Orthopedic Board Review MCQs: Lower Extremity Trauma & Arthroplasty | Part 155
Key Takeaway
This page presents Part 155 of a comprehensive orthopedic surgery board review quiz, featuring 100 high-yield MCQs. Designed for orthopedic surgeons and residents preparing for OITE/AAOS board certification exams, it offers interactive study and exam modes to master critical topics like Ankle, Foot, Knee, Fracture, and Arthroplasty for success.
About This Board Review Set
This is Part 155 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 155
This module focuses heavily on: Ankle, Arthroplasty, Foot, Fracture, Knee.
Sample Questions from This Set
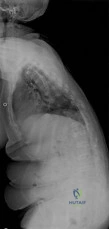
Sample Question 1: A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?...
Sample Question 2: You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an...
Sample Question 3: A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?...
Sample Question 4: A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months...
Sample Question 5: A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?
Explanation
REFERENCES: Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Timins ME: MR imaging of the foot and ankle. Foot Ankle Clin 2000;5:83-101.
Question 2
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
REFERENCES: AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. http://www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf
The Orthopaedic Surgeon’s Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. http://www.aaos.org/about/papers/ethics/1204eth.asp
AdvaMed Code of Ethics on Interactions with Health Care Professionals 2005. http://www.advamed.org/MemberPortal/searchresults.htm?query=Advamed%20Code%20of%20Ethics%20on%20Interactions%20with%20Health%20Care%20Professionals%202005
Question 3
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?
Explanation
REFERENCES: Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Question 4
A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months with persistent pain at the fracture site with ambulation. Examination reveals healed wounds with no erythema, warmth or tenderness. Erythrocyte sedimentation rate and C-reactive protein levels are within normal limits. Radiographs taken at that time are shown in Figure B. What is the next best treatment step?

Explanation
Tibial delayed union can be defined as lack of union from 20-26 weeks post-injury, while nonunion is defined as lack of healing at >9mths post-injury, or absence of progressive signs of healing on radiographs for 3 consecutive months. Persistent pain is a symptom of nonunion. ESR and CRP are performed to rule out infection.
Bhandari et al. performed a blinded, multicenter trial on 622 reamed tibial nails and 604 unreamed tibial nails. In closed fractures, patients in the unreamed nail group were at greater risk of primary events than the reamed nail group. There was no difference in groups for open fractures. Primary events were defined as bone-grafting, implant exchange/removal, dynamization, and debridement.
Hak reviewed aseptic tibial nonunion. They discuss exchanged reamed nailing for diaphyseal nonunion, adjunctive plate fixation for metaphyseal nonunion, and nail removal and plating for metadiaphyseal nonunion, external fixation for infected nonunion and distraction osteogenesis of defects.
Figure A shows a mid-diaphyseal tibial fracture Figure B shows nonunion following
IM nailing of the fracture. Illustration A shows union following exchange nailing with a larger 12mm diameter nail.
Incorrect Answers:
Question 5
A 16-year-old boy sustains a twisting injury to the left knee while wrestling. MRI scans are shown in Figures 22a through 22c. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 6
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
REFERENCES: Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Kour AK, Looi KP, Phone MH, et al: Hand infections in patients with diabetes. Clin Orthop Relat Res 1996;331:238-244.
Question 7
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
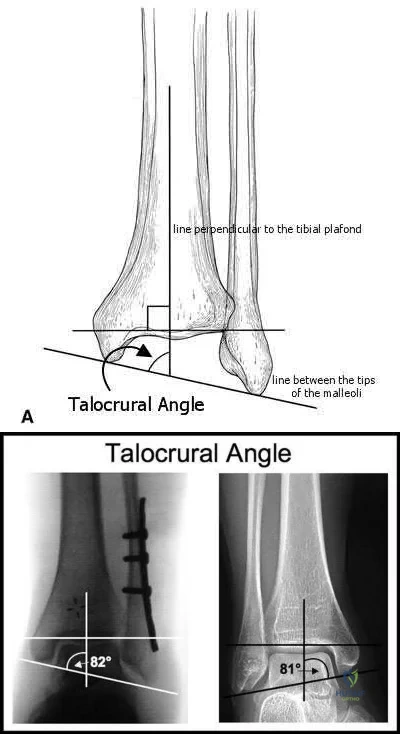
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
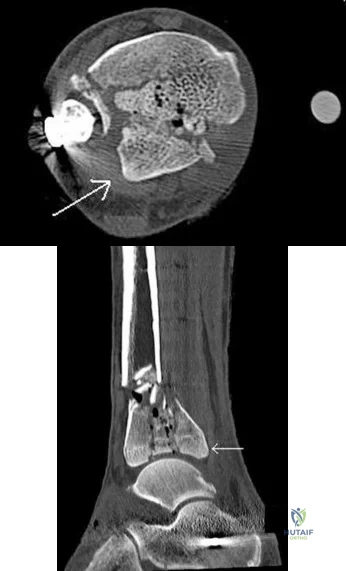
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

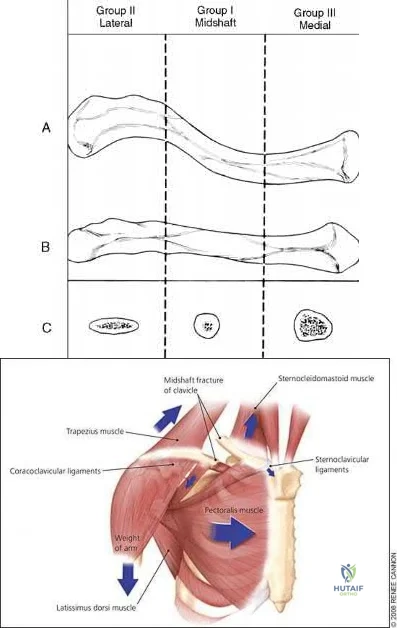
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 8
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries
of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703.
Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Hasler CC, von Laer L: Prevention of growth disturbances after fractures of the lateral humeral condyle in children. J Pediatr Orthop B 2001;10:123-130.
Question 9
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
REFERENCE: Ruedi T, Murphy WM (eds): AO Principles of Fracture Management. New York, NY, Thieme, 2000, p 221.
Question 10
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 11
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 12
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 13
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management? Review Topic
Explanation
and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses.
Question 14
Integrins function in which of the following ways?
Explanation
Integrins are a large family of heteromeric cell surface receptors composed of non-covalently bound alpha and beta subunits which interact with extracellular matrix molecules, serum constituents and various adhesion molecules. Specifically, aVß3 is a type of integrin found on osteoclasts that attaches to bone by coupling with vitronectin.
Bikle reviews the cause of bone loss during periods of unloading. They state the during periods of rest, integrin expression is decreased, leading to disuse osteoporosis. They argue that drugs that selectively regulate the integrin signaling pathway may
reverse bone loss during periods of disuse.
Illustration A shows an example of an osteoclast attaching to bone via the integrin aVß3.
Incorrect
1:
This
is
the
function
of osteocytes.
2:
This
is
the
function
of osteoblasts.
3:
This
is
the
function
of
osteoprogenitor cells.
Question 15
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 16
- In a fatigue test, the maximum stress under which the material will not fail, regardless of how many loading cycles are applied, is defined as
Explanation
Question 17
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 18
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
REFERENCES: Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496.
Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 19
What is the standard interval for placement of an anterolateral portal in ankle arthroscopy?
Explanation
Question 20
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 21
In an isolated ankle syndesmotic injury, the fibula is unstable in the incisura fibularis of the tibia. In what direction is the fibula most unstable?

Explanation
The first referenced article by Xenos et al found that stress lateral radiographs have more interobserver reliability than stress AP/mortise radiographs and that two syndesmotic screws are stronger than one.
The referenced article by Candal-Couto et al is a biomechanical study that found more anterior-posterior instability in a syndesmosis injury model, and more ankle instability is noted with syndesmosis injury and a concomitant deltoid injury. The referenced article by Zalavras et al is an excellent review article on ankle syndesmosis injuries.
Question 22
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of Review Topic
Explanation
Question 23
This reporting avoids a ceiling and floor effect, where most of the respondents score either at the top or the bottom of the assessment scale.
Explanation
The only accurate statement is that, at 1 month, patients in group 3 are more likely to live longer than patients in group 1 and 2.
The Kaplan-Meier curve is a statistical method used in survivorship analysis to estimate survival rates at different time points. The horizontal axis depicts the time points and the vertical axis depicts the probability of survival. At a given time point, greater survivorship is demonstrated by higher values on the vertical axis.
Kocher et al. reviewed clinical epidemiology and biostatistics relevant in orthopaedic
surgery. They reported that survivorship data are typically analyzed with use of the Kaplan-Meier method. This analysis is used when the actual date of the end point is known. A survivorship curve can be plotted to illustrate the percentage of patients still alive after the intervention.
Petrie et al. reviewed statistics, terminology and the principles involved in simple data analysis, and outlines areas of medical statistics that have gained
prominence in recent years in orthopaedic papers. The authors provide an insight into some of the more common errors that occur in published orthopaedic journals and which are frequently encountered at the review stage in papers submitted to the Journal of Bone and Joint Surgery.
Figure A depicts a Kaplan-Meier curve for 3 groups of patients undergoing 3 different interventions.
Incorrect Answers:
When evaluating patient-reported outcomes in spine surgery, the Patient- Reported Outcomes Measurement Information System (PROMIS) has been found to have what differences compared to other assessment tools?
Communication failures have been associated with increased treatment costs, increased complications, and delays in patient care.
The leading cause of medical errors, wrong-site surgeries, diagnostic delays and loss to follow-up is attributed to communication errors. Studies have shown that this directly leads to increased complications, increased treatment costs, and delays in patient care. In the surgical setting, the performance of the pre-surgical time-out affords clarification of the treatment plan, confirmation of the procedure and site, and an opportunity for the team to address any concerns.
Weller et al. reviewed barriers to effective teamwork in healthcare delivery. They found that effective communication across all team members, inclusive training, and the creation of democratic teams can reduce treatment delays and minimize complications. They concluded that all team members should have a shared understanding of the situation when involved in patients care.
Lingard et al. performed a prospective study determining the feasibility of a preoperative 10-item checklist discussion including nurses, surgeons, and anesthesiologists. They reported that the discussion usually took place prior to bringing the patient to the OR and took on average 3.5 minuted. Overall, the guided discussion was very well received by participants and provided an opportunity to inform providers of the patient's information to address potential problems. The authors cited that variations in workflow patterns as a potential barrier to widescale implementation of the checklist discussion.
Incorrect answers:
The outcomes of three novel interventions are investigated and the preliminary results are depicted in Figure A. Which of the following statements is most accurate?
Linezolid acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome.
Linezolid is a type of oxazolidinone, a relatively newer class of antibiotics that are active against multidrug-resistant staphylococci, streptococci, and enterococci. Although many antimicrobial agents affect or disrupt protein synthesis in bacteria, linezolid is unique in that it disrupts protein synthesis at its origin rather than later in the cascade. It achieves this by binding to the
50S subunit of the bacterial ribosome, preventing the formation of the initiation complex.
Swaney et al. performed a study to investigate the mechanism of action of linezolid. They found that linezolid inhibits the formation of the initiation complex in bacterial translation systems by preventing the formation of the N- formylmethionyl-tRNA-ribosome-mRNA ternary complex.
Thompson et al. performed a study on the efficacy of various antibiotics in treating periprosthetic joint infections (PJI). They administered oral linezolid with or without oral rifampin, intravenous vancomycin with oral rifampin, intravenous daptomycin or ceftaroline with or without oral rifampin, oral doxycycline, or sham treatment at human- exposure doses for 6 weeks in a mouse model of PJI. They found that oral-only linezolid-rifampin and all intravenous antibiotic-rifampin combinations resulted in no recoverable bacteria and minimized reactive bone changes. Additionally, although oral linezolid was found to be the most effective monotherapy, all oral and intravenous antibiotic monotherapies failed to clear infection or prevent reactive bone changes.
They concluded that the oral-only linezolid-rifampin option might reduce venous access complications and health-care costs.
Illustration A is a diagram depicting the mechanism of action of various antibiotics.
Incorrect Answers:
50S subunit of the bacterial ribosome, preventing protein chain elongation by inhibiting peptidyl transferase activity of the ribosome.
elongation by blocking aminoacyl translocation.
Failure of effective communication in the surgical setting has been associated with what?
Unfractionated heparin works in the coagulation cascade by promoting the ability of antithrombin III to inhibit factors IIa, III, Xa.
Heparin works by binding to and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. It is metabolized by the liver. The risks associated with the use of unfractionated heparin include bleeding and heparin induced thrombocytopenia (HIT). The reversal agent is protamine sulfate.
Agnelli et al. reviewed direct thrombin inhibitors for the prevention of VTE after major orthopaedic surgery. They reported widespread use, however, limitations in the use of unfractionated heparin and low-molecular-weight heparins. They highlighted that direct thrombin inhibitors (Ximelagatran) inactivate thrombin without requiring any plasma cofactor, inhibit both free
and fibrin-bound thrombin, and do not appreciably bind to plasma proteins. They concluded that the features of rapid absorption, conversion, bioavailability, low variability, dose-time, food independency, and the predictable anticoagulant activity make direct thrombin inhibitors an attractive antithrombotic agent especially for prolonged out-of hospital prophylaxis.
Kwong et al. reviewed the efficacy and safety of fondaparinux, a selective factor Xa inhibitor and reported its efficacy and safety in 4 phase III clinical trials. They reported fondaparinux usage resulted in an overall 55% decrease in the risk of venous thromboembolism (VTE) relative to the low-molecular- weight heparin enoxaparin without increasing the incidence of clinically relevant bleeding, which was similarly low for both agents. They concluded
that the superior efficacy of fondaparinux relative to enoxaparin is the result of its unique mechanism of action, clinical pharmacology.
McLynn et al. investigated the risk factors and chemoprophylaxis for VTE in elective spine surgery. They reported that independent risk factors for VTE included greater age, male gender, increasing body mass index, dependent functional status, lumbar spine surgery, longer operative time, perioperative blood transfusion, longer length of stay, and other postoperative
complications. The majority of patients received unfractioned heparin and they observed this did not significantly influence the rate of VTE, but was associated with a significant increase in hematoma requiring a return to the operating room. They concluded that there is insufficient evidence to support the routine use of chemoprophylaxis in low-risk patients, and recommended full consideration of risks and benefits after elective spine surgery.
Figure A depicts the coagulation cascade, with the factor circled in red (IIa) being the target of unfractionated heparin, through its effect on antithrombin III.
Incorrect Answers:
Which of the following antibiotics acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome?
Acetaminophen inhibits prostaglandin E2 production through its effect on interleukin-1 beta. It exerts its effects on the central nervous system.
Multimodal pain management has become an increasingly important consideration in total joint arthroplasty recovery, namely in regard to minimizing opioid requirements while optimizing pain control and patient satisfaction. Given the negative side effects and increasing scrutiny on narcotic use, modalities that help to decrease post-operative narcotic requirements have become a major focus and include nonsteroidal anti- inflammatories, selective COX-2 inhibitors, gabapentinoids, local anesthetic blocks, and acetaminophen. Acetaminophen acts directly the central nervous system, providing both pain relief and antipyretic effects. It does so by inhibiting prostaglandin E2 production through the blockade of interleukin-1 beta.
Jinnah et al. performed a comparison of two multimodal pain regimens used for postoperative pain control in total joint arthroplasty patients. They hypothesized that using a multimodal pain protocol focusing on periarticular injections including liposomal bupivacaine would have improved results when compared with a parenteral opioid- based regimen. They found a decrease in length of stay and rate of discharge to skilled nursing facilities with the implementation of a novel multimodal protocol. They concluded that a multimodal approach inclusive of periarticular injection can lead to a reduced
length of stay.
Politi et al. performed a prospective randomized trial comparing the use of intravenous versus oral acetaminophen in total joint arthroplasty. They found that IV acetaminophen did not provide a significant difference in pain relief except within the first 0-4 hours. They concluded that IV acetaminophen does not provide a significant benefit when compared to the oral form, which is also less expensive.
Incorrect Answers:
Which of the following agents results in blood anticoagulation by exerting inhibitory effects on the factor circled in the color red in Figure A?
Based on the stress-strain curve in Figure A, ceramic has the highest modulus of elasticity.
Young's modulus is a measure of the stiffness (ability to resist deformation) of a material in the elastic zone that is calculated by measuring the slope of the stress-strain curve in the elastic zone. A higher modulus of elasticity indicates a stiffer material. Relative values of Young's modulus include: (1) ceramic, (2) alloy, (3) stainless steel, (4) titanium, (5)
cortical bone, (6) matrix polymers, (7) PMMA, (8) polyethylene, (9) cancellous bone, (10) tendon/ligaments, and (11) cartilage.
Lang et al. published a review on the use of ceramics in total hip replacement. They report that properties of ceramic which make it particularly attractive for this application include its hardness, high compression strength, and excellent wettability. However, its low fracture toughness and linear elastic behavior make it prone to breakage under stress.
Figure A is a stress-strain curve, the slope of which is used to determine Young's modulus.
Incorrect Answers:
Which of the following medications work by inhibiting prostaglandin E2 production through interleukin-1 beta?
A power analysis determines the minimum number of patients needed in a study to show a clinically significant difference. It should be performed before starting the study.
Power is the probability of finding a significant association if one truly exists. It is defined as 1 minus the probability of a type 2 error (beta) and is generally set to 80% meaning that we are willing to accept a 20% chance of a type 2 error. A power analysis will determine the minimum number of patients that shows a clinically significant difference. The minimum number of patients should be determined prior to initiating a study. Calculation of power after a study has been completed is controversial and discouraged.
Vavken et al. performed a review on the management of confounding in controlled orthopaedic trials. They report that confounding occurs when the effect of exposure of an outcome is distorted by a confounding factor and will lead to spurious effect estimates in clinical studies. They performed a cross- sectional study of a sample of controlled trials reported in the orthopaedic literature in 2006. They conclude that only 30 studies reported that the had a power analysis performed.
Kocher et al. performed a review of clinical epidemiology and biostatistics as a primer for orthopedic surgeons. They report that a power analysis should be performed prior to initiating the study. This will ensure the study is appropriately powered and decrease the effects of chance. They conclude that when a study determines no significant effect the power of the study should be reported.
Incorrect Answers:
Based on the stress-strain curve in Figure A, which of the following materials has the highest modulus of elasticity?
The World Health Organization (WHO) defines osteopenia as a bone mineral density (BMD) that is between 1 and 2.5 standard deviations below young normal (T-score of - 1 to -2.5).
The WHO defines osteopenia as decreased BMD without fracture risk. Osteopenia is defined as a T-score of 1 to 2.5 standard deviations below young normals (-1 to -2.5), while osteoporosis is defined as a T-score of more than
Question 24
Which of the following statements is true regarding the superomedial fragment of an intra-articular calcaneus fracture?

Explanation
Question 25
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 26
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
REFERENCES: Harris WH, McCarthy JC, O’Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067.
Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Maloney WJ, Schmalzreid T, Harris WH: Analysis of long-term cemented total hip arthroplasty retrievals. Clin Orthop Relat Res 2002;405:70-78.
Question 27
Figure 100 is the MRI scan of a 52-year-old runner who has right knee pain that has been occurring 10 minutes into her run for 2 months. On examination, she has tenderness over the lateral epicondyle. Her Ober test result is positive. What is the most appropriate initial treatment? Review Topic
Explanation
Question 28
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?
Explanation
REFERENCE: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 29
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Explanation
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 30
The iliopectineal fascia runs between which of the following structures?
Explanation
REFERENCES: Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 31
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 32
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows
Explanation
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Vresilovic E, Hozack WJ, Rothman RH: Radiographic assessment of cementless femoral components: Correlation with intraoperative mechanical stability. J Arthroplasty 1994;9:137-141.
Question 33
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
Explanation
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If it were injured, the result would not be weakness of interphalangeal joint extension.
Question 34
Figures 71a and 71b/ are the MR images of a 65-year-old man who dislocated his shoulder. What is his most likely chief symptom?
Explanation
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation. Loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction and external rotation, which results in difficulty raising an arm. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve that supplies sensation to the lateral aspect of the shoulder, not the anterior aspect. Recurrent instability is uncommon unless there is a labral tear or massive subscapularis tear. The biceps muscle is not viewed in the MR images, and a complete proximal biceps tendon rupture would be uncommon in the setting of an anterior shoulder dislocation.

CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
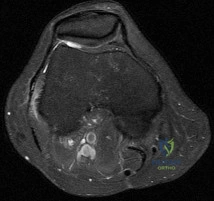
Figures 72a through 72e are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0 degrees
to 90 degrees and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted.
Question 35
An obese (BMI = 35) 72-year-old woman with diabetes mellitus, hyptertension and a 22-pack-year smoking history is scheduled to undergo posterior spinal fusion from T10 to S1 with a pedicle subtraction osteotomy at L3 for the spinal deformity seen in Figure 1. Which of the following risk factors is most predictive of major complication following surgery Review Topic
Explanation
The surgical treatment of adult spinal deformity often requires multilevel arthrodesis with complex osteotomies including three column osteotomies such as pedicle
subtraction (PSO) and vertebral column resection (VCR). They can involve both anterior and posterior surgical approaches. Surgical time, blood loss, length of hospital stay, and length of recovery can be greater than it is for the more common degenerative conditions.
Auerbach et al. characterized the risk factors for the development of major complications in patients undergoing 3-column osteotomies for adult spinal deformity correction. They also aimed to determine whether the presence of complications affected the ultimate clinical outcome. They found age > 60 years, > or = 3 comorbid conditions and preoperative sagittal imbalance of = 40mm was associated with a major complication. However, the presence of a major complication did not affect the ultimate clinical outcomes at 2 years or more.
Daubs et al. conducted a retrospective analysis of forty-six patients = 60 years of age who underwent major spinal deformity surgery requiring a minimum 5-level arthrodesis procedure to determine the rate of complication and outcomes. The overall complication rate was 37% and the major complication rate was 20%. Increasing age was a significant factor (p<0.05) in predicting the presence of a complication, while presence of comorbidities was found to have no association.
Figure A is a standing preoperative lateral radiograph of the spine demonstrating a thoracic kyphosis of ~25° and thoracolumbar kyphosis of ~25°. Illustration A demonstrates proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO.
Incorrect Answers:
Question 36
The mother of a 3-month-old infant states that she has difficulty positioning the infant’s legs during diaper changes. Examination reveals limited abduction of both hips and a negative Ortolani sign. A radiograph reveals bilaterally dislocated hips. Initial management consists of guided reduction in a Pavlik harness, with weekly follow-up. Figures 57a and 57b show the radiograph and CT scan obtained after 6 weeks in the harness. Management should now consist of
Explanation
REFERENCES: Jones GT, Schoenecker PL, Dias LS: Developmental hip dysplasia potentiated by inappropriate use of the Pavlik harness. J Pediatr Orthop 1992;12:722-726.
Atar D, Lehman WB, Grant AD: Pavlik harness pathology. Isr J Med Sci 1991;27:325-330.
Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 37
Which ligament attaches to the bony fragment identified by the CT image arrows in Figures 42a and 42b?
Explanation
The distal tibiofibular syndesmosis is a ligamentous complex that consists of the AITFL, PITFL, intertransverse ligament (ITL), and IOL. The PITFL originates on the posterior inferior aspect of the tibia (Volkmann tubercle) and inserts on the lateral malleolus. The AITFL originates on the anterolateral aspect of the tibia (Chaput tubercle) and inserts on the distal anterior aspect of the fibula (Wagstaffe tubercle). The ITL is a group of fibers running transversely just inferior to the PITFL. As a group, these structures maintain the appropriate tibial plafond and talus relationship throughout physiologic range of motion.
RECOMMENDED READINGS
Carr JB. Malleolar fractures and soft tissue injuries of the ankle. In: Browner BD, Alen LM, Peter TG, Jupiter JB, et al. Skeletal Trauma. 3rd ed. Philadelphia, PA: Saunders; 2003:2309. Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg.2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46


A 46-year-old healthy right-hand-dominant man falls and sustains the injury shown in Figures 43a and 43b.
Question 38
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?
Explanation
REFERENCE: Sutton DC, Siveri CP, Cotler JM: Initial evaluation and management of the spinal injured patient, in Cotler JM, Simpson JM, An HS, et al (eds): Surgery of Spinal Trauma. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 113-126.
Question 39
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 40
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 41
Figure 48 shows the radiograph of a 17-year-old boy who sustained a gunshot wound to his forearm. There is a small entrance wound on the volar surface. The exit wound is dorsal and more than 15 cm in size, with loss of skin and an extensive amount of devitalized muscle hanging out of the wound. Vascular supply to the hand is excellent, the ulnar and median nerves are intact in the hand, but the radial sensory nerve function is absent. After repeated surgical debridements of the wound and bone, definitive treatment for the fracture would most likely be which of the following? Review Topic

Explanation
Question 42
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 43
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Explanation
Question 44
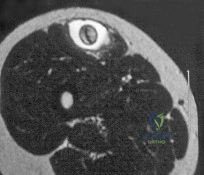
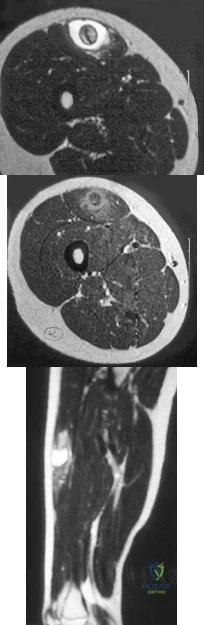
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management? Review Topic
Explanation
Question 45
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 46
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of

Explanation
Question 47
The dose of the chemotherapeutic agent doxorubicin (Adriamycin) is limited by which of the following factors?
Explanation
REFERENCE: Brockstein BE, Peabody RD, Simon MA: Soft tissue sarcomas, in Vokes EE, Golomb HM (eds): Oncologic Therapies. Berlin, Springer, 1999, pp 925-952.
Question 48
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?
Explanation
REFERENCES: Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Wells D, King JD, Roe TF, Kaufman FR: Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop 1993;13:610-614.
Question 49
A 24-year-old man with weakness and atrophy of the thumb for 12 months has very slight numbness on the radial side of his thumb that is constant and not progressing. He has no other hand or finger numbness.His 2-point static sensory examination is unremarkable in all digits and there is marked atrophy of the thenar muscles. His carpal tunnel provocative tests are negative. He has no symptoms on the opposite hand and otherwise is in excellent health. Which next step will most likely reveal the diagnosis?
Explanation

Question 50
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
Explanation
8 • American Academy of Orthopaedic Surgeons
DISCUSSION: Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
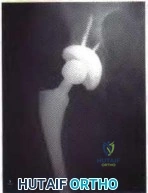
Figure 3a Figure 3b
Question 51
What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
Explanation
(SBQ12TR.86) Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intraoperatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by >or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Question 52
Figure 29 is the radiograph of a 30-year-old man who sustained an isolated tibial shaft fracture. What is the most common deformity with nonsurgical management?

Explanation
discrepancies are also common. Here the fibula acts as a strut, preventing valgus collapse but predisposing to varus collapse. Valgus and procurvatum is the typical deformity in proximal tibial fractures.
Question 53
Figure 16 shows the radiograph of a 75-year-old man who has progressive groin pain and a limp following total hip replacement. At revision surgery, the anterior and posterior columns of the acetabulum are noted to be intact. The optimal surgical technique for acetabular component reconstruction is a
Explanation
REFERENCES: Petrera P, Rubash HE: Revision total hip arthroplasty: The acetabular component. J Am Acad Orthop Surg 1995;3:15-21.
Lachiewicz PF, Poon ED: Revision of a total hip arthroplasty with a Harris-Galante porous-coated acetabular component inserted without cement: A follow-up note on the results at five to twelve years. J Bone Joint Surg Am 1998;80:980-984.
Question 54
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?
Explanation
REFERENCES: Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.
Question 55
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
REFERENCES: Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547.
Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 297, 331-332.
Question 56
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
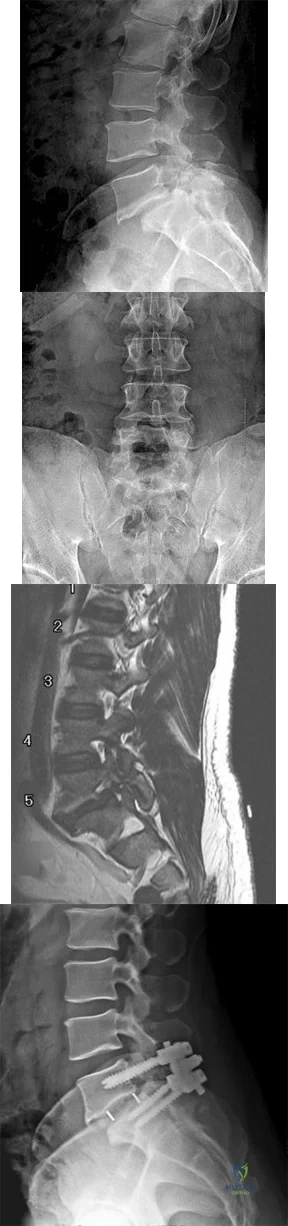
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 57
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 58
A college football player performs bicep curls as part of his weight lifting routine. During the flexion phase of the curl, what term defines the type of muscle contraction?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Evans WJ: Effects of exercise on senescent muscle. Clin Orthop 2002;403:S211-S220.
Question 59
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 60
Which of the following conditions routinely requires early surgical intervention in patients with Marfan syndrome? Review Topic
Explanation
Question 61
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
Question 62
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 63
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 64
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 65
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 66
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 67
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 295-297.
Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 379.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 23.
Ebraheim NA, Elgafy H, Xu R: Bone-graft harvesting from iliac and fibular donor sites: Techniques and complications. J Am Acad Orthop Surg 2001;9:210-218.
Question 68
A 45-year-old male falls off his motorcycle and injures his arm. AP and lateral radiographs reveal an ulnar shaft fracture, 30 degrees apex anterior, and a radial head dislocation. Which direction is the radial head most likely dislocated?

Explanation
Question 69
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 70
- What is the treatment of choice for an adult who has an isolated fracture of the ulna at the junction of the distal and middle thirds, with 5 degrees apex dorsal angulation and 25% displacement?
Explanation
Question 71
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 72
After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?
Explanation
REFERENCES: Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492.
Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 73
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?
Explanation
L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root.
REFERENCES: Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Aeschbach A, Mekhail NA: Common nerve blocks in chronic pain management. Anesthesiol Clin North Am 2000;18:429-459.
Question 74
What is the most appropriate treatment?
Explanation
A common postsurgical problem after TKA is a sudden increase of pain that typically occurs about 2 to 3 weeks after surgery. ESR findings are not reliable during the acute postsurgical period. A CRP level exceeding 100 mg/L during the acute postsurgical period is a joint aspiration indication. If the patient does not have sepsis, there is no emergency. This pain is likely attributable to too much activity during physical therapy. Observation is recommended for this patient.
Question 75
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 181-193.
Question 76
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m 2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?

Explanation
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 77
An otherwise healthy year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 78
A 12-year-old boy with a family history of neurofibromatosis has anterolateral bowing of the left tibia. He has no pain and is ambulatory. Radiographs show a narrowed medullary canal but intact cortices. Treatment should consist of which of the following?
Explanation
REFERENCES: Vander Have KL, Hensinger RN, Caird M, et al: Congenital pseudarthrosis of the tibia.
J Am Acad Orthop Surg 2008;16:228-236.
Vitale MG, Guha A, Skaggs DL: Orthopaedic manifestations of neurofibromatosis in children: An update. Clin Orthop Relat Res 2002;401:107-118.
Question 79
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 80
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 81
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 82
Figure 1 is the radiograph of an otherwise healthy 68-year-old man with a 4-year history of increasing global left knee pain. He has noticed stiffness, and despite physical therapy, bracing and nonsteroidal anti-inflammatory drugs, he has continued to develop worsening symptoms and progression in his deformity. Physical examination demonstrates 80°of flexion and a 10° flexion contracture. What is the best next step?
Explanation
Question 83
Figures 169a through 169c show the radiograph and MRI scans of a 74-year-old woman who has had back and bilateral leg pain for the past 6 months. Nonsurgical management has failed to provide relief. What is the best option for surgical treatment? Review Topic

Explanation
Question 84
Two weeks after undergoing total knee arthroplasty, a 68-year-old woman experiences moderate, yet worsening, knee pain. Upon examination, she can walk with a cane but she has swelling with mild reactive erythema. She has a well-healed incision with no drainage. A review of her medications reveals the she has been taking warfarin and has an international normalized ratio (INR) of 4.0. Her erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are slightly elevated, and radiographs are unremarkable other than for effusion. What is the most likely diagnosis?
Explanation
This patient likely has a hemarthrosis related to INR elevation. The slight elevations in ESR and CRP are likely attributable to the nature of the surgery itself rather than an infection, and the mild reactive erythema is likely attributable to the hemarthrosis.
Question 85
What is the most likely contributory factor to this patient's problem?
Explanation
Proximal humeral epiphysiolysis (little leaguer’s shoulder) is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Factors that contribute to the condition include excessive throwing, improper throwing mechanics, and muscle-tendon imbalance. Radiographic findings typically are normal but may indicate subtle widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms. Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to throwing is implemented until the patient’s condition returns to baseline. This protocol has a long-term success rate exceeding 90%. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The most common cause of this condition is overuse, as is seen in pitchers who throw all year. Internal rotation deficit and internal impingement is typically a finding in older athletes without open physes. This patient had no evidence of rotation deficit upon examination, making this diagnosis unlikely.
Question 86
A nonambulatory verbal 6-year-old child with spastic quadriplegic cerebral palsy has progressive bilateral hip subluxation of more than 50%. There is no pain with range of motion, but abduction is limited to 20 degrees maximum. An AP radiograph is seen in Figure 34. Management should consist of
Explanation
REFERENCES: Presedo A, Oh CW, Dabney KY, et al: Soft-tissue releases to treat spastic hip subluxation in children with cerebral palsy. J Bone Joint Surg Am 2005;87:832-841.
Miller F, Bagg MR: Age and migration percentage as risk factors for progression in spastic hip disease. Dev Med Child Neurol 1995;37:449-455.
Question 87
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O’Brien’s active compression test. What is the next most appropriate step in the diagnosis of this patient? Review Topic
Explanation
Question 88
Figures 81a through 81c show the MRI scans of a 53-year-old man who has experienced a long history of progressively worsening right-sided back pain with radiation to the buttocks and right lower extremity. Examination reveals weakness and hyperreflexia in the right lower extremity. He reports intermittent episodes of urinary incontinence. What is the most appropriate surgical approach? Review Topic

Explanation
Question 89
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
McCarthy JC, Noble PC, Schuck MR, et al: The role of labral lesions to development of early degenerative hip disease. Clin Orthop 2001;393:25-37.
Question 90
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
REFERENCE: Gerber C, Myer DC, Schneeberger AG, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 91
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 25-34.
Question 92
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
REFERENCES: Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281.
Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Watson HK, Ryu J: Evolution of arthritis of the wrist. Clin Orthop 1986;202:57-67.
Question 93
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 94
Which of the following is considered a limitation of the Short Form 36 (SF-36) general health status instrument when applied to musculoskeletal conditions?
Explanation
Multilingual validated translations have been produced in addition to international population data sets. The survey can be patient self-administered via office visit, mail, or telephone. A bias of lower over upper extremity function with regard to outcome measures employing the SF-36 has been demonstrated. Limits on the detection of certain changes in quality of life status may impose ceiling and floor effects on analysis and interpretation.
Question 95
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 96
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 97
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 98
At the time of arthroscopy, a 9-year-old boy was found to have a Watanabe type II discoid lateral meniscus. What is the most appropriate treatment? Review Topic
Explanation
Question 99
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 100
A 51-year-old woman who underwent a total knee arthroplasty 14 months ago for severe degenerative arthritis now reports progressive pain, swelling, and buckling of the knee. She must use crutches and is unable to negotiate stairs. Laboratory testing reveals a normal erythrocyte sedimentation rate and C-reactive protein. Radiographs of the patient are shown in Figures 17a through 17c. What is the most important test to further evaluate this problem?
Explanation
REFERENCES: Stiehl JB: Patellar instability in total knee arthroplasty. J Knee Surg 2003;16:229-235. Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
