Orthopedic Surgery Board Review MCQs: Spine, Arthroplasty & Trauma | Part 161

Key Takeaway
This page features Part 161 of a comprehensive Orthopedic Surgery Board Review. It offers 100 high-yield, verified MCQs for orthopedic surgeons preparing for their OITE and AAOS certification exams. Covering Arthroplasty, Elbow, Fracture, Hip, and Spine, the interactive quiz provides detailed explanations and flexible learning modes for optimal preparation.
About This Board Review Set
This is Part 161 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 161
This module focuses heavily on: Arthroplasty, Elbow, Fracture, Hip, Spine.
Sample Questions from This Set
Sample Question 1: A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?...
Sample Question 2: Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry a...
Sample Question 3: A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The pati...
Sample Question 4: Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?...
Sample Question 5: For halo traction, what is the preferred site for anterior pin placement?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?
Explanation
REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 2
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 3
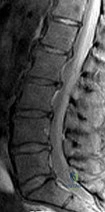
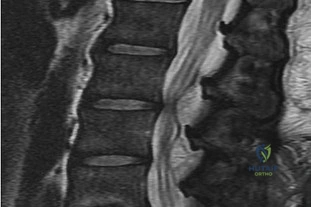
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5 out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in both lower extremities. The patient is slow in getting up from a seated position and has an unsteady wide-based gait. An MRI scan of the lumbar spine is shown in Figure 1. What is the next most appropriate course of action? Review Topic
Explanation
(SBQ12SP.92) A 36-year-old man presents to the emergency department after being involved in a motor vehicle collision. He is complaining of back pain and imaging shows the findings in Figure A. On neurological examination, he does not have any deficits. MRI shows approximately 25% canal encroachment and no evidence of injury to the posterior ligamentous complex. Which of the following is the most appropriate course in management? Review Topic

Strict bedrest for six weeks then progressive weightbearing
Ambulation as tolerated with or without a TLSO
Surgical decompression and anterior stabilization
Surgical decompression and posterior stabilization
Surgical decompression and combined anterior/posterior stabilization
The patient has a L1 burst fracture with minimal retropulsion of bony fragments in the spinal canal. In the absence of neurological deficits and injury to the PLC, the most
appropriate treatment is ambulation as tolerated with or without a thoracolumbrosacral orthosis (TLSO).
Thoracolumbar burst fractures are typically caused by an axial load with flexion and commonly found in this location due to increased motion at these segments. With an intact posterior ligamentous complex (PLC) and no neural compromise, TLSO is the mainstay of treatment. If there is evidence of neurological deficit and/or PLC injury, decompression and fusion are indicated. The degree of acceptable kyphosis is controversial. The choice of anterior versus posterior approach is based on ease of decompression.
Vaccaro et al. introduced a new classification system for thoracolumbar injuries, TLICS, based on morphological appearance, integrity of the posterior ligamentous complex, and neurological status. They advocate use of the system for nonoperative versus operative decision making and communication between surgeons.
Bailey et al. completed a randomized, nonblinded controlled trial to determine the efficacy of bracing for AO type A0-A3 thoracolumbar burst fractures. Both groups were encouraged to ambulate as tolerated and the no brace group had bending restrictions for 8 weeks. They found no difference in the Roland Morris Disability Questionnaire (RMDQ) score at 3 months after injury.
Figure A is sagittal CT scan of the lumbar spine showing a burst fracture of L1 with minimal retropulsion. Illustration A is the TLICS classification with score of 4 being the branch point for nonoperative versus operative management.
Incorrect Answers:
Question 4
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
Explanation
REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.
Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 5
For halo traction, what is the preferred site for anterior pin placement?
Explanation
REFERENCE: Ebraheim NA, Lu J, Biyani A, Brown JA: Anatomic considerations of halo pin placement. Am J Orthop 1996;25:754-756.
Question 6
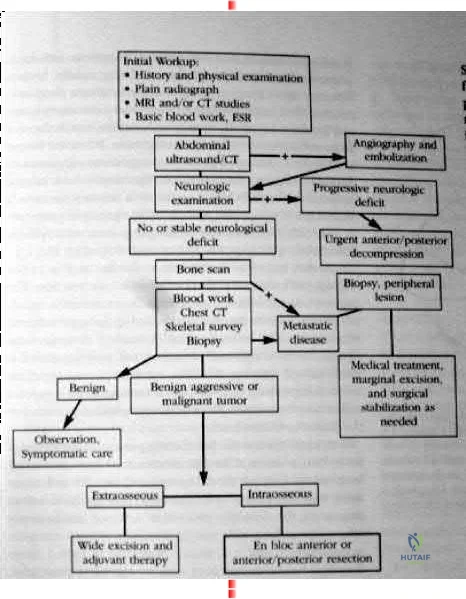
maximize physical capacity and 4) obtain local control of the disease. Other trivia from the references include: After the lung and liver the skeletal system is the third most common site of metastasis. The spine is the most common site of skeletal metastasis. 60% of all skeletal lesions and 36% are asymptomatic. Breast, prostate, lung and renal carcinoma comprise 80% of the carcinomatous skeletal metastasis. 70% metastasis occur in the thoracic and thoracolumbar regions. 21% had involvement of the lumbar and sacral regions. 8% involved the cervical and cervicothoracic regions together. As many as 90% of patients who die of cancer may have Spinal metastasis at autopsy, and only half of patients who die from cancer will have symptoms from spinal mets. Fewer than 10% with spinal mets are treated surgically. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL., American academy of orthopaedic surgeons, 2002, pp 723-736. back to this question next question 03 What is the most frequently encountered complication following juvenile hallux valgus correction?
Explanation

Coglin’s referenced paper is a study out of Idaho. 11 year retrospective study of 45 patients (60 feet). A multiprocedural approach was used to surgically correct the deformity. There were 6 recurrences of the deformities and eight
complications (6 cases of hallux varus, one case of wire breakage and one case of undercorrection.) So according to their reference this question has two correct answers.

Postoperative complications have been frequently reported following juvenile hallux valgus corrections. Recurrence following surgery is probably the most frequently reported complication and is likely due to the high rate of congruency associated with a juvenile hallux valgus deformity.

OKU Foot and Ankle 2 Rosemont IL., American academy of orthopaedic surgeons, pp135-150.
back to this question next question
Question 7
A concern when choosing irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene rather than lower dose–irradiated (4 Mrad) polyethylene is related to its inferior resistance to
Explanation
The higher the dose of radiation to the polyethylene, the higher the amount of cross-linking. Adhesive and abrasive wear resistance increases with an increase in cross-linking. However, fatigue properties of the material are decreased when polyethylene is melted (to remove free radicals) during the cross-linking process. Creep (deformation without wear) is also slightly increased with cross-linking of polyethylene.
Question 8
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 9
Which of the following enzymes is used to resorb bone by mature osteoclasts?
Explanation
Question 10
Figures 48a and 48b are the initial radiograph and clinical photograph of a 21-year-old woman who sustained a severe mangling injury to her left foot in a rollover ATV crash. After multiple dTbridements, she underwent definitive transmetatarsal amputation with split-thickness skin graft. She did have intact plantar sensation. Figure 48c shows the clinical photograph 10 days after amputation. Her wounds healed without infection and she did not require further surgery. At 2 years after injury, which of these factors is most likely to be associated with improved level of satisfaction? Review Topic

Explanation
and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
(SBQ12TR.26) A 44-year-old male presents after being struck by a car. He is hypotensive, and has an obvious open tibia and a closed femoral shaft fracture. A pelvic radiograph is obtained and shown in Figure A. A representative CT scan image in shown in Figure B. The patient is placed in a pelvic binder, and his blood pressure normalizes with crystalloid and a blood transfusion. He then undergoes pelvic angiography, and his internal iliac artery is embolized. Which of the following definitive treatment options is most appropriate in this case? Review Topic
Anterior pelvic external fixation with pins placed in the AIIS and a posterior sacroiliac screw
Open reduction and internal fixation of the pubic symphysis with a two hole plate and posterior fixation with a iliosacral screw
Open reduction and internal fixation of the pubic symphysis with a non-locking multi-hole plate and posterior fixation with a iliosacral screw
Anterior pelvic external fixation and posterior triangular osteosynthesis
Open reduction and internal fixation of the pubic symphysis with a locked multi-hole plate and posterior sacral plate fixation
The radiographs and CT scan show a fracture pattern consistent with an APC-III injury. This is most appropriately treated with pubic symphysis ORIF with a multi-hole plate and posterior iliosacral screw fixation.
APC-III pelvic ring injuries are associated with with disruption of the anterior and posterior SI ligaments (SI dislocation) as well as disruption of sacrospinous and sacrotuberous ligaments. They are commonly associated with vascular injury and retroperitoneal bleeding.
Sagi et al studied the radiographic and clinical outcome of symphyseal plating techniques, specifically comparing two hole (THP) vs multi-hole plating (MHP). Retrospective review of charts and radiographs immediately after the index procedure to latest follow-up was performed. When comparing the 2 different methods of anterior fixation, they found that the rate of fixation failure was greater in group THP (33%) than group MHP (12%). When evaluating the presence of a malunion as a result of these 2 treatment methods, there were more present in the THP group (57%) than in the MHP group (15%). On the basis of these findings, the authors recommended multi-hole plating of unstable pubic symphyseal disruptions.
Grimshaw et al performed a biomechanical study to determine the failure risk and potential benefit to use of locked fixation constructs in simulated pelvic ring injuries. The authors used a six-hole 3.5-mm plate specifically designed for the symphysis pubis with the capability of fixation in locked or unlocked mode, six pelves were fixed with locked screws and six pelves were fixed standard unlocked bicortical screws. Biomechanical testing was performed, and no abrupt failures were noted. However, locked plating of the pubic symphysis did not appear to offer any advantage over the standard unlocked technique
Illustrations A, B, and C show the AP, outlet, and inlet postoperative radiographs. Incorrect Answers:
1,4-Anterior pelvic fixation is typically not used as definitive treatment of these
injuries unless performed in a damage-control setting. The patient in this case is stable.
2-Multi-hole plate fixation of the pubic symphysis is preferred over 2-hole plate fixation.
5-Posterior sacral plating is not indicated in this fracture pattern, as there is no significant sacral comminution of vertical shear component. Furthermore, no distinct advantage has been found with locked symphyseal plating.
Question 11
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Ring D, Jupiter J, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
Question 12
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
REFERENCES: Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000.
Question 13
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
Explanation
REFERENCES: Kreig JC, Mohr M, Ellis TJ, et al: Emergent stabilization of pelvic ring injuries by controlled circumferential compression: A clinical trial. J Trauma 2005;59:659-664.
Croce MA, Magnotti LJ, Savage SA, et al: Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg 2007;204:935-942.
Routt ML Jr, Falicov A, Woodhouse E, et al: Circumferential pelvic antishock sheeting:
A temporary resuscitation aid. J Orthop Trauma 2002;16:45-48.
Question 14
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of
Explanation
REFERENCES: Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Lawrence SJ, Botte MJ: Jones’ fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.
Question 15
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew Eikenella corrodens . The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?

Explanation
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection and not a tumor, and MRI already has provided enough diagnostic information.
Question 16
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 17
Figure 1 shows the radiograph obtained from a 67-year-old man recently diagnosed with osteoarthritis, 8 years after receiving a left metal-on-metal total hip arthroplasty (THA). The acetabular component has a modular cobalt alloy acetabular liner. The patient states that he did very well postoperatively, but for the last 6 months has noted worsening pain and swelling in his left hip. Serum metal ion testing reveals a chromium level of 12.4 ng/mL, compared with a normal level of less than 0.3 ng/mL, and a cobalt level of 11.8 ng/mL, compared with a normal level less than 0.7 ng/mL. An MRI with metal artefact reduction sequence (MARS) was performed and is shown in Figure 2. What is the most appropriate management at this time?

Explanation
Metal-on-metal THA was initially introduced in the 1990s, with the proposed advantages of decreased wear and improved stability. However, catastrophic adverse local tissue reactions associated with their use has raised numerous concerns. The work-up of a patient with a prior metal-on-metal total hip arthroplasty involves a thorough history and physical examination; blood analysis, including the erythrocyte sedimentation rate, C-reactive protein, and metal ion levels; and secondary imaging, including ultrasonography, CT, and MRI. In a patient with clinical symptoms, elevated metal ion levels, and a large fluid collection seen on MRI, the most appropriate treatment would be removal of the metal-on-metal bearing. Given the presence of an adverse reaction involving cobalt and chromium, a revision ceramic head may be most appropriate to avoid the potential of trunnion-associated corrosion.
Question 18
Which of the following findings is seen in the chest radiograph shown in Figure 13?
Explanation
REFERENCE: Bone LB: Emergency treatment of the injured patient, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 133-138.
Question 19
Which of the following alternatives to autogenous bone grafting functions through osteoinduction?
Explanation
Question 20
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 21
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 22
During a dual incision fasciotomy of the leg, the soleus is elevated from the tibia to allow access to which of the following compartments?

Explanation
Question 23
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 24
A 64-year-old female sustains a nondisplaced distal radius fracture and undergoes closed treatment using a cast. Three months after the fracture she reports an acute loss of her ability to extend her thumb. What is the most likely etiology of her new loss of function?

Explanation
Question 25
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of
Explanation
REFERENCES: Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 26
A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of
Explanation
REFERENCES: Wall E, Von Stein D: Juvenile osteochondritis dissecans. Orthop Clin North Am 2003;34:341-353.
Kocher MS, Micheli LJ, Yaniv M, et al: Functional and radiographic outcome of juvenile osteochondritis dissecans of the knee treated with transarticular arthroscopic drilling.
Am J Sports Med 2001;29:562-566.
Question 27
A 35-year-old woman is involved in a head-on collision while driving. Initial radiographs are shown in Figures 8a and 8b. Injury to what vessel increases the risk for osteonecrosis of the injured bone?

Explanation
Question 28
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common source of surgical failure?
Explanation
Question 29
Treatment should include
Explanation
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.

Question 30
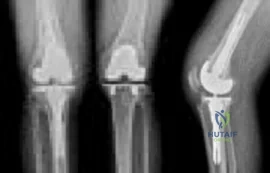
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 31
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
Question 32
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
REFERENCES: Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Barrack RL, Matzkin E, Ingraham R, Engh G, Rorabeck C: Revision knee arthroplasty with patella replacement versus bony shell. Clin Orthop 1998;356:139-143.
Question 33
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent
Explanation
Question 34
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well-fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help with tibial component extraction.
Question 35
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?
Explanation
REFERENCES: Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Mirra, JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989.
Question 36
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 37
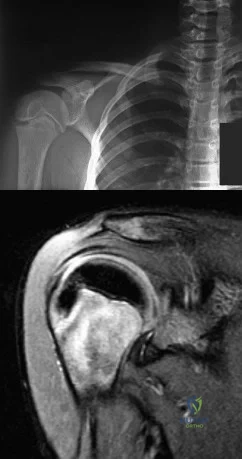
Figure 1 is the T2 coronal MRI scan of a 52-year-old woman with a 6- month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
Question 38
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
REFERENCES: Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2001;83:661-667.
Question 39
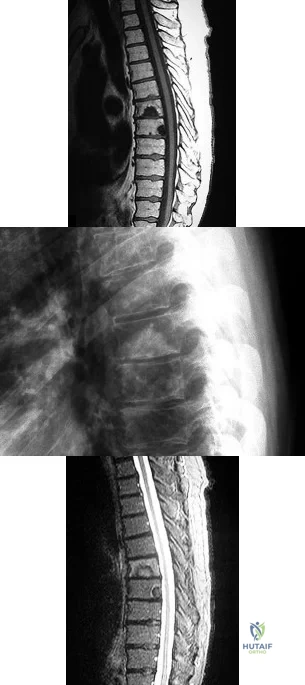
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 40
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 41
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
REFERENCES: Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Perron AD: Chest pain in athletes. Clin Sports Med 2003;22:37-50.
Question 42
A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?
Explanation
REFERENCES: Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Weigelt JA: Resuscitation and initial management. Crit Care Clin 1993;9:657-671.
Question 43
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520.
Question 44
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Explanation
Question 45
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 46
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 47
Figures 51a and 51b show the radiographs of a 12-year-old boy obtained after an attempted closed reduction of an elbow injury in the emergency department. His motor examination is intact but he reports decreased sensation along the palmar aspect of his ring and little finger. What is the best treatment plan? Review Topic

Explanation
(SBQ13PE.97) A 3-year-old boy presents to your office for evaluation. On physical examination, the patient has large calves and uses his hands to assist in rising from the floor. Laboratory results from the pediatrician reports notably high creatinine kinase of 43000 IU/L. What is the most likely inheritance pattern? Review Topic
Autosomal recessive
Autosomal dominant
X-linked recessive
X-linked dominant
Mitochondrial inheritance
Duchenne's muscular dystrophy (DMD) has an X-linked recessive inheritance pattern.
Duchenne's muscular dystrophy is characterized by a lack of dystrophin on muscle biopsy. Gower's sign is a typical physical exam finding (child uses hands to assist in rising from sitting), along with pseudohypertrophy of the calves. Notable laboratory values include elevated creatinine kinase (CK), typically above 25,000 IU/L.
Sussman et al. provide a comprehensive review of DMD, highlighting characteristic findings, including pseudohypertrophy of the calves (due to replacement of skeletal muscle with adipose tissue), Gower's sign, as well as CK levels typically above 25,000 IU/L. CK levels can aid in distinguishing between Becker's dystrophy which has levels less than 25,000 IU/L.
Figure A exhibits a muscle biopsy (calf) at low power of DMD; note the replacement of muscle with adipose tissue.
Incorrect answers:
(SBQ13PE.47) Figure A shows an ultrasound of a 2 week old infant being evaluated for developmental dysplasia of the hip. Which of the labels depict the alpha angle, and what anatomic landmarks define this angle? Review Topic
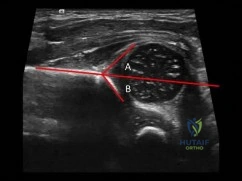
Angle A, ilium and cartilaginous acetabulum
Angle A, ilium and bony acetabulum
Angle B, ilium and cartilaginous acetabulum
Angle B, ilium and bony acetabulum
Angle B, bony acetabulum and acetabular labrum
The alpha angle is subtended by (1) a line drawn down the ilium to a point where it intersects with the bony and cartilaginous confluence of the acetabulum and (2) a line drawn along the roof of the bony acetabulum.
The coronal flexion view (as depicted in figure A) of the infant hip is perhaps more familiar if rotated 90 degrees to view as one would view an anterior posterior radiograph of the pelvis. Acetabular development is evaluated primarily by the alpha angle, indicating the morphology of the developing acetabulum, and the percentage of the femoral head that is covered by the bony acetabulum. These are each readily apparent on ultrasound. Normal hips should have an alpha angle of at least 60 degrees by 6-8 weeks of age.
Harcke et al. provide a current concepts review on the state of ultrasound in the diagnosis and management of developmental dysplasia of the hip (as of 1991). They report, since that time, ultrasound has become the mainstay for diagnostic confirmation and management of DDH.
LeBa et al. performed a study to look at whether ultrasound screening would increase in effectiveness if targeted toward infants with established risk factors for developmental dysplasia of the hip and normal findings on physical examination. They found dynamic ultrasound evaluation showed developmental dysplasia in 7.8% of patients who had normal physical exams and led to a change in treatment in 8%. They conclude selective ultrasound screening in infants with risk factors and normal
findings on physical examination is effective and leads to more effective treatment.
Figure A shows an ultrasound exam of a 2 week old infant. The alpha angle is labeled 'B'. The beta angle is lableled 'A'. Illustration A is a diagram from Tachdjian's illustrating diagrammatically the elements of these angles.
Incorrect answers.
Question 48
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 49
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 50
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 51
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings. Which of the following has been shown to decrease the risk of developing this complication?

Explanation
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to
lower infection rates). Most encouraged shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Question 52
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 53
A 3-year-old child is referred for evaluation of bowed legs. History reveals no dietary deficiencies; however, family history is significant for several members with bowed legs. Examination reveals genu varum, and the child is in the 5th percentile for height and weight. Laboratory studies show normal renal function, a normal calcium level, a decreased phosphate level, and an elevated alkaline phosphatase level. A plain radiograph of the lower extremities is shown in Figure 22. What is the most likely diagnosis?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Loeffler RD Jr, Sherman FC: The effect of treatment on growth and deformity in hypophosphatemic vitamin D-resistant rickets. Clin Orthop 1982;162:4-10.
Loder RT, Johnston CE II: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Bassett GS, Scott CI: The osteochondrodysplasias, in Morrissy RT (ed): Pediatric Orthopaedics, ed 3. Philadelphia, Pa, JB Lippincott, 1990, vol 1, pp 91-142.
Question 54
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
Explanation
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 55
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 56
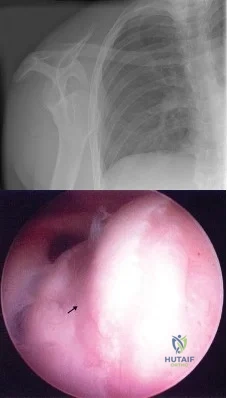
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
REFERENCES: Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 57
The mangled extremity severity score (MESS) utilizes all of the following variables EXCEPT:

Explanation
The scoring system is as follows: 1. Skeletal / soft-tissue injury: Low energy = 1; Medium energy = 2; High energy = 3; very high energy = 4; 2. Limb ischemia: Pulse reduced or absent but perfusion normal = 1; Pulseless = 2; Cool, paralyzed, insensate = 3; 3. Shock: normotensive = 0; transient hypotension = 1; persistent hypotension = 2; 4. Age:
< 30 = 0; 30-50 = 1; >50 = 2. Limb category scores are doubled for ischemia > 6 hours. The system's original designers reported a cutoff of 7 as predicting amputation.
The referenced study by Ly et al found that the scoring system did not predict functional outcomes at 6 or 24 months. They also found that the Limb Salvage Index; the Predictive Salvage Index; the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score; and the Hannover Fracture Scale-98 all did not predict outcomes at 6 or 24 months.
Question 58
A 6-month-old child has the deformity seen in Figure 10. There are no other known associated problems. What is the etiology of this condition? Review Topic

Explanation
Question 59
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 60
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 61
Rupture of the distal biceps tendon is predictably identified by the hook test, which is performed by bringing a finger from lateral to medial across the antecubital fossa of a flexed elbow, feeling for a cord-like structure on which the examiner can "hook" a finger. Bringing the finger from medial to lateral can cause a false-negative result, hooking the lacertus fibrosus, which can remain intact even with a ruptured distal biceps tendon. The Yergason test (option 3) and the Speed test (option 4) are used to assist in diagnosing proximal, not distal, biceps and labral pathology. Even if the distal biceps tendon is ruptured, the supinator remains intact. Although supination weakness may be present, an inability to supinate should not be observed. When treating a closed long finger central slip tendon rupture conservatively, what is the most appropriate plan of care?
Explanation
Closed central slip injuries treated nonsurgically require extension splinting of the PIP joint. DIP joint active range of motion is allowed during this time period. This allows the connections between the lateral bands and the central slip to pull the central slip distally with DIP joint active motion, minimizing the gap
across the central tendon injury and keeping the DIP joint from getting stiff as well.
Question 62
What is the most common causative bacteria in septic arthritis in children? Review Topic
Explanation
Question 63
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
REFERENCES: McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654.
Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study.
J Bone Joint Surg Am 2003;85:773-781.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 64
Figure 28 is the lateral radiograph of a patient who sustained an intraarticular fracture of the calcaneus. The structure (*) depicted by the arrows most likely represents which osseous component of the calcaneus?

Explanation
Question 65
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 66
The subcutaneous nerve most at risk for transection during an anterior surgical exposure of the ankle is the
Explanation
The dorsal medial cutaneous nerve arising from the superficial peroneal nerve crosses the inferior extent of a routine extensile surgical exposure to the ankle joint. The extensile anterior incision develops the interval between the tibialis anterior and extensor hallucis tendons, and, although the deep peroneal nerve is lateral and posterior to the extensor hallucis longus, the nerve most at risk during this exposure is the cutaneous branch supplying the dorsal medial foot to the great toe. Ankle replacement surgery is becoming more common; consequently, surgeons must be familiar with this anatomic landmark and risks related to its transection during surgery.
The medial plantar nerve is at risk when medial hindfoot incisions are made through the
abductor hallucis muscle during tarsal tunnel release and harvest of the flexor hallucis tendon for transfer. The dorsal cutaneous branch of the sural nerve supplies the lateral dorsal
Question 67
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
Question 68
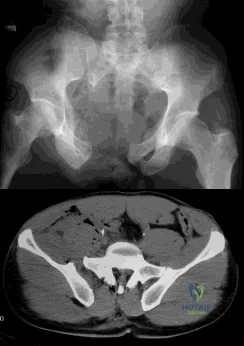
A B C What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
Explanation
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. View Abstract at PubMed
Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. View Abstract at PubMed
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29

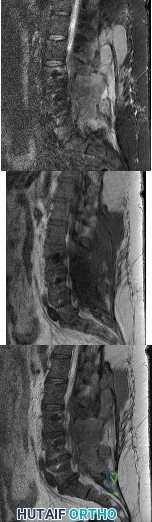
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
Question 69
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 70
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 71
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?
Explanation
REFERENCES: Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
Malhotra R, Singh KD, Bhan S, Dave PK: Primary pyogenic abscess of the psoas muscle. J Bone Joint Surg Am 1992;74:278-284.
Question 72
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-17, 4-18.
Question 73
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a Review Topic
Explanation
Question 74
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 75
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.
Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.
Question 76
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
REFERENCES: White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508.
Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Choi YS, Lee SM, Song BY, et al: Dynamic sonography of external snapping hip syndrome.
J Ultrasound Med 2002;21:753-758.
Question 77
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 78
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 79
An active 23-year-old man has right groin pain that increases with sports activity. Examination reveals decreased internal rotation of the affected hip. He has a positive impingement test and radiographs reveal no crossover sign. An MRI scan is most likely to reveal which of the following? Review Topic
Explanation
Question 80
During right knee anterior cruciate ligament (ACL) reconstruction, after drilling an appropriately positioned and referenced tibial tunnel, the surgeon finds that the transtibial guide is placing the femoral tunnel at 11:30 within the intercondylar notch. Which of the following choices will best enable appropriate graft placement in this clinical scenario? Review Topic
Explanation
minimize errant tunnel placement, demonstrated in the literature as the most common cause of ACL failure and need for revision. In this not uncommon clinical scenario, simply converting to a two-incision ACL technique or drilling through the anteromedial portal with the knee hyperflexed will permit accurate femoral tunnel placement and increase the likelihood of an optimal clinical outcome. Femoral tunnel accuracy with these techniques is enhanced by a lower starting point in the intercondylar notch. Familiarity with these techniques is valuable for surgeons performing ACL reconstruction. Revising the tibial tunnel in this scenario would likely lead to bone compromise of the proximal tibia and may interfere with graft fixation and incorporation. Converting to a double-bundle ACL with a transtibial technique would not correct the vertical femoral tunnel. Hyperflexion of the knee may improve femoral tunnel placement to some extent, but is unlikely to allow anatomic placement of a femoral tunnel when the transtibial guide lies in a clearly excessive vertical position.
Question 81
An MRI scan
Explanation
Question 82
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
REFERENCES: Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44.
Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 83
When do most symptomatic thromboembolic events occur after total joint arthroplasty?
Explanation
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events.
Question 84
What portion of the pitching phase creates forces approaching the tensile limit of the medial ulnar collateral ligament of the elbow? Review Topic
Explanation
Fleisig et al. were among the first to elucidate the elbow and shoulder kinetics in healthy adult pitchers using high-speed motion capture analysis. Inability to generate sufficient elbow varus torque may result in medial tension, lateral compression, or posteromedial impingement injury.
According to Lynch et al. the late cocking phase of the overhand throw places a marked valgus moment across the medial elbow. This repetitive force reaches the tensile limits of the medial collateral ligament, subjecting it to microtraumatic injury and attenuation. The anterior bundle of the medial collateral ligament has been identified as the primary restraint to valgus load and is the focus of reconstruction.
Incorrect Responses:
1,4,5: The medial elbow forces are less during these phases. 4: Ball release is not one of the 5 phases of throwing and marks the end of the acceleration and beginning of deceleration phase.
Question 85
Surgical arthroscopy performed 1 week after injury presents increased risk for
Explanation
The MR images show injuries to the ACL, PCL, and PLC consistent with a knee dislocation. The optimal timing of surgery after multiligament knee injury remains unclear. Two systematic reviews demonstrated superior clinical outcome scores after early treatment, including higher mean Lysholm scores and a higher percentage of good/excellent International
Knee Documentation Committee scores. Early treatment was associated with increased residual anterior knee instability but no difference in posterior instability, varus laxity, or valgus laxity. Although numbers were limited, the average range of motion and rate of extension loss of at least 5 degrees was similar between groups. More patients in the early-treatment group demonstrated a higher rate of flexion loss of 10 or more degrees and an increased need to undergo a second procedure to address arthrofibrosis, including manipulation under anesthesia and arthrolysis. Return to work did not significantly differ between groups, but return to sports was lower in the early-treatment group. Evidence demonstrates a higher rate of low-energy mechanisms resulting in multiligament knee injury and an increased odds ratio for complications among obese (= 30 degrees kg/m2 patients, including wound complications and neurovascular injury. The complication rate increased 9.2% for every 1-point increase in body mass index. There is no association between complication rate and age, injury mechanism, or timing of surgery. Orthopaedic surgeons performing arthroscopy during the early postinjury period must be mindful of the extensive soft-tissue damage present in these patients, including potential capsular defects. Use of high-pressure irrigation can lead to substantial fluid extravasation into the thigh or lower leg compartments, placing patients at increased risk for compartment syndrome. In addition to avoiding high-pressure irrigation, some orthopaedic surgeons have advocated the creation of generous capsular incisions during portal establishment to allow for ready egress of irrigation fluid from the portal sites rather than into soft tissues.
RESPONSES FOR QUESTIONS 85 THROUGH 88
Excessive medial placement of coracoid autograft
Excessive lateral placement of coracoid autograft
Excessive inferior dissection during the procedure
Excessive retraction and dissection of the medial portion of the conjoint tendon
A 20-year-old right-hand-dominant football player sustained a traumatic shoulder dislocation during a tackle. He has had multiple recurrent dislocations, and radiographs reveal anterior glenoid bone loss. He underwent a Latarjet procedure. Match the most likely complication described below with the surgical error listed above.
Question 86
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?
Explanation
are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Wang XL, De Schepper AM, Vanhoenacker F, et al: Nodular fasciitis: Correlation of MRI findings and histopathology. Skeletal Radiol 2002;31;155-161.
Question 87
What genetic defect is responsible for achondroplasia? Review Topic
Explanation
Question 88
Which of the following best describes athletic pubalgia?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 89
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
REFERENCES: Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423.
Question 90
Linazolid exerts its antimicrobial action by inhibiting bacterial
Explanation
REFERENCES: Rybak MJ, Cappelletty DM, Moldovan T, et al: Comparative in vitro activities and postantibiotic effects of the oxazolidinone compounds eperezolid (PNU-100592) and linezolid (PNU-100766) versus vancomycin against Staphylococcus aureus, coagulase-negative staphylococci, Enterococcus faecalis, and Enterococcus faecium. Antimicrob Agents Chemother 1998;42:721-724.
Sweeney MT, Zurenko GE: In vitro activities of linezolid combined with other antimicrobial agents against Staphylococci, Enterococci, Pneumococci, and selected gram-negative organisms. Antimicrob Agents Chemother 2003;47:1902-1906.
Question 91
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129.
Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Thompson JE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309-316.
Question 92
To prevent injury to the posterior interosseous nerve during the approach for reduction and fixation of a fracture of the radial head, anterior retraction should be performed with the forearm
Explanation
Deep surgical dissection-Fully pronate the forearm to move the posterior interosseous nerve away from the operative field. Incise the capsule of the elbow joint longitudinally to reveal the underlying capitulum, the radial head, and the annular ligament. Do not incise the capsule too far anteriorly; the radial nerve runs over the front of the anterolateral portion of the elbow capsule. Do not continue their dissection below the annular ligament or retract vigorously, distally, or anteriorly, because the posterior interosseous nerve lies within the substance of the supinator muscle and is vunerable to injury.
Dangers: Nerves-The posterior interosseous nerve is in no danger as long as the dissection remains proximal to the annular ligament. Pronation of the forearm keeps the nerve as far from the operative field as it possible can be. To ensure the safety of the nerve, take great care to place the retractors directly on the bone and be careful in their placement. Because the posterior interosseous nerve actually may touch the bone of the radial neck, directly opposite the bicipital tuberosity, placing retractors behind it poses a risk.
Question 93
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
Explanation
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.

CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Question 94
Which of the following statements best describes the typical early presentation of osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 95
below show the radiographs, and the CT obtained from a year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 96
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 97
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 98
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 99
Increased hip intracapusular pressures can lead to diminished femoral head perfusion. What leg position has been shown to create the lowest intracapsular hip pressures after femoral neck fracture?

Explanation
Question 100
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
