Orthopedic Surgery Board Review MCQs: Spine, Arthroplasty & Trauma | Part 157
Key Takeaway
This page offers a comprehensive bank of 100 high-yield multiple-choice questions (MCQs) for orthopedic surgeons and residents preparing for their AAOS and OITE board certification exams. Authored by Dr. Mohammed Hutaif, it provides detailed explanations and two distinct learning modes to ensure thorough, effective exam preparation.
About This Board Review Set
This is Part 157 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 157
This module focuses heavily on: Spine Surgery, Knee & Hip Arthroplasty, Trauma, Sports Medicine, Pediatric Orthopedics.
Sample Questions from This Set
Sample Question 1: Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic...
Sample Question 2: A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mmP3P and a C-reactive protein level of 10 mg/L. A ...
Sample Question 3: A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his...
Sample Question 4: Emergent management of acute tooth displacement (luxation) includes...
Sample Question 5: 3 degrees Celsius and heart rate of 105 bpm. A clinical photograph, results of synovial fluid analysis, and a polarizing microscopy image are seen in Figures A through C. Synovial fluid gram stain and cultures are pending. What is the most ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic
Explanation
Aggrecan, the most abundant proteoglycan within the intervertebral disk, is a hydrophillic molecule which helps attract and maintain water within the disc. This is important to maintain compressive strength. Early in life aggrecan has a high percentage of chondroitin sulfate chains. With aging this gradually changes to higher percentage of keratin sulfate. Other proteoglycans include decorin and versican. Decorin is believed to regulate cell cycles and influence fibrillogensis. Versican is a large extra-cellular matrix proteoglycan involved in cell adhesion and migration.
Roughley et al. provide a review of biologic changes within the intervertebral disc during development, maturation, and degeneration. They note that aggrecan works to maintain water content within the disc, thus improving its compressive strength. Aggrecan content decreases with age leading to a loss of compressive strength.
Illustration A shows the structure of aggrecan.
Incorrect answers:
Question 2
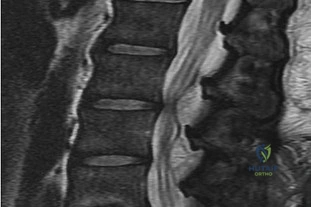
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mmP3P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of Review Topic
Explanation
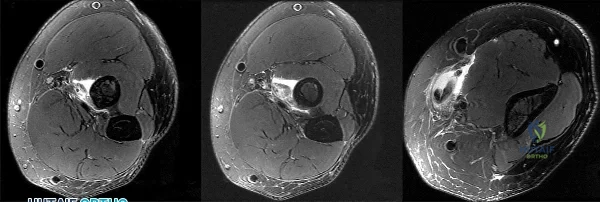
(SBQ12SP.92) A 36-year-old man presents to the emergency department after being involved in a motor vehicle collision. He is complaining of back pain and imaging shows the findings in Figure A. On neurological examination, he does not have any deficits. MRI shows approximately 25% canal encroachment and no evidence of injury to the posterior ligamentous complex. Which of the following is the most appropriate course in management? Review Topic

Strict bedrest for six weeks then progressive weightbearing
Ambulation as tolerated with or without a TLSO
Surgical decompression and anterior stabilization
Surgical decompression and posterior stabilization
Surgical decompression and combined anterior/posterior stabilization
The patient has a L1 burst fracture with minimal retropulsion of bony fragments in the spinal canal. In the absence of neurological deficits and injury to the PLC, the most appropriate treatment is ambulation as tolerated with or without a thoracolumbrosacral orthosis (TLSO).
Thoracolumbar burst fractures are typically caused by an axial load with flexion and commonly found in this location due to increased motion at these segments. With an intact posterior ligamentous complex (PLC) and no neural compromise, TLSO is the mainstay of treatment. If there is evidence of neurological deficit and/or PLC injury, decompression and fusion are indicated. The degree of acceptable kyphosis is controversial. The choice of anterior versus posterior approach is based on ease of decompression.
Vaccaro et al. introduced a new classification system for thoracolumbar injuries, TLICS, based on morphological appearance, integrity of the posterior ligamentous complex, and neurological status. They advocate use of the system for nonoperative versus operative decision making and communication between surgeons.
Bailey et al. completed a randomized, nonblinded controlled trial to determine the
efficacy of bracing for AO type A0-A3 thoracolumbar burst fractures. Both groups were encouraged to ambulate as tolerated and the no brace group had bending restrictions for 8 weeks. They found no difference in the Roland Morris Disability Questionnaire (RMDQ) score at 3 months after injury.
Figure A is sagittal CT scan of the lumbar spine showing a burst fracture of L1 with minimal retropulsion. Illustration A is the TLICS classification with score of 4 being the branch point for nonoperative versus operative management.
Incorrect Answers:
Question 3
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?
Explanation
week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice.
REFERENCES: Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 4
Emergent management of acute tooth displacement (luxation) includes
Explanation
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
Question 5
3 degrees Celsius and heart rate of 105 bpm. A clinical photograph, results of synovial fluid analysis, and a polarizing microscopy image are seen in Figures A through C. Synovial fluid gram stain and cultures are pending. What is the most appropriate next step in management?
Explanation
While the incidence of superimposed gout and septic arthritis is low (~1.5%),
it is reported. In the presence of crystals on aspiration, one should not rule out the possibility of septic arthritis. If there are other risk factors for infection, or the synovial WBC count is high (greater than 50,000), then empiric antibiotics should be initiated immediately after cultures are obtained. If the patient has other evidence supporting septic arthritis (positive Gram stain, purulence), emergent I&D is indicated. Even if the initial suspicion is lower, if they have
not respond to antibiotics after 24-48 hours they should undergo I&D.
Shah et al. investigated 265 crystal-positive joint aspirates in a 7-year retrospective study. They found the incidence of concomitant septic arthritis and crystal disease was 1.5% (4 cases including 2 knees, 1 hip, 1 ankle). All 4 patients that had superimposed infection had a WBC of > 50,000. They concluded that the presence of crystals in the synovial fluid cannot
conclusively rule out a septic joint.
Schuind et al. described a case report of concomitant septic arthritis and gout of the wrist. They found that cultures were positive for Staphylococcus aureus while pathological examination revealed aggregated crystals of monosodium urate.
Figure A shows tense, erythematous swelling of the right knee. Figure B is a table showing synovial fluid analysis with elevated WBC and PMN cell count characteristic of septic arthritis. Figure C shows needle-shaped negatively birefringent crystals on polarizing microscopy. Illustration A shows the synovial fluid characteristics in different disease conditions.
Incorrect Answers:
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Lead to lower patient satisfaction rates
Lead to higher patient satisfaction rates
Lead to higher likelihood the patient will take legal action against surgeon
Lead to higher likelihood the patient will change physicians
Prevent any legal action
The surgeon has provided all the elements of good communication with the patient and family. His actions will lead to improved patient satisfaction, compared to nondisclosure and attempting to push or shirk responsibility.
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise:
an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose
non-disclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
The acquired immune response mediated by the interaction between the T cell receptor and major histocompatibility complex requires which of the following first steps?
Antigen phagocytosis by T cells
Antigen processing and presentation to T cells
Antigen recognition by natural killer T cells
Antigen proliferation by polymerase chain reaction
T cell disulfide bond cleavage and enzymatic processing
The process of antigen processing and presentation is the first step of the acquired immune response. This is performed by the so called antigen presentation cells (APC) of which B cells and dentritic cells are two examples. The APC breaks down the protein antigen in a multitude of enzymatic reactions and presents key peptide sequences via the major histocompatibility complex
(MHC) receptors. Once presented on the surface of the APC, the T-cell receptor recognizes the MHC/antigen complex leading to T-cell activation. At no point in this process are antigens phagocytosed by T cells. Natural killer T cells are involved in this sequence, but not for antigen processing and presentation. Polymerase chain reaction is a laboratory tool used to amplify nucleic acid. Finally, disulfide bond cleavage is a step involved in the APCs antigen processing reaction and does not occur in T cells.
All of the following are true regarding a physician responding to a formal written complaint by a patient EXCEPT:
Complaint should be taken seriously
Written response by the physician is required
Physician mandated to retain an attorney to address the formal complaint
Patient should be supplied with contact information for the institution's patient representative department
Law mandates that the physician respond to the formal complaint
It is important for the surgeon to know how to manage a formal complaint. An attorney is not required to assist on behalf of the physician when addressing a formal complaint. All complaints must be taken seriously and the physician is required by law to respond to all formal complaints in writing. Verbal
responses to formal, written complaints are not sufficient. If a patient is filing a formal complaint it is advisable that the patient be supplied with contact information for the institution's patient representative department.
What laboratory findings would you expect to find in a patient newly diagnosed with renal osteodystrophy?
Decreased PTH secretion, hypophosphatemia, and hypocalcemia
Increased PTH secretion, hyperphosphatemia, and hypocalcemia
Decreased PTH secretion, hypophosphatemia, and hypercalcemia
Increased PTH secretion, hyperphosphatemia, and hypercalcemia
Hypophosphatemia and hypocalcemia
Renal osteodystrophy is characterized by bone mineralization deficiency due to the electrolyte and endocrine abnormalities associated with chronic kidney disease. The pathogenesis of renal osteodystrophy is multifactorial. Hypocalcemia occurs due to the inability of the damaged kidney to convert vitamin D3 into its active form, calcitriol. The hypocalcemia and lack of phosphate excretion by the damaged kidney causes hyperparathyroidism and secondary hyperphosphatemia.
Loss of function in the 25(OH) vitamin D1-alpha hydroxylase gene causes which of the following diseases?
Hyperphosphatemia
Vitamin D resistant rickets
Hereditary Vitamin D dependant rickets type I
Hereditary Vitamin D dependant rickets type II
Hypophosphatemic rickets
Loss of function mutations in the 25 (OH) vitamin D hydroxylase gene cause hereditary vitamin D dependant rickets type I. Hereditary vitamin D dependant rickets type II is caused by a defect in intracellular receptor for 1,25-(OH)2- vitamin D3. Both forms of
hereditary vitamin D dependent rickets show decreased serum calcium/phosphorous, elevated alkaline phosphatase/PTH,
but type I has a decrease in the 1,25(OH)2 vitamin D and type II shows a increase in 1,25(OH)2 vitamin D. Vitamin D resistant rickets (Familial Hypophosphatemic Rickets) is caused by a large deletion in the PHEX gene and results in low serum phosphorous, elevated alkaline phosphatase, and normal calcium. Hyperphosphatemia can be caused by mutation in the GALNT3 gene and results in elevated serum phosphate and decreased PTH/calcium.
Kato et al. describe the molecular physiology of vitamin D metabolism and the recognized gene mutations associated with various clinical manifestations of mutations in vitamin D homeostasis.
Figure A is a radiograph taken after an open reduction and internal fixation of a periprosthetic distal femur fracture. With this type of hybrid locked plate fixation, what is the difference between screw A and screw B?
Screw A can assist in fracture reduction while screw B provides a fixed angle support
Screw A provides improved axial stiffness while screw B provides a fixed angle support
Screw A can be used to reduce the plate to bone while screw B can be used to lag fracture fragments together
Screw A provides a fixed angle support while screw B can be used to reduce the plate to the bone
Screw A can be used to lag fracture fragments together and screw B increases the plate bone frictional stability
Locking screws provide a fixed angle support and can improve fixation in osteoporotic bone while nonlocking screws can be used to reduce the plate to the bone, lag fracture fragments together and increase the plate bone frictional stability. "Hybrid" locked plate fixation utilizes both screw types in order to assist with difficult fracture fixation such as when there is a short metaphyseal segment and osteoporotic bone.
Zura et al discusses the biomechanical and biological advantages offered by locked plate fixation.
Using levels of evidence in research studies, which of the following represents a level II study?
Retrospective case control study
Prospective cohort study
Case report of 3 patients with the same disease
High-quality randomized prospective clinical trial
The opinion of a review panel at the annual AAOS meeting
Level II Evidence includes prospective cohort studies. There are 5 levels of evidence in clinical research. Level I includes randomized clinical trials. Level II includes prospective cohort studies. Level III includes case control studies AND retrospective cohort studies. Level IV includes case series. Level V evidence includes expert opinion, case reports, and personal observation. The cited reference by Bernstein et al is an excellent review of Evidence Based Medicine (EBM) and describes the 5 step process of making medical decisions based on the available, and often limited, evidence. These steps include: 1) Formulate answerable questions. 2) Gather the evidence. 3) Appraise the evidence. 4) Implement the evidence. 5) Evaluate the process. The reference by Spindler et al is another review article that discusses the different levels of evidence for different study types.
All of the following are true regarding the assessment of bone mineral density EXCEPT?
Bone mineral density loss is not apparent on standard radiographs until 30% to 40% of mineral is lost
Dual energy x-ray absorbtiometry (DEXA) is only able to measure mineralization of the axial skeleton
Single photon absorbtiometry allows for the analysis of bone mineralization in the appendicular skeleton alone
Quantitative computed tomography (QCT) is associated with 10 times the radiation of a DEXA scan
MRI allows for accurate discrimination of normal bone from osteopenic bones
without exposing the patient to ionizing radiation
Dual energy x-ray absorbtiometry (DEXA) scans allow for accurate assessment of bone mineralization in both the axial and appendicular skeleton.
Over the last decade, DEXA has become a safe, cost-effective and reliable method to quantify bone mineral density. The World Health Organization (WHO) has adopted DEXA derived BMD measurements to define normal bone, osteopenia, and osteoporosis in the adult and paediatric population. The typical DEXA analysis therefore reports a Z-score, which is the number of standard deviations (SDs) that a patient's BMD is above or below the mean value for persons of the patient's age and sex. The T score is the number of SDs the patient's BMD is either above or below the mean value for young patients of the same gender.
Tortolani et al. provide an overview of the techniques used to assess bone mineral density, the pathophysiology of osteopenia, and the evaluation and treatment options for the general pediatric population as well as for patients with specific pediatric disorders. The authors encouraged orthopaedic surgeons to understand the problems of osteopenia in both otherwise healthy children and children with chronic disorders.
Binkovitz & Henwood provide a review of DEXA technique and interpretation with emphasis on the considerations unique to pediatrics. They found that changes in bone size over time, as occurs in normal pediatric development, confound DXA interpretation. This is one of the major limitations in the use of pediatric DXA. However, attempts to correct for or to circumvent this limitation have been proposed and show promise in improving DXA interpretation and
our understanding of bone physiology.
T-score according to the World Health Organization (WHO): A T- score of -1.0 or above is normal bone density.
A T-score between -1.0 and -2.5 means you have low bone density or osteopenia.
A T-score of -2.5 or below is a diagnosis of osteoporosis.
Incorrect Answers:
A mother brings her 4-year-old daughter to your clinic for evaluation of knocked knees and short stature. On exam, the patient ambulates with a circumduction gait pattern and frequently falls. Plain radiographs are displayed in Figure A. Laboratory data is obtained and notable for calcium 9.1 mg/dL (RR 8.5-
Question 6
Which of the following foot deformities is commonly seen in patients with Charcot-Marie-Tooth disease? Review Topic
Explanation
Question 7
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Explanation
REFERENCES: Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
Schoenecker PL: Surgical management of hip problems in children with myelomeningocele, in Sarwark KR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 117-131.
Question 8
A 16-year-old football player is participating in the second session of two-a-day preseason practices. He complains of dizziness and fatigue. He is brought to the sideline by the athletic trainer where examination demonstrates confusion and disorientation. Ambient temperature is 82°F. What would be the next most appropriate step in his treatment?
Explanation
Question 9
What is the most common malignancy involving the hand?
Explanation
REFERENCES: Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Fleegler EJ: Skin tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 2184-2205.
Question 10
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 11
Figure 1 shows the radiograph obtained from a 67-year-old woman who has progressive wrist pain. She undergoes a salvage motion-sparing surgery that relies on the intact cartilage of the capitate head. It is necessary to preserve what structure during this procedure?
Explanation
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be required. The authors did cut through the dorsal intercarpal ligament in their exposure.
Question 12
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Sim FH: Metastatic bone disease of the pelvis and femur. Instr Course Lect 1992;41:317-327.
Question 13
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?

Explanation
Question 14
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
Question 15
The dose of the chemotherapeutic agent doxorubicin (Adriamycin) is limited by which of the following factors?
Explanation
REFERENCE: Brockstein BE, Peabody RD, Simon MA: Soft tissue sarcomas, in Vokes EE, Golomb HM (eds): Oncologic Therapies. Berlin, Springer, 1999, pp 925-952.
Question 16
-Figures a and b are the T2-weighted MRI scans of a 37-year-old left-hand-dominant man with a 3-month history of neck pain radiating down the back of his left arm and into his left hand. He also noted difficulty with buttoning his shirt. Examination reveals full strength and sensation in all extremities. He has radiating pain in all extremities with neck extension and flexion. He also has hyperactive reflexes and difficulty with tandem gait. What is the most appropriate treatment?
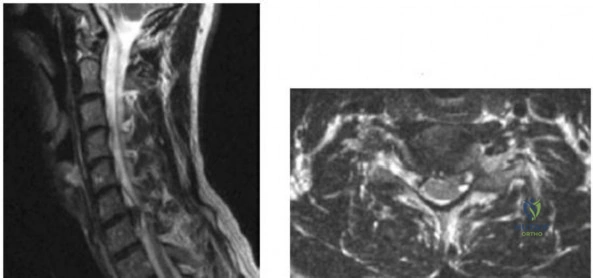
Explanation

Question 17
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 18
A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?
Explanation
REFERENCES: Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53.
Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis. J Bone Joint Surg Am 1996;78:1541-1547.
Question 19
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Explanation
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 20
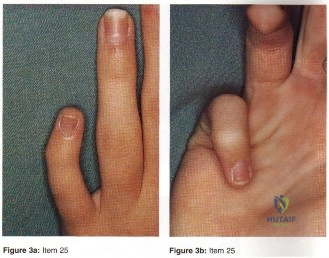
- Figures 3a and 3b show the finger deformity that a 13-year-old girl has had since birth. What is the most likely diagnosis?
Explanation
definitions of the other distracters are self-explanatory (Staheli, Fundamental of Pediatric Orthopedics, 1998): Camptodactyly: non-painful flexion deformity of the PIP joint (i.e. AP Plane); abnormality of the insertions of the intrinsics and extrinsics flexor tendons; both hereditary and non-hereditary forms. Symbrachydactyly: digital absence in the form of transverse efficiency; teratogenic etiology resulting in absence distal metacarpals with finger nubbins. Kirner’s deformity: rare progressive deformity of the terminal phalanx of the small fingers with fingernails a curved and clubbed appearance; usually bilateral and appears during adolescence. Digiti minimi adductus: no such deformity found mention in the literature.
Question 21
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
REFERENCE: Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
Question 22
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of
Explanation
REFERENCES: Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Kaplan H, Kiral A, Kuskucu M, et al: Report of eight cases of humeral fracture following the throwing of hand grenades. Arch Orthop Trauma Surg 1998;117:50-52.
Question 23
A 26-year-old female twists her knee while playing soccer and sustains the injury shown in Figure A. She undergoes a reconstructive surgery and is started on an accelerated rehabilitation program. Which of the following is true regarding this type of rehabilitation protocol? Review Topic

Explanation
Rehabilitation after ACL reconstruction is necessary for a successful surgical outcome and remains an important topic of research interest. Accelerated programs allow for earlier weightbearing and certain strengthening exercises, rather than waiting several weeks before performing certain activities which put strain on the graft. Despite initial concerns that accelerated rehabilitation programs may lead to worse outcomes, many studies have demonstrated comparable outcomes between accelerated and nonaccelerated rehabilitation programs. No significant long-term differences have been reported regarding ACL laxity, range of motion, strength, or return to sports. Use of an accelerated program does not imply earlier return to sports. The optimal time to return to sports has not yet been elucidated.
Beynnon et al. performed a randomized controlled trial of patients who underwent ACL reconstruction with bone-patellar tendon-bone autograft comparing rehabilitiaton with either accelerated (19 week) or nonaccelerated (32 week) programs. At final evaluation, patients in both programs had the same increase in the envelope of knee laxity, clinical assessment, functional performance, proprioception,
and
thigh
muscle
strength.
Kruse et al. presented a systematic review evaluating studies on rehabilitation following ACL reconstruction. The authors found that accelerated rehabilitation does not appear to be harmful. It is likely safe for patients to begin immediate postoperative weight bearing, range of motion from 0-90 degrees of flexion, and perform closed-chain exercises. Bracing following ACL reconstruction is neither necessary nor beneficial and often adds to the cost of the procedure.
Figure A is a sagittal MRI demonstrating a complete ACL tear.
Incorrect
Question 24
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 25
The patient subsequently requires split-thickness skin grafting over his lateral fasciotomy wound during soft-tissue reconstruction. In this setting, NPWT
Explanation
NPWT increases wound perfusion. The dressing may help decrease risk for wound infection, but will not do so by removing bacteria. It also helps to prevent wound contracture to improve the likelihood of primary wound closure. NPWT can help to improve tissue edema and will not elevate compartment pressure.
Hemorrhage is the most common major complication associated with NPWT. This risk is highest when NPWT is used in areas of major vessels and vessels that have been ligated and for patients undergoing anticoagulation therapy. Specialized white polyvinyl alcohol sponges are available to prevent adherence to vessels, exposed nerves, or exposed bone. NPWT should not be used directly over exposed major vessels. If major bleeding occurs, a return to the operating room for wound exploration is recommended.
Incisional NPWT is an effective treatment for persistent serous drainage. Wounds that drain persistently seal more quickly and pose lower risk for infection when incisional NPWT is used vs compressive dressings. Incisional NPWT has also demonstrated benefit when used on high-risk postsurgical wounds of the tibial plateau, pilon, and calcaneus. It has not been shown to contribute to increased risk for wound dehiscence or hematoma.
NPWT stabilizes the soft-tissue environment and does not necessitate frequent dressing changes. Despite this benefit, a delay of flap coverage after NPWT still poses higher risk for infection than early coverage. Consequently, flaps should not be delayed for long. NPWT promotes the formation of granulation
tissue and can be used over exposed bone, but it would not be expected to form granulation tissue over an exposed fracture site or hardware or promote fracture healing.
NPWT provides an excellent bolster for a skin graft and improves skin graft incorporation. It needs to be applied with nonadherent dressings to prevent adherence to the skin graft. NPWT is generally not used at skin grafting donor sites.
RECOMMENDED READINGS
Streubel PN, Stinner DJ, Obremskey WT. Use of negative-pressure wound therapy in orthopaedic trauma. J Am Acad Orthop Surg. 2012 Sep;20(9):564-74. doi: 10.5435/JAAOS-20-09-564. Review. PubMed PMID: 22941799.View Abstract at PubMed
Powell ET 4th. The role of negative pressure wound therapy with reticulated open cell foam in the treatment of war wounds. J Orthop Trauma. 2008 Nov-Dec;22(10 Suppl):S138-41. doi: 10.1097/BOT.0b013e318188e27d. Review. PubMed PMID: 19034160. View Abstract at PubMed
Question 26
Long-term alendronate (Fosamax) use for osteoporosis has been associated with which of the following?
Explanation
fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with uterine cancer or a detached retina.
Question 27
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 28
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of
Explanation
REFERENCE: Farsetti P, Weinstein SL, Ponseti IV: The long-term functional and radiographic outcomes of untreated and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265.
Question 29
5 mm of change in the atlanto-dens interval (ADI) between flexion and extension views
Explanation
With the introductions of disease-modifying antirheumatic agents (DMARDs), the incidence of RA patients undergoing cervical spine surgery has decreased significantly. Basilar invagination, atlantoaxial instability, and subaxial subluxation are the three most common manifestations of cervical disease. Multiple studies in RA patients with untreated or poorly controlled disease have led to the development of a set of measurements that identify patients who require surgical intervention and predict outcome after surgery. Additionally, progressive neurological compromise and
refractory
pain
are
indications
for
intervention.
Kim and Hilibrand reviewed management of the rheumatoid cervical spine and outline parameters for surgical intervention. These include a PADI < 14 mm, cervicomedullary angle <135 degrees, progressive neurological deficit, refractory pain, atlantoaxial impaction as determined by migration >5 mm rostral to McGregor's line, and subaxial canal diameter < 14 mm.
Boden et al. analyzed 73 patients followed for rheumatoid cervical spine disease with an average follow up of 7 years. They found that the PADI correlated with paralysis. Patients with PADI less than 10 mm had no recovery, and all patients with PADI greater than 14 mm had full recovery.
Illustration A demonstrates the measurement of the ADI and PADI. Illustration B demonstrates how to measure the cervicomedullary angle (as marked by A), which is typically determined on MRI
Incorrect
Question 30
A 41-year-old male truck driver fell off his truck and tried to break his fall by holding on to the side of the door with his left arm. His MRI is depicted in Figures A. Which of the following special tests would most likely be positive on physical examination? Review Topic
Explanation
While the subscapularis is the largest of the rotator cuff muscles, the relative
prevalence of injuries to the subscapularis tendon has only recently been recognized. The primary function of the subscapularis is to internally rotate the humerus. Patients with such injury often present with anterior shoulder pain, and increased external rotation compared to the contralateral limb. It is often associated with medial subluxation of the long head of biceps. A number of special tests have been developed to help aid in the clinical diagnosis of this injury including the belly press, lift off and bear hug tests.
Gerber et al. demonstrated the efficacy of a simple clinical maneuver called the ‘lift-off test’ to reliably diagnose or exclude clinically relevant rupture of the subscapularis tendon in 16 patients.
Barth et al. evaluated the diagnostic value of three clinical tests commonly used to diagnose subscapularis tendon tears; the lift-off test, belly-press test, and bear-hug test. They found that the lift-off test was the most difficult for patients to perform. However, when it was performed and found to be positive, it was 74% sensitive of very severe tears. They also found that the bear hug test was the most sensitive of all tests (82%).
Figures A shows an axial MRI arthrogram showing a subscapularis tear with dislocation of the biceps tendon. Illustration A demonstrates how to perform the bear hug test.
Incorrect Answers:
Question 31
Following total elbow arthroplasty, patients should be instructed to Review Topic
Explanation
Question 32
What is the most common pediatric soft-tissue sarcoma?
Explanation
REFERENCE: Wexler LH, Helman LJ: Pediatric soft tissue sarcomas. CA Cancer J Clin 1994;44:211-247.
Question 33
Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Barrack RL, et al: Resurfacing of the patella in total knee arthroplasty: A prospective, randomized, double-blind study. J Bone Joint Surg Am 1997;79:1121-1131.
Question 34
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of
Explanation
REFERENCE: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 157-161.
Question 35
Figure 177 is an intra-articular photograph taken while viewing from the anterior superior portal during arthroscopy of a right shoulder. Which of the following findings identified at the time of surgery would be the most predictive for recurrence following arthroscopic repair of the demonstrated pathology? Review Topic

Explanation
Question 36
An 11-year-old child has a tibia-fibula fracture following a fall from a swing. The fracture is reduced and placed in a long leg splint in the emergency room. What is considered the most important symptom of a developing compartment syndrome of the leg?

Explanation
The Willis article also lists the most reliable signs of a developing compartment syndrome as severe pain with passive stretching of the involved compartment, pain with palpation of the involved compartment, sensory disturbances
Question 37
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 38
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?

Explanation
Question 39
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone? Review Topic
Explanation
Question 40
Which of the following variables has been shown to have the greatest influence on the higher rate of anterior cruciate ligament (ACL) tears in women when compared to men for similar sports?
Explanation
REFERENCES: Harmon KJ, Ireland ML: Gender differences in noncontact anterior cruciate ligament injuries. Clin Sports Med 2000;19:287-302.
Arendt EA: Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med 1995;23:694-701.
Rozzi SL, Lephart SM, Gear WS, Fu FH: Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med 1999;27:312-319.
Question 41
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
REFERENCES: Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949.
Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 42
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
REFERENCES: Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 421-454.
Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 43
Figure 31 is the abdominal radiograph of a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.

CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 35
Figures 32a through 32c are the radiographs of a 30-year old man who is experiencing right hip pain. He has no current medical problems, but, with a body mass index of 41, he is morbidly obese. He was previously treated for leukemia with chemotherapy that included
high-dose steroids. He undergoes total hip arthroplasty (THA) with a ceramic-on-ceramic bearing.
Question 44
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
REFERENCES: Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 165-201.
Question 45
A 16-year-old swimmer has right shoulder pain with activity. She describes the continued sensation that her shoulder is “loose.” She has been in physical therapy for 7 months to work on strengthening the muscles around her shoulder and scapula. She denies being able to voluntarily dislocate her shoulder. Upon examination, you can feel the humeral head slide over the glenoid rim both anteriorly and posteriorly with the load and shift test. She has a grade III sulcus sign. What is the most appropriate next step?
Explanation
Nonsurgical treatment with activity modification and physical therapy is generally considered the first-line approach for young athletes with multidirectional instability (MDI) of the shoulder. Physical therapy focuses on exercises to strengthen the scapular stabilizers and rotator cuff muscles and restore scapulohumeral rhythm. Although a definitive length of time
to assess physical therapy failure is not known, many surgeons believe that a patient with MDI should undergo at least 6 months of physical therapy and activity modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.

CLINICAL SITUATION FOR QUESTIONS 21 THROUGH 25
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.
Question 46
A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
Explanation
are several treatment options available. The best option for survivorship is a cementless
porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants.
REFERENCES: Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936.
D’Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.
Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.
Question 47
The Lisfranc ligament connects the base of the
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 48
At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
Explanation
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal involvement). The radiolunate joint is often spared.
Question 49
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
Explanation
REFERENCES: Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion:
A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105.
Question 50
Linazolid exerts its antimicrobial action by inhibiting bacterial
Explanation
REFERENCES: Rybak MJ, Cappelletty DM, Moldovan T, et al: Comparative in vitro activities and postantibiotic effects of the oxazolidinone compounds eperezolid (PNU-100592) and linezolid (PNU-100766) versus vancomycin against Staphylococcus aureus, coagulase-negative staphylococci, Enterococcus faecalis, and Enterococcus faecium. Antimicrob Agents Chemother 1998;42:721-724.
Sweeney MT, Zurenko GE: In vitro activities of linezolid combined with other antimicrobial agents against Staphylococci, Enterococci, Pneumococci, and selected gram-negative organisms. Antimicrob Agents Chemother 2003;47:1902-1906.
Question 51
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?

Explanation
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p < 0.01, respectively), lower nonunion (2 vs. 7, p=0.042) & lower malunion (0 vs. 9, p=0.001). Surgery resulted in quicker radiographic union (16.4 weeks vs. 28.4 weeks, p=0.001). However, 15% had hardware and wound complications. At one year, the operative group was more likely to be satisfied with the shoulder in general (p=0.002) and the appearance of the shoulder in particular (p=0.001) in comparison to the nonoperative group.
Prior studies have shown that greater than 2cm of shortening treated non-operatively results in increased fatigueability and poor outcome, but not necessarily nonunion. The Lazarides article concluded that “Final clavicular shortening of more than 18 mm in male patients and of more than 14 mm in female patients was significantly associated with an unsatisfactory result.”
Studies have shown no difference in outcome when treated with a Figure-of-8 harness compared to a simple sling
Question 52
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?
Explanation
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 265-274.
Question 53
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?

Explanation
well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 54
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 55
Which of the following definitions best describes Batson’s vertebral vein system?
Explanation
REFERENCES: Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Coman DR, de Long RP: Role of vertebral venous system in metastasis of cancer to spinal column: Experiments with tumor-cell suspensions in rats and rabbits. Cancer 1951;4:610-618.
Question 56
A 40-year-old man sustains a scapular body fracture after an all-terrain vehicle accident. Which of the following is the most commonly associated injury?
Explanation
Question 57
When comparing gait parameters between a patient with an anterior cruciate ligament (ACL) deficiency to a patient with a normal knee, the patient with an ACL deficiency has which of the following? Review Topic
Explanation
Question 58
Which of the follow scenarios is most likely to be amenable to a complete repair of a massive rotator cuff tear? Review Topic
Explanation
Question 59
Figures 1 through 3 demonstrate the MRIs obtained from a 36-year-old man with an injury to the elbow. The expected result of nonsurgical treatment would be weakness of
Explanation
The axial T2-weighted MRIs demonstrate a distal biceps rupture. The increased signal is noted superficial to the brachialis muscle and adjacent to the biceps tuberosity. The distal biceps tendon is not seen in the distal cuts and has retracted proximally. The physical examination of patients with these injuries show abnormal contour of the arm and tenderness in the antecubital fossa. The hook test is a provocative maneuver that documents biceps integrity. When performing the maneuver, the examiner attempts to hook a finger around the distal biceps tendon while the patient actively supinates with the elbow held in flexion. Nonsurgical treatment has been documented to result in an average loss of 40% of supination strength and 30% of elbow flexion strength. Repair is optimal within several weeks of injury. The alternative options would not occur with a distal biceps rupture.
Question 60
9A 9B 9C 9D Figures 9a through 9d are the radiographs of a 21-year-old woman who is involved in a high-speed motor vehicle collision and sustains an isolated right closed-foot injury. Before surgery, the patient is advised about the relatively poor long-term outcomes associated with this injury. What is the most common reason for functional limitations after surgical treatment in this scenario?

Explanation
When a displaced talar neck fracture occurs, the rate of osteonecrosis is high; however, many revascularize the talus without collapse. A nonunion can occur but is less common than osteonecrosis and arthritis. A varus malunion can be debilitating and lead to subtalar arthritis. In a fracture with the talar body dislocated posteromedially (such as in this example) neurologic deficits in the tibial nerve distribution are common but typically improve with urgent
reduction. Studies show that posttraumatic subtalar arthritis is common after this injury and is the most likely cause of long-term functional impairment.
RECOMMENDED READINGS
Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. PubMed PMID: 15292407. View Abstract at PubMed
Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 10 THROUGH 12

10A

10B

10C
Figure 10a is the radiograph of a 30-year-old man who sustained an injury in a motor vehicle collision.
Question 61
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Baumhauer JF: Superficial peroneal nerve entrapment. Foot Ankle Clin 1998;3:439-446.
Question 62
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
Explanation
The incidence of pediatric hip dysplasia is approximately 1 per 100 live births, with hip dislocation present in 1 in 1000 births. Two surgical approaches primarily are used for surgical reduction in the dislocated pediatric hip: the modified medial approach as described by Weinstein and the
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. Orthopaedic Knowledge Update: Pediatrics 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. View Abstract at PubMed
Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
Question 63
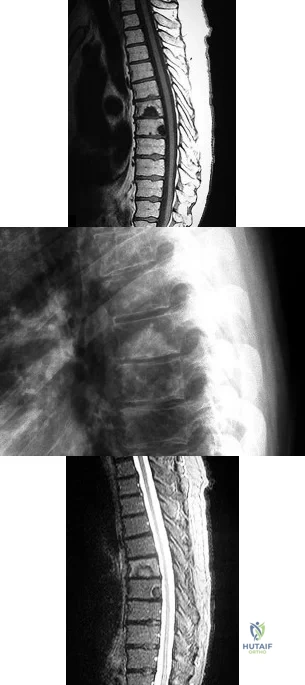
A B C What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
Explanation
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. View Abstract at PubMed
Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. View Abstract at PubMed
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29

Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
Question 64
During head-on motor vehicle collisions occurring at highway speeds, airbag-protected individuals have a decreased rate (as compared to non-airbag protected individuals) of all of the following EXCEPT:

Explanation
Question 65
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 66
The comparative outcomes of needle aponeurotomy (NA) and collagenase Clostridium histolyticum (CCH) use in the treatment of Dupuytren contracture indicate that patients treated with CCH have
Explanation
A. Proximal row carpectomy
B. Vascularized bone graft
C. Radial shortening osteotomy
D. Capitate shortening osteotomy
Osteonecrosis of the capitate is a rare condition that presents with an insidious onset of dorsal wrist pain. When nonsurgical treatment fails to alleviate symptoms, surgical intervention is appropriate. When collapse of the capitate is present, partial excision of the capitate with interposition, partial wrist arthrodesis, or wrist denervation can be considered. In the absence of collapse, capitate-preserving options are available. Vascularized grafting is a mainstay of treatment. Grafting with distal radius vascularized grafts based on the 1,2 intercompartmental supraretinacular artery or the 4 + 5 extensor compartment artery and second metacarpal graft based on the first dorsal metacarpal artery have been described.
Question 67
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following? Review Topic
Explanation
Question 68
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?

Explanation
Question 69
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
REFERENCES: Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861.
Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 70
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 71
below depicts the radiograph obtained from a year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 72
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10°. Initial management should consist of
Explanation
REFERENCES: Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 73
A year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 74
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 75
A 20-year-old collegiate pitcher has had a 5-month history of shoulder pain while throwing, decreased velocity, and difficulty with location of his pitches despite multiple attempts at rest. He reports no traumatic event. Examination with his throwing arm abducted at 90 degrees reveals external rotation to 110 degrees and internal rotation to 70 degrees when compared with his nonthrowing shoulder which has external rotation to 95 degrees and internal rotation to 85 degrees. He has a positive O'Brien's sign, positive modified Jobe's relocation test, full rotator cuff strength, no obvious muscular atrophy, and no scapular winging. Radiographs of the affected shoulder show no abnormalities. What is the next most appropriate step in management? Review Topic
Explanation
Question 76
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?
Explanation
REFERENCES: Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746.
Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Reiber GE, Smith DG, Wallace CM, et al: Effect of therapeutic footwear on foot reulceration in patients with diabetes: A randomized controlled trial. JAMA 2002;287:2552-2558.
Question 77
A 47-year-old man who is an avid tennis player and laborer has had one year of shoulder pain and weakness. His pain occurs at night and radiates to the deltoid laterally. The patient denies any anterior based pain. He reports no prior surgeries and has been managed with steroid injections and physical therapy. On examination, he has full passive motion with significant weakness with external rotation. His neurologic examination is unremarkable. MRI evaluation reveals a posterior-superior rotator cuff tear with Goutallier grade 4 fatty infiltrate in the supraspinatus and infraspinatus with retraction beyond the glenoid. He is concerned about the lack of rotation of his arm and reports that this disability creates significant disability with his occupation as a mason. What is the best next step?
Explanation
Question 78
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?
Explanation
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 480.
Question 79
-What is the most appropriate next treatment step?
Explanation
Based on the patient’s signs and symptoms, the most likely diagnosis is osteomyelitis of the spine. The imaging studies do not reveal a herniated disk, which would be unusual in someone of this age. Aneurysmal bone cysts would involve the posterior elements with a more expansive lesion of bone, whereas this lesion involves primarily the body and anterior column. Hemangioma would likely not be present with systemic signs or symptoms and has a more characteristic coarse trabecular pattern on radiographs and scans. Given the likelihood that this patient has osteomyelitis of the spine, blood cultures may yield an organism about 50% of the time. If cultures are negative, an image-guided biopsy is warranted. A diagnosis needs to be established before treatment such as extension casting or bracing is rendered. Open biopsy may still be needed if needle biopsy is not diagnostic, but this is not the first treatment option. A chest CT scan is not appropriate as a first step when a tumor is presumed and a diagnosis has not been established.
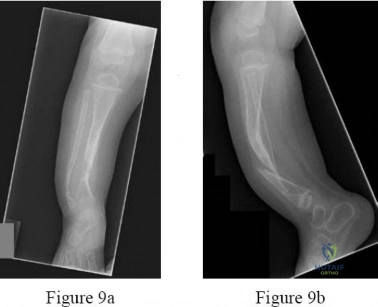
Question 80
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?

Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 81
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 82
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701.
Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg
1997;5:240-248.
Bundschuh C, Modic MT, Kearney F, et al: Rheumatoid arthritis of the cervical spine: Surface-coil MR imaging. Am J Roentgenol 1988;151:181-187.
Question 83
A 43-year-old man has had right groin pain for the past 3 months. A radiograph, CT scan, and biopsy specimen are shown in Figures 18a through 18c. What is the most likely diagnosis?
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 71-92.
Question 84
Figures 51a and 51b show subluxation of the
Explanation
REFERENCES: Rowland SA: Acute traumatic subluxation of the extensor carpi ulnaris tendon at the wrist. J Hand Surg Am 1986;11:809-811.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1026-1027.
Question 85
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?
Explanation
REFERENCES: Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330.
Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830.
Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop 1999;364:220-226.
Question 86
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?
Explanation
(a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthroplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem.
REFERENCES: Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic femoral fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.
Question 87
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 88
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 89
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
REFERENCES: Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Gertzbein SD: Metastatic spine tumors, in Herkowitz HN, Dvorak J, Bell G, et al (eds): The Lumbar Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 792-802.
Question 90
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management? Review Topic
Explanation
Question 91
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
Explanation
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.


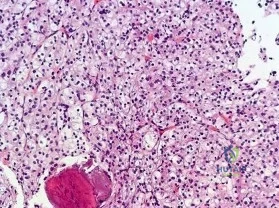
Question 92
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
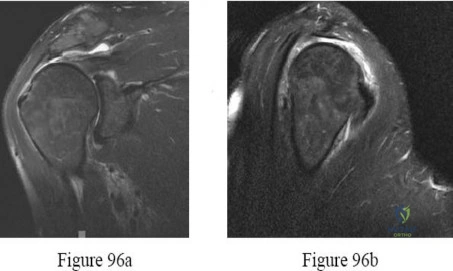
Question 93
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 94
Which factor is most important when attempting to prevent interbody graft subsidence?
Explanation
Osteoporosis can affect all aspects of spinal stability and is the most critical factor regarding spinal implant failure. Burring of the end plates may decrease strength of the interface with the uncovering of "softer" cancellous bone. Increasing the surface contact area may help prevent subsidence but is not as important as bone quality. Stress shielding through rigid fixation may lead to construct failure.
RECOMMENDED READINGS
Benzel E (ed): Biomechanics of Spine Stabilization. Rolling Meadows, IL, American Association of Neurological Surgeons, 2001, pp 446-447.
Goldhahn J, Reinhold M, Stauber M, Knop C, Frei R, Schneider E, Linke B. Improved anchorage in osteoporotic vertebrae with new implant designs. J Orthop Res. 2006 May;24(5):917-25. PubMed PMID: 16583445. View Abstract at PubMed
Question 95
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 96
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
Explanation
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
Question 97
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
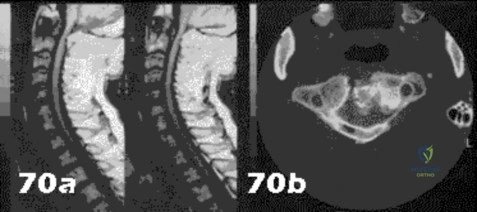
Explanation
Question 98
A 17-year-old boy with left spastic hemiplegia secondary to cerebral palsy is being evaluated for persistent swan neck deformities of the affected hand. Splinting has been tried with some improvement, but the patient does not want to wear the splints any more. On physical examination, he demonstrates full extension of the metacarpophalangeal (MCP) joints, 30° of hyperextension of the proximal interphalangeal (PIP) joints, and flexion of the distal interphalangeal (DIP) joints when he attempts to actively extend his digits. He is able to initiate flexion at the PIP joints with his MCP joints held in neutral extension. He has equal PIP flexion when the MCP joints are extended and flexed. What is the most appropriate surgical treatment to address his swan neck deformity?
Explanation
This patient demonstrates full extension of the MCP joints when he actively extends his fingers, indicative of overpull of the extrinsic finger extensors. This clinical scenario can be corrected by a central slip tenotomy. A terminal tendon release is used to address a Boutonnière deformity. The patient does not demonstrate intrinsic tightness (equal PIP flexion while the MCP flexed and extended), therefore his swan neck would be unlikely to respond to intrinsic lengthening. Dorsal rerouting of the lateral bands is performed for a Boutonnière deformity. A central slip tenotomy would balance the extension forces between the PIP and DIP joints.
Question 99
A 67-year-old man with right shoulder osteoarthritis (OA) remains symptomatic despite a course of nonsurgical treatment. A CT scan of the shoulder shows eccentric posterior glenoid wear with 10° of retroversion. What is the appropriate management of this glenoid bone loss during surgery for an anatomic total shoulder arthroplasty?
Explanation
glenoid bone grafting may be considered for glenoid retroversion >15°.
Question 100
What is the theoretical advantage of an open subpectoral technique of tenodesis of the long head of the biceps tendon compared to arthroscopic soft-tissue tenodesis techniques? Review Topic
Explanation
