Orthopedic Board Prep MCQs: Pediatric, Shoulder & Sports Medicine | Part 118

Key Takeaway
This page offers Part 118 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review. Authored by Dr. Mohammed Hutaif, it features 100 verified, high-yield multiple-choice questions (MCQs) for orthopedic surgeons and residents. Prepare effectively for your board certification exams with detailed explanations and practice modes.
About This Board Review Set
This is Part 118 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 118
This module focuses heavily on: Dislocation, Pediatric, Shoulder, Tendon.
Sample Questions from This Set
Sample Question 1: Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?...
Sample Question 2: What is the recommended insertion torque for halo pins in adults?...
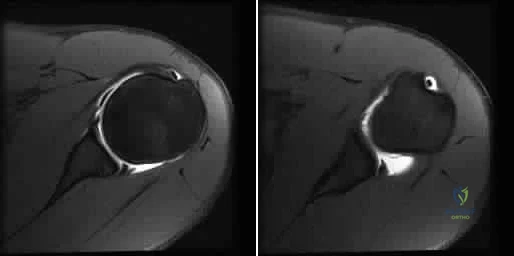
Sample Question 3: A 21-year-old basketball player reports increased left shoulder pain with all lifting and overhead activities. He denies any history of dislocations. Axial MRI arthrogram images are seen in Figures 34a and 34b. An expected finding on physic...
Sample Question 4: Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?...
Sample Question 5: The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 2
What is the recommended insertion torque for halo pins in adults?
Explanation
REFERENCES: Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752.
Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Vaccaro AR, Botte MD, Bengt IL, et al: Cervical orthotics including traction and halo devices, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 113-140.
Question 3
A 21-year-old basketball player reports increased left shoulder pain with all lifting and overhead activities. He denies any history of dislocations. Axial MRI arthrogram images are seen in Figures 34a and 34b. An expected finding on physical examination of the shoulder would be positive findings for which of the following tests? Review Topic
Explanation
then abducted, while maintaining the axial load, and the patient's subjective and objective response is observed. Comparison to the contralateral shoulder is important, especially if painless subluxation is noted, to determine potential evidence of generalized joint laxity.
Question 4
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 5
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced
Explanation
REFERENCES: Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Nistor L: Surgical and non-surgical treatment of Achilles tendon rupture. J Bone Joint Surg Am 1981;63:394-399.
Question 6
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5- 10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
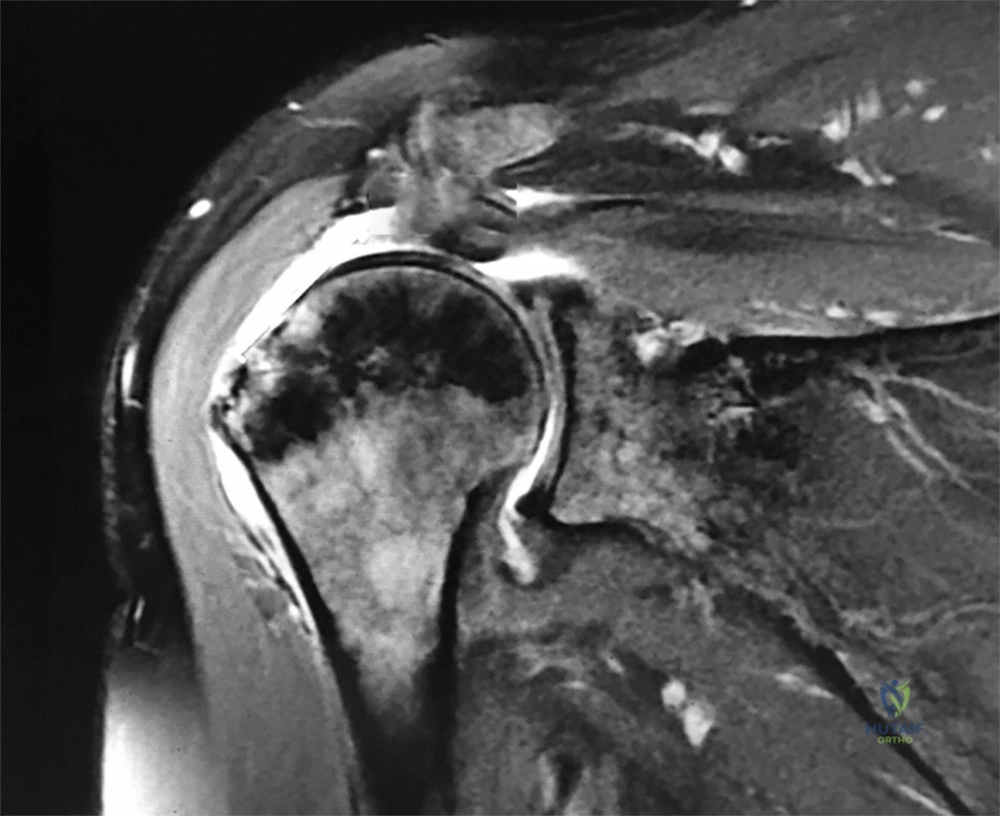
60°, and passive forward shoulder flexion of 160°. He has 2/5 forward flexion and external rotation strength. Initial plain radiographs are unremarkable. A coronal MRI scan of his shoulder is shown in Figure 1. After a thorough discussion, the patient elects to proceed with surgical intervention. During intraoperative assessment, the surgeon contemplates performing a single versus a dual row repair. Currently, what is the consistent difference between the two repair techniques?
A. Dual row repairs result in superior objective clinical outcomes
B. Dual row repairs provide a larger footprint coverage.
C. Single row repairs have a reported higher complete retear rate.
D. Single row repairs have fewer points of tendon fixation.
Question 7
A year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 8
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 9
A 54-year-old man undergoes uneventful anterior cervical diskectomy and interbody fusion at C4-5 for focal disk herniation and C5 radiculopathy. At the 3-week follow-up examination, the patient reports a persistent cough. Pulmonary evaluation reveals a mild but persistent aspiration. Laryngoscopy reveals partial paralysis of the left vocal cord, most likely caused by
Explanation
REFERENCES: Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve paralysis during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Jewett BA, Menico GA, Spengler DM, Coleman SC, Netterville JL: Vocal Cord Paralysis Following Anterior Cervical Spine Surgery. Paper presented at the annual meeting or the Cervical Spine Research Society, December 2000, Charleston SC, Paper #7.
Question 10
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
REFERENCES: Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am
1995;77:1042-1049.
Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case report. J Bone Joint Surg Am
1991;73:1555-1560.
Question 11
A 57-year-old man has right knee osteoarthritis and is indicated for a total knee arthroplasty (TKA). The patient has questions regarding the use of preoperative 3-dimensional imaging to develop custom cutting guides. Current data have been shown to support what proposed benefits with the use of custom cutting guides versus conventional instrumentation?
Explanation
Question 12
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
Explanation
REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Question 13
An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis? Review Topic
Explanation
(SBQ07SM.48) Carbohydrate loading is a common practice among endurance athletes that works by what mechanism? Review Topic
Increasing serum fructose levels
Maximizing stored muscle glycogen for endurance after 90 minutes of exercise
Diuresis
Decreasing serum glucose levels
Maximizing stored liver glycogen for endurance after 60 minutes of exercise
Carbohydrate loading is a strategy that involves changes to training and nutrition which can maximize muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes.
There continues to be varying scientific opinions as to whether athletes should eat low vs. high glycemic index foods, and how this will affect the amount that the serum glucose levels rise. Fructose is able to be converted to glycogen in the liver but not muscle, therefore high-fructose containing foods are suboptimal. This practice is recommended for athletes participating in events that are longer than 90 minutes (after the bodies normal supply of glycogen is depleted).
Coyle et al. analyzed 10 trained cyclists who performed two bicycle ergometer exercise tests 1 wk apart. They found that blood glucose concentration was 20-40% higher during the exercise after carbohydrate ingestion than during the exercise without carbohydrate feeding. The exercise-induced decrease in plasma insulin was prevented by carbohydrate feeding. Ultimately, fatigue was postponed by carbohydrate feeding during exercise in seven out of the ten subjects.
Costill et al. examined the effect of carbohydrates on muscle glycogen resynthesis in trained runners and found that muscle glycogen levels could be normalized with the proper use of carbohydrates after strenuous activity.
Sherman et al. used muscle biopsies to determine the effects of moderate- or high-carbohydrate diets on muscle glycogen and performance in runners and cyclists over 7 consecutive days of training. They found that a high carbohydrate diet restored muscle glycogen to more normal levels than a moderate carbohydrate diet but did not find any difference in the effect on performance.
Illustration A is a graph depicting the typical carbohydrate depletion/loading regimen that endurance athletes utilize to maximize muscle glycogen stores prior to endurance exercise. This typically involves a hard workout followed by three days of a low-carb diet, another hard workout, and another three days of a high-carb diet.
Incorrect
Question 14
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 15
Which of the following best characterizes the injury shown in Figure 53? Review Topic

Explanation
Question 16
Lymphatic metastasis is a common feature of which of the following lesions?
Explanation
Question 17
During total hip arthroplasty, which characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma-irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of this material is inferior to traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.

RESPONSES FOR QUESTIONS 76 THROUGH 80
Cemented full revision
Cemented femoral revision
Cemented acetabular revision
Cementless full revision
Cementless femoral revision without an extended trochanteric osteotomy
Cementless femoral revision with an extended trochanteric osteotomy
Cementless acetabular revision
Isolated liner/head exchange
Isolated liner/head exchange with cementing of the liner Select the most appropriate treatment for each clinical scenario.
Question 18
-The use of a soft cervical orthosis is most supported for which injury?
Explanation

Question 19
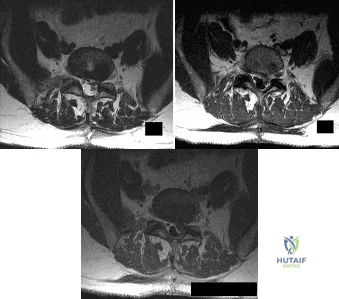
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
Explanation
Question 20
Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?
Explanation
Multiple studies have confirmed that CAM or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, CAM deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion was higher than 50% in the subgroup of athletes.
Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in the majority of nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between CAM deformity and hip osteoarthritis, a corresponding link between correction of the deformity and prevention of osteoarthritis has never been proven.
Results of CAM deformity correction, typically including repair of the degenerative labral tear, are much poorer when there is significant joint space loss. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 21
In the absence of developmental dysplasia of the hip, what is the most common cause of osteoarthritis? Review Topic
Explanation
Question 22
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?
Explanation
REFERENCES: Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330.
Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830.
Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop 1999;364:220-226.
Question 23
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 24
When performing a Kocher approach to the radial head for open reduction internal fixation the forearm is held in pronation. What structure is this maneuver attempting to protect?

Explanation
Question 25
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
Explanation
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Question 26
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 27
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely
Explanation
REFERENCES: Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am
1993;75:1282-1297.
Question 28
Figure 61 shows the current radiograph of a 69-year-old woman who fell getting out of bed 10 months ago. At the time of injury she was diagnosed with a nondisplaced humeral surgical neck fracture. After 2 weeks of sling immobilization, physical therapy was started for range of motion. She continues to have pain and is unable to elevate her arm. What is the most likely diagnosis?

Explanation
(SBQ12TR.96) Interleukin-6 levels have been shown to be a reliable measure of which of the following?
Osteoporosis
Severity of injury
Sarcomatous tumor burden
Bone turnover
Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production. Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
Question 29
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 30
A 22-year-old man sustained a shoulder dislocation while playing collegiate football at age 18. Since that time, he has dislocated the shoulder three more times despite physical therapy. His last dislocation occurred 4 weeks ago while sleeping. What is the most appropriate management for this patient? Review Topic
Explanation
Question 31
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following? Review Topic
Explanation
the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears.
Question 32
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Poole AR, Kojima J, Yasuda T, Mwale F, Kobayasai M, Laverty S: Composition and structure of articular cartilage: A template for tissue repair. Clin Orthop 2001;391:S26-S33.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 33
A B Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?

Explanation
The patient has previously undiagnosed ankylosing spondylitis. Radiographs reveal nonmarginal syndesmophytes throughout the lumbar spine. The CT scan reveals a nondisplaced 3-column fracture. Many patients with missed spinal injuries present in followup with neurologic worsening or progressive deformity. Fractures can often involve all 3 columns, including the posterior elements. In patients with ankylosing spondylitis, this represents an unstable injury and a high likelihood of displacement with nonsurgical treatment. Surgical treatment in the form of a posterior spinal fusion is indicated. Because the fracture is nondisplaced and the patient is neurologically intact, decompression via an anterior approach is not indicated. Bracing either with a TLSO brace or a soft corset will not provide sufficient stability for this fracture pattern. Physical therapy and NSAIDS are not indicated in this scenario.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.

Question 34
A 56-year-old woman presents with left hip pain and diminishing range of motion. Examination reveals pain with range of motion of the hip. Radiographs reveal multiple calcific lesions within the hip and well-preserved joint space. MRI scan shows thickened synovium nodular loose bodies with decreased signal on T1 and T2. What is the best next step?
Explanation
Question 35
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include
Explanation
a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated.
REFERENCES: Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Velmahoos GC, Demetriades D: Gunshot wounds of the spine: Should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1976;94:85-87.
Question 36
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?
Explanation
REFERENCE: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 37
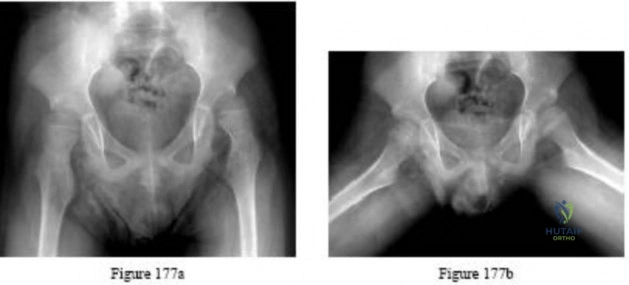
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
Explanation

Question 38
An 18-month-old child has a congenital anterolateral bowing of the tibia. The radiograph shown in Figure 13 reveals increased density with obliteration of the medullary canal at the apex of the 40-degree bow. Treatment should consist of
Explanation
Question 39
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.
Question 40
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 41
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
REFERENCES: Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 42
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
Explanation
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
Question 43
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?
Explanation
REFERENCES: Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Kurkcuoglu IC, Eroglu A, Karaoglanoglu N, et al: Soft tissue hemangioma is a common soft tissue neoplasm. Eur J Radiol 2004;49:179-181.
Question 44
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
application of a hinged external fixator may be considered.
Question 45
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
Question 46
The patient decides to pursue surgical intervention. Which compartments should be released?
Explanation
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible for the patient's symptoms and falls below current thresholds for diagnosis.
Question 47
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
REFERENCES: Fukuda K, Craig EV, An KN, et al: Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-439.
Bosworth B: Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-225.
Question 48
Which of the following statements best describes synovial fluid?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 443-470.
Question 49
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 50
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 51
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal? Review Topic
Explanation
Question 52
Of the following signs or findings, which one is most consistent with the diagnosis of cervical radiculopathy? Review Topic
Explanation
Question 53
below depict the radiographs obtained from a year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 54
-The Coleman block test is used to test for
Explanation

Question 55
..Oncologic outcome for this patient
Explanation
Question 56
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
Explanation
fragile p-values is that small sample sizes may result in wide variability of p-values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statisticalsignificance of the outcomes analysis. Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the proportion of patients with negative test results who are correctly diagnosed.
Question 57
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 58
A 50-year-old woman reports a burning sensation on the plantar aspect of her left forefoot, distal to the metatarsal heads between her third and fourth digits. Palpation of the third web space recreates her symptoms. Which of the following will most accurately aid in confirming a diagnosis?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 145-151.
Quinn TJ, Jacobson JA, Craig JG, et al: Sonography of Morton’s neuromas. Am J Roentgenol 2000;174:1723-1728.
Question 59
An 80-year-old patient presents 8 months postoperatively with right groin pain. Examination reveals a leg length discrepancy of 1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
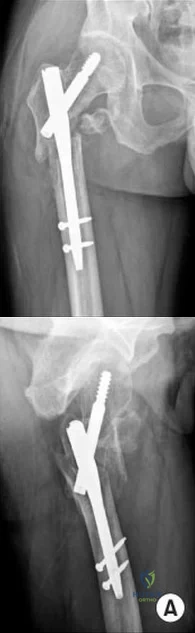
Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
(SBQ12TR.48) A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation
as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?

Age less than 30
Marijuana use
Use of negative pressure wound therapy
Male gender
Ability to return to work
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or
limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
1-4: These options are not as strong of a factor of patient satisfaction in long-term follow up after trauma-induced lower extremity amputation.
Question 60
A 12-year-old child with L4 myelomeningocele who is schedules for foot surgery has a functioning ventriculoperitoneal shunt and has no history of allergies. Management should include
Explanation
Question 61
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?
Explanation
REFERENCES: Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 182-183.
Question 62
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Hofmann A, Wenger DR: Posteromedial bowing of the tibia: Progression of discrepancy in leg lengths. J Bone Joint Surg Am 1981;63:384-388.
Question 63
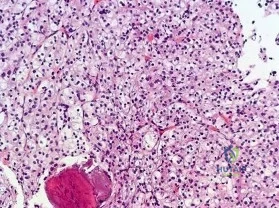
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
Explanation
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.


Question 64
A 27-year-old woman underwent shoulder arthroscopy for multidirectional instability 3 years ago. She was unable to regain shoulder range of motion despite therapy and has had progressively worsening pain. A current axillary radiograph is shown in Figure 100. In reviewing the medical records from the index procedure, what factor may be significant in contributing to her current condition? Review Topic

Explanation
Question 65
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 66
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 67
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?
Explanation
REFERENCES: Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2.
Berlin, Germany, Springer-Verlag, 1991.
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am
1996;78:1632-1645.
Question 68
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
REFERENCES: O’Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
Warner JP: The gross anatomy of the joint surfaces, ligaments, labrum and capsule, in Matsen FA, Fu FF, Hawkins RJ (eds): The Shoulder: A Balance of Mobility and Stability. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 7-28.
Question 69
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment.
J Bone Joint Surg Am 2005;87:1848-1864.
Question 70
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 71
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?
Explanation
REFERENCES: Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Easley ME, Davis WH, Anderson RB: Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999;20:147-152.
Question 72
The parents of a 15-month-old child report that he is not yet walking. Further evaluation, rather than reassurance and observation, should be conducted if the child is not performing what other activity?
Explanation
child should be able to sit by age 9 months. The remaining milestones listed are reached later
in development.
REFERENCES: Behrman RE, Kliegman RM, Jenson HB: The first year, in Fletcher J, Thorp D, Davis RE (eds): Nelson Textbook of Pediatrics, ed 17. Philadelphia, PA, WB Saunders, 2004,
p 33.
Question 73
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
REFERENCES: Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 1146-1167.
Question 74
A 70-year-old man with primary osteoarthritis undergoes a primary cementless total hip arthroplasty (THA). His history includes pelvis irradiation for prostate carcinoma (6000 rads). He is at increased risk for which complication?
Explanation
The complication associated with pelvic radiation prior to cementless THA is loosening of the acetabular component or postsurgical noningrowth of the component. Although scarring from radiation may put the hip at increased risk for arterial or nerve damage or infection, this risk has not been associated with pelvic radiation. Cementless acetabular components with porous metal surfaces such as trabecular metal should be considered.
Question 75
7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Explanation
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
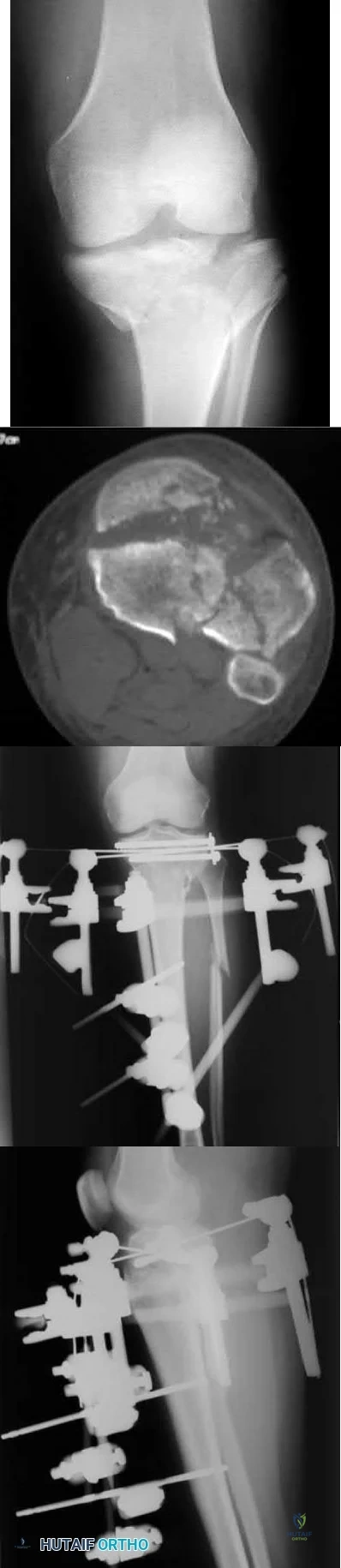
Longer operative times
Increased deep surgical infection rates
Unacceptably high malunion/nonunion rates
Slower early return to function
Longer hospital stays Corrent answer: 3
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
OrthoCash 2020
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?
Posterior approach
Anterior approach
Anterolateral approach
Use of a bipolar implant
Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?

Exchange humeral nailing
Augmentative plating
Nail removal with open reduction compression plating
Smoking cessation and medical optimization
Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
OrthoCash 2020
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
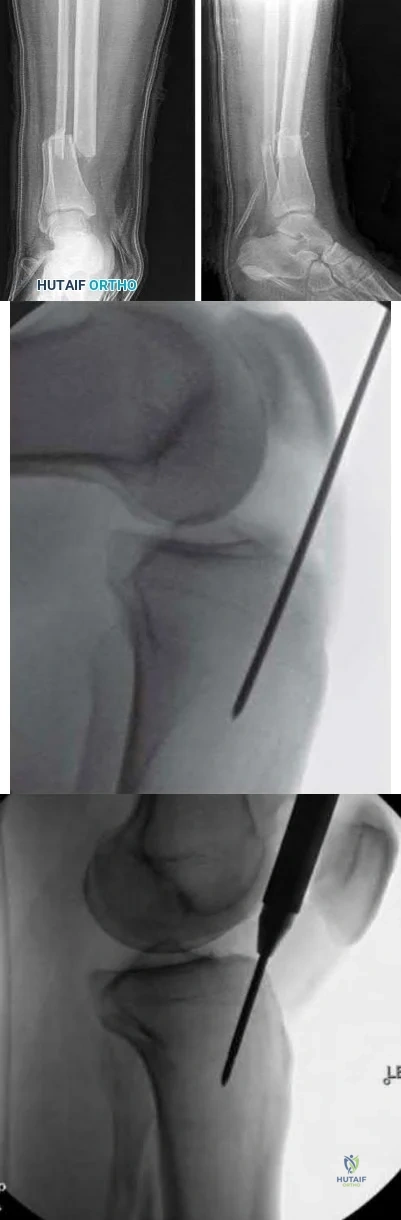
Technique depicted in Figure B is associated with an increased risk of septic arthritis
Technique depicted in Figure B is associated with increased rate of anterior knee pain
Technique depicted in Figure B is associated with improved postoperative fracture alignment
Technique depicted in Figure C is associated with an increased risk of septic arthritis
Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
OrthoCash 2020
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?

Nerve compression; open reduction internal fixation with open carpal tunnel release
Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
Decreased arterial inflow; fasciotomy with open reduction internal fixation
Reflex sympathetic dystrophy; vitamin C
Nerve compression; repeat closed reduction Corrent answer: 1
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
OrthoCash 2020
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?

Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
No difference in radiographic outcomes after ORIF vs. closed treatment
No difference in functional outcomes after ORIF vs. closed treatment
Improved functional outcomes with closed treatment vs. ORIF
Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
no difference in functional outcomes between operative and closed treatment modalities for DRF.
OrthoCash 2020
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?

Continued sling immobilization
Closed reduction percutaneous pinning
Open reduction internal fixation
Hemiarthroplasty
Reverse total shoulder arthroplasty Corrent answer: 3
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:

OrthoCash 2020
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?

MCL > LCL > anterior capsule
MCL > anterior capsule > LCL
anterior capsule > MCL > LCL
LCL > anterior capsule > MCL
LCL > MCL > anterior capsule Corrent answer: 4
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
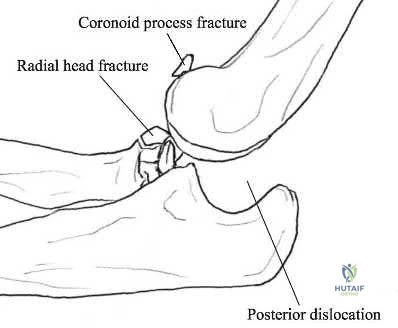
OrthoCash 2020
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
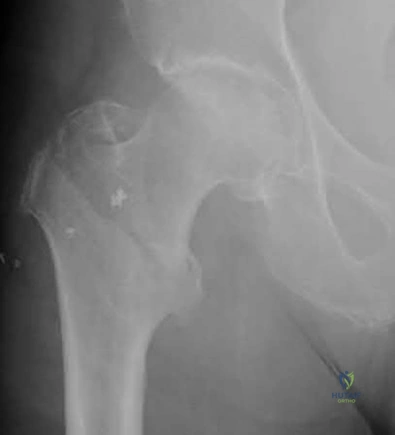
Reverse obliquity fracture pattern
Lateral wall thickness
Previous contralateral hip fracture
DEXA T-score <-2.0
Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
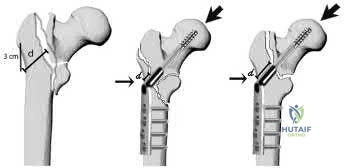
OrthoCash 2020
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?

Smaller lateral wall thickness favors sliding hip screw constructs
Unstable fractures are best treated with sliding hip screw constructs
Avoiding distal locking screws in intramedullary implants protects against refracture
Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
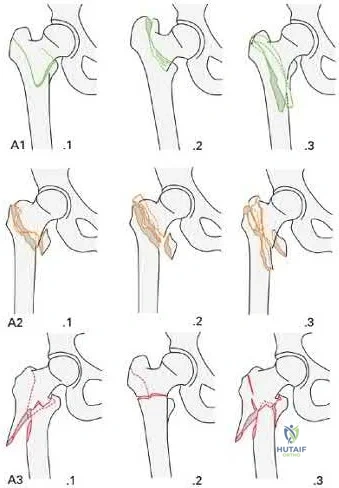
OrthoCash 2020
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference <20 mm/hr) and 0.9 mg/L (reference <2.5 mg/L), respectively. Figures A and B are the AP and lateral radiographs of the left femur. Which treatment option offers the highest chance of union and enables immediate weight-bearing?

Nail removal with compression plating and open bone grafting
Closed reamed exchange nailing
Nail dynamization
Nail retention with plate augmentation and bone grafting
Electrical bone stimulator Corrent answer: 4
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:

OrthoCash 2020
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?

External fixation with serial doppler examinations
Intramedullary nailing
Open reduction internal fixation using plates and screws
Immediate 2-compartment fasciotomies and external fixation
Immediate 4-compartment fasciotomies and external fixation Corrent answer: 5
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p) <30 mmHg may help to confirm the necessity for fasciotomy.
McQueen et al. published a report of 25 patients with tibial diaphyseal fractures which had been complicated by an acute compartment syndrome. They reported significant differences in any sequelae of acute compartment syndrome between patients who underwent compartment pressure monitoring and those who had not. They recommended that all patients with tibial fractures should have continuous compartment monitoring to minimize the incidence of acute compartment syndrome.
Mawhinney et al. reported on three cases of tibial compartment syndrome after closed intramedullary nailing of the tibia. They reported that the only predisposing factors for the development of compartment syndrome were the surgery and the fracture itself. They concluded that tibial compartment syndrome is a relatively rare but significant complication of tibial nailing.
Figure A is an AP and lateral radiograph of the leg with displaced, comminuted middle third tibia and fibula fractures.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Decreased arterial inflow; inability to dorsiflex his ankle
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:

OrthoCash 2020
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
Syme
Traumatic transtibial
Vascular transtibial
Traumatic transfemoral
Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
OrthoCash 2020
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?

It may be performed in a minimally invasive manner
It involves minimal soft tissue stripping
It leads to higher union rates
It allows the surgeon to address all sites of injury through one approach
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:

OrthoCash 2020
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
Iliac oblique view with hip and knee flexed
Iliac oblique inlet view
Obturator oblique view with hip and knee flexed
Obturator oblique outlet view
Obturator oblique inlet view Corrent answer: 2
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
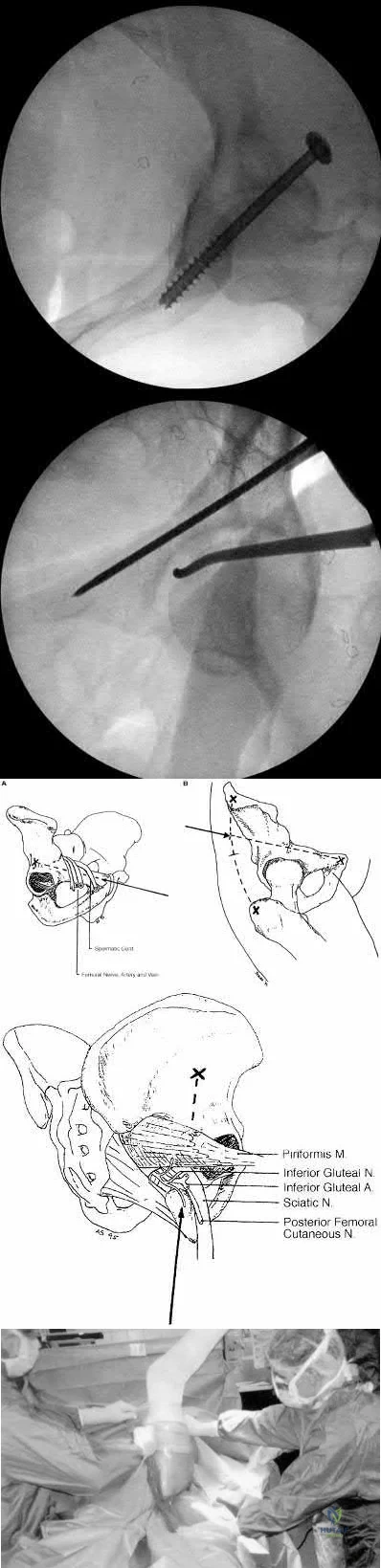
OrthoCash 2020
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
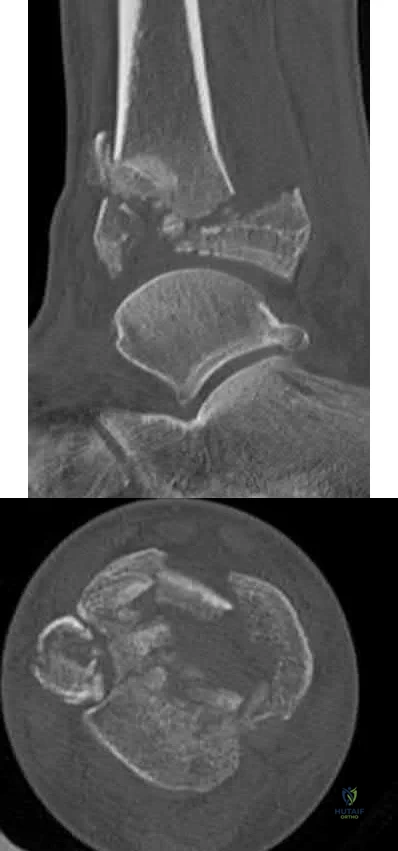
TGF-Beta
RANKL
IL-2
IL-6
cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
immune system.
OrthoCash 2020
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
Ulnar styloid nonunion
DRUJ instability
Articular step-off >3mm
Radial shortening
Workers compensation claim Corrent answer: 1
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
OrthoCash 2020
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?

Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including <8mm of calcar length attached to the articular segment, disruption of the medial hinge, displacement >10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of <8mm attached to the articular segment. Figure D is a displaced metadiaphyseal proximal humerus fracture in a skeletally immature patient. Figure E is a radiograph of a metadiaphyseal proximal humerus fracture in a skeletally mature patient with a medial calcar length >8mm.
Incorrect Answers:
OrthoCash 2020
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?

Nondisplaced medial malleolus vertical shear fracture
Nondisplaced Volkmann's fragment
Nondisplaced Chaput's fragment
Nondisplaced lateral wall talar fracture
Posterior inferior tibiofibular ligament disruption Corrent answer: 2
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
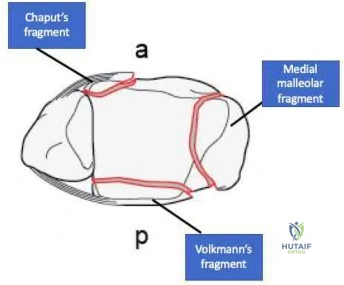
OrthoCash 2020
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
Age < 20
Male gender
Body mass index >/ 30 kg/m^2
Open fracture
Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?

Greater Mayo Elbow Performance Score
Greater Disabilities of the Arm, Shoulder and Hand Score
Increased flexion-extension arc
Increased reoperation rate
Decreased complication rate Corrent answer: 4
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:

OrthoCash 2020
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?

Anterior perforation of distal femur
Breakage of the screw
Implant cutout
Malunion
Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:

OrthoCash 2020
Figure A is the radiograph of a 42-year-old female who presents to the trauma bay following a motor vehicle collision. She subsequently undergoes ORIF through a posterior approach. Iatrogenic injury to which nerve in Figure B is most likely with this approach?
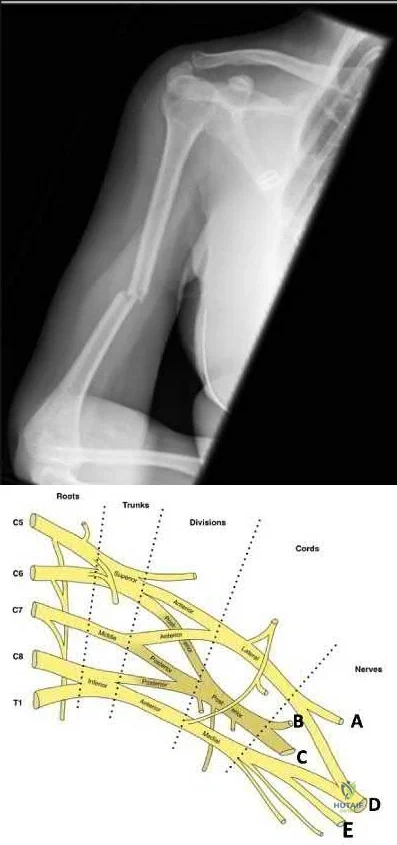
Question 76
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 77
A 30-year-old man has had leg pain for 6 months. A lesion is identified in the proximal femur and biopsy it taken. Histology is shown in Figure A and is consistent with a low-grade intramedullary osteogenic sarcoma. Additional imaging studies confirm that this is an isolated lesion with no metastasis. What is the standard treatment for this type of lesion?
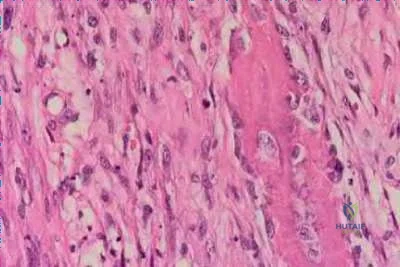
Explanation
Choong et al. reviewed the long term follow-up of 20 patients diagnosed with low grade osteogenic sarcoma and found the 5 year survival rate was 90% and at 10 years was 85%. Local recurrence is a key feature in most cases and is typically the result of inadequate surgical margins frequently arising from initial misdiagnosis. Although amputation generally is successful for primary and recurrent tumors, limb salvage surgery is a definite option.
Kurt et al reviewed 80 well-differentiated osteosarcomas. They found local excision was almost always associated with recurrence. Wide excision was
almost never followed by recurrence. The recurrent tumor was a high-grade, conventional osteosarcoma in 15% of the patients, and this was associated with a poor prognosis. They recommend wide excision as the treatment of choice for this very rare variant of osteosarcoma.
A 32-year-old male sustains a the injury shown in Figure A after a high-speed motor vehicle collision. Which factor has been found to have the highest direct correlation with severe heterotopic ossification after traumatic knee dislocation?

Injury Severity Score (ISS )
Glascow Coma Scale (GCS )
Timing of knee reconstruction
Number of ligaments reconstructed
Open ligament reconstruction
Figure A shows a knee dislocation with cruciate ligament avulsion injuries. Development of significant heterotopic ossification (HO) formation has been shown to be most directly correlated to the ISS score.
Mills and Tejwani looked at multiple variables including injury severity score
( ISS), Glascow coma scale (GCS), closed head injury (CHI), timing of surgery (> or < 3 weeks) and type of surgery (open vs. arthroscopic, number of ligaments reconstructed) in its relation to the formation of HO following knee dislocation. In the final group the sensitivity and specificity of the ISS in relation to HO formation was 100%, while presence of CHI had a specificity of 97 %. Timing, type of surgery and approach did not influence HO formation.
A 52-year-old male presents with 6 months of swelling and pain in his leg. He states the lesion has not changed in size for several months and doesn't bother him. He is otherwise healthy and has no other complaints. Representative photograph and MRI are shown in Figures A through C. What is the best initial step in his management?
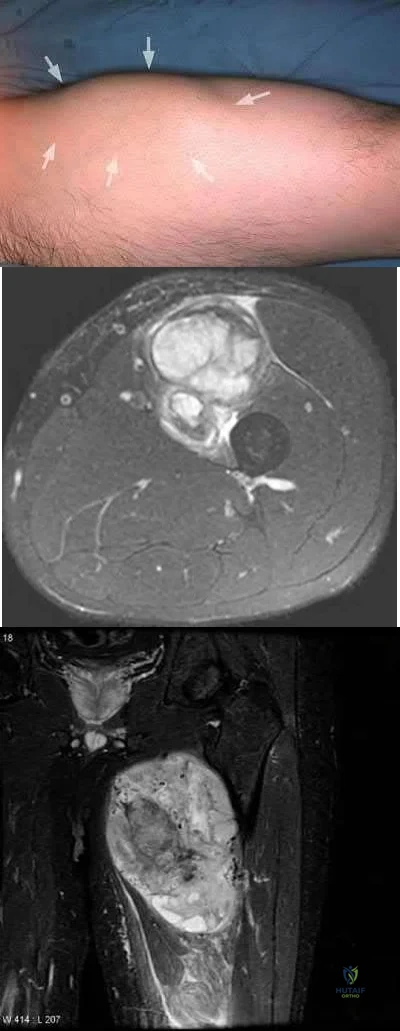
Follow-up in 6 months with repeat radiographs
Biopsy
Marginal excision
Radiation therapy
Neoadjuvant chemotherapy and wide excision
The initial step in management of a patient presenting with a large soft tissue mass deep to the fascia is to obtain a tissue diagnosis, via biopsy. Initiation of treatment prior to tissue diagnosis is inappropriate and can result in significant patient morbidity and potential mortality. While some soft tissue sarcomas may benefit from chemotherapy, this cannot be initiated prior to diagnosis.
Radiation therapy is used in the treatment of soft tissue sarcoma, but again, only after tissue diagnosis. Peabody et al review the appropriate evaluation and staging for musculoskeletal neoplasms and present flow-charts useful in the work-up of bone (Illustration A) and soft tissue (Illustration B) neoplasms. Skrzynski et al performed a comparison of outpatient core-needle biopsy with open surgical biopsy for musculoskeletal tumors. They found the diagnostic accuracy of core-needle biopsy was only 84% with many samples yielding no or different histological samples when compared to final resected specimens. They conclude that while core-needle biopsy is significantly less expensive
than surgical biopsy ($1106 vs. $7234), there is higher concern for sampling error or general diagnostic inaccuracy associated with a core-needle biopsy compared to open biopsy, the "gold standard".
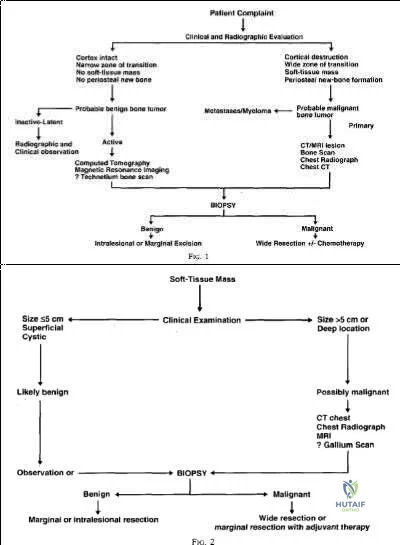
What is the appropriate treatment for a 10-year-old boy with Ewing's sarcoma isolated to the proximal femur?
Neoadjuvant chemotherapy and surgical excision
Neoadjuvant chemotherapy, surgical excision, and radiation therapy
Neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy
Neoadjuvant radiation therapy and surgical excision
Surgical excision and hormonal therapy
Ewing's sarcoma is a malignant small round blue cell neoplasm which has a predilection for long tubular bones, pelvis, and ribs. The radiographic appearance of "onion-skinning" seen in illustrations A and B is due to the body's periosteal reaction. Illustration C shows the large soft tissue extraosseous mass characteristic for Ewing's sarcoma. Finally, Illustration D shows the histology where the multiple small round blue neoplastic cells are seen.
Ewing's sarcoma is most commonly treated with neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy - in particular for tumors located in bones which can be easily resected and reconstructed. For large tumors in areas which either cannot be completely excised or where excision is associated with significant morbidity, some centers consider chemotherapy and radiation therapy without surgical excision. There is a current trend towards surgical resection and away from irradiation for Ewing's sarcoma even though it is radiosensitive, because of the risk of secondary malignancy and growth disturbance due to radiation.
Pierz et al review many of the common bone tumors including Ewing's sarcoma and discuss the relevant diagnostic factors as well as specific treatment protocols for each tumor.

A 30-year-old female presents with a painful posterior knee mass. The mass gets larger and more painful with activity. Examination reveals a boggy soft tissue mass about her knee. Radiograph and MRI are shown in Figures A and B. What is the most likely diagnosis?

Synovial sarcoma
Hemangioma
Lipoma
Parosteal osteosarcoma
Pigmented villonodular synovitis (PVNS )
This patients history, physical exam, and imaging studies are suggestive of a hemangioma. Pain in hemangiomas is thought to occur due to vascular engorgement secondary to activity and increased blood flow to the lesion. The calcification on the plain radiograph and the fat of the T1 MRI are diagnostic for hemangioma. Current treatment for symptomatic hemangiomas includes some combination of sclerotherapy or vascular coiling, with surgical excision
reserved for few cases. The two attached reviews by Gilbert et al and Damron et al review the history, diagnosis, treatment, and controversial issues in soft tissue sarcomas and benign sarcoma like conditions such as hemangiomas.
Current treatment for soft tissue sarcomas includes radiotherapy and surgical excision. While many centers in the world use chemotherapy for soft tissue sarcomas, the data supporting its use is quite limited and likely too controversial to be tested. With regard to the other answer choices, synovial sarcoma and lipoma can show calcification on radiographs, but they are usually not painful and image differently on T1 MRI. Parosteal osteosarcoma typically occurs in this location (posterior distal femur) but occurs as a lesion stuck on the bone. PVNS can have a similar appearance on imaging, but doesn't cause this type of pain.
Question 78
A 70-year-old male with longstanding diabetic neuropathy sustains a fall down a flight of stairs and sustains the injury shown in Figures A and B. In the operating room, direct reduction of the fracture is performed. The syndesmosis is assessed and found to be intact. The fibula is fixed with a small fragment locking plate and the medial malleolus is fixed with screws. What is the next best step? Review Topic

Explanation
Diabetics with ankle fractures are prone to complications. Nonoperatively treated cases have up to a 50% incidence of skin breakdown in a cast. Surgically treated patients have up to 40% complication rate. Supplemental fixation can include include multiple syndesmotic screws, spanning external fixation, tibio-talar Steinmann pins, more rigid fibular plates, supplemental intramedulary fibular pinning. Weightbearing after surgery should be delayed (8-12weeks).
McCormack and Leith reviewed the complications in 26 diabetic ankle fractures. 19 patients had surgery. The incidence of complications was 42%. Two required amputation and died. None of the non-diabetic control group had complications. They concluded that in the older, diabetic patient with lower demands, especially if insulin-dependent, it may be preferable to accept a loss of reduction and malunion rather than risk the potentially devastating complications associated with operative intervention. If surgery is necessary, the results of this study provides a more accurate prognosis and allows for better discussion of surgical risks with the patient.
Roseunbaum et al polled AOFAS members on the treatment of diabetic ankle fractures. (1) For nondisplaced bimalleolar fracture with diabetic neuropathy, respondents preferred casting and nonweightbearing (NWB) for 8-12 weeks. (2) For Weber B fracture dislocation without neuropathy, without syndesmotic injury,
respondents preferred either 1/3 tubular or small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks. (3) For bimalleolar fracture dislocation with neuropathy, without syndesmotic injury, respondents preferred small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks.
Wukich and Kline reviewed the management of ankle fractures in diabetics. They found that neuropathy is more prevalent in patients with ankle fractures than without. They stress that 1% reduction in HbA1C results in 30% reduction in complication rate. Fracture healing is slower, callus is smaller, with less stiffness, tensile strength and collagen content. Amputation rate is up to 5% for patients treated operatively or nonoperatively. Complications are higher in patients with vasculopathy, neuropathy, or Charcot arthropathy.
Incorrect Answers:
Question 79
A B Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. View Abstract at PubMed Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
Question 80
On average, the radial nerve travels from the posterior compartment of the arm to the anterior compartment at which of the following sites?

Explanation
Question 81
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
Question 82
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 83
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
Explanation
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
Question 84
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 85
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
REFERENCES: Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429.
Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 86
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 87
2ppb and chromium levels were 2.2ppn. 23 patients were revised to titanium sleeve with ceramic heads and all had improvement of their symptoms and a decrease in their metal ion levels.
Explanation
OrthoCash 2020
A 66-year-old patient is planning to undergo a right total knee arthroplasty. Figure A demonstrates the preoperative radiograph. Placing the components in a kinematic alignment (compared to neutral mechanical alignment) would result in which of the following?

Increased aseptic loosening
Varus tibial cuts and valgus femoral cuts
Lower rates of patient satisfaction
Decreased ROM
Increased reoperation rate
Kinematic alignment total knee arthroplasty is based on component placement to recreate a patient's natural anatomy. In the case of this patient, this would involve varus tibial cuts and valgus femoral cuts.
Kinematic alignment total knee arthroplasty is based on the principle of re-establishing a patient's natural anatomy. Many patients develop constitutionally varus or valgus knee alignment, in which placement of the arthroplasty components in relative varus or valgus positions would lead to symmetric mediolateral loading of the implants. This principle is further based on the idea that placing the components in neutral alignment may align the limb in an abnormal position to the patient, which may lower patient satisfaction. For varus knees, this implies varus tibial cuts with valgus femoral cuts.
Bellemans et al. performed an observational study of 250 asymptomatic study participant to determine what percentage of the population has constitutionally varus knee alignment. The authors found that 32% of males and 17.2% of females had constitutionally varus aligned knees. Furthermore, constitutionally varus knees were associated with greater physical activity during the second decade of life, believed to be secondary to Heuter-Volkmann loading of the open physis.
Lee et al. performed a systematic review of the literature comparing neutral alignment and kinematic alignment arthroplasty. Generally, the literature supported that ROM, KSS and WOMAC scores were equivalent, if not better, in kinematically aligned knees. Further, tibial components were in more varus and femoral components in more valgus. There were no differences in reoperation rates.
Figure A demonstrates a mechanical axis view radiograph with varus alignment of bilateral knees and medial compartment osteoarthritis. Illustration A demonstrates the difference in bone cuts between neutral alignment and kinematic alignment arthroplasty.
Incorrect Answers:

OrthoCash 2020
A 68-year-old patient with diabetes progressively worsening left knee pain of 6 months duration. They underwent a left total knee arthroplasty 7 years ago. Figures A-B demonstrate the current radiographs. Aspiration of the left knee demonstrated 11,500 WBCs and 94% neutrophils. Aspiration cultures grew methicillin-resistant Staphylococcus aureus. What would be the best treatment approach for this patient?
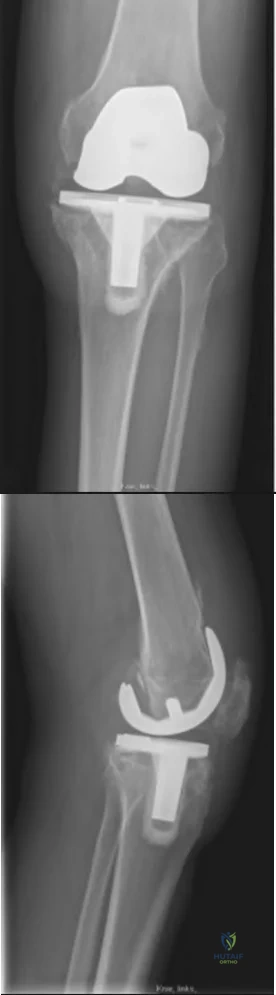
Knee arthrodesis
Long-term antibiotic suppression
One-stage revision arthroplasty
Two-stage revision arthroplasty
Above knee amputation Corrent answer: 4
The patient has several medical comorbidities and is presenting with a chronic prosthetic joint infection with a virulent organism (MRSA). The best treatment option at this time would be a two-stage revision arthroplasty.
Chronic prosthetic joint infections occur greater than 3-6 weeks from surgery and result in biofilm formation over the prosthesis, making antibiotic treatment alone ineffective for infection eradication. Diagnosis is based on the MSIS criteria, with chronic infections being suggested with CRP greater than 10, ESR greater than 30, and synovial WBCs greater than 1,100. Two-stage revision arthroplasty is the current gold standard in the United States for treating chronic prosthetic joint infections.
Kuzyk et al. 2014 reviewed two-stage revision arthroplasty for chronic periprosthetic joint infections. The authors stated that there is no consensus on laboratory and histology criteria to confirm eradication prior to proceeding with the second stage. The authors recommend holding IV antibiotics for two weeks and repeated inflammatory markers to evaluate whether to proceed with the second stage and to perform frozen section at the time of the procedure.
Nguyen et al. 2016 reviewed one-stage revision arthroplasty for the treatment of periprosthetic joint infections. The authors reported that in select patients, one-stage revision arthroplasty can have equal if not better outcomes compared to two-stage revision with less surgical morbidity and improved functional outcomes. They concluded that one-stage revision arthroplasty can be successful in patients that are not immunocompromised, minimal medical comorbidities, known pathogen prior to surgery, non-polymicrobial, no virulent pathogen (MRSA), and with good soft tissue coverage.
Figures A and B demonstrate AP and lateral radiographs of the right with radiolucencies present around the tibial and femoral prosthesis. Illustration A demonstrates a treatment algorithm proposed by Kuzyk et al. for proceeding with the second stage of a two-stage revision. Illustration B demonstrates the Musculoskeletal Infection Society diagnostic criteria for a prosthetic joint infection. Illustration C depicts specific lab values for diagnosing a prosthetic joint infection.
Incorrect Answers:
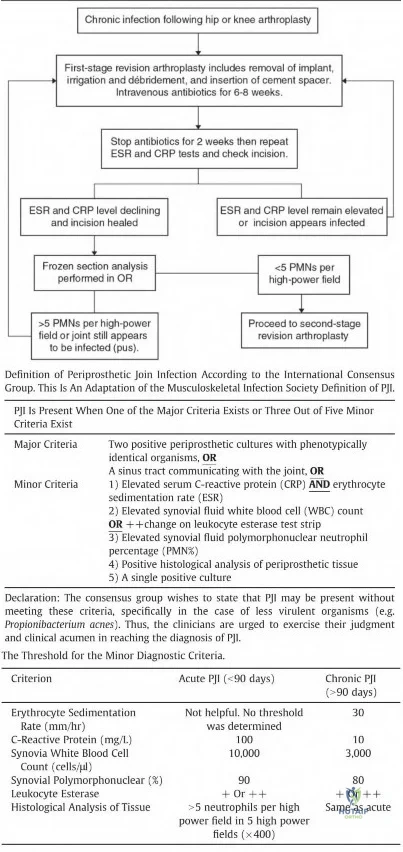
OrthoCash 2020
A 77-year-old patient presents with progressively worsening right hip pain and limp. The patient underwent a right revision total hip arthroplasty 15 years ago and is now unable to ambulate due to the pain and feels as if the hip is unstable. The patient's radiograph is shown in Figure 1. Which of the following is the appropriate classification and best treatment approach for this patient?

Paprosky 2A; multihole cup with posterior column plating
Paprosky 2B; antiprotrusio cage with structural allograft
Paprosky 3A; distraction arthroplasty
Paprosky 3B; custom triflange cup
Paprosky 3B; cemented cup Corrent answer: 4
The patient is presenting with pelvic discontinuity due to severe acetabular bone loss and superomedial cup migration consistent with Paprosky 3B
acetabular deficiency and pelvic discontinuity. Revision to a custom triflange cup would be a viable treatment approach.
Pelvic discontinuity in revision total hip arthroplasty is a rare treatment challenge due to extensive bone loss from osteolysis and prior surgery. Typically, the cup migrates superomedial towards the pelvic viscera and can place neurovascular structures at greater risk. This defect is classified as type 3B in the Paprosky classification. Treatment involves restoring pelvic stability through the healing of the anterior and posterior columns as well as reconstituting hip biomechanics with custom triflange cups, posterior column plating, distraction arthroplasty, or augments with highly porous cups.
Taunton et al. performed a multicenter retrospective review of 57 patients that underwent reconstruction of pelvic discontinuity with a custom triflange cup.
The authors found that 81% of patients had a stable implant and healed discontinuity at final follow-up with implant cost being comparable to off-the-shelf options. The authors concluded that that custom triflange cup provides adequate fixation with good outcomes at a comparable cost to other fixation methods.
Jenkins et al. performed a retrospective review of 58 hips, of which 11 had pelvic discontinuity, that underwent revision with a tantalum porous cup and augments. The authors reported a high rate of radiolucency in Delee and Charnley zone III and implant failure in patients with pre-operative pelvic discontinuity that were revised with this technique. The authors recommend the use of alternative or adjunctive fixation in patients with pelvic discontinuity.
Regis et al. performed a retrospective review of 18 patients that underwent revision with antiprotrusio cage and bulk allograft for pelvic discontinuity. The authors found a 72.2% survival rate at 16.6 years with cases of failure demonstrating graft resorption and acetabular loosening. The authors suggested that bulk allografting with antiprotrusio cages provide an effective means to address pelvic discontinuity.
Figure A demonstrates an AP radiograph of the pelvis with pelvic discontinuity. Illustration A depicts the Paprosky classification system. Illustration B depicts the DeLee and Charley as well as the Gruen zones.
Incorrect Answers:
pelvic discontinuity in such a manner to allow for healing of the anterior and posterior columns. Furthermore, cemented cups are associated with high loosening rates.
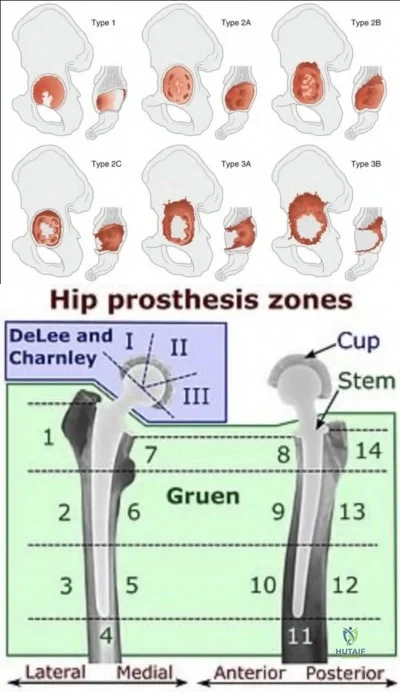
OrthoCash 2020
A 75-year-old male sustains a ground-level fall while ambulating at home. The patient has been optimized for surgical intervention. Both prosthetic components are deemed to be stable. How would you classify this fracture and what is the appropriate treatment plan?

Vancouver B1; ORIF with a lateral locking plate
Vancouver C; revision of femoral stem from hip component
Vancouver C; retrograde intramedullary nail
Vancouver B2; revision to long stem total knee component
Vancouver C; ORIF with a lateral locking plate Corrent answer: 5
This patient has a Vancouver C periprosthetic fracture about stable total hip and knee arthroplasties (an interprosthetic fracture) which can be appropriately fixed with a lateral locked plate spanning the entire femur.
The success of prosthetic surgery has led to an increase in the percentage of the population having more than one prosthetic implant. This, combined with an increase in the average life expectancy and functional requirements for the elderly, has led to a higher incidence of periprosthetic and interprosthetic fractures. Treatment must be determined and assessed according to the type of fracture, the stability of the prosthesis, the bone quality and the general condition of the patient. When the implants are stable plate fixation spanning both of the prostheses has shown favorable results. Some surgeons advocate for nail/plate combination fixation in these interprosthetic fractures in an attempt to allow early weight-bearing.
Froberg et al. reviewed 60 consecutive periprosthetic Vancouver B1 or C fractures, all fixed with plate osteosynthesis. There were a total of 8 reoperations, 4 of which were for infection and 3 for fixation failure. They conclude that locking-plate osteosynthesis of periprosthetic Vancouver type B1 and C fractures gives good results in terms of fracture union. It appears that spanning of the prosthesis to avoid stress-rising areas is important for successful treatment. Infection remains the major cause of failure.
Hoffmann et al. reviewed interprosthetic femoral fractures, defined as fractures between an ipsilateral total knee and hip arthroplasty. 27 patients were designated as having interprosthetic fractures and were treated with locked plating. They conclude that locked plating can achieve satisfactory results. Additional soft tissue damage can be prevented by submuscular plate insertion. Treatment of type B fractures resulted in significantly greater nonunion rate.
Matlovich et al. reviewed fifty-seven patients treated for supracondylar periprosthetic femur fracture with either a locking plate (n = 38) or IM nail (n
= 19). There was no statistical difference between groups in the meantime to fully weight bear, the incidence of postoperative pain, range of motion, use of gait aids, time to full radiographic union, or the overall radiographic alignment of a healed fracture. Despite this, they add caution is recommended in using IM nails for fractures below the flange where limited fixation may increase the risk of nonunion.
Figure A demonstrates a Vancouver C interprosthetic fracture with well-fixed total hip and knee components.
Illustration A is an example of another patient status-post ORIF of an interprosthetic femur fracture.
Incorrect answers:

OrthoCash 2020
A 61-year-old man with left hip OA presents to clinic for persistent left hip pain despite a trial of conservative therapy. The decision is made to proceed with total hip arthroplasty via a direct anterior approach. Which of the following correctly describes the superficial internervous plane of this approach?
Rectus femoris (femoral n.) & tensor fascia lata (superior gluteal n.)
Tensor fascia lata (femoral n.) & sartorius (superior gluteal n.)
Rectus femoris (femoral n.) & gluteus medius (superior gluteal n.)
Sartorius (femoral n.) & gluteus medius (superior gluteal n.)
Sartorius (femoral n.) & tensor fascia lata (superior gluteal n.) Corrent answer: 5
The direct anterior approach to the hip is performed using the internervous interval between the sartorius (femoral n.) and tensor fascia lata (superior gluteal n.) superficially.
Total hip arthroplasty using a direct anterior approach has become increasingly
popular, with many studies showing good long-term results. It is performed through the internervous plane between the femoral nerve and superior gluteal nerve, superficially between the sartorius and TFL, and deep between the rectus femoris and gluteus medius. Advantages of the direct anterior approach include preservation of the abductor mechanism and decreased dislocation rates compared to the posterior approach. However, this approach has a steep learning curve and its use is limited in obese patients with a large pannus. Additionally, this approach places the lateral femoral cutaneous nerve at risk and may lead to increased intraoperative fracture rates.
Bohler et al. published a review on the direct anterior approach to the hip. They report that this approach allows for direct visualization of the acetabulum and offers a complete intermuscular and internervous access to the hip joint.
They found that the approach allows for decreased muscular trauma, intraoperative blood loss, and post-operative rehabilitation.
Post et al. published a review on the indications, technique, and results of the direct anterior approach for THA. They report that the steep learning curve and complications unique to this approach (fractures and nerve damage) have been well described; however, the incidence of these complications decreases with greater surgeon experience.
Illustration A is a diagram depicting the superficial internervous plane of the direct anterior approach to the hip.
Incorrect Answers:
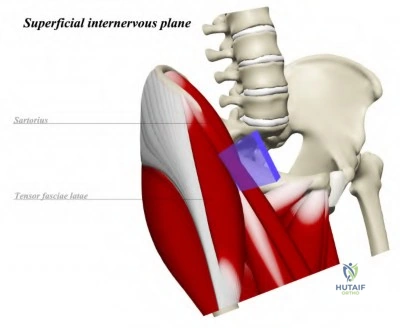
OrthoCash 2020
A 45-year-old male presents with increasing left groin pain. He has a history of bilateral hip avascular necrosis and underwent bilateral hip resurfacing arthroplasties 3 years ago. He is a recreational runner and recently ran a 10-kilometer race several weeks ago. Figure A demonstrates an AP radiograph of his pelvis. Serum testing demonstrated a cobalt level of 10 mcg/L (reference 0.8
- 5.1 mcg/L) and chromium level of 7 mcg/L (reference 0.5 - 2.5 mcg/L). What is the likely cause of the patient's symptoms?
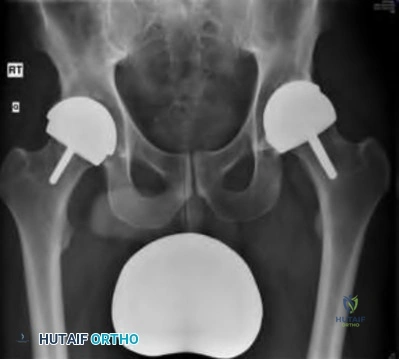
Iliopsoas tendonitis
Edge-loading
Prosthetic joint infection
Increased activity-related wear
Femoral neck stress fracture Corrent answer: 2
The patient is presenting with increased left hip pain after bilateral Birmingham Hip Resurfacing (BHR) arthroplasties and elevated ion levels consistent with metallosis. The most likely cause of metallosis in this patient is the edge-loading of the implant.
Hip resurfacing arthroplasty is a bone preserving procedure that is favorable in young male patients and utilizes metal-on-metal articulations. Metallosis is, therefore, a concerning complication of these implants and can result in pseudotumor formation and subsequent destruction of the hip abductors.
Patients presenting with a painful prosthesis should be screened with metal ion levels as well as a metal artifact reduction sequence MRI. Possible causes of metallosis include edge-loading, component malpositioning, third bodywear, impingement, and sensitivity to cobalt.
Brooks performed a retrospective review of patients undergoing BHR with regards to outcomes. The author found a 0.23% rate of metallosis in the study population, with all cases being attributed to edge-loading. The author recommended a preoperative CT scan and lateral pelvic radiographs to prevent component malposition and better identify surgical candidates.
Matharu et al. performed a prospective cohort study examining metal ion levels in patients with bilateral BHRs. The authors found that cobalt, chromium, cobalt-chromium ratio, and maximum cobalt and chromium levels to be significantly higher in patients with metallosis. They recommended using a cut-off of 5.7 mcg/L for cobalt and 5.5 mcg/L for chromium for metallosis in patients with bilateral BHRs.
Figure A demonstrates an AP radiograph of a pelvis with bilateral BHR implants and an increased inclination angle of the left acetabular component.
Incorrect Answers:
OrthoCash 2020
An ambulatory 57-year-old man with post-polio syndrome presents for follow-up of his right knee pain. He has failed all nonoperative measures for his right knee pain. On exam, he hyperextends to 15° and flexes to 120° with global instability of the knee. He has maintained antigravity strength in the right limb. Radiographs are shown in Figures A and B. What is the best treatment option for this patient?

Cruciate retaining knee with ligamentous reconstruction
Robotic-assisted posterior stabilized total knee arthroplasty
Distal femoral osteotomy with total knee arthroplasty
Hinged total knee arthroplasty
Above-knee amputation
The best treatment for this patient with post-polio syndrome is a hinged total knee arthroplasty.
Patients affected by the 1950 poliomyelitis outbreak are now approaching an age where degenerative knee changes are impacting their quality of life. These patients often have global instability and significant hyperextension deformity and require a hinged prosthesis. Any less constrained components put the patient at risk for continued instability and early failure. Patients with maintained antigravity strength in the operative limb may have improved outcomes in the setting of post-polio syndrome.
Gan et al. reviewed 16 knee replacement in patients with post-polio syndrome and degenerative knee changes. They found an improvement in the mean of all outcomes scoring measures including the AKSS, Oxford knee scores, AKSS pain scores, and SF-36 scoring. They concluded that primary knee arthroplasty for patients with post-polio syndrome shows a good improvement in patients quality of life and decreases pain.
Giori et al. retrospectively reviewed 16 patients with a history of poliomyelitis and a history of primary total knee arthroplasty. They found four cases of recurrent instability, two of which had a preoperative hyperextension deformity of 20 degrees. They concluded that pain and knee scores improved in these patients and that recurrent instability or functional deterioration occurred more often in the most severely affected knees. They recommend consideration of hinged arthroplasty or arthrodesis in this challenging subgroup of patients.
Figures A and B are AP and lateral radiographs of the right knee showing and severe valgus-hyperextension deformity and degenerative changes in a post-polio limb. Illustrations A and B show an AP and lateral postoperative radiograph following a hinged arthroplasty.
Incorrect Answers:

OrthoCash 2020
When compared to a median parapatellar approach which of the following approaches may lead to higher rates of component malposition?
Quadriceps sparing
Lateral parapatellar
Midvastus
Quadriceps snip
V-Y turndown
A quadriceps-sparing approach has been found to lead to a high rate of component malpositioning.
Improvements in surgical instrumentation and techniques drove surgeons to perform total knees replacement in a less invasive manner. One such technique was the quadriceps-sparing approach which uses minimal subluxation of the patella and special side cutting instruments. This technique was thought to lead to quicker recovery due to the minimal disturbance of the extensor mechanism however, studies have shown that it may lead to statistically significant higher rates of component malposition when compared to a traditional median parapatellar approach.
Kazarian et al. reviewed the outcomes of the quadriceps-sparing (QS) approach compared to a median parapatellar(MP) approach for total knee arthroplasty. They found statistically and clinically significant disadvantages to the QS approach including femoral and mechanical axis outliers, increased surgical time, and increased tourniquet time. They concluded the QS approach does not demonstrate any clinically significant advantages and leads to higher rates of component malalignment.
Kelly et al. randomized 42 consecutive total knee patients to either median parapatellar (MP) approach or a vastus splitting (VS) approach. They found a statistically significant increase in the rate of lateral release and blood loss in the MP approach but showed no difference in functional parameters, tourniquet time, or patellar resurfacing. They conclude the VS approach is a reasonable alternative to the MP approach and may lead to lower rates of lateral releases without impairment of quadriceps function.
Liu et al. compared outcomes of the minimally invasive midvastus (MV) and
subvastus (SV) approaches compared to a traditional median parapatellar (MP) approach for total knee arthroplasty. They found the number of days needed to perform a straight leg raise was significantly longer following MP compared to SV or MV approaches. They conclude that further studies should be performed to assess the outcomes of the various minimally invasive approaches for total knee arthroplasty.
Illustration A shows four different approaches for a total knee arthroplasty including three minimally invasive approaches.
Incorrect Answers:

OrthoCash 2020
A 66-year-old patient that underwent a right total knee arthroplasty approximately 4 years ago presents with worsening right knee pain over the last 48 hours. The patient has a history of rheumatoid arthritis and recently underwent a dental procedure a week ago. Labs were significant for CRP of 212, ESR 105, and a WBC count of 11K. Aspiration yielded a milky-looking fluid with 55K nucleated cells with 97% PMN. Radiographs are shown in Figures A and B. What is the next best step?
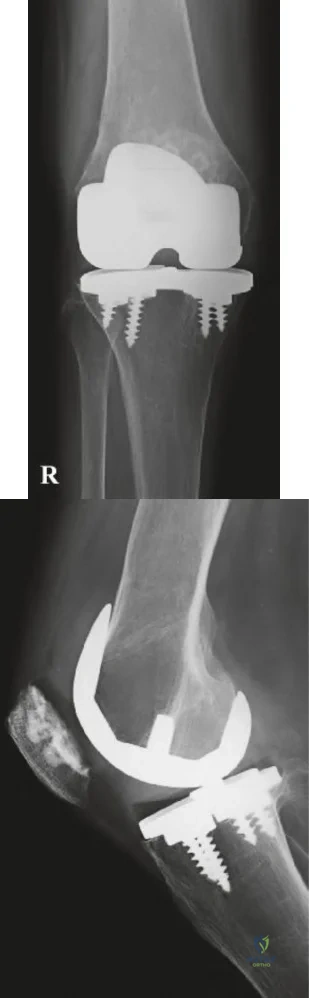
Surgical intervention after cultures finalize
Repeat aspiration of the knee and send for alpha-defensin
Begin IV antibiotics and re-evaluate in 24-48 hours
Proceed with surgical intervention now
IR guided drain placement Corrent answer: 4
The patient is presenting with an acute hematogenous prosthetic joint infection, which requires surgical treatment as soon as safely possible.
Periprosthetic joint infections (PJI) are generally managed surgically. Diagnosis is composed of a battery of findings as established by the Musculoskeletal Infection Society (MSIS), which requires the presence of one of two major criteria or four of six minor criteria (Illustration A). Acute infections can often be treated with irrigation and debridement with polyethylene exchange (IDPE), whereas chronic infections are best managed with a two-stage revision.
Buller et al. performed a retrospective study looking at variable affecting the success of IDPE treatment for PJI. The authors found that infections with MRSA or VRE, higher ESR levels, symptoms longer than 3 weeks, and previous joint infections were strong risk factors for failure of IDPE. The authors
concluded that patients presenting with these characteristics may be best treated with a two-stage revision rather than IDPE.
Figures A and B are AP and lateral radiographs of a right knee with a stable appearing total knee arthroplasty prosthesis. Illustration A is a table that depicts the 2011 MSIS criteria for diagnosing prosthetic joint infections.
Incorrect Answers:
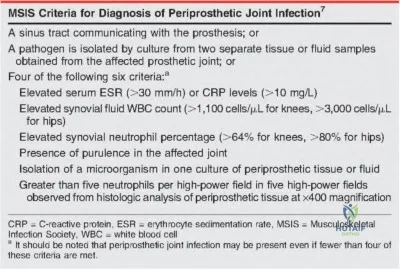
OrthoCash 2020
A 63-year-old patient with a previous right TKA 4 years ago presents with worsening pain in the right knee. The patient reports that pain is worsened when starting physical activity, but is also present at night. Two weeks prior to presentation the patient was given a 1-week course of oral antibiotics for cellulitis affecting the right knee. Serum labs were significant for a CRP of 11 mg/L and an ESR of 35 mm/hr. Synovial fluid analysis revealed 1,000/µL nucleated cells with 85% PMNs and no evidence of crystals. Synovial cultures were negative for any bacterial or fungal growth. Synovial alpha-defensin is positive. Figures A and B are the AP and lateral
radiographs of the right knee. The patient opts to undergo a revision total knee arthroplasty. What is the best management at this point?
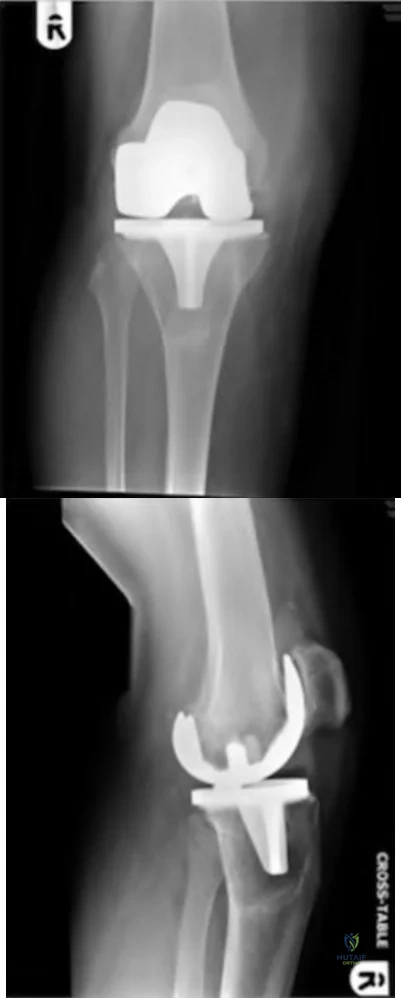
Femoral component revision
Tibial component revision
Polyethylene component revision
One-stage revision of both the femoral and tibial components
Two-stage revision of both the femoral and tibial components Corrent answer: 5
The patient is presenting with increasing knee pain consistent with either septic or aseptic loosening of the prosthesis. Serum and synovial labs are not diagnostic for an infection, but there is a positive synovial alpha-defensin suggesting the presence of a chronic prosthetic joint infection.
Prosthetic joint infections are diagnostic challenges as there is no single confirmatory test. Rather, diagnosis is composed of a conglomerate of physical and laboratory findings as laid forth by the Musculoskeletal Infection Society criteria. Diagnosis can be made by either the presence of one major criterion or four minor criteria. Synovial alpha-defensin is a new assay that tests for the presence of an antimicrobial peptide that is part of the innate immune system. Recent studies have suggested a high sensitivity and specificity of this test for prosthetic joint infections, even with prior antibiotic administration. Treatment involves two-stage revision arthroplasty with culture-specific antibiotics for at least six weeks. Reimplantation of a prosthesis is done with infection eradication is confirmed.
Shahi et al. performed a retrospective diagnostic study looking at whether prior antibiotic administration affected synovial alpha-defensin levels. The authors found that alpha-defensin was not affected by prior antibiotic administration. The authors concluded that since many patients with PJI will present with prior antibiotic administration, alpha-defensin may be an ideal diagnostic adjunctive test.
Frangiamore et al. performed a prospective cohort study on the sensitivity and specificity of alpha-defensins in diagnosing prosthetic joint infections. The authors found that alpha-defensin has a sensitivity and specificity of 100% and 98%, respectively, for diagnosing PJI in single-stage and first-stage revisions. The authors concluded that alpha-defensin has the potential as a useful adjunct in diagnosing PJI.
Figures A and B demonstrate AP and lateral radiographs of the right knee with loosening of the tibial and femoral components. Illustration A depicts the MSIS criteria for the diagnosis of PJI.
Incorrect Answers:
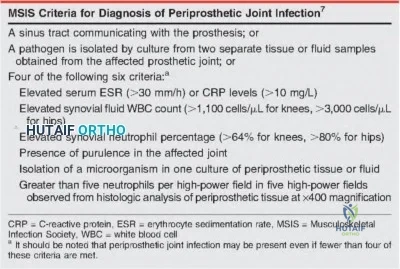
OrthoCash 2020
Of the following, which has the highest strength of recommendation according to the AAOS Clinical Practice Guidelines (CPG) for Surgical Management of Osteoarthritis of the Knee?
Preoperative physical therapy improves pain and physical function postoperatively
Tourniquet use during total knee arthroplasty (TKA) decreases short-term postoperative function
Continuous passive motion (CPM) after TKA improves outcomes
Rehabilitation started on the day of TKA reduces length of hospital stay
Surgical navigation should be used because there is a decrease in pain and functional outcomes
Rehabilitation started on the day of TKA decreasing length of stay has been deemed a "strong recommendation" by the AAOS.
Postoperative management following TKA is an important aspect of achieving an optimal outcome following total knee arthroplasty. The general recommendation is that patients should work with a physical therapist on the
day of surgery or as early as possible as it will decrease pain and improve function. Early rehabilitation is felt to also decrease the length of stay.
Recommendations against cryotherapy machines and CPM are moderate and strong, respectively, as they do not appear to improve outcomes.
McGrory et al. present the AAOS CPG's for surgical management of osteoarthritis of the knee. Strong evidence supports postoperative rehabilitation started on the day of surgery, which has been shown to decrease the length of stay. Moderate evidence supports rehabilitation starting the day of surgery compared to postoperative day 1 reduced pain and improves function. Various other preoperative and intraoperative topics are reviewed for the corresponding strength of recommendation.
Incorrect Answers:
OrthoCash 2020
A 62-year-old patient that underwent a right hip resurfacing arthroplasty 3 years ago develops worsening right hip pain over the past 6 months. The pain is present at all times, including at night. The patient does not walk with a Trendelenburg gait and does not have reproducible pain on hip examination. Laboratory inflammatory markers from 1 week ago were erythrocyte sedimentation rate of 66 mm/hr (reference <20 mm/hr), C-reactive protein of 22 mg/dL (reference <2.5 mg/dL), cobalt 0.5 µg/L (reference <0.7 µg/L), and chromium of 0.4 µg/L (reference <0.4 µg/L). Figure A demonstrates an AP radiograph of the pelvis. What is the next best step in management?

Physical therapy
Routine follow-up
Arthrocentesis with synovial fluid analysis
stage revision
Metal artifact reduction sequence MRI Corrent answer: 3
The patient is presenting with a painful right hip after a metal-on-metal arthroplasty with recent elevated inflammatory markers and normal metal ion levels. The best next step in diagnostic workup would include an arthrocentesis with synovial fluid analysis.
Diagnosis of chronic prosthetic joint infections is challenging due to the requirement of a conglomerate of physical and laboratory findings for the diagnosis. The most common presenting symptom is pain in the affected joint, but there may be draining sinus tracts and systemic inflammatory signs.
Work-up should start with serum inflammatory markers, which if elevated should prompt an arthrocentesis with synovial fluid analysis. If the diagnosis is still not clear a repeat aspiration can be performed or frozen section performed in the operating room. It is important in aspiration of metal on metal joints to request manual cell counts as the metal debris can often result in faulty automated counts.
Connelly et al. performed a prospective cohort study of indications for performing metal artifact reducing sequence (MARS) MRI on patients with metal-on-metal hip resurfacing arthroplasty. They found that elevated cobalt and chromium were the strongest predictors for an adverse local tissue reaction and using 1.15 ppb of Co and 1.09 ppb for chromium as cut-offs for
performing a MARS MRI.
Yi et al. performed a retrospective study evaluating the diagnostic accuracy of serologic and synovial tests for PJI in MoM hip arthroplasty. The authors found that a high rate of inaccurate reporting of MoM aspirations, with 35% of inaccurate reports having a synovial WBC count >3000 suggesting a false positive for infection. The authors concluded that using synovial WBC >4350 and PMN >85% provided greater diagnostic sensitivity and specificity than standard MSIS criteria.
Figure A demonstrates an AP pelvis radiograph with a stable appearing right hip resurfacing arthroplasty.
Incorrect answers:
OrthoCash 2020
Compared to a cruciate retaining knee prosthesis, an anterior stabilized prosthesis has what effect on the contact area and what effect on the stability in PCL deficient knees?
Decreased contact area; increased stability
Increased contact area; increased stability
No change in contact area; no change in stability
Decreased contact area; decreased stability
Increased contact area; decreased stability Corrent answer: 2
An anterior stabilized knee prosthesis is composed of highly conformed polyethylene component with a large anterior lip, which prevents anterior translation of the femur on the tibia. The high conformity of the polyethylene component increases the contact area of the implant.
In arthroplasty, several factors can affect wear characteristics and stability at the bearing surface. Articular surfaces that are more congruous decrease the contact stresses at the surface by dispersing the joint reactive forces across a greater area. There are drawbacks to this as the articular surface is less anatomic and can prevent the natural roll back kinematics in total knee arthroplasty. New prosthesis designs with a large anterior lip formed on the bearing can be used to stabilize the knee in the absence of a functional PCL without sacrificing bone stock for the box cut and potential patellar complications.
Peters et al. performed a retrospective cohort study of total knee arthroplasty outcomes between cruciate retaining prostheses in intact PCL knees and anterior stabilized bearing prostheses in PCL deficient knees. They found that anterior stabilized bearing prostheses had similar knee society scores, radiographic alignment, component loosening, and major complications but had a significantly lower number of revisions performed. They concluded that the use of anterior stabilized bearings is an effective implant to stabilize PCL deficient knees.
Brockett et al. performed a biomechanical study that examined wear characteristics of poly-ether-ether-ketone (PEEK) and carbon fiber reinforced PEEK (CFR-PEEK) and compared to ultra-high molecular weight polyethylene (UHMWPE). It was found that PEEK had worse wear characteristics compared to UHMWPE, specifically with increasing contact pressures, decreased contact surface, and increased cross-shear. However, CFR-PEEK had similar wear performance as UHMWPE, but there were increased wear characteristics with increasing shear and contact pressure. They concluded that CFR-PEEK may be a potential alternative bearing surface in arthroplasty, but further investigation is needed to determine it's role in less conforming bearing due to the increased shearing wear.
Illustration A depicts the design of a cruciate retaining total knee prosthesis and an anterior stabilized total knee prosthesis.
Incorrect Answers:
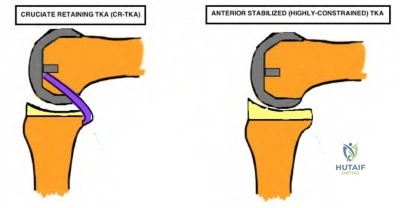
OrthoCash 2020
Resection of the posterior cruciate ligament during total knee arthroplasty simulates which of the following techniques below?
Excessive distal femur resection
Excessive distal femur augmentation
Excessive posterior femur resection
Excessive posterior femur augmentation
Oversized femoral component Corrent answer: 3
Posterior cruciate ligament (PCL) resection during total knee arthroplasty (TKA) results in a relative increase in the flexion gap compared to the extension gap. This effect simulates excessive posterior femur resection, which also results in an increased flexion gap.
The PCL acts as a central stabilizer to prevent posterior subluxation, allows femoral condyle roll back on the tibial plateau during flexion, and permits clearance of the tibia in high degrees of flexion to improve the mechanical efficiency of the extensor mechanism. The PCL may be preserved or resected during TKA. Biomechanical studies have demonstrated that after PCL resection, the flexion gap increases significantly compared with the extension gap. This has implications on gap balancing during posterior-stabilizing (PS) TKA, as the flexion gap must match the extension gap.
Park et al. performed a study to investigate the change in the medial-lateral gap in flexion and extension after PCL resection in severely deformed knees and its effect on bone resection, rotation, and size of the femoral component. They reported that after PCL resection, the flexion gap increased significantly compared with the extension gap. They concluded that PCL resection in PS-TKA designs necessitates an increase in the size of the femoral component to
balance the resulting gap mismatch.
Sierra et al. published an article on the surgical technique differences between cruciate-retaining (CR) and PS TKA designs. They reported that PCL resection selectively opens the flexion space approximately 2mm more than the extension space, resulting in some flexion instability. They recommended that in PS-TKA, surgeons must avoid flexion instability due to an extra large flexion space caused by PCL sacrifice and postoperative knee flexion contracture by underresection of the distal femur.
Incorrect Answers:
OrthoCash 2020
A 70-year-old healthy woman presents with recurrent left prosthetic hip dislocations after undergoing total hip arthroplasty 6 months ago. Workup for infection has been negative. Radiographs from her visit today are depicted in Figure A. Which of the following will most definitively prevent further dislocations?

Exchange polyethylene liner to a lipped acetabular liner
Exchange polyethylene liner to a thinner liner and increase the size of femoral head component
Cemented acetabular component revision
Uncemented acetabular component revision
Exchange polyethylene liner to a constrained acetabular liner Corrent answer: 4
This patient appears to have a significantly increased acetabular abduction (theta) angle, which places her at a high risk of periprosthetic dislocation. She should undergo revision of her malpositioned acetabular component to prevent further dislocation events.
Variables that help determine stability after total hip arthroplasty (THA) include component design, component position, soft tissue tension, and soft tissue function. The component position comprises of both femoral and acetabular implants. The recommendations are femoral component anteversion of 10-15 degrees, acetabular anteversion of 5-25 degrees, and acetabular abduction of 30-50 degrees. Excessive abduction may result in posterosuperior instability whereas inadequate abduction may result in impingement during flexion as well as inferior instability. Component malposition generally requires revision and cannot be compensated for by abductor strengthening or orthoses.
Dewal et al. retrospectively reviewed THA dislocations to determine the effectiveness of abduction bracing following closed reduction. They observed no significant differences in first-time dislocators or recurrent dislocators with or without the use of abduction braces. They concluded that abduction bracing following closed reduction of THA dislocation is ineffective in preventing re-dislocation.
McCarthy et al. performed a study to investigate cup position angles associated with impingement in a group of subjects during different activities. They reported that true acetabular target for impingement-avoidance is much smaller than previously believed and varies considerably between patients and that certain tasks including low-chair rise and squatting decrease the size of the target zone. As such, they recommended preoperative patient-specific planning and intraoperative execution for placement of the components.
Figure A depicts a THA construct with significantly increased acetabular abduction angle.
Incorrect Answers:
OrthoCash 2020
A 65-year-old woman with a history of right total hip arthroplasty presents with a fall. Her injury radiographs are depicted in Figure A. What are the fracture classification and most appropriate treatment?

Vancouver AG; nonoperative with partial weight bearing
Vancouver AG; open reduction internal fixation with trochanteric claw plate
Vancouver AG; femoral component revision
Vancouver AL; open reduction internal fixation with trochanteric cables
Vancouver B1; open reduction internal fixation with lateral locking plate Corrent answer: 2
This patient has a displaced (> 2cm) greater trochanteric periprosthetic fracture around her previous right total hip arthroplasty (THA). Her fracture is classified in the Vancouver classification as AG, and is best treated with open reduction internal fixation (ORIF) using a trochanteric claw plate.
The Vancouver hip periprosthetic classification system is one of the most useful classifications in the field of orthopaedic surgery, as it can reliably guide decision-making regarding fixation versus revision of the femoral component. Vancouver A fractures confer fractures about the femoral trochanters, with AG and AL fractures depicting greater and lesser trochanters, respectively. While nondisplaced and minimally displaced (<2cm) Vancouver AG fractures may be managed nonoperatively with protected weight-bearing, displaced AG fractures should be treated with ORIF using wires, cables, or claw plates.
Sariyilmaz et al. performed a biomechanical study to compare fixation techniques (cables, trochanteric grip plates, and locking plates) in Vancouver
type AG periprosthetic femoral fractures. They reported that locking plate versus cable fixation and grip plate fixation versus cable fixation showed statistically significant superior results in axial distraction tests. They concluded that Vancouver type AG fractures may be treated with either grip plate fixation or locking plates, with the former ensuring more stable osteosynthesis.
Masri et al. published a review article on the evaluation and management of periprosthetic fractures. They reported that the best outcome is achieved when the surgeon has a thorough understanding of the principles of treatment of periprosthetic fractures with access to various fixation and prosthetic devices. They concluded that the Vancouver classification offers a reproducible description of these factors and easily guides treatment.
Figure A depicts a displaced greater trochanteric periprosthetic fracture. Illustration A depicts the Vancouver periprosthetic hip classification system. Illustration B depicts an example of a Vancouver AG fracture treated with ORIF using a claw plate.
Incorrect Answers:
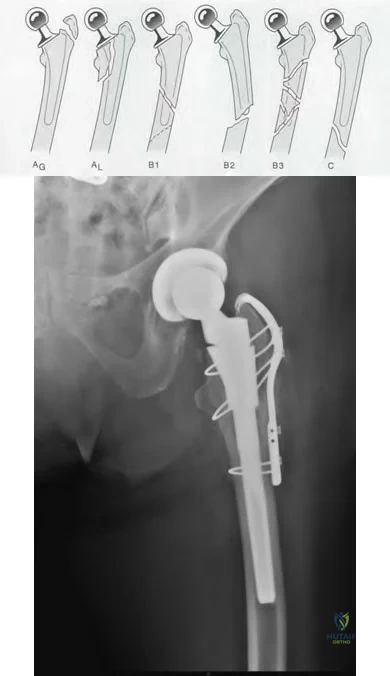
OrthoCash 2020
A 79-year-old man sustains a fall and presents with the injury depicted in Figures A and B. He underwent total knee arthroplasty (TKA) 5 days ago and had been doing well prior to his recent fall. What is the TKA implant design and what is the most appropriate treatment?
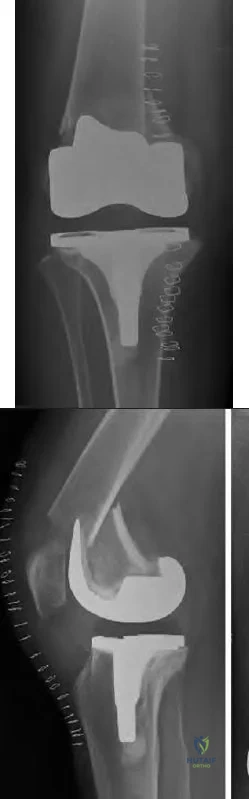
Cruciate-retaining; Open reduction internal fixation with lateral locking plate
Cruciate-retaining; Retrograde femoral nail
Cruciate-retaining; Open reduction internal fixation with medial locking plate
Posterior-stabilized; Open reduction internal fixation with lateral locking plate
Posterior-stabilized; Femoral component revision Corrent answer: 4
The TKA prosthesis in question is a posterior-stabilized (PS) design. Open reduction and internal fixation (ORIF) with a lateral locking plate is a viable treatment option for a periprosthetic femur fracture around the femoral component of a well-fixed PS TKA.
Femoral periprosthetic fractures after TKA may occur following low-energy trauma in osteopenic bone. Nondisplaced fractures with a stable prosthesis may be treated nonoperatively in a cast or brace. The decision for revision of the femoral component is guided by component stability versus loosening, with ORIF and revision arthroplasty indicated, respectively. ORIF options include locked femoral plating or retrograde intramedullary nailing (IMN).
Retrograde IMN is not a viable option for stemmed femoral prosthesis and posterior-stabilized (PS) TKA systems without an open box design.
Haidukewych et al. published an instructional course lecture on periprosthetic
fractures of the hip and knee. They reported internal fixation is indicated for the majority of periprosthetic distal femoral fractures. Both locked plates and retrograde IMNs can provide good outcomes, and that revision arthroplasty is indicated in fractures around loose components, nonunions, or fractures for which internal fixation attempts are likely to fail.
Su et al. published a review on periprosthetic femoral fractures above total knee replacements. They reported that periprosthetic femoral fractures above TKAs can be managed by a variety of methods, including casting, ORIF, external fixation, or revision arthroplasty. They highlighted that classification based on fracture location helps guide treatment. They concluded that IMNs are best for proximal fractures, fixed-angle devices for fractures originating at the component, and revision arthroplasty for very distal fractures or those with component loosening.
Figures A and B depict a periprosthetic femoral fracture originating at the anterior flange of the femoral component of a PS-TKA. Illustrations A and B depict radiographs of the periprosthetic femur fracture after ORIF with a lateral locking plate.
Incorrect Answers:

OrthoCash 2020
A 67-year-old woman presents with chronic right hip pain, exacerbated by long walks. She has limited hip range of motion, particularly in flexion and internal rotation. Radiographs are depicted in Figure A. This is her first time seeking treatment. What is the mechanism of action of a medication strongly recommended for short-term pain relief according to the most recent (2013) AAOS Clinical Practice Guidelines?

Direct action on hypothalamic regulating center with anti-pyretic effects
Binds to cannabinoid receptors in neural tissues
Binds directly to nuclear receptors to interrupt the inflammatory and immune cascade via mRNA changes
Maintains synovial fluid viscosity and supports articular cartilage shock absorption
Inhibits sodium ion channels to inhibit sensory nerve impulse initiation and conduction
This patient presents with right hip osteoarthritis. In the 2013 AAOS Clinical Practice Guidelines (CPG), intraarticular corticosteroids usage in improving function and pain reduction in the short-term for patients with symptomatic osteoarthritis of the hip was strongly recommended. Corticosteroids function by direct binding to nuclear steroid receptors to interrupt the inflammatory cascade through mRNA changes.
The 2013 AAOS CPG for the treatment of symptomatic arthritis discuss both operative and non-operative treatment options and scrutinizes the literature for each modality. Amongst the strong recommendations are weight loss, low impact physical activity, and non-narcotic analgesia including nonsteroidal anti-inflammatory drugs (NSAIDs). Numerous modalities were not supported including the use of prescription opioids, acupuncture, needle lavage, hyaluronic acid, glucosamine and chondroitin, and arthroscopic lavage.
Dieppe et al. published a review article on the management of hip osteoarthritis. They reported that shock absorbing shoe insoles and walking sticks can be of great benefit, while physiotherapy and hydrotherapy should be considered for more severe cases. They recommended simple analgesics such as paracetamol and NSAIDs as first-line treatment, with joint replacement considered in patients with severe pain or disability.
Quinn et al. published a review article on the management of hip osteoarthritis using the AAOS Appropriate Use Criteria (AUC). Evidence-based information, in conjunction with the clinical expertise of physicians, was used to develop the criteria to improve patient care and obtain the best outcomes while considering the subtleties and distinctions necessary in making clinical decisions.
Figure A depicts right hip osteoarthritis with evidence osteophytes, narrowed joint space, and subchondral sclerosis.
Incorrect Answers:
OrthoCash 2020
A 70-year-old man presents with chronic persistent right knee pain and erythema which has been present for 7 weeks after having undergone total knee arthroplasty (TKA) 7 years ago. He is referred after completing a course of oral antibiotics prescribed by his primary care physician, which did not improve his symptoms. His current radiograph is shown in Figure A. Laboratory testing reveals a serum C-reactive protein (CRP) of 50mg/L and an erythrocyte sedimentation rate (ESR) of 67 mm/h. Arthrocentesis is performed and reveals a synovial WBC of 1,500 WBC/uL, with 85% polymorphonuclear cells (PMNs), and negative final cultures. The alpha-defensin test is positive. What is the next best step?

Repeat knee arthrocentesis after 2-week antibiotic holiday
Revision of femoral component without antibiotic therapy
One-stage revision arthroplasty with intravenous antibiotic therapy for 4-6 weeks
Two-stage revision arthroplasty with intravenous antibiotic therapy for 4-6 weeks
Revision of tibial component without antibiotic therapy
Based on the 2018 revised Musculoskeletal Infection Sociecty (MSIS) criteria, the elevated ESR, serum CRP, positive alpha defensin, and elevated PMNs convey a score of 1, 2, 3, and 2, respectively, for a combined score >6. This is diagnostic of a chronic prosthetic joint infection (PJI), for the most supported management strategy is two-stage revision arthroplasty with intravenous (IV) antibiotic therapy for 4-6 weeks.
PJI after TKA is estimated to be 2.5%. The chronicity of the infection determines management. Non-MRSA PJI within 4 weeks of surgery is considered acute and may be treated with irrigation, debridement, polyethylene exchange, component retention, and IV antibiotics, as the organism has purportedly had too little time to form a robust biofilm. PJI occurring more than 4 weeks after TKA is considered chronic and, due to a high likelihood of biofilm formation, requires two-stage revision arthroplasty with IV antibiotic therapy.
Ting et al. reviewed an algorithm-based approach for diagnosis of PJI. They reported that the diagnosis of PJI is made in 90% of patients by ESR and CRP, followed by arthrocentesis if the results are high, with a focus on synovial WBC count, differential, and cultures.
Everhart et al. developed and validated a preoperative surgical site infection (SSI) risk score for primary or revision TKA and hip arthroplasty (THA). They reported that patient comorbidities composing the risk significantly influence SSI risk for primary or revision TKA and THA. They concluded that preoperative SSI risk can be objectively determined by the proposed SSI risk score.
Parvizi et al. most recently presented the 2018 updated MSIS evidence-based criteria for diagnosis of periprosthetic hip and knee infections (Illustration A). The authors updated the original crtieria, expanding and refining the contributions from each of the minor criteria. The authors supported that a score >6 was diagnostic of periprosthetic infection. They concluded that this criteria was 97.7% sensitive and 99.5% specific for diagnosis of prosthetic joint infection.
Figures and Illustrations:
Figure A shows the AP and lateral radiographs of a TKA prosthesis with evidence of osteolysis and marked loosening of the femoral and tibial components.
Illustration A is the updated 2018 MSIS criteria for diagnosis of a PJI.
Incorrect Answers:
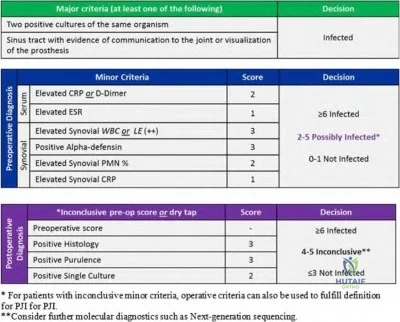
OrthoCash 2020
Figure A depicts the intraoperative findings during a revision total hip arthroplasty (THA) in a patient with chronic pain for the last two years after undergoing his index THA 10 years ago. Workup for infection was negative. The acetabular and femoral components are assessed to be well-fixed intraoperatively. Which of the following describes the best treatment option?
Suppressive intravenous antibiotics
Two-stage revision arthroplasty
Irrigation and debridement
Acetabular component revision
Revision to new ceramic femoral head with titanium sleeve Corrent answer: 5
This patient's symptoms and intraoperative image are consistent with trunnionosis. As the components appear well-fixed, the best treatment is a revision to a ceramic head with a titanium sleeve.
Metal-on-metal (MoM) total hip arthroplasty (THA) has been associated with complications from metal debris and toxicity. Although morse taper technology allows machined taper trunnion to fit with the femoral head, complications have been reported including corrosion at the trunnion, which results in pain and is often associated with adverse local tissue reactions (ALTR). During revision surgery, a ceramic head with a titanium sleeve adaptor is advocated, as an exchange of the metal femoral head to another metal femoral head may result in recurrence of ALTR. Lastly, while no cutoffs for serum cobalt chromium ion levels have been identified as pathognomonic for trunnion corrosion, a serum cobalt level of 1.6 ng/mL (ppb) and greater has been suggested as a threshold for mechanically-assisted crevice corrosion.
Weiser et al. published a current concepts review of trunnionosis in THA. They stated that the complication of trunnionosis in THA is likely underreported since it often causes concurrent osteolysis and loosening, which are more universally accepted diagnoses. They recommended analysis of serum cobalt and chromium ions as well as metal artifact reduction MRI during workup. In revision surgery, they advocated for head and liner exchange, with retention
of the acetabular and femoral components.
Raju et al. published a case series on trunnionosis in metal-on-polyethylene (MoP)THA. They reported three failures (two dissociations of the femoral head from the neck), with the most likely contributing factors to failure being a large femoral head size, high horizontal offset, a low angled neck, and a titanium alloy taper with a cobalt-chromium head. They recommended high vigilance for any alteration of alignment between the femoral head and neck in follow-up radiographs after THA.
Figure A is an intraoperative image depicting severe corrosion at the trunnion in a metal-on-metal THA.
Incorrect Answers:
OrthoCash 2020
Figure A depicts the current radiograph of a 66-year-old man with significant right groin pain after undergoing right total hip arthroplasty (THA) 10 years ago. Revision surgery is planned after infection workup is negative. What is the classification of his diagnosis and what would the most appropriate treatment for the acetabulum?

Paprosky I; cementless hemispheric cup with screw fixation
Paprosky I; cemented hemispheric cup without screw fixation
Paprosky IIB; cementless hemispheric cup with screw fixation
Paprosky IIIA; cup/cage construct
Paprosky IIIA; triflange reconstruction Corrent answer: 3
This patient demonstrates superior acetabular rim loss and superolateral migration that can be characterized as Paprosky IIB in the Paprosky classification for acetabular bone loss. This may be managed with a hemispheric acetabular cup with screw fixation.
Acetabular bone loss poses a technical challenge in THA. The Paprosky classification for acetabular bone loss helps guide treatment for revision THA. Broadly speaking, Paprosky Type I and II defects may be managed with a porous-coated hemisphere cup secured with screws, and Type III defects managed with reconstruction cages protected with cups, structural augments, or custom triflange implants.
Sheth et al. published a review article on the evaluation and management of acetabular bone loss in revision THA. They reported that appropriate radiographs are key in quantifying acetabular bone loss, and specific classification schemes can assist in identifying bone loss patterns which guide available treatment options. They concluded that depending on the severity of bone loss, treatment may include impaction grafting and acetabular cementation, cementless hemispheric acetabular reconstruction, structural allograft reconstruction, cementless reconstruction with modular porous metal
augments, ring and cage reconstruction, cup-cage reconstruction, and triflange reconstruction.
Paprosky et al. performed a 6-year follow up evaluation study on acetabular defect classification and surgical reconstruction in revision THA. They typed acetabular defects from 1 to 3 and reconstructed with bulk or support allograft depending on the type. They concluded that the size, orientation, and method of fixation of the allografts utilized during revision THA play a pivotal role in the integrity of structural allografts, and stressed the importance of adequate host-bone to ensure solid bone ingrowth.
Dennis et al. published on the outcomes after Paprosky Type III acetabular bone loss reconstructed using custom triflanged acetabular components. They reported stable fixation and reconstruction of periacetabular bone in over 80% of patients at short-term follow up. They recommended that this technique be used with caution in cases of preoperative hemipelvis dissociation unless additional column plating is performed.
Figure A demonstrates Paprosky IIB acetabular bone loss with superolateral migration of the acetabular component. Illustration A depicts the Paprosky classification.
Incorrect Answers:
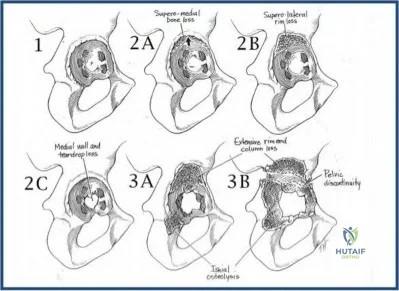
OrthoCash 2020
A 72-year-old male presents with worsening left hip pain 12 years after total hip arthroplasty. On examination, the patient has a Trendelenburg gait with a 3.5 cm leg length discrepancy. The patient denies any fevers or chills. Current radiographs are shown in figure A. Recent ESR and CRP are 21 mm/hr and 1.2 mg/L, respectively. What is the preferred treatment option to address these findings?
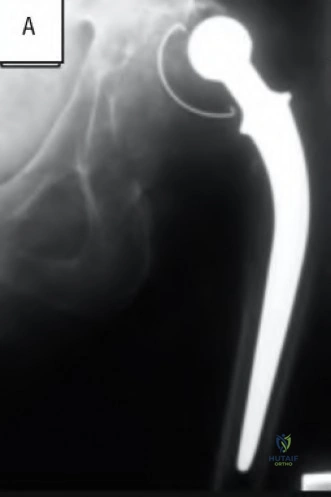
Large porous hemispheric cup with particulate bone graft and augmented with screw fixation
Custom triflanged acetabular component
Cemented large porous hemispheric cup
Metal augments with large porous hemispheric cup and bone grafting combined with screw augmentation
stage revision arthroplasty Corrent answer: 4
The patient is presenting with a Paprosky type IIIA acetabular defect with the migration of the hip center in a superolateral direction. The preferred treatment option would be to provide structural stability of the cup with metal augments combined with bone grafting and cement reinforcement and screw fixation.
Acetabular bone loss can make revision total hip arthroplasty challenging due to lack of structural support of the acetabular cup as well as concerns for bony ingrowth potentially compromising implant longevity. The Paprosky classification was designed to identify the location and degree of acetabular bone loss and thereby to guide treatment of the respective defects. In type IIIA defects there is bone loss of the superolateral acetabulum with greater than 3 cm migration of the center of the femoral head, also described as "up and out." Intraoperatively structural support must be reestablished for the revision cup by either structural allograft or metal augments. Further bone grafting is performed to enhance long term bone ingrowth of the prosthesis.
Sheth et al. performed a literature review on the evaluation and management of acetabular bone loss in revision total hip arthroplasty. The authors reviewed the Paprosky classification for acetabular bone loss and recommended the use of noncemented, porous-coated, hemispheric cups with adjunctive screw fixation in type I, IIA, and IIB defects. For type IIC defects, the authors recommended highly porous, noncemented, hemispheric cups with screw fixation and bone grafting of the medial wall defect. For type IIIA defects, they advocated for the use of metal augments or structural allograft combined with porous hemispheric cups and augmentation with screw fixation and cement.
Lastly, for type IIIB defects, they recommended the use of noncemented acetabular devices combined with structural allograft, structural augments, and a reconstruction cage.
Paprosky et al. performed a retrospective study of patients undergoing revision total hip arthroplasty and proposed a classification system of acetabular bone loss, recommending treatment options for each type. The authors found that of the 147 implants included in the study, only 6 required repeat revision, all of which were type IIIB defects. The authors concluded that adherence to this classification system and the recommended reconstruction techniques can produce acceptable and predictable results in acetabular revision surgery.
Dennis et al. performed a retrospective review of twenty-four patients with Paprosky type IIIB acetabular defects treated with a custom triflanged acetabular component (CTAC). The authors found that of the twenty-four patients treated, three (87.5%) were considered to have radiographic and clinical signs of failure, with one requiring resection arthroplasty. There were two hip dislocations necessitating only closed reduction. The authors concluded that CTAC is an effective means to treat type IIIB acetabular defects, but should be used with caution in cases of pelvic discontinuity unless additional column plating performed.
Figure A is the AP radiograph of a pelvis with a Paprosky type IIIA acetabular defect. Illustration A is the post-op radiograph after reconstruction with metal augments and large porous hemispheric cup. Illustration B is a table with the description of the Paprosky classification. Illustration C is a diagram depicting the Paprosky classification.
Incorrect Answers:
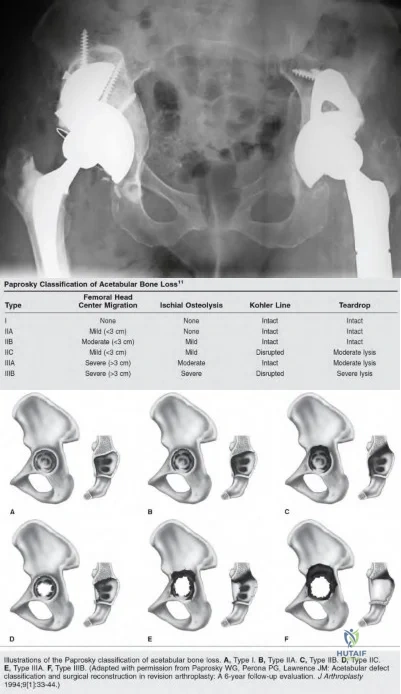
OrthoCash 2020
A 67-year-old woman with poliomyelitis presents with quadriceps weakness and chronic right knee pain for the last 2 years. She is scheduled to undergo right total knee arthroplasty (TKA) after failing nonoperative modalities. Her preoperative radiographs are shown in Figures A and B. What technique should be utilized to optimize her function and to prevent the recurrence of her deformity?
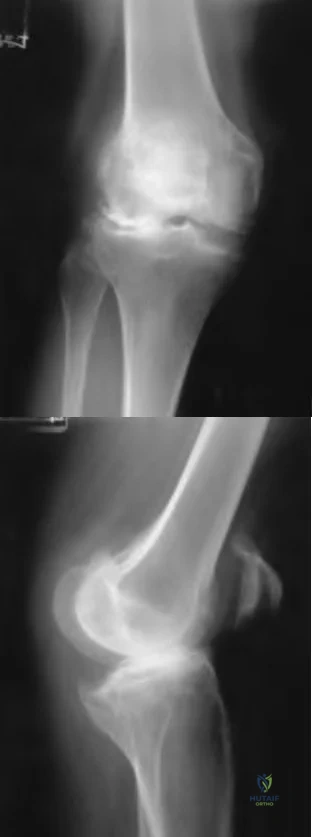
Posterior stabilized design with under-resection of distal femur
Posterior stabilized design with under-resection of proximal tibia
Posterior stabilized design with under-resection of posterior femur
Varus-valgus constrained design
Rotating hinge design
This patient with neuromuscular disease has genu valgum with recurvatum (hyperextension). Of the techniques listed above, utilization of a rotating hinge TKA design would most likely optimize her function and prevent recurrence of her recurvatum deformity because of the implant’s extension stop.
Genu recurvatum is associated with deformities such as genu valgum, ligamentous laxity, and neuromuscular diseases, which are often accompanied by equinus ankle contractures. Knee hyperextension is likely to recur after TKA in patients with neuromuscular disorders such as poliomyelitis due to the bony deformity, muscle weakness, and paralysis seen in these patients. Several strategies to correct knee hyperextension at the time of primary TKA have been described and include posterior capsular plication, proximal and posterior transfer of collateral ligaments, under-resection of distal femur and proximal tibia, and the use of thicker components. In severe cases where ligament integrity is likely compromised, utilization of more constrained prostheses is recommended.
Giori et al. performed a retrospective study of patients with poliomyelitis involving a limb that underwent primary TKA. Complications reported included two periprosthetic fractures, one peroneal nerve palsy, one patellar tendon avulsion, and four cases of recurrent instability, all attributable to the poor bone quality, valgus deformity, patella baja, poor musculature, and attenuated soft tissues observed in knees with poliomyelitis. They concluded that pain and knee scores improved following TKA this cohort of patients and recurrence of instability and progressive functional deterioration is possible postoperatively.
Paratte et al. published an AAOS Instructional Course Lecture on instability after TKA. They reported knee hyperextension before TKA is seen in <1% of patients and is most commonly seen in patients with neuromuscular disease like poliomyelitis. They recommended solutions to be considered for such patients such as distal femur under-resection, distal femoral augmentation blocks with the knee left with a slight flexion contracture, translation of the femoral origins of the medial collateral ligament and lateral collateral ligaments proximally and posteriorly to recreate the normal tightening action during full extension of the knee, and the use of a rotating-hinge total knee prosthesis with an extension stop.
Meding et al. published a review article on the etiology and surgical treatment of genu recurvatum during TKA. They emphasized the importance of diagnosing and elucidating the etiology of the hyperextension deformity prior to surgery since the deformity is known to recur in patients with certain neuromuscular disorders. They recommended a meticulous approach and
avoiding even mild degrees of residual instability in the coronal plane at surgery since this is associated with increased extension in the postoperative period.
Figures A and B depict severe right knee osteoarthritis with valgus and recurvatum deformities. Illustration A depicts a rotating-hinge TKA prosthesis.
Incorrect Answers:

OrthoCash 2020
A 57-year-old man with a history of chronic lower back pain and right hip arthritis is postoperative day 2 from an uncomplicated right total hip arthroplasty with a spinal block. Since the procedure, he has reported persistent pain in his right leg with a focal point in the proximal lateral leg. He has had difficulty getting out of bed for physical therapy due to pain reproduced in his leg. He is voiding but has not yet had a bowel movement. Physical exam is only significant for decreased ankle dorsiflexion strength on the right. Plantarflexion strength remains 5/5 bilaterally. No point tenderness was elicited and Homan's sign is negative. His wound is unremarkable with typical post-operative swelling of the leg and no significant drainage. He has
been receiving ASA 81mg PO daily since surgery and has been wearing compression stockings full-time. Postoperative repeat radiographs of the hip are unremarkable and his hemoglobin is stable. Which of the
following etiologies is most likely responsible for this patient's symptoms?
Residual effect of the spinal block
Lumbar lateral recess stenosis
Gluteal hematoma
Acute post-operative infection
Venous thomboembolism
During total hip arthroplasty, a "double crush" injury can occur to the sciatic nerve in the presence of pre-existing degenerative lumbar spondylosis, leading to persistent pain and post-operative motor weakness. The best study would be a lumbar MRI to evaluate for lumbar spinal stenosis.
Nerve injuries following total hip arthroplasty are rare and usually affect the sciatic nerve. The peroneal branch appears to be the most commonly affected due to its more superficial and lateral position, more the tightly packed fascicles, and greater adherence to the surrounding tissues compared to the tibial division. Lumbar degenerative disc disease commonly occurs in the presence of coxarthrosis, with spinal stenosis being exacerbated by traction neurapraxia during the procedure.
DeHart et al. reviewed nerve injuries and postoperative management. The authors stated that the sciatic nerve is the most commonly injured nerve, with up to 70% of cases have subclinical electrodiagnostic changes. The cause of this is multifactorial, but the vast majority of studies reviewed reported complete spontaneous recovery by 6-12 months. The authors recommend observation of the nerve deficit with ankle-foot-orthosis and follow-up EMG to determine the level of the injury.
Pritchett performed a review of 21 patients that presented with a foot drop after total hip arthroplasty. All patients reported prior back and leg pain prior to the procedure, with post-op MRI demonstrating severe spinal stenosis. The author postulated there to be a double crush phenomenon, with patients undergoing lumbar laminectomy having improvement or complete resolution. The author concluded that select patients presenting with foot drop following THA may benefit from a lumbar laminectomy.
Incorrect Answers:
and paresthesias are uncommon after a spinal block but have been reported with regional anesthesia, such as a sciatic nerve block. Furthermore a spinal would be unlikely to have any residual effect still post-operative day 2.
OrthoCash 2020
A 65-year-old female presents to the clinic with isolated medial-sided left knee pain. She has since exhausted conservative management but remains persistently symptomatic. The physical exam and radiographic work-up demonstrates isolated medial tibiofemoral compartment involvement. After discussion of the surgical options, she undergoes the procedure shown in Figure A. She initially does well but returns to clinic 3 months post-operatively with significantly increased medial-sided knee pain and the injury shown in Figure B. All of the following technical errors likely contributed to this complication EXCEPT?

Excessive force impacting the tibial component
Penetration of the posterior tibial cortex with proximal guide pin
Placement of a peripheral medial cortical guide pin
Tibial resection guide replacement with re-drilling of the two proximal guide holes
Under-sizing of the tibial component Corrent answer: 1
The patient presents with a periprosthetic tibial stress fracture following a medial unicompartmental knee arthroplasty. Excessive force used when impacting the tibial component could potentially lead to intra-operative fracture, but this would be recognized in the acute post-operative period.
With continuing advances in surgical technique, UKA has demonstrated increasingly promising midterm outcomes. However, there are number of technical considerations that directly impact survivorship and the potential for post-operative complications. While aseptic loosening remains the most common mode of early failure necessitating conversion to TKA, literature is replete with reports of early failure secondary to proximal tibia stress fractures. Stress fractures have been linked to a number of largely non-modifiable patient characteristics to include bone quality, but technical errors remain a controllable contributing factor. Recent studies have found that excessive guide pin number and suboptimal placement for the tibial resection guide as well as tibial component undersizing are associated with increased proximal tibial mechanical stress and may result in fracture.
Brumby et al. described a series of tibial plateau stress fractures subsequent to UKA. The authors attributed these to mechanical weakening of the proximal tibia from the guide pin and lug holes drilled for the guide and tibial component, respectively. They noted that this even occurred in some cases with penetration of the medial tibial cortex by a single pin. Stress fractures presented at a median of 8 weeks post-operatively and in all cases required revision to TKA. They recommended post-operative monitoring of patients in whom a guide with 3 or more pins was utilized, or with any peripheral pins that breach the medial tibial cortex.
Vince et al. present a review of the evolution, indications, and outcomes following UKA. The authors specifically highlight guide pin holes as a major contributing factor to periprosthetic fractures. They recommend limiting the number of holes drilled for placement of the tibial resection guides and paying careful attention to placement, specifically with regard to violation of the medial cortex. Furthermore, the authors advocated that a single proximal pin, placed centrally, and the guide secured distally by the ankle clamp would be
sufficient for stability and alignment while avoiding increased stress on the proximal tibia.
Figure A is an AP weight-bearing radiograph of the left knee demonstrating isolated medial tibiofemoral arthritis.
Figure B is a post-operative radiograph of the left knee significant for a medial UKA. Figure C is a follow-up AP radiograph of the left knee demonstrating a periprosthetic fracture involving the medial UKA with significant varus collapse.
Incorrect answers:
OrthoCash 2020
A 65-year-old male presents to your clinic for evaluation of right hip pain. He underwent a right total hip arthroplasty (THA) 20 years prior and was doing very well until 2 years ago. He admits to groin pain when getting up from a seated position. He denies any fevers or chills. Radiograph is shown in Figure A. Which of the following would preclude the patient from undergoing a single-stage surgical intervention without further workup?

Elevated serum cobalt
Metallosis noted intra-operatively
Significantly higher serum cobalt then serum chrome levels
Elevated ESR and CRP
Pseudotumor noted on MRI Corrent answer: 4
An elevated ESR and CRP are screening labs used to determine if further workup is required to rule out a periprosthetic joint infection (PJI). A patient with an elevated ESR and CRP should thus undergo further workup including a joint aspiration prior to consideration of a single-stage revision THA.
The differential diagnosis of pain after THA encompasses a number of etiologies. While radiographs may point to loosening of the stem or the cup, osteolysis or a stress fracture, the first step in management needs to evaluate for a PJI. Accordingly, ESR and CRP are logical next screening steps in the workup. If elevated, additional studies need to be obtained such as joint aspiration with manual diff (to look for elevated synovial WBC, synovial PMNs or a positive culture), immunoassays (alpha-defensive, leukocyte esterase colorimetric strip) and serum IL-6. If the additional workup for infection is negative, it is safe to proceed with a single-stage revision THA. Metal on metal THA have their own set of modes of failure leading to bony erosion and pain.
The majority of these are aseptic and allow for a single-stage revision including metallosis, pseudotumor, and metal hypersensitivity.
Parvizi et al. performed a retrospective cohort study to examine the effectiveness of surgical treatment in treating hip and knee PJI caused by MRSA. They looked at 127 patients with a minimum of 2 years follow-up or until recurrence of PJI. In 35 patients, only an I&D with prosthetic retention was performed while a 2 stage explantation and reimplantation was performed in the other 92 patients. Of those who underwent an I&D and implant retention, only 37% of cases had successful eradication of the infection
whereas two-stage exchange arthroplasty controlled the infection in 75% of hips and 60% of knees in the other 92 patients. Furthermore, cardiac disease was associated with a higher likelihood of failure to control infection in all treatment groups.
Shukla et al. evaluated 87 hips with a PJI that were treated with explantation, antibiotic spacer and 6 weeks of antibiotics. The authors looked at ESR and CRP before reimplantation and obtained synovial WBC at the time of reimplantation. The authors noted 9 hips (10.1%) had persistent infections at the time of re-implantation. The mean ESR, CRP, and synovial fluid WBC count had significantly decreased between stages; however, the ESR remained elevated in 50 patients (62.5%) and the CRP remained elevated in 22 patients (27.5%) in whom the infection had been eradicated. The authors noted that the synovial fluid WBC count was the best test for identifying persistent infection, with an optimum cutoff of 3528 WBCs/microL (sensitivity, 78%; specificity, 96%).
Browne et al. evaluated 37 patients with metal on metal THA or resurfacing arthroplasties who underwent revision to determine the clinical, radiographic, laboratory, intraoperative, and histopathologic findings to determine the cause of failure. Of the 37 patients, 10 were revised due to metal on metal hypersensitivity, 8 due to chronic inflammation with lymphocytic infiltration, 8 with aseptic loosening, 2 with iliopsoas impingement, 3 with femoral neck fracture after resurfacing arthroplasty and 6 due to infection, instability, and periprosthetic fracture. The authors stressed increased awareness of the wide variety of modes of failure associated with metal-on-metal articulations.
Figure A is an AP pelvis showing a characteristic appearance of a metal-on-metal THA with a large femoral head.
Incorrect Answers:
OrthoCash 2020
The use of a high-offset femoral stem leads to which of the following changes with regard to total hip arthroplasty?
Increased joint reactive forces
Increased leg length
Increased risk of acetabular component loosening
Increased soft tissue tension
A higher rate of dislocation Corrent answer: 4
A high-offset femoral stem leads to increased soft tissue tension without affecting leg length.
Femoral offset is defined as the distance from the femoral head center of rotation to the center of the long axis of the femur. Restoration of offset improves overall arthroplasty biomechanics with decreased cup strain and polyethylene wear, decreased dislocation risk, increased hip abductor strength, and lower rates of postoperative limp. The drawback of too much femoral offset is an increased risk of lateral prominence and subsequent trochanteric bursitis.
Lecerf et al. reviewed the femoral offset with regard to total hip arthroplasty. They state femoral offset does correlate closely with the hip abductor lever arm and hip abductor strength. They conclude that femoral offset is important for improved hip function and longevity after total hip arthroplasty.
Flecher et al. reviewed limb lengthening as it pertains to total hip arthroplasty. They discuss methods of assessing limb length including EOS and CT imaging as well as intraoperative robotic or computer assistance. They comment that the expectations of limb function after total hip make it crucial for surgeons to understand the three-dimensional geometry and placement of prostheses.
Illustration A shows an example of a standard and high offset stem and how it maintains leg length while increasing offset.
Incorrect Answers:

OrthoCash 2020
You are currently evaluating a 68-year-old woman who has met indications for a total knee arthroplasty. You finally have finished documenting the patient’s extensively detailed social and family history. As you finish, the patient tells you that she has spoken with her friends regarding her knee and tells you that she wants a prescription for preoperative physical therapy, would like a drain placed, an order for a cryotherapy device and use of a patient-controlled analgesia (PCA), in addition to being mobilized with physical therapy on the day of surgery. As an astute resident you inform the patient that based on the current AAOS clinical practice guidelines (CPG), there is strong evidence against using which of the patient’s request?
Preoperative physical therapy
Drain placement
Cryotherapy device
Postoperative day 0 mobilization
Patient-controlled analgesia
Based on the most recently published AAOS CPG, there is strong evidence to support not using a drain with total knee arthroplasty (TKA) because there is not any difference in complications or outcomes.
The use of a drain was postulated to aid in decreasing postoperative infection, swelling, blood transfusions, hematoma formation, pain, length of hospital stay, and re-operation rates. In addition, their use was meant to improve
postoperative range of motion. However, after review of the high- and moderate-quality studies and with input from the multiple orthopaedic and medical societies, there has not been any clear advantage to the use of drains after unilateral total knee arthroplasty when comparing complication profiles and outcomes.
McGrory et al. published a systematic review on the surgical management of osteoarthritis of the knee. In an effort to improve the surgical management of patients with osteoarthritis, the authors provide 38 evidence-based recommendations on topics specific to the preoperative, perioperative and postoperative treatment of such patients. Additionally, each topic was further classified based on the level of evidence available (limited, moderate, and strong) to support or not support a give recommendation.
MacDonald et al. completed a prospective randomized clinical trial using continuous passive motion (CPM) following TKA. The patients were separated into two separate treatment groups plus a control group. The patients were followed over the course of one year from surgery. Similar to postoperative drain placement following TKA, MacDonald et al. were unable to demonstrate any significant difference in outcomes for CPM versus no CPM.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a male who fell down the stairs. He is 8 years status post right total hip arthroplasty. All of the following are indications for a proximal femoral replacement EXCEPT?

<4cm of diaphyseal cortical bone
Age <50 years
Extensive metadiaphyseal proximal bone loss with <4cm of intact isthmic bone
Nonunion of the proximal femur with multiple failed attempts at osteosynthesis
Paprosky IV femoral bone loss Corrent answer: 2
The radiograph demonstrates a Paprosky type IV femoral deficiency. Given the substantial bone loss with limited proximal femoral support, a proximal femoral replacement is recommended.
Postoperative fractures around a total hip prosthesis has an incidence of 0.1% and occurs most commonly at the tip of the stem. Proximal femoral support is important to evaluate following a periprosthetic fracture of the hip. The Paprosky classification of femoral bone loss helps guide treatment. A Paprosky type IIIb or IV femoral deficiency would benefit from either an allograft prosthetic component or a megaprosthesis/modular oncology component.
Additionally, impaction bone grafting is indicated with a large canal and thin cortices for Paprosky IIIb and IV defects. Revising the femur to a proximal
femoral replacement would allow early mobility and provide better fixation, given the substantial bone loss for proximal support and is typically reserved for the elderly or sedentary patient.
Parvizi et al. review the use of a proximal femoral replacement (megaprosthesis) in revision hip surgery. They report that with the increased use of cortical strut grafts to augment host bone, the indications for the use of megaprostheses have narrowed. They conclude that currently, the use of megaprostheses is reserved for elderly or sedentary patients with massive proximal femoral bone loss that cannot be reconstructed by other reconstructive procedures.
Brown et al. tests the inter-observer and intra-observer reliability of this Paprosky classification of femoral bone loss. They report an inter-observer reliability of 0.61, indicating substantial agreement between surgeons. They also show a high intra-observer reliability, indicating substantial to almost perfect agreement. They conclude that there is substantial agreement among experienced arthroplasty surgeons when using the Paprosky Classification to characterize femoral bone loss.
Figure A is the AP radiograph of the right hip which demonstrates a Paprosky type IV femoral deficiency. Illustration A is the Paprosky classification of proximal femoral bone loss.
Incorrect Answers:
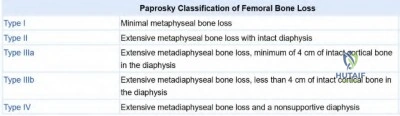
OrthoCash 2020
A healthy, active, 65-year-old male underwent a total knee arthroplasty 1 year ago. He presents to the emergency room after a ground-level fall earlier in the day. On exam, the patient is unable to perform a straight leg raise. Figure A is his current lateral radiograph. What is the most appropriate treatment for this patient?

Immediate active and passive range of motion in a hinged brace
Immobilization for 2 weeks followed by aggressive physical therapy
Cylinder cast for 6 weeks
Open Reduction Internal Fixation
Partial patellectomy
This patient has a displaced patella fracture with a disrupted extensor mechanism; therefore, (4) open reduction internal fixation is the correct answer.
Risk factors for patella fracture following total knee arthroplasty include trauma, the performance of a lateral release, damage to the blood supply, and excessive resection at the time of resurfacing. Indication for non-operative management includes both implant stability and extensor mechanism competency. If the implant is unstable or the extensor mechanism is disrupted a variety of surgical options exist including open reduction internal fixation (ORIF), component revision, partial or complete patellectomy or extensor mechanism allograft.
Konan et al. reviewed the management of periprosthetic total knee fractures. They report that non-operative treatment for periprosthetic patella fractures with an intact extensor mechanism leads to better outcomes when compared to surgery. Surgery is associated with high complication rates, including infection and nonunion. They conclude that regardless of the treatment employed, the goal should be early patient mobilization.
Kuyzk et al. reviewed the management of periprosthetic total knee fractures. They note that periprosthetic patella fractures are the least common type of fracture in this population. Their review concludes that host bone stock is one of the most important factors when determining the revision implant type.
Figure A demonstrates a displaced patella fracture in a patient with a previous total knee arthroplasty.
Incorrect answers
OrthoCash 2020
A 91-year-old, minimally ambulatory male presents with acute on chronic progressive right thigh pain. Fifteen years ago, he underwent a right total hip replacement and he had been having progressive thigh start-up pain over the prior 5 months. He sustained a ground-level fall yesterday and he is now unable to bear any weight on the right leg. His current radiograph is shown in Figure A. His labs, including CBC, ESR, and CRP are all within normal limits. Which of the following represents the most appropriate next step in definitive management?

Revision to a proximal femoral replacement
Open reduction and internal fixation with proximal femoral locking plate and cerclage cables
Revision to a cemented long femoral stem
Open reduction and internal fixation with iliac crest bone grafting
Revision to a cementless long porous-coated femoral stem Corrent answer: 1
The patient has a Vancouver B3 periprosthetic femur fracture and requires revision. Given the extensive amount of bone loss in the proximal segment as well as a loose stem, a proximal femoral replacement would be an appropriate treatment
Post-operative periprosthetic femur fractures are classified based on the Vancouver classification which classifies fractures based on the location of the fracture, implant stability, and bone loss. Vancouver B3 periprosthetic femur fractures are defined as fractures at, around, or just below the stem with significant proximal bone loss/osteopenia or comminution which is unable to allow for reconstruction. In the setting of these injuries, treatment would consist of endoprosthetic proximal femur replacement or replacement with a large proximal femur allograft.
Della Valle et al. discuss the challenges associated with pre-operative planning for femoral revision total hip arthroplasty. The authors provide a classification of femoral bone loss that guides the surgeon in selecting an appropriate method of reconstruction. They conclude that appropriate pre-operative planning is required for the management of femoral implant revision in the setting of fracture, osteolysis, and instability.
Brown et al. reviewed the indications for revision THA to include instability, aseptic loosening, osteolysis, infection, periprosthetic fracture, component malposition, and catastrophic implant failure. They note that femoral component revision presents a complex challenge to the arthroplasty surgeon because of modern implant design as well as bone loss in the proximal femur. They conclude that knowledge of various reconstructive options and the indications for each is necessary to achieve a successful outcome.
Figure A is the radiograph of a periprosthetic femur fracture with extensive proximal femoral bone loss consistent with a Vancouver B3 periprosthetic femur fracture. Illustrations A and B are the radiographs revealing a revision total hip arthroplasty with proximal femur endoprosthetic reconstruction.
Incorrect Answers:
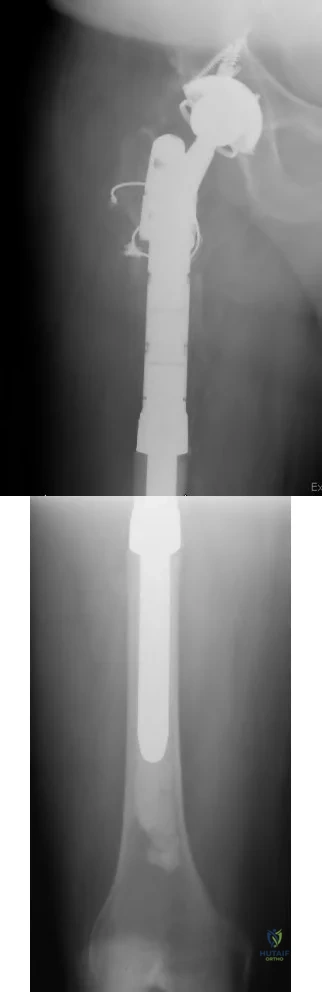
OrthoCash 2020
A 64-year-old male is 6 months out from left total knee arthroplasty. He has had at least two months of pain and swelling to the operative joint. In your initial workup, he is found to have a well-healed surgical incision, a serum CRP of 13mg/L and an ESR of 19mm/h. You perform arthrocentesis, which results in a negative alpha-defensin, synovial WBC of 1000 cells/µL, synovial PMNs of 90%, and synovial CRP of 4mg/L. What is the next best step in management?
Corticosteroid injection
Proceed to OR for histologic examination
Proceed with two stage revision
Proceed with single stage polyethylene exchange with irrigation and debridement
6 weeks of IV antibiotics
The patient has a score of 4 (2 points for elevated serum CRP, 2 points for elevated synovial PMN %) according to Parvizi et al's "The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria". This results in an ‘inconclusive’ determination of whether the patient has a periprosthetic joint infection. The best next step is to proceed to the OR in order to obtain tissue for histologic examination, cultures, and to determine whether purulence is present.
Periprosthetic joint infections can be devastating. Chronic PJI of the hip and knee is typically treated with two-stage revision arthroplasty. The first stage involves removal of the orthopaedic implants, placement of an antibiotic spacer, and at least 6 weeks of intravenous antibiotics. Once there is evidence that the infection has cleared (i.e. serum and synovial analysis), the second stage involves removal of the antibiotic spacer and placement of revision components.
Parvizi et al. updated their definition of PJI in 2018. They kept the major criteria for a chronic periprosthetic joint infection the same (an infection is indicated when 2 positive cultures of the same organism are isolated, or a sinus tract is present), but made several changes to the minor criteria.
Namely, they assign a point criteria in which a score of ≥6 is reliably infected, 2-5 is inconclusive, and 0-1 is not infected. In the case of infection, their recommendation is to proceed with a two-stage revision. If an inconclusive score is met, the recommendation is to proceed to the OR for histologic examination, cultures, and to determine whether purulence is present. The update to the MSIS criteria provides a sensitivity of 97.7% and a specificity of 99.5%.
Parvizi et al. reviewed 54 consecutive THA two-stage revisions. In their review, they determined MRSA to be the most common causative organism: MRSA 27.7%, S.epidermidis 18.4%, followed by MSSA 14.8%. They followed patients for a mean of 32 months, during which 26% had a recurrent infection and 8% developed mechanical failure (loose acetabular or femoral components).
Della Valle et al. made 15 CPGs (clinical practice guidelines) in JAAOS 2010. Among their recommendations: 1) they recommended utilizing serum CRP and ESR in assessing for PJI, 2) they recommended aspiration if serum CRP/ESR are abnormal, 3) if the initial aspiration has unexpected results they recommend repeat aspiration, and 4) 2 week antibiotic holiday before attaining cultures.
Illustration A shows the scoring criteria for the 2018 PJI update.
Incorrect Answers:
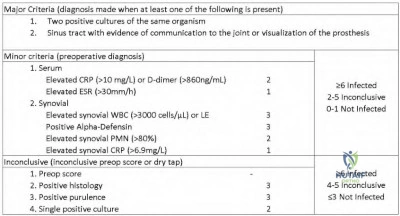
OrthoCash 2020
A 66-year-old male is undergoing a total knee arthroplasty using a fixed bearing posterior stabilized component. During the intraoperative trialing of the components, it is noted that the flexion gap is loose, and the extension gap is appropriate. Compared to a patient with appropriate flexion and extension gaps, this patient would be at an increased risk for which of the following?
Manipulation under anesthesia
Knee hyperextension
Posterior knee dislocation
Anterior knee dislocation
Patella fracture
A loose flexion gap in a posterior stabilized primary total knee arthroplasty can lead to an atraumatic posterior knee dislocation during knee flexion.
A posteriorly stabilized knee has a post built into the polyethylene bearing that articulates with the box of the femoral component in flexion to act as a cam mechanism. It is felt to occur when the patient is in moderate to deep flexion and tibia is able to translate posteriorly. The post becomes locked behind the cam and the patient is unable to extend the knee. The etiology is felt to be related to implant design, soft tissue laxity over time, and surgeon technique.
Clarke et al. review flexion instability as a mode of failure in knee replacements. They describe how this is usually due to a lack of adequate balance at the time of surgery. They also report that revision surgery is usually the only way to correct symptomatic flexion instability.
Lombardi et al. reviewed 15 cases of dislocation in three different implant designs given the statistically significant difference in the rate of dislocation. They found the only significant difference between the group of patients with dislocation was increased flexion. They state the majority of the dislocations occurred prior to a modification in the tibial polyethylene insert of the specific knee design they studied.
Illustration A shows an example of a posteriorly dislocated total knee arthroplasty following a "jumped post" dislocation.
Incorrect Answers:

OrthoCash 2020
A 78-year-old woman who has a history of an uncomplicated right total hip arthroplasty presents after a fall. Figure A is the radiograph obtained in the emergency department. What is the most appropriate treatment for the femoral component?

Retained femoral stem with open reduction internal fixation
Revision femoral stem to an uncemented long stem with strut allograft
Revision femoral stem to a cemented long stem with open reduction internal fixation
Revision femoral stem to an uncemented long stem with open reduction internal fixation
Proximal femoral replacement Corrent answer: 4
In this scenario, the stem is loose with good proximal bone stock. The best option would be revision femoral stem to an uncemented long stem with an open reduction of the fracture.
Operative treatment of periprosthetic fractures is directed by the location of the fracture, the stability of the implant, and remaining bone stock. In circumstances where the femoral implant has loosened or subsided revision to a long stem is recommended. Cemented fixation is less ideal in a fracture scenario given cement interference with fracture healing. After bypassing the fracture with a long stem the fracture is reduced and stabilized to provide an environment for healing and long term durability.
Ko et al. reviewed 14 patients who underwent revision to a Wagner stem
following a B2 periprosthetic fracture. They found all 12 patients who followed up went on to union with 10 achieving good or excellent outcomes. They concluded the Wagner revision stem is a satisfactory prosthesis for Vancouver B2 periprosthetic femur fractures.
Kwong et al. reviewed 143 patients who underwent revision total hip for a proximally compromised femur to a modular cementless femoral stem.
Roughly ~10% of these patients were revised for periprosthetic fracture. They found a 97.2% survival rate and an average Harris hip score of 92. They concluded that the modular cementless diaphyseal engaging revision stem allows for adequate revisions THA for the proximally compromised femur.
Figure A shows a loose femoral component with subsidence and a periprosthetic fracture. Illustration A shows an AP of the right hip following open reduction internal fixation as well as a revision to an uncemented long stem and revision of the acetabular components.
Incorrect Answers:

OrthoCash 2020
A 78-year-old female with end-stage arthritis of the left hip is schedule for a total hip arthroplasty. Her contralateral hip was replaced 4 years prior and a current radiograph is shown in Figure A. Which of the following would be the most effective at preventing the complication shown in the Figure?

Indomethacin treatment for 2 days postoperatively
Leaving 2 drains in place until at least 4 days post-operatively
Postoperative administration of ethylhydroxydiphosphonate
Preoperative administration of radiation therapy 1 week before surgery
Postoperative administration of radiation therapy 8 hours following the surgery
This patient has developed heterotopic ossification (HO) following a total hip arthroplasty. Radiation therapy administered within 24-48 hours postoperatively would best prevent this from forming.
Heterotopic ossification following arthroplasty is relatively rare, but is more common following total hip arthroplasty (THA) as compared to total knee arthroplasty (TKA). Symptoms can range from subtle pain to complete loss of motion. The trigger for HO formation is unknown but this process involves mesenchymal cell stimulation within the muscle and fascia to form osteoblast and osteoid formation. This process begins within 16 hours of the insulting event and continues for over 1 year, maturing into a ossified mass of lamellar bone.
Iorio and Healy discussed management of HO following arthroplasty. They note the most effective treatment at preventing HO is radiation therapy given 6 hours or sooner pre-operatively, or within 4 days post-operatively.
Indomethacin is an alternative to radiation, with variable regimens showing relatively equivalent results. They make a point to note that despite appropriate prophylaxis, 2-5% of individuals still develop HO.
Pelligrini et al. evaluated the outcomes of 2 groups undergoing THA who received either 800 cGy or fractionated 1000 cGy radiation therapy postoperatively. Equivalent outcomes were shown between the groups, as evidenced by 79% disease-free at 6 month follow-up. Of note, the implants used were all cemented which do not rely on bone ingrowth.
Pelligrini and Gregoritch then prospectively followed 2 groups undergoing THA that were randomized to receive either pre- or post-operative radiation therapy. At final 6 month followup, both groups showed similar disease-free rates (73% vs. 76%). This demonstrated that pre-operative radiation was as effective as post-operative, at a time when it's utility was unknown and unstudied.
Figure A shows a radiograph with HO formation nearly completely bridging the hip joint.
Incorrect Answers:
OrthoCash 2020
A 62-year-old woman with a valgus knee as seen in Figures A and B who underwent a primary total knee arthroplasty with a tourniquet presents 5 hours postoperatively with severe pain in the extremity and inability to dorsiflex or plantarflex the ankle. Narcotic pain medication does not improve her symptoms. The knee is flexed and the bandage is loosened and she is re-examined one hour later. On examination, the patient is unable to dorsiflex or plantarflex the foot and the pulses are asymmetric. What is the next most appropriate step in management?

Serial neurologic examinations and EMG in 3 months
Pain service consultation for adductor canal block
Return to the OR for peroneal nerve exploration
Vascular surgery consultation
Thrombectomy
The patient's asymmetric pulses, pain, and loss of motor function are evidence of an acute vascular injury for which an immediate vascular surgery consultation should be obtained.
Acute vascular injury following TKA is a rare but devastating complication that can result in wound healing complications, permanent neurologic injury, and loss of limb. Preoperative knowledge and evaluation of patients at risk for vascular injury allows optimization and potential modifications of surgical techniques to limit the chances of a vascular injury. Early recognition of an injury and consultation with a vascular surgeon is paramount to limit the chances of loss of limb. Patients with pre-existing vascular disease may be better served to have a TKA without the use of a tourniquet. If an injury occurs aggressive revascularization may be indicated for limb salvage.
Calligaro et al. report on their experience with vascular injuries following total hip and total knee arthroplasty in 32 patients, 24 TKA and 8 THA, for a rate of 0.13%. They found 44% of these vascular injuries were noted after the day of surgery and late-diagnosed injuries tended to have a higher rate of fasciotomies and foot drop. They also found thrombectomy alone was only successful in 28% of patients. They concluded that arterial injury after TKA and THA is rare, and aggressive revascularization is often needed for limb salvage.
Smith et al. review arterial injuries following total knee arthroplasty. They state preoperative risk factors of a history of vascular disease, intermittent claudication, ischemic ulcers, rest pain, asymmetric pulses, suspected popliteal aneurysm, radiographic evidence of vascular disease, or prior vascular surgery should alert the orthopedic surgeon of an increased risk for vascular complications following total knee arthroplasty. If performing a TKA on a patient with a history of vascular disease they recommend evaluation by a vascular surgeon and consideration of not using a tourniquet intraoperatively versus a tourniquet with an intravenous dose of heparin.
Ninomiya et al. reviewed the anatomy of the popliteal artery and when it could be injured during various portions of total knee arthroplasty. They state the popliteal artery is lateral to the midline at the tibial plateau in 95% of cadavers. To avoid vessel injury they recommend a preoperative vascular workup for high risk patients, careful placement of posterior retractors, and avoidance of hyperextension of the knee.
Figure A shows an AP and lateral of the knee respectively demonstrating a valgus knee with degenerative changes as well as posterior arterial calcifications.
Incorrect Answers:
OrthoCash 2020
A 70-year-old female patient on chronic steroids for severe lupus presents with worsening bilateral hip pain over the last several years. She has been on chronic corticosteroids for p-ANCA vasculitis. The current radiograph is shown in figure A. Which treatment will have the most reliable pain relief and return of function in this patient?

Vascularized fibular graft
Proximal femoral osteotomy
Core decompression
Total hip arthroplasty
Hip resurfacing arthroplasty Corrent answer: 4
Total hip arthroplasty would provide the most reliable pain relief and return of function in this patient with bilateral femoral head avascular necrosis with collapse.
Hip avascular necrosis, also known as osteonecrosis, leads to progressively worse hip pain and femoral head collapse. Idiopathic avascular necrosis is most common, which is the result of intravascular coagulation. In 80% of
cases, it is bilateral. Core decompression, vascularized fibular autograft, and rotational osteotomies are treatment options for pre-collapse osteonecrosis. Once Total hip arthroplasty or hip resurfacing arthroplasty are treatment options for lesions with femoral head collapse. Hip resurfacing is reserved for young male patients with good femoral bone stock. Total hip arthroplasty is a better option for older, female patients and those with chronic steroid use as there is poorer bone quality.
Jawad et al. reviewed the Ficat classification system for hip osteonecrosis. They described stage 0 as preclinical disease that is suspected when the contralateral hip is affected, stage 1 as preradiographic disease with groin pain, stage 2 as increased femoral head density or cystic lesions with or without a crescent sign, stage 3 occurs when there is the loss of the femoral head contour and stage 4 with complete collapse of the femoral head with associated osteoarthritis. The authors concluded that the Ficat classification system is the most widely used, but has limitations with prognostication of outcomes and reliability among researchers.
Zalavras and Lieberman reviewed the diagnosis and management of hip osteonecrosis. They identified risk factors for developing hip osteonecrosis including trauma, corticosteroid use, excessive alcohol consumption, coagulation disorders, hemoglobinopathies, dysbaric phenomena, autoimmune diseases, storage diseases, smoking, and hyperlipidemia.
Figure A is the AP pelvis radiograph demonstrating bilateral hip avascular necrosis with the collapse of the femoral head. Illustration A is a diagram of a vascularized fibular autograft used for hip avascular necrosis. Vascularized fibular autograft involves the harvesting of a portion of the peroneal artery pedicle. The femoral neck and head are reamed to accommodate the graft, which provides structural support to the subchondral bone. This is fixed with a K-wire or screw. The graft is anastomosed with the lateral femoral circumflex artery. Illustration B is a table of the Ficat classification system.
Incorrect Answers:
increasing vascular flow. It is not effective once femoral head collapse has occurred. It can be augmented with bone morphogenic proteins or bone marrow aspirate.
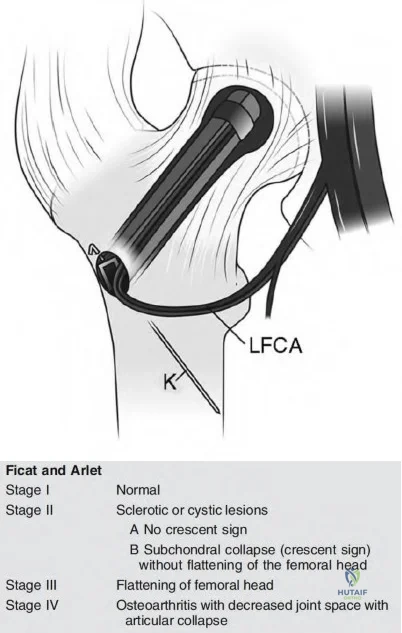
OrthoCash 2020
Medial knee osteoarthritis is associated with which biomechanical change?
Decreased knee flexion moment
Increased knee abduction moment
Increased knee adduction moment
Increased knee extension moment
None of the above Corrent answer: 3
An increased adductor moment during gait is associated with progression of medial knee osteoarthritis.
Altered joint loading during ambulation contributes to the onset and progression of knee osteoarthritis. The external knee adduction moment is considered a surrogate measure for the medial tibiofemoral contact force. An adduction moment is experienced by the knee when the ground reaction force passes medial to the center of the joint. This is seen when the knee has a varus mechanical alignment. An abnormally large peak adduction moment has been linked to increased pain and rate of disease progression. Strategies to decrease the knee adduction moment have been developed such as offloader braces.
Chehab et al. performed a biomechanical, clinical and MRI study on the progression of knee osteoarthritis. They found that the knee adduction and flexion moments were associated with decreases in medial femoral and tibial cartilage thickness, with the knee adduction moment being most associated with diminished medial femoral cartilage thickness and the knee flexion moment being most associated with diminished medial tibial cartilage thickness. They concluded that both knee adduction moment and knee flexion moment increase with medial arthritis and varus alignment, and must be taken into consideration when designing interventions that address knee osteoarthritis progression.
Manal et al. performed a biomechanical study in which they determined knee compartment loading utilizing video-based motion capture and electromyographic (EMG) recordings. They determined that peak adduction moment was the leading predictor of peak medial loading, and that peak knee flexor moment was also a significant predictor of peak medial joint loading.
They concluded that the combined use of peak knee adductor and flexor moments provides a more accurate estimate of peak medial joint loading than the peak adduction moment alone.
Illustration A is a diagram that shows how a knee adduction moment is produced by a varus mechanical alignment.
Incorrect Answers:
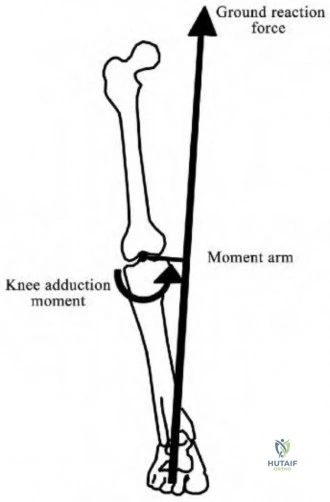
OrthoCash 2020
With regard to a mobile-bearing unicompartmental knee arthroplasty (UKA), which of the following is the most common cause of late (>10 years) failure?
Aseptic loosening
Progression of osteoarthritis
Unexplained pain
Instability
Infection
The most common cause of late failure and revision of unicompartmental knee arthroplasty (UKA) is the progression of osteoarthritis.
Late failure (>10 years) of UKA is most commonly caused by progression of arthritis. Other causes of failure include aseptic loosening, instability, infection, unexplained pain, and polyethylene wear. Interestingly, while TKA saw improved survival with improved polyethylene from the 1990s to the 2000s, UKA did not see a large change in survivorship suggesting that progression of osteoarthritis may be an unmodifiable mode of failure of these implants.
Jennings et al. review medial UKA. They state early medial UKA failures (<5 years) were from aseptic loosening (25%) with the progression of osteoarthritis second at 20%. However midterm and late failures were more commonly due to the progression of osteoarthritis (38 to 40%) with aseptic loosening (29%) and polyethylene wear (10%) as the next most common modes of failure.
Borus et al. reviewed UKA with regard to the evolution of the procedure. They found that at 10 years, one registry study found the progression of arthritis (51%) to be the most common cause of failure. They also cite a study that showed that mobile-bearing UKA tended to fail more from the progression of arthritis while fixed-bearing UKA failed due to tibial component failure.
Incorrect Answers:
OrthoCash 2020
Placement of an acetabular cup with a high inclination angle decreases the stability benefit of which of the following?
Larger femoral head size
Smaller femoral head size
Acetabular cup medialization
Increased femoral offset
Femoral stem anteversion Corrent answer: 1
Placement of an acetabular cup with a high inclination (abduction, theta) angle decreases the benefit of a larger head size by allowing dislocation with minimal translation.
Dislocations following THA occurs in approximately 1-3% of cases with an increased risk following revision surgery. Increased femoral head size improves stability by increasing jump-distance. In addition, an increased head-neck ratio allows a greater arc of motion prior to neck-socket impingement.
However, the increased stability provided by larger head sizes can be negated by other factors, including poor component positioning, poor soft tissue tensioning, and abductor deficiency. The use of a larger femoral head will not compensate for instability caused by a vertically positioned cup or abductor deficiency.
Burroughs et al. performed an in-vitro study evaluating the range of motion and stability in THA with 28, 32, 38, and 44-mm femoral head sizes. They found femoral heads >32-mm provide greater ROM and decreased component impingement. The authors conclude that large femoral heads offer potential in providing greater hip ROM and joint stability.
Kung et al. studied the effect of femoral head size and abductor integrity on dislocation rates in 230 patients who underwent revision THA. Four groups were identified: 1) intact abductor mechanism and 28-mm head, 2) absent abductor mechanism and 28-mm head, 3) intact abductor mechanism and 36-mm head, and 4) absent abductor mechanism and 36-mm head. The dislocation rate was higher with a 28-mm head compared to a 36-mm head when abductors were intact (groups 1 & 3). Dislocation rates were also higher if the abductors were absent, regardless of head size. The authors conclude the use of a large-diameter head does not reduce the rate of dislocation if the abductor mechanism is absent.
Illustration A is a low AP pelvis demonstrating an inclination (abduction, theta) angle of 63º.
Incorrect Answers
increasing the moment arm of the abductors, which is not biomechanically dependent on cup position.
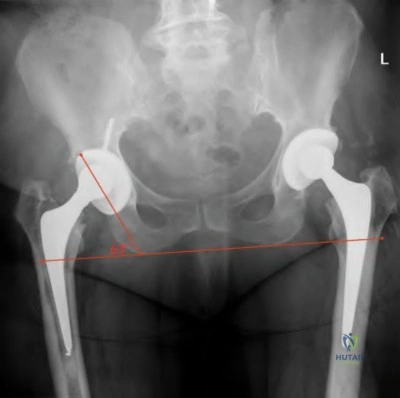
OrthoCash 2020
A 65-year-old woman who underwent left total hip arthroplasty 10 years ago now reports groin pain over the past year. An immediate postoperative (left image) and current radiograph (right image) are shown in Figure A. Laboratory studies show an elevated ESR and CRP. Aspiration results from one day prior shows 500 WBC with 50% neutrophils. She is presently taking oral antibiotics for a upper respiratory tract infection. What is the next most appropriate step in management?

Triple phase bone scan
Repeat aspiration today sent for cell count, gram stain, and culture
Open biopsy and frozen sections
Revision arthroplaty of acetabular component
Repeat aspiration today sent alpha-defensin synovial fluid immunoassay Corrent answer: 5
Oral antibiotics can decrease the yield of aspiration. In this circumstance, the aspiration should be repeated after 2 weeks off antibiotics or a repeat aspiration can be sent for alpha-defensin synovial fluid immunoassay.
The diagnosis of periprosthetic joint infection remains a challenge with no single test with 100% accuracy. The highest accuracy can be achieved with a combination of tests and the knowledge of the pretest probability given the clinical history. Elevated inflammatory markers are an indication to aspirate the joint. Aspiration can yield a false-negative result if the patient is on antibiotics at the time of aspiration (often for UTI, URI, or cellulitis). A repeat aspiration after 2 weeks off antibiotics can yield more accurate information, or an alpha-defensin synovial fluid immunoassay can be performed as these results are not affected by antibiotics.
Della Valle et al. reviewed preoperative and intraoperative evaluation for periprosthetic infection. They state that patients should be off antibiotics for 2 weeks prior to aspiration as being on antibiotics can lead to false-negative results. They state there is no gold standard single test to diagnose a periprosthetic infection so a combination of tests will lead to the highest proportion of correct diagnoses.
Lachiewicz et al. reviewed 142 patients who underwent revision total hip arthroplasty and had a preoperative aspiration. They found no patients were infected if their implant had been in for >5 years and they had a normal ESR. They conclude that all patients with a painful total hip should be aspirated if
<5 years have elapsed from the index surgery or they have an elevated CRP.
Kelly et al. looked at synovial alpha-defensin in cases of an unclear diagnosis of PJI. They retrospectively reviewed 41 cases of possible PJI with prior aspiration and found in patients with recent antibiotic use alpha-defensin correctly diagnosed 83% of patients. They concluded alpha-defensin may be a useful data point in patients with and unclear diagnosis in cases of recent antibiotic use, equivocal laboratory findings, or suspected false-positive or false-negative cultures.
Figure A shows a left total hip with immediate post-op and current radiographs with interval loosening of the acetabular component.
Incorrect Answers:
OrthoCash 2020
An otherwise healthy 62-year-old woman presents 6 months postop from a TKA. For the past 6 weeks, she has noted pain and swelling with one week of drainage from the knee as seen in Figure A. Inflammatory markers and aspiration cell counts are elevated. Which of the following treatments give her the highest chance of eradication of infection?

Chronic lifelong suppressive antibiotic therapy
Urgent debridement, antibiotics, and implant retention (DAIR)
Urgent irrigation and debridement with modular component exchange
stage revision of all components
stage revision of all components Corrent answer: 5
The patient has a confirmed chronic postoperative periprosthetic joint infection (PJI) based on positive aspiration and a draining sinus. A 2-stage revision would give her the best chance of successful eradication.
Chronic PJI are difficult to eradicate without the removal of components due to biofilm on the prosthesis surface. A 2-stage revision with the removal of all components and placement of an antibiotic-eluting spacer and 6 weeks of culture directed IV antibiotics is the gold standard for chronic infections.
Parvizi et al. reviewed the literature on diagnostic strategies for assessing PJI and compared these data to a single large-volume institution's findings. Joint fluid aspirates with high cell counts and high percentage-neutrophils as well as positive FDG-PET scans have high sensitivities for diagnosing periprosthetic infections. While properly performed aspirates and intraoperative cultures
have near-perfect specificities (0.97, 1.0 respectively), they found a 10-14% false-negative rate. They go on to describe their institutional diagnostic protocol defining numerical cutoffs based on predictive value thresholds.
Koyonos et al. performed a single-institution retrospective review of irrigation and debridement alone for various time intervals from index surgery (acute, acute delayed, and chronic). They found irrigation and debridement was an ineffective way to definitively treat PJI for acute post-op infections (<4 wks from surgery 69% failure), acute delayed infections (>4 wks from surgery, 56% failure), and chronic infections (months after index surgery, 72% failure). They concluded that I&D should be reserved for acute onset symptoms with a non-staphylococcal infection in an optimized host with a previously normal total joint arthroplasty.
Figure A shows a draining sinus tract over a standard midline TKA incision. Incorrect Answers:
successful infection eradication compared to 2-stage revision.
OrthoCash 2020
A 62-year-old female is referred to you by your partner for continued groin pain after undergoing an uneventful total hip arthroplasty utilizing the direct anterior approach. On exam, her pain is reproduced with resisted hip flexion. Workup for infection and loosening were negative. Radiographs and CT show well-placed implants. An ultrasound-guided lidocaine injection eliminated her pain completely for one day but returned. When arthroscopically addressing the pathologic structure, in what position should the hip be placed to avoid damaging the nearest major neurovascular structure?
Internal rotation to avoid the sciatic nerve
Internal rotation to avoid the ascending medial femoral circumflex artery
Internal rotation to avoid the femoral neuromuscular bundle
External rotation to avoid the ascending medial femoral circumflex artery
External rotation to avoid the femoral neurovascular bundle
This patient has iliopsoas tendinitis following total hip arthroplasty (THA). The leg should be externally rotated when performing extra-capsular tenotomy to protect the femoral neurovascular bundle.
Hip arthroscopy was a previously daunting procedure given the deep location of the hip joint, limitations of available instrumentation, and close proximity of the peri-articular anatomy. Significant advances in these areas have allowed for safer and more reproducible results in treating common hip pathology.
Iliopsoas tenotomy is now commonly performed but relies heavily on a thorough understanding of the surrounding anatomy. The two most common iliopsoas tenotomy techniques are the trans-capsular and extra-capsular releases. Trans-capsular release involves making a capsulotomy between the anterior labrum and zona orbicularis to access the iliopsoas tendon (Illustration A). The extra-capsular tenotomy is more commonly done following total hip arthroplasty and involves accessing the iliopsoas at the level of the lesser trochanter (Illustration C). Both techniques require slight flexion of the hip and external rotation to bring the tendon towards the surgeon and away from the femoral neurovascular structures.
Robertson and Kelly performed a cadaveric study demonstrating which neurovascular structures are at risk with common arthroscopic portals. The traditional anterior portal (AP) was an average of 15mm from the branches of the lateral femoral cutaneous nerve. They concluded that by shifting the anterior portal further lateral to a longitudinal line drawn from the ASIS, the LFCN is less in danger.
Ilizaliturri et al. performed a prospective trial following two cohorts undergoing either the extra-capsular or trans-capsular iliopsoas tenotomy. They found both cohorts had significant improvements in both groups without significant differences between them. This shows arthroscopic/endoscopic iliopsoas tenotomy to be a safe and reliable procedure.
Illustration A shows the trans-capsular iliopsoas tenotomy. Illustration B is a panel intra-operative photos of this release, showing the subsequent release of the bright white psoas tendon (PT) to reveal the iliac muscle fibers (ZO= zone orbicularis, AHC= anterior hip capsule). Illustration C is an axial MRI at the level of the central compartment, with the femoral neurovascular bundle (arrow) and psoas labelled.
Illustrations D and E demonstrate the extra-capsular iliopsoas tenotomy. Again, note the bright appearance of the psoas tendon before release.
Illustration F is an axial MRI at the level of the lesser trochanter with the femoral neurovascular bundle (arrow) and psoas tendon labelled.
Incorrect Answers:

OrthoCash 2020
A 65-year-old male presents to your clinic with right hip pain. He underwent right metal-on-metal total hip arthroplasty (THA) 20 years prior and had been doing well until 5 years ago. He notes groin pain with ambulation and thigh pain when getting up from a seated position. His radiographs are shown in Figure A. MRI studies with metal artifact reduction sequence reveal a pseudotumor noted in the periprosthetic soft tissues. Which of the following is true with respect to this patient's clinical picture?

The majority of patients with metal-on-metal THA have a pseudotumor
The presence of a pseudotumor is associated with increased implant linear wear rate
The pseudotumors are composed of both macrophages and lymphocytes, with macrophages being predominant
The presence of a pseudotumor is associated with relatively high ratio of serum cobalt to chromium
Observation is recommended given the absence of loosening on radiographs Corrent answer: 2
The patient has a metal-on-metal (MoM) THA with a pseudotumor present on MRI studies. The presence of a pseudotumor is associated with increased linear wear of both the acetabulum and the femoral components.
A pseudotumor is a mass-forming tissue reaction caused by metal-on-metal wear most notably seen in MoM total hip arthroplasty. These lesions are noted in 10-15% of patients with MoM THAs. The etiology is unclear but is thought to be associated with local high wear debris as well an increased hypersensitivity to metal wear. The lesions are lymphocyte-predominant although macrophages are also present throughout. Treatment of patients with hip pain and pseudotumor noted on MRI studies is generally revision to a ceramic-on-polyethylene THA.
Kwon et al. compared the in vivo wear rate of MoM THAs revised due to a pseudotumor compared to those MoM THAs that were revised for other reasons. The authors noted that the pseudotumor group (n = 8) had median linear wear of the femoral component of 8.1 microns/year and the non-pseudotumor group (n =22) had a linear wear rate of 1.79 microns/year. A similar discrepancy was noted for acetabulum wear with 7.36 microns/year in the pseudotumor group compared to 1.28 microns/year in the non-pseudotumor group. The authors conclude that the presence of a pseudotumor is associated with increased wear at the metal-on-metal articulation.
Daniel et al. performed a review of pseudotumors associated with MoM THA. They reviewed the potential causes to include foreign-body reaction, hypersensitivity and wear debris. They discussed that patients with pseudotumors associated with a MoM THA should undergo prompt revision to a nonmetal-on-metal bearing THA since prolonged delay can lead to soft tissue envelope compromise, recurrent dislocations, nerve palsies, and femoral artery stenosis. Furthermore, they also noted that hip function scores for patients who had revision for pseudotumors were significantly worse than those for patients who had MoM THA revision for other reasons.
Figure A is an AP pelvis showing the characteristic appearance of an MoM THA with a large metallic femoral head.
Incorrect Answers:
OrthoCash 2020
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
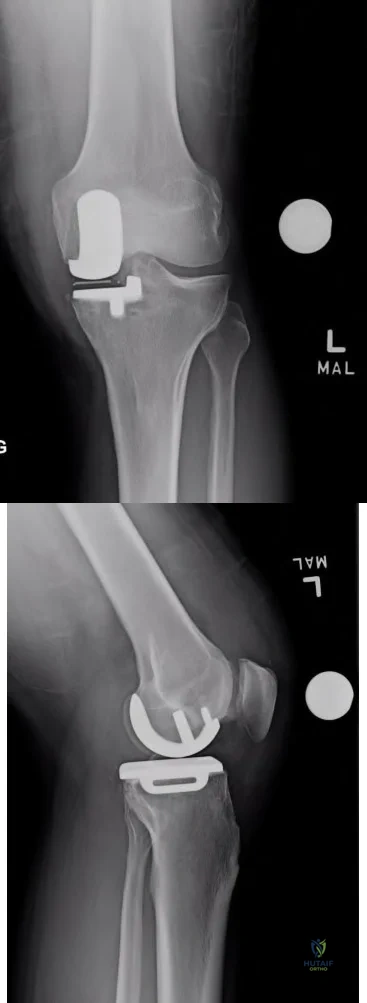
Question 88
A 30-year-old right hand-dominant woman is seen in the trauma unit after a high-speed motor vehicle accident. She sustained a right shoulder anterior dislocation that is gently reduced under sedation. A CT scan is shown in Figure 3. If left untreated, the patient is at greatest risk for
Explanation
more common.
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med 1998;26:41-45.
Question 89
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Explanation
REFERENCES: Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: Review of a series of 25 cases. J Pediatr Orthop 1987;7:444-449.
Question 90
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 91
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Explanation
3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 92
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 93
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery? Review Topic
Explanation
Question 94
Which of the following changes is seen with age and degeneration in the intervertebral disk? Review Topic
Explanation
Question 95
- Which of the following injuries is most commonly associated with a fracture of the scapular body?
Explanation
Question 96
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?
Explanation
REFERENCES: Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
Gerster JC, Landry M, Dufresne L, Meuwly JY: Imaging of tophaceous gout: Computed tomography provide specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002;61:52-54.
Question 97
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Explanation
Question 98
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 99
What is the most likely diagnosis? Review Topic
Explanation
Question 100
below show the radiograph and the MRI scan obtained from a year-old woman with a month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
