Orthopedic Board Exam MCQs: Upper Extremity, Spine & Foot/Ankle | Part 112

Key Takeaway
This page presents Part 112 of an expert-authored orthopedic surgery board review quiz. It features 100 high-yield, verified MCQs mirroring OITE/AAOS exam formats, focusing on Deformity, Elbow, Fracture, Infection, and Nerve. Designed for orthopedic residents and surgeons, it offers interactive modes to optimize board certification preparation.
About This Board Review Set
This is Part 112 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 112
This module focuses heavily on: Deformity, Elbow, Fracture, Infection, Nerve.
Sample Questions from This Set
Sample Question 1: What is the most frequent location of entrapment of the deep peroneal nerve?...
Sample Question 2: Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing ...
Sample Question 3: An 80-year-old man with a history of chronic obstructive pulmonary disease (COPD) and dementia is involved in a fall from standing height, striking his forehead. He is seen in the emergency department with predominantly mechanical neck pain...
Sample Question 4: A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?...
Sample Question 5: Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
REFERENCES: Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 2
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?
Explanation
REFERENCES: Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573.
Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Pinzur M: Surgical versus accommodative treatment for Charcot arthropathy of the midfoot.
Foot Ankle Int 2004;25:545-549.
Question 3
An 80-year-old man with a history of chronic obstructive pulmonary disease (COPD) and dementia is involved in a fall from standing height, striking his forehead. He is seen in the emergency department with predominantly mechanical neck pain but no obvious neurologic deficits. Radiographs reveal a nondisplaced type II odontoid fracture. What is the most appropriate treatment? Review Topic
Explanation
Question 4
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 100.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 106.
Question 5
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
Explanation
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D. 1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Question 6
What is the most common problem seen following epiphysiodesis for limb-length discrepancy?
Explanation
REFERENCES: Blair VP III, Walker SJ, Sheridan JJ, Schoenecker PL: Epiphysiodesis: A problem of timing. J Pediatr Orthop 1982;2:281-284.
Raney ER: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
Question 7
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion- extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior
surgery was not deemed a contraindication.
Question 8
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?
Explanation
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
Question 9
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
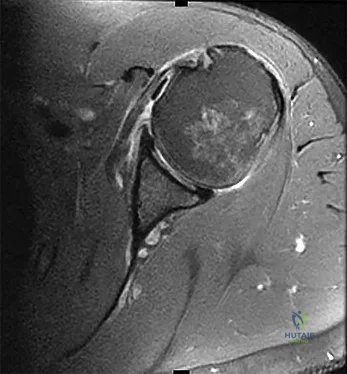
Question 10
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
REFERENCE: Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
Question 11
A 45-year-old male presented to the trauma department 10 hours after sustaining a fracture-dislocation of his ankle. The patient underwent an attempted closed reduction of his ankle which can be seen in Figures A and B. The splint was removed, and the appearance of the leg is shown in Figure C. Regarding the best next step in management and the intended goals, which of the following is most accurate?

Explanation
Patients with high-energy periarticular fractures in the lower extremity are at risk for surgical wound complications due to compromised soft tissues. As in this case, joint dislocations can place harmful tension on the skin that leads to blistering and/or skin necrosis. An urgent reduction is indicated, and if it cannot be obtained with a closed manipulation alone, percutaneous or open treatment is indicated. Staged joint-spanning external fixation can both hold a reduction and allow access for skin or wound care prior to a definitive open reduction of an articular fracture. Fracture healing during external fixation occurs by enchondral ossification by way of the relative stability.
Strauss et al. developed a treatment protocol for the treatment of fracture blisters. They used silver sulfadine to minimize soft tissue complications by promoting re-epithelialization. After providone-iodine prep, each blister was unroofed by removing the overlying epithelium of the fracture. Once the blister was unroofed, silver sulfadiazine was applied and covered with dry gauze. They would then perform bid dressing changes. Extremities were deemed operable when skin wrinkles were visible on the overlying skin of the injured extremity.
Anglen et al. in a review of external fixation, report that fractures of the lower extremity are frequently associated with soft tissue trauma that precludes safe surgical treatment in the early period. They present a technique of temporary joint-spanning external fixation which allows stabilization of length and alignment while awaiting resolution of soft tissue swelling. They report no differences between patients who had a temporary external fixator and those who did not with respect to healing time, time to partial or full weight bearing, or clinical score.
Figures A and B demonstrate a pronation-external rotation type fracture with disruption of the syndesmosis. Figure C demonstrates fracture blisters.
Illustration A demonstrates an ankle-spanning external fixator. Illustration B demonstrates skin wrinkling to indicate that the skin is safe to incise.
Incorrect Answers:

OrthoCash 2020
Question 12
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic
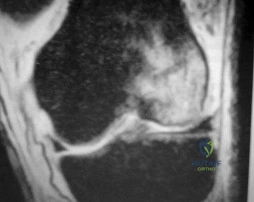
Explanation
Question 13
A fracture in the following location is most commonly associated with procurvatum and valgus malalignment?
Explanation
Proximal third tibial shaft fractures are often difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. Many different techniques have been devised to overcome the deforming forces. These include (1) Poller blocking screws posterior and lateral to the intramedullary nail (IMN), (2) utilizing a semiextended knee position during IMN of proximal tibia fractures (3) use of a suprapatellar approach for IMN, (4) usage of a slightly more lateral starting point during conventional IMN, and (5) application of unicortical plate.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibia. Post-operatively, all patients in their series had less than 5 degrees of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Illustration A shows intra-operative sagittal radiographs of the proximal tibia. Note the use of Poller blocking screws in the posterior and lateral aspects of the proximal tibia.
Incorrect Answers:
Question 14
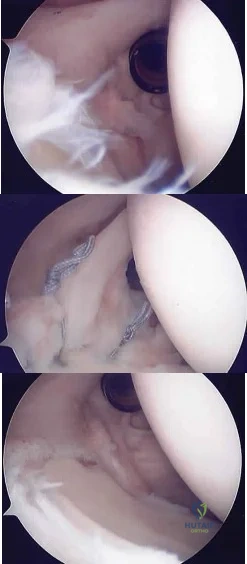
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
Toe is fused too straight (plantar flexed)
Toe is fused in too much valgus
Toe is fused in too much dorsiflexion
There is a nonunion of the fusion
Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 15
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
Explanation
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.
Question 16
Which of the following best describes the course of the ulnar nerve in the midforearm?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 17
Moderate distance running has what effect on knee articular cartilage in asymptomatic distance runners?
Explanation
Question 18
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
REFERENCES: Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343.
Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
Morsy HA: Complications of fracture of the neck of the femur in children: A long-term follow-up study. Injury 2001;32:45-51.
Question 19
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis? Review Topic
Explanation
Question 20
Figures 11a and 11b show the T 2 -weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?
Explanation
REFERENCES: Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972.
Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Question 21
A 23-year-old male college quarterback presents with acute left shoulder pain after being tackled. A radiograph of the injury is shown in figure A. After successful closed reduction, what shoulder position should be avoided in order to minimize the risk of a repeat injury? Review Topic

Explanation
Shoulder stability is achieved through the both dynamic and static stabilizers. The static stabilizers include the bony morphology of the joint, glenoid labrum, capsule, and glenohumeral ligaments. The contributions of the glenohumeral ligaments to shoulder stability are dependent upon the position of the humerus relative to the glenoid. Posterior stability is afforded to the joint by the superior glenohumeral ligament (SGHL) and the posterior band of the inferior glenohumeral ligament (IGHL). The SGHL specifically is taught and provides posterior stability with the shoulder in flexion, adduction, and internal rotation.
Kim et. al. reviewed their experience treating 27 athletes diagnosed with traumatic posterior shoulder instability and treated with arthroscopic posterior labral repair and capsular shift. Most patients were found to have an incompletely stripped posterior capsulolabral complex. After arthroscopic repair and shift, all 26 of the 27 patients treated had improved shoulder function and objective scores, a stable shoulder, and were able to return to sport.
Millett et. al. reviewed posterior shoulder instability. They describe the static restraints of the posterior shoulder as the SGHL, posterior band of IGHL, and the coraohumeral ligament (CHL). The SGHL and CHL are both taught in the position of flexion, adduction, and internal rotation, whereas the posterior band of the IGHL is taught in abduction. They describe posterior instability occuring secondary to overhead sports due to repetitive microtrauma causing gradual capsular failure.
Figure A is an axillary radiograph of the left shoulder demonstrating a posterior dislocation and an engaging reverse Hill-Sachs lesion.
Incorrect Answers:
Question 22
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 23
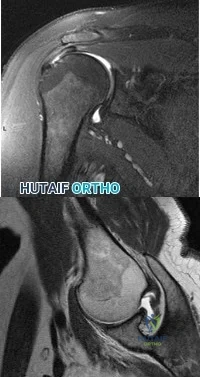
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?

Explanation
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more appropriate in the older patient with pre-existing advanced degenerative changes.
Question 24
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 25
In which scenario is application of NPWT contraindicated?
Explanation
The most common complication associated with NPWT is a rash on the skin resulting from contact with a suction sponge. In a 2001 study by Webb and Schmidt, 2.2% of patients treated with NPWT had a rash that resolved within 48 hours. To minimize risk for this rash, care should be taken to avoid overlap of the sponge onto intact skin. If skin overlap is unavoidable, a lower-pressure setting should be used.
Acute bacterial infection is possible in this scenario, but there would likely be additional findings such as purulence in the wound itself. Similarly, an acute allergic reaction could be found within the wound and not just at the skin edge. Skin irritation from excessive adhesive plastic tension can result in blistering or shearing avulsion but not skin-edge erythema. Skin necrosis from the original trauma would result in skin-edge duskiness instead of erythema.
A study by Timmers and associates showed a statistically significant increase in microvascular blood flow to the skin under a sponge at subatmospheric pressures. Angiogenesis occurs in the area of the wound vacuum from the negative pressure and increased blood flow, not from the sponge material itself. There has been no indication that antibiotic concentration is increased in the setting of negative pressure therapy because antibiotics would be evacuated along with the fluid. NPWT does not result in increased temperatures that would kill pathogens.
NPWT is contraindicated in the setting of neoplasm because its effect on tumors is unknown. There is potential for increased angiogenesis in residual tumor cells, which could lead to recurrence or even metastasis. NPWT has been used safely and effectively for coverage of open fractures between initial debridement and definitive coverage. Fasciotomy wounds are frequently covered with NPWT dressings on a temporary basis with excellent results.
NPWT has been used to temporize wounds with exposed bone before flap coverage. Wounds with excessive tension frequently can be closed after short-term coverage with NPWT dressings.
RECOMMENDED READINGS
Webb LX, Schmidt U. [Wound management with vacuum therapy]. Unfallchirurg. 2001 Oct;104(10):918-26. German. PubMed PMID: 11699301.View Abstract at PubMed
Webb LX. New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg. 2002 Sep-Oct;10(5):303-11. PubMed PMID: 12374481. View Abstract at PubMed
Timmers MS, Le Cessie S, Banwell P, Jukema GN. The effects of varying degrees of pressure delivered bynegative-pressure wound therapy on skin perfusion. Ann Plast Surg. 2005 Dec;55(6):665-71. PubMed PMID: 16327472. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 68 AND 69

Figure 68 is the radiograph of a 17-year-old girl who is treated with closed reduction and percutaneous screw fixation for her displaced femoral neck fracture. Capsulotomy of the hip is not performed. After surgery, the patient is instructed to maintain touch-down weight-bearing status for 3 months.
Question 26
Which of the following preoperative findings is a predictor of poor outcome following arthroscopic debridement for glenohumeral arthritis? Review Topic
Explanation
Question 27
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
REFERENCES: Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 28
A 51-year-old female presents with an acute inability to extend her thumb, four months after she was treated with cast immobilization for a minimally-displaced distal radius fracture. What is the most appropriate treatment at this time?

Explanation
Magnussen et al. reviewed results of EIP transfer following ruptures of the EPL, with 19/21 good results. None of the cases had any loss of independent index finger extension although index extensor strength reduced to half of that of the contralateral side.
Hove et al. reported a similar satisfaction rate following treatment of 15 patients. In his series of 4,400 distal radius fractures treated over a 5 year period, the incidence of delayed tendon rupture following distal radius fracture was 0.3 percent.
Question 29
The MRI scans and diagnostic ultrasound shown in Figures 2a through 2c show what pathologic condition? Review Topic
Explanation
Question 30
A 74-year-old woman with rheumatoid arthritis has pain in the shoulder that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 24a and 24b. Active forward elevation is 120 degrees and external rotation is 30 degrees. At the time of surgery, a 1-cm rotator cuff tear is found, which is repairable. Which of the following treatment options will result in the most predictable pain relief and function? Review Topic

Explanation
Question 31
-Figures a and b are the plain radiographs of a 26-year-old man with an elbow contracture. He denies any specific elbow trauma but reports a history of a closed-head injury sustained in a motor vehicle collision. Examination reveals the elbow lacked 55 degrees of extension and has flexion of 85 degrees.Supination and pronation are well preserved. Release of which structure is essential to restore elbow flexion?

Explanation

Question 32
A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Shoulder arthroscopic views are shown in Figures 16a through 16c. What is the underlying association with this condition? Review Topic
Explanation
Question 33
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.
Question 34
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was
Explanation
REFERENCES: Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208.
Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107.
Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Fredrickson BE, Baker D, McHolik WJ, Yuan HA, Lubicky JP: The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 1984;66:699-707.
Question 35
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
Explanation
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.

Question 36
What type of medial collateral ligament tear heals the most reliably? Review Topic
Explanation
Question 37
A 12-year-old girl has scoliosis at T5-T10 that measures 62°. A clinical photograph of the axilla is shown in Figure 56. Management should consist of
Explanation
REFERENCES: Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 38
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints? Review Topic
Explanation
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
Question 39
A 17-year-old high school athlete comes in with a 6-month history of right midfoot pain. She has been treated with cast immobilization, crutches, and physical therapy. She still has significant pain with activities and cannot participate in sports. Her radiograph is shown in Figure 93a, and MR images are shown in Figures 93b and 93c. What is the most appropriate 79 next step? A B C

Explanation
RECOMMENDED READINGS
Lee S, Anderson RB. Stress fractures of the tarsal navicular. Foot Ankle Clin. 2004 Mar;9(1):85-104. Review. PubMed PMID: 15062216. View Abstract at PubMed
Anderson RB, Cohen BE. Stress fractures of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:1590-1597.
Question 40
What is the most appropriate orthosis for hallux rigidus?
Explanation
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Watson AD, Wapner KL: Foot and ankle reconstruction, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, p 635.
Question 41
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 42
below shows the abdominal radiograph obtained from a year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 43
A patient with myelopathy underwent a one-level corpectomy 1 day ago and is now home. In the middle of the night he calls to report markedly increased difficulty in swallowing, diaphoresis, a change in his voice, and difficulty lying flat. What is the best course of action?
Explanation
REFERENCES: Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multilevel cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
McAfee PC, Bohlman HH, Riley LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surg Am 1987;69:1371-1383.
Question 44
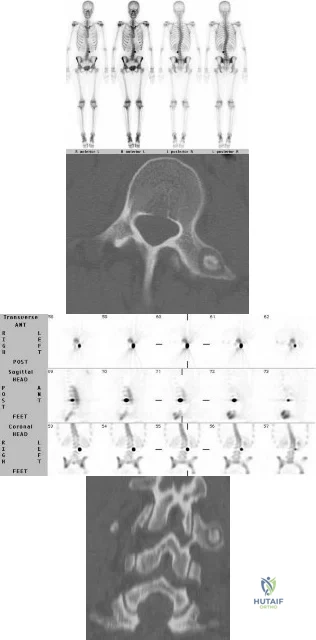
A 13-year-old premenarchal girl presents with back pain and scoliosis. Figures A through D are the bone scan, SPECT scan, axial and coronal images respectively. What is the most likely diagnosis? Review Topic
Explanation
patient
has
osteoid
osteoma
(OO).
OO and osteoblastoma (OB) of the spine commonly present in the 2nd decade of life. CT shows a low attenuation nidus with central mineralization and varying degrees of perinidal sclerosis. NSAIDS are thought to inhibit PGE 2 and PGI 2 produced within the nidus, and suppress perinidal edema arising from high levels of COX2 expression in neoplastic nidal osteoblasts.
Burn et al. reviewed pediatric OO and OB of the spine. OB is more likely to have neurological deficit because of spinal canal encroachment. Surgery involves complete resection. They recommend onlay fusion when the facet and pedicle have been resected, and instrumentation if resection of the vertebral body is carried out.
Jayakumar et al. discuss a case report of OO of the T6 vertebra that was treated successfully with NSAIDS alone. OOs of the spine are the most common cause of painful scoliosis in children and young adults. They caution against a non-operative course in patients with an immature skeleton, significant skeletal deformity or with a long delay before diagnosis.
Figures A and B are bone scan and SPECT scans respectively that demonstrate intense tracer uptake in the left transverse process of L3 characteristic of an osteoid osteoma. Dextroconvex scoliosis of the thoracic and levoconvex scoliosis of the lumbar spine is noted. Figures C and D are axial and coronal reconstructed CT images
showing show a lesion of the left transverse process of L3 with a dense "nidus" with surrounding lucency characteristic of osteoid osteoma. Illustration A is a table showing the characteristics of pediatric epidural spinal tumors.
Incorrect
Question 45
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 46
Mirror therapy is indicated for which of the following clinical conditions?
Explanation
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror
image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Question 47
Which repair technique for an osteochondral lesion of the medial talus shoulder produces hyaline cartilage that is similar to native cartilage and will not degrade over time?
Explanation
Autologous osteochondral transplantation (typically involving tubular grafts harvested from the knee) has been shown to replace a talar defect with viable hyaline cartilage. The results over the medium term show good clinical outcomes, and MRI studies reveal cartilage repair similar to native cartilage. Chondroplasty and arthroscopic bone-marrow stimulation are both associated with good clinical results for smaller lesions, but these techniques develop fibrocartilaginous repair tissue composed of type I collagen instead of hyaline cartilage. Osteochondral transplantation of fresh allografts performed less than 14 days after harvest contains high chondrocyte viability. Few clinical studies report long-term results, but radiographic studies demonstrate high rates of collapse and resorption. Joint space narrowing has been noted in 60% of ankles treated with bulk grafts after an average of 44 months. Autologous chondrocyte implantation (both periosteum-covered and matrix-associated techniques) has been shown to create hyaline cartilage in some studies, but fibrocartilage creation has been reported in others.
RECOMMENDED READINGS
Schachter AK, Chen AL, Reddy PD, Tejwani NC. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2005 May-Jun;13(3):152-8. Review. PubMed PMID: 15938604. View Abstract at PubMed
Mitchell ME, Giza E, Sullivan MR. Cartilage transplantation techniques for talar cartilage lesions. J Am Acad Orthop Surg. 2009 Jul;17(7):407-14. Review. PubMed PMID: 19571296. View Abstract at PubMed
Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013 Jun 5;95(11):1045-54. doi: 10.2106/JBJS.L.00773. Review. PubMed PMID: 23780543. View Abstract at PubMed
Question 48
- The Magnetic resonance imaging signal characteristics of a high-grade soft-tissue sarcoma are best described as
Explanation
other characteristics, such as size, pattern of growth, integrity of natural boundaries, and homogeneity.
Intravenous contrast agents are not necessary to evaluate neurovascular structures. Both the T1 & T2 weighted images are essential to detect and characterize soft tissue lesions.
Most Tumors have long T1 and T2 relaxation times, therefore, in most instances signal intensity alone is of limited benefit. Exceptions are lipoma, hematoma, intra-lesional hemorrhage.
Hemorrhage may occur in some soft tissue lesions, especially sarcomas, leading to the low T1 and high T2 intensity sound on MR. Miller, indicates that Water, CSF, acute hemorrhage and soft tissue tumors appear dark on T1 and light on T2.
Question 49
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?
Explanation
REFERENCES: Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22.
Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Morrey BF, Westholm F, Schoifet S, Rand JA, Bryan RS: Long-term results of various treatment options for an infected total knee arthroplasty. Clin Orthop 1989;248:120-128.
Question 50
- A patient reports persistent pain in the wrist 6 months after undergoing open reduction and internal fixation of a Galleazi fracture. Radiographs of the wrist in a neutral position are normal. Which of the following studies would best evaluate the reduction of the distal radioulnar joint?
Explanation
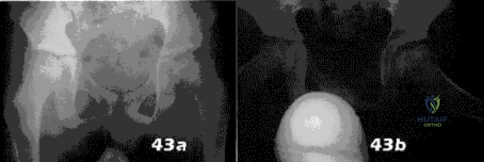
Question 51
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Thometz J: Tarsal coalition. Foot Ankle Clin 2000;5:103-118.
Question 52
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 53
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm P 3 P , an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?
Explanation
REFERENCES: Morrisy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 466-470.
Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis, and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 54
A 20-year-old college soccer player comes for an evaluation 6 months after an injury during which he landed awkwardly from a jump. Although physical therapy, ice, and activity modification have helped him return to baseline motion, strength, and swelling, he continues to have lateral knee pain. He also notes a popping sensation on the lateral side of his knee with activity. A Lachman test, anterior and posterior drawer tests, a pivot shift test, and McMurray test findings are all negative. MR images reveal a 12-mm x 15-mm osteochondral defect in the lateral femoral condyle with full-thickness cartilage loss and approximately 4 mm of subchondral bone loss.
Explanation
Patellofemoral pain in a young athlete without patellar instability or a chondral or osteochondral defect often can be managed with nonsurgical treatment such as physical therapy and a home exercise program. Microfracture surgery is associated with good short-term results for younger athletes. Patients with no history of prior surgery, primary chondral rather than osteochondral lesions, and lesions smaller than 2 cm have experienced the best results. Microfracture surgery performed for chondral lesions of the central aspect of the medial femoral condyle is associated with worse results. Decreased activity levels over time of patients who undergo microfracture surgery are a concern. OAT provides good outcomes and return-to-sports rates for athletic people who are younger and have lesions smaller than 2 cm. Patients with lesions on the lateral femoral condyle have better success rates. Both microfracture surgery and OAT provide better results for chondral defects than osteochondral defects. OAT is associated with better results than microfracture for medium-sized lesions between 2 cm and 4 cm, while autologous chondrocyte implantation yields better improvement for patients with defects larger than 4 cm. All of the surgical techniques listed for articular cartilage repair are associated with better outcomes for patients younger than age 30.
Question 55
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?
Explanation
REFERENCES: Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Morrey BF: Arthroscopy of the elbow. Instr Course Lect 1986;35:102-107.
Question 56
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis? Review Topic
Explanation
Question 57
A 31-year-old high school football coach has right medial knee pain that is made worse with prolonged standing. His knee is minimally painful in the morning but by the end of the school day, he must sit down. The pain often makes sleeping difficult. He states that several years ago he underwent a surgical procedure to "clean out" the cartilage of the knee; however, he only had several months of pain relief. He is noted to be an athletic male (BMI of less than 30). Knee examination is unremarkable except for medial joint line pain that is exacerbated with standing and walking. Radiographs, including a long-leg view, and MRI scans are seen in Figures 153a through 153d. He wishes to remain active and asks whether he would be a candidate for allograft meniscus transplantation. You advise him that Review Topic

Explanation
Question 58
A 44-year-old recreational weight lifter reports chronic deep pain in his left shoulder that is aggravated by any pressing exercises. He also notes a painful catch in the shoulder occurring with rotational movements. Physical therapy and nonsteroidal anti-inflammatory drugs for 3 months have failed to provide relief. Examination reveals pain with O’Brien’s test but no signs of instability. MRI scans are shown in Figures 4a and 4b. Treatment should now consist of
Explanation
REFERENCE: Snyder SJ, Karzel RP, Delpizzo W: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch cysts. J Shoulder Elbow Surg 2002;11:600-604.
McFarland EG, Kim TK, Savino RM: Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
O’Brien SJ, Pagnani MJ, Fealy S, et al: The active compression test: A new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med
1998;26:610-613.
Question 59
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Explanation
REFERENCE: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
Question 60
A 25-year-old athlete presents with symptoms attributed to injury to ligament D in Figure A. Which of the following symptoms and signs is characteristic of this injury? Review Topic
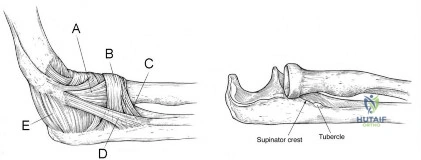
Explanation
PLRI can be diagnosed using the lateral pivot shift or posterolateral drawer. According to O’Driscoll, the elbow dislocates in 3 stages from lateral to medial (circle of Horii). Stage 1 involves disruption of the LUCL and partial/total disruption of the LCL complex (creating PLRI). Patients have pain with varus stress. Stage 2 includes disruption of the anterior capsule from incomplete elbow posterolateral dislocation. Stage 3 is divided into:
(a) Disruption of all soft tissues surrounding/ including the posterior MCL except for the anterior bundle. This bundle forms the pivot around which the elbow dislocates in a posterior direction by way of a posterolateral rotatory mechanism; and (b) complete disruption of the MCL.
O'Driscoll et al. describe PLRI diagnosed in 5 patients who had elbow dislocation using the posterolateral rotatory instability test, which they describe as being analogous to the test for lateral rotatory instability of the knee after ACL rupture. They believed the condition was laxity of the LUCL, which allowed transient rotatory subluxation of the ulnohumeral joint and secondary dislocation of the radiohumeral joint, without radio-ulnar joint dislocation. They recommended repair of the LUCL to eliminate PLRI.
Sanchez-Sotelo et al. retrospectively described 12 cases of direct repair and 33 ligamentous reconstructions for PLRI. 86% were satisfied with the procedure. Better results were obtained with patients with post-traumatic etiology, instability at presentation, and those with augmented reconstruction with tendon graft (compared with ligament repair alone).
Figure A shows structures on the lateral side of the elbow. The corresponding labels are seen in Illustration A. Illustration B shows the lateral pivot shift (also known as the posterolateral rotatory instability test).
Incorrect Answers:
Question 61
- Figures 43a and 43b show the radiographs of an 8-year-old boy who was referred by his gym teacher because of an awkward running pattern. The patient denies any pain in his hips. Examination reveals a mild Trendelenberg gait and decreased internal rotation of the left hip to 25 degrees compared to 40 degrees on the right. What is the most likely diagnosis?
Explanation
Symptoms include-pain, effusion (from synovitis), and a limp, decreased ROM especially Abduction internal rotation. Trendelenburg stance is common.
The key in this question is the age, decreased ROM, Trendelenburg gait. The prognosis is directly related to the age at presentation, after 8 years old the prognosis is poor. SCFE(Slipped Capital Femoral Epiphysis)-Usually seen in obese adolescent boys with a family history. African American more common. Often related to endocrine abnormalities, presenting with externally rotated gait, decreased internal rotation, thigh atrophy, with hip or knee pain, symptoms vary with the acuteness of the slip.
Hypothyroidism is often a finding with patients presenting with SCFE and chondrolysis is a known complication of SCFE.
Question 62
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no

Explanation
Question 63
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
tibial insertion, separated only by the posterior capsule of the knee. When performing
a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation
of the tibial tunnel.
REFERENCES: Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Malek MM, Fanelli GC: Technique of arthroscopically assisted PCL reconstruction. Orthopedics 1993;16:961-966.
Question 64
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
REFERENCES: Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77.
Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
Zwipp H, Tscherne H, Wulker N: Osteosynthesis of dislocated intra-articular calcaneus fractures. Unfallchirurg 1988;91:507-515.
Question 65
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 66
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Explanation
Question 67
A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action?
Explanation
REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 953-954.
Stinchfield FE, Bigliani LU, Neu HC, et al: Late hematogenous infection of total joint replacement. J Bone Joint Surg Am 1980;62:1345-1350.
Question 68
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 69
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 70
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 71
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
Explanation
REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213.
Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.
Early JS, Ricketts DS, Hansen ST: Treatment of compartmental liquefaction as a late sequelae of a lower limb compartment syndrome. J Orthop Trauma 1994;8:445-448.
Question 72
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome? Review Topic
Explanation
(SBQ12SP.35) A 16-year-old male football player is tackled into the ground during a game. He comes to the sideline with unilateral upper extremity pain, burning dysesthesias, and muscle weakness. Several minutes later, his symptoms resolve. In this scenario, what muscles are most likely to be affected? Review Topic
Deltoid and biceps
Triceps
Wrist flexors
Finger flexors
Interossei
This patient presents with a 'burner' or 'stinger,' a transient unilateral neurapraxia that most commonly involves the biceps, deltoid and rotator cuff muscles.
Hypotheses for the mechanism of neurapraxia in stingers include nerve root compression in the neural foramen as a result of extension and compression, traction on the brachial plexus or a direct blow to the plexus. C5-C6 is the most commonly involved level, indicating root injury or upper trunk brachial plexus injury. Unilateral and transient symptoms are required for diagnosis. Bilateral 'stinger' symptoms of numbness, tingling, and weakness are consistent with cervical spinal cord neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine.
Shannon et al. review burner syndrome in athletes. They emphasize that criteria for return to play are based on a complete and thorough neurologic and physical exam. Normal strength and sensation in both upper extremities as well as a normal cervical spine exam (including range of motion, compression, Spurling's, Adson's, and resistive head pressures) are required for return to play. Any positive findings mandate withdrawal of the player from competition.
Illustration A shows hypothesized areas of involvement by mechanism according to
Shannon et al. A, Extension-ipsilateral compression. B, Flexion-contralateral flexion (traction) or direct trauma.
Incorrect Answer Answer Answer
2:
3:
4:
Wrist Finger
Triceps
flexors flexors
C7 C7 C8
Question 73
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 74
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 75
A 68-year-old patient undergoes total knee arthroplasty for end-stage degenerative joint disease. Two years later, she trips and falls at home and sustains a fracture seen in Figures A and B. Before her fall, she was a community ambulator and had no knee pain. The component is determined to be stable and the surgeon decides to treat this fracture with closed reduction and retrograde intramedullary fixation with a supracondylar nail. Which of the following statements is true?

Explanation
Periprosthetic femur fractures above total knee implants occur in 2% of patients. It is important to note: (1) pre-injury function, to determine if the prosthesis was loose, (2) the type of implant (CR vs posterior stabilized, PS) as a PS implant with a closed box would make retrograde intramedullary nailing more difficult (the surgeon has to consider the size of the box vs size of the nail, and if the box is smaller than the nail,
must be prepared to enlarge the box with a metal-cutting burr, which has inherent problems of introducing wear debris into the joint), (3) pre-fracture radiographs help determine the position of the implants (flexion-extension, varus-valgus). These fractures can be treated with non-locking condylar buttress plates (not recommended today), fixed angle devices and intramedullary nailing.
McLaren et al. describe 7 osteopenic patients (mean age, 61yrs, range 47-84yrs) treated with retrograde supracondylar nailing. They suggest not reaming, and placing 2-3 screws in the distal fragment. This may require leaving the nail protruding by 1cm. They then suggest removing the protruding segment with a burr at the end of the procedure.
Haidukewych et al. debate plating vs nailing in a 80yr old osteopenic patient. It may be difficult to introduce retrograde intramedullary nails through the same incision if dense scar tissue is present. On the other hand, most plates require extensive dissection and do not respect the soft tissues and fracture biology, except for LISS plates and nails.
Figures A and B show a displaced Lewis and Rorabeck type II periprosthetic fracture. Illustration A shows the technique of retrograde supracondylar nailing. With the knee flexed, the fracture is reduced and the entry point is in the intercondylar notch. Illustration B shows a comparison between PS and CR implants. Note the "box" in the PS implant. This is absent in the CR implant. Illustration C shows the Lewis and Rorabeck classification.
Incorrect Answers:
1 (at most 2) point of fixation in the distal segment. Answer 5: The backup plan should include devices that resist varus collapse (especially in cases with medial comminution), such as angle-stable devices (ABP, DCS and locking plates). Non-locking condylar buttress plates will not resist varus collapse.
Question 76
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
REFERENCES: Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 77
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?

Explanation
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 78
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?
Explanation
REFERENCE: Nielson JH, Sallis JG, Potter HG, et al: Correlation of interosseous membrane tears to the level of the fibular fracture. J Orthop Trauma 2004;18:68-74.
Question 79
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?
Explanation
REFERENCES: Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Blaha JD: Well-fixed acetabular component retention or replacement: The whys and the wherefores. J Arthroplasty 2002;17:157-161.
Question 80
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 81
There is a risk of impaired forearm rotation after tension band fixation of an olecranon fracture with which of the following?

Explanation
The referenced study by Candal-Couto et al is a cadaveric study that found that K-wire insertion in less than 30 degrees in an ulnar direction led to impingement of the K-wire on the radial head/neck, biceps or supinator. They recommend placing these wires away from this danger zone in order to minimize rotation blocks.
The referenced study by Matthews et al is a case series of two patients who had limited forearm rotation after K-wire fixation. The etiology of limited rotation was found to be from direct overpenetration of the K-wire, which led to a mechanical block.
Question 82
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 83
Which of the following is the strongest contraindication for expansive open door laminoplasty for cervical myelopathy? Review Topic
Explanation
Open door laminoplasty allows decompression direct posterior decompression of the neural elements, as well as an indirect anterior decompression by allowing the cord to drift posteriorly. Posterior drift of the cord relies upon the presence of natural cervical lordosis. In the setting of kyphosis, the cord is tensioned ventrally over the vertebral bodies and discs, and does not have the redundancy to drift backward. Patients without lordosis would therefore be expected to show less post-operative improvement than those with normal cervical curvature.
Chiba et al. performed a retrospective review of patients treated with expansive open door laminoplasty for cervical spondylotic myelopathy (CSM) and ossification of the posterior longitudinal ligament (OPLL). They found that for patients with OPLL, cervical kyphosis was associated with lower recovery rates than those patients with pre-operative lordosis. The authors recommended against posterior decompression for CSM in the setting of OPLL with concomitant cervical kyphosis.
Suda et al. performed a retrospective review of 114 patients who underwent expansive
open door laminoplasty for cervical myelopathy in order to evaluate clinical outcomes and effects on cervical alignment. They found patients with C2-C7 kyphosis >13° had much lower rates of improvement compared with those patients with less kyphosis. The authors suggest an anterior decompression be used for patients with kyphosis greater than 13°, unless kyphotic correction was planned in addition to a laminoplasty.
Illustrations:
Illustration A demonstrates a lateral cervical spine x-ray which shows focal kyphosis at C4-5 and C5-6. Illustration B demonstrates the C7-sagittal vertical axis. Illustration C demonstrates the compression ratio.
Incorrect
<0.4 implies a poor prognosis.
Question 84
A 50-year-old patient underwent multiple débridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
The patient developed a large bone defect after undergoing multiple débridements for an open fracture. The most appropriate graft in this setting is a vascularized bone graft. Considering the length of the defect, a free vascularized fibular graft would be a suitable graft. The indications for a vascularized bone graft include infection, inadequate vascularity of the surrounding tissues, bone defects larger than 6 centimeters, and previous failed bone grafts. The osteocytes survive in the vascularized graft, allowing primary bone healing and thereby limiting a loss of graft strength. In contrast, nonvascularized bone graft heals by creeping substitution with a loss of its initial strength. Calcium sulfate pellets and calcium phosphate cement are synthetic bone substitutes with osteoconductive properties. Their role in fracture healing is limited. Demineralized bone matrix is the matrix remaining after allograft undergoes decalcification processing. These products alone would not be optimal in the treatment of such a large bone defect.
Question 85
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?
Explanation
REFERENCES: Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323.
Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
Kitamura N, Naudie DD, Leung SB, et al: Diagnostic features of pelvic osteolysis on computed tomography: The importance of communication pathways. J Bone Joint Surg Am 2005;87:1542-1550.
Question 86
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
Explanation
REFERENCES: Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475.
McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement: Surgical technique. J Bone Joint Surg Am 2005;87:41-50.
Question 87
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 88
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 89
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time? Review Topic

Explanation
(SBQ13PE.82) A renal ultrasound should be obtained in a patient with which of the following diagnoses? Review Topic
Congenital pseudoarthrosis of the clavicle
Accessory navicular
Congenital scoliosis
Charcot-Marie-Tooth Disease
Congenital curly toe
A renal ultrasound should be obtained in a patient with congenital scoliosis.
Congenitial scoliosis has a prevalence that is estimated at 1% to 4% in general population. It is associated with systemic anomalies in up to 61% of cases. The most common anomalies are cardiac defects, genitourinary defects and spinal cord malformations. As such, additional imaging of these systems should be considered in the initial work-up of these patients.
Ruf et al. retrospectively investigated 56 consecutive operative cases of congenital scoliosis. The average age at surgery was 9.9 years (1.5–17 years). There was one wound complication, 2 hardware failures, 1 revision and no neurological complications. They concluded that one-stage posterior hemivertebra resection and instrumentation was safe in this population.
Xu et al. examined the efficacy of selective partial hemivertebra excision via posterior-only approach in 17 adolescent patients with congenital kyphoscoliosis. There were no postoperative infections and no neurological complications. They concluded that this approach may be most successful in patients aged 9 to 14 years old, with the Risser sign grades from 0–3 and Cobb angles <60°.
Illustration A from Erol et al (UPOJ, Vol 15, 2002;37-42) shows a diagram of 'types' of congenital scoliosis based on the morphology of the vertebrae.
Incorrect Answers:
Question 90
Figures 33a and 33b show the radiographs of a 10-year-old girl who reports a 4-month history of medial foot pain after she was kicked while playing soccer. The pain is worse with activity and partially relieved by rest. Examination reveals tenderness directly over a prominent navicular tuberosity. Management should consist of
Explanation
REFERENCES: Sella EJ, Lawson JP, Ogden JA: The accessory navicular synchondrosis. Clin Orthop 1986;209:280-285.
Bennett GL, Weiner DS, Leighley B: Surgical treatment of symptomatic accessory tarsal navicular. J Pediatr Orthop 1990;10:445-449.
Question 91
Figures 1 and 2 are the radiographs of a 36-year-old man who has had left wrist pain for the past 6 months following a fall onto his outstretched arm. Examination reveals a positive ballottement test, dorsal and ulnar carpal tenderness, and a painful snap with ulnar deviation, pronation, and axial compression. Injury to what ligament is the cause of this patient's pain?
Explanation
The radiographs reveal a volarly tilted lunate on the lateral view (Figure 1) and an incongruous lunotriquetral articulation on the AP gripped view (Figure 2). The patient has what appears to be radiographic findings of volar intercalated segmental instability (VISI), a type of carpal instability, dissociative. An injury to the volar lunotriquetral ligament is the most important contributor to this type of instability. An injury to the dorsal scapholunate ligament typically leads to a dorsal intercalated segmental instability. Isolated injuries to the dorsal radiocarpal ligament and the radioscaphocapitate
ligament do not lead to VISI, although combined injuries may lead to instability between the radius and the proximal row.
Question 92
- Which of the following radiographic findings would be characteristic of the knee joints of a patient with neuropathic osteoarthropathy of the knee?
Explanation
The loss of sensation to the joint is followed by severe degenerative changes, osteophyte formation, articular and subchondral fractures, and often calcification of surrounding soft tissues. In the knee, this is a tricompartmental disease and will not selectively affect one compartment over another.
Question 93
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of
Explanation
open reduction.
REFERENCES: Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocations using traction weight up to 140 pounds. Spine 1993;18:386-390.
Question 94
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)?
Explanation
REFERENCES: Selecky MT, Tibone JE, Yang BY, et al: Glenohumeral joint translation after arthroscopic thermal capsuloplasty of the rotator interval. J Shoulder Elbow Surg 2003;12:139-143.
Harryman DT, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Question 95
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4°F (37.4°C), and examination reveals that abduction of the left hip is limited to 30°. Laboratory studies show a WBC of 11,000/mm 3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
REFERENCE: Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 505-513.
Question 96
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of Review Topic

Explanation
Question 97
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 98
What is an example of cognitive rest after concussion? Review Topic
Explanation
Question 99
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered? Review Topic

Explanation
Question 100
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)? Review Topic
Explanation
