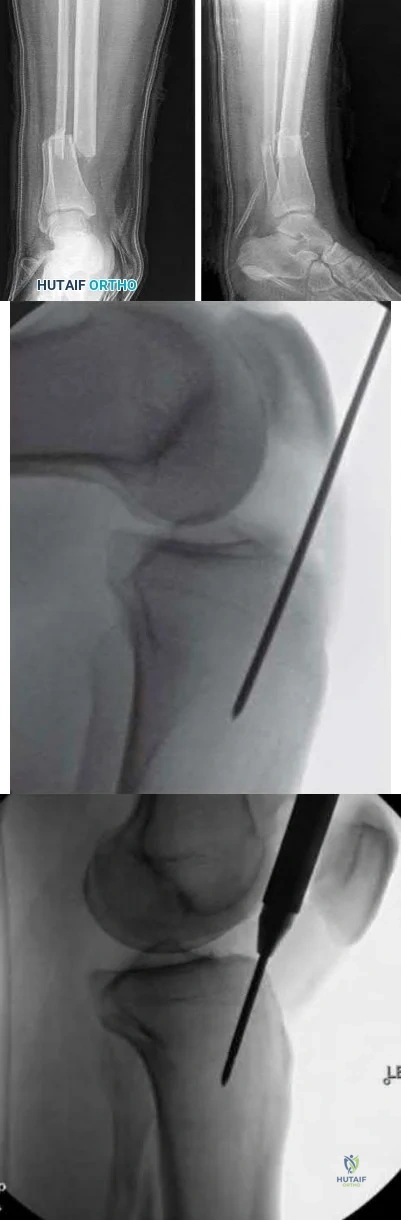
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
Technique depicted in Figure B is associated with an increased risk of septic arthritis
Technique depicted in Figure B is associated with increased rate of anterior knee pain
Technique depicted in Figure B is associated with improved postoperative fracture alignment
Technique depicted in Figure C is associated with an increased risk of septic arthritis
Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
OrthoCash 2020
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?

Nerve compression; open reduction internal fixation with open carpal tunnel release
Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
Decreased arterial inflow; fasciotomy with open reduction internal fixation
Reflex sympathetic dystrophy; vitamin C
Nerve compression; repeat closed reduction Corrent answer: 1
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
OrthoCash 2020
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?

Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
No difference in radiographic outcomes after ORIF vs. closed treatment
No difference in functional outcomes after ORIF vs. closed treatment
Improved functional outcomes with closed treatment vs. ORIF
Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
no difference in functional outcomes between operative and closed treatment modalities for DRF.
OrthoCash 2020
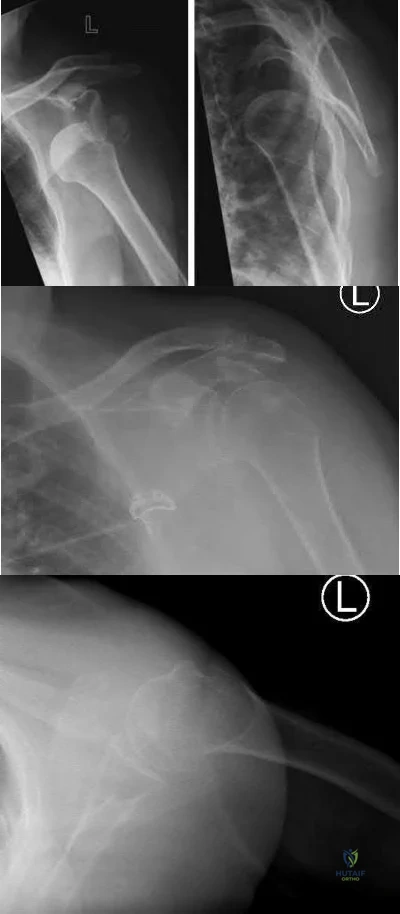
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?
Continued sling immobilization
Closed reduction percutaneous pinning
Open reduction internal fixation
Hemiarthroplasty
Reverse total shoulder arthroplasty Corrent answer: 3
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:

OrthoCash 2020
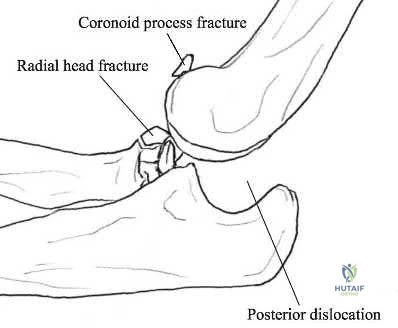
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?

MCL > LCL > anterior capsule
MCL > anterior capsule > LCL
anterior capsule > MCL > LCL
LCL > anterior capsule > MCL
LCL > MCL > anterior capsule Corrent answer: 4
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
OrthoCash 2020
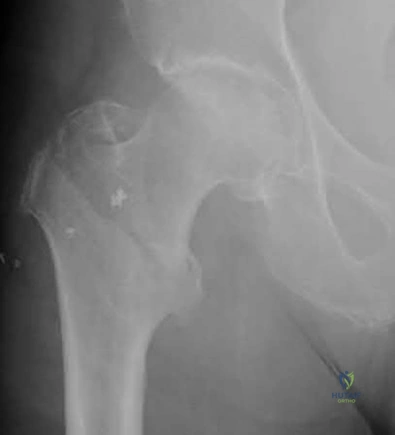
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
Reverse obliquity fracture pattern
Lateral wall thickness
Previous contralateral hip fracture
DEXA T-score <-2.0
Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
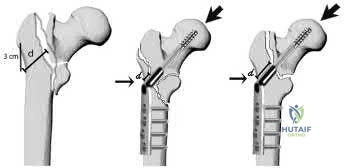
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
OrthoCash 2020
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?

Smaller lateral wall thickness favors sliding hip screw constructs
Unstable fractures are best treated with sliding hip screw constructs
Avoiding distal locking screws in intramedullary implants protects against refracture
Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
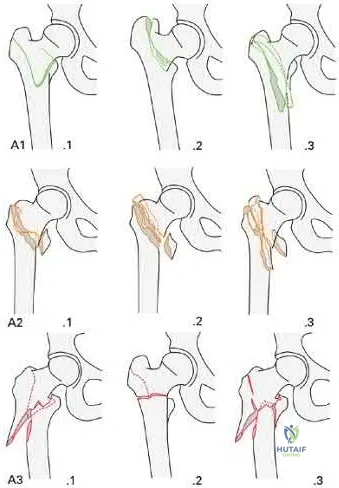
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
OrthoCash 2020
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference <20 mm/hr) and 0.9 mg/L (reference <2.5 mg/L), respectively. Figures A and B are the AP and lateral radiographs of the left femur. Which treatment option offers the highest chance of union and enables immediate weight-bearing?

Nail removal with compression plating and open bone grafting
Closed reamed exchange nailing
Nail dynamization
Nail retention with plate augmentation and bone grafting
Electrical bone stimulator Corrent answer: 4
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:

OrthoCash 2020
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?

External fixation with serial doppler examinations
Intramedullary nailing
Open reduction internal fixation using plates and screws
Immediate 2-compartment fasciotomies and external fixation
Immediate 4-compartment fasciotomies and external fixation Corrent answer: 5
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p) <30 mmHg may help to confirm the necessity for fasciotomy.
McQueen et al. published a report of 25 patients with tibial diaphyseal fractures which had been complicated by an acute compartment syndrome. They reported significant differences in any sequelae of acute compartment syndrome between patients who underwent compartment pressure monitoring and those who had not. They recommended that all patients with tibial fractures should have continuous compartment monitoring to minimize the incidence of acute compartment syndrome.
Mawhinney et al. reported on three cases of tibial compartment syndrome after closed intramedullary nailing of the tibia. They reported that the only predisposing factors for the development of compartment syndrome were the surgery and the fracture itself. They concluded that tibial compartment syndrome is a relatively rare but significant complication of tibial nailing.
Figure A is an AP and lateral radiograph of the leg with displaced, comminuted middle third tibia and fibula fractures.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Decreased arterial inflow; inability to dorsiflex his ankle
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:

OrthoCash 2020
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
Syme
Traumatic transtibial
Vascular transtibial
Traumatic transfemoral
Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
OrthoCash 2020
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?

It may be performed in a minimally invasive manner
It involves minimal soft tissue stripping
It leads to higher union rates
It allows the surgeon to address all sites of injury through one approach
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:

OrthoCash 2020
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
Iliac oblique view with hip and knee flexed
Iliac oblique inlet view
Obturator oblique view with hip and knee flexed
Obturator oblique outlet view
Obturator oblique inlet view Corrent answer: 2
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
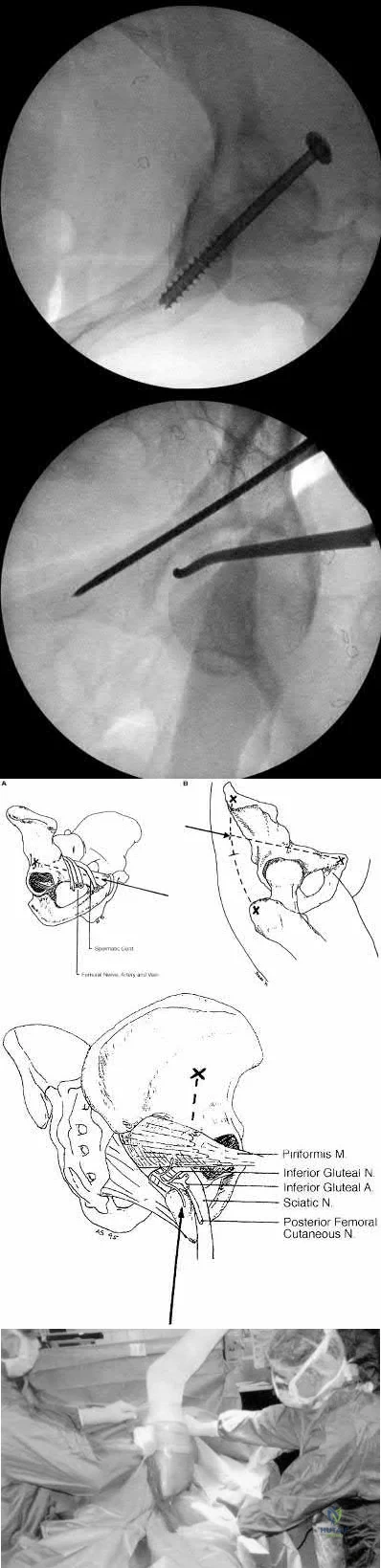
OrthoCash 2020
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
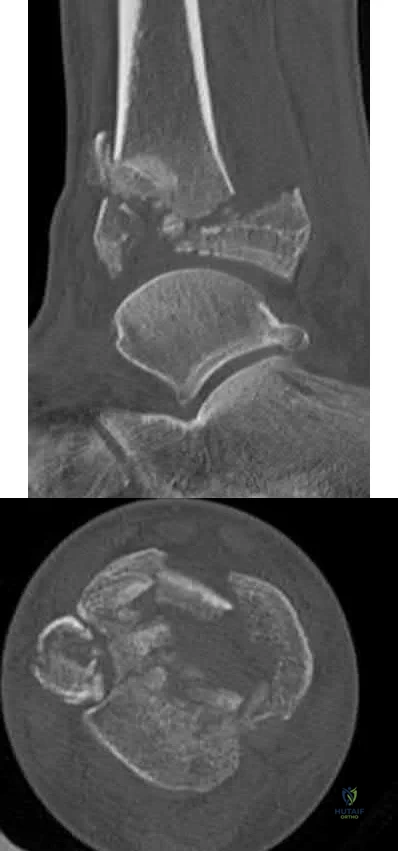
TGF-Beta
RANKL
IL-2
IL-6
cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
immune system.
OrthoCash 2020
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
Ulnar styloid nonunion
DRUJ instability
Articular step-off >3mm
Radial shortening
Workers compensation claim Corrent answer: 1
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
OrthoCash 2020
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?

Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including <8mm of calcar length attached to the articular segment, disruption of the medial hinge, displacement >10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of <8mm attached to the articular segment. Figure D is a displaced metadiaphyseal proximal humerus fracture in a skeletally immature patient. Figure E is a radiograph of a metadiaphyseal proximal humerus fracture in a skeletally mature patient with a medial calcar length >8mm.
Incorrect Answers:
OrthoCash 2020
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?

Nondisplaced medial malleolus vertical shear fracture
Nondisplaced Volkmann's fragment
Nondisplaced Chaput's fragment
Nondisplaced lateral wall talar fracture
Posterior inferior tibiofibular ligament disruption Corrent answer: 2
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
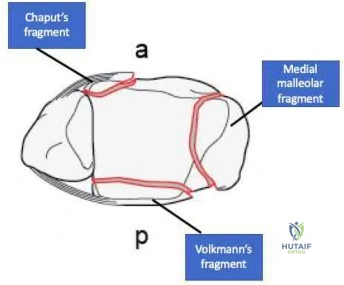
OrthoCash 2020
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
Age < 20
Male gender
Body mass index >/ 30 kg/m^2
Open fracture
Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?

Greater Mayo Elbow Performance Score
Greater Disabilities of the Arm, Shoulder and Hand Score
Increased flexion-extension arc
Increased reoperation rate
Decreased complication rate Corrent answer: 4
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:

OrthoCash 2020
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?

Anterior perforation of distal femur
Breakage of the screw
Implant cutout
Malunion
Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:

OrthoCash 2020
Figure A is the radiograph of a 42-year-old female who presents to the trauma bay following a motor vehicle collision. She subsequently undergoes ORIF through a posterior approach. Iatrogenic injury to which nerve in Figure B is most likely with this approach?
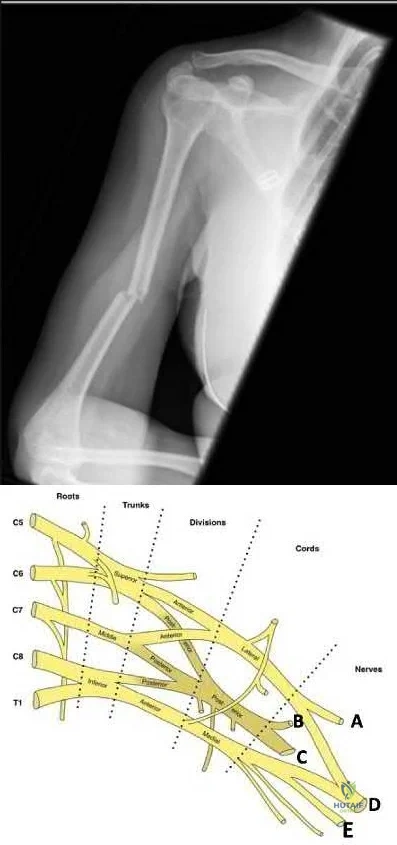
Question 45
Figures below depict the AP and lateral radiographs obtained from a 64-year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?

Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 46
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?
Explanation
REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.
Templeman DC, Schmidt AH, Sems SA, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.
Question 47
The Chi-square test is most appropriate for which of the following?
Explanation
When considering which statistical test to use the investigator must consider how many groups are being compared, and if the data collected is numerical or categorical, and parametric or non-parametric. When the study is comparing proportions of categorical data the appropriate test will be either a Chi-square test, or a Fisher exact test. The Fisher exact test is preferred when there is less than 5 data points in any group being compared.
Illustration A is a flow chart demonstrating how to determine which statistical test is most appropriate.
Incorrect answers:
with the Mann-Whitney U test Answer 3: Comparing means of parametric data between 3 or more groups is best done with Analysis of variance (ANOVA) Answer 5: Comparing proportions of categorical data between groups when at least one group has less than 5 samples or data points is best done with the Fisher exact test
Question 48
Metastatic disease of several cancers create lytic lesions because these cancers:
Explanation
Cancers that originate or metastasize to bone can be blastic, lytic, or mixed when viewed on radiographs. Lytic lesions appear radiolucent due to bone resorption that occurs around the cancer cells. This is secondary to direct production and release of RANKL by the cancer cells themselves. RANKL then stimulates osteoclastogenesis and an increase in local bone resorption. Denosumab is a monoclonal antibody against RANKL that has been shown to decrease rates of pathologic fractures.
Lynch et al. review the progression of metastatic disease. They note that cancer cells can stimulate both osteogenesis and osteolysis, and that this pathologic increase in bone matrix turnover is what allows the cancer to progressively expand or metastasize to distant sites. They discuss the role of matrix metalloproteinases as primary regulators of this process.
Illustration A is a diagram illustrating how the binding of RANKL to receptors on the surface of osteoclast precursors activates them and begins the process of bone resorption. Cancer cells can directly produce RANKL thus increasing the rate of local bone resorption.
Incorrect Answers:
Question 49
A 22-year-old male cyclist was struck by a car. He complains of right knee pain and swelling, as well as reduced sensation and weakness in his right foot. His leg compartments are soft and not tender. Distal pulses in the extremity are palpable. Radiographs of the knee, as shown in Figures A and B, were taken after a closed reduction maneuver was performed. What would be the next best step in management of this patient?

Explanation
Fracture-dislocations of the knee must be suspected with all Schatzker type IV injuries as this fracture pattern is usually associated with high energy trauma. Identifying this injury should prompt a thorough assessment of the neurovascular structures across the knee. After closed reduction and emergent immobilization of the knee, ankle brachial indices (ABI) must be immediately performed. If <0.9, further vascular testing is warranted, such as MR or CT angiography.
Berkson et al. reviewed high energy tibia fractures. They state that Schatzker Type IV fractures typically requires more energy than corresponding lateral plateau fractures, due to denser bone on the medial side.
Chang et al. described an anatomic sub-classification of Schatzker IV fractures. They describe Group 1 fractures as classic medial unicondylar fractures. Group 2 fractures are complicated variants characterized by medial condyle fractures with lateral plateau extension. Usually these have articular impaction of the centroposterior lateral plateau.
Figures A and B show AP and lateral radiographs of the knee demonstrating a classic medial unicondylar Schatzker IV fracture. Note the anterior subluxation of the tibia in relation to the femur. Illustration A shows the multiple CT images of this fracture pattern.
Incorrect Answers:
Question 50
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.
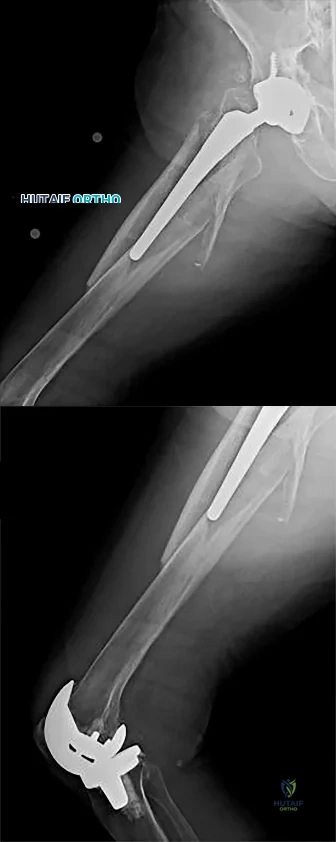
Question 51
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
motor function.
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Leventhal MR: Fractures, dislocations and fracture-dislocations of spine, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 8. St. Louis, MO, Mosby, 1992.
Question 52
A 25-year-old patient presents with a posterior wall/ posterior column acetabular fracture. She is scheduled for open reduction internal fixation through a posterior approach. What position of the leg exerts the least amount of intraneural pressure on the sciatic nerve?

Explanation
Question 53
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the
Explanation
REFERENCE: Coleman SS, Chestnut WJ: A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop 1977;123:60-62.
Question 54
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport?
Explanation
REFERENCES: Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Altchek DW, Andrews JR (eds): The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams
& Wilkins, 2001, p 91.
Question 55
Central cord syndrome would most likely be seen in which of the following patients? Review Topic
Explanation
Central cord syndrome is most commonly caused by cervical hyperextension in older patients with underlying cervical spondylosis. It is thought to be due to compression between anterior osteophytes and posterior infolded ligamentum flavum during hyperextension. This preferentially affects the motor tracks closest to midline, and thus motor function is impaired greater than sensation, and upper extremities more affected than lower extremities (remember upper motor tracks are more central in the lateral corticospinal tract)
Nowak et al. present a review article on central cord syndrome. They cite the most common cause of central cord syndrome as a hyperextension mechanism in an elderly patient with preexisting spondylosis.
Gupta et al. present a review article on the management of spinal cord injuries. They discuss advances and ongoing study in acute management, surgical techniques, pharmacoptherapies, and cellular transplantation. They recommend a multidisciplinary approach to treating spinal cord injuries.
Dvorak et al. present results of long term follow-up after traumatic central cord syndrome. They found average improvement of ASIA motor scores (AMS) from 58.7 to 92.3. Bowel and bladder control returned in 81% and independent ambulation returned in 86%. Variables correlated with final AMS were AMS at injury, formal education, and presence of spasticity during follow-up.
Illustration A shows the blood supply to the spinal cord. Illustration B shows the area affected by central cord syndrome to help explain why it produces the described deficits.
Incorrect answers:
may be seen in the presence of congenital cervical stenosis. However, this is not the most common cause. Answer 4: Aortic aneurysm repair would more commonly lead to anterior cord syndrome.
Question 56
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury,
a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation endpoints: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 57
Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active

Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
Question 58
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Explanation
REFERENCES: Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806.
Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
Schwarz EM: Infections in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 59
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 60
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?

Explanation
Question 61
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 62
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
REFERENCE: Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, p 1465.
Question 63
A 78-year-old woman reports a 1-week history of severe low back pain. She denies any trauma or recent falls. She is neurologically intact, and is able to ambulate, although she does require the use of a walker. Radiographs of the lumbar spine show a T11 compression fracture with a 20% loss of anterior column height. What is the most appropriate management at this time? Review Topic
Explanation
Question 64
A study is being designed to compare the effectiveness of an antibiotic. The choice of the number of patients (ie, the sample size) depends on several factors. What type of calculation assesses the potential of the study to successfully address the effectiveness of the antibiotic?
Explanation
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 65
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
REFERENCE: Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 66
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 67
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?
Explanation
REFERENCES: Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Bilos ZJ, Pankovich AM, Yelda S: Fracture-dislocation of the radiocarpal joint: A clinical study of five cases. J Bone Joint Surg Am 1977;59:198-203.
Question 68
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
REFERENCE: St Pierre P, Olson EJ, Elliott JJ, et al: Tendon healing to cortical bone compared with healing to a cancellous trough. J Bone Joint Surg Am 1995;77:1858-1866.
Question 69
Primary arthrodesis is associated with which outcome when compared to outcomes associated with open reduction and internal fixation (ORIF) without arthrodesis?
Explanation
There are longitudinal, oblique, and transverse ligaments at the TMT complex that are further defined by their location as dorsal, interosseous, or plantar. There are 3 ligaments between the medial cuneiform and the second MT base, the most important of which is the oblique interosseous ligament, which is also known as the Lisfranc ligament. Plantar and dorsal oblique ligaments contribute to stability to a lesser degree. The dorsal ligaments are weakest and may be the first to fail in a Lisfranc injury.
The second MT base should be aligned with the middle cuneiform at the medial borders, and the fourth MT base should be aligned with the cuboid at the medial borders on the oblique view. The dorsal and plantar aspects of the MTs
should align with the cuneiforms/cuboid on the lateral view. Any malalignment should raise the suspicion of a Lisfranc injury. Diastasis between the second MT and the first MT/medial cuneiform complex of more than 2 mm indicates injury, as does TMT joint subluxation of 2 mm more than seen on the uninjured contralateral side. Diastasis between the first and second MT up to 2.7 mm can be normal. Another radiographic sign of injury includes avulsion fracture of the second MT base or medial cuneiform. Additional imaging studies that may be helpful in identifying subtle injuries include weight-bearing radiographs and CT or MRI images.
Two prospective randomized studies compared primary fusion with ORIF Lisfranc injuries. The second study included fracture-dislocations, whereas the first looked at primarily ligamentous injuries. Results conflicted with an earlier study demonstrating improved results (less pain, better function) with primary fusion, while a more recent study showed no difference. Neither study showed worse results with primary fusion, and the rate of secondary surgery was more common in the ORIF group (salvage arthrodesis or hardware removal).
RECOMMENDED READINGS
Solan MC, Moorman CT 3rd, Miyamoto RG, Jasper LE, Belkoff SM. Ligamentous restraints of the second tarsometatarsal joint: a biomechanical evaluation. Foot Ankle Int. 2001 Aug;22(8):637-41. PubMed PMID: 11527024.View Abstract at PubMed
Watson TS, Shurnas PS, Denker J. Treatment of Lisfranc joint injury: current concepts. J Am Acad Orthop Surg. 2010 Dec;18(12):718-28. Review. PubMed PMID: 21119138.View Abstract at PubMed
Faciszewski T, Burks RT, Manaster BJ. Subtle injuries of the Lisfranc joint. J Bone Joint Surg Am. 1990 Dec;72(10):1519-22. PubMed PMID: 2254360.View Abstract at PubMed
Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816.View Abstract at PubMed
Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583. View
Abstract at PubMed
Question 70
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
Explanation
REFERENCES: Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Pugh DM, Wild LM, Schemitsch EH, et al: Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86:1122-1130.
Question 71
The spread of malignant cells to the vertebrae is often through
Explanation
REFERENCE: Batson OV: The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-149.
Question 72
During the first stage of osteoarthritis, which of the following processes predominates?
Explanation
aggrecan concentration are both decreased. Increased water content tends to decrease the stiffness of the matrix, rendering cartilage tissue more susceptible to further mechanical damage. In the second stage, chondrocytes detect tissue damage and respond by releasing mediators to increase proliferation. Clusters or clones of proliferating chondrocytes are hallmark of the response to articular degeneration. In the third stage, both the proliferative response and anabolic activity are decreased. In this stage, the loss of articular cartilage is more evident and leads to clinical signs of degenerative joint disease.
Question 73
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 74
What is the primary mechanism of degradation of calcium phosphate cement?
Explanation
To treat depressed tibial plateau fractures, surgeons must elevate the depressed segments, which results in a metaphyseal bone void. This void can be filled with multiple materials, including autograft and allograft bone. The addition of BMP-2 or BMP-7 is not recommended to fill contained bone defects. These materials are indicated for application between bone and soft tissue and they do not provide the volume or strength to fill closed defects. Calcium phosphates have been use to fill these voids, demonstrating improved strength and resistance to subsidence when compared to autograft. Although polymethylmethacrylate is commonly used to fill bone voids in patients with cancer, it is not preferred in the setting of acute fracture because of the exothermic reaction that may compromise local bone healing. Although hydroxyapatite may be degraded by macrophage and giant-cell-mediated processes, the calcium phosphate degrades mainly by an osteoclast-mediated method. The calcium phosphate is not soluble in interstitial fluid, so simple dissolution does not occur.
RECOMMENDED READINGS
Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J Bone Joint Surg Am. 2008 Jun;90(6):1186-
Question 75
The failure of the acetabular component shown in Figure 15 is most likely the result of the use of a 32-mm head and
Explanation
REFERENCE: Astion DJ, Saluan P, Stulberg BN, Rimnae CM, Li S: The porous-coated anatomic total hip prosthesis: Failure of the metal-backed acetabular component. J Bone Joint Surg Am 1996;78:755-766.
Question 76
What is the most specific physical examination finding? Review Topic

Explanation
Question 77
A 35-year-old man presents with mechanical knee pain after a fall. An arthroscopic picture taken during diagnostic arthroscopy is shown in Figure A. His surgeon considers treatment with Technique B and Technique C, which are shown in Figures B and C, respectively. Which of the following statement is true with respect to Technique B and C? Review Topic
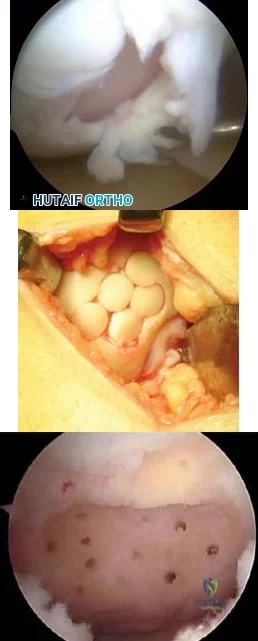
Explanation
The initial treatment for small articular cartilage defects is rest, NSAIDS and bracing. For larger defects (<2-4cm2), options include marrow stimulation procedures (abrasion chondroplasty, microfracture, osteochondral drilling) and autograft procedures (Mosaicplasty, a technique of osteochondral autograft transfer (OAT).
Alford et al. reviewed cartilage restoration. They defined a spectrum of treatment option ranging from (1) palliative (debridement/lavage), intended to reduce irritation
and inflammation, (2) reparative (marrow stimulation techniques), intended to recruit stem cells to proliferate fibrocartilage repair tissue, to (3) restorative (osteochondral grafting), designed to replace articular cartilage and subchondral bone as a single unit.
Magnussen et al. reviewed the treatment of cartilage defects in the knee. They compared autologous chondrocyte implantation (ACI), OATs, matrix-induced ACI, and microfracture. No one technique was superior to the rest. Outcomes for microfracture tended to be worse in larger lesions.
Figures A is an arthroscopic picture showing a grade IV chondral defect. Figure B shows microfracture. Figure C shows the multiple cylindrical plugs of mosaicplasty, a technique of osteochondral autograft transfer (OAT). Illustration A shows donor and recipient sites in mosaicplasty. Illustration B shows the spectrum of treatment options defined by Alford et al (MST = marrow stimulation; ACI = autologous chondrocyte implantation; OCG = osteochondral grafting with autograft/allograft).
Incorrect Answers:
Question 78
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 79
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule? Review Topic
Explanation
Question 80
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 81
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 82
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 83
Initial management of a pathologic fracture of the humerus secondary to a unicameral bone cyst should include
Explanation
REFERENCES: Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224.
Bensahel H, Jehanno P, Desgrippes Y, Pennecot GF: Solitary bone cyst: Controversies and treatment. J Pediatr Orthop B 1998;7:257-261.
Question 84
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 85
Citrate dextrose - anticoagulant used with whole blood during the process of preparation of the PRP before centrifugation. 3,4,5) TGF-beta, IL-8, and PDGF are all proteins released by the platelets upon activation.
Explanation
Arrington et al reviewed 414 consecutive iliac crest harvest procedures and reported a 10% rate of minor complications and 5.8% of major complications (deep infection, nerve injuries, herniation, fractures, hematomas). They note that with proper surgical technique, the incidence of the complications can be minimized.
Ahlmann et al compared the morbidity related to the harvest of anterior iliac crest bone graft with that related to the harvest of posterior iliac crest bone graft and to determine differences in functional outcome. The rates of both minor complications (p = 0.006) and all complications (p = 0.004) were significantly higher after the anterior harvest procedures than they were after the posterior procedures. The postoperative pain at the donor site was significantly more severe (p = 0.0016) and of significantly greater duration (p
= 0.0017) after the anterior harvests.
Which of the following statements is inaccurate in describing the origin and purpose of the Institutional Review Boards (IRB)?
Began with the Nuremberg Code of Medical Ethics, which was developed by the Nuremberg Military Tribunal after the investigation of Nazi physicians
Fetuses, pregnant women, and children are considered vulnerable populations but prisoners are not
Emphasizes dignity and autonomy, and encompasses informed consent (quid vide)
The process for obtaining informed consent for patients included in clinical trials is mandated by the Institutional Review Board (IRB).
Requires fair selection of subjects and equal distribution of the benefits and burdens of research
Fetuses, pregnant women, prisoners, and children are all considered vulnerable populations by Institutional Review Boards (IRB). The process for obtaining informed consent for patients included in clinical trials is mandated by the IRB.
The article by Fisher is a commentary that reviews the clinical trials industry. She urges researchers to communicate the larger details of the research enterprise to patients and to compensate for asymmetrical power relations in society as a whole. Without these things, she believes, it will be impossible to protect against misunderstandings and therapeutic misconceptions.
Which of the following best describes a Bonferroni correction?
An analysis that starts with a particular probability of an event (the prior probability) and incorporates new information to generate a revised probability (a posterior probability)
Human behavior that is changed when participants are aware that their behavior is being observed.
Used to assess the relationship between two normally distributed continuous variables
A post-hoc statistical correction made to P values when several dependent
or independent statistical tests are being performed simultaneously on a single data set
The ability of a study to detect the difference between two interventions if one in fact exists
A Bonferroni correction is a post-hoc statistical correction made to P values when several dependent or independent statistical tests are being performed simultaneously on a single data set.
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect Answers:
A 10-year-old child falls from a standing height and sustains the injury shown in Figure A. Her medical history includes hearing defects and the facial appearance shown in Figure B. In addition to operative fixation of her fracture she is scheduled to receive cyclical intravenous
pamidronate administration as a treatment after the fracture is healed. Which of the following is associated with this form of treatment?
No change in bone pain
No change in future fracture incidence
An increase in osteoblast density
An increased risk of secondary osteosarcoma
An increase in bone density
The history and images are consistent with osteogenesis imperfecta (OI). Olecranon avulsion fractures are often seen in patients with OI and children presenting with these should be evaluated for OI. The clinical image of blue sclera can also be a characteristic finding in patients with OI. The Bisphosphonates have been shown to decrease fracture incidence and bone pain while improving bone density and overall function in OI patients.
Zeitlin et al performed a Level 5 review of OI. They state that Sillence Types I through IV are a mutation in the COL1A1 and COL1A2 genes that encode type I collagen. They report that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence, and increases bone density and
level of ambulation.
Burnei et al also performed a Level 5 review of OI. They report that the use of bone marrow transplantation to increase osteoblast density in OI patients is currently being
researched as a potential treatment of OI.
A 35-year-old male presents with pain and limited range of motion 3 months after arthroscopic Bankart repair of his right shoulder. His postoperative course included a continuous intra- articular infusion pump for 3 days, use of a sling for 4 weeks, and initiation of passive range of motion below the level of the shoulder. At 4 weeks postoperatively he started active range of motion exercises, and started an isotonic strengthening program at the 9 week interval. Which of the following options is the MOST appropriate step in his management?
Reassurance and appropriate followup
Focused physical therapy on aggressive ROM exercises and modalities
Intra-articular injection of corticosteroids to decrease post-operative inflammation
Shoulder radiograph series to assess for chondrolysis
Arthroscopic vs open Bankart revision surgery for failed repair
The above patient was issued an intra-articular infusion of lidocaine for pain control after his surgery and may have developed shoulder chondrolysis. This complication after the use of intra-articular pumps has recently become more well known. The U.S. Federal drug and Administration (FDA) has issued a warning on the adminstration of continuous intra-articular infusion of local anesthestics for pain control.
The FDA has reviewed 35 cases of patients developing chondrolysis after intra- articular infusions, some being as early as 2 months after their surgery. The average time of diagnosis in these cases with chondrolysis were at an average of 8.5 months after the infusion. The majority of the reported cases occurred following shoulder surgeries. Joint pain, stiffness, and loss of motion were the most common physical complaints. As a result of their findings, the FDA issued
a warning for surgeons to be aware and monitor for signs and symptoms of chondrolysis.
Illustration A shows a radiograph consistent with chondrolysis in a patient status post arthroscopic Bankart repair. This image shows the loss of joint height in the glenohumeral joint due to chondrolysis. Also, 2 suture anchors are visible as well in the glenoid from the Bankart repair. Illustration B shows an arthroscopic image of chondrolysis and Illustrations C and D demonstrate chondrolyis viewed from an open approach.
Regarding bone densitometry, a T-score of -3.5 is defined as which of the following?
Normal bone
Osteopenia
Age appropriate bone loss
Osteoporosis
None. One cannot make this diagnosis without further information.
A T-score of -3.5 is defined as osteoporosis, regardless of the other clinical factors.
As described in the review by Kanis et al., the World Health Organization (WHO) has defined the following categories based on bone density in white women:
Normal bone: T-score greater than -1 Osteopenia: T-score between -1 and -2.5 Osteoporosis: T-score less than -2.5
The WHO committee did not have enough data to create definitions for men or other ethnic groups. T-score is a comparison of a patient's BMD to that of a healthy thirty-year- old of the same sex and ethnicity. Z-score is the number of standard deviations a patient's BMD differs from the average BMD of their age, sex, and ethnicity.
A 67-year-old female presented 2 months ago to her primary care physician with left sided thigh pain. A radiograph was taken at that time and is shown in Figure A. She was diagnosed at that time with a quadriceps strain and given a prescription for ibuprofen and physical therapy. She is now in the emergency room with severe left thigh pain and inability to bear weight on the left lower extremity after bending down to tie her shoes. She denies any constitutional symptoms. A current radiograph from the emergency room is shown in Figure B. Which of the following most likely explains this patient's fracture?
Long-term corticosteroid use
Secondary malignancy arising from Paget disease
Long-term alendronate use
Long-term ergocalciferol use
Short-term teraparatide use
Subtrochanteric stress reaction (Figure A) and low-energy transverse fracture (Figure B) is a complication of long-term bisphosphonate use documented in the literature. Of note, a healed right sided subtrochanteric femur fracture is also visualized in Figure A.
Neviaser et al conducted a Level 4 study of 70 patients with low energy femur fractures. They found that a simple, transverse pattern and hypertrophy of the diaphyseal cortex are associated with alendronate use with 98% specificity. They report that the average alendronate usage time was 6.9 years in patients exhibiting this pattern of fracture.
Capeci et al performed a Level 4 review of alendronate therapy and its association with unilateral low-energy subtrochanteric and diaphyseal femur fractures. They recommended consideration of discontinuing alendronate with the consultation of an endocrinologist if a fracture occurs. They also recommend routine contralateral leg surveillance after to rule out contralateral stress fracture. If contralateral stress fracture is found, it it is recommended that it is treated with prophylactic intramedullary fixation.
Imaging typically shows lateral cortical thickening in the subtrochanteric femur as demonstrating on the coronal and axial CT scans shown in Illustration A and B, respectively.
In the study by Moseley et al published in the New England Journal of Medicine, 180 patients with knee osteoarthritis were randomly assigned via sealed envelope to receive arthroscopic débridement, arthroscopic lavage, or placebo surgery. Outcomes were assessed by blinded evaluators at several points over a 2 year period
with the use of five self-reported pain and function scores. There was a greater than 90% follow-up in the study. This study is best described as having which level of evidence?
Therapeutic study, evidence level I
Therapeutic study, evidence level II
Diagnostic study, evidence level I
Diagnostic study, evidence level II
Prognostic study, evidence level I
Therapeutic studies investigate the results of treatment. Level 1 evidence includes randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence interval.
A level II therapeutic study would include a lesser-quality randomized controlled trial (eg,
<80% follow-up, no blinding, or improper randomization). A non-randomized prospective cohort study that compares the results of treatment or systematic reviews of level II studies or level I studies with heterogenous results would also be considered a level II study.
Prognostic studies investigate the effect of a patient characteristic on the outcome of disease. Diagnostic studies investigate the efficacy of a diagnostic test. Illustration A is a table detailing the levels of evidence.
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
Per-protocol
Crossover analysis
Intent-to-treat
Bayesian analysis
Effect size
The following is an example of intent-to-treat analysis.
The intent-to-treat approach aims to keep similar groups similar by not
allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per- protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
guidelines
A 32-year-old male is being seen in your office for evaluation of a possible rotator cuff tear. He has been seen in your office by one of
your partners previously after surgical treatment of a femoral shaft fracture. How much time has to pass since last evaluation or treatment in your group for this patient to revert to a new patient under CPT guidelines?
6 months
1 year
18 months
2 years
3 years
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.” By contrast, an established patient has received professional services from the physician or another physician in the same group and the same specialty within the prior three years.
The referenced study by Shalowitz reviewed 500 Medicare claims and found an overall coding error rate of 32.4%, with high levels of consultation coding errors. He reports that changing ambulatory consultation codes to those for new patient visits would save Medicare $534.5 million per year.
As a result of this study, as well as others, Medicare does not recognize consultation codes.
A 55-year-old healthy female presents for a routine physical exam. When discussing bone health and osteoporosis prevention, what dose of calcium and vitamin D should be recommended for daily consumption?
1,500mg of calcium and 1,000 IUs of vitamin D
2,200mg of calcium and 1,000 IUs of vitamin D
750mg of calcium and 5,000 IUs of vitamin D
750mg of calcium and 10,000 IUs of vitamin D
2,200mg of calcium and 5,000 IUs of vitamin D
The National Osteoporosis Foundation recommends a daily intake of 1,200- 1500mg of calcium 800-1,000 IUs of vitamin D for adults over the age of 50.
The review article by Gehrig et al discusses the factors surrounding osteoporosis that can be modified to optimize fracture risk reduction. They report that non-prescription interventions such as calcium and vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs are treatment options.
What is the function of the core binding factor alpha-1 (Cbfa1/Runx2)?
Phosphorylation and intracellular activation of signal transducers and activators of transcription (STATs)
Chemotaxis of mesenchymal stem cells to sites of skeletal fractures
Tumor-induced osteolysis
Osteoclastic apoptosis
Osteoblastic differentiation
As described by Ducy et al., Cbfa1/Runx2 is a key transcription factor associated with osteoblast differentiation, skeletal morphogenesis, and acts as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression. A stop codon mutation in the Cbfa 1 gene causes cleidocranial dysplasia. Stem cell chemotaxis (moving to various sites in the body) is accomplished through a variety of cytokines, one of which is platelet derived growth factor. Tumor-induced osteolysis occurs secondary to tumor-produced cytokine activation of osteoclasts. Osteoclastic apoptosis occurs secondary to bisphosphonates.
Ballock and O'Keefe review the development, growth, and complex cytokine interaction required for normal growth plate function.
A 20-year-old male is involved in motor vehicle collision and sustains a depressed tibial plateau fracture. When performing surgery, if calcium sulfate is used as the primary bone substitute void filler, an increase in which of the following outcomes may be expected as compared to autograft?
Increased complications due to serous drainage
Improved clinical outcomes as shown by more rapid time to healing
Improved clinical outcomes as shown by SF-36 scores
Increased complications due to autoimmune reactions and graft rejection
Equivalent complication rates and clinical outcomes
Calcium sulfate bone graft substitute has demonstrated an increased rate of serous drainage at the surgical site. Evidence examining the use of calcium sulfate in the treatment of bone nonunions revealed a significant failure rate, suggesting that this material, used in isolation, is not optimal to promote union in that setting.
Beuerlein and Mckee reviewed the literature, showing that calcium sulfate is
an effective void filler in metaphyseal defects after impacted fracture reduction (calcaneus, tibial plateau) or simple bone cysts. However, they report that calcium sulfate is associated with serous wound drainage especially when used at subcutaneous sites and in amounts greater than 20ml.
Ziran et al present a series of 41 patients undergoing bone grafting for atrophic/avascular nonunions with adjunctive calcium sulfate-demineralized bone matrix (Allomatrix). Of the 41 patients, 13 (32%) had drainage that necessitated surgical procedures and 14 (34%) developed a deep infection.
A 46-year-old female begins to have personality changes, cognitive decline, and chorea. Her father began having similar but less severe symptoms at age 55 before passing away 6 years later. One of her 2 older siblings has also begun to show deterioration. Which of the following describes the hereditary pattern of this disease?
Autosomal dominant with variable penetrance
Autosomal recessive with variable penetrance
X-linked recessive
Autosomal dominant with anticipation
Autosomal dominant with imprinting
This clinical vignette describes a patient with Huntington's disease. Huntington's disease has an autosomal dominant hereditary pattern with anticipation.
Anticipation is a term used to describe trinucleotide repeat
disorders that if passed on, will present earlier and more severely in affected subjects than in their affected parent. In Huntington's disease, it is due to a "CAG" trinucleotide repeat on chromosome 4. Subjects with an affected parent have a 50% chance of inheriting the disease from them, and if present will have more severe disease.
Deighton et al provide a review on the genetics of musculoskeletal disease including the hereditary pattern of anticipation.
All of the following are indications for locked plating technology EXCEPT:
Periarticular fracture with metaphyseal comminution
Fracture in osteoporotic bone
Bridge plating for severely comminuted fractures
Compression plating of transverse fracture
Plating of fractures where anatomical constraints prevent plating on the tension side of the bone
Locked plates are indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone.
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Approaches to internal fixation have become more biologic. Greater emphasis is placed on vascularity and soft tissue integrity. Locked plates, analogous to rigid internal fixators, can provide relative stability favorable to secondary fracture healing. If applied appropriately, they can
avoid soft tissue compromise. The key to this new generation of plates is the locking mechanism of the screw to the plate, which provides angular stability and avoids compression of the plate to the periosteum. Favorable biomechanical and clinical results continue to expand the number of appropriate indications for use of locked plating devices, although exact indications for their use have yet to be precisely defined.
The referenced articles by Haidukewych and Egol et al are reviews of the biomechanical characteristics of locked plating technology.
Which of the following lists these materials in order of increasing modulus of elasticity?:
Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Which of the following substances increases the chondrogenic phenotype of intervertebral disk cells and matrix synthesis?
Osteoprotegrin
Osteonectin
Hyperosmotic saline
Corticosteroids
Bone morphogenic proteins
Bone morphogenic proteins have been shown to increase chondrogenic phenotype expression and increase matrix synthesis of the intervertebral disc in animal studies.
Bone morphogenetic protein-2, bone morphogenetic protein-7, and
transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of the disk matrix. Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
Miyamoto et al. evaluated rabbits that underwent annulus fibrosus (AF) injury where they either injected a control or BMP into the nucleus pulposus. The BMP injection significantly restored disc height and improved the modulus as compared to control injections. They concluded the biochemical data suggested that the OP-1-induced restoration of the disc space was a consequence of the increased activity of anabolic pathways that resulted in biochemical changes in the IVD.
Kim et al. evaluated mRNA levels of BMP-2, BMP-7, and TGF-beta in a rabbit model of intervertebral discs. Compared to young rabbits, old rabbits generally had higher levels of mRNA expression of these three cytokines in both the annulus fibrosus and nucleus pulposus. The similar patterns of up-regulation in gene expression with age shown by these 3 anabolic cytokines suggest a common pathway in terms of regulation and transcription in the early stage of disc degeneration.
Incorrect Answers:
A colleague is struggling to obtain a perfect lateral radiograph for distal locking screw placement. Other than good technique, how might the surgeon best reduce the amount of radiation exposure to the patient and personnel when using fluoroscopy?
The use of continuous fluoroscopy while manipulating the leg
Standing directly behind the cathode ray tube
Advising the technician to position the fluoroscopy beam on command
Placement of the image intensifier receptor as close to the patient as possible
Placement of the cathode ray tube as close to the patient as possible
Placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Numerous steps have been described to decrease radiation in the operating room. They include:
Decrease time of exposure
Decrease dose of exposure
Beam collimation
The use of mini C arm
Inverting the C arm (shortens distance between body part and collection surface)
Surgeon’s control of the C arm
Use of protective equipment (glasses, thyroid shields, aprons)
Increase the distance from the X ray source
Maniscalco et al. compared the amount radiation exposure during open lumbar microdiscectomy and minimally invasive microdiscectomy. MIS lumbar microdiscectomy cases expose the surgeon to significantly more radiation than open microdiscectomy.
Interestingly, standing in a substerile room during x- ray localization in open cases is not fully protective.
Illustration A shows an image of radiation scatter with fluoroscopy. Radiation hits the patient’s tissue, interacts and then changes direction. The greatest dose received is directly perpendicular to the fluoroscopy and next to the patient.
Incorrect Answers:
A 72-year-old active man presents with chronic right-sided pelvic pain for the last 2 years. His radiographs are depicted in Figure A. He has tried multiple courses of activity modification and anti- inflammatory medications to no avail. His orthopedic oncologist performs a biopsy (depicted in Figure B) and elects to initiate Zoledronate. Which of the following is a known complication
associated with this treatment if rendered long-term?
Malignant degeneration to osteosarcoma
Malignant degeneration to chondrosarcoma
Malignant degeneration to fibrosarcoma
Atypical distal femur transverse fractures
Osteonecrosis of mandible
This patient's pelvic radiograph reveals cortical thickening, coarse trabeculae, and sclerosis, which is characteristic of Paget's disease, depicted in the histological section in Figure B. Bisphosphonate treatment is an appropriate treatment for Paget's disease. However, long-term administration of intravenous (IV) bisphosphonates (i.e.
Zoledronate) may result in osteonecrosis of the jaw.
Osseous lesions from Paget's disease have increased osteoclastic bone resorption, marrow fibrosis, increased bone vascularity, and increased disorganized bone formation, resulting in a mosaic (woven and lamellar bone) appearance on histology. Asymptomatic patients may be treated with
observation and symptomatic management reserved as first-line management. When recalcitrant to symptomatic management, bisphosphonate therapy helps control osteoclast lytic activity and reduces pain. However, when administered long-term, side-effects may include atypical subtrochanteric femur fractures and jaw osteonecrosis (especially when given IV). Administration of Teriparatide (Forteo) is contraindicated in these patients due to the increased risk of Pagetoid malignant transformation. Malignant transformation to Paget's sarcoma occurs in 1% of patients.
Langston et al. performed a randomized trial of intensive bisphosphonate treatment versus symptomatic management in Paget's disease of bone. They reported that while serum alkaline phosphatase (ALP) levels were significantly lower in the intensive treatment group than in with the symptomatic treatment group, there was no difference in the quality of life, pain scores, hearing loss, or rates of surgical intervention in the two cohorts. They concluded that
striving to maintain normal ALP levels with intensive bisphosphonate therapy confers no clinical advantage over symptom-driven management in patients with Paget's disease of bone.
Figure A demonstrates Paget's disease of the right hemipelvis. Figure B demonstrates the
histology of Paget's disease of bone (woven bone and irregular broad trabeculae with disorganized cement lines in a mosaic pattern). Illustration A and B demonstrate osteonecrosis of the jaw and atypical subtrochanteric femur stress fracture, respectively, after long-term bisphosphonate use.
Incorrect Answers:
A long oblique diaphyseal fracture is internally fixed with 2 lag screws. There is 2 mm of residual fracture fragment gap following screw fixation. This construct has which of the following compared to a comminuted diaphyseal fracture
internally fixed with a long bridge plating technique?
Greater interfragmental strain
Greater ductility
Greater primary Haversian remodeling
Greater union rate
Greater callus volume formation
A long oblique diaphyseal fracture with 2 mm of residual displacement after being internally fixed with lag screws has greater interfragmental strain than comminuted fractures treated with bridge plating or fractures that are anatomically reduced and internally fixed.
Perrens’ theory of strain states that there is a relationship between decreasing strain and increasing the potential for osteogenesis across a fracture or fusion site. The strain theory states that for two given fracture segments, the healing interface will possess a force- generated motion potential that is contingent on the stability of the original fixation construct. Mathematically, the strain for
any given force is equal to the change in the interface length divided by the original interface length. Therefore, with an unstable construct, the healing gap may undergo excessive motion with resultant increasing strain. It has been shown that strain of less than 2% will yield absolute stability and subsequent primary bone healing. Comminuted fractures have multiple fracture lines therefore the force is dissipated over multiple fracture lines and interfragmentary strain is decreased.
A 75-year-old woman presents with acute severe back pain after sustaining a mechanical fall while walking out of her yard. She denies pain in her buttocks or legs. On physical exam she has point tenderness over the L1 spinous process. Figure A depicts her current radiograph. Which of the following statements is true regarding here underlying metabolic condition and associated pathology?
Kyphoplasty is indicated within the first week if the pain is severe enough to warrant narcotic medication.
Her underlying metabolic bone condition leads to decreased bone quantity with normal bone quality.
A DEXA T-score of -2.1 in this individual would confirm the diagnosis of osteoporosis according to the WHO.
A 25-hydroxy Vitamin D level of 16ng/mL in this individual would confirm the diagnosis of osteoporosis according to the WHO.
The fracture pattern in Figure A is the third most common fragility fracture in the United States
This clinical presentation is consistent with an L1 osteoporotic compression fracture due to underlying osteoporosis. Osteoporosis is characterized by decreased bone quantity with normal bone quality.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Vertebral compression fractures are the most common type of fragility fracture in patients with osteoporosis. Management should begin with a proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology.
Evaluation includes bone densitometry, lab testing of Vitamin D and calcium. The World Health Organization (WHO)
classifies bone density in postmenopausal women based on T-scores, with classification based on the lowest T-score of the spine, femoral neck, trochanter, or total hip. Osteoporosis is defined by T-scores 2.5 or greater standard deviations below the peak bone mass of a 25-year-old individual.
Gehrig et al. published an Instructional Course Lecture on the management and treatment strategies for orthopaedic surgeons. They reported that osteoporosis may be present in patients with and without fracture and that the ultimate goal in managing and treating osteoporosis is to optimize fracture risk reduction. They recommended non-pharmacologic interventions including calcium, vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs to minimize fracture risk.
The United States Preventive Services Task Force published clinical guidelines on osteoporosis screening. They recommended screening for osteoporosis in women aged 65 years or older and in younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors. They concluded that the current evidence is insufficient to assess the balance of risks and benefits of screening for osteoporosis in men.
Figure A depicts an L1 vertebral compression fracture. Incorrect Answers:
year-old woman with long standing rheumatoid arthritis presents with worsening bilateral foot pain. She sees a podiatrist for shaving of her plantar forefoot calluses. She has tried orthotics and custom shoes but notes worsening foot pain that is limiting her daily activities. Plain radiographs of her feet are pictured in Figure A. Which
of the following images depicts the surgical treatment that would result in the best functional outcome for this patient?
This patient has a classic rheumatoid arthritis (RA) forefoot deformity and would benefit most from first metatarsophalangeal (MTP) joint fusion, hammertoe correction and lesser metatarsal (MT) head resections, pictured in Figure E.
Nearly 90% of patients with chronic RA develop forefoot deformities, most commonly hallux valgus, fixed hammering of the lesser toes and subluxation/dislocation of the lesser MTP joints. Nonoperative management includes orthotic use and shoewear modification. The gold standard surgical treatment involves stabilization of the first ray with a first MTP joint fusion, hammertoe correction and resection of the lesser MT heads (Hoffman-Clayton procedure).
Coughlin et al highlighted that achievement of stable realignment of the first ray is the key factor in reconstruction of a RA forefoot. Stable fusion of the first MTP joint increases weight-bearing along the medial column, minimizes stress on the lesser MTP joints and protects the relocated plantar fat pad. Patients who underwent first MTP fusion, lesser MT head resections and open hammertoe correction had a high level of satisfaction postoperatively.
Mann et al performed a retrospective review of 20 patients with severe RA forefoot deformities who underwent first MTP joint fusion. These patients demonstrated an increase in weight-bearing of the hallux and resultant decrease in metatarsalgia and plantar callosities compared to patients who underwent a first MTP resection arthroplasty
(Keller arthroplasty). The patients in this study noted significant functional improvement postoperatively and no patients required custom shoes or orthotics.
Figure A is an AP radiograph of bilateral feet demonstrating the classic RA forefoot deformity with severe hallux valgus, dislocation of the lesser MTP joints and erosive changes of the MT heads. Figure B shows a hallux valgus realignment procedure with a distal osteotomy and hammertoe correction with a 2nd MT shortening osteotomy (Weil osteotomy), proximal interphalangeal (PIP) joint resection and K wire fixation. Figure C displays a first tarsometatarsal (TMT) joint fusion (Lapidus procedure) and Weil osteotomies
of the 2nd through 4th MTs. Figure D demonstrates a first MTP joint fusion and Weil osteotomies of the 2nd through 4th MTs. Figure E shows a first MTP joint fusion, resection of the 2nd through 5th MT heads and hammertoe correction with PIP joint resection and K wire fixation. Figure F displays a resection of the
first MTP joint proximal phalanx base (Keller arthroplasty) and hammertoe correction with PIP joint resection and K wire fixation.
Incorrect Responses:
What type of fracture healing occurs in a femoral shaft fracture treated with an intramedullary nail?
Primary fracture healing
Secondary fracture healing
Extramembranous ossification
Haversian remodelling
"Cutting cone" remodelling
Intramedullary nails function as internal splints that allow for secondary fracture healing.
Secondary bone healing involves responses in the periosteum and external soft tissues. Here both committed osteoprogenitor cells and uncommitted undifferentiated mesenchymal cells contribute to the process of fracture healing by recapitulation of embryonic intramembranous ossification and endochondral bone formation. The response from the periosteum is a fundamental reaction to bone injury and is enhanced by motion and inhibited by rigid fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intrameduallary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extra
osseous circulation and applies bone graft to the fracture site.
Illustration A shows a series of radiographs of a fracture healed by secondary intention with an IM nail.
Incorrect Answers:
healing of bone.
A 67-year-old woman sustained the injury shown in Figure A approximately 14 months ago, which was managed with closed reduction and casting. She presents with new symptoms of hyperalgesia, allodynia, and hyperhidrosis of her wrist. She denies any recent fevers or chills. Her current radiographs reveal a well-healed fracture without any significant malunion. What is the
pathophysiology likely attributable to her current symptoms?
Pre-ganglion brachial plexopathy
Aberrant inflammatory and vasomotor response
Exaggerated vasoconstriction of the wrist and digital arteries
Incomplete glycosaminoglycan breakdown products causing dysfunction
Connective tissue disorder
The patient is presenting with complex regional pain syndrome (CRPS) after a healed distal radial fracture. The pathophysiology of CRPS is that of aberrant inflammatory and vasomotor response in a region of prior trauma resulting in pain out of proportion, skin discoloration, and vasomotor disturbances.
Patients who develop CRPS often have a history of trauma, but the condition may also occur after surgery. Common symptoms of CRPS include hyperalgesia, often described as burning, throbbing, shooting, or aching. Patients may also experience hyperalgesia, allodynia, and hyperpathia. More objective signs of CRPS may include motor dysfunction (tremors, dystonia, loss of strength), skin, hair, and other trophic changes about the affected extremity, as are symptoms of autonomic dysfunction. CRPS is often sub- classified into 2 types. Type 1 is more common and does not involve specific nerve damage, whereas type 2 involves damage to a specific nerve.
Hogan et al. reviewed the evaluation and treatment of complex regional pain syndrome. They report that although there are many divergent and often conflicting theories, the cause of the severe pain, alterations in regional blood flow, and edema noted in CRPS is unknown. They concluded that CRPS is a challenging diagnosis and as such should be managed by a multidisciplinary team, including chronic pain management specialists,
physical therapists, and orthopedic surgeons.
Shah et al. reviewed the diagnosis and treatment of CRPS. They reported that sweat quantification testing, skin thermography, and electromyography may
be useful in the diagnosis of CRPS, but these tests are often unreliable given is a lack of diagnostic sensitivity. They concluded that the treatment of CRPS remains controversial, and includes medications (antiepileptics, antidepressants, NSAIDS, bisphosphonates, free radical scavengers, vitamin C, and topical anesthetics), physical therapy, regional anesthesia, and neuro- modulation.
Figure A depicts an extra-articular distal radius fracture. Illustration A depicts an example of a wrist affected by CRPS, with notably increased swelling, which is a common finding in patients afflicted with the disease.
Incorrect Answers:
After application of a unilateral tibial external fixator, it is observed that the frame does not provide sufficient rigidity across the fracture site. Altering the external fixator in which of the following ways will have the greatest impact on frame stiffness?
Increasing the distance between pins in each fragment
Increasing the pin diameter
Reducing the distance between bone and connecting bar
Increasing the connecting bar diameter
Adding one stacked connecting bar
While all of the aforementioned factors will increase frame stiffness, pin diameter has the greatest influence on stability of unilateral frames.
Unilateral frames are distinguished from circular frames in that they are positioned on one side of the limb. The overall stability of the frame can be varied by altering the number of pins, the distance between pins, pin diameter, connecting rod diameter, number of connecting rods, distance between bone and connecting rods, and use of multiplanar fixation. The pin diameter has the biggest contribution, as the stiffness of the pin is correlated to the fourth power of its radius.
Fragomen et al. looked at the mechanics of external fixation. They state that the diameter of the half Schantz pin should be less than one-third of the bone diameter to minimize the risk of fracture at the pin site. Unicortical half pins also increase the risk of fracture.
Therefore, pins should be bicortical.
Tencer et al. examined the mechanical properties of external fixation. They showed that frame rigidity could be maximized by increasing the pin separation distance in each fracture fragment, increasing the number of pins and decreasing the sidebar offset distance from bone.
Illustration A shows a schematic of the factors contributing to frame stability. Incorrect Answers:
Locking plate technology is least indicated for which of the following Figures?
Of the fracture patterns listed, all have some indication for locking plate fixation except answer 2. Transverse midshaft both bone forearm fractures are typically treated with non- locked compression plating techniques.
The use of locking plate fixation is an evolving topic in orthopaedics, and exact uses may vary. Well accepted indications for locking plate fixation include indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging of severely comminuted fractures, and plating of fractures where anatomical constraints prevent plating on the tension side of the bone (e.g. short segment fixation).
Anglen et al. performed a level-IV meta-analysis of 33 papers reviewing the use and outcomes of locking plate fixation. They found no standard indications for use, and due to heterogeneity of the studies reviewed had no specific
recommendations for use.
Cantu et al. presented a level-V review of the use of locking plate fixation. They cite 5 indications for use: metaphyseal or intra-articular fractures, highly comminuted fractures particularly involving diaphyseal and metaphyseal bone, osteoporotic bone, proximal tibia and distal femur fractures, and periprosthetic fractures. They also cite 4 relative contraindications: fractures best served
with a construct other than a plate, severe soft tissue injury precluding placement of a plate, simple fracture patterns that can be adequately treated with non-locking constructs, and fractures that would require bending the plate.
Figure A is a comminuted Schatzker VI tibial plateau fracture. Figure B is a transverse both bone forearm fracture. Figure C is an intra-articular pilon fracture. Figure D is a comminuted distal humerus fracture. Figure E Vancouver B1 periprosthetic hip fracture.
Incorrect Answers:
All of the following are true regarding osteocalcin EXCEPT which of the
following?
It is the most prevalent non-collagenous protein in bone
It is expressed by mature osteoblasts
It is considered a marker for osteoblast differentiation
It is a glycoprotein that binds calcium
Higher levels are correlated with increases in bone mineral density during osteoporosis treatment
Pure fact question from basic science. “Osteocalcin is the most prevalent noncollagenous protein in bone” (from Miller's Review). It is expressed by mature osteoblasts and is a marker of osteoblast differentiation. Osteocalcin is the most specific marker of the osteoblast phenotype and is expressed only in mature osteoblasts. During osteoporosis treatment, serum levels correlate
with increases in bone mineral density. Osteonectin, not osteocalcin, is a glycoprotein that binds calcium.
An otherwise healthy young male sustains a significantly comminuted fracture of the 2nd metacarpal shaft and undergoes external fixation as definitive management. The type of bony healing obtained with this treatment is similar to the bony healing for the appropriate treatment of all the following injuries EXCEPT?
The patient has undergone external fixation for his 2nd metacarpal shaft fracture which is an example of enchondral healing (secondary bone healing) which occurs with non- rigid fixation, such as bracing, casting, external fixation, bridge plating, and intramedullary nailing. Of the images shown, Figure D is an example of a patient with an unstable Weber B ankle fracture
with a simple oblique pattern that would preferentially be treated with primary bone healing with ORIF (anatomic stability).
Bone healing occurs via primary healing (intramembranous healing, absolute stability) or secondary healing (enchondral healing, relative stability) depending on the method of fixation. Fractures that require primary bone healing are ones in which anatomic reduction without callus formation is preferred (peri-articular fractures, both bone forearm fractures, non- comminuted ankle fractures with disruption of the ankle syndesmosis).
Primary healing leads to healing via cutting cones and occurs without the production of any callus (which may impede rotation in both bone forearm fractures and cause articular malalignment in peri-articular and peri- syndesmotic fractures). Fractures that may be treated with secondary bone healing and callus formation, do not require anatomic stability and may have fracture site micromotion during the healing process. Intramedullary nailing, external fixation and closed treatment with bracing/splinting/casting all allow motion at the fracture site and lead to secondary bone healing.
Perren reviews the biological and mechanical properties of bone remodeling and the complex interplay of patient, injury and surgical factors that influence healing. The use of relative stability fixation techniques allows the bone to overcome the initial excess strain at a fracture site and build a scaffold that brings the strain to more reasonable levels. The author stresses the importance of understanding bone biology to select optimal implant and methods of surgical fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intramedullary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extraosseous circulation and applies bone graft to the fracture site.
Figure A shows the AP and lateral radiographs of a segmental oblique midshaft tibia fracture. Figure B is an AP radiograph of an unstable intertrochanteric femur fracture with disruption of the calcar. Figure C shows the AP and lateral radiographs of a midshaft transverse femur fracture. Figure D shows the AP and lateral radiographs of a simple oblique weber B ankle fracture with medial clear space widening. Figure E shows a displaced 5th metacarpal neck fracture with dorsal angulation.
Illustration A is the injury in Figure A treated with intramedullary nailing with resulted callus formation. Illustration B is the injury in Figure B treated with cephallomedullary nailing with resulting callus formation. Illustration C is the injury in Figure C treated with intramedullary nailing with resulting callus formation. Illustration D is the injury in Figure D treated with a lag screw and neutralization plating (anatomic stability). Illustration E is the injury in Figure
E treated with closed reduction and casting with subsequent healing with callus formation.
Incorrect Answers:
This is an example of secondary bone healing.
A 7-year-old recent immigrant presents with pain and tenderness over the legs. Physical exam shows the gums have a bluish-purple hue with areas of hemorrhages. A radiograph is shown in Figure A. In Figure B, what region of the growth plate is most affected in this condition?
A
B
C
D
E
The clinical presentation and radiographs are consistent with scurvy. The radiographs show a dense band (White line of Frankl) at the growing metaphyseal end which is characteristic of scurvy. Scurvy is a disease resulting from a deficiency of vitamin C (ascorbic acid), which is required for the synthesis of collagen in humans. Impaired collagen synthesis in scurvy leads to fragile capillaries, resulting in abnormal bleeding, and altered bone formation at the growth plate. More specifically, scurvy affects the spongiosa
the most (but not exclusively) in the metaphysis, which is depicted by region E in the illustration.
It is considered optimal to obtain written informed consent for an elective surgical procedure in which of the following clinical settings?
By the hospital risk manager upon admission
By the nurse in pre-op holding
By the surgeon in pre-op holding
By the surgeon's scheduler greater than 7 days prior
By the surgeon in the office within 7 days prior
The reference by Bhattacharyya et al notes that the location where the informed consent was obtained is important. When informed consent was obtained by the operating surgeon in the office, there was a decreased risk of indemnity payment (p < 0.004). This finding is likely due to the effect of communication on malpractice claims. Poor communication has been established as the critical factor linked to malpractice claims. It seems logical that the physician-patient communication that occurs in the office is more interactive and substantive than discussions that occur on the hospital floor or in the preoperative holding area. A closed claims analysis conducted in Florida, which included 127 mothers of infants who had experienced permanent perinatal injuries and who subsequently sued their physicians, showed that nearly all complained that their physicians would not talk, answer questions,
or listen. Clearly, the office is the best setting for quality discussions on informed consent to occur.
A 45 year-old woman who has not reached menopause yet falls from a standing height and sustains a distal radius fracture. A DEXA scan reveals a T- score of -2.2. Which of the following treatments is indicated in this patient?
1,700 mg of calcium
1,200 mg of calcium
1,700 mg of vitamin D
1,200 mg of iron
1,700 mg of PTH
The current recommendations for further prevention of any fragility fracture include 1200- 1500mg of elemental calcium intake per day and 400-800 IU of vitamin D per day. Of note, these doses are indicated only for prevention and not sufficient for active treatment of osteoporosis (T score less than -2.5).
Medications that are approved by the FDA for active treatment of osteoporosis: alendronate, risedronate, raloxifene, estrogen, calcitonin. These medications and preventative measures help to reduce fragility fractures by as much as 50%.
Freedman et al. performed a retrospective study that looked at a cohort of patients with fragility fractures and then looked at the type and frequency of osteoporosis related interventions. They found that only 60% of patients actually were either prescribed a
medication, given a referral, or ordered additional workup (DEXA scan).
Schulman et al. reviewed a series of 80 female patients regarding osteoporosis and bone health, and found that the outpatient sports medicine office setting was an excellent opportunity to educate patients on these topics. The patients' post-education test scores increased significantly after a brief counseling session, and increases in daily calcium intake and exercise levels were also seen.
Hypophosphatasia is associated with which of the following laboratory findings?
Hyperbilirubinemia
Decreased urinary phosphoethanolamine
Decreased urinary inorganic pyrophosphate
Decreased serum phosphate
Decreased serum alkaline phosphatase
Alkaline phosphatase is a marker of bone formation and is elevated when bone formation is increased. Hypophosphatasia is an autosomal recessive disorder caused by an inborn error in the production of alkaline phosphatase (tissue- nonspecific isoenzyme of alkaline phosphatase: TNSALP), leading to low alkaline phosphatase levels. Increased urinary phosphoethanolamine is also diagnostic.
Which of the following statements regarding COX-2 is FALSE?
It causes mesenchymal stem cells to differentiate into osteoblasts
COX-2 knockout mice heal fractures more quickly than control mice
COX-2 is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2
Most NSAIDS non-specifically inhibit both COX-1 and COX-2 enzymes
The expression of COX-2 is upregulated in several human cancers
Cycloxygenase-2 (COX-2,aka prostaglandin-endoperoxide synthase 2) is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2. COX-2 is not expressed under normal conditions, but elevated levels are found during general states of inflammation. Zhang et al and Simon et al have both studied the role of COX-2 with regard to fracture healing. Zhang et al created
a COX-2 knockout mouse (one which does not express the COX-2 gene). This COX-2 knockout mouse has been shown to heal fractures more slowly than COX-1 knockout
mice or normal controls, thus identifying the role of COX-2 in general inflammation and bone repair. Zhang et al hypothesize that COX-2 causes mesenchymal progenitor cells to differentiate into osteoblasts, thus promoting new bone formation. Simon et al showed the delayed effects of fracture healing when animals were treated with COX-2 inhibitors.
Gerstenfeld et al. studied the reversibility of COX-2 inhibition on the short term bone healing in an animal model. They found that COX-2 inhibitors block fracture healing more than NSAIDS and the magnitude of this effect is related to the duration of treatment.
While specific inhibitors of COX-2 exist, traditional
NSAIDs non-specifically inhibit both COX-1 and COX-2 enzymes. In addition to its role in inflammation, COX-2 has been shown to be upregulated in many human cancers such as gallbladder carcinoma.
A 60-year-old man has had intermittent pain in his right great toe for the past 2 years. What is the most likely cause for the lesions shown in Figure A?
Monosodium urate crystal deposition
Calcium pyrophosphate deposition
Renal osteodystrophy
Tuberculosis
Sarcoidosis
Gout is a disorder of nucleic acid metabolism that leads to monosodium urate crystal deposition in the joints. The most common area of the body to be affected by gout is the first toe. The radiograph in Figure A demonstrates joint space narrowing of the 1st
metarsalphalangeal joint and the arrows show medial soft tissue swelling at the 1st MTP with soft tissue radio-densities and some erosive changes consistent with gout.
Weinfeld et al report their experience over a 7 year period with hallux MTP arthritis in 439 patients they treated. Surgical indications included pain, shoewear problems, and failure of non-operative management.
Reber et al describe a rare case of tophaceous gout in the medial sesamoid of the hallux and review the diagnosis, pathophysiology, and suggested management.
Eggebeen reports "gout is caused by monosodium urate crystal deposition in tissues leading to arthritis, soft tissue masses (i.e., tophi), nephrolithiasis, and urate nephropathy. The biologic precursor to gout is elevated serum uric acid levels (i.e., hyperuricemia). The diagnosis is confirmed if monosodium urate crystals are present in synovial fluid."
Incorrect Answers:
Which of the following pharmacologic agents is associated with the highest risk of bleeding and thrombocytopenia?
Coumadin
Enoxaparin
Unfractionated heparin
Dalteparin
Protamine sulfate
Of the options listed unfractionated heparin is associated with the highest rate of bleeding and thrombocytopenia. This may occur as part of a syndrome called Heparin Induced Thrombocytopenia (HIT).
Unfractionated heparin works in the coagulation cascade by binding and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. A known complication of unfractionated heparin use is Heparin Induced Thrombocytopenia (HIT). Heparin Induced Thrombocytopenia (HIT) is caused by the formation of abnormal antibodies that activate platelets leading to abnormal formation of blood clots inside a blood vessel, leading to
bleeding and thrombocytopenia.
Dorr et al. reviewed multimodal thromboprophylaxis for total hip and knee arthroplasty based on risk assessment in 1179 patients. They recommend careful use and monitoring of thromboprophylaxis after arthroplasty procedures to protect patients from thromboembolic events while also limiting adverse clinical outcomes secondary to thromboembolic, vascular, and bleeding complications.
Mont et al. performed a study on preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. They recommended all patients do early mobilization and receive pharmacologic prophylaxis and mechanical compressive devices for the prevention of thromboembolic disease. The group did not recommend any specific pharmacologic agents and/or mechanical devices.
Illustration A shows a figure of the coagulation cascade and the target molecule of both unfractionated heparin and low molecular weight heparin.
Incorrect Answers:
Which of the following series of lab values is most consistent with a diagnosis of high turnover renal osteodystrophy?
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Decreased calcium, decreased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Increased calcium, normal serum phosphate, increased alkaline
phosphatase, normal parathyroid hormone
Decreased calcium, increased serum phosphate, normal alkaline phosphatase, decreased parathyroid hormone
Increased calcium, normal serum phosphate, normal or high alkaline phosphatase, increased parathyroid hormone
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, and increased parathyroid hormone are all characteristic of renal osteodystrophy.
Renal osteodystrophy represents a spectrum of disease seen in patients with chronic renal disease. It is characterized by bone mineralization deficiency due to electrolyte and endocrine abnormalities. High turnover renal osteodystrophy is classically associated with significantly increased phosphate and parathyroid hormone (PTH) levels. Chronic renal disease leads to a decrease in renal phosphorus excretion, which leads to phosphate retention and a significant increase in PTH levels. This ultimately can lead to tertiary hyperparathyroidism.
Tejwani et al present a review article on renal osteodystrophy. They state that in high- turnover renal osteodystrophy PTH secretion is increased and, in the absence of medical intervention, leads to parathyroid gland hyperplasia. This hyperplasia is associated with loss of feedback inhibition in normal regulation of PTH secretion; consequently, even after correction of the renal disease, the parathyroid gland continues to secrete excessive levels of PTH.
Illustration A shows a pathologic fracture secondary to renal osteodystrophy. Incorrect Answers:
This series of lab values is consistent with a diagnosis of nutritional rickets due to vitamin D deficiency.
This series of lab values is consistent with a diagnosis of low-turnover renal osteodystrophy. This is classically caused by excess deposition of aluminum into bone which impairs PTH release from the parathyroid gland and disrupts the mineralization process.
This series of lab values is consistent with a diagnosis of hypoparathroidism. 5-This series of lab values is consisten with a diagnosis of primary hyperparathryoidism.
A 28-year-old African-American male with a history of Sickle Cell Disease complains of progressive left hip pain for the past two years. He denies any causative injuries. His images are shown in Figures A and B. Which of the following mechanisms is most likely responsible for his symptoms?
Blood disorder due to abnormal hemoglobin S alleles
Progressive slippage of physis though the hypertrophic zone
Osteomyelitis most likely due to Salmonella species
Accumulation of glycosaminoglycan breakdown products
COL5A1 or COL5A2 mutation
The clinical presentation and images are most consistent with left hip osteonecrosis as a result of coagulation and vascular occlusion caused by sickle cell anemia.
Sickle cell disease is a genetic disorder of hemoglobin synthesis characterized by 2 abnormal hemoglobin S alleles. Under low oxygen conditions the affected blood cells become "sickle shaped" and unable to pass through vessels. This results in vascular occlusion that may have a variety of clinical consequences depending on the body part affected.
Hernigou et al. review the natural history of symptomatic osteonecrosis in adults with sickle cell disease. Once symptomatic , osteonecrosis of the hip in sickle cell disease has a high likelihood of progressing and leading to femoral head collapse. Deterioration can be rapid and in most patients operative intervention is necessary to prevent further collapse or alleviate intractable pain.
Mont et al. performed a literature review on the natural history of untreated asymptomatic osteonecrosis of the femoral head. Their findings supported that asymptomatic osteonecrosis had a high prevalence of progression to symptomatic femoral head collapse. Small, medially located lesions had a low rate of progression, while medium to large sized osteonecrotic lesions did progress in a substantial number of patients. They recommended
consideration of joint-preserving surgical treatment in asymptomatic patients with a medium-sized or large, laterally located lesion.
Figure A shows an AP pelvis with left hip osteonecrosis. Figure B shows a T2 coronal MRI with left hip osteonecrosis. Illustration A shows an example of a hemoglobin molecule which has become "sickle shaped," and as a result is unable to pass through vessels efficiently.
Incorrect Answers:
slipped capital femoral epiphysis.
What mechanism allows Staphylococcus epidermidis to adhere to surfaces and resist phagocytosis?
Creation of active efflux pumps
Methylation of 23s rRNA
Biofilm production
Alteration of cell wall permeability
Beta-lactamase production
Staphylococcus epidermidis is a gram-positive bacteria that utilizes a glycocalyx/biofilm to adhere to orthopedic implants and other surfaces and resist phagocytosis.
The biofilm creates a well-protected environment where bacteria can proliferate and thrive essentially undetected by the host immune system. This leads to chronic infections of orthopedic implants that can go undetected for years.
Arciola et al note that S. epidermidis can colonize surfaces in a self-generated viscous biofilm composed of polysaccharides and that the ica genes found in
56% of S. epidermidis isolates were associated with their ability to produce biofilm.
Olson et al discuss the importance of polysaccharide intercellular adhesin (PIA), a
substance produced by 50-60% of S. epidermidis strains, in the adherence of S. epidermidis to biomaterials through biofilm creation. PIA plays a critical role in initial adherence of S. epidermidis to biomaterials, biofilm
maturation and aggregation.
Illustration A shows microscopy of Staphylococcus epidermidis, which is a gram- positive, coagulase-negative cocci. Illustration B is an overview of the different classes of organisms in microbiology.
Incorrect Answers:
Compared to cold-forged cobalt chrome, titanium alloys have which property?
Increased fatigue strength
Increased yield strength
Increased endurance limit
Decreased ductility
Decreased tensile strength
Titanium implants have decreased tensile (ultimate) strength when compared to cobalt chrome.
Ultimate strength, or tensile strength, is the maximum stress a material can withstand before undergoing breakage or failure. The ranking of ultimate strength, from highest to lowest is: 1) cobalt chrome, 2)titanium, 3)stainless steel, and 4) cortical bone.
Young's modulus of elasticity is defined as the measure of stiffness of a material in the elastic zone. A higher Young's modulus indicates a stiffer material. While titanium is highly biocompatible with a low modulus of elasticity (Young's modulus), it has poor wear characteristics making it non- suitable for femoral heads in total hip arthroplasty.
Long et al. present a review on titanium implants with a focus on bio- mechanical properties. Their study supports previous data which showed high rates of ultra-high molecular weight polyethylene wear due to accelerated breakdown when in contact with a titanium surface.
Incorrect Answers:
Peak bone mass attainment in both men and women is most dependent on which sex-steroid?
Testosterone
Progesterone
Growth Hormone
Estrogen
Cortisol
Estrogen has been shown to be important for both men and women in attaining peak bone mass.
Risk factors for osteoporosis are: increasing age, female sex, early menopause, fair-skinned, family history of hip fracture, low body weight, smoking, glucocorticoid use, excessive alcohol, low protein intake, and anticonvulsant or antidepressant use.
Which of the following contributes most to the ability of hyaline cartilage to attract water?
Aggrecan
Biglycan
Decorin
Fibromodulin
Osteocalcin
Aggrecan molecules bind to hyaluronic acid molecules via link proteins to form a macromolecule complex, known as a proteoglycan aggregate, which attracts water.
Proteoglycans are composed of subunits known as glycosaminoglycans. Glycosaminoglycans include two subtypes: chondroitin sulfate and keratin sulfate. These glycosaminoglycans link to a protein core by sugar bonds to form an aggrecan molecule. Link proteins then stabilize many of these aggrecan molecules to hyaluronic acid to form the proteoglycan aggregate. Cartilage also contains ancillary proteoglycans that are much smaller than the aggregating proteoglycans. These small proteoglycans include decorin, biglycan, and fibromodulin. They bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Ulrich-Vinther et al. authored a Level 5 review on cartilage structure. The negative charge present within the hyaline cartilage extracellular matrix attracts cations and results in an increase in tissue osmolality. This then attracts water, which decreases the osmolality. Thus, articular cartilage has a high tissue pressure, but the presence of type II collagen matrix prevents it from swelling.
Nap et al. present a basic science review article on aggrecans. They discus that the main function of aggrecan in cartilage is to resist compressive forces.
They note that the negative charge of the aggrecan molecule disaccharides create the high osmotic swelling pressure of cartilage.
Illustration A depicts the molecular organization of an aggregated proteoglycan molecule. Incorrect Answers:
What effect do bisphosphonate medications have on spinal fusion surgery when taken in the postoperative period?
Any effect can be counteracted by taking calcium supplements
No effect
Increased risk of wound infection
Smaller fusion mass
Decreased fusion rate
Bisphosphonates (e.g. alendronate) are used to treat osteoporosis. The mechanism of action is inhibiting the formation of the ruffled border of osteoclasts, resulting in decreasing bone turnover.
Huang et al performed a rat study comparing alendronate to placebo and found that fusion rates were lower in those treated with alendronate. However,
the fusion masses were larger in the alendronate treated rats despite lower fusion rates (why #4 is incorrect).
Lehman et al in another placebo controlled rate study found that the fusion rates for placebo (76%) were greater than the alendronate group (45%). Alendronate works on osteoclasts and does not affect calcium directly. Taking calcium should have no effect on alendronate (why #1 is incorrect). At this time there are no formal recommendations of when to stop bisphosphonate medication prior to spinal fusion surgery.
A therapeutic study presents a systematic review of 15 high- quality randomized controlled trials with homogeneous results. What level of evidence is this considered?
I
II
III
IV
V
A systematic review of high-quality clinical trials is considered a Level I study.
A systematic review is a powerful tool used to identify, evaluate and appraise all high- quality research related to a specific question. Systematic reviews, in contrast to most narrative review articles, adhere to strict scientific design by following eight steps; 1) defining a question and developing inclusion criteria,
Question 86
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause
Explanation
REFERENCES: Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology, and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 87
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 88
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of
Explanation
REFERENCES: Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 409-420.
Question 89
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?
Explanation
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Figure 29a Figure 29b
Question 90
What is the most common surgical cause of the foot deformity shown in Figure 9?
Explanation
REFERENCES: Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Myerson MS, Komenda GA: Results of hallux varus correction using an extensor brevis tenodesis. Foot Ankle Int 1996;17:21-27.
Question 91
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic
Explanation
Question 92
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?

Explanation
Question 93
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted? Review Topic

Explanation
Question 94
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient’s symptoms?
Explanation
REFERENCE: Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 95
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Explanation
REFERENCES: Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164.
Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
Alfredson H, Bjur D, Thorsen K, et al: High intratendinous lactate levels in painful chronic Achilles tendinosis: An investigation using microdialysis technique. J Orthop Res
2002;20:934-938.
Question 96
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
Explanation
REFERENCES: Swanson TV, Bray TJ, Holmes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Lawrence S, Botte M: The sural nerve of the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 97
A 74-year-old man underwent a hemiarthroplasty with acromioplasty for rotator cuff tear arthropathy 2 years ago. Despite continued therapy, he is still unable to elevate his arm beyond 40 degrees. Attempted elevation is painful and demonstrates bulging in the anterosuperior aspect of his shoulder. Radiographs show a well-positioned hemiarthroplasty without signs of loosening. What is the most appropriate treatment for this patient? Review Topic
Explanation
Question 98
below show the clinical photograph and radiograph obtained from a year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 99
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm 3 . The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.
Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 100
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
