Orthopedic Board Review MCQs: Arthroplasty, Foot & Ankle, Trauma | Part 128

Key Takeaway
This page offers Part 128 of a comprehensive orthopedic board review. It provides 100 high-yield MCQs for orthopedic residents and surgeons preparing for OITE, AAOS, and ABOS exams. Authored by Dr. Hutaif, it includes study and exam modes with detailed explanations.
About This Board Review Set
This is Part 128 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 128
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Foot, Fracture, Hip, Knee, Shoulder.
Sample Questions from This Set
Sample Question 1: What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?...
Sample Question 2: A 45-year-old right hand dominant female sustains a left shoulder injury after falling on ice 2 weeks ago. She is brought to the operating room for surgical intervention and positioned upright in a beach chair. Figures A and B are images ta...
Sample Question 3: A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?...
Sample Question 4: A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent? Review Topic...
Sample Question 5: Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?

Explanation
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are biomechanically the most important aspect of the construct whether a plate is used or not.
Question 2
A 45-year-old right hand dominant female sustains a left shoulder injury after falling on ice 2 weeks ago. She is brought to the operating room for surgical intervention and positioned upright in a beach chair. Figures A and B are images taken from a posterior viewing portal with a 70 degree arthrosope. Figure C demonstrates the surgically repaired structure. Which of the following physical examination maneuvers would have been most likely abnormal in this patient PREOPERATIVELY? Review Topic

Explanation
Figure A as viewed from a posterior portal in the beach chair position of the left shoulder demonstrates a subscapularis tear with Figure B demonstrating medial instability of the long head of the biceps tendon. Figure C shows a repaired subscapularis to its footprint with double loaded screw-in anchors. A biceps tenodesis was concomitantly performed.
The key physical exam findings are positive Belly-press and Lift-off maneuvers, as well as weakness in internal rotation and increased passive external rotation. An MRI would confirm the diagnosis with discontinuity of the subscapularis and long-head of the biceps not located in the bicipital groove.
Faruqui et al present a Level 4 retrospective analysis of 52 patients. They found that the use of the belly press, lift-off, and bear hug tests had a collective sensitivity of 81%.
Yoon et al author a Level 2 prospective evaluation of 312 patients that underwent arthroscopic rotator cuff tear surgery. They investigated the sensitivity and specificity of the lift-off, internal rotation lag sign, belly-press, and bear-hug tests to evaluate subscapularis integrity. They found that a positive lift-off test was specific for the finding a full-thickness subscapularis tear. The lift-off, internal rotation lag sign, belly-press, and bear-hug tests show internal rotation strength deficit.
Figure A depicts an abnormal belly-press examination whereby the wrist flexes, and the elbow will fall posteriorly as the patient recruits the posterior deltoid to compensate for lack of the subscapularis. Illustration B demonstrates a normal belly-press examination. Illustration C shows a normal lift off test.
Incorrect Answers:
1: Jerk Test is positive if there is a 'clunk' or pain with the maneuver and is associated with posterior labral pathology. 2: Wright's test is where the shoulder is passively externally rotated and abducted while the patient turns their neck away from the tested extremity. It is a test for thoracic outlet syndrome. 4: Jobe's test is positive with supraspinatus weakness and or impingement. 5: Hornblower's test is positive if the arm falls into internal rotation. It may represent teres minor pathology.
Question 3
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
Marmor L, Bechtal CO: Paralysis of the serratus anterior due to electric shock relieved by transplantation of the pectoralis major muscle: A case report. J Bone Joint Surg Am 1983;45:156-160.
Question 4
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent? Review Topic
Explanation
Question 5
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55-year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 6
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 7
What is the next most appropriate step in the orthopaedic management of this patient?

Explanation
OrthoCash 2020
Which of the following findings best describes the acetabular fracture shown in Figure 38?
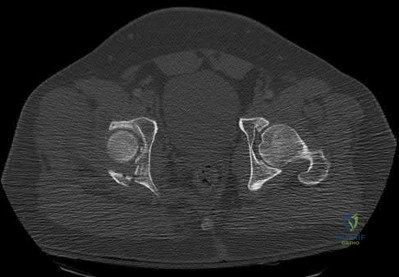
Posterior column with articular impaction and a free fragment
Anterior column with articular impaction
Posterior wall with an intra-articular fragment
Posterior wall with articular impaction and a free intra-articular fragment
Posterior wall with articular impaction Corrent answer: 4
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.
OrthoCash 2020
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
normal sexual function and normal vaginal childbirth.
sexual dysfunction (dyspareunia) and normal vaginal childbirth.
normal sexual function and caesarean section childbirth.
sexual dysfunction (dyspareunia) and caesarean section childbirth.
normal sexual function and caesarean section childbirth until hardware removal.
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is
almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.
OrthoCash 2020
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Closed treatment and casting
Open reduction and internal fixation
Primary subtalar arthrodesis
Percutaneous fixation
External fixation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.
OrthoCash 2020
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
Radial head resection and lateral collateral ligament repair
Radial head arthroplasty alone
Radial head arthroplasty and lateral collateral ligament repair
Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.
OrthoCash 2020
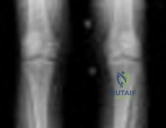
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C).
What is the most appropriate management for the femoral shaft fracture at this point?
Reamed intramedullary nailing
Traction
External fixation
Open plating
Mast suit
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.
OrthoCash 2020
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?

MRI scan
Physical examination
Workers’ compensation status
Surgeon availability
Patient age
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
OrthoCash 2020
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Consult the ethics committee before giving blood.
Use cell saver blood.
Ask the patient’s family for consent to give blood.
Use plasma expanders.
Give the patient blood.
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open wound is not recommended nor would there likely be enough from an open pelvic fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.
OrthoCash 2020
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

talectomy.
reimplantation of the talus.
reimplantation of the talus with acute triple arthrodesis.
Syme amputation.
transtibial amputation.
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.
OrthoCash 2020
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Spiral
Oblique
Transverse
Segmental
Comminuted
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.
OrthoCash 2020
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?

Kocher-Langenbeck
Iliofemoral
Ilioinguinal
Extended iliofemoral
Triradiate approach
The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate
approaches although useful for this fracture, have a higher rate of complications.
OrthoCash 2020
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

plating of the radial shaft fracture then open repair of the triangular fibrocartilage complex.
open reduction and internal fixation of the radius and ulna.
plating of the radius then closed reduction and evaluation of the distal radioulnar joint (DRUJ).
closed reduction of the radius and DRUJ.
plating of the radius then pinning of the DRUJ in pronation.
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
OrthoCash 2020
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Chronic osteomyelitis
Planovalgus hindfoot
Plantar nerve entrapment
Wound dehiscence
Painful hardware
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.
OrthoCash 2020
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
A primed immune system with an increased risk of a systemic inflammatory response
Nothing since they are no longer in uncompensated shock and their vital signs have normalized
Higher nonunion rates after fracture fixation
Higher infection rates after definitive fracture fixation
Higher complication rates after temporizing external fixation of long bone fractures
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.
OrthoCash 2020
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is
intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?

Emergent four compartment fasciotomies
Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
Elevation of the limb overnight and four compartment fasciotomies in the morning
Elevation of the limb overnight and a recheck of compartment pressures in the morning
Emergent MRI of the knee and leg Corrent answer: 2
The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
OrthoCash 2020
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
The mean arterial blood pressure is above 90 mm Hg.
The pulse pressure has normalized.
Urine output is greater than 0.5 to 1 mL/kg/h.
Oxygen delivery has been maximized.
Aerobic metabolism has been restored in all tissue beds.
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.
OrthoCash 2020
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Infection
Malunion
Loss of forearm rotation
Refracture
Delayed union/nonunion
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.
OrthoCash 2020
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
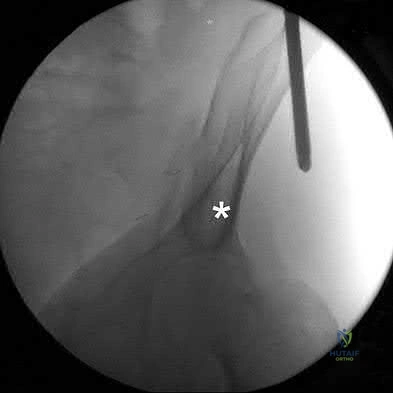
Anterior superior iliac spine
Sciatic buttress
A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
The most superior portion of the roof of the acetabulum
Iliopectineal line
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.
OrthoCash 2020
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure
Question 8
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown Figure 18. What is the most likely diagnosis?
Explanation
REFERENCES: Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Brown MF, Dandy DJ: Intra-articular ganglia of the knee. Arthroscopy 1990;6:322-323.
Question 9
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 10
Varus intertrochanteric osteotomy for coxa valga commonly produces which of the following results?
Explanation
REFERENCE: Millis MB, Murphy SB, Poss R : Osteotomies about the hip for the prevention and treatment of osteoarthrosis. Instr Course Lect 1996;45:209-226.
Question 11
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 12
Which of the following statements is true regarding articular cartilage?
Explanation
Proteoglycans, the most common of which is aggrecan, are produced by chondrocytes and give articular cartilage its hydrophilic properties. Multiple glycosaminoglycans (GAGs), such as chondroitin and keratin can attach to core proteins to form aggrecans. Link proteins then help aggrecans interact with hyaluronic acid. The negative charge of this complex helps create a strong osmotic gradient, which attracts water and increases tissue pressures. Normal aging involves a decrease in the water content of the extracellular matrix while osteoarthritis is associated with increased water content, which leads to loss of strength and elasticity.
Chen et al. evaluated the strain and depth related properties of articular cartilage in bovine models. They found that the zero-strain permeability, zero-strain equilibrium confined compression modulus, and deformation dependence constant differed among the layers of cartilage. They suggest that the complex strain-dependent properties of articular cartilage of different thickness and location have clinical implications for tissue engineering.
Illustration A is a diagram depicting the extracellular matrix of articular cartilage. Incorrect Answers:
Question 13
Figures 15a and 15b are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared to traditional arthroscopic techniques when evaluating which outcome?
Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the 2 techniques.

CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 17
Figure 16 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop," and then he needed help walking off the field. His knee is visibly swollen.
Question 14
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 15
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?
Explanation
REFERENCE: Mazzoca AD: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 308-309.
Question 16
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 17
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 18
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
REFERENCES: Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 19
A 32-year-old man is brought to the emergency department after being involved in an MVC. He is found to have a closed left femoral shaft fracture (Figures A and B) and a Glasgow Coma Scale (GCS) score of 13. A CT scan of the head is performed and demonstrates no significant bleeding. He has no other injuries and is hemodynamically stable. Which of the following statements is true?
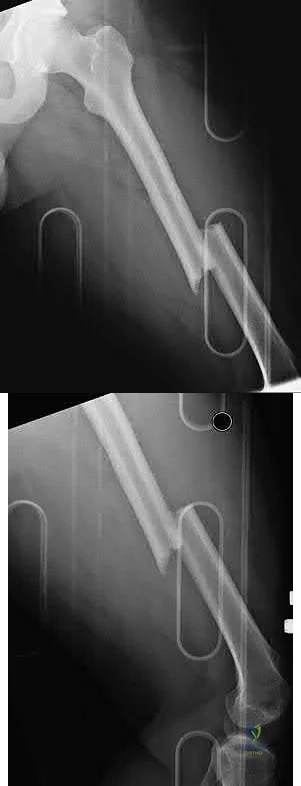
Explanation
Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggests that intramedullary nails done acutely
leads to decreased pulmonary complications, decreased thromboembolic events, improved rehabilitation, decreased length of stay and cost of hospitalization, and improved GCS scores on discharge. However, it is important to note that intraoperative hypotension should be avoided in these patients, as it has been associated with worsening outcomes following acute intramedullary nailing of the femur.
Starr et al. performed a retrospective study to determine if the timing of treatment of femur fractures in patients with an associated head injury had an effect on the risk of pulmonary and CNS complications. They found that delaying fracture stabilization (> 24 hours) made pulmonary complications 45 times more likely, while early fracture stabilization had no effect on the risk of CNS complications.
McKee et al. performed a retrospective case-control study to determine the effect of early intramedullary nailing of femoral shaft fractures on the neurologic outcome of patients with multiple injuries and a concomitant head injury. They found no significant differences between the two groups in terms of early mortality, length of hospital/ICU stay, level of neurologic disability, or results of cognitive testing. Their results support the continued early intramedullary nailing of femoral fractures for patients with a concomitant head injury.
Richards et al. performed a retrospective study evaluating lactate levels before reamed intramedullary nailing (IMN) of femur fractures treated with early fixation (< 24 hours) and its effects on pulmonary complications (defined as mechanical ventilation lasting ≥ 5 days). They found that a median admission lactate of 3.7 mmol/L was associated with duration of mechanical ventilation ≥ 5 days, whereas a median preoperative lactate of 2.8 mmol/L was not.
Figures A and B are radiographs demonstrating a transverse femoral shaft fracture.
Incorrect Answers:
OrthoCash 2020
Question 20
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 21
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 22
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 23
Figure below shows the radiograph obtained from a 76-year-old woman who has sharp pain in her groin, thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best to proceed. What is the best next step?
Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
Question 24
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness? Review Topic
Explanation
Question 25
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Loebenberg MI, Cuomo F: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface defects. Orthop Clin North Am 2000;31:23-24.
Question 26
Which of the following pieces of equipment currently offers the greatest opportunity for lowering the number of equestrian injuries? Review Topic
Explanation
> or = 12). Injuries included the chest (54%), head (48%), abdomen (22%), and extremities (17%). Only 9% of riders wore helmets, and 64% believed the accident was preventable. The authors noted that "helmet and vest use will be targeted in future injury prevention strategies." In another study, Frankel and associates noted that helmet use was only documented in 34% of riders. Although orthopaedic injuries are common, knee pads, wrist guards, boots, and quick release stirrups would most likely have less impact on injury prevention.
Question 27
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 28
A 70-year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in Figures 1 through 4. What is the most appropriate treatment for the fracture below the implant?

Explanation
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 29
A resident arrives to the operating room late for a LEFT carpal tunnel release procedure. The patient is prepped and draped under general anaesthesia, and the attending surgeon and assistant are about to make an incision to the RIGHT carpal tunnel. The resident mentions to the attending surgeon that surgery was booked for the opposite limb, but he ignores the residents confers by saying the surgical mark is under the drape. What would be the most appropriate course of action for the resident at this time? Review Topic
Explanation
Wrong-site surgery is completely preventable by having the surgeon, in consultation with the patient when possible, place his or her initials on the operative site using a permanent marking pen and then operating through or adjacent to his or her initials. The intended site should be marked such that the mark will be visible after the patient has been prepped and draped. A "time-out" procedure should be done before the initiating of any surgical procedure to confirm the type of procedure, site, and side with all operating room personnel including residents.
Haynes et al. reviewed the effect of surgical safety checklists before surgery on the morbidity and mortality in a global population. They found the rate of death was 1.5% before the checklist was introduced and declined to 0.8% afterward (P=0.003). Inpatient complications occurred in 11.0% of patients at baseline and in 7.0% after introduction of the checklist (P<0.001).
Incorrect Answers:
Question 30
Long-term alendronate (Fosamax) use for osteoporosis has been associated with which of the following?
Explanation
fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with uterine cancer or a detached retina.
Question 31
-A 32-year-old man who is a smoker sustained an open tibial fracture and underwent a staged treatment with placement of an intramedullary nail. Four weeks after surgery, he developed a pseudomonas deepwound infection. What is the strongest predictor of persistent infection if implants are retained until fracture union?
Explanation

Question 32
A 41-year-old male underwent intramedullary nailing for a low-energy left femoral shaft fracture. At his follow-up appointment, he complains that his feet are pointing in opposite directions when walking. Using the imaging study shown in Figure A, which of the following represents this patient's left femur malalignment?
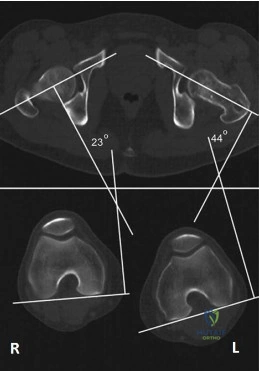
Explanation
Radiographic rotational malalignment after fixation of femoral shaft fractures may be measured by comparing the femoral anteversion of both femurs. This can be determined by measuring the angle between a line tangential to the dorsal bony contours of the femoral condyles and a line drawn through the axis of the femoral neck. Rotational differences of less than 10° are considered variations of normal.
Jaarsma et al. reviewed rotational malalignment after intramedullary nailing of femoral fractures. They report that rotational measurements by CT are superior to clinical assessment. They note a high incidence of malrotation after IM nailing of fractures. This has shown to be in the range 15% to 30%.
Figure A shows left femoral malrotation using CT-torsion measurements with axial cuts of the femoral neck and distal femoral condyles. Note the normal anteversion of the right femur (23 degrees; normal range 10-25).
Incorrect Answers:
Question 33
Which of the following findings is an indication for adjunctive use of high-dose steroids?
Explanation
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 319-328.
Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 34
A 24-year-old professional male soccer player has lower abdominal pain on exertion. He has pain with resisted hip adduction and with sit-ups. There is no palpable inguinal hernia with a Valsalva maneuver. Nonsurgical management has failed to provide relief. After ruling out malignancies, what is the next most appropriate step in management? Review Topic
Explanation
Question 35
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of
Explanation
REFERENCES: Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Sangeorzan BJ, Veith RG, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joint by arthrodesis. Foot Ankle 1990;10:193-200.
Question 36
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?
Explanation
REFERENCES: Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Hamilton WG: Sprained ankles in ballet dancers. Foot Ankle 1982;3:99-102.
Question 37
An article in a leading orthopaedic journal describes a randomized controlled study comparing 2 popular and comparable surgical methods for fixation of hip fractures. Patients were randomized by a predetermined computer-generated list. There was approximately 20% crossover between treatment groups. Evaluation of study outcomes (clinical and radiographs) was performed by one of the surgeons participating in the study. Enrollment goals for appropriate power were achieved and final 1-year follow-up was obtained for 65% of patients. According to Oxford Group criteria, what is the appropriate level of evidence for this study? Review Topic
Explanation
Question 38
A 66-year-old woman with known poorly controlled rheumatoid arthritis reports that for the past 4 weeks she has been unable to extend the metacarpophalangeal (MCP) joints of her right hand index, middle, ring and little fingers. She cannot hyperextend the thumb interphalangeal joint. Active wrist extension is possible, but shows radial deviation. Examination reveals mild synovitis at the wrist and MCP joints of the affected hand. There is no ulnar deviation at the MCP joints with normal alignment. When the MCP joints are passively extended, the patient is unable to maintain them in this position. There is no piano key sign at the distal ulna. Passive wrist motion shows a normal tenodesis effect. Which of the following would most likely confirm your diagnosis? Review Topic
Explanation
Question 39
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of
Explanation
REFERENCE: Pauli RM, Breed A, Horton VK, Glinski LP, Reiser CA: Prevention of fixed angular kyphosis in achondroplasia. J Pediatr Orthop 1997;17:726-733.
Question 40
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
Explanation
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Question 41
A year-old man with a body mass index of 31 had a month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
Question 42
A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
Explanation
REFERENCES: Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:216-222.
Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J: The deleterious effects of intraoperative hypotension on outcome in patients with severe head injury. J Trauma 1992;33:403-407.
Schmeling GJ, Schwab JP: Polytrauma care: The effect of head injuries and timing of skeletal fixation. Clin Orthop 1995;318:106-116.
Townsend RN, Lheureau T, Protech J, Reimer B, Simon D: Timing fracture repair in patients with severe brain injury (Glascow Coma Scale score <9). J Trauma 1998;44:977-983.
Question 43
A defect in the gene coding for fibrillin-1 would lead to which diagnosis? Review Topic
Explanation
Marfan Syndrome is a genetic disorder of connective tissue typically caused by a mutation in the gene coding for the fibrillin-1 protein. Affected patients are typically very tall with long limbs and thin fingers and toes. Marfan Syndrome patients have many common features including ectopic lens, aortic root dilation, scoliosis, protrusio acetabuli, and ligamentous laxity.
Shirley et al. present a review of Marfan Syndrome with emphasis on the musculoskeletal manifestations including ligamentous laxity, protrusio acetabuli, and scoliosis. They note that scoliosis in these patients, when compared to those with idiopathic scoliosis, commonly progresses faster, is more resistant to bracing, and has a higher association with dural ectasia.
Dean presents a review of Marfan Syndrome and its underlying genetic cause of a mutation in fibrillin. They state that diagnosis can be made using the Ghent nosology (see Illustration A) which can diagnose or rule out the condition in 86% of patients. They caution using these criteria in young children as some features of Marfan Syndrome may not present until later ages.
Illustration A is a summary of the 2010 Revised Ghent nosology for diagnosing Marfan Syndrome.
Incorrect Answers:
Question 44
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure 2. Which interposed structure is preventing reduction?

Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
Question 45
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 46
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4°F (37.4°C), and examination reveals that abduction of the left hip is limited to 30°. Laboratory studies show a WBC of 11,000/mm 3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
REFERENCE: Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 505-513.
Question 47
What do the T2-weighted, fat-saturated MRI scans shown in Figures 76a through 76d reveal? Review Topic
Explanation
Question 48
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 49
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 50
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of Review Topic
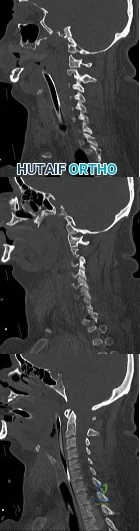
Explanation
Question 51
- The radiograph shown in Figure 50a and the CT scan shown in Figure 50b reveal a lesion in the left femoral neck of a 12-year-old boy who has pain in the left hip. The most likely cause of the osteopenia of the left proximal femur is
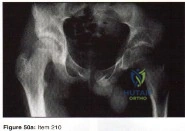
Explanation
Question 52
Figures 233a through 233c are the radiographs and biopsy specimen of a 32-year-old woman who has had progressive ankle pain for 6 months. What is the most appropriate treatment option?

Explanation

Question 53
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 54
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 55
A 39-year-old man presents with back pain radiating to the left lower extremity for the past 6 weeks. Magnetic resonance images of the pathology are
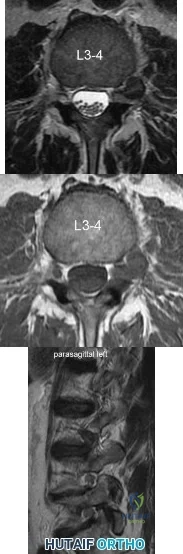
Explanation
Far lateral disc herniations constitute approximately 5-10 percent of disc hernations in the lumbar spine. Given the more vertical anatomy of lumbar nerve roots, at a given disc level, a central or paracentral herniation will affect the traversing nerve root (e.g. nerve root of level below) and a far lateral herniation will affect the exiting nerve root (e.g. nerve root of the level above). Similar to the more common central and paracentral herniations, approximately 90% of patients will improve without surgical intervention. When surgical intervention is needed, the paraspinal approach of Wiltse is utilized.
Marquadt et al. reported long term outcomes of surgical management of far lateral disc herniations. At an average of 146 months follow up, 56.3% of patients had complete relief of symptoms and 27.6% had permanent residual symptoms. Over 75% of patients subjectively rated their outcomes as excellent.
Figure A and B are T2 and T1 axial MRI images, respectively, showing the L3-L4 disc space with a left far lateral disc herniation. Figure C is a left parasagittal T2 MRI image showing impingement on the L3 nerve root. Structures are labeled in illustration A. Illustration B shows the dermatomes of the lower extremity.
Incorrect Answers:
Question 56
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Hadjipavlou AG, Lander PH, Marchesi D, et al: Minimally invasive surgery for ablation of osteoid osteoma of the spine. Spine 2003;28:E472-E477.
Question 57
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
(p < 0.001) after surgery.
REFERENCES: Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Feagan BG, Wang CJ, Kirkley A, et al: Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: A randomized, controlled, trial. Ann Intern Med 2000;133:845-854.
Question 58
What is the preferred treatment of a patient with breast cancer and a pathologic fracture of the clavicle in her dominant arm?
Explanation
REFERENCES: Weber KC, Lewis VO, Randall RL, Lee AK, Springfield D: An approach to the management of the patient with metastatic bone disease. Instr Course Lect 2004;53:663-676.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons 2002, p 331.
Question 59
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by
Explanation
REFERENCES: Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 60
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan? Review Topic
Explanation
Question 61
Figure 91 is the radiograph of a 20-year-old man who kicked a door while intoxicated. At the emergency department, his leg is placed into a long-leg cast. After 2 hours, he reports increasing pain, numbness, and tingling in his toes. What is the most appropriate initial treatment?

Explanation
(SBQ12TR.88) When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture. Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
(SBQ12TR.78) A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure A. What would be the most appropriate treatment for this patient at this time? Review Topic

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Question 62
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 63
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
REFERENCES: Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Maron BJ, Thompson PD, Puffer JC, McGrew CA: Cardiovascular preparticipation screening of competitive athletes: A statement for health professionals from the Sudden Death Committee (Clinical Cardiology) and Congenital Cardiac Defects Committee (Cardiovascular Disease in the Young), American Heart Association. Circulation 1996;94:850-856.
Question 64
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?
Explanation
REFERENCES: Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.
Question 65
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic

Explanation
Question 66
Figures 39a through 39c show a clinical photograph and the radiographs of a 32-year-old woman who has been unable to actively extend her dominant ring and small finger for the past two weeks. She has no history of trauma and has minimal pain. Examination reveals full passive range of motion (ROM) of the fingers. Active ROM of the wrist is extension of 40 degrees and flexion of 35 degrees. Active forearm pronation is 45 degrees, and supination is 50 degrees. Treatment should consist of
Explanation
“like a buzzsaw” on the overlying tendons. This is called a Vaughan-Jackson lesion when extensor tendons are ruptured at the distal radial-ulnar joint. Of the dorsal/extensor compartments, typically the digiti minimi is involved first and further ruptures progress radially as the hand ulnarly deviates and the other tendons sublux and are brought within range of the “buzzsaw.” The cited articles state that after a dorsal exposure the hypertrophic tenosynovium is removed from each tendon sytematically, and the wrist joint then evaluated. Any bony spicules which may further damage tendons are removed, and the distal ulna is excised. Tendon transfers, grafts, or repairs are then performed. Surgical results tend to be better with single or double tendon ruptures than with multiple tendon ruptures.
Question 67
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 68
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
REFERENCES: Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
Question 69
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
REFERENCES: Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 70
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Explanation
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 71
A year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 72
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
Explanation
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 73
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
Explanation
REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 74
A 48-year-old man undergoes arthroscopy to repair a rotator cuff tear. During the arthroscopy, the tear is characterized and found to involve the entire supraspinatus and a majority of the infraspinatus tendons. After mobilization, the posterior rotator cuff can reach the greater tuberosity. However, the supraspinatus tendon cannot reach its insertion point at the greater tuberosity. What is the most appropriate treatment? Review Topic
Explanation
release, reverse acromioplasty, and tenotomy of the biceps tendon may improve shoulder pain. If these procedures fail, then a muscle transfer procedure can also be considered in select patients. If, however, a portion of the rotator cuff can be repaired, even partial repair can balance the coronal and axial forces about the shoulder to restore the kinematics of the joint. Reverse total shoulder arthroplasty is not appropriate for this relatively young patient.
Question 75
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
REFERENCES: Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach,
an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 76
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?
Explanation
REFERENCES: Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Cohen MS, Taleisnik J: Direct ligamentous repair of scapholunate dissociation with capsulodesis augmentation. Tech Hand Up Extrem Surg 1998;2:18-24.
Question 77
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-17, 4-18.
Question 78
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
REFERENCES: Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am
2003;85:109-115.
Caplan AI, Elyaderani M, Mochizuki Y, et al: Principles of cartilage repair and regeneration. Clin Orthop 1997;342:254-269.
Question 79
An otherwise healthy 25-year-old man with an isolated closed mid-diaphyseal femoral fracture undergoes intramedullary nailing. Compared with nonreamed nailing, reamed femoral nailing is associated with a higher rate of Review Topic
Explanation
Question 80
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 81
The term anorexia athletica refers to a problem whose criteria include all of the following, EXCEPT Review Topic
Explanation
Question 82
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 83
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 84
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 85
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 334.
Question 86
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 87
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of
Explanation
REFERENCES: Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791.
Question 88
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 89
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
REFERENCES: Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253.
Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL: The radiological investigation of lumbar spondylolysis. Clin Radiol 1998;53:723-728.
Question 90
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Explanation
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. View Abstract at PubMed Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. View Abstract at PubMed
Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. View Abstract at PubMed
Question 91
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
REFERENCES: Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 92
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 93
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 2010 Pediatric Orthopaedic Examination Answer Book • 55 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 94
An 85-year-old right hand dominant male sustains a fall onto his elbow while trying to get out of the car. His past medical history is significant for diabetes, congestive heart failure, and COPD. He lives in a nursing home, and is able to ambulate at baseline without and assistive devices. What would be the ideal definitive surgical treatment options in this patient? Review Topic

Explanation
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, and suffer less complications with TEA than ORIF in select cases.
Sorensen et al evaluated short- to medium term outcome of total elbow arthroplasty (TEA) in complex fractures of the distal humerus by evaluating 24 consecutive cases. Twenty of the patients were followed for almost 2 years, and their MEPS were 15 excellent, 4 good and 1 fair result. They concluded that TEA in complex fractures of the distal humerus in elderly patients can result in acceptable short- to medium term outcome.
Mckee et al conducted a prospective, randomized, controlled trial to compare
functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary total elbow arthroplasty (TEA). They randomized 42 patients and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF, based on the MEPS.
Illustration A shows radiographs of a TEA. Incorrect Answers:
Question 95
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
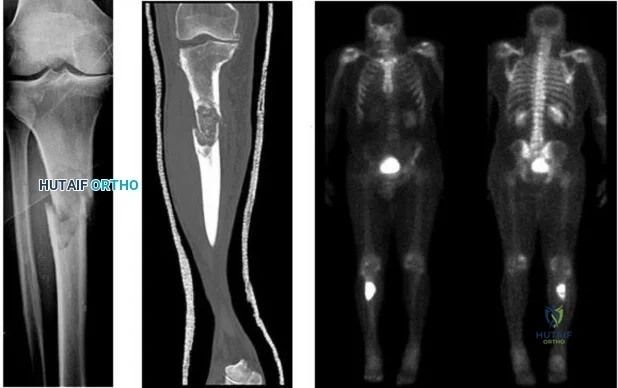
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 96
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
Explanation
REFERENCES: May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.
Question 97
03 The sagittal oblique MRI scan shown in Figure 70 reveals a lesion in the shoulder that typically affects what neurologic structure?
Explanation
The cysts form either because of a lesion of the capsulolabral complex at the superior/posterosuperior glenoid in the shoulder or because of myxoid degeneration of the capsule.
back to this question next question
Question 98
By which mechanism can a true aneurysm of the ulnar artery result?
Explanation
Question 99
A B C Figures 91a through 91c are CT images of a 76-year-old man who was involved in a motor vehicle collision. Which of the following scenarios would pose a contraindication to closed reduction of this injury prior to MR imaging?

Explanation
This patient has bilateral jumped facet joints at C6-7. Although MR imaging is useful for revealing disk herniations, cord injuries, and bony fragments, early closed reduction to restore anatomic alignment may be attempted prior to MR imaging because reduction will decrease pressure on the cord. There have been reports of catastrophic outcomes with closed reduction in patients who are intubated when disk fragments are pushed into the spinal cord. Consequently, closed reduction should be attempted only in awake and cooperative patients for whom neurologic status monitoring is possible. MR imaging is generally performed after reduction is attempted (successful or not).
RECOMMENDED READINGS
Initial closed reduction of cervical spine fracture-dislocation injuries. Neurosurgery. 2002 Mar;50(3 Suppl):S44-50. Review. PubMed PMID: 12431286. View Abstract at PubMed Radcliff K, Sonagli MA, Delasotta L, Singh N, Morrison E, Levine AM, Vaccaro AR. Cervical facet fractures and dislocations. In: Zigler JE, Eismont FJ, Garfin SR, Vaccaro AR, eds. Spine Trauma. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:441-464.
Vaccaro AR, Falatyn SP, Flanders AE, Balderston RA, Northrup BE, Cotler JM. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine (Phila Pa 1976). 1999 Jun 15;24(12):1210-7. PubMed PMID: 10382247. View Abstract at PubMed
Wimberley DW, Vaccaro AR, Goyal N, Harrop JS, Anderson DG, Albert TJ, Hilibrand AS. Acute quadriplegia following closed traction reduction of a cervical facet dislocation in the setting of ossification of the posterior longitudinal ligament: case report. Spine (Phila Pa 1976). 2005 Aug 1;30(15):E433-8. PubMed PMID: 16094262. View Abstract at PubMed
Question 100
A B C Figures 89a through 89c are the radiographs of a 35-year-old woman who has had 7 years of progressive ankle pain. She experiences stiffness and pain despite the use of an ankle-foot orthosis. Examination reveals pain along the anterior tibiotalar joint without tenderness to the subtalar or talonavicular joints. What is the most appropriate surgical intervention?

Explanation
This patient has isolated posttraumatic ankle arthritis with significantly decreased ankle range of motion that is best treated with an isolated ankle arthrodesis to eliminate pain. Because this patient is younger than 50 years of age and has limited presurgical range of motion, she is not a candidate for ankle arthroplasty. Additionally, TAA outcomes among patients who have a posttraumatic etiology are worse than for those with osteoarthritis. Tibiotalocalcaneal arthrodesis is suited for patients with associated subtalar
arthritis or rigid hindfoot deformity that necessitates correction. Anterior tibial exostectomy will not resolve the underlying arthritic pain and is not indicated.
RECOMMENDED READINGS
Easley ME, Adams SB Jr, Hembree WC, DeOrio JK. Results of total ankle arthroplasty. J Bone Joint Surg Am. 2011 Aug 3;93(15):1455-68. doi: 10.2106/JBJS.J.00126. Review. PubMed PMID: 21915552. View Abstract at PubMed
Spirt AA, Assal M, Hansen ST Jr. Complications and failure after total ankle arthroplasty. J Bone Joint Surg Am. 2004 Jun;86-A(6):1172-8. PubMed PMID: 15173289. View Abstract at PubMed
Ajis A, Henriquez H, Myerson M. Postoperative range of motion trends following total ankle arthroplasty. Foot Ankle Int. 2013 May;34(5):645-56. doi: 10.1177/1071100713481433. Epub 2013 Mar 11. PubMed PMID: 23478890. View Abstract at PubMed
Thomas R, Daniels TR, Parker K. Gait analysis and functional outcomes following ankle arthrodesis for isolated ankle arthritis. J Bone Joint Surg Am. 2006 Mar;88(3):526-35. PubMed PMID: 16510818. View Abstract at PubMed
Coester LM, Saltzman CL, Leupold J, Pontarelli W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am. 2001 Feb;83-A(2):219-28. PubMed PMID: 11216683. View Abstract at PubMed
