Orthopedic Board Prep MCQs: Arthroplasty, Fracture, Hip, Knee, Shoulder | Part 116
Key Takeaway
This page offers Part 116 of a comprehensive orthopedic surgery board review quiz, featuring 100 high-yield MCQs. Designed for orthopedic residents and surgeons, it mirrors OITE and AAOS exam formats. Utilize interactive Study or Exam modes with explanations to optimize your board certification preparation for ABOS and AAOS exams.
About This Board Review Set
This is Part 116 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 116
This module focuses heavily on: Arthroplasty, Fracture, Hip, Knee, Shoulder.
Sample Questions from This Set
Sample Question 1: The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the...
Sample Question 2: Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?...
Sample Question 3: A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is seve...
Sample Question 4: Figure 61 shows the current radiograph of a 69-year-old woman who fell getting out of bed 10 months ago. At the time of injury she was diagnosed with a nondisplaced humeral surgical neck fracture. After 2 weeks of sling immobilization, phys...
Sample Question 5: When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
REFERENCES: Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 2
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?
Explanation
REFERENCES: Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Ritter MA, Keating EM, Faris PM: Closed wound drainage in total hip or total knee replacement: A prospective, randomized study. J Bone Joint Surg Am 1994;76:35-38.
Question 3
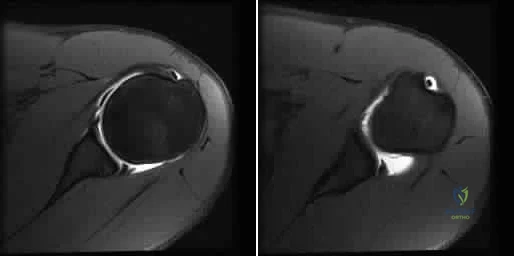
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 4
Figure 61 shows the current radiograph of a 69-year-old woman who fell getting out of bed 10 months ago. At the time of injury she was diagnosed with a nondisplaced humeral surgical neck fracture. After 2 weeks of sling immobilization, physical therapy was started for range of motion. She continues to have pain and is unable to elevate her arm. What is the most likely diagnosis?

Explanation
(SBQ12TR.96) Interleukin-6 levels have been shown to be a reliable measure of which of the following?
Osteoporosis
Severity of injury
Sarcomatous tumor burden
Bone turnover
Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production. Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
Question 5
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 6
What type of metastatic tumor most often has a lytic radiographic appearance?
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Mulvey RB: Peripheral bone metastasis. Am J Roentgenol 1964;91:155.
Question 7
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
REFERENCES: Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692.
Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
Rao R: Neck pain, cervical radiculopathy, and cervical myelopathy: Pathophysiology, natural history, and clinical evaluation. Instr Course Lect 2003;52:479-488.
Question 8
After the athlete undergoes the appropriate treatment of the postsurgical complication and recovers without further incident, which muscle most likely will be last to experience return of function?
Explanation
This patient sustained an eccentric contracture (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest
potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed.
The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared to the 2-incision technique. The most troubling complication for most surgeons is the development of a PIN palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABC nerve injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button.
Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The EIP is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC followed by the ECU, EDQ, and, finally, the EIP.
RESPONSES FOR QUESTIONS 26 THROUGH 27
Anterior tibial artery
Posterior tibial artery
Superficial peroneal nerve
Deep peroneal nerve
Match the neurovascular structure at risk (listed above) with the compartment undergoing fasciotomy (listed below).
Question 9
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 10
Figures 38a and 38b are the MRI scans of a 28-year-old man who reports progressively worsening severe back pain for the past 3 months. He denies fevers, chills, weakness, or neurologic dysfunction. Examination reveals tenderness to palpation over the lumbar spine but normal neurologic findings. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein; blood cultures are positive for methicillin-sensitive Staphylococcus aureus. In addition to intravenous antibiotics, what is the next step in management? Review Topic

Explanation
Question 11
What structure is the primary restraint to inferior translation of the shoulder? Review Topic
Explanation
Question 12
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
REFERENCE: Herring JA (ed): Tachjians Pediatric Orthopedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 2, p 984.
Question 13
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten-year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
Explanation
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates 10-year risk of fracture based on the following variables: age, sex, race, height, weight,
BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool (http://www.shef.ac.uk/FRAX/tool.aspx?country=9). Illustration B shows the clinical risk factors considered in FRAX calculation.
Incorrect Answers:
Question 14
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 15
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Kamineni S, Hirahara H, Pomianowski S, et al: Partial posteromedial olecranon resection:
A kinematic study. J Bone Joint Surg Am 2003;85:1005-1011.
Question 16
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 17
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter “A”?
Explanation
REFERENCES: Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 400, 405, 407, 450.
Question 18
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
Question 19
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 20
A 51-year-old butcher has an 18-month history of recalcitrant medial elbow pain, which is affecting his occupational demands. He describes the pain as mainly anterior and distal to the medial epicondyle. His symptoms are exacerbated with resisted wrist flexion and forearm pronation. On examination, he is also found to have a positive Tinel's sign at the elbow with weakness of intrinsic strength. He has attempted physical therapy, activity modification, bracing, and anti-inflammatory medication without any significant improvement. Presurgical counseling should include the understanding that
Explanation
of pathologic tissue, release of the flexor carpi radialis - pronator teres origin, and/or repair of the flexor carpi radialis - pronator teres origin. Several authors have raised concern of the impact of concomitant ulnar neuropathy on results following surgical treatment for medial epicondylitis. Kurvers and Verhaar and Gabel and Morrey, among others, have reported a statistically significant association between concomitant ulnar neuropathy and worse outcomes following surgery. Most patients can anticipate a return to prior activity levels after surgery without any consistently reported loss of flexor/pronator strength. Prior corticosteroid injections
have not been found to impact results.
Question 21
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 22
What condition favors pollicization in hypoplasia of the thumb?
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. View Abstract at PubMed
Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.View Abstract at PubMed
Question 23
- Successful healing of a meniscal repair is most likely associated é which of the following tear patterns?
Explanation
Arnoczky et al described the vascular supply to the meniscus and showed that tears within the outer one third of the meniscus have the best healing potential. Rim width is the most important prognostic factor for meniscal repairs; the vascular one third of the meniscus is most conductive to healing. Scott et al found better results when the tear was within 2mm of the meniscosynovial junction. Stone et al found improved healing with rim widths of 6mm or less. Tenuta et al found best results within a rim width of 3mm or less.
Question 24
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 25
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 26
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 27
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 28
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30 degrees and 90 degrees. What is the best treatment strategy at this time? Review Topic
Explanation
Question 29
An 85-year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 1.0 mg/L (reference range 0.08 to 3.1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly difficult with activities of daily living and mobility.
Question 30
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
REFERENCES: Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463.
Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.
Nunez D Jr: Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries:
A prospective study. J Trauma 2000;48:988-989.
Question 31
A 74-year-old man underwent a hemiarthroplasty with acromioplasty for rotator cuff tear arthropathy 2 years ago. Despite continued therapy, he is still unable to elevate his arm beyond 40 degrees. Attempted elevation is painful and demonstrates bulging in the anterosuperior aspect of his shoulder. Radiographs show a well-positioned hemiarthroplasty without signs of loosening. What is the most appropriate treatment for this patient? Review Topic
Explanation
Question 32
What is the most appropriate orthosis for hallux rigidus?
Explanation
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Watson AD, Wapner KL: Foot and ankle reconstruction, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, p 635.
Question 33
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?
Explanation
REFERENCES: Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398.
McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Schock HJ, Pinzur M, Manion L, et al: The use of the gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br 2007;89:1055-1059.
Question 34
A 23-year-old woman with recurrent anterior instability undergoes an open Bankart procedure. Six months after surgery the patient reports shoulder

Explanation
Question 35
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 36
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 37
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 38
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 39
A 45-year-old male laborer injured his right elbow trying to catch a heavy object. He has antecubital pain and forearm ecchymosis. MRI scans are shown in Figures 4a and 4b. Nonsurgical management of this injury is most associated with the loss of Review Topic
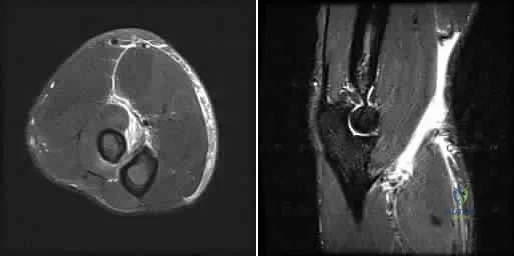
Explanation
Question 40
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 41
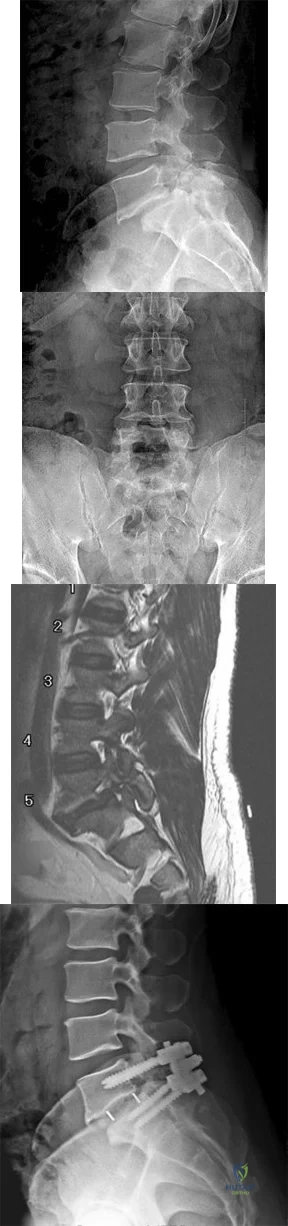
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 42
A 7-year-old boy is seen for follow-up for a scoliotic deformity. His parents are concerned because his deformity seems to have increased. He has no pain and is neurologically intact. A radiograph is shown in Figure 94, and measurement of his curve reveals that it has increased 10 degrees. What is the most appropriate recommendation for this patient at this time? Review Topic

Explanation
Question 43
Figure 93 shows the axial T2-weighted MRI scan of the lumbar spine of a 70-year-old man. The arrow points to which of the following structures? Review Topic
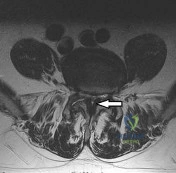
Explanation
(SBQ12SP.14) A 36-year-old male presents with acute onset of right buttock and leg pain following lifting a heavy object. On physical exam he has weakness to knee extension, numbness over the medial malleolus, and a decreased patellar reflex. Which of the following would most likely explain this clinical presentation. Review Topic
Lumbar arachnoiditis
L4/L5 paracentral disc herniation
L3/L4 far lateral (foraminal) disc herniation
L4/L5 far lateral (foraminal) disc herniation
L5/S1 far lateral (foraminal) disc herniation
The clinical presentation is consistent with a L4 radiculopathy. A L4/L5 far lateral (foraminal) disc herniation would compress the exiting root (L4) and cause these symptoms.
The location of a prolapsed lumbar disc determines its symptoms. Central disc herniations may give rise to back pain or cauda equina syndrome. Paracentral disc herniations (90-95% of cases) affect the traversing nerve root. Far lateral disc herniations (5-10%) affect the exiting nerve root.
Gregory et al. summarize physical signs in lumbar disc herniation. They state that the straight-leg-raise is the most sensitive (73-98% sensitive) test and the crossed straight-leg-raise is the most specific (88-98% specific) test for lumbar disc herniation. Other specific tests include weak ankle dorsiflexion (89% specific), absent ankle reflex (89% specific), and calf wasting (94% specific, but a late finding).
Illustration A shows how a paracentral L4/L5 disc herniation affects the traversing L5 root, but a far lateral L4/L5 disc herniation affects the L4 root. Illustration B shows the dermatomal distribution of pain with root involvement from L3 to S1.
Incorrect Answers:
Question 44
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 45
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of
Explanation
REFERENCES: Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350.
Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Tivnon MC, Anzel SH, Waugh TR: Surgical management of osteochondritis dissecans of the capitellum. Am J Sports Med 1976;4:121-128.
Question 46
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 47
below depict the radiographs obtained from a year-old man who has had swelling in his right knee for 2 years, with minimal pain. He did not note an injury to the knee but has been unable to ambulate without crutches during this period. His past history is unremarkable, and he denies a history of diabetes or problems. The social history reveals that he emigrated from China, and he works at a desk job. Physical examination shows a healthy man in no acute distress. Range of motion of the right knee is 5° to 120° actively and 0° to 120° passively, without pain. Sensation is decreased on the bottom of both feet, but otherwise the neurologic examination is unremarkable. Laboratory testing reveals a positive rapid plasma reagin (RPR) test. What is the best next step?
Explanation
This patient has a neuropathic knee caused by neurosyphilis, as shown by the joint destruction on the radiographs, with a lack of pain and a positive RPR test. He has a low-demand job and would be best treated with a hinged knee arthroplasty to provide stability for his knee.
Question 48
A 51-year-old female sustained a comminuted radial head fracture with 4 fragments and an associated elbow dislocation. She was initially closed reduced and splinted with the elbow joint in a reduced position and presents to the orthopedists office 10 days later. In response to the patient's question of what treatment offers the best chance for a good outcome, the surgeon should recommend?

Explanation
Question 49
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Explanation
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 50
Figure 99 is the radiograph of an 18-year-old National Collegiate Athletic Association Division I basketball player who jumped for a basket. After landing, he was unable to put weight on his left great toe. He developed pain, swelling, and ecchymosis maximally around the sesamoids. When assessing stability of the first metatarsophalangeal joint, he appears to have more laxity on the left. What is the best next step?

Explanation
This patient jumped on his forefoot and landed with pain in his great toe. His radiograph shows possible increased space between the sesamoids and the base of the phalanx. A comparison radiograph on the other side will reveal if this position is normal for this patient. If findings are asymmetric, turf toe injury is a possibility based on this patient's symptoms and mechanism of injury.
RECOMMENDED READINGS
Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clanton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013 Mar;34(3):403-8. doi: 10.1177/1071100712464953. Epub 2013 Jan 14. PubMed PMID: 23520299. View
Abstract at PubMed
McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009 Jun;14(2):135-50. doi: 10.1016/j.fcl.2009.01.001. Review. PubMed PMID: 19501799. View Abstract at PubMed
Question 51
A 72-year-old woman presents for follow-up after elbow surgery. Her radiographs are shown in Figures A and B. Which of the following pre-operative diagnoses is a relative contraindication to the use of this prosthesis design? Review Topic
Explanation
Unconstrained (unlinked or resurfacing prosthesis) TEA depend on intact bony and ligamentous constraints for stability. These are appropriate for humeroulnar conditions with intact collateral ligaments and radiocapitellar articulation e.g. osteoarthritis, post-traumatic arthritis, intra-articular distal humerus fracture, and malunion of the distal humerus. Conditions with increased risk of instability (ligamentous injury, rheumatoid arthritis) will benefit from a linked or semiconstrained prosthesis.
Mansat et al. reviewed the Coonrad-Morrey linked (semi-constrained) TEA implant in 70 patients after 5 years. They found that patients with inflammatory arthritis had higher function than those with traumatic conditions (fractures, nonunions and posttraumatic arthritis). Survival rate was 98% and 91% at 5 and 10 years, respectively. They concluded that this implant provided satisfactory treatment for different indications although radiolucent lines and bushing wear were a concern.
Hildebrand et al. reviewed the functional outcome of the Coonrad-Moorey prosthesis in 51 elbows after 50 months. The inflammatory arthritis group had higher performance scores than the traumatic/post-traumatic conditions group. Isometric extensor torque was found to be less than the nonoperated side. Radiolucency was noted in 11 elbows.
Figures A and B show an unconstrained TEA with radial head replacement. Illustration A shows more examples of unconstrained TEA. Illustration B shows a semiconstrained TEA. The arrow points to the anterior flange. Illustration C shows radiolucent lines around the stems. Illustration D shows severe bushing wear leading to locking mechanism failure. Illustration E is a table comparing linked and unlinked implants.
Incorrect Answers:
Question 52
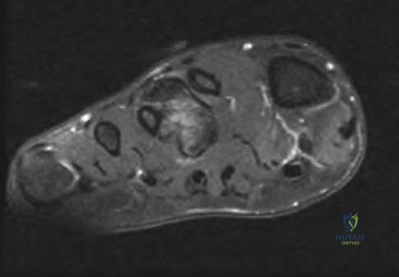
An athletic 55-year-old man reports a painless mass in the anterior aspect of the thigh that appeared 3 weeks ago and has not changed in size. The patient denies any history of trauma. Examination reveals a firm, well-defined nontender mass in the anterior thigh and no inguinal adenopathy or cutaneous changes. Plain radiographs are unremarkable. T1- and T2-weighted MRI scans are shown in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 53
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 54
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 55
A patient has a large T11-T12 disk herniation that is causing substantial compression of the spinal cord. The patient reports walking imbalance over the past few weeks. Examination of the patient's reflexes is likely to show Review Topic
Explanation
Question 56
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 100.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 106.
Question 57
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 58
A 21-year-old basketball player reports increased left shoulder pain with all lifting and overhead activities. He denies any history of dislocations. Axial MRI arthrogram images are seen in Figures 34a and 34b. An expected finding on physical examination of the shoulder would be positive findings for which of the following tests? Review Topic
Explanation
then abducted, while maintaining the axial load, and the patient's subjective and objective response is observed. Comparison to the contralateral shoulder is important, especially if painless subluxation is noted, to determine potential evidence of generalized joint laxity.
Question 59
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1986;68:724-731.
Pollock RG, Bigliani LU: Recurrent posterior shoulder instability: Diagnosis and treatment.
Clin Orthop 1993;291:85-96.
Question 60
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 61
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
inlay reconstruction.
REFERENCES: Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Burks RT, Schaffer JJ: A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop 1990;254:216-219.
Question 62
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 63
Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm 3 , a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm 3 . What treatment has the best potential to optimize his survival and independence?
Explanation
REFERENCES: Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Pinzur MS, Smith D, Osterman H: Syme ankle disarticulation in peripheral vascular disease and diabetic foot infection: The one-stage versus two-stage procedure. Foot Ankle Int 1995;16:124-127.
Question 64
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 65
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
(TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene).
REFERENCES: Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Roodman GD: Mechanisms of bone metastasis. N Engl J Med 2004;350:1655-1664.
Question 66
In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
Explanation
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 67
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
Explanation
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
Question 68
What is the most likely primary cause of decreased success rates of bony fusion in smokers undergoing lumbar arthrodesis?
Explanation
REFERENCES: Andersen T, Christensen FB, Laursen M, et al: Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine 2001;26:2623-2628.
Silcox DH III, Daftari T, Boden SD, et al: The effect of nicotine on spinal fusion. Spine 1995;20:1549-1553.
Question 69
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
REFERENCE: Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 70
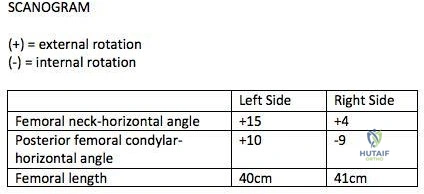
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 71
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist’s office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
Explanation
Question 72
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Explanation
REFERENCES: Campbell P, Ma S, Yeom B, McKellop H, Schmalzried TP, Amstutz HC: Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. J Biomed Mater Res 1995;29:127-131.
Shanbhag AS, Jacobs JJ, Glant TT, Gilbert JL, Black J, Galante JO: Composition and morphology of wear debris in failed uncemented total hip replacement. J Bone Joint Surg Br 1994;76:60-67.
Maloney WJ, Smith RL, Schmalzried TP, Chiba J, Huene D, Rubash H: Isolation and characterization of wear particles generated in patients who have had failure of a hip arthroplasty without cement. J Bone Joint Surg Am 1995;77:1301-1310.
Question 73
03 Early failure of a unicompartmental knee arthroplasty that is the result of polyethylene wear is primarily caused by
Explanation
back to this question next question
Question 74
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 75
In total hip arthroplasty, increasing the perpendicular distance from the center line of the femur to the center of rotation of the femoral head (femoral offset) results in
Explanation
include an increased range of motion, better mechanical advantage for the abductors and decreased instability because of better soft tissue tension. According to Charnley,
increasing the femoral offset should improve the abductor lever arm which should decrease the abductor force required for walking, and therefore decrease the energy requirement for gait as well as the overall joint reactive force. The largest possible disadvantage of increasing the femoral offset is increasing the out of plane bending moment which puts stress on the prosthetic stem. Poly wear is a direct effect of surface area contact which is not changed with femoral Offset.
Question 76
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 77
Which of the following statements best describes the anatomy of the sartorial branch of the saphenous nerve during medial meniscal repair?
Explanation
REFERENCES: Dunaway DJ, Steensen RN, Wiand W, et al: The sartorial branch of the saphenous nerve: Its anatomy at the joint line of the knee. Arthroscopy 2005;21:547-551.
Rodeo SA: Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect 2000;49:195-206.
Question 78
03 A 23 year old sustains an isolated right knee dislocation in an MVA. A closed reduction is performed and confirmed with radiographs. What is the next appropriate study?
Explanation
OKU Truama 2 says “the use of ABI with the blood pressure cuff and Doppler evaluation of the distal circulation has been proposed as effective in determining any occult vascular injury. A ratio > 0.9indicates a normal study.”[1] The referenced article confirms this. “Confirmation of the safety and accuracy of physical exam in the evaluation of knee dislocation for injury of the popliteal artery.” J. Trauma2002; 52: 247-252
back to this question next question
[1] OKU Trauma 2 pg 151-153
Question 79
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 80
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
REFERENCES: Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
Kibler WB (ed): ACSM’s Handbook for Team Physician. Philadelphia, PA,
Williams & Wilkins, 1996, p 151.
Question 81
What anatomic site is considered at highest risk for pathologic fracture?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1055.
Question 82
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
Explanation
REFERENCE: Simon JA, Puopolo SM, Capla EL, et al: Accuracy of the axillary projection to determine fracture angulation of the proximal humerus. Orthopedics 2004;27:205-207.
Question 83
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 84
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 85
After sustaining a muscle contusion injury, prolonged immobilization leads to Review Topic
Explanation
Question 86
What sign or symptom may occur with cubital tunnel syndrome that does not occur with Guyon neuropathy?
Explanation
Ulnar neuropathy at the elbow is termed cubital tunnel syndrome, whereas ulnar nerve compression at the wrist is considered Guyon neuropathy. Patients with cubital tunnel syndrome have numbness on the dorsal ulnar aspect of the hand due to involvement of the dorsal ulnar sensory nerve branch (DUSN). Ulnar neuropathy at both the elbow and the wrist may manifest with abnormal sensation about the volar ring and small fingers and with weakness of the interosseous muscles, which can lead to a positive Froment sign. The Froment sign is considered positive when flexion of the thumb interphalangeal joint occurs to compensate for a lack of adductor function. Patients with a Guyon neuropathy do not have symptoms of numbness in the dorsal ulnar distribution, because the DUSN branch arises more proximally in the forearm and is not compressed in the ulnar tunnel at the wrist.
Question 87
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and

Explanation
Question 88
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.
Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL,
American Academy of Orthopaedic Surgeons, 2003, pp 135-143.
Question 89
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?
Explanation
REFERENCES: Gould N, Seligson D, Gassman J: Early and late repair of lateral ligament of the ankle. Foot Ankle 1980;1:84-89.
Hamilton WG, Thompson FM, Snow SW: The modified Brostrom procedure for lateral ankle instability. Foot Ankle 1993;14:1-7.
Chrisman OD, Snook GA: Reconstruction of lateral ligament tears of the ankle: An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am 1969;51:904-912.
Evans DL: Recurrent instability of the ankle: My method of surgical treatment. Proc R Soc Med 1953;46:343.
Watson-Jones R: Fractures and Joint Injuries, ed 3. Baltimore, MD, Williams and Wilkins, 1946, p 234.
Liu SH, Baker CL: Comparison of lateral ankle ligamentous reconstruction procedures. Am J Sports Med 1994;22:313-317.
Brostrom L: Sprained ankles: VI. Surgical treatment of “chronic” ligament ruptures. Acta Chir Scand 1966;132:551-565.
Question 90
What type of medial collateral ligament tear heals the most reliably? Review Topic
Explanation
Question 91
Figures 26a and 26b show the radiograph and MRI scan of a 22-year-old man with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 92
The development of complex regional pain syndrome (CRPS) following distal radius fracture is associated with what factor?
Explanation
CRPS is an uncommon complication following distal radius fractures; its incidence is reported to range between 1% and 37%. Two recent studies have evaluated for risk factors in the development of CRPS following distal radius fractures. Female gender, concomitant fracture of the distal ulna, and surgical treatment were all associated with an increased likelihood of CRPS, as was fibromyalgia. Older age was identified as conferring both an increased and a decreased risk for CRPS in the two studies.
Question 93
positive skin-test response to CSD skin-test antigen; 3) characteristic lymph node lesions; and 4) negative laboratory investigation for unexplained lymphadenopathy. Treatment consists of azithromycin, ciprofloxacin, doxycycline, or multiple other antibiotics, all of which have been used successfully. Radiation therapy and chemotherapy would be reserved for malignant diseases and would not be appropriate in this setting. Treatment is necessary for this infectious entity; therefore, observation or physical therapy is not indicated.
Explanation
A 56-year-old right hand dominant male presents to your office complaining of right thumb pain worsened with pincer grip and using his mobile phone. He is a writer, and is having difficulty holding his pen. Radiographs from this visit are shown in Figure A. Compared with trapeziectomy alone, which of the following treatment options is likely to result in superior pain relief and improvement of key-pinch strength?

Trapeziometacarpal corticosteroid injection followed by aggressive occupational therapy
Trapeziectomy with interpositional palmaris longus arthroplasty
Trapeziectomy, interpositional arthroplasty, and palmar oblique ligament reconstruction using flexor carpi radialis autograft
Partial trapeziectomy with capsular interpositional arthroplasty
None of the above CORRECT ANSWER: 5
This patient has symptomatic basal joint arthritis with radiographic evidence of pantrapezial arthritis. Simple trapeziectomy has been shown to provide pain relief and improvement of key-pinch strength that is comparable to trapeziectomy plus interpositional arthroplasty.
Definitive surgical management of basal joint arthritis commonly involves excision of the diseased trapezium with concomitant interpositional arthroplasty at the carpometacarpal joint in an effort to mantain the height of the metacarpal. This is commonly done with flexor carpi radialis (FCR) or palmaris longus (PL) autograft. Recent studies have called into question the need for interpositional arthroplasty, suggesting that excision of the trapezium alone can provide non-inferior results.
Davis et. al. randomized 183 symptomatic trapeziometacarpal joints to one of three procedures: trapeziectomy alone, trapeziectomy with palmaris longus interpositional arthroplasty, or trapeziectomy with FCR interpositional arthroplasty and reconstruction of the palmar oblique ligament. For all patients, the thumb metacarpal was percutaneously pinned to the distal pole of the scaphoid to maintain the height of the digit. Patients were evaluated at three and 12 months post-operatively. At both time-points, they found no difference between groups with respect to subjective accounts of pain, function, stiffness, and weakness. Objective measures of thumb key-pinch strength were no different at either time point. The authors concluded that there may be no benefit to ligament reconstruction or tendon interposition in
the short term.
Li et. al. performed a systematic review of four randomized controlled trials and two systematic reviews to evaluate outcomes of trapeziectomy with and without LRTI for treatment of basal joint osteoarthritis. In their review, there were no statistically significant differences in post-op grip strength, pinch strength, visual analog pain scores, DASH scores, and complications. The authors concluded that both procedures produced similar clinical results.
Raven et. al. performed a retrospective analysis of 54 patients who underwent one of three procedures for basal joint osteoarthritis: resection arthroplasty, trapeziectomy with tendon interposition, or trapeziometacarpal arthrodesis.
The authors found resection arthroplasty to be a simple procedure with longterm results pain and functional outcomes comparable to trapeziectomy with tendon interposition.
Naram et. al. retrospectively reviewed 200 patients who underwent simple trapeziectomy with or without LRTI and with or without Kirschner wire stabilization, or a Weilby ligament reconstruction. They found that patients undergoing trapeziectomy with LRTI or a Weilby procedure had a greater incidence of complications compared to trapeziectomy alone, including infection and reoperation.
Figure A is a plain radiograph demonstrating pantrapezial arthritis with the thumb trapeziometacarpal joint being most significantly affected.
Incorrect Answers:
A 31-year-old patient has had a left medial elbow mass for 1 month. The mass has been increasing in size and has now become very painful and erythematous. MRI scans are shown in Figures 76a and 76b. Laboratory studies show an erythrocyte sedimentation rate of 49 mm/h (normal 0 to 20 mm/h) and C-reactive protein level of 23 mg/L (normal 0 to 0.3 mg/L). Histology showed lymphoid tissue and multiple necrotizing granulomas. What organism is responsible for this clinical picture?
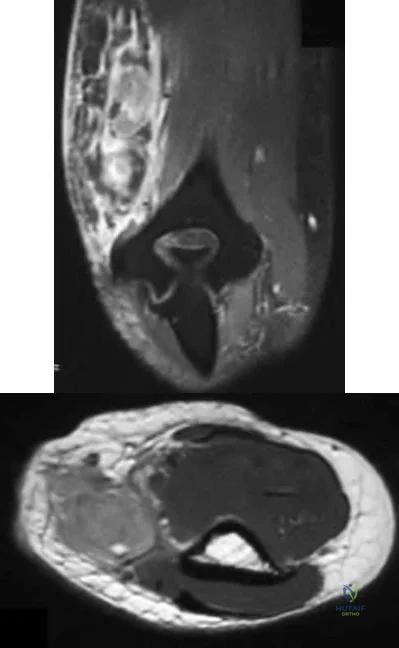
Borrelia burgdorferi
Trichophyton tonsurans
Bartonella henselae
Mycobacterium avium
Corynebacterium minutissimum
Cat scratch disease (CSD) is an important diagnosis for the orthopaedic surgeon to consider in the differential diagnosis of soft-tissue masses adjacent to epitrochlear or cervical lymph nodes. It is a soft-tissue tumor simulator and a high index of suspicion is necessary in all patients with upper extremity or head and neck adenopathy and a history of cat exposure. Although generally not required for diagnosis, cross-sectional imaging will reveal a mass with surrounding edema in an area of lymphatic drainage. A peripheral blood sample can be tested for Bartonella henselae - the offending organism with this diagnosis. Classically the histology of these lesions when biopsied will show multiple necrotizing granulomas. Mycobacterium avium is the only other organism that would demonstrate a granulomatous reaction and the location is classic for CSD. Borrelia burgdorferi is associated with Lyme disease.
Mycobacterium avium may be a source of immunocompromised infections in HIV patients. Trichophyton tonsurans and corynebacterium minutissimum are not associated with orthopaedic diseases.
A 45-year-old woman has a painful mass in the dorsum of the right wrist. It is firm and nontender to palpation. She states it has slowly gotten bigger over the past 3 years. You suspect a dorsal wrist ganglion. What is the most definitive way to confirm this diagnosis?
Observe it for 1 year to see if it changes dramatically in size.
Obtain a gadolinium enhanced MRI scan.
Obtain radiographs, looking for scapholunate joint degenerative changes.
Perform a needle aspiration and send the aspirate for cytologic examination.
Apply direct firm manual pressure over the mass to see if it can be ruptured.
Dorsal wrist ganglions are synovial cysts that arise most frequently from the scapholunate joint. They often extend between the extensor digitorum communis and extensor pollicis longus tendons at the wrist. Aspiration of the cyst is both oncologically safe if done appropriately and also the easiest way to definitively confirm the diagnosis. Clear, yellow viscous fluid/gel is most often aspirated. Cytologic evaluation is mandatory to exclude myxoid neoplasms.
Because the lesion has been present for 3 years, further observation is not warranted. The classic presentation, physical examination findings, and location make MRI and radiographs unnecessary. Manual rupture of the mass is not recommended.
A 28-year-old man fell while ice skating 6 months ago and has had ulnar-sided wrist pain ever since. The patient's wrist radiograph is shown in Figure A and a CT scan is shown in Figure B. What is the most appropriate treatment?
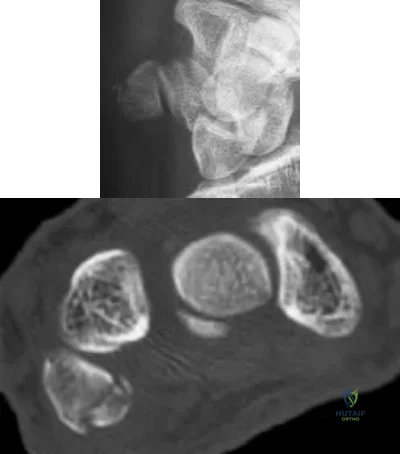
Scapholunate ligament repair
Excision of the hook hamate
Excision of the pisiform
Open reduction internal fixation of the hamate
Open reduction internal fixation of the pisiform
Based on clinical history and imaging shown, this patient has developed a pisiform fracture nonunion. Treatment of symptomatic nonunions of the pisiform is by pisiformectomy
Fractures of the pisiform are rare. They often occur in conjunction with injuries to the distal radius or carpus. Non-operative management with cast immobilization in 30 degrees of wrist flexion is the first line of treatment.
Symptomatic nonunions are treated with pisiformectomy.
Palmieri et al. performed pisiformectomies on 21 patients who had pisiform area pain that was refractory to conservative management. Patients had a history of painful union or nonunion of pisiform fractures, arthritis or FCU tendonitis. In all cases, wrist strength and mobility was retained.
Lam et al. reviewed the effect of pisiform excision on wrist function in patients with piso-triquetral dysfunction. After an average follow up of 65 months, 75%
of patients had complete relief of pisiform area symptoms. No differences in grip, wrist motion, strength or power were found in comparison to the contralateral side.
Figure A shows an oblique radiograph of a pisiform fracture nonunion. Figure B shows an axial CT scan sequence of the wrist. A pisiform fracture nonunion is identified with subtle comminution. The pisotriquetral joint appears to be congruent.
Incorrect Answers
A 32-year-old woman jammed her ring finger. Figures 77a and 77b show radiographs of the finger after a closed reduction. Which of the following interventions, if done correctly, is likely to result in the best possible final clinical outcome?

Early removal of a splint and application of continuous passive motion
Application of dynamic extension bracing after the first week
Maintaining reduction of the middle phalanx on the condyles of the proximal phalanx with dynamic external fixation
Open reduction and anatomic restoration of the middle phalanx articular surface
Surgical advancement of the volar plate into the middle phalanx base
The most important determinant in the final clinical outcome in proximal interphalangeal (PIP) joint fracture locations is the maintenance of the PIP joint alignment on the lateral view. This can sometimes be done with just extension block splinting, sometimes the fracture requires dynamic external fixation, and sometimes the fracture requires open reduction or volar plate arthroplasty. Good function can be the result in the setting of an incongruent middle phalanx base as long as the PIP joint alignment is maintained.
Continuous passive motion has not been shown to be of benefit. Whereas dynamic external fixation in a flexed position is a very good treatment, dynamic extension bracing will just precipitate loss of PIP joint reduction and is therefore not indicated. Whereas open reduction of the articular surface is theoretically desirable, it is generally impossible in the setting of the comminution of the volar middle phalanx base. Furthermore, open reduction and internal fixation by itself does not guarantee that the PIP joint alignment will be maintained, and typically it causes finger stiffness given the extensive surgical approach. Likewise, volar plate arthroplasty is a surgery of last resort and requires careful attention to PIP joint alignment before joint pinning. In this case, with characteristics of comminution, dynamic external fixation is the preferred choice.
A 20-year-old woman sustained a laceration to her volar forearm 4 cm proximal to the wrist flexion crease. She has numbness in the thumb, index, and middle fingers. After microscopic repair of the median nerve, 2 weeks of splinting, and commencement of a hand therapy program, the patient is most likely to require what secondary operation 6 months after the injury?
Tenolysis of the profundus tendons at the wrist
Nerve transfer of the ulnar motor nerve to the median motor nerve
Opponensplasty with the extensor indicis
Open carpal tunnel release
Transfer of the extensor digiti minimi to the first dorsal interosseous tendon
The patient sustained a laceration of the median nerve in what would be considered a low median nerve injury. Standard treatment entails exploration and microscopic repair of the median nerve. With a good quality nerve repair in a young adult, return of some sensory function (albeit reduced compared with the normal nerve) is usual. Return of motor function to the thenar muscles is more unpredictable. If the patient begins a therapy program within a few weeks after nerve repair, it is unlikely that tenolysis of the profundus tendons would be required. An open carpal tunnel release would be unlikely to change functional return. The patient would not be expected to have lost first dorsal interosseous function after a median nerve laceration because this muscle is innervated by the ulnar nerve. A neurotization procedure for low median nerve palsy has been described, but it consists of transfer of the distal anterior interosseous nerve into the median nerve motor fascicles, not transfer of the ulnar nerve. Therefore, the most likely secondary procedure required in this scenario is an opponensplasty procedure to improve thumb opposition.
What is the most efficient pressure for use with negative pressure wound therapy?
25 mm Hg
75 mm Hg
125 mm Hg
300 mm Hg
500 mm Hg CORRECT ANSWER: 3
In animal and clinical studies, a range of pressures between 50 mm Hg to 500 mm Hg were tested; the most efficient pressure was 125 mm Hg, resulting in a fourfold increase in blood flow, 63% increase in granulation tissue with continuous pressure, and 103% increase in granulation tissue with intermittent pressure. When 125 mm Hg pressures were compared with either those less than 50, or those greater than 250, there was a decrease in granulation tissue in swine models.
Figures 125a and 125b are the current radiographs of a 52-year-old man who sustained an injury to his dominant wrist 8 weeks ago. He is an alcoholic and does not remember the details of how he injured it. Paperwork showing what treatment he received at an
urgent care facility indicates that he was given a splint for his "sprained wrist." Examination reveals the pain is getting better, but there is persistent swelling and range of motion is very limited.
Recommended treatment at this time should consist of

discontinuation of the splint and commencement of a regimen of hand therapy.
casting for an additional 2 weeks and reassessment of the fracture healing at that time.
open reduction and internal fixation of the injury.
proximal row carpectomy.
wrist arthrodesis.
The injury represents a very uncommon presentation of a perilunate injury pattern. Whereas these injuries are sometimes overlooked on initial radiographic studies, they are usually recognized much sooner. In this case of a late presenting perilunate injury in a patient that is not entirely responsible, a proximal row carpectomy represents the best treatment option. Open reduction and internal fixation is generally not successful because of cartilage degeneration and contracture that has developed in the interim. No further splinting or casting is indicated, and neglecting the injury would be indicated only if the patient refused any further treatment. Wrist arthrodesis is generally indicated only as a salvage procedure if a proximal row carpectomy is unsuccessful.
A 47-year-old woman sustained a nondisplaced distal radius fracture 6 months ago and is unable to extend her thumb. When performing reconstruction using the extensor indicis proprius to the extensor pollicis longus transfer, tension is ideally determined by securing the tendons in what manner?
In maximum tension with the wrist and thumb in extension
In maximum tension with the wrist and thumb in neutral
In maximum tension with the wrist and thumb in flexion
According to the tenodesis effect with wrist flexion and extension
According to functional testing with the patient awake under local anesthesia
Extensor pollicis longus rupture can result from distal radius fractures. Synergistic tendon transfer can be achieved using the extensor pollicis longus as the motor donor. Whereas different schemes for achieving optimal tension are available, the most reliable method is to tension the repair under local anesthesia while asking the patient to perform thumb flexion and extension. Tendon transfer tension can be adjusted accordingly to achieve maximum extension without compromising active flexion range. Other methods of tensioning are estimates at best, and maximum tensioning in patients without neuromuscular disease is rarely used in tendon transfers.
Which of the following substances is likely to cause the most soft-tissue damage in the long term if injected into a fingertip under
high pressure?
Grease
Latex paint
Water
Oil-based paint
Chlorofluorocarbon-based refrigerant
This type of injury represents a difficult problem in hand surgery. The factors that most determine outcome after high-pressure injection injuries into the fingertip include: involvement of the tendon sheath, extent of proximal spread of the injected substance, pressure setting, and delay to surgical treatment.
The other factor that likely is most important is the type of substance injected. Water and latex-based paints are least destructive. Grease and chlorofluorocarbon-based substances are intermediate, but aggressive surgical debridement can restore reasonable function. Oil-based paints are highly inflammatory and can cause such chronic inflammation such that amputation may be the only reasonable treatment option despite early aggressive surgical treatment.
A 37-year-old woman has right-hand numbness and tingling. Based on the history and examination, carpal tunnel syndrome is suspected, and electrodiagnostic tests also point to the same diagnosis. The patient has worn night splints for the last 8 weeks with continued persistent symptoms. What is the next most appropriate step in management?
Continue the night splinting for 1 additional month.
Continue the night splinting for 3 more months.
Switch to full-time splinting and reevaluate in 1 month.
Switch to full-time splinting for 3 more months.
Perform carpal tunnel release.
Various nonsurgical management options exist for carpal tunnel syndrome (local and oral steroids, splinting, and ultrasound). All effective or potentially effective nonsurgical forms of management have measureable effects on symptoms within 2 to 7 weeks of the initiation of treatment. If a treatment is not effective within that time frame, a different treatment option should be
chosen. In this case, continued splinting is unlikely to improve symptoms and steroid injection or surgery is indicated.
A 46-year-old man sustains an injury to his left index finger while cleaning his paint gun with paint thinner. Examination reveals a small puncture wound at the pulp. The finger is swollen. What is the next most appropriate step in management?
Elevation and observation
Surgical debridement and lavage
Infiltration with corticosteroids
Infiltration with a neutralizing agent
Administration of antibiotics
High-pressure injection injuries are associated with a high risk of amputation. The risk of amputation is highest with organic solvents. The presence of infection and the use of steroids do not impact the amputation rate.
Amputation risk is lower if surgical debridement is performed within 6 hours. Elevation and observation would delay necessary care. Neutralizing agents may be used in specific situations, such as hydrofluoric acid exposure or chemotherapeutic agent extravasation, but in high pressure paint thinner injection, the best outcome is achieved through early surgical lavage.
A 54-year-old woman who has a history of undergoing left trapezium excision with ligament reconstruction and tendon interposition using the entire flexor carpi radialis performed by another surgeon, now reports left basilar thumb pain. Examination reveals pain and subluxation of the carpometacarpal joint with axial loading. The metacarpophalangeal joint hyperextends to 60 degrees, but radiographs show intact joint space. What is the best option to improve function?
Bracing with a hand-based thumb spica splint
Pinning of the carpometacarpal joint
Pinning of the carpometacarpal and metacarpophalangeal joints
Carpometacarpal revision stabilization
Carpometacarpal revision stabilization and metacarpophalangeal joint fusion
The patient previously underwent ligament reconstruction and tendon interposition. However, the previous surgeon failed to address metacarpophalangeal joint hyperextension, which leads to adduction contracture and collapse of the basilar joint. With the basilar joint causing pain and instability, repeat ligament reconstruction should be performed. Splinting alone is unlikely to resolve instability problems. Because the flexor carpi radialis was used, the next option is to use the abductor pollicis longus.
Additionally, the severe metacarpophalangeal joint hyperextension should be corrected by fusion. Simple pinning is unlikely to provide long-term stability when this degree of hyperextension exists.
When evaluating a patient with suspected purulent flexor tenosynovitis in the thumb, the distal forearm and little finger are found to be swollen as well. The most likely anatomic explanation is the existence of a potential space in which of the following?
Through the carpal tunnel
Across the midpalmar space
Communicating with the subcutaneous tissue
Superficial to the distal antebrachial fascia
Between the fascia of the pronator quadratus and flexor digitorum profundus conjoined tendon sheaths
Pyogenic flexor tenosynovitis is an infection within the flexor tendon sheath that can involve the fingers or thumb. The tendon sheaths begin at the metacarpal neck level and extend to the distal interphalangeal joint. In the little finger and the thumb, the sheaths usually communicate with the ulnar and radial bursae, respectively. The potential space of communication, Parona's space, lies between the fascia of the pronator quadratus muscle and flexor digitorum profundus conjoined tendon sheaths. Infection tracking through this space presents as a horseshoe abscess.
Which of the following proximal phalanx fractures can most reliably be treated with a closed reduction and avoidance of surgical measures?
Midshaft transverse diaphyseal fracture with 30 degrees of angulation
Long spiral diaphyseal fracture with 15 degrees of malrotation
Open fracture with skin loss and exposed extensor tendon
Distal condylar intra-articular fracture with minimal displacement
Proximal metaphyseal fracture location with 30 degrees of dorsal tilting
Proximal phalanx fractures are very common, but care must be taken to understand which injuries are reliably treated with nonsurgical measures, and which ones are prone to clinically symptomatic malunion without surgical treatment. The proximal metaphyseal location is a problematic fracture to get reduced with closed measures, and due to the forces of the extensor apparatus, is prone to collapse into the original deformity. Imaging is also frequently difficult because of the overlap of the other fingers and frequently the true angulation is underappreciated. With 30 degrees of angulation, consideration should be given to surgical treatment. Long oblique/spiral fractures with malrotation are also most reliably treated with multiple lag screws, because maintaining the reduction with nonsurgical measures is unreliable, and can lead to significant functional problems in the form of crossover of the fingers with gripping. Open fractures with skin loss clearly are treated with surgical measures. Distal condylar fractures with minimal displacement are another fracture pattern that have a high rate of loss of reduction when treated nonsurgically. Like most articular fractures, they are best treated with anatomic reduction and rigid internal fixation. By comparison, closed midshaft transverse diaphyseal fractures can usually be anatomically reduced and held in this position with closed measures.
Figure 3 shows an arthroscopic view of the radiocarpal joint from the 3-4 portal, looking volarly and radially (Sc=scaphoid, R=Radius). What structure is marked by the asterisk?
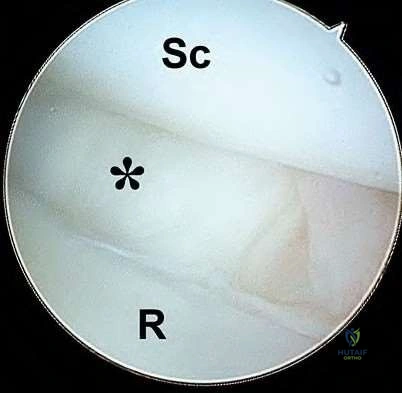
Radioscaphocapitate ligament
Scapholunate ligament
Palmar oblique ligament
Dorsal intercarpal ligament
Triangular fibrocartilage complex (TFCC)
The radioscaphocapitate ligament is a volar capsular structure running obliquely from the radial styloid to the scaphoid waist, ultimately inserting on the proximal radial aspect of the capitate. The radioscaphocapitate ligament is important in preventing ulnar translocation of the carpus. The scapholunate ligament is located intra-articularly, between the scaphoid and lunate. The dorsal intercarpal ligament is a dorsal structure, and not visible during routine wrist arthroscopy. The palmar oblique ligament connects the first and second metacarpal bases. The TFCC is visible during wrist arthroscopy between the radius and ulna.
A 22-year-old man reports a 2-week history of a burning pain along the dorsoradial aspect of the distal forearm. The pain radiates to the dorsum of the thumb. Examination reveals tenderness and reproduction of symptoms with percussion 8 cm proximal to the radial styloid. Reproduction of symptoms also occurs with forearm pronation
and ulnar deviation of the wrist. No discrete sensory deficit is noted and electrodiagnostic studies are normal. Nonsurgical management consisting of rest, splinting, and anti-inflammatory medications for 6 weeks has failed to provide relief. Treatment should now consist of decompression of the
lateral antebrachial cutaneous nerve in the interval between the abductor pollicis longus and the extensor pollicis brevis in the forearm.
lateral antebrachial cutaneous nerve in the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
radial sensory nerve in the interval between the extensor carpi radialis longus and the extensor carpi radialis brevis in the distal forearm.
radial sensory nerve in the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
radial sensory nerve in the interval between the brachioradialis and the extensor carpi radialis brevis in the distal forearm.
Wartenberg's syndrome, or compression of the sensory branch of the radial nerve, occurs in the interval between the brachioradialis and the extensor carpi radialis longus approximately 8 cm proximal to the radial styloid. There may be history of repetitive wrist/forearm circumduction activity (ie, knitting) or of wearing a tight wristwatch or jewelry. It can occur in patients who have been handcuffed. Typical clinical findings are pain, paresthesia, and/or hypesthesia in the dorsoradial aspect of the wrist and hand in the distribution of the radial sensory nerve. There is often a positive Tinel's sign over the compression site. Hypesthesia may be present in the distribution of the radial sensory nerve which is typically on the dorsal aspect of the first dorsal web space and dorsum of the thumb; however, with overlap in the distribution of the superficial radial nerve and the lateral cutaneous nerve of the forearm this may not always be present. Surgical management consists of release of the nerve as it exits the interval between the brachioradialis and the extensor carpi radialis longus in the distal forearm.
A 55-year-old woman with rheumatoid arthritis reports that she awoke with an inability to flex the interphalangeal joint of her thumb. Figure 8 shows an intraoperative finding. What is the most appropriate surgical treatment?

Primary repair of the tendon
Tendon reconstruction with the palmaris longus tendon
Tendon reconstruction using a transfer of the flexor digitorum profundus (FDP) of the ring finger
Thumb metacarpophalangeal fusion
End-to-side repair of the flexor pollicis longus to the FDP of the index finger
The patient has sustained a chronic flexor pollicis longus rupture (Mannerfelt lesion). The injury is most likely a result of tendinopathy and attritional rupture of the tendon secondary to synovitis and bony osteophytosis at the scaphotrapeziotrapezoid joint. Because of the attritional injury and inherent tendinopathy, primary repair is unlikely to be successful. Among the options listed, tendon graft reconstruction with the palmaris longus tendon is the most appropriate treatment. Tendon reconstruction is possible with the flexor digitorum profundus of the index finger, not the flexor digitorum profundus of the ring finger. If osteophytes are encountered, these should be debrided.
Thumb interphalangeal fusion is an option, but metacarpophalangeal fusion is not beneficial. End-to-side repair of the flexor pollicis longus to the FDP of the index finger is not appropriate and would sacrifice needed function of the index finger.
Figures A and B show the initial radiographs of a 27-year-old snow boarder who fell backward onto his left outstretched hand. Which of the following most accurately describes the sequence of events that occurred during this injury?

Lunotriquetral ligament failure followed by distal row dissociation, scaphoid extension, scaphoid failure, and dorsal dislocation of the carpus
Volar dislocation of the lunate followed by scaphoid extension, scaphoid failure, lunotriquetral failure, and distal row dissociation
Dorsal intercarpal ligament failure followed by distal row dissociation, scaphoid failure, lunotriquetral ligament failure, and dorsal dislocation of the carpus
Short radiolunate ligament failure followed by volar dislocation of the lunate, lunotriquetral ligament failure, scaphoid failure, and distal row dissociation
Scaphoid extension followed by scaphoid failure, distal row dissociation, lunotriquetral ligament failure, and dorsal dislocation of the carpus
As described by Mayfield and associates, the typical sequence of events referred to as "progressive perilunar instability" that result in a volar
perilunate dislocation are as follows: scaphoid extension, followed by opening of the space of Poirer, scaphoid failure, and distal row dissociation, which in turn lead to hyperextension of the triquetrum, lunotriquetral ligament failure, and finally dorsal dislocation of the carpus. The lunate remains in the lunate fossa in a perilunate fracture-dislocation but is dislocated in a lunate dislocation. The short radiolunate and dorsal intercarpal ligaments typically remain intact.
Which of the following is the most consistently proposed tendon transfer for radial nerve palsy?
Pronator teres to extensor carpi radialis brevis
Brachioradialis to extensor carpi radialis brevis
Flexor carpi radialis to extensor digitorum communis
Palmaris longus to extensor pollicis longus
Flexor digitorum superficialis to abductor pollicis longus and extensor pollicis brevis
Whereas there are many variations of tendon transfers for radial nerve palsy, the most consistently proposed tendon transfer is the pronator teres to extensor carpi radialis brevis. The brachioradialis is innervated by the radial nerve so that is not an option. The flexor digitorum superficialis, flexor carpi radialis, and flexor carpi ulnaris are appropriate options to transfer to the extensor digitorum communis. The palmaris longus is not always present. A transfer to the abductor pollicis longus and extensor pollicis brevis may not be necessary if the extensor pollicis longus is rerouted to allow for abduction of the first ray.
A patient has severe cubital tunnel syndrome and marked wasting of the intrinsic muscles of the hand. Why is the little finger held in an abducted position?
Accessory slip of the extensor digiti minimi attaching to the abductor digiti minimi tendon
Tetanic contraction of the abductor digiti minimi
Radial collateral ligament insufficiency of the fifth metacarpophalangeal (MCP) joint
Unopposed pull of the flexor digitorum profundus
Muscle innervation from a Martin-Gruber anastomosis
A Wartenberg's sign, where the little finger is held in an abducted position, is associated with an ulnar nerve palsy. This happens when there is an accessory slip of the extensor digiti minimi, which is innervated by the radial nerve, crossing ulnar to the center of the MCP joint to attach to the tendon of the abductor digiti minimi and the proximal phalanx. The abductor digiti minimi and the volar interosseous muscles are both innervated by the ulnar nerve; therefore, there is no tetanic contraction of the abductor digiti minimi.
Unopposed pull of the flexor digitorum profundus results in excess flexion of the proximal interphalangeal and distal interphalangeal joints of the hand as seen with a clawing-type deformity. A Martin-Gruber anastomosis, which is a neural connection between the ulnar and median nerves in the forearm, cannot explain this finger position.
Figure 38 shows the radiograph of a 41-year-old man who reports ulnar palmar pain, decreased sensibility and tingling in the ring and little fingers, and a grating sensation in the ulnar fingers with motion. He reports that he sustained a fall on an outstretched hand 6 months ago. What is the most appropriate treatment option?

Ulnar gutter cast
Short arm cast
Carpal tunnel release
Decompression of Guyon's canal
Excision of a fractured hook of hamate
Excision of a fractured hook of hamate is the most appropriate management. The patient has a hook of hamate fracture with ulnar nerve compression and irritation of the flexor tendons by the fracture surfaces; this puts the tendons at risk for rupture. Cast treatment will most likely not gain union of the fracture and will not address the nerve or tendon problems. Decompression of Guyon's canal alone will not address the tendon issue.
A 25-year-old man was involved in an altercation. Examination reveals loss of active extension of the middle finger metacarpophalangeal (MCP) joint. A diagnosis of sagittal band rupture is made. Which of the following is considered the key diagnostic finding?
Extensor lag of 30 degrees
Extensor lag of 60 degrees
Positive Bunnell intrinsic tightness test
Ability to maintain active extension of the interphalangeal joints
Ability to maintain MCP extension after passive extension
In sagittal band rupture, the extensor tendon may subluxate into the valley between the metacarpal heads. The patient will not be able to actively extend the MCP joint from a flexed position with the subluxated tendon, but will be able to maintain MCP extension after it has been passively extended. Extensor lags can have other etiologies other than extensor digitorum communis subluxation such as tendon laceration or rupture, posterior interosseous nerve palsy, but in these conditions, patients cannot maintain MCP extension. Active interphalangeal extension can be achieved with the intrinsic muscles that are not affected by sagittal band rupture.
What is the effect of shortening of metacarpal fractures?
Causes the greatest degree of extensor lag in the index finger
Causes the greatest degree of extensor lag in the little finger
Results in an average extensor lag of 7 degrees for every 2 mm of shortening
Results in an average extensor lag of 14 degrees for every 2 mm of
shortening
Has no effect on grip strength
Cadaveric models have demonstrated a 7-degree extensor lag for every 2 mm of metacarpal shortening, with the amount of lag increasing in a linear fashion. There was no statistical difference in the amount of lag in regard to the digit involved. Based on muscle length-tension relationships, cadaveric models have also been used to demonstrate an 8% loss of power secondary to decreased interosseous force generation with 2 mm of shortening. Because the intrinsic muscles of the hand contribute anywhere from 40% to 90% of grip strength, decreased interosseous force generation secondary to metacarpal shortening will invariably cause a decrease in grip strength.
A 22-year-old motorcyclist sustains open fractures to the left radial shaft and second and third metacarpals with exposed extensor tendon and bone. The fractures are approached via the dorsal open wounds of the forearm and hand with no additional incisions made. The radiograph and clinical photograph of the remaining defect in the hand are shown in Figures 55a and 55b. The remaining wound can be most appropriately covered with which of the following?

Split-thickness skin grafting
Posterior interosseous rotational flap
Radial forearm rotational flap
Groin flap
Free lateral arm flap CORRECT ANSWER: 3
After adequate debridement, there is exposed bone, tendon, and hardware. Split-thickness skin grafting over exposed tendon will not have a viable bed to support the graft. The tendons would not have healthy surrounding tissue, resulting in poor tendon gliding. The dorsal wound has disrupted the posterior interosseous artery that runs in the septum between the extensor digiti minimi and the extensor carpi ulnaris. Following the reconstructive ladder, the radial forearm rotational flap accomplishes wound coverage with a local flap rather
than a groin flap (a distant flap) or a lateral arm flap (microvascular free tissue transfer).
What is the effect of performing a flexor tenosynovectomy with an open carpal tunnel release for idiopathic carpal tunnel syndrome?
Increased risk of nerve injury
Improved postoperative finger flexion
No added long-term clinical benefit versus open carpal tunnel release alone
Increased postoperative pain
Decreased recurrence of carpal tunnel syndrome
In patients with idiopathic carpal tunnel syndrome, flexor tenosynovectomy has not been shown to change the clinical outcome compared with open carpal tunnel release alone. This has been demonstrated in a randomized clinical trial of open carpal tunnel release with or without flexor tenosynovectomy. There has also been no evidence to suggest there is an added risk to performing the flexor tenosynovectomy. At time of surgery, the gross or histologic appearance of the flexor tenosynovium does not correlate with preoperative symptoms nor with clinical outcomes. The histology of the tenosynovium has been shown to be that of fibrosis in a setting of chronic inflammatory changes and no evidence of an acute inflammatory process exists. There may be an added role for flexor tenosynovectomy in non-idiopathic carpal tunnel syndrome such as in patients with renal disease or diabetes.
Figures 69a and 69b show the radiographs of a 62-year-old man with severe radially sided wrist pain. Management has consisted of wrist splinting, nonsteroidal anti-inflammatory drugs, and activity modification, but he continues to have pain and reports difficulty sleeping. What is the most appropriate treatment for this patient?

Arthroscopic debridement
Open reduction and internal fixation
Scaphoid nonvascularized bone graft and screw fixation
Scaphoid vascularized bone graft and screw fixation
Scaphoid excision and 4-corner fusion
Scaphoidectomy and 4-bone fusion is the most appropriate management based on the choices available. The patient has arthritic changes of SNAC (scaphoid nonunion advanced collapse) wrist, stage III. Stage I is at the radial styloid, stage II is at the radioscaphoid joint, and stage III is at the midcarpal joint. Arthroscopic debridement is not appropriate in patients with arthrosis.
Attempting to achieve scaphoid union is only appropriate if there is no arthrosis or the changes are classified as stage I where radial styloidectomy can be performed.
A 7-year-old boy is referred to your office 3 months after jamming his finger while playing basketball. Examination reveals 40 degrees of active and passive motion at the proximal interphalangeal (PIP) joint. The PIP joint is stable to radial and ulnar stressing. Radiographs are shown in Figures 76a and 76b. What is the most appropriate management?

Observation
Corrective osteotomy
Ostectomy
Hand therapy for aggressive stretching
Dynamic splinting CORRECT ANSWER: 3
The most appropriate management is an ostectomy, or resection of the bone in the subcondylar fossa region. This is a malunion where the subcondylar fossa is blocked by malaligned bone. Because it is a bony block to motion, stretching or dynamic splinting will be of no benefit. The physis of the proximal phalanx is proximal, making remodeling of a fracture at the distal end very
unlikely. A corrective osteotomy has a risk of osteonecrosis of the very small distal fragment.
Figure 78 shows the clinical photograph of a patient who injured his finger while playing football. He cannot actively flex the distal interphalangeal joint of the ring finger. Which of the following is the most accurate statement regarding the injury shown?

The tendon is attached to the avulsed fragment from the distal phalanx.
There is no difference in time sensitivity in an acute injury whether or not the tendon has retracted into the palm.
In a chronic (> 3 months) case of flexor digitorum profundus (FDP) avulsion, the FDP should be tenodesed to the flexor digitorum sublimis (FDS).
If the FDP is advanced more than 1.5 cm, there is a risk for quadriga effect.
The method of repair does not affect repair gapping or strength of the tendon repair.
Overadvancement of the FDP tendon is one of the causes of the quadriga effect. Relative shortening of an FDP tendon decreases the excursion of the neighboring FDP tendons because they originate from a common muscle belly. The patient reports a weak grasp. Answer 1 is not correct because there can be a fracture and the tendon can avulse off of the fracture fragment (Trumble JHS-A 1992). Whether the tendon has retracted into the palm or not does matter because retraction into the palm allows pulleys to collapse and contract and it also means that the vinculae have been stripped off of the tendon.
Regarding answer 3, in chronic cases where the FDS is intact and strong, many patients may be better off with a sublimis finger and no FDP reconstruction that could, in the worst case scenario, worsen a functional proximal interphalangeal joint. Regarding the repair method, there is recent
research showing method of repair (button vs anchor), suture type, and method do affect the biomechanical properties of the repair.
A 44-year-old woman with cubital tunnel syndrome and associated ulnar nerve subluxation with elbow flexion has failed to respond to nonsurgical management. Which of the following statements is most acccurate regarding in situ simple decompression of the nerve compared with subcutaneous anterior transposition?
Patients undergoing anterior transposition have improved motor outcomes.
Patients undergoing anterior transposition have improved sensory outcomes
Patients undergoing simple decompression have improved motor outcomes.
Patients undergoing simple decompression have improved sensory outcomes.
No differences in outcome are likely between treatment types.
Recent reports comparing outcomes of surgical treatment of ulnar nerve compression at the elbow have demonstrated no differences in outcome between simple decompression and anterior transposition. The presence of subluxation of the ulnar nerve was not a contraindication to in situ decompression in the study by Keiner and associates.
What anatomic structure must be excised when performing a volar plate arthroplasty of the proximal interphalangeal joint?
Central slip
Collateral ligament
Checkrein ligament
Triangular ligament
Flexor digitorum superficialis insertion
The collateral ligament must be excised or released from the proximal phalanx to allow gliding of the middle phalanx on the articular surface of the proximal phalanx. Failure to do so may prevent this gliding motion and make the middle phalanx just hinge on the proximal phalanx.
Figures 97a and 97b show a clinical photograph and radiograph of a patient who has a history of repeated drainage from the lesion. What is the preferred surgical treatment?

Excision of the lesion alone
Removal of the osteophyte alone
Distal interphalangeal joint fusion
Excision of the mass and osteophyte removal
Removal of the mass and skin with skin grafting
The patient has a mucoid cyst. Whereas many of these lesions are associated with osteoarthritis, the best surgical treatment of the lesions in patients who have little or no pain is typically excision of the mass with osteophyte removal. Studies have shown that osteophyte excision helps minimize the risk of recurrence. Distal interphalangeal joint fusion is reserved for patients with pain and more advanced radiographic arthritis. Excision of the lesion alone is a less favorable option than excision of the mass and osteophyte removal. The lesion is independent of the skin and thus, skin removal with the mass is unnecessary.
Which of the following structures cannot be seen during standard radiocarpal arthroscopy?
Scapholunate ligament
Lunotriquetral ligament
Radioscaphocapitate ligament
Extensor carpi ulnaris tendon
Superficial insertion of the triangular fibrocartilage complex (TFCC)
The extensor carpi ulnaris tendon is located in an extra-articular position, and as such, cannot be seen during arthroscopy. Wrist arthroscopy is a useful technique for evaluation and treatment of radiocarpal and midcarpal maladies. During standard radiocarpal arthroscopy, the scapholunate and lunotriquetral ligaments can be easily visualized. The superficial TFCC is seen overlying the ulnar head. Volarly, the radioscaphocapitate ligament can be seen as a discrete band of the capsule.
A 20-year-old skateboarder fell 6 months ago and has had radial-sided wrist pain since. His radiograph upon presentation to your office is shown in figure A. What is the most appropriate treatment at this time?

four corner fusion
long arm thumb spica cast
wrist arthroscopy to evaluate intercarpal ligaments
open reduction internal fixation with autologous bone graft
wrist arthrodesis CORRECT ANSWER: 4
This patient has a scaphoid waist fracture nonunion. Several studies indicate that scaphoid nonunions left untreated have a determined course of collapse and progressive arthritis (scaphoid nonunion advanced collapse - SNAC). Per Markiewitz et al, the standard treatment of scaphoid nonunions is open reduction internal fixation with bone graft; non-operative treatment is not appropriate. Proximal row carpectomy and wrist fusion are salvage procedures reserved for patient that has an advanced scaphoid nonunion, collapse and wrist arthritis.
Figures 112a and 112b show the radiographs of a 28-year-old motorcyclist who sustained a closed hand injury in a collision. What is
the most appropriate definitive treatment?

Closed reduction and a hand/forearm cast in the intrinsic plus position
Closed reduction and a hand splint
Primary fusion of the carpometacarpal joints
Closed versus open reduction and internal fixation
Closed reduction and external fixation
Closed versus open reduction and internal fixation is the most appropriate treatment. The radiographs show fracture-dislocations of all five carpometacarpal joints. These injuries are extremely unstable and not amenable to closed (splint or cast) treatment only. External fixation may be warranted in an open, contaminated injury. Fusion would be an option if this were a chronic, painful condition on presentation.
What additional procedure should be done when performing a radioscapholunate fusion for posttraumatic arthrosis following a distal radius fracture?
Excision of the triquetrum and distal pole of the scaphoid
Anterior interosseous neurectomy
Fascial interposition arthroplasty of the capitolunate joint
Sectioning of the dorsal intercarpal ligament
Ulnar shortening osteotomy
Excision of the triquetrum and distal pole of the scaphoid frees up the midcarpal joint, improving radial deviation and the flexion-extension arc of motion of the wrist. This offers an alternative to complete wrist arthrodesis for posttraumatic arthrosis of the radiocarpal joint. An anterior interosseous neurectomy is believed to decrease some pain transmission from the wrist but because the fusion is done dorsal, cutting this volar structure is not routinely done. Fascial interposition is not needed because the capitolunate should be preserved in posttraumatic radiocarpal arthrosis. Sectioning of the dorsal intercarpal ligament would provide no benefit. If the triquetrum is excised, then an ulnar shortening osteotomy is unnecessary.
Apert's syndrome is caused by a mutation in what gene?
Fibroblast growth factor receptor 2 (FGFR2)
Fibroblast growth factor receptor 3 (FGFR3)
Collagen type II alpha 1 chain (COL2A1)
SED late (SEDL)
Fibrillin
Apert's syndrome (acrocephalosyndactyly type 1) is characterized by anomalies of the cranium, hands, and feet. Mutations in the FGFR2 gene cause Apert syndrome.
Anderson et al report that in Apert's syndrome there is widespread anomalies of the feet, with defects including both predictable dysmorphic changes and progressive fusions of the skeletal components during skeletal maturity.
Incorrect Answers:
2: Achondroplasia is related to abnormalities in the FGFR3, not FGFR2.
3: SED congenita is caused by mutations in COL2A1 (type II collagen alpha 1 chain) on chromosome 12. These result in abnormal type II collagen.
4:The X-linked form of SED tarda is caused by mutation in SEDL (SED late)
gene.
5: Marfan syndrome is caused by defects in the fibrillin gene.
What is the most important measure to take to reduce the risk of frostbite of the toes while hiking in extreme temperatures?
Stop often for recovery breaks.
Drink enough warm liquids.
Reduce thermal heat loss from shoes.
Use triple socks.
Adequately "carbo load" before the start.
Several studies showed the most reliable method to reduce the risk of cold exposure injury is to reduce thermal heat loss. This can be done with a combination of protective socks and shoes, and reducing moisture in the shoes.
Figures 45a through 45e are the MRI scans, gross specimen, and histology of the specimen of a 19-year-old man who has an enlarging mass in the second interspace. He reports forefoot pain that is worse with athletic activity. Radiographs show erosive changes of the third metatarsal head. What is the most common complication associated with incomplete excision?
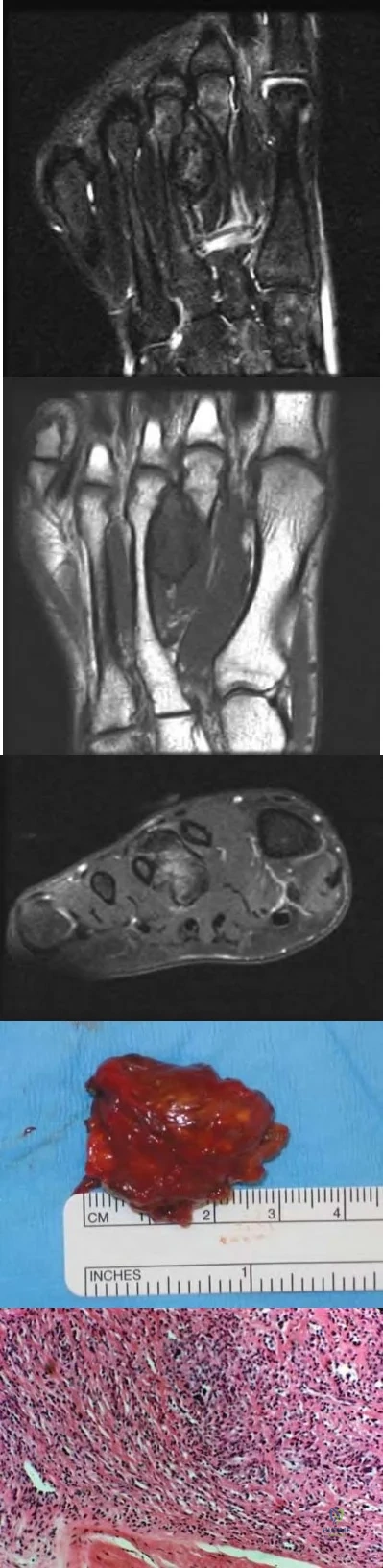
Metastatic disease
Malignant degeneration
Recurrence
Pathologic fracture
Infection
Giant cell tumor of the tendon sheath often arises from the synovial lining of tendon sheaths. This lesion is frequently found in the hand and foot. The lesion is slow growing and can invade adjacent structures. In the foot, wearing shoes or increased activity can cause pain. Incomplete or piecemeal excision can lead to recurrence.
A 42-year-old construction worker presents with pain in his right wrist. A current radiograph of the wrist is shown in Figure A. He reports that rotating activities, such as turning a screw driver, are bothersome and the pain is preventing him from working. A current MRI reveals a TFCC tear, and nonsurgical treatment has failed to provide relief. Treatment should now consist of:

Repair of the ulnar styloid nonunion
Darrach resection of the distal ulna
Complete ulnar head resection
Ulnar hemiresection arthroplasty and TFCC reconstruction/repair
Isolated arthroscopic TFCC reconstruction
The clinical presentation is consistent with DRUJ arthritis in a heavy laborer. Of the options listed, ulnar hemiresection arthroplasty with concurrent TFCC reconstruction or repair would be the most appropriate treatment.
While there are multiple treatment options, the ulnar hemiresection arthroplasty with concurrent TFCC reconstruction or repair is considered most appropriate in heavy laborers, as it would likely resolve the pain and enable them to return to work sooner. The TFCC should be intact when performing an ulnar hemiresection arthroplasty to prevent distal ulna instability with forearm rotation. One could also consider performing a Suave-Kapandji procedure. This procedure creates a distal radioulnar fusion and an ulnar pseudarthrosis proximal to the fusion site through which rotation can occur. The advantage is that the ulnocarpal joint is not sacrificed, and a stable wrist is created.
Scheker et al reported on the outcome of ulnar shortening performed on 32 wrists with early osteoarthritis of the DRUJ. The postoperative wrist ratings were 7/32 excellent, 11/32 good, 9/32 fair, 5/32 poor, with plate irritation being the most frequent postoperative complication.
Figure A is a radiograph showing significant DRUJ arthritis. Illustration A shows ulnar hemiresection arthroplasty. Illustration B shows a Darrach procedure.
Illustration C shows a Sauve-Kapandji procedure. Illustration D is a treatment schematic of TFCC reconstruction.
Incorrect Answers:

Figures 113a and 113b are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step?

Child abuse workup
Closed reduction
Open reduction with possible osteotomy
Observation CORRECT ANSWER: 4
The most appropriate management of this condition is observation. The patient most likely has a congenital dislocation of the radial head, although this may also represent a posttraumatic deformity. The absence of findings on physical examination speaks against an acute injury. The appearance of the radial head reveals the typical findings of a congenital dislocation, namely the convex appearance of the proximal radial articular surface. These children typically have very functional range of motion and do not require treatment unless they are symptomatic. There is nothing in this child's history to suggest abuse.
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves
wrist extension and forearm pronation.
wrist extension and forearm supination.
wrist flexion and forearm pronation.
wrist flexion and forearm supination.
axial load in ulnar deviation.
TFCC tears are common in athletes. As the athlete braces for a fall, the wrist is most commonly in an extended position and the forearm is pronated.
A 28-year-old woman fell on her right wrist while rollerblading 6 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Arthroscopy of the wrist
CT of the wrist
Bilateral PA clenched fist radiograph
Electromyography and nerve conduction velocity studies
AP and lateral radiographs of the forearm
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool.
Figures 12a through 12c show the radiographs of a 28-year-old professional baseball player who has ulnar-sided wrist pain and
numbness and tingling in the fourth and fifth digits for the past 6 weeks. Management should consist of

cast immobilization.
bone stimulation and splinting.
ulnar nerve exploration.
open reduction and internal fixation.
excision of the fragment.
Hook of the hamate fractures typically occur as a result of direct force from swinging a bat, golf club, or racket. Pain is localized to the hypothenar eminence. The injury is best seen on a carpal tunnel view. CT will confirm the diagnosis. Chronic cases can be associated with neuropathy of the ulnar nerve. Excision of the hook through the fracture site usually yields satisfactory results, allowing the athlete to return to competition.
A 40-year-old right-handed professional football player reports persistent right wrist pain after falling during a game 5 days ago. A radiograph is shown in Figure 21. Management should consist of

immobilization in a short arm thumb spica cast.
immobilization in a long arm thumb spica cast.
arthroscopic repair and percutaneous pinning.
open repair and percutaneous pinning.
dorsal capsulodesis.
The radiograph reveals an increased distance between the scaphoid and the lunate, which is indicative of scapholunate disassociation. A ring sign is also present, which represents the distal pole of the scaphoid viewed end on in a palmarly flexed position. In the acute setting, the scapholunate can be repaired. Open repair and percutaneous pinning is the treatment of choice. Dorsal capsulodesis is performed in the chronic setting if such an injury is initially missed.
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Acute tendon repair
DIP joint extension splinting for 6 weeks
DIP and proximal interphalangeal joint extension splinting for 6 weeks
Buddy taping to the middle finger for 2 weeks
Early range-of-motion exercises and return to play as pain permits
Flexor digitorum profundus rupture or “rugger jersey finger” often occurs in the ring finger after the player misses a tackle and catches the digit on the shirt of the opposing player. Surgical repair is required for zone I-type injuries.
A 65-year-old right-hand-dominant man has a 5 year history of progressive right wrist pain. He relates spraining his wrist playing football in college, but otherwise has had no prior traumatic injury. He is a pack per day smoker. An AP radiograph of the wrist is shown in Figure A. Wrist immobilization, anti-inflammatory medications, and injections have failed to provide relief. Which appropriate surgical treatment option offers the lowest risk of postoperative complications?

Radial styloidectomy
Total wrist arthroplasty
Proximal row carpectomy
Scaphoid excision with four-corner fusion
Complete radiocarpal arthrodesis
Proximal row carpectomy (PRC) and scaphoid excision with four-corner fusion are both appropriate surgical treatment options for stage II scapholunate advanced collapse (SLAC) wrist; however PRC is associated with fewer postoperative complications, particularly in active smokers.
Scapholunate interosseous ligament disruption leads to abnormal wrist biomechanics and degenerative arthritis. This progression follows a predictable pattern termed scapholunate advanced collapse. In stage II disease where the entire radioscaphoid articulation is affected but the capitolunate articulation is spared, both proximal row carpectomy (PRC) and scaphoid excision with four-corner fusion offer long-term pain relief while preserving wrist motion and grip strength. Scaphoid excision with four-corner fusion has a higher rate of complications owing to nonunion, hardware issues, and dorsal impingement from malunion. PRC is not recommended in the setting of capitolunate arthritis (stage III).
Tomaino, et al. retrospectively compared PRC and limited intercarpal arthrodesis with scaphoid excision (LWF) at a mean of 5.5 years postoperatively in 24 symptomatic SLAC wrists. They noted good pain relief, grip strength, and function in all but 3 patients having undergone PRC - one of whom required revision to wrist arthrodesis (these patients had symptomatic capitate arthrosis). They concluded that in wrists without capitolunate arthritis, PRC had the benefit of being technically easier to perform, did not require prolonged postoperative immobilization, and avoided the risk of nonunion associated with LWF; however it was not an appropriate surgical option in stage III SLAC wrists with capitolunate involvement.
Strauch reviewed the evaluation and treatment of SLAC and SNAC (scaphoid nonunion advanced collapse) wrists. Treatment options for SLAC wrist include four-corner fusion, capitolunate arthrodesis, PRC, radial styloidectomy, wrist denervation, and complete radiocarpal fusion. Excision of the distal ununited scaphoid fragment is an additional option in the setting of SNAC wrist. He additionally highlights current controversies between PRC vs. four-corner fusion.
Figure A shows an AP radiograph with stage II SLAC wrist. The entire radioscaphoid articulation is arthritic with sparing of the capitolunate surface.
Illustration A shows the modified Watson classification of scapholunate advanced collapse.
Incorrect Answers:

A 25-year-old male presents to the clinic with a painful, enlarging mass at the volar radial wrist. He initially noticed the mass 6 months ago after he hurt his wrist golfing. Figure A shows a clinical photograph of the patient's wrist. Radiographs are unremarkable. An ultrasound of the mass is shown in Figure B. Surgical excision is planned. Which of the following is the most appropriate type of resection and histologic finding?
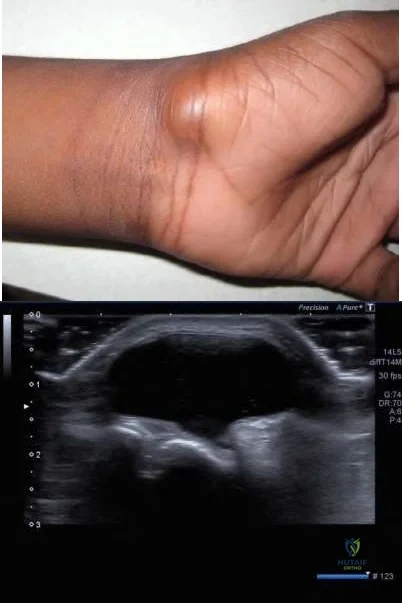
Intralesional excision; synovial cells with mucin accumulation
Incision & drainage; polymorphonuclear cells
Wide excision; histiocytes with frequent giant cells
Marginal excision; synovial cells with mucin accumulation
Intralesional excision; histiocytes with frequent giant cells
The patient presents with a volar wrist ganglion cyst. Surgical treatment consists of marginal excision. Histologic analysis demonstrates synovial cells with mucin accumulation.
Ganglion cysts are the most commonly presenting masses in the hand. These cysts consist of a synovial cell lining filled with mucin. Dorsal wrist ganglion cysts originate from the scapholunate interval and are more common than volar wrist ganglions, which typically originate from the scapho-trapezio-
trapezoidal joint articulation. Ganglion cysts can cause pain related to mass effect. Ultrasound can help differentiate these masses from vascular malformations or other tumors; ganglion cysts present as homogenous anechoic masses with well-defined borders.
Mayerson, et al. reviewed the diagnosis and management of soft-tissue masses. They highlight the typical presentation of ganglion cysts, which wax and wane in size and transilluminate with a pen light. The authors concluded that MRI is diagnostic if there remains any uncertainly after history and clinical exam.
Head et al compared surgical excision versus needle aspiration of 2,239 adult wrist ganglions in a meta-analysis of 35 studies. Surgical excision resulted in a 76% reduction in recurrence compared to aspiration. Mean recurrence for arthroscopic excision (6%), open surgical excision (21%) and aspiration (59%) and mean complication rate for arthroscopic excision (4%) open surgical excision (14%) and aspiration (3%) were also determined. Data from arthroscopic excision was limited but is a promising technique. Open surgical excision has a significantly lower recurrence rate as compared to aspiration.
Figure A shows a clinical photo of a volar wrist ganglion cyst. Figure B shows the ultrasound image of a volar wrist ganglion cyst.
Incorrect Answers:
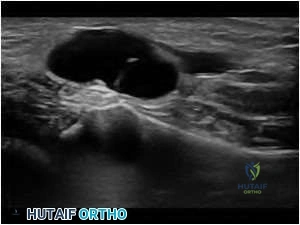
A 27-year-old man falls on his hand at work. He notices an immediate deformity of his ring finger. Radiographs are provided in Figure A. Which of the following is the most appropriate initial treatment?

Closed reduction, buddy taping, and early motion to prevent stiffness
Closed reduction and full time extension splinting
Open reduction and repair of the central slip of the extensor tendon
Open reduction and repair of the volar plate
Amputation and immediate return to work
The radiograph demonstrates a volar PIP dislocation. The central slip of the extensor tendon is frequently ruptured and will lead to a boutonneire deformity if left untreated. The PIP must be immobilized in extension to allow the extensor mechanism to heal. Immobilization in extension should be maintained for 6 weeks to allow soft tissue healing. Open reduction and repair of the central slip would be the appropriate treatment for a developing boutonneire deformity that presents in a subacute or chronic time basis.
Illustrations A and B demonstrate a schematic and clinical photo of central slip disruption and secondary deformity with PIP flexion and DIP hyperextension (Boutonniere Deformity).
Posner et al reviewed 7 patients with chronic palmar dislocations of the PIP joint who were treated with open reduction and reconstruction of the extensor mechanism. All patients acheived satisfactory range of motion and the authors concluded that this technique is preferable to arthrodesis.
Peimer et al reviewed 15 patients with palmar dislocations of the PIP joint. Twelve of the fifteen were evaluated on a delayed basis (average 11 weeks following injury) and underwent open reduction and surgical repair of the extensor tendon. Three of the fifteen were seen earlier following injury and were treated with closed reduction and pinning. All fifteen patients acheived satisfactory clinical outcomes although finger range of motion was not fully recovered in any case.
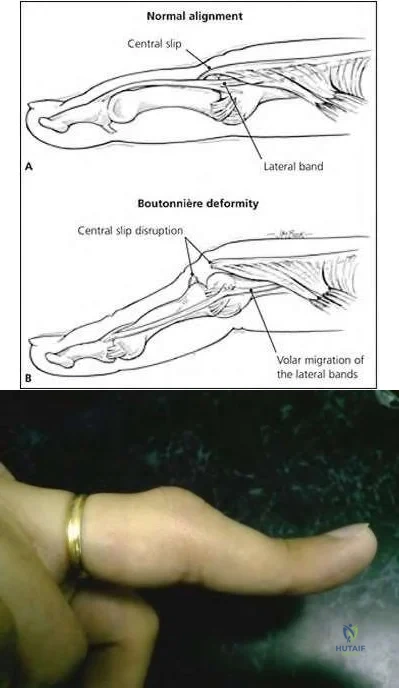
Figure A is of a 22-year-old male college basketball player presents for evaluation of a right index finger deformity. He reports a fall during a game 8 weeks ago, with resultant deformity to the index finger. He "popped it back in" and returned to play. Physical exam is most likely to demonstrate:

Inability to passively extend the PIP joint to neutral, able to passively flex and extend the DIP joint
With the PIPJ flexed, resistance to PIPJ extension causes the DIPJ to become supple
Dorsal subluxation of the PIP joint, able to passively flex and extend DIP joint
With the PIPJ flexed, resistance to PIPJ extension causes the DIPJ to become rigid
Inability to actively flex the DIP joint, able to actively flex the PIP and the MCP joints
The patient presents with a Boutonniere deformity secondary to a traumatic central slip disruption in the setting of volar PIP joint dislocation. Physical exam will demonstrate a positive Elson's test, which is described in answer 4.
The digital extensor mechanism consists of the central slip and two lateral bands, all of which arise from the extensor digitorum communis (EDC) tendon. Flexion of the PIP joint puts the central slip on tension, and volarly subluxes the lateral bands causing them to become slack. Tension on the central slip causes extension of the PIP joint, with concomitant dorsal shift of the lateral bands which help to bring the DIP joint into extension.
In 1986, Elson described his physical examination maneuver for diagnosis closed rupture of the central slip. With the hand resting on the edge of a table, the PIP joint is flexed to 90 degrees over the table edge, and the patient is asked to extend the digit against resistance. Active extension of the middle phalanx can only be observed with an intact central slip, and the adjacent lateral bands will remain slack which allows the DIP joint to remain flail. In central slip ruptures, effort to extend the middle phalanx will be accompanied
by DIP rigidity/extension as the lateral bands are forced to contribute to extension.
Rubin et. al. performed a cadaveric study evaluating the efficacy of physical examination maneuvers to identify acute ruptures of the central slip. They
found that Elson’s test was the only maneuver that could discern central slip integrity in both tested scenarios: 1) pre-boutonniere deformity with division of the central slip and 2) passively correctible boutonniere deformity caused by division of the central slip, the triangular ligament, and the oblique fibers of the extensor expansion.
Figure A is a clinical image of an index finger with boutonniere deformity. Video A is a short demonstration of how to perform the Elson test.
Incorrect answers:
A 25-year-old woman presents to the clinic after knife injury to the volar aspect of her long finger 2 weeks ago. She is evaluated and diagnosed with tendon rupture of the flexor digitorum profundus (FDP). What finding on examination can be expected in this patient?
With passive wrist extension, extension remains at the distal interphalangeal joint
With passive wrist extension, extension remains at the proximal interphalangeal joint
With passive wrist flexion, extension is limited at the distal interphalangeal joint
With passive wrist flexion, flexion remains at the distal interphalangeal joint
With passive wrist flexion, flexion remains at the proximal interphalangeal joint
With an FDP rupture, physical exam would likely reveal loss of flexion at the DIP joint both actively and passively with wrist extension.
When the wrist is in extension, flexor tendons are stretched and should result in flexion at the DIP (FDP) and PIP (FDS) joints. The FDP tendon is responsible for flexion of the DIP joint, and this joint would remain extended during normal tenodesis on passive wrist exam. Inversely, with extensor tendon injuries, there may be a loss of digit extension with passive wrist flexion.
Strickland presents a review article (Part 1) on flexor tendon injuries discussing clinical presentation and repair techniques. A commonly tested concept is that tendon repair is proportional to the number of core sutures, and currently recommended repair includes at least 4 core sutures for strength with epitendinous suture to aid in gliding and provide some strength.
Kamal et al. present current evidence regarding flexor tendon injuries, reviewing examination, repair, and rehab. They note that to date there still remains heterogeneity in treatment patterns and no clear standard of care. Rehab options include no motion, early active range of motion, and controlled passive range of motion. The authors note that early loading may lead to improved strength.
Illustration A depicts the usual tenodesis effect of the digits where passive extension of the wrist produces flexion of the fingers.
Incorrect Answers:

A 20-year-old college football lineman sustains an injury to his index finger during a game. A radiograph of the hand is demonstrated in Figure A. What is the mechanism of injury and most common reason for unsuccessful closed reduction?

Hyperextension mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Hyperextension mechanism causes volar plate avulsion and entrapment dorsal to the metacarpal head
Rotational mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Hyperflexion mechanism causes volar plate avulsion and entrapment dorsal to the metacarpal head
Hyperflexion mechanism causes the metacarpal head to button hole between the flexor tendon and the lumbrical
Irreducible dorsal metacarpophalangeal (MP) joint dislocations occur from a hyperextension moment, which causes volar plate displacement and incarceration dorsal to the metacarpal head.
MP joint dislocations are most commonly dorsal and occur with hyperextension injuries. Simple dislocations are reducible with wrist flexion (to relax the intrinsic muscles) and direct palpation over the proximal phalanx base.
Complex dislocations occur with interposition of the volar plate. When irreducible, open reduction is required.
Afifi et al. performed a cadaver study defining the anatomy surrounding irreducible dorsal index MP joint dislocations. They found that of all local structures, only release of the volar plate allowed for reduction of the MP joint. They concluded that volar plate interposition dorsal to the metacarpal head was responsible for irreducible MP joint dislocations.
Bohart et al. describe 9 patients with irreducible dorsal MP joint dislocations (5 thumbs and 4 index fingers). A dorsal approach was performed in each case to allow for reduction of the volar plate. A stable MP joint was achieved in each case. They advocate for a dorsal approach, which minimizes the risk of iatrogenic injury to the neurovascular bundles, which are displaced volarly by the metacarpal head.
Figure A shows an oblique radiograph of the hand demonstrating a dorsal dislocation of the index MP joint. Illustration A provides a schematic of both a simple and a complex dorsal MP joint dislocation. In the case of a complex dislocation, the volar plate avulses from its origin and becomes entrapped dorsal to the metacarpal head.
Incorrect Responses:
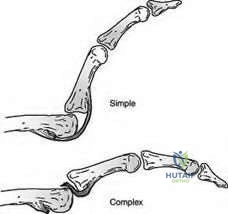
A 3-year-old patient presents to clinic with her parents for the chest wall anomaly seen in Figure A. What other congenital disorder is associated with this syndrome?

Flexible pes planovalgus
Syndactyly
Polydactyly
Macrodactyly
Accessory navicular CORRECT ANSWER: 2
The figure shows an individual with Poland's Syndrome, as demonstrated by the absent sternoclavicular head of the pectorals major. Syndactyly and symbrachydactyly is often seen, in addition to hypoplasia and shortening of the fingers.
Poland's Syndrome, or Poland anomaly/sequence, is thought to be caused by disruption of the subclavian artery in utero, causing various hypoplastic anomalies of the upper extremity. These are typically ipsilateral ranging from aplasia of the sternocostal head of the pectorals major, radio-ulnar synostosis, symbrachydactyly and other limb hypoplasias, or syndactyly of the central digits. Syndactyly is often simple and either complete or incomplete. It is addressed surgically early on, with the chest wall deformities needing reconstruction and muscle transfers closer to sexual maturity. Thoracic, cardiovascular, and genitourinary anomalies may also be present.
Catena et al. proposed a new classification system for Poland Syndrome based on the degree of clinical severity of the entire upper extremity. The classification type increased with more proximal involvement up the upper extremity. This new system may help guide treatment as is takes into account the functional state of the rest of the upper extremity and not just the hand, as previous systems have.
Ireland et al. analyzed 43 consecutive cases of Poland's Syndrome. All cases involved congenital aplasia and syndactyly which was typically simple and incomplete. The thumb can be involved putting it the same plane as the fingers. Anomalies were more frequently seen on the right side. They noted favorable outcomes with surgical correction by syndactyly release initiated by 1 year, with some requiring periodic revision releases, while others required an amputation producing a three-fingered hand.
Figure A shows an absent stenocostal head of the pec major. Only the right side is involved. Illustrations A-C show pre-op and post-op digital release of an individual with syndactyly
Incorrect Answers:
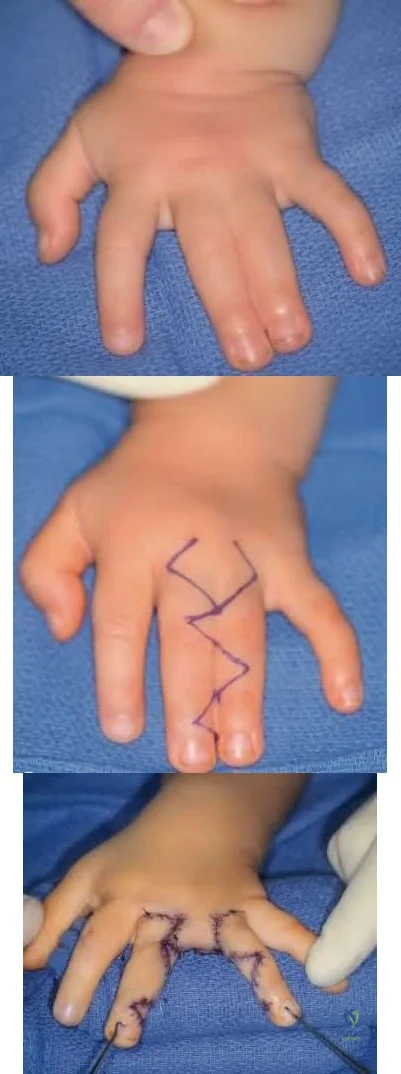
A 32-year-old man sustains an injury to his left thumb. Examination in the ER demonstrates a 2x4 cm wound on the dorsal thumb overlying the proximal phalanx with exposed tendon and bone. What is the most appropriate option for soft tissue coverage?
Cross-finger flap
Moberg advancement flap
Full-thickness skin graft
First dorsal metacarpal artery flap
V-Y advancement CORRECT ANSWER: 4
The first dorsal metacarpal artery flap (Kite flap) is the most appropriate soft tissue coverage option for dorsal thumb wounds that disrupt vascularized tissue overlying the extensor tendon and bone (including the epidermis, dermis, subcutaneous tissue, and tenosynovium) when primary closure is not possible.
Kite flaps are based off of the first dorsal metacarpal artery, which overlies the index finger metacarpal. It offers a pedicle length up to 7 cm and can reliably cover soft tissue defects up to 3x5 cm in area. Given its location, it is appropriate for the treatment of thumb wounds including those to the web space, dorsum, and volar pulp, particularly when injury compromised the vascularity of the wound bed. It can be modified to include both dorsal branches of the proper digital nerve, thereby conferring sensibility to the covered wound. The donor site can subsequently be covered with a full-thickness skin graft.
Rehim et al. reviewed local flaps of the hand. They offer treatment options and appropriate indications based upon the anatomic location and size of the wound within the hand. They conclude that when there are no clinical limitations, local flaps provide ideal soft tissue coverage and function for hand wounds based upon the local anatomy without the need for more complex free tissue transfers.
Eberlin et al. review soft tissue coverage options in the hand. They present four clinical cases and offer one established and one non-traditional surgical treatment option for each. They recommend the first dorsal metacarpal artery flap as an established treatment option in a case of thumb volar pulp injury as it offers contour restoration as well as sensibility when the digital nerves are included with the vascular pedicle.
Illustration A demonstrates a large dorsal thumb soft-tissue injury that is treated with first dorsal metacarpal artery flap coverage and full-thickness skin grafting to cover the donor site.
Incorrect Answers:

A 65-year-old man complains of numbness and tingling in the thumb, index, and long fingers of his dominant right hand for 3 months. An EMG demonstrates prolonged median sensory latency and low amplitude compound muscle action potentials with fibrillations in the abductor pollicis brevis. What is the most appropriate treatment option and the rate of continued symptoms at 1 year after treatment?
Splinting and corticosteroids; 5%
Open carpal tunnel release; 20%
Splinting and corticosteroids; 30%
Endoscopic carpal tunnel release; 2%
Open carpal tunnel release; 5%
The most appropriate treatment of carpal tunnel syndrome (CTS) with EMG evidence of denervation is surgical release. The rate of residual symptoms at 1 year is approximately 20%.
The American Association of Electrodiagnostic Medicine (AAEM) criteria delineates CTS severity by EMG. Mild CTS is purely sensory. Moderate disease demonstrates prolonged sensory and motor latencies. Severe disease progresses to involve muscle denervation. Mild and moderate CTS may be treated with carpal tunnel release following failure of nonoperative treatment; however, early operative treatment is supported for severe disease to limit further denervation. Patients experience significant improvement in
symptoms; however, recovery is prolonged and persistent symptoms may be present in ~20% at 1 year.
Kronlage et al. compared changes in numbness and pain following carpal tunnel release in 47 patients with moderate and 48 patients with severe CTS diagnosed on EMG. At 1 year or longer, 1 (2%) patient with moderate disease had continued symptoms compared to 9 (19%) of patients with severe CTS. They concluded that patients with severe CTS experience significant reductions in symptoms following carpal tunnel release; however, recovery may be prolonged or incomplete at 1 year postop.
Ono et al. performed a systematic review of 25 studies reporting outcomes for the treatment of carpal tunnel syndrome. They noted an increasing trend towards recommending earlier surgery for CTS with or without median nerve denervation. They conclude that this differed from the 2007 AAOS guidelines, which recommended early surgery only in the setting of muscle denervation.
Incorrect Answers:
A 23-year-old man presents with chronic, progressive right wrist pain. He remembers falling onto an outstretched hand 2 years ago. Radiographs, CT scans and a T1-weighted coronal MRI are shown in Figures A through E. No bleeding was identified at surgery. In addition to surgical stabilization, what is the next best step?

Corticocancellous autograft inserted through a dorsal approach
Pedicled distal radius graft inserted through a dorsal approach
Pedicled distal radius graft inserted through a volar approach
Free vascularized femoral bone graft inserted through a dorsal approach
Free vascularized femoral bone graft inserted through a volar approach
This patient has an old scaphoid waist fracture with nonunion, proximal pole avascular necrosis (AVN), and carpal collapse. Optimal treatment is with a free vascularized medial femoral condyle (MFC) graft through a volar approach.
Where there is proximal pole AVN, union was achieved in 88% of patients with a vascularized graft versus 47% with screw and nonvascularized wedge bone graft fixation. The 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) pedicle graft leads to union rates of 71% for scaphoid nonunions and 50% for AVN. The risk for failure is higher when there is DISI or humpback deformity (underscoring the need to restore scaphoid geometry). The MFC graft uses a pedicle from the descending genicular artery or the superomedial genicular artery when the descending genicular artery is not present. The volar approach is preferred as it allows correction of the humpback deformity and anastomosis of the MFC pedicle to the radial artery.
Jones et al. retrospectively compared 2 vascularized bone grafts for treatment of scaphoid waist nonunions with proximal pole AVN and carpal collapse. 4 of
10 nonunions treated with distal radial pedicle graft healed at 19 weeks. 12 of 12 nonunions treated with free vascularized medial femoral condyle (MFC) graft healed at median of 13 weeks. Rate of union was higher, and time to healing was shorter for the MFC graft. They recommend the MFC vascularized bone graft for treatment of scaphoid waist nonunion with proximal pole AVN and carpal collapse.
Figures A, B, C and D are PA and lateral radiographs and coronal and sagittal CT images showing scaphoid waist nonunion with carpal collapse and osteonecrosis of the proximal pole, respectively. Figure E is a T1-weighted coronal image shows diffusely decreased signal within the proximal pole.
Illustrations A and B show harvest and inlay of the 1,2 ICSRA graft. Illustration C shows the MFC graft.
Incorrect Answers:
A 38-year-old female develops pain and pallor in all the digits of the right hand daily. Her symptoms have progressed over 2 years despite avoiding direct cold exposure and multiple medications including nifedipine. Recently she has developed the lesions seen Figure A. Workup for underlying disease by her rheumatologist was negative. She is a candidate for Botuninum toxin A injections. What is the physiologic effect of botulinum toxin in the hand for her condition?

Improving proprioception in the fingers and hand by binding to postsynaptic acetylcholine receptors
Improving digital perfusion by cleaving pre-synaptic SNAREs and preventing the release of acetylcholine
Decreasing glabrous skin sensation by reducing hyperexcitability of voltage dependent calcium channels
Strengthening the intrinsic muscles by increasing hyperexcitability of voltage dependent calcium channels
Increasing sympathetic innervation by cleaving pre-synaptic SNAREs and preventing the release of acetylcholine
The patient is displaying Raynaud's Disease with the development of ulcerations from chronic vasoconstriction. Botulinum toxin has been shown to increase the blood supply throughout the hand through the its well-known mechanism of pre-synaptic SNARE cleavage.
Botulinum toxin cleaves the pre-synaptic SNAREs (soluble NSF attachment potion receptor) and prevents the release of acetylcholine from the intracellular vesicles. This has been used for multiple medical purposes, including vasospastic disorders. Raynaud's Disease is characterized by idiopathic vasospasm of the digital arteries without known underlying cause. Usually afflicting pre-menopausal women, it begins with pain and pallor in the digits, typically affecting the bilateral hands. Avoiding cold environments and tobacco are the mainstays of treatment, with calcium-channel blockers being the most common medication used. When these and other medications fail, botulinum toxin injections have been shown to be of benefit by relieving vasoconstriction and decreasing ischemia and pain.
Neumeister et al. reviewed the application of botulinum toxin A and individuals with Raynaud's Disease and Syndrome. They showed marked increases (up to 300%) in digital perfusion in patients receiving these injections into the common digital vessel at the level of the palm. They concluded the mechanisms for this response are likely multifactorial, involving central and systemic effects on neurotransmitters involved in chronic pain pathways, local digital vessel tone, and sympathetic innervation.
Iodio et al. reviewed all clinical studies regarding the use of bootulinum toxin A in raynaud's. There was high variability among the studies in terms of dosage and application method, but all studies reported favorable patient outcomes and some showed improved healing of ulcerations. These studies are promising but are limited due to study design and lack of standardization of botulinum toxin application.
Figure A shows non-infected ulcerations in the digits, common in progressive raynaud's disease.
Illustration A shows ischemic digits due to Raynaud's Syndrome. Illustration B is the same hand after botulinum toxin A injection. Illustration C is a laser doppler of a hand both pre- and post-injection perfusion of botulinum toxin A in an individual with Raynaud's Disease. Illustration D depicts the recommended method of injection, placing 10 units of botulinum around the common digital vessel at the level of the palm.
Incorrect Answers: There is no shown effect on digital proprioception, skin sensation, muscle strengthening.
A 27-year-old male injures his thumb during a fall onto an outstretched hand. He has pain at the MCP joint and difficulty grasping objects between the thumb and index finger. He undergoes surgery with the planned incision shown in Figure A. What muscle and corresponding nerve innervates the structure that blocks reduction of the ligament shown in Figure B?
Opponens pollicis, median nerve
Flexor pollicis brevis, ulnar nerve
Adductor pollicis, ulnar nerve
Abductor pollicis brevis, median nerve
Adductor pollicis, median nerve
The patient has an ulnar collateral ligament injury. The structure that blocks reduction of the ligament is the adductor pollicis aponeurosis, which is innervated by the ulnar nerve.
Thumb ulnar collateral ligament injuries occur after a radially directed force on an extended thumb, stressing the ulnar collateral ligament, dorsal capsule and volar plate. The thumb should be radiographed before stress exam if the history warrants so as not to displace a possible bony avulsion. Exam includes valgus stress on the thumb at 0 and 30 degrees of flexion to test the accessory and proper collateral ligaments respectively. With complete rupture of both ligaments, a bump over the ulnar thumb MCP joint may be palpated, signifying a Stener lesion. The ligament usually tears at the distal insertion and displaces proximal and superficial to the adductor aponeurosis. The dorsal capsule and volar plate may also be injured.
Bean et al. evaluated the biomechanics of non-anatomic reconstruction of the ulnar collateral ligaments in cadaveric specimens. They showed that 2mm of volar displacement of the ligament origin will allow for 10 degrees more radial deviation than anatomic placement will. This highlights the need for anatomic reconstruction and that deviation from this will alter joint kinematics.
Figure A shows a planned incision over the ulnar aspect of the thumb MCP joint
Fibure B shows a Stener lesion that is migrated proximally compared to the aponeurosis which is marked by the forceps
Illustration A depicts the retraction of the collateral ligament proximal to the aponeurosis
Illustration B shows a T1 MR coronal image showing a distal avulsion of the UCL and the Stener lesion, denoted by the asterisk, and the arrow pointing to the aponeurosis
Incorrect Answers:

An otherwise healthy 5-year-old female is brought to your office for the deformity shown in Figures A and B. Only the small digit of the left hand is involved and it may be fully flexed, but there is limited passive extension. What is the next best step in treatment?
Observation and reassurance
Nighttime extension splinting and stretching regimen
Nighttime extension splinting and stretching regimen with full genetic workup
FDS transfer to radial lateral band
FDS split with transfer of limbs to A2 pulley and central tendon hood
The patient described has isolated camptodactyly with a mild flexion contracture. The best next step in treatment is to begin a stretching and splinting regimen.
Camptodactyly is a nontraumatic flexion deformity isolated to the proximal interphalangeal joint, typically involving the small finger. This is often seen
bilaterally and sporadically, although many congenital disorders are associated. Many underlying anatomical structures have been implicated in the pathogenesis of this condition, with various surgical techniques having been described to address these. If this condition remains untreated, adjacent joint involvement can develop, with MCP hyperextension seen most commonly.
Intrinsic-plus splinting of the hand with passive stretching exercises should be initiated first. Surgery is usually reserved in cases of failed splinting or significant contractures approaching 60 degrees.
Comer et al. reviewed the complications of campylodactly. Most common complications were progression or failed improvement of both PIP contracture and MP hyperextension, isolated PIP postoperative residual stiffness, and bony remodeling of proximal phalanx head preventing full extension. They note inconsistent results after surgical correction which supports early detection and conservative modalities as the mainstay of treatment, focusing heavily on a stretching program and night splinting.
Rhee et al. reviewed outcomes of passive stretching for isolated camptodactyly flexion contractures in a series of children under the age of three years. They showed marked improvement of contracture deformity in all children across all levels of severity, though to less extent with more severe deformities.
Figures A and B demonstrate early contracture of the left small finger. Illustration A is a radiograph showing maintenance of articular congruity.
Incorrect Answers:

A collegiate rower complains of dorsal wrist pain for 6 weeks refractory to NSAIDs and bracing. Maximal tenderness is palpated on the dorsoradial forearm approximately 5 cm proximal to the wrist. Pain is exacerbated with resisted wrist extension. Radiographs are unremarkable. A steroid injection should be directed into the compartment containing which of the following structures?
APL and EPB tendons
ECRL and ECRB tendons
EPL tendon
APL and ECRB tendons
Brachoradialis tendon CORRECT ANSWER: 2
The clinical scenario is consistent with intersection syndrome, a inflammatory response to overuse at the site of the second dorsal compartment crossing under the first dorsal compartment approximately 5 cm proximal to the wrist. An anatomical depiction is provided in illustration A. Injections of the second dorsal compartment, which includes ECRL and ECRB, may relieve symptoms
and quell inflammation. Intersection must be differentiated from DeQuervain's syndrome, which is tenosynovitis of the first dorsal compartment. Injections of the first dorsal compartment, which includes APL and EPB, are part of the treatment algorithm for Dequervain's. Wood et al summarizes the evaluation and treatment of sports-related wrist injuries. Grundberg et al demonstrates the pathologic abnormality of intersection syndrome is stenosing tenosynovitis of the second compartment explaining the rationale behind steroid injections into the sheath.
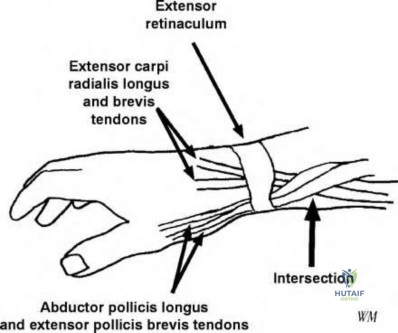
A 42-year-old chef has finally been transferred to the hand specialist 15 hours after injuring his non-dominant hand index finger with a butcher's knife as seen in figure A. He has kept the finger with him, which has been wrapped in saline-soaked gauze and placed on ice. What is the best reason the finger tip should not be replanted?

The replanted digit will likely have poor function due to the delay in care
Possible malingering
The replanted digit will likely have poor function due to the local anatomy
Patient age
Workers compensation patients will have worse outcomes
Single digit amputations proximal to the insertion of the flexor digitorum superficialis (FDS), in generally have poor function and severe stiffness following replantation.
Replantation between the FDS insertion and the distal palmar crease (zone 2 flexor tendon injuries) has historically led to poor results due to stiffness at the proximal interphalangeal joint, decreased sensation in the finger, and tendon adhesions between the FDP and slips of the FDS. Furthermore, outcome studies have demonstrated patients with index finger amputations through this region are more likely to bypass their stiff index finger and utilize their long finger for most tasks. However, amputation of multiple digits through zone 2 would be considered for replantation.
Urbaniak et al performed a retrospective case series of 59 patients who
underwent finger (thumb excluded) replantation for traumatic amputation. They found the functional results were most dependent on level of amputation and patients with amputation proximal to the insertion of the FDS had significantly decreased PIP motion. They concluded that replantation through zone 2 is seldom indicated due to severe stiffness.
Boulas et al reviewed digital replantation and recommend initial treatment should consist of wrapping amputated parts in moistened gauze and placing on ice. Sharp and clean amputations are considered more viable candidates for replantation due to limited damage to the replantation junction compared to crush injuries. Additionally, they state the patients with major psychiatric disorders or those that are unable to comply with postoperative protocols should also be considered poor candidates for replantation.
Figure A demonstrates an amputation through the left index finger proximal phalanx with no evidence of comminution or crush injury. Illustration A demonstrates the flexor tendon zones.
Incorrect Answers:
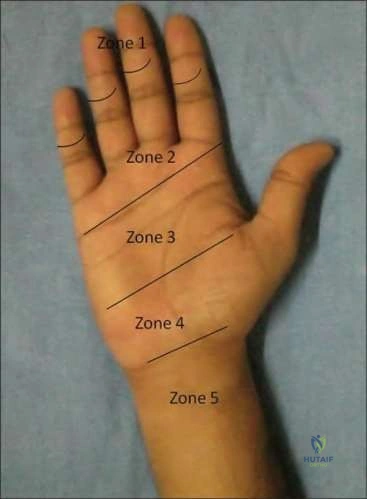
A patient sustains an acute, closed injury to his index finger. The clinical appearance of the finger is shown in Figure A. The patient is asked to extend the finger against resistance, with the PIP joint in 90 degrees of flexion. You note that PIP joint extension was weak, with hyperextension and restricted passive flexion of the DIP joint. When planning to treat this injury non-operatively which active joint motion is encouraged?
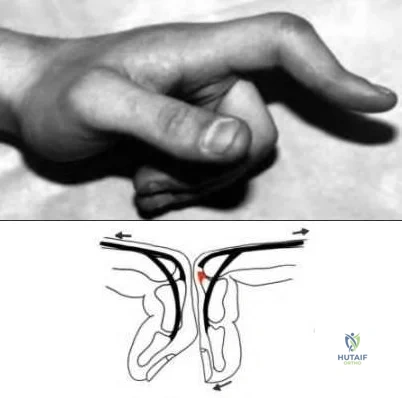
DIP flexion
MCP flexion
MCP extension
PIP extension
PIP flexion CORRECT ANSWER: 1
This patient has sustained a central slip injury. Treatment consists of full time extension splinting of the PIP joint for 5 weeks with active DIP motion (flexion) encouraged.
A central slip injury, or a zone 3 extensor tendon injury, is characterized by PIP flexion and DIP extension (boutonniere deformity). This is most often caused by a rupture of the central slip over the PIP joint caused by a laceration, a traumatic avulsion, or capsular distension in rheumatoid arthritis. A rupture of the central slip causes the extrinsic extension mechanism from the EDC to be lost and prevents extension at the PIP joint. This allows the lumbricals' pull to become unopposed, causing PIP flexion and DIP extension. The examination maneuver described in the question stem is the Elson Test. It is the most reliable way to diagnose a central slip injury before the deformity is present. Non-operative treatment may be undertaken if the injury is closed and presents acutely. The PIP is splinted in full extension for 5 weeks. Active DIP extension and flexion in the splint is encouraged to avoid contraction of the oblique retinacular ligament.
Posner et al. describe the diagnosis and treatment of finger deformities following injuries to the extensor tendon mechanism. They suggest that treatment of a boutonniere deformity depends on its stage. For the acute injury (within the first 2 weeks), immobilization of the proximal interphalangeal joint in full extension for 5 weeks using a static splint that permits active and passive flexion of the DIP joint is usually effective.
Figure A is a clinical photograph demonstrating an index finger with the classic boutonniere deformity of flexion at the PIP joint and hyperextension of the DIP joint. Figure B is a diagram showing the Elson test. When the central slip is intact, there is no hyperextension of the distal phalanx. When the central slip is disrupted, the distal phalanx can hyperextend due to the function of the tight lateral bands.
Incorrect Answers:
A 25-year-old male is stabbed in the proximal volar forearm while fighting in a bar. He presents to the ED with a 1 cm wound and moderate oozing of blood. On exam, he has normal sensation throughout all distributions in his hand, normal radial and ulnar pulses, and a normal tenodesis effect. He is unable to actively flex his index finger DIP joint. Which muscle will also likely not function as a result of his injury?
Flexor digitorum brevis
Flexor carpi radialis
Flexor carpi ulnaris
Flexor pollicis longus
Pronator teres CORRECT ANSWER: 4
The patient has sustained a laceration of the anterior interosseous nerve (AIN), which is a branch of the median nerve and innervates the flexor pollicis longus, pronator quadratus, and the flexor digitorum profundus to the index and long fingers. An intact tenodesis effect signifies that all of his tendons are structurally intact.
The AIN can be injured by a penetrating injury or chronic compression. It
arises from the dorsoradial aspect of the median nerve distal to the elbow. It then passes between the FPL and FDP to lie on the anterior interosseous membrane en route to the pronator quadratus and wrist capsule (Illustration A). Compression sites of the AIN include the deep head of the pronator teres, FDS arcade, edge of the lacertus fibrosus, an accessory head of the FPL, or other accessory muscles of the forearm (FDS, FDP, FCR). In this particular scenario of an acute, penetrating AIN injury, exploration and primary end-to-end suture repair is appropriate.
Rodner et al. review AIN syndrome and stress the importance of ruling out a tendon rupture, which can present similarly and can be differentiated by testing the patient's tenodesis effect. Non-traumatic AIN syndrome is usually the result of a neuritis, similar to Parsonage-Turner Syndrome (brachial plexus neuritis), and may have similar triggers such as viral infection or autoimmune disease. They recommend a prolonged period of observation (~12 months; in the absence of an obvious compressive or space-occupying lesion) due to high rates of spontaneous recovery at about one year.
Park et al. report on 11 patients that underwent surgical exploration for spontaneous AIN syndrome at an average of 7.8 months. The most common compressive structure was a fibrous band of the FDS, however, four patients had no obvious compressive structure, emphasizing the importance of at least six months of conservative treatment.
Incorrect answers:
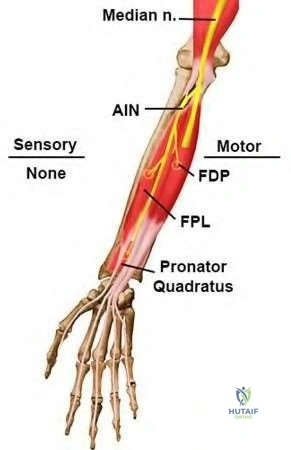
A 38-year-old female presents with 8 months of gradual weakness of her right hand. She denies paresthesias, numbness, and pain in the right upper extremity. She has compensatory thumb interphalangeal flexion during key pinch and intact two point discrimination. She has a negative Tinel's sign at the wrist and elbow. Electromyography (EMG) shows normal sensory conduction velocities but delayed motor conduction to the first dorsal interosseous muscle. Figure A and B show MRI images of pre and post contrast, respectively. Ultrasound is shown in Figure C. What is the next best step?
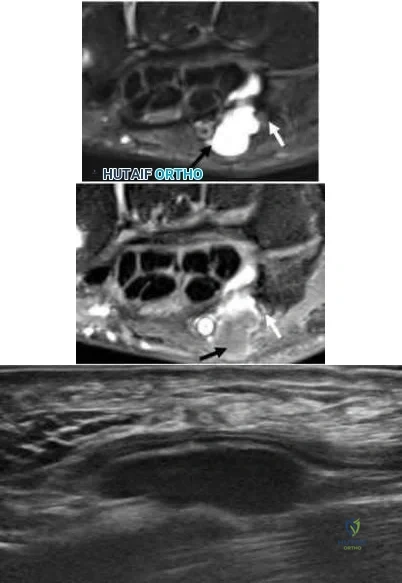
Biopsy of the mass
Cyst excision
MRI of cervical spine
Excision of the hook of hamate
Cubital tunnel release CORRECT ANSWER: 2
The patient has pure motor symptoms from ulnar nerve compression by a ganglion cyst at Guyon's canal. The next best treatment is excision of the ganglion cyst.
Atraumatic compression of the ulnar nerve at Guyon's canal is caused by a ganglion cyst 80% of the time. Compression may present with mixed motor and sensory or pure motor symptoms. With purely motor compression the deep branch of the ulnar nerve is affected resulting in weakness of adductor pollicis. Subsequent loss of metacarpophalangeal flexion and adduction leads to a positive Froment's sign with compensatory thumb IP flexion. Pure motor compression will result in normal sensory examination and intact two point discrimination as sensory branches are unaffected. EMG will localize decreased velocities at the wrist. When neurologic symptoms are present, cyst excision is recommended. Ganglion cysts in this location often arise from the pisohamate joint and excision of the stalk is important to prevent recurrence.
Wang et al. retrospectively investigated the outcomes of 9 patients with
ganglion cysts with symptomatic compression of the deep branch of the ulnar nerve. At a mean follow-up of 23 months they found all patients had improved grip and tip pinch strength. They conclude that surgical intervention can lead to satisfactory outcomes.
Shen et al review the imaging findings possible in patients with ulnar neuropathy. They present a case of a patient with ulnar neuropathy secondary to a ganglion cyst in guyon's canal.
Maroukis et al. review the history of the clinical anatomy of Guyon's canal. They conclude that the three zone theory helped simplify the complex anatomy of ulnar nerve compression at Guyon's canal.
Figure A (Shen et al) shows a T2 fat saturation MRI of a well circumscribed lesion (black arrow) with homogeneous fluid signal intensity at Guyon's canal compressing the ulnar nerve (white arrow). Figure B (Shen et al) shows a post contrast T1 fat saturation MRI showing rim enhancement consistent with a cyst (black arrow) and compression of the ulnar nerve (white arrow). Figure C shows an longitudinal ultrasound view of a anechoic well defined structure consistent with a cyst. Illustration A shows the areas of potential ulnar nerve compression in Guyon's canal. Illustration B shows a table with potential causes for compression at each zone and expected symptoms.
Incorrect Answers:
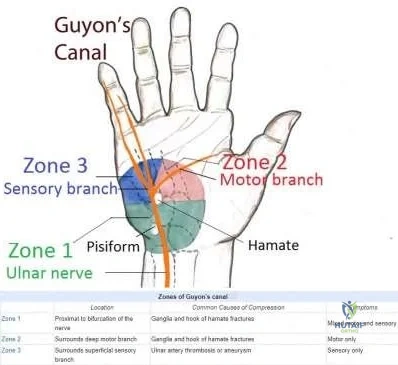
A 20-year-old male presents to clinic for evaluation of right wrist pain. He fell playing flag football about 6 weeks ago. He initially had significant pain but since it slowly improved he did not seek immediate treatment. His improvement has now plateaued. Figures A and B are x-rays, and figures C and D select CT scan images of his right wrist. What is the best treatment option?

Percutaneous screw fixation
Open reduction internal fixation through a volar approach
Open reduction internal fixation through a dorsal approach
Open reduction internal fixation with bone grafting through a volar approach
Open reduction internal fixation with bone grafting through a dorsal approach
The patient presents with a displaced right scaphoid waist fracture with cyst formation. The best treatment would open reduction internal fixation (ORIF) with bone grafting through a volar approach.
The surgical management of scaphoid fracture depends on location and characteristics of the fracture as well as time from injury. Displaced distal pole and waist fractures are typically approached from the volar side, especially if there is a humpback deformity; the proximal pole is more easily accessed from the dorsal side. Injuries with significant comminution or cyst formation due to extended time to treatment are often augmented with bone graft. There is controversy as to the use of vascularized bone graft in nonunion cases.
Rettig et al. reported on fourteen patients undergoing acute surgical fixation for displaced scaphoid waist fractures. Thirteen patients united and regained functional wrist range of motion and grip strength. They advocate for early
operative intervention in these fractures.
Raskin et al. describe the utility of the dorsal approach for proximal pole scaphoid fractures. They report good fracture visualization and the ability to bone graft through the same incision with successful union in a majority of cases.
Pinder et al. reviewed the literature on management of scaphoid nonunions. They found no difference in use of nonvascularized or vascularized bone graft, choice of approach, or use of Kirschner wires versus screw fixation.
Figures A and B are postero-anterior lateral right wrist radiographs with a displaced scaphoid waist fracture and mild humpback deformity. Figures C and D are coronal and sagittal CT cuts, respectively, demonstrating cyst formation and better showing the humpback deformity.
Incorrect Answers:
A 53-year-old white male presents with contractures of his ring finger and lesions over the dorsum of his hand. On examination of the lesions, they are subcutaneous, solid, and firm lesions measuring about 5 mm in diameter. They are located over the dorsum of the PIP joints of his ring and long finger. They become more mobile while the joint is in neutral and less mobile when the joint is in flexion. He also has a 5 degree flexion contracture his ring finger MCP joint. Examination of his palm reveals a palpable cord over the volar ring finger. His neurovascular examination is normal. The appearance of the dorsum of his hand is seen in Figure A. What is the next most appropriate step in treatment?

Collagenase injection and resection of dorsal finger lesions
Collagenase injection without resection of dorsal finger lesions
Observation and follow up
Surgical resection/fasciectomy and resection of dorsal finger lesions
Surgical resection/fasciectomy without resection of dorsal finger lesions
This patient has mild Dupuytren's disease with associated dorsal Dupuytren nodules, which may be observed.
Dupuytren’s disease is a proliferative disorder characterized by fascial nodules and contractures of the hand. It is autosomal dominant with variable penetrance. It exhibits a 2:1 male to female ratio and is classically seen in Caucasian males of northern European descent. The main pathology of
Dupuytren’s disease is excessive myofibroblast proliferation and altered collagen matrix composition lead to thickened and contracted palmar fascia. Surgical intervention is often indicated in cases of ≥30° of MCP contracture or any PIP contracture (usually >15°).
Rayan et al report that dorsal Dupuytren's nodules are a subcutaneous, solid, firm, well-defined, tumor-like mass or a nodule 3 mm in diameter or larger, located over the dorsum of the PIP joint. It is seldom painful and becomes more mobile while the joint is in neutral position and less mobile during joint flexion.
Black et al report that diseased tissue is referred to as nodules or cords. The Dupuytren nodule is a palpable subcutaneous lump that may be fixed to the skin. Cords are highly organized collagen structures arranged in parallel with a relatively hypocellular matrix. Cords are predominantly composed of collagen III while normal palmar fascia is predominantly collagen I.
Figure A is a picture of a dorsal Dupuytren's nodule. Incorrect Answers:
at this time. The dorsal finger lesions should not be resected.
A 37-year-old man has a 2-year history of increasing right wrist pain that is worse at night and aggravated by activity. He denies systemic symptoms, history of trauma, or recent weight loss. On physical exam he has tenderness over the dorsal radiocarpal joint. Radiographs of the right wrist are shown in Figure A. Which of the following imaging studies would be most sensitive for determining the stage of this patient's underlying condition?

Ultrasound
Angiography
CT scan of the wrist
Clenched fist AP radiograph of wrist
Bone scan of the wrist CORRECT ANSWER: 3
The clinical presentation of dorsal radiocarpal wrist pain is suggestive of Kienbock’s disease. Figure A shows an AP radiograph of the right wrist with
evidence of lunate sclerosis with no obvious collapse. The imaging study most sensitive for identifying early lunate collapse in Kienbock's disease is CT scanning of the wrist.
Kienbock’s disease is defined by avascular necrosis of the lunate. It is classified into 4 stages under the Lichtman Classification. In stage 1, plain radiographs appear normal and magnetic resonance imaging is required for diagnosis. MRI is useful for detecting early disease when sclerosis is not evident on plain film radiographs. In stage 2, plain radiographs and/or CT scan images will show sclerosis of the lunate but no evidence of collapse. In stage 3, radiographs and/or CT scan images will show lunate collapse. For stage 4, radiographs show degenerative changes to the adjacent carpus and intercarpal joints.
Imaeda et al. examined the use of MRI for the diagnosis and staging of Kienbock's disease. They found that MRI was most sensitive in detecting early focal loss of signal intensity in the lunate on T1-weighted images. This was a key diagnostic feature in early stages of Kienböck's disease when plain radiographs appear normal.
Cross et al. reviewed the latest concepts for diagnosis, staging, and management of Keinbock's disease. They suggest that computed tomography (CT) or tomography will better characterize lunate necrosis and trabecular destruction once collapse or sclerosis has occurred in late stage disease.
Illustration A is a collection of CT scanning images that show osteonecrosis of the lunate. The blue arrow shows lunate flattening and sclerosis. The red double arrow shows a loss of lunate height and the yellow shows fragmentation of the bone.
Incorrect Answers:
widening of the scapholunate interval.

Each of the following are indications for microvascular replantation EXCEPT?
Thumb amputation
Index finger amputation in a child
Through wrist amputation
Long finger amputation through the proximal phalanx
Mid-palm amputation of all four fingers
As reviewed by Soucacos, there are several major indications for single digit replantation: 1) Level of the amputation is distal to the insertion of FDS. 2) Amputations at the level of the distal phalanx. 3) Ring avulsion injuries involving both the dorsal and palmar skin and blood supply in an isolated finger, as long as FDS is intact. 4) Any amputation in a child. 5) Thumb amputation. Replantation of a single digit, which is amputated at the level of the proximal phalanx or at the PIP joint, particularly in avulsion or crush injury is contra-indicated. Soucacos also discusses appropriate surgical teams, transport, and other related issues surrounding a "transplant team."
All of the following are predictive findings for correctly diagnosing carpal tunnel syndrome EXCEPT:
Abnormal hand diagram
Abnormal Semmes-Weinstein testing in wrist-neutral position
Positive median nerve compression test (Durkan's sign)
Presence of night pain
Loss of small digit adduction (Wartenberg sign)
All of the listed physical exam findings, except for loss of small digit adduction (Wartenberg sign), has been found to be predictive for diagnosing carpal tunnel syndrome.
Szabo et al in a Level 3 study used a regression model to analyze the most predictive factors for correctly diagnosing carpal tunnel syndrome (CTS). Their analysis found that with an abnormal hand diagram, abnormal sensibility by Semmes-Weinstein testing in wrist-neutral position, a positive Durkan's test, and night pain, the probability that carpal tunnel syndrome will be correctly diagnosed is 0.86. They found the tests with the highest sensitivity were Durkan's compression test (89%), Semmes-Weinstein testing after Phalen's maneuver (83%), and hand diagram scores (76%). Night pain was a sensitive symptom predictor (96%). The most specific tests were the hand diagram (76%) and Tinel's sign (71%). The authors concluded that the addition of electrodiagnostic tests did not increase the diagnostic power of the combination of these 4 clinical tests, and proceeding with surgical release is appropriate even if the EMG is normal.
Wartenberg sign is persistent abduction and extension of the small digit when a patient is asked to adduct the digits and is seen in cubital tunnel syndrome, but not carpal tunnel syndrome.
Illustration V demonstrate the Durkan's Compression test for carpal tunnel syndrome.
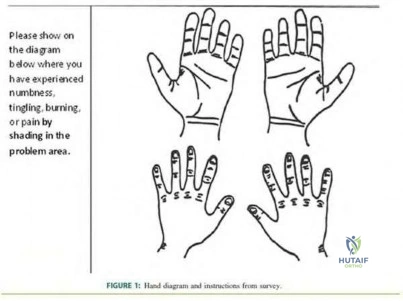
Extrinsic imbalance from splinting a crushed hand with metacarpophalangeal joint extension causes what characteristic hand deformity?
Distal interphalangeal joint extension
Ulnar subluxation of the metacarpophalangeal joints
Proximal interphalangeal joint extension
Proximal interphalangeal joint flexion
Swan-neck deformity CORRECT ANSWER: 4
Failure to splint the hand in an intrinsic positive position leads to increased extrinsic finger flexor tension, leading the DIP and PIP joints to have an increasing flexion position. Illustration A and B show a clinical image and illustration of intrinsic minus hand.
von Schroeder et al present a Level 5 review of hand crush injuries. They conclude that early diagnosis and treatment is critical, but the functional outcome is often poor with associated Volkmann's contracture.
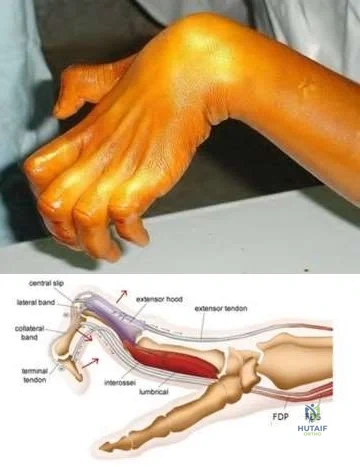
Axon regeneration almost always occurs following a Sunderland second-degree nerve injury because which anatomic structure is not injured?
Epineurium
Endoneurium
Perineurium
Myelin sheath
Schwann cell CORRECT ANSWER: 2
Following a Sunderland second-degree injury, axon regeneration is possible because the endoneurium is intact.
There are two classification schemes for peripheral nerve injuries, which include the Seddon and the Sunderland systems. Under the Sunderland
classification, a second-degree injury is considered a part of the axonotmesis spectrum. The endoneurium, perineurium and epineurium are still intact. This enables complete functional recovery.
Lee et al. review the pathophysiology and evaluation of peripheral nerve injuries. They note that in Sunderland type two injuries, there is physiologic disruption of the axons. Because the endoneurium is still intact, axons are able to regenerate. This process takes months.
Illustration A is a schematic of the various stages of peripheral nerve injury. Incorrect Answers
Sunderland type 2 injury, axon regeneration is possible because of an intact endoneurium.
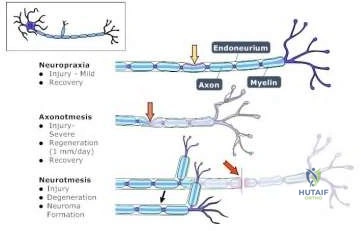
A 29-year-old intravenous drug user undergoes irrigation and debridement of a ring finger abscess. After adequate eradication of the infection, he is left with the skin defect shown in Figure A. What is the most appropriate treatment at this time?

Local woundcare and healing by secondary intention
V-Y advancement flap
Thenar flap
Moberg flap
Cross-finger flap CORRECT ANSWER: 5
Based on the location of the lesion, a cross-finger flap would be most appropriate.
Cross finger flaps are indicated in patients > 30 years of age when the lesion is a volar oblique finger tip lacerations or a volar proximal finger lesions. The advantage is it leads to less stiffness.
Martin et al review the treatment options available for digit injuries. They report treatment of fingertip injuries is a continuous focus of controversy among hand and orthopaedic surgeons. Different treatment options have been described, depending on the affected segment and finger, type of lesion, gender and age of the patient, location, size, and depth of the defect.
Fassler et al reviews the proper management of fingertip injuries discussing variables such as the severity of soft tissue loss and whether bone is exposed.
Incorrect Answers:
A 4-year-old boy sustains a flexor tendon laceration in Zone 2 of his 4th digit when he attempts to grab a knife. Optimal surgical management and postoperative rehabilitation consists of:
2 strand core suture technique and gentle active flexion and extension exercises with wrist in extension
2 strand core suture technique and cast immobilization for 8 weeks
4 strand core suture technique and gentle active flexion and extension exercises with wrist in extension
4 strand core suture technique and cast immobilization for 4 weeks
4 strand core suture technique and cast immobilization for 8 weeks
4 strand core suture technique and cast immobilization for 4 weeks is the preferred postoperative rehabiltation in a 4 year old child.
Ordinarily, adult flexor tendon repair postoperative rehab protocols call for early light active digital flexion with wrist in gentle flexion as long as the tendon has been repaired with a 4 or 6 strand core suture technique and strong epitendinous suture. However, this method cannot succeed without the cooperation of a mature and motivated patient. Children or the mentally disabled are often lacking some of these prerequisites. Therefore, a flexor tendon repair in a child should be treated like a flexor tendon repair with interposed graft in an adult. Immobilization for a minimum of 3 – 4 weeks with a posterior molded plaster splint or cast from the tips of the fingers to just above the elbow. Wrist is flexed 35 degrees, MCPs flexed 60 – 70 degrees and IP joints relaxed in extension. Active motion can be started after the cast is removed at 4 weeks.
A 45-year-old male sustained a fall onto his right wrist 2 weeks ago. A radiograph is shown in figure A. What joint is first affected if left untreated with subsequent development of a SLAC (scapholunate advanced collapse) wrist?

Capitolunate joint
Radioscaphoid
Radioulnar
Radiolunate
STT (scaphotrapezotrapezoidal)
The clinical presentation is consistent with a SLAC wrist. The radioscaphoid joint is the first to be affected in this process.
The radiographs of the right wrist demonstrate a scapholunate dissociation, as evidenced by an increased scapholunate joint space, referred to as scapholunate diastasis (abnormal when the gap is greater than 2 mm and increased from the opposite extremity and other intercarpal spaces).
If left untreated, the wrist may progress to a "SLAC" wrist, as originally described by Watson and Ballet in 1984, which is the most common form of wrist arthritis. The repetitive sequence of degenerative changes is based on and caused by articular alignment problems between the scaphoid, the lunate and the radius.
Kuo et al. review the stages of SLAC wrist. They report stage I SLAC wrist involves changes limited to an area of abnormal contact between the abnormally rotated scaphoid and the radial styloid. In stage II the remaining radioscaphoid joint is affected, as persistent abnormal load transfer and shear across the cartilaginous surfaces leads to degeneration of the proximal scaphoid facet. In stage III, the dorsally translated capitate migrates proximally into the widened scapholunate interval, and degenerative changes occur at the capitolunate joint. The relative congruency of the radiolunate joint in all positions of lunate rotation due to the spherical shape of the lunate facet preserves this articulation, and at all stages of SLAC wrist the radiolunate joint is not involved. The lunate is congruently loaded in every position and, thus, highly resistant to degenerative changes.
Illustration A below shows the stages of involvement in the SLAC wrist.
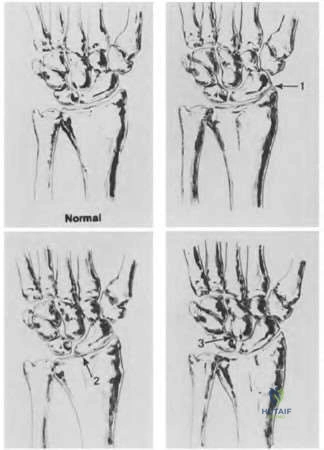
Question 94
Figures 15a and 15b are the radiographs of a 28-year-old man who fell from a height and sustained an isolated closed diaphyseal femur fracture that was treated with reamed antegrade femoral nailing 8 months ago. He now reports persistent pain during ambulation. He smokes one pack of cigarettes per day but is otherwise healthy. He denies any infectious history or symptoms, and laboratory studies show a normal WBC count, erythrocyte sedimentation rate, and C-reactive protein. What is the most appropriate treatment?

Explanation
Question 95
A 30-year-old man has had severe knee pain and swelling for 1 week. He reports he previously had acromioclavicular joint pain that disappeared. He denies any fever. Aspiration of a cloudy fluid from the knee reveals a WBC count of greater than 50,000 with 90% polymorphonucleocytes. While awaiting culture results, what is the most appropriate action?
Explanation
Question 96
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 97
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 98
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 99
The lesion seen in Figure 4 is most likely the result of metastases from what solid organ?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Leeson MC, Makley JT, Carter JR: Metastatic skeletal disease distal to the elbow and knee. Clin Orthop 1986;206:94-99.
Question 100
A 70-year-old female presents with right thigh ache for 6 months. Except for a history of osteoporosis, she is otherwise healthy. She has been on antiresorptive therapy for 8 years. Her radiograph is shown in Figure A. Four months later, she trips over a rug and falls, sustaining the injury shown in Figures B and C. Which of these statements is TRUE regarding surgical fixation of this fracture compared with conventional fractures?

Explanation
Subtrochanteric fractures are fractures extending from the lesser trochanter to 5cm distal to it. BP fractures are characterized by (1) focal lateral cortical thickening, (2) transverse fracture orientation, (3) medial spike and (4) lack of comminution. There is increased risk of iatrogenic fracture with IM nailing because BP fractures have thickened, brittle cortices and the mismatch between medullary diameter and increased proximal nail diameter results in iatrogenic fracture.
Weil et al. reviewed the outcome of surgically treated bisphosphonate fractures. IM nailing resulted in healing in 54% of bisphosphonate fractures with 98-99% of conventional fractures. In their study, 46% required revision procedures.
Prasarn et al. compared plate and nail treated bisphosphonate fractures with conventional fractures. They found that the bisphosphonate group had more major and minor complications (68%) than the conventional group (10%). The most common complications were intraoperative femoral shaft comminution (nail) and hardware failure (plate).
Figure A shows diffuse cortical thickening with an antero-lateral cortical ridge. Figure B shows a transverse subtrochanteric fracture extending through the middle of the cortical ridge seen previously. Note also healed fractures of the left superior and inferior rami. Figure C is a post-reduction radiograph showing the transverse fracture through the beak-shaped region of the previous insufficiency fracture. Illustration A shows a typical bisphosphonate-related fracture with transverse fracture orientation,
focal lateral cortical thickening (white arrows), medial beak (black arrow), and lack of comminution. Illustration B shows a conventional subtrochanteric fracture. Illustration C shows intraoperative iatrogenic fracture with anterolateral comminution during nailing. Illustration D shows fixation with a proximal femoral hook LCP Plate with late hardware failure at 3 months.
Incorrect Answers:
