Orthopedic Board Review MCQs: Knee, Shoulder, Trauma & Infection | Part 159

Key Takeaway
This page offers Part 159 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs in exam format. Designed for orthopedic residents and surgeons, this quiz helps master topics like dislocations, fractures, and knee/shoulder pathologies for certification success.
About This Board Review Set
This is Part 159 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 159
This module focuses heavily on: Dislocation, Fracture, Infection, Knee, Shoulder.
Sample Questions from This Set
Sample Question 1: A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?...
Sample Question 2: A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination ...
Sample Question 3: A 32-year-old patient reports progressively increasing pain and stiffness after undergoing arthroscopic shoulder stabilization 1 year ago. The stabilization procedure was a Bankart repair with anchor fixation and supplemented with the heat ...
Sample Question 4: What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?...
Sample Question 5: A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
Question 2
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of
Explanation
REFERENCES: Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
Mendez AA, Keret D, MacEwen GD: Treatment of patellofemoral instability in Down’s syndrome. Clin Orthop 1988;234:148-158.
Question 3
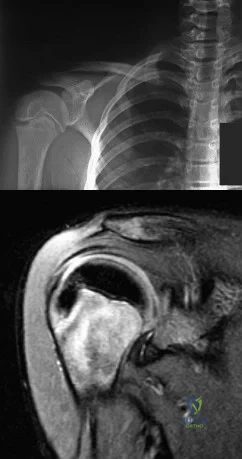
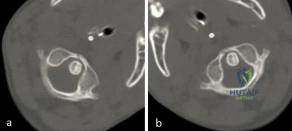
A 32-year-old patient reports progressively increasing pain and stiffness after undergoing arthroscopic shoulder stabilization 1 year ago. The stabilization procedure was a Bankart repair with anchor fixation and supplemented with the heat probe. Radiographs are shown in Figures 45a and 45b. What is the most likely diagnosis?
Explanation
REFERENCES: Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Petty DH, Jazrawi LM, Estrada LS, et al: Glenohumeral chondrolysis after shoulder arthroscopy: Case reports and review of the literature. Am J Sports Med 2004;32:509-515.
Question 4
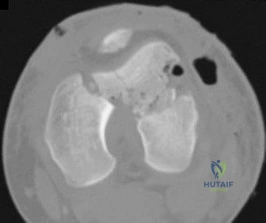
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 5
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
Explanation
REFERENCES: Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Beals RK, Bryant RE: The treatment of chronic open osteomyelitis of the tibia in adults.
Clin Orthop Relat Res 2005;433:212-217.
Question 6
What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates? Review Topic
Explanation
Question 7
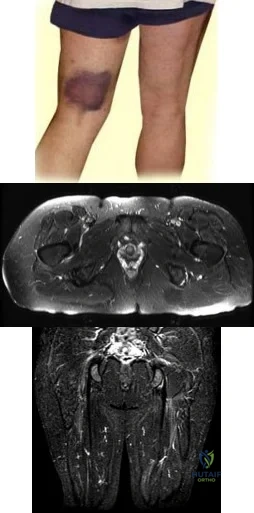
Figures 24a through 24c show the coronal T 1 -weighted, T 2 -weighted fat-saturated, and T 1 -weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCE: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 8
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
REFERENCES: Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000.
Question 9
A 35-year-old male has a closed mid-shaft tibia fracture following a skiing accident. You have recommended intramedullary nailing of the tibia. What is the most common complication he must be advised about?

Explanation
Question 10
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?
Explanation
REFERENCES: Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3.
Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Fountas KN, Kapsalaki EZ, Karampelas I, et al: Results of long-term follow-up in patients undergoing anterior screw fixation for type II and rostral type III odontoid fractures. Spine 2005;30:661-669.
Question 11
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. What is an acceptable arrangement to learn more about this system?
Explanation
Question 12
All of the following have been shown to negatively affect clinical outcomes in treating displaced acetabular fractures, EXCEPT:

Explanation
The referenced study by Matta evaluated outcomes of displaced acetabular fractures. The overall clinical result was excellent for 104 hips (40 per cent), good for ninety-five (36 per cent), fair for twenty-one (8 per cent), and poor for forty-two (16 per cent). The clinical result was related closely to the radiographic result. These findings indicate that in many patients who have a complex acetabular fracture the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 13
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
Explanation
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
Question 14
A college athlete has a knee injury requiring surgery. He has acne, gynecomastia, and well-developed muscles related to the use of anabolic steroids. What association with steroid use is concerning for surgery and anesthesia?
Explanation
REFERENCES: Kam PC, Yarrow M: Anabolic steroid abuse: Physiological and anesthetic considerations. Anaesthesia 2005;60:685-692.
Ansell JE, Tiarks C, Fairchild VK: Coagulation abnormalities associated with the use of anabolic steroids. Am Heart J 1993;125:367-371.

Question 15
Figure 19 is the clinical photograph of a 54-year-old man who underwent a total ankle replacement (TAR). Three weeks after surgery he has increasing pain and a deep wound as seen in the photograph. What is the best next step?

Explanation
The patient is 3 weeks out from TAR. The wound is erythematous, and the tendon is visible. At 3 weeks this is an acute wound breakdown. The preferred treatment is a return to the operating room, an exchange of the polyethylene because the wound appears deep enough to go down to the joint, and a flap for coverage. Removal of the total ankle and placement of an antibiotic spacer should be considered in the settings of subacute (6 weeks postop) or chronic infection following TAR. A below-the-knee amputation may be considered with a failed salvage or a chronically infected TAR. Conversion to a fusion may be considered in situations in which the wound bed is not infected. In this case, there is concern for ongoing active infection, and an intercalary allograft is not appropriate.
RECOMMENDED READINGS
Cho EH, Garcia R, Pien I, Thomas S, Levin LS, Hollenbeck ST. An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle. Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. PubMed PMID:
Question 16
Which of the following statements best describes synovial fluid?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 443-470.
Question 17
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient’s neurologic recovery can be best determined by
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1185-1194.
Question 18
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 19
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
Question 20
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, plate 4-46.
Question 21
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 22
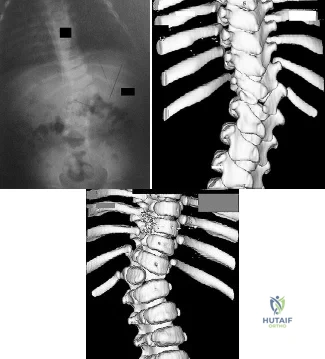
A 39-year-old male falls off his bicycle and complains of neck pain and tingling in his fingers. Trauma series radiographs are seen in Figures A and B. Which of the following is likely to be true? Review Topic

Explanation
Cervical spine fractures are not uncommon in ankylosing spondylitis because of osteoporosis and the long lever arm from fused vertebrae. They commonly occur because of hyperextension of the cervical spine (usually C5-7) and have a high rate of neurologic injury. AS fractures have a higher rate of neurologic injury than DISH fractures. Posterior decompression and stabilization with long constructs is necessary
Whang et al. reviewed spine injuries in 12 patients with AS and 18 patients with DISH. Most injuries involved C5-C7. Patients with AS were more likely to have severe neurologic injury (41% ASIA A) than DISH (44% ASIA E). There was 81% good-excellent outcome and 4 deaths related to halo vest use.
Caron et al. reviewed spine fractures in patients with ankylosing spine disorders (AS and DISH). AS patients were younger than DISH patients. Spinal cord injury was present in 58%. Surgery was performed on 67% and comprised instrumentation 3 levels above/below the injury. Mortality correlated with age. Mortality was 32%.
Westerveld et al. performed a systematic review on spine injuries in ankylosing spinal disorders. Most patients had sustained low energy trauma (fall from sitting/standing). In DISH, most fractures were through the vertebral body. In AS, vertebral body fractures equaled those through the disc. Surgery was performed for neurological deterioration, unstable fracture and the presence of an epidural hematoma.
Figure A shows a hyperextension injury at C6-7 (Type I, disc or Type IV,anterior disc, posterior body) cervical spine fracture in ankylosis spondylitis. Visible radiographic characteristics include osteopenia, bamboo spine, marginal syndesmophytes and ossfication of the disc space. Figure B is a chest radiograph showing thoracic syndesmophytes consistent with ankylosing spondylitis. Figure C shows bilateral sacroilitis and hip joint space narrowing typical of ankylosing spondylitis. Illustration A shows the Caron classification of spine fractures in ankylosing spondylitis (Type A, disc injury; Type B, body injury; Type C, anterior body, posterior disc injury; Type D, anterior disc, posterior body injury). Illustration B shows the difference between the marginal osteophytes of AS and nonmarginal osteophytes of DISH in the cervical spine. If you have osteophytes that are building up, and project out anterior to the anterior cortex of the vertebral bodies, like "flowing wax" it is DISH.
Incorrect Answers:
1:
This
is
characteristic
of
Klippel-Feil
syndrome
Question 23
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 24
A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 25
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure? Review Topic
Explanation
Question 26
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps.
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 200-210.
Question 27
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
REFERENCE: Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
Question 28
Figures 4a and 4b are the radiographs of an isolated injury. What is the next most appropriate step in management?

Explanation
Question 29
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 30
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
Explanation
REFERENCE: Skubic JW, Kostuik JP: Thoracic pain syndromes and thoracic disc herniation, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, pp 1443-1464.
Question 31
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
REFERENCES: Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 32
A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?
Explanation
REFERENCES: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Yorimitsu E, Chiba K, Toyama Y, et al: Long-term outcomes of standard discectomy for lumbar disc herniation: A follow-up study of more than 10 years. Spine 2001;26:652-657.
Question 33
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 34
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
REFERENCES: Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Bergsma JE, de Bruijn WC, Rozema FR, et al: Late degradation tissue response to poly
(L-lactide) bone plates and screws. Biomaterials 1995;16:25-31.
Question 35
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
Question 36
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm 3 . The aspirate should also yield which of the following findings?
Explanation
REFERENCES: Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
Hough AJ Jr, Webber RJ: Pathology of the meniscus. Clin Orthop 1990;252:32-40.
Question 37
Changes to the properties of ultra-high molecular weight polyethylene with increasing irradiation dose include improved
Explanation
Irradiation leads to the production of free radicals, requiring a step in the manufacturing process (melting, annealing, vitamin E doping) to stabilize the free radicals and reduce the potential for oxidation. Wear resistance is improved with irradiation; however, there is minimal benefit with doses of greater than 10 Mrads.
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop Relat Res 2003;414:289-304.
Gordan AC, D’Lima DD, Colwell CW Jr: Highly cross-linked polyethylene in total hip arthroplasty. J Am Acad
Orthop Surg 2006;14:511-523.
Jacobs CA, Christian CP, Greenwald AS, et al: Clinical performance of highly cross-linked polyethylenes in total hip arthroplasty. J Bone Joint Surg Am 2007;89:2779-2786.
Question 38
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively
Explanation
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 39
Figure 3 is the clinical photograph of a 20-year-old college soccer player who has a 7-day history of worsening left ankle pain and swelling after being slide-tackled in a game. Radiograph findings of his ankle and foot are normal. He complains of malaise. His history includes a severe ankle sprain 3 months ago. The sprain caused him to miss half the season, but he was able to play in the last 2 games. What is the most appropriate treatment? Review Topic

Explanation
Question 40
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Explanation
REFERENCE: Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: The seventh ACCP Conference on antithrombotic and thrombolytic therapy. Chest 2004;126:338S-400S.
Question 41
Figure 21 is the intraoperative fluoroscopic image of a 40-year-old man who felt a pop during a twisting injury to his right ankle. He underwent open reduction and internal fixation (ORIF) of a bimalleolar ankle fracture. During the surgery the medial and lateral malleoli fractures were reduced and rigidly was internally fixed. Following fracture fixation, which additional test is recommended to ensure mortise stability?

Explanation
Following ORIF of a known osseous injury, stress testing of the syndesmosis is recommended, especially for pronation-external rotation injuries. The Cotton test applies a laterally directed force to the fibula to assess for widening of the distal tibiofibular joint space. A positive Cotton test result indicates that syndesmotic stabilization is indicated. The Thompson test is used to determine Achilles tendon integrity. The squeeze test is a clinical, not intraoperative, assessment of syndesmotic injury. The anterior drawer test assesses the integrity of the anterior talofibular ligament.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
Question 42
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Deyo RA, Diehl AK, Rosenthal M: How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med 1986;315:1064-1070.
Question 43
-What is the most appropriate next treatment step?
Explanation
Based on the patient’s signs and symptoms, the most likely diagnosis is osteomyelitis of the spine. The imaging studies do not reveal a herniated disk, which would be unusual in someone of this age. Aneurysmal bone cysts would involve the posterior elements with a more expansive lesion of bone, whereas this lesion involves primarily the body and anterior column. Hemangioma would likely not be present with systemic signs or symptoms and has a more characteristic coarse trabecular pattern on radiographs and scans. Given the likelihood that this patient has osteomyelitis of the spine, blood cultures may yield an organism about 50% of the time. If cultures are negative, an image-guided biopsy is warranted. A diagnosis needs to be established before treatment such as extension casting or bracing is rendered. Open biopsy may still be needed if needle biopsy is not diagnostic, but this is not the first treatment option. A chest CT scan is not appropriate as a first step when a tumor is presumed and a diagnosis has not been established.
Question 44
What percentage of bone weight is collagen?
Explanation
Question 45
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
REFERENCES: Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears.
Am J Sports Med 2005;33:1405-1417.
Fukuda H: The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br 2003;85:3-11.
Question 46
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
Explanation
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Question 47
There is a risk of impaired forearm rotation after tension band fixation of an olecranon fracture with which of the following?

Explanation
The referenced study by Candal-Couto et al is a cadaveric study that found that K-wire insertion in less than 30 degrees in an ulnar direction led to impingement of the K-wire on the radial head/neck, biceps or supinator. They recommend placing these wires away from this danger zone in order to minimize rotation blocks.
The referenced study by Matthews et al is a case series of two patients who had limited forearm rotation after K-wire fixation. The etiology of limited rotation was found to be from direct overpenetration of the K-wire, which led to a mechanical block.
Question 48
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 49
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?

Explanation
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Which treatment option listed is best for each patient described?
71A

B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Question 50
When planning pin placement for external fixation of the tibia, what is the maximum extent of the knee capsular reflection from the subchondral joint line?
Explanation
Question 51
Figure 1 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snowboarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in

Explanation
Question 52
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of
Explanation
REFERENCES: Gilmore J: Groin pain in the soccer athlete: Fact, fiction, and treatment. Clin Sports Med 1998;17:787-793.
Irshad K, Feldman LS, Lavoie C, et al: Operative management of “hockey groin syndrome”:
12 years of experience in National Hockey League players. Surgery 2001;130:759-766.
Question 53
Which of the following factors has the most effect on the pullout strength of lumbar transpedicular screw fixation?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, Lee KS, White AA III, Hayes WC: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 54
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Explanation
REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.
Question 55
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 56
A 23-year-old otherwise healthy 6-ft, 4-in basketball player complains of pain in his knees. An examination reveals localized tenderness to palpation over the inferior pole of the patella. The patient notes a significant exacerbation of his pain when the examiner takes the knee from flexion to extension. Review Topic
Explanation
Question 57
What approach should be chosen for the injury seen in Figure 67? Review Topic

Explanation
Innervates the medial aspect of the proximal thigh
Originates from the dorsal roots of L4-L5
Course runs medial to the femoral artery
Courses along the medial border of the psoas muscle
Courses under the inguinal ligament PREFERRED RESPONSE 5
Question 58
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 59
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
REFERENCES: Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368.
Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
Siambanes D, Martinez JW, Butler EW, et al: Influence of school backpacks on adolescent back pain. J Pediatr Orthop 2004;24:211-217.
Question 60
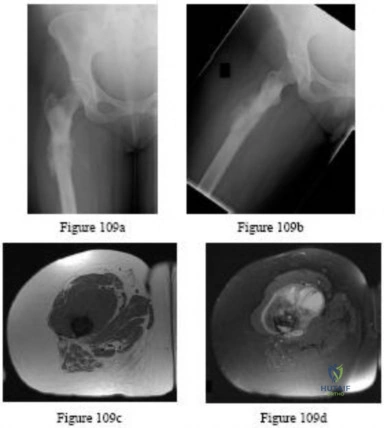
- Figures 59a and 59b show the plain radiographs, and Figures 59c and 59d show the CT scan of a 77-year-old woman who has had pain in her back and both buttocks for the past 6 months. She reports that the pain radiates down her right thigh and leg when she is standing. What is the most likely diagnosis?
Explanation
Question 61
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
Explanation
Question 62
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 63
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm P 3 P , an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Kocher MS, Zurakowski D, Kasser JR: Differentiating between septic arthritis and transient synovitis of the hip in children: An evidence-based clinical prediction algorithm. J Bone Joint Surg Am 1999;81:1662-1670.
Question 64
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
Question 65
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
Explanation
Several studies have found that rates of neurologic deficit and mortality are higher for patients with ankylosing spondylitis and a spinal fracture than for age-matched controls. The 2011 work of Schoenfeld and associates, which directly compared patients with cervical fractures in ankylosed spines to age-and sex-matched controls who also had cervical fractures but no ankylosing condition, demonstrated that those with ankylosing spondylitis were at elevated risk for mortality for up to 2 years after sustaining a fracture. In a study by Westerveld and associates, the rate of neurologic deficit among patients with ankylosing spondylitis and a spinal fracture was 57.1% compared to 12.6% among controls.
RECOMMENDED READINGS
Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. View Abstract at PubMed
Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. View Abstract at PubMed
Question 66
What cardiac condition causes most upper extremity emboli?
Explanation
Atrial fibrillation is responsible for approximately 80% of all upper extremity emboli. All other cardiac conditions listed can cause upper extremity emboli; however, atrial fibrillation is the most common cause. Patients with an upper extremity embolic event should undergo prompt evaluation, with a careful history and physical examination as well as focused laboratory tests for hypercoagulability. Arterial Doppler studies or angiography is/are warranted. Electrocardiogram and echocardiogram are also used to evaluate for potential cardiac abnormalities. Consultation with vascular, radiology, and cardiology personnel is often necessary when patients present with upper extremity emboli. Treatment usually involves anticoagulation, embolectomy if necessary, and treatment for any recognized cardiac abnormality.
Question 67
- Which of the following neurovascular structures is at greatest risk during the introduction of acetabular component fixation screws during total hip replacement?
Explanation
system they found that the posterior superior and posterior inferior quadrants of the acetabulum are the safest locations for screw placement because of better bone stock as well as less neurovascular structures as compared to the anterior quadrants.
Question 68
03 A 26-year-old woman has chronic toe pain after hitting a bedpost 3 months ago. A radiograph is shown in Figure 27. Her injury represents an avulsion of the

Explanation
The EDB originates on the distal lateral and superior surface of the calcaneus and inserts on the
lateral aspect of the flexor digitorum longus tendon and also on to the base of the proximal phalanx of the first through fourth toes. There is no EDB tendon to the fifth toe. If an EDB laceration is easily identified at the time of an EDL repair, than it may be repaired as well, otherwise repair of the EDL alone is sufficient.
Heckman JD: Fractures and dislocation of the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds):Rockwood and Green’s Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 2166-2169.
Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 787-788.
back to this question next question
Question 69
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon MA, Springfield DS, et al: Chondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 70
A 70-year-old female with a history of poorly controlled diabetes mellitus presents with purulent ulcers along the plantar aspect of her right forefoot and exposed metatarsal bone. She elects to undergo an amputation. She is insensate to the midfoot bilaterally. Her ankle-brachial index (ABI) for her right posterior tibial artery is 0.4. Further preoperative evaluation demonstrates a transcutaneous oxygen pressure of 45 and an albumin of 3.4. Which of the following would be a contraindication to performing a Syme amputation (ankle disarticulation) in this patient?

Explanation
Pinzur et al retrospectively reviewed their results when performing a single-stage Syme ankle disarticulation in patients with diabetes either for peripheral neuropathy or infection. Patients with ABIs less than 0.5 for the posterior tibial artery had significantly decreased healing rates and smokers had a three-fold increased risk of postoperative infection.
Incorrect Answers:
Question 71
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
Explanation
Question 72
In a diagnostic test, the proportion of individuals who are truly free of a designated disorder identified by the test is known as
Explanation
Question 73
A neurologic injury at T11-L2 with loss of bowel and bladder control is best described as what syndrome?
Explanation
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Weisberg LA: Neurologic localization: Lesions below foramen magnum, in Weisberg LA, Strub RL, Garcia CA (eds): Adult Neurology, ed 2. St. Louis, MO, Mosby, 1993.
Question 74
A 35-year-old skiier presents with pain in the left buttock and proximal posterior thigh after a fall. His clinical appearance is shown in Figure A. He is enrolled in 8 weeks of physical therapy after 2 weeks of rest, icing and NSAIDS. He returns for follow-up 6 months after his injury and has persistent ischial tuberosity pain with running. Examination confirms focal ischial tuberosity tenderness. MRI images are seen in Figures B and C. Which surgical option is most appropriate? Review Topic
Explanation
Untreated partial hamstring ruptures may present with residual pain, weakness and hamstring dysfunction. The mechanism is eccentric lengthening (sprinting or cutting) A proposed treatment algorithm is: (1) Nonoperative management for single tendon avulsion with <2cm retraction. The ruptured tendon scars to intact tendons. (2) Repair for acute 3-tendon rupture (semitendinosus, semimembranosus, biceps femoris) with retraction >= 2cm. (3) Surgery for young (<50y) patients with 2 tendon avulsion and retraction >= 2cm.
Bowman et al. examined the outcomes of operative management of partial hamstring tears in 17 patients. They found no postoperative difficulties with ADLs, and no recurrent surgery was required. All patients returned to their preoperative level of activity. They concluded that surgery can lead to good function with low complications and is reserved for patients who have failed nonoperative management.
Hofmann et al. retrospectively reviewed 19 patients with nonoperatively managed complete hamstring avulsions. They found diminished SF-12 scores, diminished hamstring strength at 45° and 90° of flexion (62% and 66%, respectively) compared with the normal side. They concluded that nonsurgical management leads to both subjective functional and objective strength deficits.
Figure A shows pronounced bruising from hematoma tracking following the injury. Figures B and C are coronal and axial images showing partial avulsion of the right hamstring insertion. The images correspond with Illustration B, with arrows pointing to the "sickle sign" . Illustration A shows the origins of the hamstring tendons. Illustration C shows the origins of the hamstring group (bf, biceps femoris; st, semitendinosus; sm, semimembranosus; qf, quadratus femoris; am, adductor magnus)
Incorrect Answers:
Question 75
below demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 76
A 54-year-old man undergoes uneventful anterior cervical diskectomy and interbody fusion at C4-5 for focal disk herniation and C5 radiculopathy. At the 3-week follow-up examination, the patient reports a persistent cough. Pulmonary evaluation reveals a mild but persistent aspiration. Laryngoscopy reveals partial paralysis of the left vocal cord, most likely caused by
Explanation
REFERENCES: Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve paralysis during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Jewett BA, Menico GA, Spengler DM, Coleman SC, Netterville JL: Vocal Cord Paralysis Following Anterior Cervical Spine Surgery. Paper presented at the annual meeting or the Cervical Spine Research Society, December 2000, Charleston SC, Paper #7.
Question 77
Figures 82a through 82c show the radiograph and 3-dimensional (3-D) CT scans of a 2-year-old boy whose scoliosis has progressed 15 degrees during the past year. The child is clinically healthy. He has been walking since 11 months of age. An MRI scan of the entire spine revealed no other anomalies. What additional study is indicated? Review Topic
Explanation
Question 78
Which examination finding points toward a brachial plexus injury rather than root avulsion?
Explanation
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus injury.
Question 79
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 80
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
REFERENCES: Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Pape HC, Zelle BA, Hildebrand F, et al: Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am 2005;87:2515-2522.
Question 81
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 82
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
Explanation
Question 83
An 11-year-old child has Ewing’s sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
REFERENCES: Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing’s sarcoma of the limbs. Clin Orthop 1991;286:225.
Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing’s sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant Bone Tumors. Instr Course Lect 2002;51:413-428.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 84
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 85
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?
Explanation
REFERENCES: Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Berlet GC, Lee TH, Massa EG: Talar neck fractures. Orthop Clin North Am 2001;32:53-64.
Question 86
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Explanation
3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 87
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 88
A 32-year-old woman has had progressive left foot pain over the first metatarsophalangeal (MTP) joint. Footwear is becoming problematic. There is full range of motion of the first MTP with medial eminence pain. Her weightbearing radiograph reveals a hallux valgus angle (HVA) of 35 degrees and a 1-2 intermetatarsal angle (IMA) of 10 degrees. What is the best next step?
Explanation
Patients with painful progressive hallux valgus are surgical candidates. Presurgical evaluation includes radiographic examination. The IMA between the first and second metatarsals as well as the HVA must be measured. If the IMA is smaller than 15 degrees and the HVA is smaller than 35 degrees, a distal osteotomy is preferred. Distal soft-tissue reconstruction is only useful for IMAs smaller than 11 degrees and HVAs smaller than 25 degrees. Proximal osteotomies and the Lapidus bunionectomy are reserved for larger hallux valgus deformities with IMAs exceeding 15 degrees and HVAs exceeding 35 degrees.
RECOMMENDED READINGS
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J. Distal Chevron Osteotomy: Preoperative Radiological Factors Contributing to Long-Term Radiological Recurrence of Hallux
Valgus. Foot Ankle Int. 2014 Sep 5. pii: 1071100714548703. [Epub ahead of print] PubMed PMID: 25192724. View Abstract at PubMed
Fakoor M, Sarafan N, Mohammadhoseini P, Khorami M, Arti H, Mosavi S, Aghaeeaghdam A. Comparison of Clinical Outcomes of Scarf and Chevron Osteotomies and the McBride Procedure in the Treatment of Hallux Valgus Deformity. Arch Bone Jt Surg. 2014 Mar;2(1):31-
Question 89
An 18-year-old male football player dislocated his elbow during a game. A post-reduction MRI scan is shown in Figure 1. The injury is initially treated non-operatively, but the patient continues to note subjective instability and pain when attempting to push up from a chair. Surgical intervention is planned for repair/reconstruction. What guidance should be provided to the patient and therapist in the early postoperative period?
Explanation
Question 90
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Explanation
REFERENCES: Kaplan FS, Singer FS: Paget’s disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Siris ES: Paget’s disease of bone, in Favus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. New York, NY, Raven Press, 1993, pp 375-384.
Question 91
-What is the most appropriate initial treatment for her condition?
Explanation
This patient has a history most consistent with multidirectional instability. A lax capsule causes subluxation of the shoulder and strain on the rotator cuff and may result in pain and instability. The capsule is most closely associated with the cause of her problem. Initial treatment for multidirectional instability is physical therapy focusing on restoring balance to the shoulder with rotator cuff and scapular stabilization exercises. Nonsurgical therapy should be protracted and is the mainstay of treatment in this scenario. This patient has exhausted all nonsurgical measures and is now a candidate for surgical reconstruction. Capsular plication will best address the lax capsule and provide the best option for reducing her symptoms. The rotator cuff and biceps tendon may be secondarily strained but are not the primary sources of the problem. The brachial plexus does not address the etiology, but rather the symptoms that may occur as a result of instability of the shoulder joint.
Complete rest will not alleviate the patient's underlying condition because the shoulder girdle may still be weak and symptoms likely will return. A corticosteroid injection and arthroscopic surgery are too invasive as initial treatment for this condition. Arthroscopic rotator cuff repair, a biceps tenodesis, and superior labral anterior-posterior repair are unlikely to result in symptomatic improvement for this patient and are not associated with pathologic findings in the setting of multidirectional instability.
Question 92
A 25-year-old patient presents with a posterior wall/ posterior column acetabular fracture. She is scheduled for open reduction internal fixation through a posterior approach. What position of the leg exerts the least amount of intraneural pressure on the sciatic nerve?

Explanation
Question 93
Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation? Review Topic
Explanation
Question 94
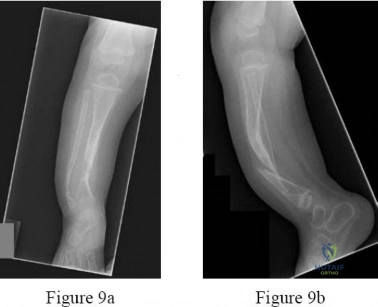
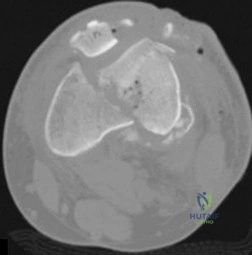
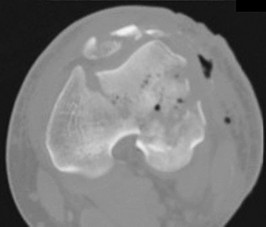
9A 9B 9C 9D Figures 9a through 9d are the radiographs of a 21-year-old woman who is involved in a high-speed motor vehicle collision and sustains an isolated right closed-foot injury. Before surgery, the patient is advised about the relatively poor long-term outcomes associated with this injury. What is the most common reason for functional limitations after surgical treatment in this scenario?

Explanation
When a displaced talar neck fracture occurs, the rate of osteonecrosis is high; however, many revascularize the talus without collapse. A nonunion can occur but is less common than osteonecrosis and arthritis. A varus malunion can be debilitating and lead to subtalar arthritis. In a fracture with the talar body dislocated posteromedially (such as in this example) neurologic deficits in the tibial nerve distribution are common but typically improve with urgent
reduction. Studies show that posttraumatic subtalar arthritis is common after this injury and is the most likely cause of long-term functional impairment.
RECOMMENDED READINGS
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407. View Abstract at PubMed
Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 10 THROUGH 12

10A

10B

10C
Figure 10a is the radiograph of a 30-year-old man who sustained an injury in a motor vehicle collision.
Question 95
Figures 1a and 1b show the sagittal T 2 - and T 1 -weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm 3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of
Explanation
REFERENCES: Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 431-439.
Question 96
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s diagnosis?

Explanation
Question 97
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
REFERENCES: Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Dias LS: Surgical management of acquired foot and ankle deformities, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 161-170.
Question 98
When performing a Green transfer for cerebral palsy—flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB)—in addition to improving wrist extension, what other motion may be improved if the FCU is routed around the ulna instead of through the interosseous membrane?
Explanation
The typical upper extremity deformity in spastic hemiplegic cerebral palsy consists of shoulder internal rotation, elbow flexion, forearm pronation and wrist flexion, and ulnar deviation. The pronation position of the forearm can make bimanual activities more challenging for the child. The wrist flexion and ulnar deviation deformity interferes with finger function and therefore with grasp and release patterns. By transferring the FCU tendon to the ECRB, the deforming force is released, and central wrist extension is augmented. This transfer can lead to a supination moment when it is routed around the ulna to the ECRB insertion on the dorsum of the wrist. Thumb and finger extension are not affected by an FCU-to-ECRB tendon transfer. Forearm supination, not pronation, is potentially improved with this tendon transfer.
Question 99
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391.
Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Naranja RJ Jr, Chan PS, High K, Esterhai JL Jr, Heppenstall RB: Treatment considerations in patients with compartment syndrome and an inherited bleeding disorder. Orthopedics 1997;20:706-711.
Question 100
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
Explanation
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
