Full Question & Answer Text (for Search Engines)
Question 1:
An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
Options:
- Nerve conduction velocity studies and electromyography
- Exploration and grafting of the radial nerve
- Tendon transfers
- Observation for another 2 months
- Removal of the plate, neurolysis of the radial nerve, and intramedullary rodding of the humerus
Correct Answer: Observation for another 2 months
Explanation:
DISCUSSION: Most radial nerve palsies associated with closed fractures of the humerus resolve spontaneously, including Holstein-Lewis lesions (radial nerve palsy associated with oblique distal third fractures of the humerus). Initial sign of recovery at the brachioradialis may not occur for 4 months. There has been no evidence of deleterious effects occurring during this observation period. There are advocates of early exploration of the nerve. Exploration in the intermediate period between 1 and 4 months is not supported. As overall alignment of the fracture is acceptable, there is no need for hardware exchange until nonunion is clearly identified.
REFERENCES: Shao YC, Harwood P, Grotz MR, et al: Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-1652.
Green DP: Radial nerve palsy, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 112.
Question 2:
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
Options:
- The examiner brings a finger from medial to lateral across the antecubital fossa, feeling for a cord-like structure.
- The examiner brings a finger from lateral to medial across the antecubital fossa, feeling for a cord-like structure.
- With the elbow flexed to 90°and the forearm pronated, the examiner resists patient supination, evaluating for pain at the bicipital groove.
- With the patient’s arm elevated to 90° of forward flexion, the elbow extended, and the forearm supinated, the examiner resists elevation distal to the elbow, evaluating for pain at the bicipital groove.
Correct Answer: The examiner brings a finger from lateral to medial across the antecubital fossa, feeling for a cord-like structure.
Explanation:
Question 3:
What is the most common benign bone tumor in childhood?
Options:
- Unicameral bone cyst
- Fibrous dysplasia
- Nonossifying fibroma
- Aneurysmal bone cyst
- Chondromyxoid fibroma
Correct Answer: Nonossifying fibroma
Explanation:
DISCUSSION: The most common benign bone tumor in childhood is a nonossifying fibroma. It is estimated that 30% of children have a nonossifying fibroma. In most patients, the lesion is not identified until a radiograph is obtained for unrelated reasons. Similarly, most identified cases of fibrous cortical defect are not biopsied because the radiographic and clinical presentations are diagnostic.
REFERENCES: Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 4:
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Options:
- Semitendinosus tendon
- Gracilis tendon
- Sartorius tendon
- Semimembranosus tendon
- Medial collateral ligament
Correct Answer: Semitendinosus tendon
Explanation:
DISCUSSION: The semitendinosus and gracilis tendons lie beneath the superficial fascia and superficial to the medial collateral ligament. The semitendinosus is located more inferior to the gracilis tendon. The sartorius is more posterior and distal as is the medial collateral ligament. The semimembranosus is posterior.
REFERENCES: Pagnani MJ, Warner JJ, O’Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Warren LF, Marshall JL: The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 5:
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?
Options:
- worse functional results
- higher need for subsequent surgeries
- less blood loss
- higher union rates
- increased postoperative shoulder stiffness
Correct Answer: worse functional results
Explanation:
DISCUSSION: Lin et al found less blood loss with intramedullary nailing than plating, but nailing was also associated with increased shoulder surgery due to disruption of the rotator cuff tendon during insertion. Meekers et al found a higher union rate, better functional results and a lower reoperation rate after plate and screw fixation versus nailing. They concluded that plating was superior in most cases of humeral shaft fracture, except for pathological fractures, very obese patients, and open fractures.
Question 6:
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic
Options:
- MRI of the spinal axis
- Physical therapy
- A brace for scoliosis
- Observation, with reevaluation in 6 to 12 months
- Posterior spinal fusion from T6 to T12
Correct Answer: MRI of the spinal axis
Explanation:
The patient has an abnormal neurologic exam as shown by the abnormal abdominal reflexes. Furthermore, she has a significant curve and is younger than age 10 years. These findings are not consistent with idiopathic scoliosis. MRI will best rule out syringomyelia or an intraspinal tumor. Bracing and surgery are not indicated for this small curvature prior to obtaining an MRI scan.
Question 7:
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Options:
- Collagen type I
- Collagen type II
- Collagen type X
- Proteoglycan aggrecan
- Hyaluronic acid
Correct Answer: Collagen type X
Explanation:
DISCUSSION: Collagen type X is produced only by hypertrophic chondrocytes during enchondral ossification (growth plate, fracture callus, heterotopic ossification) and is associated with calcification of cartilage in the deep zone of articular cartilage. Collagen type I is the predominant collagen in bone, ligament, and tendon. Collagen type II is the predominant collagen in articular cartilage. Proteoglycan aggrecan and hyaluronic acid are components of the extracellular matrix and are involved in the compressive strength characteristics of articular cartilage.
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Poole AR, Kojima J, Yasuda T, Mwale F, Kobayasai M, Laverty S: Composition and structure of articular cartilage: A template for tissue repair. Clin Orthop 2001;391:S26-S33.
FOR ALL MCQS CLICK THE LINK ORTHO
MCQ BANK
Question 8:
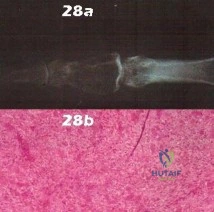
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Options:
- reduction of the serum alkaline phosphatase level by 50%.
- preoperative radiation therapy of 600 cGy to the surgical site.
- aspiration of the knee joint with cell count.
- insertion of a vena caval filter.
- administration of 25 mg of indomethacin three times a day.
Correct Answer: reduction of the serum alkaline phosphatase level by 50%.
Explanation:
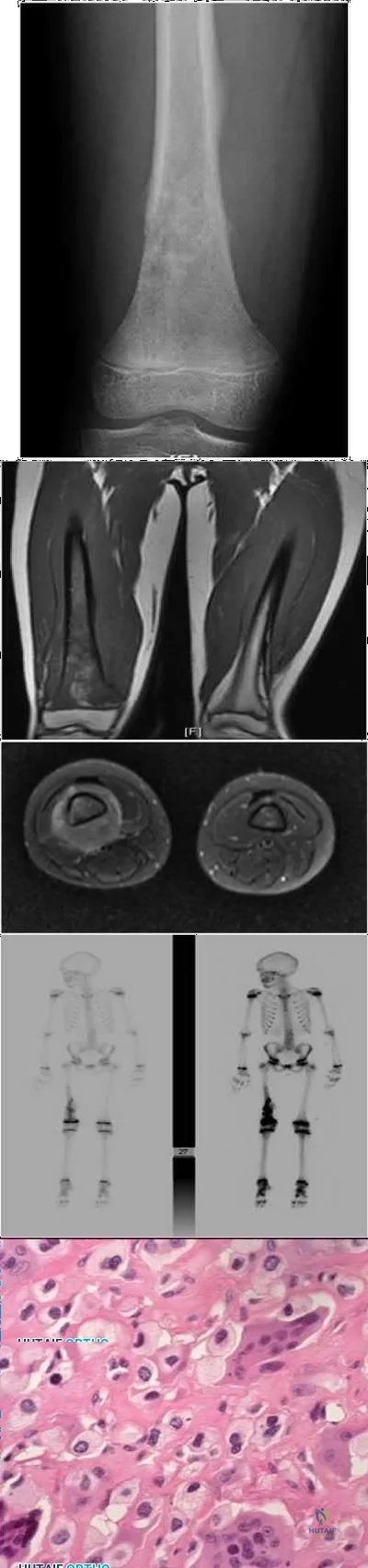
DISCUSSION: The radiographs show established Paget’s disease. Bony expansion is evident, with thickened trabeculae consistent with the disordered bone remodeling process. A reduction of the serum alkaline phosphatase level to 50% of the pretreatment level may reduce pain from Paget’s disease, and it is recommended prior to consideration of joint replacement. In elective cases, treatment of Paget’s disease should begin at least 6 weeks prior to surgery. The other modalities are not related to the treatment of Paget’s disease.
REFERENCES: Kaplan FS, Singer FS: Paget’s disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Siris ES: Paget’s disease of bone, in Favus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. New York, NY, Raven Press, 1993, pp 375-384.
Question 9:
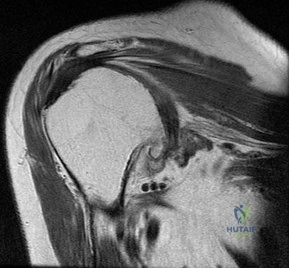
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Options:
- Suprascapular nerve entrapment
- Supraspinatus and infraspinatus tendon tear
- Muscular dystrophy
- Thoracic outlet syndrome
- Spinal accessory nerve disruption
Correct Answer: Suprascapular nerve entrapment
Explanation:
DISCUSSION: The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy.
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 10:
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder “slip out” when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management? Review Topic
Options:
- Echocardiography
- Abdominal ultrasound
- Skeletal survey
- Glenoid osteotomy
- Physical therapy
Correct Answer: Physical therapy
Explanation:
The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert’s. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral.
Question 11:
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Options:
- Extensor digiti minimi
- Extensor carpi radialis brevis
- Extensor pollicis longus
- Extensor indicis proprius
- Abductor pollicis longus
Correct Answer: Extensor indicis proprius
Explanation:
DISCUSSION: The terminal branch of the posterior interosseous nerve is contained in the fourth dorsal compartment. The contents of the various dorsal wrist compartments are as follows:
1
st
Compartment: Abductor pollicis longus, extensor pollis brevis
2
nd
Compartment: Extensor carpi radialis brevis, extensor carpi radialis longus
3
rd
Compartment: Extensor pollicis longus
4
th
Compartment: Extensor digitorum comminus, extensor indicus proprius, posterior interosseous nerve
5
th
Compartment: Extensor digiti minimi
6
th
Compartment: Extensor carpi ulnaris
The extensor indicis proprius is also contained in the fourth dorsal compartment. The extensor digiti minimi is located in the fifth dorsal compartment. The extensor carpi radialis brevis is located in the second dorsal compartment. The extensor pollicis longus is located in the third dorsal compartment, and the abductor pollicis longus is located in the first dorsal compartment.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 150-151.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 60.
Question 12:
An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
Options:
- Electrical stimulation with an implanted coil
- Ultrasound stimulation for 30 minutes per day
- Locked intramedullary nailing with bone graft
- Ilizarov external fixation with intermittent distraction and compression
- Plate and screw fixation with bone graft
Correct Answer: Plate and screw fixation with bone graft
Explanation:
DISCUSSION: The patient has a well-established nonunion in a very porotic bone. Electrical stimulation has been found effective in treating tibial nonunions, but there is very little data on humeral nonunions, especially chronic well-established ones. Ultrasound stimulation is effective in accelerating fracture healing, but there is little data concerning the treatment of nonunions. Intramedullary nailing with bone graft is an option, but it maybe difficult to obtain a rigid construct in a very porotic bone. An Ilizarov-type external fixator would be an alternative, but there is little clinical data for the humerus and it may be poorly tolerated. A plate and screw construct with bone graft combines rigidity with the biologic advantage of the bone graft. A recent series reported on the use of a plate combined with onlay allograft for recalitrant nonunions. Cement augmentation for screw fixation either in the canal or added to the screw holes may be helpful in select cases.
REFERENCES: Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
Jupiter JB: The treatment of complex non-unions of the humeral shaft with a combination of surgical techniques. J Bone Joint Surg Am 1990;72:701-707.
Question 13:
A patient who was involved in a motor vehicle accident 2 days ago now reports neck pain. He denies any other symptoms. Radiographs reveal a type II odontoid fracture that is 2 mm anteriorly displaced. Management consists of halo vest immobilization in extension, and repeat radiographs reveal that the fracture is completely reduced. The patient is discharged to home, but later that evening he notes difficulty swallowing while trying to eat dinner. What is the most likely cause of this difficulty?
Options:
- Injury to the recurrent laryngeal nerve
- Injury to the superior laryngeal nerve
- Esophageal trauma at the time of the fracture or at the time of the reduction
- Retropharyngeal edema or hematoma from the fracture
- Halo vest placement
Correct Answer: Halo vest placement
Explanation:
DISCUSSION: If the neck is immobilized in excessive extension, it can be difficult for the patient to swallow. If the patient had injured the recurrent or superior laryngeal nerve at the time of the accident, it is likely to have manifested itself earlier on. Esophageal trauma or retropharyngeal edema or hematoma from the fracture also should have manifested itself earlier. Because the fracture was completely reduced, it is unlikely that moving the small fragment posteriorly would have injured the esophagus.
REFERENCES: Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Glaser JA, Whitehill R, Stamp WG, Jane JA: Complications associated with the halo-vest: A review of 245 cases. J Neurosurg 1986;65:762-769.
Question 14:
A 58-year-old man has a painful right hip 3 years after undergoing a large head metal-on-metal total hip arthroplasty (THA) in which the components are well positioned. MR imaging confirms a cystic mass around the hip and metal ion levels show a marked increase in cobalt compared to chromium levels. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are within defined limits. What is the most likely cause for his discomfort?
Options:
- Chronic periprosthetic infection
- Trochanteric bursitis
- Pseudotumor related to corrosion at the head/neck taper junction
- Tendonitis from iliopsoas tendon impingement
Correct Answer: Pseudotumor related to corrosion at the head/neck taper junction
Explanation:
DISCUSSION
This patient presents with a pseudotumor likely attributable to local tissue reaction resulting from either articular metal wear debris and/or corrosion and fretting of the trunnion. The trunnion is a more likely source of the problem for a number of reasons: good position of metal articulation, increased trunnion corrosion and fretting associated with large-head THA, and markedly increased cobalt levels compared to chromium levels. Infection is very unlikely
in the setting of normal ESR and CRP findings. MR imaging findings are consistent with pseudotumor and not iliopsoas tendonitis or trochanteric bursitis.
CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 45
Figures 42a through 42e are the radiographs, MR image, and MR arthrogram of a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has either competed or practiced 5 to 6 times per week since the age of
Question 15:
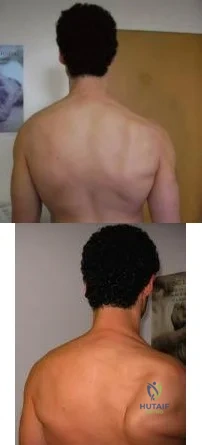
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B. What nerve is most likely injured? Review Topic
Options:
- Long thoracic
- Suprascapular
- Spinal accessory
- Axillary
- Thoracodorsal
Correct Answer: Spinal accessory
Explanation:
The patient is presenting with LATERAL scapular winging which is a result of injury to the spinal accessory nerve and resultant trapezius muscle palsy.
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.
An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
An injury to the axillary nerve would result in deltoid muscle weakness.
An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging
Question 16:
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Options:
- Valgus laxity at 30 degrees of knee flexion
- Varus laxity at 30 degrees of knee flexion
- Posterior drawer
- Pivot shift
- Patellar apprehension
Correct Answer: Pivot shift
Explanation:
DISCUSSION: The T
2
-weighted sagittal MRI scan shows the classic “bone bruise” pattern seen with an anterior cruciate ligament (ACL) tear. These lesions are thought to represent subcortical trabecular hemorrhages and are manifested as an increase in signal intensity on T
2
-weighted images and diminished signal intensity on T
r
weighted images. They are classically located in the mid-portion of the lateral femoral condyle and posterior aspect of the lateral tibial plateau. This is due to the fact that an ACL tear typically is the result of a valgus-extemal rotation of the femur on the fixed tibia. This places most of the weight-bearing stress on the lateral femoral condyle, which rotates laterally and impacts the posterior lip of the lateral tibial plateau. This may result in an impaction fracture if the force is great enough, but more frequently causes merely a microfracture of the involved subcortical trabeculae.
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 17:
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Options:
- Spinal cord injury
- Nerve root injury
- Vagus nerve injury
- Recurrent laryngeal nerve injury
- Horner’s syndrome
Correct Answer: Recurrent laryngeal nerve injury
Explanation:
DISCUSSION: The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury.
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 18:
Figure 51 shows the standing AP radiograph of a 56-year old woman who has multiple toe deformities and pain beneath the metatarsal heads. Shoe modification has failed to provide relief. In addition to correction of the proximal interphalangeal joint deformities, surgical treatment should consist of
Options:
- resection of the metatarsal heads of the first through fifth toes.
- Silastic MP joint arthroplasties of the first through fifth toes.
- fusion of the hallux MP joint and resection arthroplasty of the 2 nd through fifth metatarsal heads.
- fusion of hallux MP joint and distal osteotomy of the 2 nd through 5 th MT.
- plantar condylectomy of the 2 nd through 5 th MT heads & resection of proximal phx of the hallux.
Correct Answer: fusion of the hallux MP joint and resection arthroplasty of the 2 nd through fifth metatarsal heads.
Explanation:
Surgical correction of severe rheumatoid forefoot deformities with resection arthroplasties of the lesser metatarsal phalangeal joints and arthrodesis of the first metatarsal phalangeal joint resulted in a significant long-term improvement with respect to shoe wear, pain and the ability to stand and walk in 95% of the patients. There was minimal recurrence of the deformity. Previous procedures attempt to correct the lesser MTP joint deformities and a resection-type arthroplasty procedure to the 1st MTP joint. Recurrent symptomatic deformities were found in the latter.
A modification was then used that maintained the proximal phalangeal bases and used K-wires to fixate the MTP arthroplasty and IP joints which resulted in improved cosmetic result and simplified post-op management. Equal results were seen w/ no increase in recurrence or complications.
Question 19:
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Options:
- Abduction and external rotation
- Abduction and internal rotation
- Adduction and external rotation
- Adduction and internal rotation
- Extension
Correct Answer: Adduction and external rotation
Explanation:
DISCUSSION: Following anterior dislocation of the shoulder, the affected arm is typically placed in a sling with the shoulder in adduction and internal rotation. A recent study has shown that placement in this position actually results in laxity of the anterior supporting structures of the shoulder, allowing the postinjury hemarthrosis to push the labrum and capsular ligaments away from the anterior glenoid rim. Thus, immobilization in this position may actually impede healing of these structures. Alternatively, resting the arm in a position of adduction and external rotation allows the anterior supporting structures to abut against the anterior glenoid rim by forcing the hemarthrosis posteriorly. Placing the arm in this position following anterior dislocation is believed to allow for better healing of the anterior labrum and ligaments.
REFERENCE: Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2002;84:873-874.
Question 20:
A 56-year-old male sustains a Type IIIB open, comminuted tibial shaft fracture distal to a well-fixed total knee arthroplasty that is definitively treated with a free flap and external fixation. Nine months after fixator removal, he presents with a painful oligotrophic nonunion. Laboratory workup for infection is negative. Passive knee range of motion is limited to 15 degrees. What is the most appropriate treatment for his nonunion?
Options:
- Knee manipulation under anesthesia
- Cast immobilization and use of a bone stimulator
- Unilateral external fixation
- Intramedullary nailing
- Compression plating
Correct Answer: Knee manipulation under anesthesia
Explanation:
DISCUSSION: At 9 months, observation is no longer an option, as the fracture is not healing and is adjacent to a arthrofibrotic joint. Plate osteosynthesis has been shown to be an effective method of treatment for patients who have had an open fracture of the tibia that has failed to unite after external fixation and/or immobilization in a cast.
Wiss et al reported a series of fifty tibial non-unions with a similar clinical scenario. He reported that, with compression plating, 92% of the nonunions healed without further intervention. In their study, 39/50 patients, had autogenous bone grafting in addition to compression plating.
Question 21:
At what age does the lateral epicondyle normally ossify in males?
Options:
- 2 to 4 years
- 5 to 6 years
- 7 to 8 years
- 9 to 11 years
- 12 to 14 years
Correct Answer: 12 to 14 years
Explanation:
The lateral epicondylar epiphysis is the last to ossify in the elbow at age 12 to 14 years in males. The first secondary ossification center to ossify is the capitellum, which ossifies during the first 6 months of life. Next is the radial head, ossifying between age 3 and 6 years. The medial epicondyle appears between 5 and 7 years; the trochlea and olecranon at 8 and 10 years, respectively. In females, the appearance of ossification centers is about a year earlier than males.
Question 22:
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow? Review Topic
Options:
- Infraspinatus
- Teres minor
- Subscapularis
- Long head of triceps
- Latissimus dorsi
Correct Answer: Teres minor
Explanation:
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor.
Question 23:
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Options:
- Knee aspiration with cell count/cultures, C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), CT
- Knee aspiration with cell count/cultures, CRP, ESR
- Fresh-frozen specimen at the time of revision knee arthroplasty only
- Technetium-99m bone scan, knee aspiration with cell count/cultures
Correct Answer: Knee aspiration with cell count/cultures, CRP, ESR
Explanation:
DISCUSSION:
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 24:
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Options:
- Administration of broad spectrum IV antibiotics
- Irrigation and debridement in OR followed by broad spectrum IV antibiotics
- NSAIDS and observation with repeat ESR and CRP in 24 hours
- Joint aspiration and blood cultures
Correct Answer: Joint aspiration and blood cultures
Explanation:
Discussion: The patient is demonstrating signs of septic shock. Administration of antibiotics should not be delayed. Aspirating the knee joint and obtaining blood cultures can be rapidly accomplished to obtain accurate specimens. This should be followed immediately by administration of broad spectrum IV antibiotics. Patients with septic shock can be identified with a clinical construct of sepsis with persisting hypotension requiring vasopressors to maintain mean arterial pressure (MAP) ≥ 65 mmHg and having a serum lactate level > 2mmol/L (18 mg/dL) despite adequate volume resuscitation. With these criteria, hospital mortality is in excess of 40%.
Question 25:
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?
Options:
- Aggressive physical therapy
- Manipulation under anesthesia
- Investigation for periprosthetic infection
- Revision knee arthroplasty
- Resection arthroplasty
Correct Answer: Investigation for periprosthetic infection
Explanation:
DISCUSSION: Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined.
REFERENCES: Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Gonzalez MH, Mekhail AO: The failed total knee arthroplasty: Evaluation and etiology. J Am Acad Orthop Surg 2004;12:436-446.
Question 26:
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Options:
- Flexion contracture of 5°
- Subchondral cyst in the medial tibial condyle
- Lateral meniscal degeneration seen in an MRI scan
- Rheumatoid arthropathy
- Previous medial meniscectomy
Correct Answer: Rheumatoid arthropathy
Explanation:
DISCUSSION: Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15°), anatomic varus of greater than 10°, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
REFERENCE: Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 27:
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
Options:
- early motion and muscle strengthening.
- immobilization in a thumb spica cast with the thumb abducted.
- open reduction and internal fixation through a volar approach.
- open reduction and internal fixation through a dorsal approach.
- closed reduction and percutaneous pin fixation.
Correct Answer: open reduction and internal fixation through a dorsal approach.
Explanation:
DISCUSSION: The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper’s injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach.
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
Question 28:
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation?
Options:
- Anterior horn of the lateral meniscus
- Posterior cruciate ligament
- Posterior horn of the medial meniscus
- Popliteus tendon
- Quadriceps muscle
Correct Answer: Posterior horn of the medial meniscus
Explanation:
DISCUSSION: Cadaveric studies have demonstrated the important role of the posterior horn of the medial meniscus in stabilizing the anterior cruciate ligament-deficient knee with significantly greater resultant force in the medial meniscus when subjected to anterior tibial loads. The posterior horn of the medial meniscus is thought to limit anterior tibial translation by acting as a buttress by wedging against the posterior aspect of the medial femoral condyle. The other soft tissues mentioned do not play any significant role in prevention of anterior tibial translation in the anterior cruciate ligament-deficient knee.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 200.
Allen CR, Wong EK, Livesay GA, et al: Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res 2000;18:109-115.
Levy IM, Torzilli PA, Warren RF: The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am 1982;64:883-888.
0
•v.
.
jfp
JM
w
!i
1
mf
m
Question 29:
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient’s neurologic recovery can be best determined by
Options:
- myelography with CT.
- spinal cord-evoked potentials.
- repeat physical examinations.
- MRI.
- electromyography and nerve conduction velocity studies.
Correct Answer: repeat physical examinations.
Explanation:
DISCUSSION: The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient’s neurologic recovery is repeated physical examinations over the first 48 to 72 hours.
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1185-1194.
Question 30:
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic
Options:
- Sling immobilization and rest
- Physical therapy for aggressive stretching
- Intra-articular corticosteroid injection and stretching program
- Manipulation of the shoulder under anesthesia
- Arthroscopic subacromial decompression and capsular release
Correct Answer: Intra-articular corticosteroid injection and stretching program
Explanation:
The patient has stage II adhesive capsulitis. Patients most commonly affected are women between the ages of 40 and 60, and most cases are considered idiopathic. The preferred method of treatment is an intra-articular corticosteroid injection to decrease inflammation in the joint and allow for a gentle stretching therapy program. Sling immobilization is contraindicated because it likely will promote further joint contracture and prolonged recovery. Aggressive capsular stretching in the early stages of the disease is often counterproductive, unless pain can be adequately controlled with medication or injections. Manipulation under anesthesia and arthroscopic surgical treatment are used when symptoms remain refractory despite initial nonsurgical management.
Question 31:
A healthy, active year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in A radiograph taken after the fall is shown in He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Options:
- Open reduction and cerclage fixation of the fracture
- Open reduction and revision of the femoral implant to a long cemented stem
- Open reduction and revision of the femoral implant to a long fluted and tapered uncemented stem
- Application of balanced traction followed by surgery after the ecchymosis has resolved
Correct Answer: Application of balanced traction followed by surgery after the ecchymosis has resolved
Explanation:
DISCUSSION:
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 32:
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm 3 . Management should consist of
Options:
- suppressive antibiotics.
- open irrigation and debridement with polyethylene exchange.
- one-stage resection arthroplasty and reimplantation.
- two-stage resection arthroplasty and reimplantation.
- arthroscopic irrigation and debridement.
Correct Answer: two-stage resection arthroplasty and reimplantation.
Explanation:
DISCUSSION: The treatment of choice for a late hematogenous infection is two-stage resection arthroplasty and reimplantation, with parenteral antibiotics prior to reimplantation. This is particularly true when septic loosening has occurred as in this patient. Open irrigation and debridement with polyethylene exchange has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient’s medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement.
REFERENCES: Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
Hanssen AD, Rand JA, Osmon DR: Management of the infected total knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 1070-1089.
Question 33:
If heel varus corrects with a Coleman block test, then the hindfoot deformity is flexible. This test proves that the varus is due to a
Options:
- dorsiflexed first ray.
- varus position of the forefoot.
- plantar flexed first ray.
- valgus hindfoot.
- rigid flatfoot.
Correct Answer: plantar flexed first ray.
Explanation:
DISCUSSION: The Coleman block test is used to evaluate the effect of the forefoot on the rearfoot varus. If the deformity corrects with the block, then the hindfoot deformity is flexible and the varus position is secondary to the plantar flexed first ray or valgus position of the forefoot. A rearfoot orthotic will not correct the forefoot cause of the deformity. The patient still may need a lateralizing calcaneal osteotomy to realign the hindfoot.
REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.
Alexander IJ, Johnson KA: Assessment and management of pes cavus in Charcot-Marie-Tooth disease. Clin Orthop Relat Res 1989;246:273-281.
Question 34:
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Options:
- Radially
- Circumferentially
- Vertically
- Obliquely
- Randomly
Correct Answer: Circumferentially
Explanation:
DISCUSSION: The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers.
REFERENCES: Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Question 35:
Figure 16 shows the radiograph of a 75-year-old man who has progressive groin pain and a limp following total hip replacement. At revision surgery, the anterior and posterior columns of the acetabulum are noted to be intact. The optimal surgical technique for acetabular component reconstruction is a
Options:
- threaded (screw-in) cup with a hydroxyapatite coating.
- protrusio cage reconstruction with a cemented cup.
- large cementless cup with bone grafting of defects.
- small cup with a high and lateral hip center.
- bulk allograft reconstruction of the defect with a cemented cup.
Correct Answer: large cementless cup with bone grafting of defects.
Explanation:
DISCUSSION: Large cementless acetabular components have been shown to perform well in revision acetabular reconstruction. The use of such components is predicated on the presence of adequate anterior and posterior column bone. If a good press-fit can be achieved between the anterior and posterior columns, typically, the remaining defects can be filled with morcellized bone graft. Protrusio cages are typically used in situations where it is not possible to obtain adequate fixation with a large acetabular component. The use of a high hip center with small sockets is more typical of primary arthroplasty in patients with developmental dysplasia of the hip. Bulk acetabular allografts for large segmental defects might be necessary in certain situations, although the use of bulk allografts has resulted in a high failure rate after 5 years. Early results of the use of protrusio cages and bone grafting for large segmental defects have been favorable.
REFERENCES: Petrera P, Rubash HE: Revision total hip arthroplasty: The acetabular component. J Am Acad Orthop Surg 1995;3:15-21.
Lachiewicz PF, Poon ED: Revision of a total hip arthroplasty with a Harris-Galante porous-coated acetabular component inserted without cement: A follow-up note on the results at five to twelve years. J Bone Joint Surg Am 1998;80:980-984.
Question 36:
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Options:
- fascia lata graft to restore the coracoacromial arch.
- immediate subscapularis repair.
- revision arthroplasty with glenoid reaming to centralize the component.
- revision arthroplasty with increased retroversion in the humeral component.
- arthroscopic subacromial decompression.
Correct Answer: immediate subscapularis repair.
Explanation:
DISCUSSION: Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture.
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 37:
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Options:
- Improvement in range of motion
- Reduction in range of motion
- Increase in extensor mechanism lag
- No differences in motion and strength
Correct Answer: No differences in motion and strength
Explanation:
DISCUSSION:
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 38:
A 13-year-old boy has a radiographically mild, clinically stable slipped capital femoral epiphysis (SCFE). What is the most appropriate treatment? Review Topic
Options:
- Spica casting
- Open reduction and internal fixation
- Single screw in situ fixation of the epiphysis
- Two-screw in situ fixation of the epiphysis
- Crutches and no weight bearing for 6 weeks
Correct Answer: Spica casting
Explanation:
The accepted treatment of a stable SCFE lesion involves fixation of the epiphysis in situ with a single screw that is perpendicular to the epiphysis and central in both the AP and lateral planes. Constructs such as the three-screw inverted triangle configuration have increased rates of penetration of the femoral head as well as femoral head osteonecrosis. Spica casting was once a popular treatment modality but is associated with a high incidence of chondrolysis and is no longer recommended. Closed reduction attempts increase the risk of osteonecrosis.
(SBQ13PE.46) What developmental milestones are likely to be present in a 30-month-old child?
Review Topic
Hand dominance established
Hops on one foot
Heel-to-toe walk
Puts shoes on correct feet
Manages buttons
Hand dominance is usually established in the third year of life.
Normally, children younger than 2 years of age are ambidextrous. In some normal cases this persists after 2 years. Although there is some variability in this timing, strong hand preference in a younger child may be the result of a neurologic deficit.
Frankenburg et al. used the Denver Developmental Screening Test (DDST) to evaluate 1036 Denver area children from 2 to 6.4 years. The ages at which 25, 50, 75 and 90 percent of children could perform tasks were calculated to establish norms for the sample. The authors stress that the DDST is not an intelligence test, but rather a screening test to be used in clinical practice to determine whether a child's development is within the normal range.
Illustration
A
shows
the
DDST.
Incorrect
2:
Normal
for
Question 39:
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Options:
- Deep to the arcuate ligament
- Closer to bone in larger legs
- On the muscle belly of the popliteus
- On the bony posterolateral corner of the tibia
- Superficial to the lateral head of the gastrocnemius
Correct Answer: Superficial to the lateral head of the gastrocnemius
Explanation:
DISCUSSION: At the level of tibial bone resection in total knee arthroplasty, the common peroneal nerve lies superficial to the lateral head of the gastrocnemius and is therefore protected by this structure. In an MRI study of 60 knees, the mean distance from the bony posterolateral corner of the tibia to the nerve was 1.49 cm, with no distance less than 0.9 cm. The distance from the bone to nerve was greater in larger legs.
REFERENCES: Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the “pie crust” technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-52, 4-53.
Question 40:
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be
Options:
- activity limitations because of localized pain.
- the likelihood of development of malignant degeneration in adulthood.
- the likelihood of development of a growth deformity.
- ambiguity regarding the diagnosis based on the imaging studies.
- obvious progression over the past 5 years, raising suspicion of malignant degeneration.
Correct Answer: activity limitations because of localized pain.
Explanation:
DISCUSSION: In a young person with solitary osteochondroma, the best surgical indication is symptoms that limit activity. A growth deformity is unlikely to occur at this age. Malignant degeneration is exceptionally rare and noted most commonly in adults. Growth is expected until skeletal maturity.
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors and Usual Treatment: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 181-205.
Question 41:
What effect does deep freezing have on allograft tissue?
Options:
- Causes no deleterious clinical effect on ligamentous grafts
- Causes a less deleterious effect on cartilage than on ligamentous grafts
- Causes degradation of the extracellular matrix
- Allows for preservation of cells with tissue
- Eliminates the chance of human immunodeficiency virus (HIV) transmission
Correct Answer: Causes no deleterious clinical effect on ligamentous grafts
Explanation:
DISCUSSION: Deep freezing is the simplest and most widely used method of ligament allograft storage. All cells in the tissue are destroyed with the freezing. However, for this reason, it is not a preferred storage method for menisci or cartilage allografts. Although this method may enhance success because it removes potential antigens located on the cells, it cannot guarantee elimination of HIV transmission. The advantage of cryopreservation storage is that a significant number of cells will survive the process, a factor important in meniscal allograft survival after implantation. No deleterious effects are noted clinically because of the acellularity of the tissue.
REFERENCES: Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in
knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
Question 42:
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Options:
- Long thoracic/rhomboid
- Long thoracic/serratus anterior
- Long thoracic/supraspinatus
- Dorsal scapular/trapezius
- Spinal accessory/trapezius
Correct Answer: Long thoracic/serratus anterior
Explanation:
DISCUSSION: The clinical picture reveals medial scapular winging, which involves the serratus anterior muscle, potentially due to an injury to the long thoracic nerve that innervates this muscle. Injury to the long thoracic nerve is usually due to closed trauma, direct compression, traction or stretching injury, a direct blow, or, very rarely, viral infection such as Parsonage-Tumer syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 43:
Figure 43 shows an arthroscopic view of the posteromedial compartment of a patient’s left knee using a 70-degree arthroscope placed through the intercondylar notch. The arrow is pointing to what structure?
Options:
- Posterior horn of the medial meniscus
- Semimembranosus tendon
- Medial tibial plateau
- Medial head of the gastrocnemius tendon
- Medial plica
Correct Answer: Posterior horn of the medial meniscus
Explanation:
DISCUSSION: Passing the 70-degree arthroscope through the intercondylar notch provides excellent visualization of the posteromedial corner of the knee. This view should be part of every knee arthroscopy because these structures are often not well visualized from the anterior portals. If this view is omitted, tears of the peripheral posterior horn of the medial meniscus can be overlooked. The arrow points to the peripheral aspect of the posterior horn of the medial meniscus. With an intact medial meniscus, the medial tibial plateau should not be seen from this view. The semimembranosus and gastrocnemius tendons are extra-articular and not visualized.
REFERENCES: Miller MD: Basic arthroscopic principles, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, pp 224-237.
Gold DI, Schaner PJ, Sapega AA: The posteromedial portal in knee arthroscopy: An analysis of diagnostic and surgical utility. Arthoscopy 1995;11:139-145.
Question 44:
Which of the following conditions precludes performing a tendon transfer?
Options:
- The target joint has a full passive range of motion.
- The range of motion of the target joint only occurs in the direction of correction.
- The target joint cannot be passively corrected to its neutral position.
- The muscle to be transferred is out-of-phase.
- There is no pulley to assist the transferred muscle’s fulcrum.
Correct Answer: The target joint cannot be passively corrected to its neutral position.
Explanation:
DISCUSSION: Several conditions must be met before a tendon transfer has the potential to correct a dynamic deformity. If the target joint cannot be passively corrected to neutral, it indicates that a static joint contracture or bony deformity exists that cannot be corrected with a dynamic tendon transfer. While in-phase muscles are best, out-of-phase muscles are often the only muscles available for transfer. Tendon transfer should pull in a straight line to avoid tethering and late failure.
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.
Coughlin MJ, Mann RA: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 786-861.
Question 45:
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of
Options:
- lateral retinacular release and medial reefing.
- patellar tendon transfer medially.
- lateral release and patellar tendon transfer.
- femoral and tibial derotation osteotomies.
- continued observation.
Correct Answer: continued observation.
Explanation:
DISCUSSION: Chronic dislocation of the patella is occasionally seen in patients with Down syndrome. In early childhood, patellar realignment may restore stability of the patellae. In later childhood, bony changes in the patellar groove interfere with stability, even if surgical realignment is performed. Realignment can also lead to increased knee pain postoperatively. In asymptomatic patients who are able to extend their knees, continued observation is the management of choice.
REFERENCES: Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
Mendez AA, Keret D, MacEwen GD: Treatment of patellofemoral instability in Down’s syndrome. Clin Orthop 1988;234:148-158.
Question 46:
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Options:
- Start IV antibiotics, obtain wound swab for culture, perform irrigation and debridement and retain hardware
- Start IV antibiotics, obtain deep soft tissue and bone cultures in OR, perform irrigation and debridement and remove hardware
- Obtain wound swab for culture, start IV antibiotics, perform irrigation and debridement and remove hardware
- Obtain deep bone and soft tissue cultures in OR, start IV antibiotics, perform irrigation and debridement and remove hardware
Correct Answer: Obtain deep bone and soft tissue cultures in OR, start IV antibiotics, perform irrigation and debridement and remove hardware
Explanation:
Discussion: Management of acutely infected wounds is primarily surgical. Osteomyelitis frequently involves Orthopaedic hardware, which would ideally be removed or replaced given biofilm involvement. Multiple operative cultures of fluid collections, soft tissues and bone should routinely be obtained. Culture yield is highest if cultures are obtained before empiric antibiotic treatment is started. Tissue samples are greatly preferred to swabs, which are notoriously inaccurate.
Question 47:
-During preparticipation physicals for college football, an athlete tests positive for the sickle-cell trait.With regard to clearance to play, his team physician should
Options:
- counsel the athlete about his personal risk for bone infarcts.
- recommend a prophylactic splenectomy prior to participation.
- bar the athlete from participating in National Collegiate Athletic Association-sanctioned events.
- assure the athlete that he can participate in football without concern.
- ensure that the athlete is given adequate recovery time and remains hydrated.
Correct Answer: ensure that the athlete is given adequate recovery time and remains hydrated.
Question 48:
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Options:
- L4 nerve root radiculopathy
- L5 nerve root radiculopathy
- Associated bowel and bladder dysfunction
- Symptoms associated with arachnoiditis
- Wide-based gait, left-sided Hoffman’s sign
Correct Answer: L4 nerve root radiculopathy
Explanation:
DISCUSSION: The MRI scan reveals a L4-L5 foraminal disk herniation originating from the L4-5 disk space that has migrated up into the foramen, compressing the left L4 nerve root. There is normal distribution of the roots in the cerebrospinal fluid, excluding arachnoiditis as a diagnosis, and disk herniation in this location would not result in cauda equina syndrome or myelopathy.
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 49:
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T 1 -weighted MRI scan are shown in Figures 28a and 28b. Management should consist of
Options:
- external beam radiation.
- curettage and cementation of the lesion with a compression hip screw and side plate fixation.
- curettage and cementation of the lesion with intramedullary fixation.
- cemented bipolar hemiarthroplasty.
- radioactive iodine infusion.
Correct Answer: cemented bipolar hemiarthroplasty.
Explanation:
DISCUSSION: The radiograph and MRI scan reveal a lytic lesion in the left femoral neck region that extends to the lesser trochanter. Although external beam radiation and radioactive iodine infusion may be helpful in controlling the local disease, the patient is at high risk for femoral neck fracture given the location of the lesion. Prophylactic surgery is indicated; therefore, the treatment of choice is a cemented bipolar hemiarthroplasty. The use of a compression hip screw and side plate or an intramedullary nail has a high likelihood of failure with disease progression. Postoperative treatment with radiation therapy and bisphosphonates is also indicated.
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Clarke HD, Damron TA, Sim FH: Head and neck replacement endoprosthesis for pathologic proximal femoral lesions. Clin Orthop 1998;353:210-217.
Question 50:
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Options:
- Co-Cr, stainless steel, stainless steel.
- stainless steel, stainless steel, Co-Cr.
- stainless steel, Co-Cr, Co-Cr.
- titanium alloy, titanium alloy, titanium alloy.
- titanium alloy, stainless steel, Co-Cr.
Correct Answer: titanium alloy, titanium alloy, titanium alloy.
Explanation:
DISCUSSION: Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other.
REFERENCES: Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 51:
What pharmacologic agents are preferred for the treatment of symptomatic active Paget’s disease?
Options:
- Nasal calcitonin
- Bisphosphonates
- Nonsteroidal anti-inflammatory drugs
- Furosemide
- Antiviral therapy
Correct Answer: Bisphosphonates
Explanation:
DISCUSSION: Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget’s disease.
REFERENCE: Delman PD, Meunier PJ: The management of Paget’s disease. N Eng J Med 1997;336:558-566.
Question 52:
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan? Review Topic
Options:
- Maintain sling immobilization for 6 weeks, and then begin a global range-of-motion program.
- Maintain sling immobilization for 3 weeks, and then begin a global range-of-motion program.
- Immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side.
- Immediately begin a passive range-of-motion program for forward elevation only; no external rotation is allowed for 6 weeks.
- Immediately begin active range of motion in forward elevation and external rotation to the side with a progression to full rotator cuff strengthening in 3 weeks.
Correct Answer: Immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side.
Explanation:
The patient needs to immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side. Sling immobilization without stretching for either 3 or 6 weeks will result in severe stiffness that will compromise her ultimate range of motion. Since she has a good quality subscapularis tendon, there is no need to avoid beginning external rotation to the side. However, starting a strengthening program at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal.
Question 53:
03 The sagittal oblique MRI scan shown in Figure 70 reveals a lesion in the shoulder that typically affects what neurologic structure?
Options:
- – Axillary nerve
- – Musculocutaneous nerve
- – Long thoracic nerve
- – Suprascapular nerve to the infraspinatus muscle
- – Suprascapular nerve to the supraspinatus muscle back answer Question 199.03
Correct Answer: – Suprascapular nerve to the infraspinatus muscle
Explanation:
Ganglion cysts in the shoulder has been reported in the literature and when they occur in the shoulder typically compress the suprascapular nerve at the spinoglenoid notch primarily affecting the infraspinatus muscle, but depending on their size may also affect the supraspinatus motor brances.
The cysts form either because of a lesion of the capsulolabral complex at the superior/posterosuperior glenoid in the shoulder or because of myxoid degeneration of the capsule.
back to this question next question
Question 54:
Which study is most useful for diagnosis of exertional compartment syndrome?
Options:
- MRI
- Arterial Doppler
- Static compartment pressures
- Exertional compartment pressures
Correct Answer: Exertional compartment pressures
Explanation:
DISCUSSION
The most sensitive study in the diagnosis of exertional compartment syndrome is intracompartmental pressures taken at rest (compared to pressures taken immediately after exercise). MRI often can reveal nonspecific muscle edema in exertional compartment syndrome, but this is usually not diagnostic. Arterial Doppler studies are usually unremarkable unless they are taken after exercise, in which case these findings may be abnormal.
CLINICAL SITUATION FOR QUESTIONS 48 THROUGH 50
Figures 48a through 48f reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures.
Question 55:
What is the main biologic effect of aggrecan in cartilage? Review Topic
Options:
- Extracellular matrix protein involved in the organization of collagen
- Proteoglycan involved in the hydrophilic behaviour of cartilage
- Cartilage matrix protein that plays a role in cartilage tissue organization
- Collagen component responsible for stability
- Non-collagenous extracellular matrix protein that regulates chondrocyte proliferation
Correct Answer: Extracellular matrix protein involved in the organization of collagen
Explanation:
Aggrecan binds hyaluronic acid to attract water, which accounts for its hydrophilic property.
Aggrecan is the predominant proteoglycan in cartilage. It contains a large number of negatively charged sequences that attract water called sulfated glycosaminoglycan (GAG) chains. Its the N-terminal globular domain of aggrecan that binds hyaluronan to form huge aggregates. Together with its chondroitin sulfate chains, they help to create a hydrophilic viscous gel that decreases the coefficient of friction as well as to help absorb compressive loads.
Ulrich-Vinthe et al. reviewed the biology of articular cartilage. They report that matrix metalloproteinases and aggrecanases play a major role in aggrecan degradation and their production is upregulated by mediators associated with joint inflammation and overloading.
Illustration A shows a depiction of the function of aggrecan in articular cartilage. In the relaxed state, the aggregates draw water into cartilage. With compressive loads, the water is displaced to cushion the load. Upon removal of the load, the water content is restored.
Incorrect Answers:
Question 56:
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Options:
- a short leg cast with the ankle in slight plantar flexion.
- a corticosteroid injection into the retrocalcaneal bursa.
- excision of the os trigonum.
- excision of the superior tuberosity of the calcaneus.
- ankle arthroscopy with loose body removal.
Correct Answer: excision of the os trigonum.
Explanation:
DISCUSSION: The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic.
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 57:
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
Options:
- He has osteomyelitis with a significant subperiosteal abscess that will necessitate open drainage in the operating room.
- He has osteomyelitis without any abscess, so continued IV antibiotics and clinical observation are recommended.
- He has a muscle abscess that would best be treated by percutaneous drainage in interventional radiology.
- The MR image shows cellulitis with some adjacent myositis, so a short course of IV antibiotics followed by 2 to 3 weeks of appropriate oral antibiotics is recommended.
Correct Answer: He has osteomyelitis with a significant subperiosteal abscess that will necessitate open drainage in the operating room.
Explanation:
DISCUSSION
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.
CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Question 58:
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Options:
- Superior labrum anterior and posterior (SLAP) lesion
- Bankart lesion
- Rotator cuff interval tear
- Rotator cuff tendinitis
- Posterior glenohumeral subluxation
Correct Answer: Posterior glenohumeral subluxation
Explanation:
DISCUSSION: A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging.
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 59:
A 10-year-old boy has 2 months of right knee pain that started at summer camp. The patient denies constitutional symptoms. There is no lymphadenopathy present. CT of the chest shows no signs of metastatic disease. Imaging studies and biopsy results are shown in Figures A-E. What is the most likely diagnosis?
Options:
- Synovial sarcoma
- Malignant fibrous histiocytoma
- Chondrosarcoma
- Ewing's sarcoma
- Osteosarcoma
Correct Answer: Osteosarcoma
Explanation:
The age, imaging and histology are consistent with an osteosarcoma. The radiograph shows an aggressive (lytic, mottled, sclerotic) appearing lesion around the distal femur metadiaphyseal region. The T2 weighted MRI image shows a significant soft tissue mass which appears to arise from the distal femur with destruction of the adjacent cortex. The biopsy shows an infiltrative pattern with elements of osteoid and bone.
Treatment for osteosarcoma includes neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy.
Question 60:
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Options:
- a sling, ice, and isometric exercises.
- a glenohumeral cortisone injection.
- surgical repair of the coracoclavicular ligaments.
- chin-ups and latissimus pull-down exercises.
- cross-chest stretches.
Correct Answer: a sling, ice, and isometric exercises.
Explanation:
DISCUSSION: The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 61:
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
Options:
- Brostrom procedure
- Syndesmosis repair or stabilization
- Allograft lateral ligament reconstruction
- Excision of loose body/fracture fragment
- Repair of the SPR with possible fibular groove deepening
Correct Answer: Syndesmosis repair or stabilization
Explanation:
DISCUSSION FOR QUESTIONS 107 AND 108:
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.
Question 62:
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Options:
- mm femoral head in combination with a metal-backed polyethylene component
- mm femoral head in combination with an all-polyethylene acetabular component
- mm femoral head in combination with a metal-backed polyethylene component
- mm femoral head in combination with an all-polyethylene component
- mm femoral head in combination with a metal-backed polyethylene component
Correct Answer: mm femoral head in combination with a metal-backed polyethylene component
Explanation:
The size of the femoral head and the calculated mean annual rate of volumetric wear has a significant relationship. Rate of volumetric wear was highest in assoc with 32 mm femoral lowest in assoc with 22 mm heads. The predominant mechanisms of wear of the polyethylene were abrasion and adhesions rather than fatigue-cracking or delamination on the subsurface. Decreased thickness of the polyethylene has an adverse effect on the rate of wear of the metal-backed components. Rate of linear wear is highest in assoc. with 22-mm heads and lowest in relation to 32-mm heads, so the optimal size of a femoral head should be 28 mm where there is minimal linear and volumetric wear.
Question 63:
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Options:
- Biceps tendon
- Coracohumeral ligament
- Superior glenohumeral ligament
- Middle glenohumeral ligament
- Inferior glenohumeral ligament
Correct Answer: Biceps tendon
Explanation:
DISCUSSION: This view from the lateral portal shows a full-thickness rotator cuff tear. The glenohumeral joint can be visualized through this tear. The glenoid, labrum, and biceps tendon attaching to the superior aspect of the glenoid are easily viewed from this portal, and the arrow is pointing to the biceps tendon. Arthroscopic rotator cuff repair can be performed while visualizing from this portal and using anterior and posterior working portals.
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 64:
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T 1 -weighted, STIR, and T 1 -weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Options:
- Peripheral nerve sheath tumor
- Malignant peripheral nerve sheath tumor
- Malignant fibrous histiocytoma
- Liposarcoma
- Synovial sarcoma
Correct Answer: Malignant peripheral nerve sheath tumor
Explanation:
DISCUSSION: The images reveal a large mass in the posterior thigh arising from the sciatic nerve. The lesion is edematous, and the gadolinium image reveals rim enhancement, suggesting necrosis, given that the STIR image is not uniformly bright as would be seen in a cystic lesion. The PET scan has increased uptake, in this case a standard unit value (SUV) of greater than 2.0. These findings are all very suggestive of a malignant process. The history of neurofibromatosis makes a malignant peripheral nerve sheath tumor, or neurofibrosarcoma, the most likely diagnosis. The term “peripheral nerve sheath tumor” has replaced neurolemmoma and schwannoma.
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 65:
- A 40-year-old woman has progressive pain and limited range of motion in her long finger. Figure 28a shows the radiograph, and Figure 28b shows a biopsy specimen of the same lesion. What is the most likely diagnosis?
Options:
- Enchondroma
- Osteoblastoma
- Giant cell tumor
- Aneurysmal bone cyst
- Fibrous dysplasia
Correct Answer: Giant cell tumor
Explanation:
Giant Cell tumors (GCT) are relatively common in the appendicular skeleton, most common during the 4th or 5th decades of life. GCT’s are destructive lesions with variable amounts of reactive bone at their margin. Successful treatment requires complete surgical excision.
Question 66:
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of
Options:
- cast immobilization for 6 weeks.
- brief immobilization followed by rest for 6 weeks.
- internal fixation with a compression screw.
- internal fixation with a tension band wire.
- bone stimulation.
Correct Answer: internal fixation with a compression screw.
Explanation:
DISCUSSION: The CT scan shows a stress fracture of the olecranon. This injury is the result of repetitive abutment of the olecranon into the olecranon fossa, traction from triceps activity during the deceleration phase of the throwing motion, and impaction of the medial olecranon onto the olecranon fossa from valgus forces. Fractures may be either transverse or oblique in orientation. Initial treatment consists of rest and temporary splinting. Electrical bone stimulation may also be considered. Open fixation with a large compression screw is recommended when nonsurgical management has failed to provide relief.
REFERENCES: Ahmad CS, ElAttrache NS: Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 2004;23:665-676.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Question 67:
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Options:
- a BMI lower than 30.
- diabetes mellitus, with a hemoglobin A1c test result less than 7.
- tranexamic acid use.
- metabolic syndrome.
Correct Answer: metabolic syndrome.
Explanation:
DISCUSSION:
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 68:
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Options:
- Contracted plantar fascia and weakness of the tibialis anterior
- Overpull of the gastrocnemius-soleus complex and weakness of the anterior tibialis
- Overpull of the posterior tibialis and weakness of the peroneals
- Overpull of the peroneus brevis and weakness of the posterior tibialis
- Overpull of the tibialis anterior and weakness of the peroneus longus
Correct Answer: Overpull of the tibialis anterior and weakness of the peroneus longus
Explanation:
DISCUSSION: Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior.
REFERENCES: Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Tachdjian MO: Pediatric Orthopedics ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 1937-1946.
Question 69:
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
Options:
- the approach used reduces the torque-to-failure (fracture) of the construct to less than 50% of the intact femur.
- the technique of repair can return the reconstructed prosthesis/bone composite to nearly the strength of the intact femur.
- there is no relationship between the density of the native bone and the strength of the prosthesis/bone composite.
- the addition of bone graft substitute or autograft has been shown to lessen the time to complete healing.
- there is a one in five chance of fracture with this technique; therefore, the surgeon must carefully weigh the potential benefits versus this risk.
Correct Answer: the approach used reduces the torque-to-failure (fracture) of the construct to less than 50% of the intact femur.
Explanation:
DISCUSSION: The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.
REFERENCE: Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.
Question 70:
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Options:
- an electromyogram and nerve conduction velocity studies.
- an MRI scan.
- a bone scan.
- physical therapy.
- bed rest.
Correct Answer: an MRI scan.
Explanation:
DISCUSSION: In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk.
REFERENCES: Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, Kojimoto H, Shimomura Y: Lumbar disc herniation in children. J Pediatr Orthop 1990;10:394-396.
Question 71:
A hip compression screw is placed in a test jig and a bending load is applied to the tip of the screw. After the load is released, the screw returns completely to its original shape. What is this type of deformation called?
Options:
- Plastic
- Elastic
- Fatigue
- Creep
- Torsion
Correct Answer: Elastic
Explanation:
When an implant is loaded below the yield point, by definition, it undergoes elastic deformation, meaning that all of the deformation recovers when the load is removed. If it is loaded above the yield point, then plastic or permanent deformation occurs. Fatigue is the gradual accumulation and progression of cracks in the material, which, after many cycles of loading, can lead to gross failure. Creep is the gradual accumulation of permanent (plastic) deformation over time, which may occur with polymeric materials but is not typical of metals or ceramics. Torsion refers to a torque being applied about the long axis of a bone or an implant. In general, the materials and dimensions of an implant are chosen to avoid plastic deformation or fatigue failure during typical clinical use.
Question 72:
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Options:
- Resistance to adhesive wear B. Resistance to abrasive wear C. Resistance to fatigue wear
- Resistance to creep
Correct Answer: Resistance to creep
Explanation:
DISCUSSION:
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 73:
Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population?
Options:
- Swimmers and divers
- Football lineman
- Rugby players
- Gymnasts and throwing athletes
- Cyclists
Correct Answer: Gymnasts and throwing athletes
Explanation:
DISCUSSION: The etiology of osteochondritis dissecans of the capitellum is somewhat unclear. However, trauma has been implicated in this disease process. Gymnasts who load their upper extremities during tumbling and throwing athletes with repetitive trauma during the throwing motion are common patient subgroups in which osteochondritis dissecans of the elbow is seen. This often occurs in the adolescent age population.
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-523.
Takahara M, Ogino T, Fukushima S, et al: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum. Am J Sports Med 1999;27:728-732.
Question 74:
A 10-month-old boy has an untreated developmental hip dislocation.
Options:
- Sclerosis of the proximal femoral epiphysis with subchondral lucency
- Abnormal femoral head-neck junction offset
- Widening of the proximal femoral physis with normal femoral head-neck junction offset
- Absence of the proximal femoral epiphysis secondary ossification center
Correct Answer: Absence of the proximal femoral epiphysis secondary ossification center
Explanation:
DISCUSSION
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Question 75:
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Options:
- Hemoglobin A1c of 8.2
- Serum albumin of 2.5 g/dL
- Hemoglobin of 10 g/dL
- Ankle-brachial index of 1.0
- Transcutaneous partial pressure of O 2 (TcPO 2 ) of 50 mm Hg
Correct Answer: Transcutaneous partial pressure of O 2 (TcPO 2 ) of 50 mm Hg
Explanation:
DISCUSSION: The TcPO
2
measures the O
2
delivering capacity of the local vasculature. Values above 40 mm Hg have been shown to correlate with positive healing potential. The hemoglobin A1c is a good indicator of long-term glucose levels; however, it has no direct correlation with wound healing potential. Serum albumin is an indirect measure of nutritional status, and deficiencies in nutrition must be addressed before any surgery. Adequate hemoglobin levels are also necessary to promote adequate oxygenation to the amputation site. The ankle-brachial index may be falsely elevated as a result of calcified vessels in patients with diabetes mellitus.
REFERENCES: Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
Dwars BJ,van den Broek TA, Rauwerda JA, et al: Criteria for reliable selection of the lowest level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
Question 76:
What is the most common malignancy involving the hand?
Options:
- Epithelioid sarcoma
- Synovial sarcoma
- Metastatic lung carcinoma
- Chondrosarcoma
- Squamous cell carcinoma
Correct Answer: Squamous cell carcinoma
Explanation:
DISCUSSION: Skin cancers far outnumber primary musculoskeletal malignancies of the hand and the most common of these is squamous cell carcinoma. Metatastic lung carcinoma, while classic for the carcinoma that metastasizes to the hand, does so at an extremely low rate.
REFERENCES: Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Fleegler EJ: Skin tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 2184-2205.
Question 77:
-The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the
Options:
- artery of the ligamentum teres.
- epiphyseal branch of the lateral femoral circumflex artery.
- posterosuperior and posteroinferior retinacular branches of the lateral femoral circumflex artery.
- posterosuperior and posteroinferior retinacular branches of the medial femoral circumflex artery. DISCUSSION-Before the age of 4 years, blood to the femoral head is supplied by the medial and lateral femoral circumflex arteries as well as the artery of the ligamentum teres. After the age of 4, the blood supply through the artery of the ligamentum teres diminishes. The lateral femoral circumflex system regresses,and its flow into the physis and epiphysis diminishes significantly so the medial femoral circumflex artery becomes the predominant blood supply to the metaphysis. The medial femoral circumflex artery provides the principal blood supply to the proximal femur via its posterosuperior and posteroinferior retinacular branches.
Correct Answer: posterosuperior and posteroinferior retinacular branches of the medial femoral circumflex artery. DISCUSSION-Before the age of 4 years, blood to the femoral head is supplied by the medial and lateral femoral circumflex arteries as well as the artery of the ligamentum teres. After the age of 4, the blood supply through the artery of the ligamentum teres diminishes. The lateral femoral circumflex system regresses,and its flow into the physis and epiphysis diminishes significantly so the medial femoral circumflex artery becomes the predominant blood supply to the metaphysis. The medial femoral circumflex artery provides the principal blood supply to the proximal femur via its posterosuperior and posteroinferior retinacular branches.
Question 78:
Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
Options:
- Placing a pelvic external fixator followed by packing the pelvis with lap pads via a subumbilical incision
- Placing lap pads for packing via a subumbilical incision in the angiography suite
- Placing lap pads for packing using the lateral window of the ilioinguinal approach (anterior approach to the internal iliac fossa)
- Packing the retroperitoneum with lap pads after exploration of the abdomen by the general surgeons
- Direct exploration of the pelvic vasculature via a midline incision followed by packing with lap pads
Correct Answer: Placing a pelvic external fixator followed by packing the pelvis with lap pads via a subumbilical incision
Explanation:
For the technique of pelvic packing patients are placed supine on an operating room table. For rotationally and/or vertically unstable fracture patterns, an external fixator is then placed to stabilize the pelvis so that the volume of the pelvis is decreased and the packing has counterforce acting against it. An approximately 6 cm to 8 cm midline incision is made extending upwards from the pubic symphysis and heading toward the umbilicus. The rectus fascia is then divided in the midline. The bladder is retracted to one side and three lap pads are packed deep to the pelvic brim. The bladder is retracted to the other side and three more lap pads are placed on that side as well. The first sponge is placed at the level of the sacroiliac joint, the second anterior to the first sponge, and the third in the retropubic space lateral and just deep to the bladder. All should be placed below the level of the pelvic brim. The fascia is then closed. If the patient is hemodynamically unstable after stabilization, then packing of the pelvis angiography should be considered.
Question 79:
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Options:
- >4 degrees (normal = neutral), the posterior condylar angle was more internally rotated relative to the transepicondylar axis. Therefore, to prevent internal malalignment using standard components, the femoral component should be more externally rotated relative to the posterior condylar axis in this scenario.
- Incorrect Answers:
Correct Answer: >4 degrees (normal = neutral), the posterior condylar angle was more internally rotated relative to the transepicondylar axis. Therefore, to prevent internal malalignment using standard components, the femoral component should be more externally rotated relative to the posterior condylar axis in this scenario.
Question 80:
An 85-year-old right hand dominant male sustains a fall onto his elbow while trying to get out of the car. His past medical history is significant for diabetes, congestive heart failure, and COPD. He lives in a nursing home, and is able to ambulate at baseline without and assistive devices. What would be the ideal definitive surgical treatment options in this patient? Review Topic
Options:
- ORIF through an olecranon osteotomy with 90-90 plating
- Total elbow arthroplasty through an anterolateral approach between the brachialis and biceps
- Acute elbow fusion
- ORIF through a tricep splitting approach with parallel plating
- Total elbow arthroplasty through a direct posterior tricep sparing approach
Correct Answer: Total elbow arthroplasty through an anterolateral approach between the brachialis and biceps
Explanation:
This elderly low-demand patient would most benefit from a total elbow arthroplasty (TEA) done through a direct posterior tricep sparing approach.
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, and suffer less complications with TEA than ORIF in select cases.
Sorensen et al evaluated short- to medium term outcome of total elbow arthroplasty (TEA) in complex fractures of the distal humerus by evaluating 24 consecutive cases. Twenty of the patients were followed for almost 2 years, and their MEPS were 15 excellent, 4 good and 1 fair result. They concluded that TEA in complex fractures of the distal humerus in elderly patients can result in acceptable short- to medium term outcome.
Mckee et al conducted a prospective, randomized, controlled trial to compare
functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary total elbow arthroplasty (TEA). They randomized 42 patients and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF, based on the MEPS.
Illustration A shows radiographs of a TEA. Incorrect Answers:
Question 81:
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Options:
- observation.
- closed reduction and cast immobilization.
- bilateral medial open reduction of the hips.
- anterior open reduction with femoral shortening.
- valgus osteotomy.
Correct Answer: observation.
Explanation:
DISCUSSION: Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
REFERENCE: Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 82:
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Options:
- anterior superior escape.
- rheumatoid arthritis.
- an acromial stress fracture.
- a centered head and an external rotation lag sign of 50 degrees.
- active forward elevation of 130 degrees.
Correct Answer: anterior superior escape.
Explanation:
Reverse total shoulder arthroplasty is relatively contraindicated in patients with acromial stress fractures and rheumatoid arthritis. A patient with active forward elevation to 130 degrees is better treated with a hemiarthroplasty because the motion already exceeds the average forward elevation attained in most studies using the reverse prosthesis. A centered case of rotator cuff tear arthropathy is also better treated with a hemiarthroplasty, especially in patients with a large external rotation lag sign because the reverse prosthesis has been shown to decrease active external rotation. However, hemiarthroplasties have not performed well in patients with anterior superior escape and in this group of patients, the reverse prosthesis is best.
Question 83:
…The patient underwent an uneventful arthroscopic repair and did well until 1 year later when she crashed during a race. She tore her anterior cruciate ligament (ACL) and underwent reconstruction. Followup after her successful ACL reconstruction reveals complaints of new shoulder pain and posterior instability from using crutches after her ACL surgery. A new MRI scan is shown in Figure 24. What factors are most likely associated with this patient’s recurrence?
Options:
- Gender
- Age
- Sport
- Bone loss DISCUSSION… Nonsurgical treatment for a first-time traumatic dislocation may not be effective in a young, athletic patient; moreover, a Bankart lesion may be present in 70% of all traumatic subluxations. A period of immobilization in external rotation may decrease the risk for recurrence, but only if the patient is placed in a brace immediately and complies with the treatment. Return to play may be possible after 2 weeks of immobilization, provided the patient undergoes appropriate range of motion, cuff strengthening, and scapular stabilization exercises. Among athletes in 1 study, 80% were able to finish the season, but 40% experienced episodes of subluxation or recurrent dislocation prior to the end of the season. The rate of recurrence after arthroscopic stabilization should be lower than 10% and may be equivalent to open repair for most patients. Bone loss remains the primary indication for open procedures, as coracoid transfers or other bone-grafting operations may be needed to reconstruct the glenoid if more than 20% of its surface area is missing. Furthermore, collision athletes may fare better with open surgery than arthroscopic options. Bone loss remains the most significant factor for recurrence across many studies. Glenoid bone loss may be present in 20% of primary dislocations and 70% of recurrent dislocations. Age younger than 30 has a high correlation with recurrence. Although men may be almost twice as likely as women to have a recurrent dislocation, age seems to be the most reliable patient-related risk factor for recurrence. Thermal capsulorrhaphy has not proven to be effective and carries a high risk for complication. More recent studies have found equal recurrence rates between open and arthroscopic Bankart repair, with a greater loss of motion in patients who underwent open repair. Longitudinal studies have demonstrated that 40% to 50% are likely to develop arthritis after a shoulder dislocation; however, recurrent dislocation seems to be the most important factor for early development of arthritis, while age younger than 25 may be protective. Postcapsulorrhaphy arthropathy may be more associated with open repairs or those that severely limit external rotation.
Correct Answer: Age
Question 84:
The patient has weakness with elbow flexion and has numbness down the anterior lateral aspect of the forearm.
Options:
- Excessive medial placement of coracoid autograft
- Excessive lateral placement of coracoid autograft
- Excessive inferior dissection during the procedure
- Excessive retraction and dissection of the medial portion of the conjoint tendon
Correct Answer: Excessive retraction and dissection of the medial portion of the conjoint tendon
Explanation:
DISCUSSION
The Latarjet procedure was initially described in 1959 as a modification of the Bristow procedure. It has been used as a primary procedure to address instability, but is used more commonly for patients with instability and glenoid bone loss. In 2000, Burkhart and associates reported a 67% failure rate of the Bankart procedure in patients with an inverted pear-shaped glenoid (glenoid bone loss) or an engaging Hill-Sachs lesion, with a suggestion that a bone graft procedure would be optimal in this population. Complications following the Latarjet procedure have been reported as high as 25%, with the majority attributable to nerve injury, recurrent instability, and arthritis. Many of these complications are likely secondary to surgical technique. A coracoid graft that is placed too laterally or with prominent screws will overhang the glenoid and lead to early degenerative glenohumeral arthritis. A coracoid graft placed too medially can lead to recurrent instability secondary to an ineffective subscapularis sling and bone block. A coracoid graft placed inferiorly indicates dissection close to the axillary nerve, which can place tension on the axillary nerve or cause injury from direct trauma. After harvesting the coracoid graft, the surgeon must find the musculocutaneous nerve as it enters the conjoint tendon on the medial surface about 5 cm distal to the coracoid. Excessive dissection or retraction can lead to musculocutaneous nerve palsy.
Question 85:
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Options:
- She was noncompliant in physical therapy.
- The original surgery should have included resurfacing the glenoid.
- The humeral head was too large.
- The humeral component was placed too proud.
- The tuberosities are malpositioned.
Correct Answer: The tuberosities are malpositioned.
Explanation:
DISCUSSION: The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement.
REFERENCES: Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748.
Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Tanner MW, Cofield RH: Prosthetic arthroplasty for fractures and fracture-dislocations of the proximal humerus. Clin Orthop Relat Res 1983;179:116-128.
Question 86:
In X-linked hypophosphatemic rickets, the gene defect may be found in which of the following?
Options:
- GNAS1
- CLCN7
- TGF-BR2
- PHEX
- COLIA1
Correct Answer: PHEX
Explanation:
Mutations of PHEX are responsible for X-linked hypophosphatemic rickets. Mutations of CLCN7 and TC1RG1 cause osteopetrosis. COLIA1 or COLIA2 mutations cause osteogenesis imperfecta (OI) which has literally hundreds of genotypes causing a more limited number of phenotypes as described by Silence. GNAS1 is the gene mutation of fibrous dysplasia that results in an activating mutation of the GSalpha1 protein. TGF-BR2 or FBN1 cause Marfan syndrome.
Question 87:
Which of the following is helpful on physical examination to diagnose a fixed posterior shoulder dislocation? Review Topic
Options:
- Apprehension sign
- Jobe relocation test
- Sulcus sign
- Jerk test
- Lack of external rotation
Correct Answer: Lack of external rotation
Explanation:
The apprehension sign and Jobe relocation test are helpful for the diagnosis of anterior shoulder instability. The sulcus sign provides information on the status of the rotator interval. The jerk test is helpful for the diagnosis of posterior instability, but a fixed posterior shoulder dislocation is associated with loss of external rotation. Since an AP radiograph may miss this diagnosis, an axillary view should be obtained on patients with a shoulder injury.
Question 88:
A 45-year-old distance runner has a hyaluronic acid injection to his knee because of degenerative arthritis. He immediately develops a severe rash and a systemic hypersensitivity reaction. This patient most likely is also allergic to which of the following?
Options:
- Penicillin
- Sulfur
- Shellfish
- Chicken or eggs
- Lidocaine
Correct Answer: Chicken or eggs
Explanation:
DISCUSSION: Preparations of hyaluronic acid can be divided into low and high molecular weight compounds. Contraindications to intra-articular hyaluronic acid include joint or skin infection, overlying skin disease, and allergies to chicken or egg products if using a preparation derived from rooster comb.
REFERENCES: Gloyscen DN, Gillespie MJ, Schenek RC: The effects of medication in sports injuries, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopedic Sports Medicine: Principles and Practice, ed 2.
Philadelphia, PA, WB Saunders, 2003, vol 1, pp 121-124.
Schenck RC Jr: New approaches to the treatment of osteoarthritis: Oral glucosamine and chondroitin sulfate. Instr Course Lect 2000;49:491-494.
Question 89:
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
Options:
- a painful nonunion.
- asymptomatic nonunion.
- chronic elbow instability.
- tardy ulnar nerve palsy.
- cubitus varus.
Correct Answer: asymptomatic nonunion.
Explanation:
DISCUSSION: The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures.
REFERENCES: Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
Question 90:
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint? Review Topic
Options:
- Concavity compression
- Isometric articular ligaments
- Increased tensile force of the capsule
- Biceps tendon
- Deltoid contraction
Correct Answer: Concavity compression
Explanation:
Concavity compression is a stabilizing mechanism by which muscular compression of the humeral head into the glenoid fossa stabilizes the glenohumeral joint against shear forces. This is dependent on the depth of the concavity and the magnitude of the compressive force.
Question 91:
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Options:
- Rheumatoid arthritis
- Diffuse idiopathic skeletal hyperostosis (DISH)
- Normal findings
- Ankylosing spondylitis
- Osteopetrosis
Correct Answer: Ankylosing spondylitis
Explanation:
DISCUSSION: The studies show marginal syndesmophyte formation characteristic of ankylosing spondylitis. These patients typically have diffuse ossification of the disk space without large osteophyte formation. DISH typically presents with large osteophytes, referred to as nonmarginal syndesmophytes. In this patient, the zygoapophyseal joints are fused rather than degenerative as would be seen in rheumatoid arthritis, and the costovertebral joints are also fused. Osteopetrosis does not normally ankylose the disk space.
REFERENCES: McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 92:
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist?
Options:
- Ulnar head
- Volar ulnar corner
- Radial styloid
- Lister tubercle
Correct Answer: Volar ulnar corner
Explanation:
Medoff described the radiographic teardrop of the distal radius. This radiographic landmark matches the critical volar ulnar corner of the distal radius. A malreduction of the volar ulnar corner of the distal radius in an intra-articular distal radius fracture leads to volar subluxation of the lunate and the rapid development of posttraumatic arthritis at the distal radioulnar and radiolunate joints. Knowledge of the specific shape and appearance of this radiographic landmark helps the surgeon when he or she is critically analyzing postreduction imaging. The volar portion of the ulnar head may be mistaken for this teardrop sign and should be separately identified as distinct from the distal radius. The radial styloid and Lister tubercle are not part of the volar aspect of the lunate facet.
Question 93:
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Options:
- Medial plantar
- Medial calcaneal
- First branch of lateral plantar
- Lateral plantar
- Lateral calcaneal
Correct Answer: Lateral calcaneal
Explanation:
DISCUSSION: The first branch of the lateral calcaneal nerve innervates the abductor digiti minimi. It is reported to be trapped at the interval between the abductor hallucis and the quadratus plantae muscles.
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 94:
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?
Options:
- Use of cut or trimmed plates
- Use of straight (uncontoured) plates
- Use of locked plating
- Low plate placement with a prominent screw head in the distal hole
- Low antiglide plate placement
Correct Answer: Low plate placement with a prominent screw head in the distal hole
Explanation:
Low plate positioning with a prominent screw head in the most distal hole of the plate was shown to be correlated with peroneal tendon lesions. Distal plate placement in the absence of prominent screws was not associated with tendon lesions. Trimmed plates, locked plates, and uncontoured plates have not been shown to increase the risk of peroneal tendon pathology.
Question 95:
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Options:
- Follow-up in 2 weeks with a repeat white blood cell count and erythrocyte sedimentation rate
- Shoulder aspiration with Gram stain and culture of fluid
- Prescription strength nonsteroidal anti-inflammatory drugs
- Physical therapy for shoulder stretching and modalities
- Emergent surgical irrigation, debridement, and revision shoulder arthroplasty
Correct Answer: Shoulder aspiration with Gram stain and culture of fluid
Explanation:
The patient may have hematologic spread of the pulmonary infection to the shoulder arthroplasty; however, further work-up is necessary at this point. The elevated laboratory studies may still be secondary to the pulmonary infection. Aspiration of the shoulder joint with stat Gram stain and culture of the fluid is indicated. If the aspirate shows signs of infection and irrigation and debridement is indicated, complete revision of the well-seated implants may not be necessary. Physical therapy and nonsteroidal anti-inflammatory drugs are not indicated until the possibility of a shoulder infection has been ruled out. A wait of 2 weeks to repeat the laboratory values, in the presence of new shoulder pain, is contraindicated.
Question 96:
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of
Options:
- an occult fracture of the tibial plateau.
- a tear of the medial collateral ligament and the posteromedial capsule.
- a tear of the posterior cruciate ligament.
- a tear of the anterior and posterior cruciate ligaments.
- a tear of the anterior cruciate and medial collateral ligaments and the posteromedial capsule.
Correct Answer: a tear of the anterior cruciate and medial collateral ligaments and the posteromedial capsule.
Explanation:
DISCUSSION: The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal.
REFERENCES: Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Indelicato PA: Injury to the medial capsuloligamentous complex of the knee, in Feagin J (ed): The Crucial Ligaments, ed 2. 1994, pp 351-360.
Question 97:
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Options:
- surface irrigation, sterile dressing, and a short leg cast.
- surface irrigation, sterile dressing, a short leg cast, and oral antibiotics.
- surface irrigation, sterile dressing, a short leg cast, and IV antibiotics.
- surgical debridement, a short leg cast, and IV antibiotics.
- surgical debridement, external or internal fixation, and IV antibiotics.
Correct Answer: surgical debridement, external or internal fixation, and IV antibiotics.
Explanation:
DISCUSSION: The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean.
REFERENCES: Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res
2003;408:86-91.
Bartlett CS, Helfet DL, Hausman MR, et al: Ballistics and gunshot wounds: Effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000;8:21-36.
Question 98:
The Lisfranc ligament connects the base of the
Options:
- first metatarsal and the medial cuneiform.
- first metatarsal and the base of the second metatarsal.
- first metatarsal and the middle cuneiform.
- second metatarsal and the medial cuneiform.
- second metatarsal and the middle cuneiform.
Correct Answer: second metatarsal and the medial cuneiform.
Explanation:
DISCUSSION: The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments.
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 99:
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Options:
- early mobilization only.
- surgical reconstruction of medial and lateral collateral ligaments.
- active motion in a hinged brace from 30° to 120°.
- application of hinged external fixator with early mobilization.
Correct Answer: early mobilization only.
Explanation:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
Question 100:
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Options:
- 9 degrees internal rotation
- 14 degrees external rotation
- 18 degrees internal rotation
Correct Answer: 9 degrees internal rotation
Explanation:
All of the above
Corrent answer: 4
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±