Orthopedic Board Review MCQs: Upper Extremity & Trauma | Part 120

Key Takeaway
This page offers Part 120 of a comprehensive orthopedic board review series by Dr. Mohammed Hutaif. It features 100 high-yield MCQs on Elbow, Fracture, Shoulder, Wrist, mirroring OITE/AAOS exam formats. Designed for orthopedic residents and surgeons preparing for board certification exams.
About This Board Review Set
This is Part 120 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 120
This module focuses heavily on: Elbow, Fracture, Shoulder, Wrist.
Sample Questions from This Set
Sample Question 1: Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 de...
Sample Question 2: Which of the following structures may help maintain radial length after a radial head fracture?...
Sample Question 3: Which of the following anatomic structures is labeled 6 in Figure 27?...
Sample Question 4: A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?...
Sample Question 5: A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nons...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 2
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
REFERENCES: Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 3
Which of the following anatomic structures is labeled 6 in Figure 27?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 309.
Question 4
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
REFERENCES: Cheng CY, Shih HN, Hsu KY, et al: Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res 2001;383:221-228.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 263-284.
Question 5
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of
Explanation
REFERENCE: Peterson CA, Altchek DW, Warren RF: Shoulder arthroscopy, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 290-335.
Question 6
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 7
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of
Explanation
REFERENCES: Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Warren SB, Brooker AF Jr: Excision of heterotopic bone followed by irradiation after total hip arthroplasty. J Bone Joint Surg Am 1992;74:201-210.
Question 8
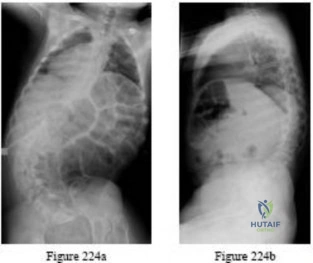
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of
Explanation
REFERENCE: Pauli RM, Breed A, Horton VK, Glinski LP, Reiser CA: Prevention of fixed angular kyphosis in achondroplasia. J Pediatr Orthop 1997;17:726-733.
Question 9
A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 10
- Analysis of which of the following proteins is used to establish the diagnosis of Becker muscular dystrophy?
Explanation
A 25-year-old woman with spastic diplegia has a painful progressive bunion deformity that has failed to respond to nonsurgical treatment. Examination reveals tenderness and erythema over the bunion prominence; however, the hallux metatarsophalangeal joint has full range of motion. A standing AP radiograph shows a hallux valgus angle of 30 degrees and a 1-2 intermetatarsal angle of 13 degrees. Treatment should now consist of
arthrodesis of the hallux metatarsophalangeal joint.
arthrodesis of the first tarsometatarsal joint.
excision of the medial eminence and medial capsular reefing of the metatarsophalangeal joint.
osteotomy of the distal first metatarsal.
proximal metatarsal osteotomy with distal soft-tissue realignment.
Treatment of hallux valgus in a patient with cerebral palsy is largely dependent on the degree of spasticity and the pattern of gait. The only way to adequately eliminate spastic deforming forces is with an arthrodesis of the MTP joint. Any other procedure will most likely lead to a high incidence of either hallux varus or recurrent hallux valgus.
The optimal arthrodesis angle is 25-30 degrees, and the metatarsal inclination angle should be 25-30 degrees also. Sagittal plane position should be checked intraoperatively and the proximal phalanx should clear the table by 5-10mm with simulated WB
Question 11
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation

Question 12
Which of the following is considered a major characteristic of hyaluronate?
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78.
Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Hurd ER: Extraarticular manifestations of rheumatoid arthritis. Semin Arthritis Rheum 1979;8:151-176.
Question 13
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?
Explanation
Question 14
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 15
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 16
Which of the following best characterizes bone mineralization?
Explanation
REFERENCES: Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Gehron RP, Boskey AL: The biochemistry of bone, in Marcus R, Feldman D, Kelsey J (eds): Osteoporosis. San Diego, CA, Academic Press, 1996, pp 95-184.
Question 17
Figure 1 is the radiograph of an 18-year-old, right hand-dominant man who has right side thumb pain after a tackle during a rugby game. Examination shows ecchymosis and swelling of the right thumb along with tenderness to palpation about the thumb CMC joint and metacarpal base. What ligament is holding the small fracture fragment in anatomical location to the trapezium?

Explanation
Bennett fractures are defined as intra-articular thumb metacarpal base fractures. The fracture is often caused by axial loading, and concomitant injuries to the thumb MCP joint and trapezium are common. The palmar ulnar aspect of the base of the metacarpal stays in place through its attachment to the trapezium by way of the anterior oblique ligament. The metacarpal shaft is displaced dorsally, proximally, and radially by the pull of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and adductor pollicis brevis. These fractures are often considered unstable and are treated surgically.
Question 18
A football player injures his knee when he is tackled and falls awkwardly. He does not note any discreet “pop,” but pain prevents him from returning to the game. An effusion is noted the following day and an MRI scan is ordered. Selected images are shown in Figures 1 through 3. Based on these images, physical examination findings likely include

Explanation
Question 19
Two major pharmacologic classes of bisphosphonates exist: nitrogen-containing and non-nitrogen-containing compounds. The nitrogen-containing compounds work by which of the following actions?
Explanation
Question 20
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
Explanation
REFERENCES: Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863.
Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 21
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed? Review Topic
Explanation
Question 22
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 23
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of
Explanation
REFERENCES: American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154.
Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Question 24
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 25
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
Explanation

Video 1 for reference
For severe tibial defects (Anderson Orthopaedic Research Institute [AORI] types 2 and 3), metaphyseal fixation is necessary to achieve construct fixation during revision TKA. Metaphyseal fixation may be achieved with cement, structural allograft, or conical metallic implants. The major concerns regarding structural allograft are graft resorption and mechanical failure and technical issues related to fashioning the graft and obtaining a good host-allograft interface. In a systematic review, porous metal cones were associated with a decreased loosening rate in AORI 2 and 3 defects compared to structural allografts. Metallic trabecular metal cones and metaphyseal porous coated sleeves provide a stable construct with which to support the tibial component during revision TKA. Clinical results with these devices include good metaphyseal fixation for severe tibial bone defects.
Question 26
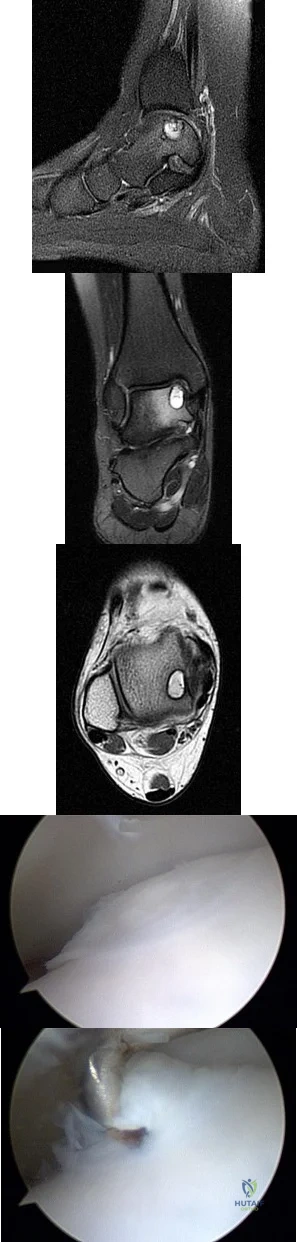
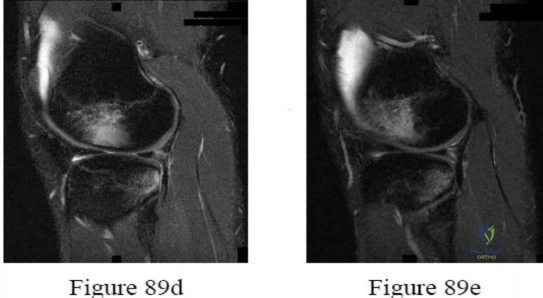
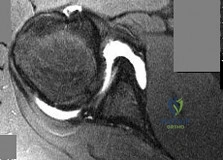
A B C D E Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?
Explanation
The MR images reveal a large cystic medial talar dome osteochondral lesion (OCL) in a patient who has failed nonsurgical treatment. Ankle fusion is inappropriate because the patient has an otherwise normal ankle. Arthroscopic debridement and drilling are appropriate for smaller (< 1.5 cm sq) noncystic lesions. Retrograde drilling and bone grafting is an option in the treatment of cystic OCL if the cartilage surface is intact; however, intraoperative arthroscopy images show that this patient's cartilage surface is unstable. Osteochondral allografts and autografts are effective in the treatment of large cystic talar dome OCLs but are not appropriate for the initial surgical treatment of smaller lesions like this one.
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
Question 27
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
/
Figure 55a Question 55
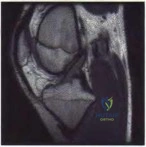
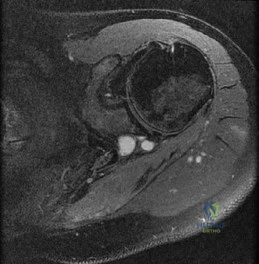
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
Locked lateral meniscus tear
Anterior cruciate ligament tear
Ganglion cyst of the anterior cruciate ligament
Synovial osteochondromatosis
Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.

Question 28
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
REFERENCES: Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Ereth MH, Weber JG, Abel MD, et al: Cemented versus noncemented total hip arthroplasty: Embolism, hemodynamics, and intrapulmonary shunting. Mayo Clin Proc 1992;67:1066-1074.
Question 29
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint? Review Topic
Explanation
Question 30
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of
Explanation
REFERENCES: Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Ark JW, Flock TJ, Flatow EL, Bigliani LU: Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy 1992;8:183-188.
Question 31
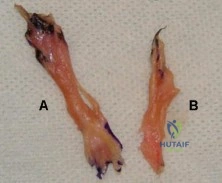
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true? Review Topic
Explanation
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle.
Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion
>30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect
Question 32
A 43-year-old man has had right groin pain for the past 3 months. A radiograph, CT scan, and biopsy specimen are shown in Figures 18a through 18c. What is the most likely diagnosis?
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 71-92.
Question 33
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
Explanation
Dysphagia after anterior cervical diskectomy and fusion is a common, usually transient finding after anterior cervical approaches to the spine. While it has been reported to occur in up to 70% of patients 2 weeks following surgery, in most cases the symptoms quickly resolve. There is, however, a small subset of patients for whom symptoms of dysphagia will persist. Lee and associates prospectively studied the rate of dysphagia after anterior cervical diskectomy and fusion, reporting a 15% rate of dysphagia at 12 months, and 12% at 24 months. Phillips and associates analyzed the 2-year data from the PCM FDE clinical trial and found a 12.1% incidence of dysphagia in the ACDF arm.
RECOMMENDED READINGS
Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. View Abstract at PubMed
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. View Abstract at PubMed
Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. View Abstract at PubMed
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.View Abstract at PubMed
Question 34
An otherwise healthy adolescent girl was treated for left slipped capital femoral epiphysis. The contralateral hip had not slipped, but was stabilized prophylactically with a single cannulated screw. The implants were removed after 1 year. The pelvic radiographs (Figures 215a and 215b) and the MRI scans of the hip that had not originally slipped (Figures 215c through 215e) were obtained 10 months after screw removal (22 months after the original fixation). Which findings are shown in these studies?
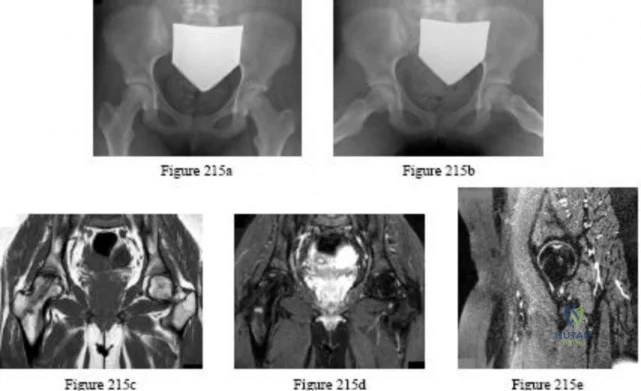
Explanation
Question 35
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future? Review Topic
Explanation
Question 36
The lesion seen in Figure 4 is most likely the result of metastases from what solid organ?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Leeson MC, Makley JT, Carter JR: Metastatic skeletal disease distal to the elbow and knee. Clin Orthop 1986;206:94-99.
Question 37
What is the most common complication following surgical fixation of a distal humeral fracture?
Explanation
REFERENCES: Sanders RA, Raney EM, Pipkin S: Operative treatment of bicondylar intra-articular fractures of the distal humerus. Orthopedics 1992;15:159-163.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 397-404.
Question 38
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include
Explanation
REFERENCES: Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
p 2030.
Question 39
A 72-year-old man with diabetic neuropathy and 5 degrees of valgus talar tilt; he has pursued nonsurgical treatment for 30 years and now has unrelenting pain
Explanation
Arthritis of the ankle and hindfoot can pose challenges. Depending upon patient age, comorbidities, and alignment, a variety of surgical interventions may be offered. A total ankle replacement may be considered for patients older than 60 years of age who have minimal misalignment and low-demand lifestyles. In all other cases, ankle fusion must be considered. The nonsurgical care of ankle arthritis includes anti-inflammatory medication, intra-articular steroid injections, bracing with customized products such as the Arizona brace, or a molded foot and ankle orthosis.
Patients with diabetes and Charcot arthropathy may be treated nonsurgically with total-contact casting during acute and active or "hot" phases and accommodative shoes during consolidation and stable or "cool" phases. When the patient has recurrent ulcers or major anatomy changes, surgical intervention must be considered. Tibiotalocalcaneal fusion helps to realign the foot and ankle and make it more braceable in the setting of ankle and hindfoot Charcot disease.
RECOMMENDED READINGS
Queen RM, Adams SB Jr, Viens NA, Friend JK, Easley ME, Deorio JK, Nunley JA. Differences in outcomes following total ankle replacement in patients with neutral alignment compared with tibiotalar joint malalignment. J Bone Joint Surg Am. 2013 Nov 6;95(21):1927-34. doi: 10.2106/JBJS.L.00404. PubMed PMID: 24196462. View Abstract at PubMed
Nunley JA, Caputo AM, Easley ME, Cook C. Intermediate to long-term outcomes of the STAR Total Ankle Replacement: the patient perspective. J Bone Joint Surg Am. 2012 Jan 4;94(1):43-8. doi: 10.2106/JBJS.J.01613. PubMed PMID: 22218381. View Abstract t PubMed
Saltzman CL, Mann RA, Ahrens JE, Amendola A, Anderson RB, Berlet GC, Brodsky JW, Chou LB, Clanton TO, Deland JT, Deorio JK, Horton GA, Lee TH, Mann JA, Nunley JA, Thordarson DB, Walling AK, Wapner KL, Coughlin MJ. Prospective controlled trial of STAR total ankle replacement versus ankle fusion: initial results. Foot Ankle Int. 2009 Jul;30(7):579-96. doi: 10.3113/FAI.2009.0579. PubMed PMID: 19589303. View Abstract at PubMed
Faraj AA, Loveday DT. Functional outcome following an ankle or subtalar arthrodesis in adults. Acta Orthop Belg. 2014 Jun;80(2):276-9. PubMed PMID: 25090803. View Abstract at PubMed Grear BJ, Rabinovich A, Brodsky JW. Charcot arthropathy of the foot and ankle associated with rheumatoid arthritis. Foot Ankle Int. 2013 Nov;34(11):1541-7. doi: 10.1177/1071100713500490. Epub 2013 Jul 30. PubMed PMID: 23900228. View Abstract at PubMed
Question 40
Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain? Review Topic
Explanation
Question 41
Intermittent daily administration of recombinant parathyroid hormone (rhPTH) is an FDA-approved treatment for osteoporosis. Intermittent rhPTH treatment targets which of the following cells in osteoporotic patients?
Explanation
Question 42
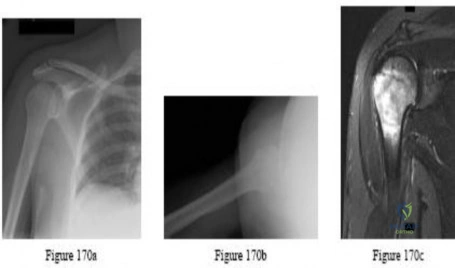
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 43
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
Explanation
REFERENCES: Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.
Question 44
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 45
- Which of the following conditions is most likely inherited as an autosomal dominant trait?
Explanation
Question 46
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 47
A 30 year-old male is involved in a motor vehicle collision and sustains a scapular fracture. In patients with scapular fractures, what other fracture is MOST commonly observed?
Explanation
Scapular fractures are associated with high-energy trauma, with motor vehicle collisions being a common mechanism of injury. These fractures are also associated with increased Injury Severity Scores and therefore clinicians need to be cognizant of concomitant injuries. In addition to associated orthopaedic injuries, pulmonary injuries (contusions, hemothorax, and pneumothorax) and head injuries are associated with scapular fractures. A CT chest should be considered in patients with scapula
fractures, to best visualize associated rib fractures and pulmonary injuries.
Baldwin et al. conducted a retrospective case control analysis using the US National Trauma Database that included 9,453 scapular fractures. In their study, the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). Lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Incorrect Answers:
(SBQ12TR.107) An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?

Intramedullary nail
Hemiarthroplasty
Closed reduction percutaneous pinning
Total hip arthroplasty
Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture Incorrect answers:
Question 48
Figures below show the radiographs obtained from a 75-year-old woman who underwent right total hip arthroplasty in 2009. She did well until last month, when a right posterior hip dislocation occurred after she fell from her bed to the floor. Successful closed reduction was performed. She sustained two more posterior dislocations requiring closed reduction under anesthesia. The surgical report from the index arthroplasty notes a 54-mm monoblock acetabular component with a 28-mm inner diameter compression molded polyethylene and a high offset neck cementless stem with a +8-mm length, 28-mm head. What is the best next step?

Explanation
This patient has demonstrated recurrent instability, and her current implants lack the modularity to upsize and improve the head-neck ratio and range to impingement. Given the monoblock acetabular component and a +7-mm neck length, the best option is revision to a large-diameter femoral head or dual-mobility component. Placement of a hip spica cast and resection arthroplasty are unreasonable. Revision to a longer ball length likely would not solve this recurrent instability pattern.
Question 49
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment?

Explanation
Question 50
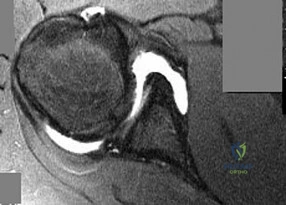
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a
Explanation
REFERENCES: Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 611-754.
Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principals of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 51
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 52
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
Question 53
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
REFERENCES: Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 54
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 55
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon: Results of operative treatment. J Bone Joint Surg Am 1996;78:1015-1023.
Question 56
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Explanation
Question 57
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 58
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient’s ability to heal the wound postoperatively?
Explanation
A transcutaneous oxygen level should be greater than 40 mm Hg for healing.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Pinzur MS, Stuck R, Sage R: Benchmark analysis on diabetics at high risk for lower extremity amputation. Foot Ankle Int 1996;17:695-700.
Question 59
A 48-year-old woman with a history of a spinal cord injury as a teenager, has unilateral weakness in the left lower extremity. She has used an ankle-foot orthosis for many years without difficulty but recently has had a recurrent painful callus beneath the great toe that has been recalcitrant to nonsurgical management. Examination reveals intact sensation with an intractable plantar keratosis (IPK) beneath the first metatarsal head. Motor examination reveals no active ankle or great toe dorsiflexion, and 4/5 plantar flexion strength at the ankle and great toe. Passive ankle dorsiflexion is 10 degrees, whereas passive plantar flexion is 40 degrees. Passive great toe dorsiflexion is 30 degrees and plantar flexion is 10 degrees. Foot alignment on standing is normal. Radiographs are shown in Figures 47a and 47b with a marker beneath the IPK. Based on her request for surgical treatment, what is the most appropriate procedure?
Explanation
REFERENCES: Grace DL: Sesamoid problems. Foot Ankle Clin 2000;5:609-627.
Mizel MS, Miller RA, Scioli MW (ed): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 135-150.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
Question 60
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Martin GJ Jr, Boden SD, Titus L: Recombinant human bone morphogenetic protein-2 overcomes the inhibitory effect of ketorolac, a nonsteroidal anti-inflammatory drug (NSAID), on posterolateral lumbar intertransverse process spine fusion. Spine 1999;24:2188-2193.
Question 61
-Figures a through c are the MRI scans of a 21-year-old woman with recurrent shoulder instability and pain after an open anterior stabilization procedure. Positive belly-press test findings were positive.At surgery she was found to have an irreparable tear of the tendon injury identified preoperatively. The procedure to address the dynamic stabilizer deficit places which nerve at most risk?
Explanation
Question 62
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
REFERENCES: Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Greis PE, Scuderi MG, Mohr A, et al: Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg 2002;11:442-451.
Question 63
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?
Explanation
REFERENCES: Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 64
EXT1
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following would be the most appropriate treatment:
Question 65
What is the main mechanism for nutrition of the adult disk?
Explanation
REFERENCES: Biyani A, Andersson GB: Low back pain: Pathophysiology and management. J Am Acad Orthop Surg 2004;12:106-115.
Urban JG, Holm S, Maroudas A, et al: Nutrition of the intervertebral disc: Effect of fluid flow on solute transport. Clin Orthop 1982;170:296-302.
Park AE, Boden SD: Intervertebral disk: Form and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 66
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 67
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete’s shoulder?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Wilk KE, Arrigo C: Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther 1993;18:365-378.
Question 68
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 69
Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best next treatment step?

Explanation
Question 70
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 71
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
Explanation
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. View Abstract at PubMed
Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
A B
Question 72
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 73
The nucleus pulposus of the intervertebral disk consists of chondrocyte-like cells that have a limited vascular supply and generate energy through which of the following?
Explanation
Question 74
Anterior subluxation in a throwing athlete is most commonly the result of
Explanation
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
Question 75
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room. Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present? Review Topic
Explanation
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3).
Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
Question 76
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Explanation
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 77
- Figure 35 shows a postoperative radiograph of a femur fracture proximal to a total knee prosthesis that was treated by open reduction and blade plate fixation 9 months ago. What is the most likely reason the previously well seated screw has backed out of the central portion of the plate?
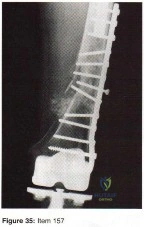
Explanation
The referenced article clearly states that the major cause of failure of fractures to heal is nonunion. From the radiograph it appears the screw at one time was long enough. While the distal fragment perhaps has some disuse osteopenia there is no focal area of what could be considered osteonecrosis. We are not given any history of possible infection even though this could be the case.
Question 78
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing’s sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 79
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
REFERENCES: McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654.
Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study.
J Bone Joint Surg Am 2003;85:773-781.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 80
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?
Explanation
REFERENCES: Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 81
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?

Explanation
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter. Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Question 82
-Radiographs are shown in Figures 89a through 89c. What is the most likely diagnosis?
Explanation
Question 83
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
REFERENCES: Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358.
McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484.
Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Question 84
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure 2. What is the most appropriate management at this time?
Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 85
A patient with a history of chronic low back pain for several years reports decreased pain visual analog scores with the home use of a transcutaneous electrical neuromuscular stimulation (TENS) unit. This pain relief is most likely due to which of the following?
Explanation
Question 86
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 87
A 77-year-old woman underwent semiconstrained right total elbow arthroplasty 4 weeks ago through a Bryan-Morrey approach. Her recovery was uneventful until 2 days ago when she began her physical therapy session at an outpatient clinic. During resisted extension exercises, she felt a "pop" in her elbow, accompanied with pain and inability to extend her elbow against resistance. What is the most likely cause of her symptoms? Review Topic
Explanation
Question 88
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 89
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?

Explanation
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p < 0.01, respectively), lower nonunion (2 vs. 7, p=0.042) & lower malunion (0 vs. 9, p=0.001). Surgery resulted in quicker radiographic union (16.4 weeks vs. 28.4 weeks, p=0.001). However, 15% had hardware and wound complications. At one year, the operative group was more likely to be satisfied with the shoulder in general (p=0.002) and the appearance of the shoulder in particular (p=0.001) in comparison to the nonoperative group.
Prior studies have shown that greater than 2cm of shortening treated non-operatively results in increased fatigueability and poor outcome, but not necessarily nonunion. The Lazarides article concluded that “Final clavicular shortening of more than 18 mm in male patients and of more than 14 mm in female patients was significantly associated with an unsatisfactory result.”
Studies have shown no difference in outcome when treated with a Figure-of-8 harness compared to a simple sling
Question 90
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 91
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
REFERENCE: Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 92
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 93
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?
Explanation
REFERENCES: Poolman RW, Kocher MS, Bhandari M: Pediatric femoral fractures:
A systematic review of 2422 cases. J Orthop Trauma 2006;20:648-654.
Anglen JO, Choi L: Treatment options in pediatric femoral shaft fractures. J Orthop Trauma 2005;19:724-733.
Beaty JH: Operative treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 2005;434:114-122.
Question 94
A patient sustains a transection of the posterior cord of the brachial plexus from a knife injury. This injury would affect all of the following muscles EXCEPT?

Explanation
Question 95
A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of
Explanation
REFERENCES: Herzberg G, Forissier D: Acute dorsal trans-scaphoid perilunate fracture-dislocations: Medium-term results. J Hand Surg Br 2002;27:498-502.
Melone CP Jr, Murphy MS, Raskin KB: Perilunate injuries: Repair by dual dorsal and volar approaches. Hand Clin 2000;16:439-448.
Herzberg G, Comtet JJ, Linscheid RL, et al: Perilunate dislocations and fracture-dislocations:
A multicenter study. J Hand Surg Am 1993;18:768-779.
Question 96
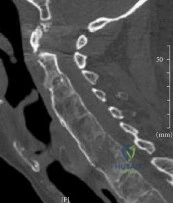
A 48-year-old man is brought in by emergency services after falling down a flight of stairs. He complains of weakness in both hands. Examination reveals weak grip bilaterally. Injury CT scans are shown in Figure A. What is the most appropriate treatment option? Review Topic
Explanation
The C-spine is the most common site of fracture in AS and is most susceptible to hyperextension injuries. When surgical intervention is required, multiple points of fixation both above and below the fracture are necessary. This is due to co-existing osteoporosis and abnormally increased forces from long lever arms of the ankylosed spine, both of which make the construct susceptible to failure and screw pullout.
Kubiak et al. reviewed the orthopaedic management of AS. They report bone scan, MRI or fine-cut CT is necessary because fractures are often missed on plain x-rays because of distortion of anatomy or difficulty with positioning.
Whang et al. reviewed spinal injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likley to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Figure A is a sagittal CT reconstructed image showing a nondisplaced shear fracture through the C6 vertebral body and C5 posterior elements. Illustrations A and B are postop AP and lateral radiographs showing posterior decompression and C3-T2 fusion with lateral mass fixation in the cervical spine and pedicle screw fixation in the upper thoracic spine.
Incorrect Answers:
performed through a posterior approach. If there is significant osteoporosis and the risk of construct failure is high, a 360-approach may be necessary.
Question 97
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
REFERENCES: Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Micheli LJ: Strength training, in Sullivan JA, Grana WA (eds): The Pediatric Athlete. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 17-20.
Question 98
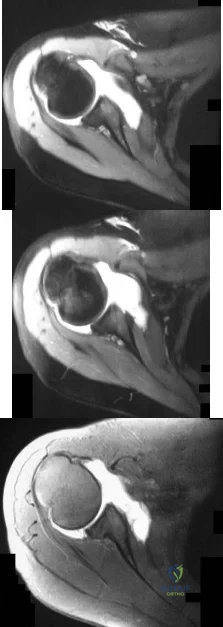
A 16-year-old right-hand dominant pitcher has had pain with throwing for the past 6 months but denies any history of trauma. Figures 9a and 9b show noncontrast MRI scans of the involved shoulder. What is the most likely diagnosis? Review Topic

Explanation
Question 99
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
Explanation
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Naudie DD, Rorabeck CH: Managing instability in total knee arthroplasty with constrained and linked implants. Instr Course Lect 2004;53:207-215.
Question 100
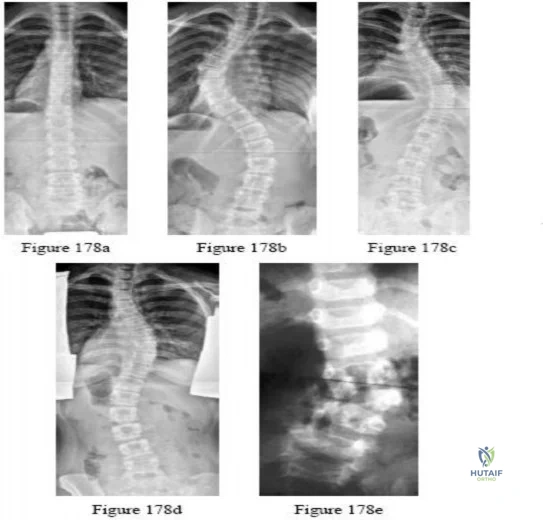
-Figures a and b are the posteroanterior and lateral radiographs of a 13-year-old girl with a progressive curve despite bracing with a thoracolumbosacral orthosis. Examination reveals no pain or neurologic findings. The lumbar curve measures 59 degrees and the thoracic curve measures 52 degrees.The most appropriate treatment is

Explanation