Orthopedic Board Prep MCQs: Joints, Fractures & Arthroscopy | Part 122

Key Takeaway
This page offers Part 122 of a comprehensive OITE & AAOS Orthopedic Board Review. It features 100 high-yield, verified MCQs, mirroring actual exam formats. Designed for orthopedic residents and surgeons, this interactive quiz helps master topics like Arthroscopy, Elbow, Fracture, and Hip for certification success.
About This Board Review Set
This is Part 122 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 122
This module focuses heavily on: Arthroscopy, Elbow, Fracture, Hip.
Sample Questions from This Set
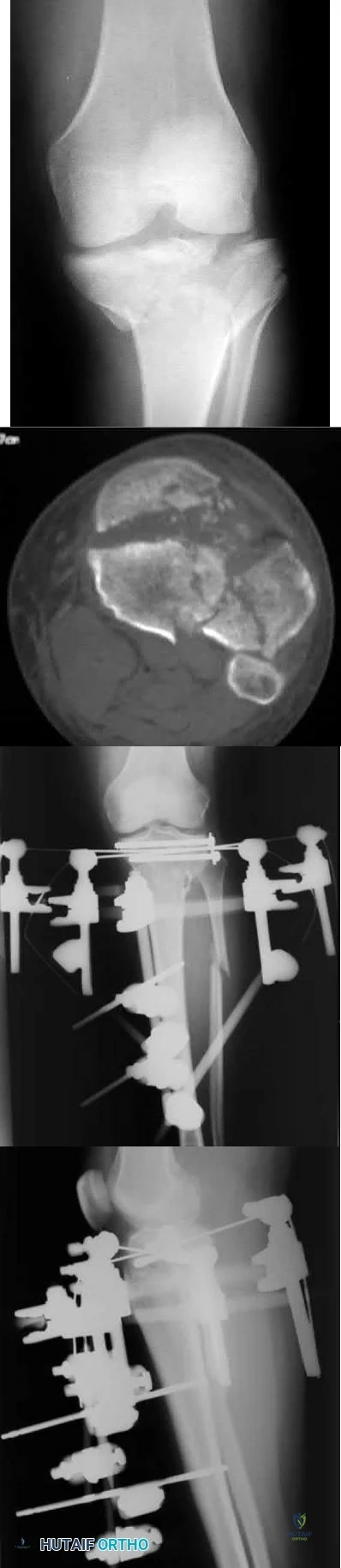
Sample Question 1: Mutations of what gene are associated with subsequent development of osteosarcoma?...
Sample Question 2: Which of the following bones is most frequently involved in stress fractures in athletes? Review Topic...
Sample Question 3: The most appropriate next surgical procedure is...
Sample Question 4: Which of the following is considered a contraindication to elbow arthroscopy? Review Topic...
Sample Question 5: A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs....
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4.
Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Hovig E, Lothe R, Farrants G, et al: Chromosome thirteen alterations in osteosarcoma cell lines derived from a patient with previous retinoblastoma. Cancer Genet Cytogenet 1991;57:31-40.
Question 2
Which of the following bones is most frequently involved in stress fractures in athletes? Review Topic
Explanation
Question 3
The most appropriate next surgical procedure is
Explanation
This patient’s arthritis likely has progressed to the lateral compartment. The location and degree of local pain and tenderness are the most important physical findings. History and physical findings indicate arthritis progression to the lateral and anterior compartments. This scenario suggests the need for conversion of the unicompartmental arthroplasty to TKA.

Question 4
Which of the following is considered a contraindication to elbow arthroscopy? Review Topic
Explanation
Question 5
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 6
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?
Explanation
REFERENCES: Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45.
Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Lins RE, Simovitch RW, Waters PM: Pediatric elbow trauma. Orthop Clin North Am 1999;30:119-132.
Question 7
In total hip arthroplasty, increasing the perpendicular distance from the center line of the femur to the center of rotation of the femoral head (femoral offset) results in
Explanation
include an increased range of motion, better mechanical advantage for the abductors and decreased instability because of better soft tissue tension. According to Charnley,
increasing the femoral offset should improve the abductor lever arm which should decrease the abductor force required for walking, and therefore decrease the energy requirement for gait as well as the overall joint reactive force. The largest possible disadvantage of increasing the femoral offset is increasing the out of plane bending moment which puts stress on the prosthetic stem. Poly wear is a direct effect of surface area contact which is not changed with femoral Offset.
Question 8
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Torg J, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-712.
Question 9
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 10
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.
Question 11
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
REFERENCES: Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Dias LS: Surgical management of acquired foot and ankle deformities, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 161-170.
Question 12
-A 42-year-old patient with a right distal radius fracture underwent open reduction and internal fixation. To reduce the likelihood of complex regional pain syndrome, the most appropriate medication is
Explanation

Question 13
Radiotherapy for palliative pain control as the risk for pathological fracture is very small
Explanation
some centers, this procedure may contaminate the entire bone with tumor and make limb salvage nearly impossible if this is a sarcoma. If the incisional biopsy shows carcinoma, then intramedullary nailing with adjuvant radiotherapy would be completely appropriate.
Question 14
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Explanation
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.

CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 15
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
Explanation

OrthoCash 2020
Question 16
A 14-year-old football player has had thigh pain and weakness following a full-contact scrimmage 24 hours ago. He recalls that he felt a sharp pain in his back after colliding with a much heavier player. Examination reveals that the spine is minimally tender to palpation in the upper lumbar region. Motor testing reveals quadriceps weakness bilaterally, and a reverse straight leg raising test is positive. Plain radiographs of the thoracolumbar spine are normal. A myelogram, a CT scan with contrast, and an MRI scan are shown in Figures 41a through 41c. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
Epstein NE, Epstein JA, Mauri T: Treatment of fractures of the vertebral limbus and spinal stenosis in five adolescents and five adults. Neurosurgery 1989;24:595-604.
Question 17
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 18
What is the most common physical finding in myelopathic patients? Review Topic
Explanation
Question 19
5 degrees medial and 10 degrees cephalad
Explanation
Question 20
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
REFERENCES: Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242.
Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Veltri DM, Xeng XH, Torzilli PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 21
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
REFERENCES: Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont IL, American Academy of Orthopaedic Surgeons, 2002, pp 489-511.
Question 22
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 23
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
REFERENCES: Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119.
Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362.
Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 24
A 69-year-old female sustains the injuries seen in Figures A and
Explanation
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
Question 25
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
REFERENCES: Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394.
Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Weil WM, Trumble TE: Treatment of distal radius fractures with intrafocal (Kapandji) pinning and supplemental skeletal stabilization. Hand Clin 2005;21:317-328.
Question 26
A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile. Management at this time should consist of
Explanation
Question 27
7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Explanation
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
Longer operative times
Increased deep surgical infection rates
Unacceptably high malunion/nonunion rates
Slower early return to function
Longer hospital stays Corrent answer: 3
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
OrthoCash 2020
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?

Posterior approach
Anterior approach
Anterolateral approach
Use of a bipolar implant
Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?

Exchange humeral nailing
Augmentative plating
Nail removal with open reduction compression plating
Smoking cessation and medical optimization
Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
OrthoCash 2020
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
Technique depicted in Figure B is associated with an increased risk of septic arthritis
Technique depicted in Figure B is associated with increased rate of anterior knee pain
Technique depicted in Figure B is associated with improved postoperative fracture alignment
Technique depicted in Figure C is associated with an increased risk of septic arthritis
Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
OrthoCash 2020
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?

Nerve compression; open reduction internal fixation with open carpal tunnel release
Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
Decreased arterial inflow; fasciotomy with open reduction internal fixation
Reflex sympathetic dystrophy; vitamin C
Nerve compression; repeat closed reduction Corrent answer: 1
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
OrthoCash 2020
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?

Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
No difference in radiographic outcomes after ORIF vs. closed treatment
No difference in functional outcomes after ORIF vs. closed treatment
Improved functional outcomes with closed treatment vs. ORIF
Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
no difference in functional outcomes between operative and closed treatment modalities for DRF.
OrthoCash 2020
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?

Continued sling immobilization
Closed reduction percutaneous pinning
Open reduction internal fixation
Hemiarthroplasty
Reverse total shoulder arthroplasty Corrent answer: 3
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:

OrthoCash 2020
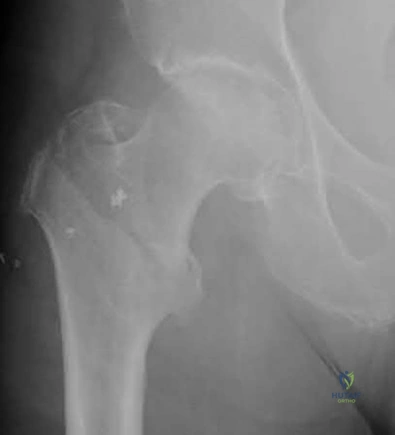
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?

MCL > LCL > anterior capsule
MCL > anterior capsule > LCL
anterior capsule > MCL > LCL
LCL > anterior capsule > MCL
LCL > MCL > anterior capsule Corrent answer: 4
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
OrthoCash 2020
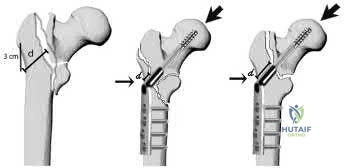
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
Reverse obliquity fracture pattern
Lateral wall thickness
Previous contralateral hip fracture
DEXA T-score <-2.0
Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
OrthoCash 2020
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?

Smaller lateral wall thickness favors sliding hip screw constructs
Unstable fractures are best treated with sliding hip screw constructs
Avoiding distal locking screws in intramedullary implants protects against refracture
Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
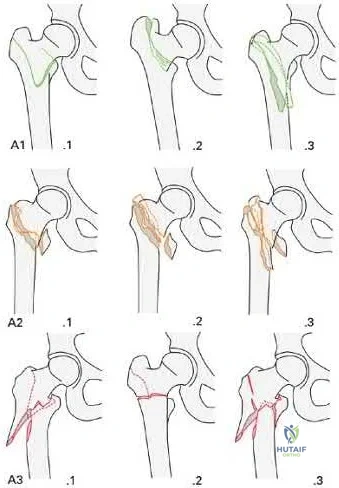
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
OrthoCash 2020
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference <20 mm/hr) and 0.9 mg/L (reference <2.5 mg/L), respectively. Figures A and B are the AP and lateral radiographs of the left femur. Which treatment option offers the highest chance of union and enables immediate weight-bearing?

Nail removal with compression plating and open bone grafting
Closed reamed exchange nailing
Nail dynamization
Nail retention with plate augmentation and bone grafting
Electrical bone stimulator Corrent answer: 4
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:

OrthoCash 2020
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?

External fixation with serial doppler examinations
Intramedullary nailing
Open reduction internal fixation using plates and screws
Immediate 2-compartment fasciotomies and external fixation
Immediate 4-compartment fasciotomies and external fixation Corrent answer: 5
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p) <30 mmHg may help to confirm the necessity for fasciotomy.
McQueen et al. published a report of 25 patients with tibial diaphyseal fractures which had been complicated by an acute compartment syndrome. They reported significant differences in any sequelae of acute compartment syndrome between patients who underwent compartment pressure monitoring and those who had not. They recommended that all patients with tibial fractures should have continuous compartment monitoring to minimize the incidence of acute compartment syndrome.
Mawhinney et al. reported on three cases of tibial compartment syndrome after closed intramedullary nailing of the tibia. They reported that the only predisposing factors for the development of compartment syndrome were the surgery and the fracture itself. They concluded that tibial compartment syndrome is a relatively rare but significant complication of tibial nailing.
Figure A is an AP and lateral radiograph of the leg with displaced, comminuted middle third tibia and fibula fractures.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Decreased arterial inflow; inability to dorsiflex his ankle
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:

OrthoCash 2020
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
Syme
Traumatic transtibial
Vascular transtibial
Traumatic transfemoral
Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
OrthoCash 2020
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?

It may be performed in a minimally invasive manner
It involves minimal soft tissue stripping
It leads to higher union rates
It allows the surgeon to address all sites of injury through one approach
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:

OrthoCash 2020
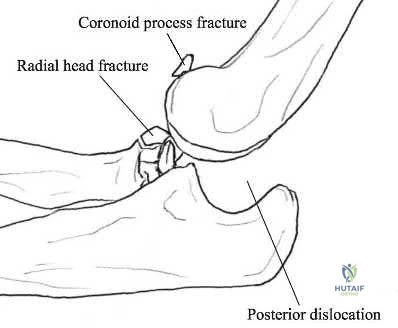
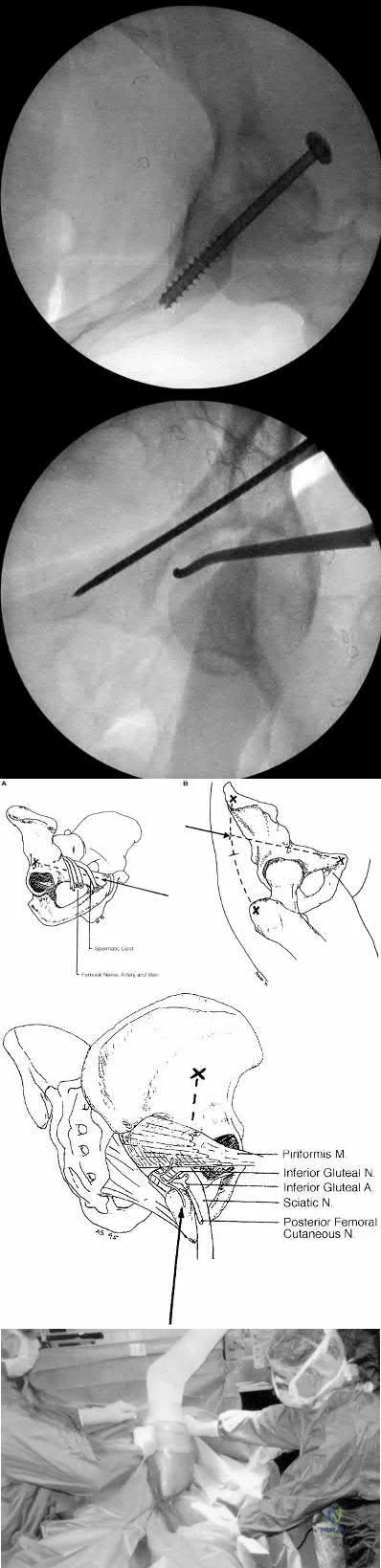
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
Iliac oblique view with hip and knee flexed
Iliac oblique inlet view
Obturator oblique view with hip and knee flexed
Obturator oblique outlet view
Obturator oblique inlet view Corrent answer: 2
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
OrthoCash 2020
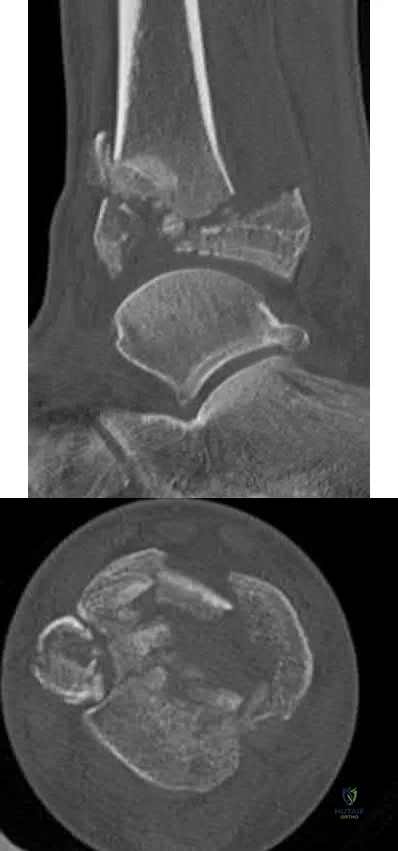
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
TGF-Beta
RANKL
IL-2
IL-6
cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
immune system.
OrthoCash 2020
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
Ulnar styloid nonunion
DRUJ instability
Articular step-off >3mm
Radial shortening
Workers compensation claim Corrent answer: 1
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
OrthoCash 2020
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?

Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including <8mm of calcar length attached to the articular segment, disruption of the medial hinge, displacement >10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of <8mm attached to the articular segment. Figure D is a displaced metadiaphyseal proximal humerus fracture in a skeletally immature patient. Figure E is a radiograph of a metadiaphyseal proximal humerus fracture in a skeletally mature patient with a medial calcar length >8mm.
Incorrect Answers:
OrthoCash 2020
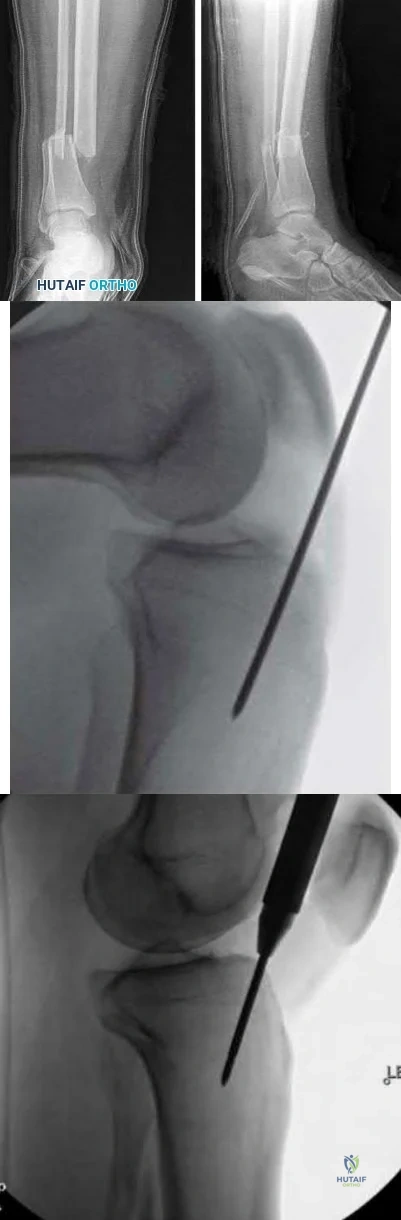
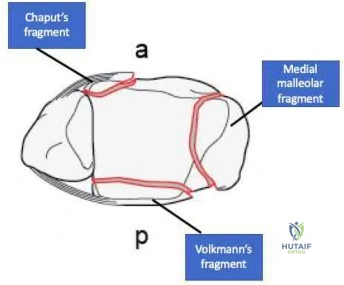
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?

Nondisplaced medial malleolus vertical shear fracture
Nondisplaced Volkmann's fragment
Nondisplaced Chaput's fragment
Nondisplaced lateral wall talar fracture
Posterior inferior tibiofibular ligament disruption Corrent answer: 2
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
OrthoCash 2020
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
Age < 20
Male gender
Body mass index >/ 30 kg/m^2
Open fracture
Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?

Greater Mayo Elbow Performance Score
Greater Disabilities of the Arm, Shoulder and Hand Score
Increased flexion-extension arc
Increased reoperation rate
Decreased complication rate Corrent answer: 4
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:

OrthoCash 2020
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?

Anterior perforation of distal femur
Breakage of the screw
Implant cutout
Malunion
Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:

OrthoCash 2020
Figure A is the radiograph of a 42-year-old female who presents to the trauma bay following a motor vehicle collision. She subsequently undergoes ORIF through a posterior approach. Iatrogenic injury to which nerve in Figure B is most likely with this approach?
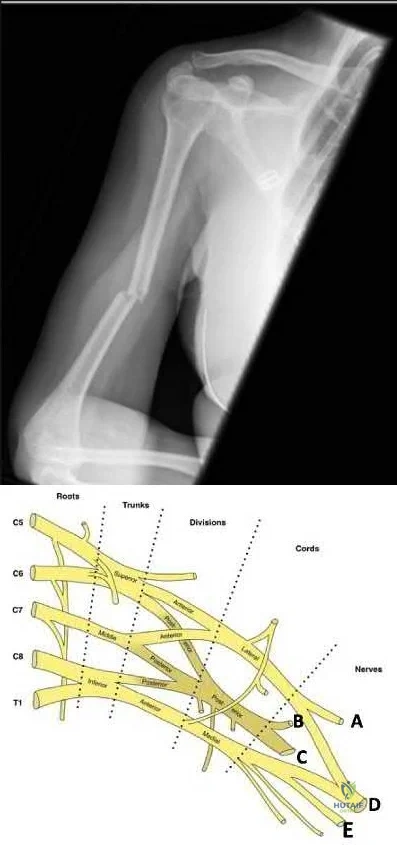
Question 28
Communication breakdown is the leading cause of which of the following?
Explanation
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Question 29
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
Explanation
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22- mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Question 30
During the cocking and acceleration phases of the overhand throw (pitch), there are several static and dynamic restraints to provide medial elbow support and prevent valgus instability. The dynamic structures found to be most important during these phases of the overhand throw are the flexor digitorum Review Topic
Explanation
Question 31
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 32
A 56-year-old woman underwent a total knee arthroplasty 2 years ago and now has pain and swelling. Radiographs of her knee are unremarkable. Her C-reactive protein (CRP) level is 3.0 (reference range [rr], 0.08–3.1 mg/L), and her erythrocyte sedimentation rate (ESR) is 18 mm/h (rr, 0-20 mm/h). Aspiration of the knee reveals a white blood cell (WBC) count of 1200/mm3 with a differential of 30% neutrophils and 70% monocytes. Cultures will not be available for several days, and the patient has not been taking antibiotics. Based on these findings, the most appropriate next step is
Explanation
ESR and CRP level are recommended as starting points in the workup for the diagnosis or exclusion of periprosthetic joint infection (PJI). When both the ESR and CRP findings are within defined limits, PJI is unlikely. When both test findings are positive, PJI must be considered and further investigation is warranted. Clinicians need to be aware of other inflammatory conditions such as rheumatoid arthritis that can lead to elevation of inflammatory markers.
A high likelihood of infection is noted when the knee aspirate contains more than 2500 WBCs per high-powered field (HPF) with a differential count exceeding 60% neutrophils. Using these criteria, Mason demonstrated a sensitivity of 98% and a specificity of 95% for infection diagnosis.
For this patient, the inflammatory markers are within normal limits. The aspiration result is below 2500 WBC/HPF with a low percentage of neutrophils. The likelihood of infection is remote, and further nonsurgical treatment should not include antibiotics. There is no indication for surgery based upon the information presented.

Question 33
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 34
A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
Explanation
Question 35
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
REFERENCES: Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Nora FE, Dahlin DC, Beabout JW: Bizarre parosteal osteochondromatous proliferations of the hands and feet. Am J Surg Pathol 1983;7:245-250.
Question 36
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 37
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
REFERENCE: Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 38
A 16-year-old female with adolescent idiopathic scoliosis undergoes posterior spinal fusion with instrumentation. The thoracic pedicle screws were placed using a tap 1 mm smaller than the screw diameter and a straightforward trajectory that runs parallel to the superior endplate. This techniques allows for which of the following: Review Topic
Explanation
Contemporary segmental pedicle screw placement used in the treatment of scoliosis deformity offer significantly higher screw pullout and deformity correction than prior hook and wire constructs. Additionally, screw insertional torque has been found in numerous studies to correlate with resistance to screw pullout. Several factors have been found to increase maximum screw insertional torque, including tapping 1mm smaller than the screw diameter and using the straightforward trajectory. It is important to note that while undertapping makes for a stronger screw, there are some studies that suggest not tapping at all makes for an even stronger screw.
Lehman et al. performed a biomechanical study evaluating maximum insertional torque when tapping line to line, undertapping by 0.5mm, and undertapping by 1mm in 34 fresh frozen cadavers. They found undertapping the thoracic pedicle by 1mm increased maximum insertional torque by 47% when compared to undertapping by 0.5mm and by 93% when compared to line to line tapping.
Kuklo et al. performed a biomechanical study on thirty cadavers using the straightforward technique (sagittal trajectory of the screws parallels the superior endplate of the vertebral body) versus anatomic trajectory (22 degrees in the cephalo-caudad direction in the sagittal plane). They found maximum insertional torque to be
Question 39
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 40
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
Question 41
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment? Review Topic

Explanation
Question 42
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 43
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm 3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?
Explanation
REFERENCES: McCarthy JJ, Dormans JP, Kozin SH, et al: Musculoskeletal infections in children: Basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-528.
Calhoun JH, Manring MM: Adult osteomyelitis. Infect Dis Clin North Am 2005;19:765-786.
Question 44
Figure 24 shows the radiograph of a 36-year-old volleyball player with right hip pain. What is the cause of the pain?
Explanation
REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
Question 45
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of
Explanation
REFERENCES: Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
Question 46
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 47
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
REFERENCES: Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 48
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
Explanation
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 49
- Which of the following shoulder girdle muscles is most active during forward flexion?
Explanation
Question 50
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 51
What clinical scenario is most consistent with the MR image of the L4-L5 disk level shown in Figure 14? Review Topic
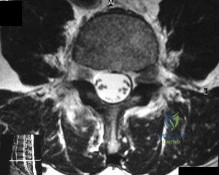
Explanation
Question 52
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 53
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 54
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 55
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
REFERENCES: Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 56
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Explanation
REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 57
What is the primary role of superficial zone protein (SZP) in articular cartilage?
Explanation
REFERENCES: Hlavacek M: The influence of the acetabular labrum seal, intact articular superficial zone and synovial fluid thixotropy on squeeze-film lubrication of a spherical synovial joint. J Biomech 2002;35:1325-1335.
Jay GD, Tantravahi U, Britt DE, et al: Homology of lubricin and superficial zone protein (SZP): Products of megakaryocyte stimulating factor (MSF) gene expression by human synovial fibroblasts and articular chondrocytes localized to chromosome 1q25. J Orthop Res 2001;19:677-687.
Question 58
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 59
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer’s representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture’s representative suggests a partnership in a boat costing $200,000. The manufacture’s representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest.
Question 60
The lesion seen in Figure 4 is most likely the result of metastases from what solid organ?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Leeson MC, Makley JT, Carter JR: Metastatic skeletal disease distal to the elbow and knee. Clin Orthop 1986;206:94-99.
Question 61
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Dillin L, Hoaglund FT, Scheck M: Brachial neuritis. J Bone Joint Surg Am 1985;67:878-880.
Question 62
What is the primary mechanism of degradation of calcium phosphate cement?
Explanation
To treat depressed tibial plateau fractures, surgeons must elevate the depressed segments, which results in a metaphyseal bone void. This void can be filled with multiple materials, including autograft and allograft bone. The addition of BMP-2 or BMP-7 is not recommended to fill contained bone defects. These materials are indicated for application between bone and soft tissue and they do not provide the volume or strength to fill closed defects. Calcium phosphates have been use to fill these voids, demonstrating improved strength and resistance to subsidence when compared to autograft. Although polymethylmethacrylate is commonly used to fill bone voids in patients with cancer, it is not preferred in the setting of acute fracture because of the exothermic reaction that may compromise local bone healing. Although hydroxyapatite may be degraded by macrophage and giant-cell-mediated processes, the calcium phosphate degrades mainly by an osteoclast-mediated method. The calcium phosphate is not soluble in interstitial fluid, so simple dissolution does not occur.
RECOMMENDED READINGS
Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J Bone Joint Surg Am. 2008 Jun;90(6):1186-
Question 63
A 26-year-old mixed martial arts fighter sustains a posterolateral elbow dislocation. The primary stabilizers of the elbow joint are the
Explanation
extensor origins, and the joint capsule. The muscles that cross the elbow joint act as dynamic stabilizers.
Question 64
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?
Explanation
REFERENCES: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Simon MA, Karluk MB: Skeletal metastases of unknown origin: Diagnostic strategy for orthopedic surgeons. Clin Orthop Relat Res 1982;166:96-103.
Question 65
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
REFERENCES: Blazina ME, et al: Jumper’s knee. Orthop Clin North Am 1973;4:665.
Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper’s knee. Am J Sports Med 1984;12:375-380.
Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Rows J, et al: Patella tendinitis (jumper’s knees). Am J Sports Med 1978;6:362.
Question 66
A 24-year-old woman is thrown from her motorcycle and sustains the closed injury shown in Figures A through C. Open reduction and internal fixation is planned. What surgical technique will best allow visualization of the joint surface and allow early range of motion?

Explanation
Bicolumnar fixation of distal humerus fractures should follow the principles outlined by O'Driscoll: Distal fragments should be held by as many screws as possible; every screw in the distal fragments should pass through a plate; each screw should engage as many articular fragments as possible.
Galano et al. review treatment for bicolumnar distal humerus fractures. They note that the olecranon osteotomy, Alonso-Llames triceps sparing and Campbell triceps splitting approaches expose 57%, 46% and 35% of the articular surface, respectively. The OO and paratricipital (triceps sparing) approaches allow for early ROM. Protected motion is required for the O'Driscoll TRAP and Bryan-Morrey approaches for tendon-to-bone healing.
Coles et al. retrospectively reviewed the OO in fixation of 70 fractures. Osteotomy fixation was with an intramedullary screw and dorsal ulnar wiring, or with a plate.
The rate of OO increased with fracture difficulty (from AO type C1-C3). There was 1 delayed union but no nonunions.
Figures A and B show a AO/OTA type C2 intraarticular distal humerus fracture. Figure C is a coronal CT scan showing intraarticular comminution. Illustration A shows fixation of the fracture with bicolumnar plating through an olecranon osteotomy approach. Illustration B shows the various approaches to the distal humerus (left, Campbell triceps splitting; center left, O'Driscoll triceps reflecting anconeus pedicle; center right, Bryan-Morrey approach, leaving the triceps attached laterally to the fasciocutaneous flap, but elevating it off the ulna; right, olecranon osteotomy). Illustration C shows 3 methods of olecranon osteotomy (A and B, Intraarticular transverse; C-F, Extra-articular oblique; G, Intra-articular chevron).
Incorrect Answers:
(SBQ12TR.84) Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage? Review Topic

Chronic suppressive, culture-directed, antibiotic therapy
Above knee amputation
Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical
debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
Question 67
Figure 48 shows a current lateral radiograph of a 23-year-old man who sustained a closed femoral diaphyseal fracture 5 months ago. Treatment consisted of placement of a retrograde femoral nail for the femoral fracture. The patient now reports a sudden onset of pain in the midthigh and cannot bear weight on his leg. Management should consist of

Explanation
In Webb, et al. one hundred five consecutive patients with a diagnosis of delayed union (61 patients) or nonunion (44 patients) of the femoral shaft from February 1968 to November 1983 were managed by intramedullary reaming and nailing. The procedure was accomplished by closed techniques in 82 of the cases. Adequate follow-up study was obtained in 101 patients; all but four showed clinical and radiologic union at an average of 20 weeks following the procedure, with an overall union rate of 96%. The four patients whose fractures failed to consolidate with this treatment had repeat procedures with placement of thicker nails, and all subsequently healed.
The fracture pictured for this question is an oblique, distal 1/3 diaphyseal femur fracture with a butterfly fragment, an axially and rotationally unstable fracture configuration. The clinical history and x-ray are consistent with delayed union, therefore response #4 is the only sensible management option.
Question 68
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
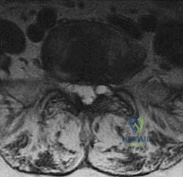
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
Question 69
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. Stress radiographs show a 2-mm medial physeal widening with valgus stress. What is the best initial treatment strategy for this patient?
Explanation
Question 70
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
REFERENCES: Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 71
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
REFERENCES: Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 1146-1167.
Question 72
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
REFERENCES: Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Bansal P, Deehan DJ, Gregory RJ: Diagnosing the acutely locked knee. Injury 2002;33:495-498.
Question 73
What is the most common primary malignant bone or cartilage tumor in children?
Explanation
1 million children younger than age 15 years), and Ewing’s sarcoma is second (2.1 per
1 million children). Giant cell tumor and chondrosarcoma are rare in children. Osteochondroma is more common than any of the above tumors in children, but it is not malignant.
REFERENCES: Himelstein BP, Dormans JP: Malignant bone tumors of childhood. Pediatr Clin North Am 1996;43:967-984.
Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma, Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001;21:412-418.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence.
N Engl J Med 1999;341:342-352.
Question 74
4A 4B 4C A 30-year-old man was involved in a high-speed motorcycle collision and sustained the injury shown in Figure 4a. Hypotension ensued shortly after arrival in the emergency department. Figure 4b is the initial contrast pelvic CT image with an unrecognized blush consistent with arterial bleeding. During surgical repair, the patient was noted to have active bleeding and an angiogram was obtained (Figure 4c). Which structure is the likely cause of his bleeding?
Explanation
Pelvic bleeding occurs predominantly from disruption of the posterior venous plexus and bleeding from the fractured bone. Occasionally arterial bleeding is seen, with injury to the superior gluteal artery most common. Anterior pelvic bleeding occurs from injury to the obturator artery (commonly from a pubic bone fracture laceration) and less frequently from the pudendal artery near the symphysis. The location of the bleeding on CT and angiography images does not correspond to the superior gluteal, external iliac, or femoral arteries.
RECOMMENDED READINGS
Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. 2009 Apr;40(4):343-53. Epub 2009 Mar 17. Review.PubMed PMID: 19278678. View Abstract at PubMed
Loffroy R, Yeguiayan JM, Guiu B, Cercueil JP, Krausé D. Stable fracture of the pubic rami: a rare cause of life-threatening bleeding from the inferior epigastric artery managed with transcatheter embolization. CJEM. 2008 Jul;10(4):392-5. PubMed PMID: 18652733. View Abstract at PubMed
White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures.Injury. 2009 Oct;40(10):1023-30. Epub 2009 Apr 16. Review. PubMed PMID:19371871. View Abstract at PubMed
RESPONSES FOR QUESTIONS 5 THROUGH 8

5A

5B
- Avascular necrosis, head collapse, and screw penetration
- Fixation failure and varus collapse
- Humeral stem loosening
- Glenoid component loosening
- Hardware failure (breakage of plate or screws)
- Shoulder dislocation
Please choose from the responses to identify the most likely complication in each scenario.
Question 75
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 76
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Beredjiklian PK, Nalbantoglu U, Potter HG, et al: Prosthetic radial head components and proximal radial morphology: A mismatch. J Shoulder Elbow Surg 1999;8:471-475.
Question 77
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?
Explanation
REFERENCE: Buckwalker JA, Einhorn TA, Simon SR (ed): Orthopedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 182-215.
Question 78
Treatment should include
Explanation
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.

Question 79
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
REFERENCES: Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand
2004;75:309-314.
Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Leniz P, Ripalda P, Forriol F: The incorporation of different sorts of cancellous bone graft and the reaction of the host bone: A histomorphometric study in sheep. Int Orthop 2004;28:2-6.
Question 80
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
REFERENCE: Mulvey TJ, Thornhill TS: Infected total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2,
pp 1857-1890.
Question 81
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
REFERENCE: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 82
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 83
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193.
Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Fiore AJ, Haid RW, Rodts GE, et al: Atlantal lateral mass screws for posterior spinal reconstruction: Technical note and case series. Neurosurg Focus 2002;12:E5.
Question 84
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 85
Chondrosarcoma The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
Slide 5 Slide 6
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. A needle biopsy is also performed (Slides 5 and 6). Which of the following treatment regimens would be the most appropriate:
Question 86
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves? Review Topic
Explanation
(SBQ12TR.106) A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?

Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
A delay in surgery greater than 48 hours is recommended if the patient has multiple medical comorbiditiesm which are not fully optimized
Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months. Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of
early surgery on incidence of AVN. However, delay of internal fixation of more than
24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Question 87
The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intrasurgically, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation

Video 67 for reference
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown.
The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. An ultrasound may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasound is not commonly used to diagnose labral pathology.
Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 88
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 89
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 90
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 91
A 19-year-old woman has had a painful prominence on the lateral border of her fifth metatarsal head since she was a young girl. Nonsurgical management, including the use of a wide toe box shoe, has failed to provide relief. Examination reveals a callus over the lateral prominence and on the plantar portion as well. A clinical photograph and a radiograph are shown in Figures 34a and 34b. Treatment should consist of
Explanation
REFERENCES: Shereff MJ, Yang QM, Kummer FJ, Frey CC, Greenidge N: Vascular anatomy of the fifth metatarsal. Foot Ankle 1991;11:350-353.
Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term follow-up. Foot Ankle 1991;11:345-349.
Question 92
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
Explanation
this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
Question 93
-The Coleman block test is used to test for
Explanation

Question 94
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701.
Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg
1997;5:240-248.
Bundschuh C, Modic MT, Kearney F, et al: Rheumatoid arthritis of the cervical spine: Surface-coil MR imaging. Am J Roentgenol 1988;151:181-187.
Question 95
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
REFERENCES: Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706.
Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49.
Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am
2002;84:250-255.
Templeton JE, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC: Revision of a cemented acetabular component to a cementless acetabular component. A ten- to fourteen-year follow-up study. J Bone Joint Surg Am 2001;83:1706-1711.
Question 96
The spread of malignant cells to the vertebrae is often through
Explanation
REFERENCE: Batson OV: The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-149.
Question 97
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?
Explanation
REFERENCE: Millis MB, Murphy SB, Poss R: Osteotomies about the hip for the prevention and treatment of osteoarthritis. Instr Course Lect 1996;45:209-226.
Question 98
Which 2 tendons are identified in the dissection shown in Video 92?
Explanation
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 99
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 100
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
