Orthopedic Surgery MCQs: Trauma, Hip Arthroplasty & Elbow | Part 153

Key Takeaway
This page presents Part 153 of a comprehensive Orthopedic Surgery board review quiz. It features 100 high-yield MCQs, formatted like OITE/AAOS exams, designed for orthopedic residents and surgeons preparing for certification. It offers detailed explanations and references for optimal exam preparation and mastery.
About This Board Review Set
This is Part 153 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 153
This module focuses heavily on: Arthroplasty, Deformity, Dislocation, Elbow, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?...
Sample Question 2: A 41-year-old woman with diabetes mellitus fell onto her outstretched arm and sustained an injury to the right elbow. Radiographs are shown in Figures 53a and 53b. What is the most appropriate management?...
Sample Question 3: A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?...
Sample Question 4: What factor is associated with a higher risk of dislocation after total hip arthroplasty?...
Sample Question 5: A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite ade...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 2
A 41-year-old woman with diabetes mellitus fell onto her outstretched arm and sustained an injury to the right elbow. Radiographs are shown in Figures 53a and 53b. What is the most appropriate management?

Explanation
Question 3
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?
Explanation
REFERENCE: Haentjens P, Autier P, Collins J, et al: Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women: A meta-analysis. J Bone Joint Surg Am 2003;85:1936-1943.
Question 4
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
Explanation
Question 5
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
REFERENCES: Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84.
Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Ganz R, Krushell RJ, Jacob RP, Kuffer J: The antishock pelvic clamp. Clin Orthop 1991;267:71-78.
Question 6
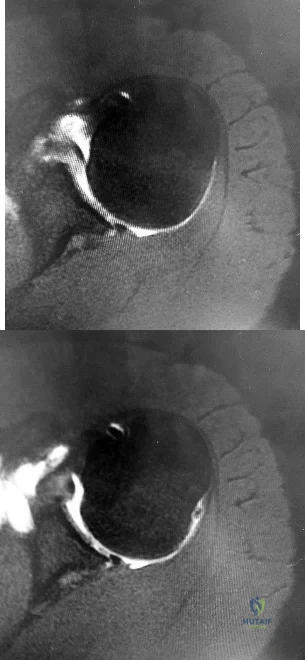
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?

Explanation
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 7
When performing a radioscapholunate (RSL) fusion for posttraumatic radiocarpal arthritis, excision of the distal pole of the scaphoid will cause a decrease in
Explanation
RSL arthrodesis is a motion-sparing option for posttraumatic radioscaphoid or radiolunate arthritis when the midcarpal joint is preserved. Preserving the midcarpal joint allows the dart-thrower motion to remain. Mühldorfer-Fodor and associates reported that the rates of nonunion for RSL fusion were reduced by excision of the distal pole of the scaphoid. Multiple studies have shown increased radial and ulnar deviation with excision of the distal pole of the scaphoid; excision of the triquetrum further increases the radial-ulnar arc of motion. Bain and associates and Pervaiz and associates reported increased wrist
flexion-extension arcs with distal scaphoid and triquetrum excisions in cadaveric models; other authors have reported no difference.
Question 8
-The center of rotation of the knee can be best described as
Explanation
Question 9
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 10
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle? Review Topic
Explanation
(SBQ12FA.1) Figure A is a radiograph of a healthy, independent 51-year-old male. He is treated with immediate open reduction internal fixation to prevent which of the following complications?

Fracture non-union
Avascular necrosis
Skin necrosis
Plantar flexion weakness
Ankle stiffness
Figure A shows an avulsion fracture of the calcaneal tuberosity. Immediate open reduction and internal fixation is required to prevent wound complications.
Displaced avulsion fractures of the calcaneal tuberosity should be managed urgently to prevent necrosis of the soft tissues overlying the heel. In these injuries, the Achilles tendon is securely attached to the fractured tuberosity. Urgent closed reduction and casting is usually not possible due to the power and proximal pull of the triceps surae. Surgical fixation is required. The best treatment modality is open reduction and bone-to-bone fixation with screws. Closed reduction and percutaneous pinning fixation is not strong enough to provide a stable fixation of the tuberosity.
Lui reported on avulsion fractures of the bony insertion of the Achilles tendon at the calcaneus. He stated that screw fixation alone is not sufficient for repair of these injuries. His technique involved two suture anchors used capture the small bone fragment to the calcaneus. This allowed for the pull of the triceps surae to be neutralized and early physical therapy.
Hess et al. looked at a case series of calcaneal tuberosity avulsion fractures that were
treated in a delayed fashion. All three patients with posterior tuberosity calcaneal avulsion fractures developed skin necrosis because of a delay in treatment.
Figure A shows a displaced posterior tuberosity calcaneal avulsion fracture. Illustration A shows skin breakdown overlying the posterior tuberosity calcaneal avulsion fracture.
Incorrect Answers:
Question 11
Studies have shown that the parents and grandparents of people with developmental dysplasia of the hip (DDH)
Explanation
The hip arthritis RR is significantly increased in patients with DDH (RR = 82.4; P < 2e-16), their parents (RR = 2.22; P = 0.0003), and their grandparents (RR = 1.33; P = 0.011). The THA RR also is significantly increased for patients with DDH (RR = 1168; P < 3e-08) and their grandparents (RR = 2.06; P = 0.01). First-degree and second-degree relatives were not at higher risk for knee arthritis or knee arthroplasty. The RR for DDH was significantly increased for first-degree relatives (RR = 12.1; P < 0.000001) and siblings (RR = 11.9; P < 0.000001).
Question 12
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%. A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
Explanation
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
Question 13
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?
Explanation
REFERENCES: Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Eckman MH, Greenfield S, Mackey WC, et al: Foot infections in diabetic patients: Decision and cost-effectiveness analyses. JAMA 1995;273:712-720.
Question 14
During the ilioinguinal approach to the pelvis, the corona mortis artery must be identified and ligated if present. The corona mortis artery joins the external illiac artery with which other major artery?

Explanation
Question 15
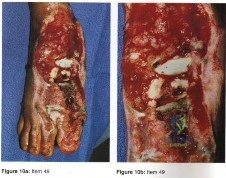
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 16
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
Explanation
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
Question 17
-A 10-year-old boy sustained a displaced Salter-Harris type II supination/plantar flexion fracture of the left ankle. He underwent closed reduction under conscious sedation; however, postreduction radiographs showed continued 5-mm anterior widening of the tibial physis. What is the most likely cause of the widening?
Explanation
Question 18
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
REFERENCES: Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 19
- In revision hip arthroplasty, which of the following is the 5- to 10-year reported graft failure rate when using structural acetabular allografts in the repair of acetabular deficiencies?
Explanation
Question 20
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. Knee range of motion is between 0° and 70°. What is the most appropriate treatment option?

Explanation
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibial plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated versus nonaccelerated rehabilitation programs have demonstrated no significant differences in long-term results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 21
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
Explanation
Question 22
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
REFERENCES: Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Bansal P, Deehan DJ, Gregory RJ: Diagnosing the acutely locked knee. Injury 2002;33:495-498.
Question 23
Figures 174a and 174b are the radiograph and clinical photograph of a 64-year-old obese woman (body mass index [BMI] of 48) who has controlled diabetes and hypertension. She has failed nonsurgical treatment and a weight loss program. She is considering total knee arthroplasty (TKA). What is the most significant postsurgical risk for this patient?
Explanation
The literature has demonstrated increased risk for complications among obese patients undergoing TKA (10%-30%). An evaluation of TKA among obese patients revealed 3- to 9-fold higher incidence of wound complications and deep-seated infection. Belmont and associates demonstrated that patients with a BMI higher than 40 are at higher risk for overall complications than patients with a BMI lower than 25, with a particularly high risk for developing local wound complications and infection. An increased risk for thromboembolic complications was not shown among obese patients undergoing TKA. Patient-reported outcome scores among obese patients undergoing TKA are equivalent to those of nonobese
patients. There are conflicting data regarding the outcome and survivorship following TKA for obese patients. Although some studies show a difference in patient-reported outcomes at differing postsurgical intervals, most obese patients undergoing TKA are satisfied with the procedure.
Question 24
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
Explanation
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
Question 25
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic

Explanation
Question 26
Figure 1 is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?
Explanation
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A "V sign" (Figure 2) is evident, indicating dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress. Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 3 through 5.






Question 27
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 28
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of Review Topic

Explanation
Question 29
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 82-85.
Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 638-639.
Question 30
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 31
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing’s specific antigen (CD99) negative, and keratin negative. What is the next step in management?
Explanation
REFERENCES: Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Lems P, Primus G, Anastas J, Doherty D, Montag AG, Peabody TD, Simon MA: Oncologic outcomes of primary lymphoma of bone in adults. Clin Orthop 2003;415:90-97.
Question 32
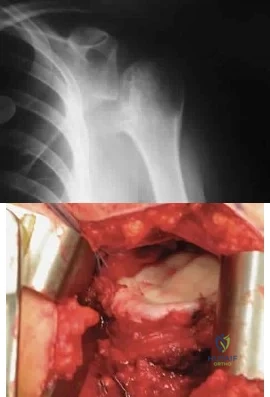
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?
Explanation
REFERENCES: Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23.
Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Oreck SL, Burgess A, Levine AM: Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption. J Bone Joint Surg Am 1984;66:758-763.
Question 33
A patient who underwent total knee arthroplasty 6 years ago now reports knee pain for the past 3 days following dental surgery. Cultures of the aspirate are positive for Staphylococcus epidermidis. Management should consist of
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Goldman RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 34
The vascular supply to the medial meniscus comes primarily from what artery?
Explanation
REFERENCE: Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, p 4.
Question 35
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 36
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Fiddian NJ, Kling RJ: The winged scapula. Clin Orthop 1984;185:228-236.
Question 37
When a Workers' Compensation patient recovers after an injury to a point that further restoration of function is no longer anticipated, he or she is said to have reached which of the following?
Explanation
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner. 3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined. 4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation. 5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
Question 38
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 39
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 40
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 41
The patient fails nonsurgical treatment for this condition. What is the best next step?
Explanation
Osgood-Schlatter disease is an apophysitis of the tibial tubercle. This condition is present in males more than females and occurs prior to fusion of the tubercle to the epiphysis of the tibia. The apophysis is cartilaginous before 11 years of age and begins to ossify between 11 and 14 years of age. The apophysis fuses to the epiphysis between 14 and 18 years of age (females before males). Symptoms are pain and swelling, and pain is worse with jumping and running. Initial treatment should consist of activity limitation, ice, quadriceps and hamstring stretching, and possible bracing. NSAIDs may be used to control symptoms. When symptoms resolve, the athlete may return to activities. In fewer than 10% of cases, symptoms persist after skeletal maturity. For these patients, excision of the ossicle will usually resolve symptoms. The ossicle is usually not part of the tendon attachment and can be resected without detaching any of the patellar tendon.
RECOMMENDED READINGS
Vergara-Amador E, Davalos Herrera D, Moreno LÁ. Radiographic features of the development of the anterior tibial tuberosity. Radiologia. 2016 Feb 22. pii: S0033-8338(16)00019-9. doi: 10.1016/j.rx.2016.01.005. [Epub ahead of print] English, Spanish. PubMed PMID: 26917430. View Abstract at PubMed
Frank JB, Jarit GJ, Bravman JT, Rosen JE. Lower extremity injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2007 Jun;15(6):356-66. Review. PubMed PMID: 17548885. View Abstract at PubMed
Question 42
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 43
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.
Question 44
A 3-year-old boy who was treated with Ponseti-method casting demonstrates supination of the affected foot during swing phase of gait. His ankle has 20 degrees of active and passive dorsiflexion and 45 degrees of plantar flexion. What is the most appropriate treatment? Review Topic
Explanation
Question 45
A year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 46
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of
Question 47
Which component position is associated with poor patellar tracking during total knee arthroplasty (TKA)?
Explanation
Internal malrotation of the femoral or tibial component is associated with lateral tracking of the patella in TKA. Lateral placement of the femoral component and medial placement of the patella component can aid in preventing lateral tracking of the patella. Varus alignment of the proximal tibia has not been associated with patella maltracking.







RESPONSES FOR QUESTIONS 106 THROUGH 109
Immobilization/nonsurgical management
Irrigation and debridement
stage reimplantation total knee arthroplasty (TKA)
Increased constraint/polyethylene exchange
Revision of the femoral component only
Revision of the tibial component only
Revision of both components
Revision of the patellar component
Select the treatment listed above that most appropriately addresses each scenario described below.
Question 48
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 49
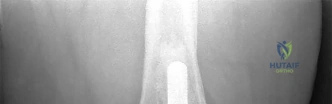
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
Explanation
flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant.
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Fehring TK, Odum S, Griffin WL, et al: Early failures in total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 50
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 51
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 52
A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile. Management at this time should consist of
Explanation
Question 53
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?
Explanation
REFERENCES: Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1995;23:746-750.
Question 54
Following total elbow arthroplasty, patients should be instructed to Review Topic
Explanation
Question 55
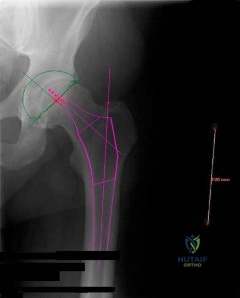
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
REFERENCES: Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels’ Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 56
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
REFERENCES: Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
Stein F, Grabias SL, Deffer PA: Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am 1971;53:1432-1436.
Question 57
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?
Explanation
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 58
When performing a cruciate-retaining total knee arthroplasty, trial components are inserted. The knee comes to full extension but is tight in flexion. The surgeon should consider
Explanation
In this scenario, the flexion gap needs to be increased. Increase in flexion gap can be accomplished by downsizing the femoral component and increasing posterior tibial slope. In posterior cruciate-retaining TKA procedures, recession or release of the posterior cruciate ligament can loosen the flexion gap, allowing for an increase in flexion. Flexing the femoral
component tightens the flexion gap, and downsizing the tibial insert thickness decreases flexion and extension gaps, while resection of the distal femur only increases the extension gap.

CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
Figure 52 is the standing anteroposterior radiograph of a 55-year-old man who has a 5-year history of daily left knee pain with weight-bearing activities. He denies night pain or symptoms of instability. Upon examination his range of motion is 0 to 140 degrees. He has a mild, fully correctable varus deformity and a negative Lachman test result. He has failed nonsurgical treatment.
Question 59
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 60
The flexor hallucis longus tendon is at greatest risk of injury with a lateral-to-medial drill or screw during fixation of what structure?

Explanation
Question 61
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 62
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
Explanation
and degenerative joint disease.
Question 63
Fully dense alumina and zirconia materials have been used as bearing materials in hip arthroplasty to provide greater wear resistance than polished metallic surfaces. Although both have shown reduced wear clinically, what concerns continue to exist about the use of zirconia?
Explanation
REFERENCES: Clarke IC, Manaka M, Green DD, et al: Current status of zirconia used in total hip implants. J Bone Joint Surg Am 2003;85:73-84.
Haraguchi K, Sugano N, Nishii T, et al: Phase transformation of a zirconia ceramic head after total hip arthroplasty. J Bone Joint Surg Br 2001;83:996-1000.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 64
A 53-year-old man with insulin-dependent diabetes has the ulcer on his heel shown in Figure 9. Radiographs and an MRI scan are consistent with osteomyelitis of the calcaeus, contiguous with the ulcer itself. Arterial flow to the foot is adequate. Management should consist of

Explanation
Question 65
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
REFERENCES: Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 66
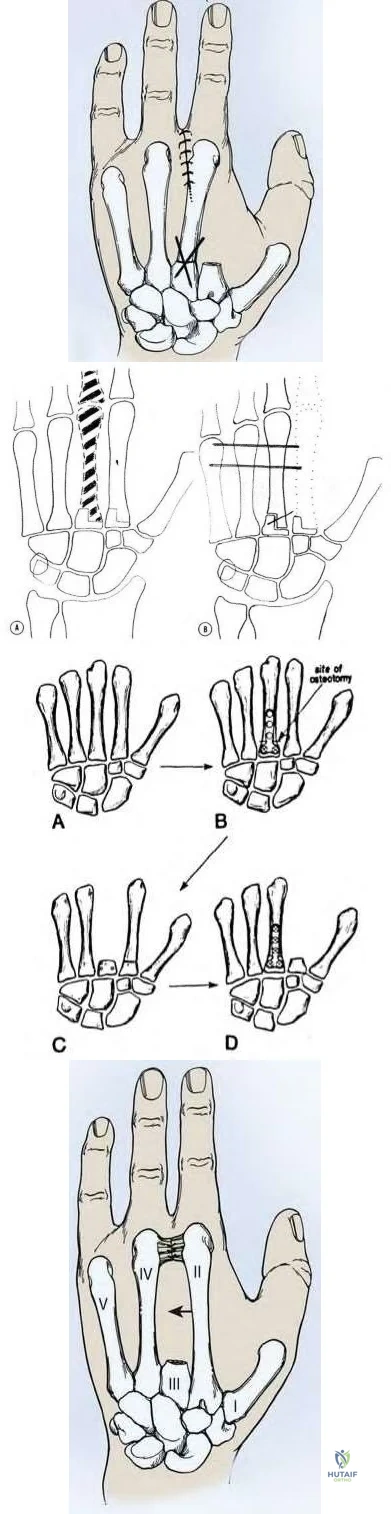
5cm from the carpometacarpal joint. The attached deep transverse intermetacarpal ligaments are sacrificed. To prevent scissoring of the remaining digits and small objects falling through the gap between index and ring fingers, which of the following procedures should be performed?

Explanation
With amputation of the middle or ring metacarpals, small objects fall through the gap and the adjacent fingers scissor. For single central ray defects, techniques to reduce the gap include transposition of the index finger (for middle ray amputation), small finger (for ring ray amputation), complete removal of the metacarpal (without leaving a proximal metacarpal base stump) to allow the bases of index and ring metacarpals to migrate together and reconstruction of the deep transverse metacarpal ligament. The technique of index transposition may vary depending on the osteotomy (straight vs step-cut) and fixation (K wires vs plate) as seen in the illustrations below.
Muramatsu et al. describe bony transposition for reconstruction after ray amputation for malignancy. The advantage is immediate closure of the space. The disadvantages include prolonged postoperative immobilization until union, malrotation (leading to scissoring), mal-tension of tendon (because of different metacarpal heights), and delayed or nonunion.
Lyall et al. advocate total middle ray amputation. They believe that leaving the metacarpal base behind leads to difficulty in aligning the adjacent rays as the index and ring must angulate over the bony obstruction to close the distal gap, leading to scissoring. They believe that index transposition leaves an abnormally wide 1st web space and a remnant 2nd metacarpal stump that can protrude dorsally.
Figure A is an AP radiograph of the right hand showing a destructive lesion of the proximal phalanx of the middle finger abutting the metacarpophalageal joint. Figure B is a STIR coronal MRI image showing the tumor mass extending into surround soft tissue. Illustration A is a diagram showing index transposition for middle ray amputation using a straight osteotomy and crossed K-wires. Illustration B is a diagram showing index transposition using a step-cut osteotomy and multiple K-wire fixation to the adjacent metacarpals. Illustration C is a diagram showing index transposition using a straight osteotomy and plate fixation. Illustration D is a diagram showing an alternative technique of suturing deep transverse metacarpal ligaments together to close the gap.
Incorrect Answers
A 65-year-old man fell and injured his right wrist. Radiographs taken in the emergency room are seen in Figure A. He was treated as a sprain and no further follow-up was planned. He sustained 2 minor falls over the next 6 years and his wrist pain recurred. Recent radiographs are seen in Figure B. Surgical treatment that will best address his symptoms and preserve wrist motion consists of

Anterior and posterior interosseous neurectomy
Scaphotrapezialtrapezoidal (STT) fusion
Complete wrist arthrodesis
Proximal row carpectomy
Four-corner fusion with scaphoidectomy
Four-corner fusion with scaphoidectomy is indicated for Stage III SLAC wrist.
Surgical treatment of SLAC wrist is stage dependent. Stage I disease (scaphoid-radial styloid arthritis) is treated with AIN/PIN neurectomy. This procedure can also be done in addition to other bony procedures for Stages II-III disease. Stage II (scaphoid-entire scaphoid facet) is treated with PRC or scaphoid excision with 4-corner fusion (4CF). Stage III (capitolunate arthritis with proximal migration of the capitate into the scapholunate interval) is treated with either scaphoidectomy with 4CF or total wrist fusion.
Some other conditions exist: If capitolunate arthritis exists, PRC is contraindicated and 4CF is performed. If radiolunate arthritis exists, both PRC and 4CF are contraindicated and total wrist fusion is performed. If both radiolunate and capitolunate surfaces are preserved, then either PRC or a 4CF may be performed.
Cohen et al. compare PRC with 4-corner fusion plus scaphoid excision. PRC is technically easier, but leads to shortening of the carpus with weakness and incongruity exists between the capitate and lunate fossa of the distal radius. Scaphoid excision and four-corner fusion maintains carpal height and preserves the radiolunate relationship, but is more technically demanding, there is risk of nonunion, and it requires longer postop immobilization. Pain relief is more reliable following 4-corner fusion.
Figure A shows scapholunate ligament disruption. Figure B shows late stage SLAC wrist. There is capitolunate arthritis but no radiolunate arthritis.
Illustration A shows an example of PRC. Illustration B shows an example of 4CF and scaphoidectomy.
Incorrect Answers

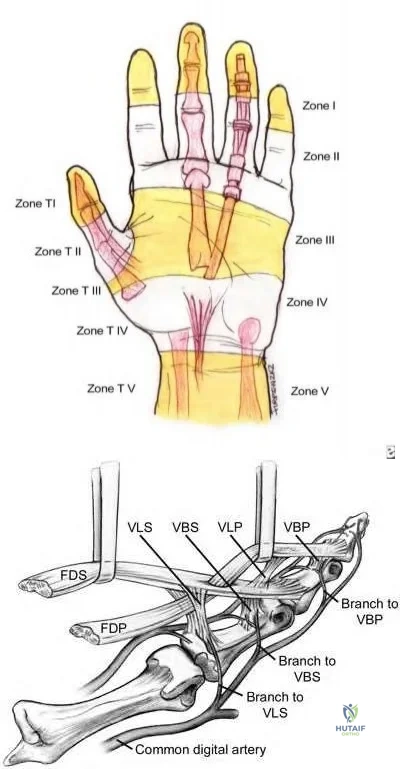
Which of the following statements is true regarding zone II flexor tendon injuries?
At this level, FDS and FDP are located within separate tendon sheaths
FDS repair has not been shown to improve outcomes
Improved gliding is seen with repair of 1 slip of FDS compared to repairing both slips
Repairing FDS does not affect post-operative digit strength
FDP repair has not been shown to improve outcomes
In zone II flexor tendon injuries, repairing only one slip of FDS has been shown to improve gliding when compared to repair of both slips.
Zone II flexor tendon injuries have notoriously had poor outcomes secondary to high rates of adhesion formation at the pulleys. However, new advances in post-operative rehabilitation have significantly improved outcomes to the point where it is no longer considered "no man's land." Management of the FDS has been a source of controversy. In the past, the FDS was occasionally excised to theoretically make more room for the FDP. This has now been largely abandoned and the FDS is repaired whenever possible. Whether or not to repair both slips of FDS remains controversial, with in vitro data suggesting that gliding resistance is improved if only one slip is repaired.
Zhao et al. review the effect of partial vs. complete FDS excision following repair of FDP for zone II flexor tendon injuries. Preserving the whole FDS resulted in a significantly larger increase in gliding resistance after FDP repair than did full or partial FDS removal, which were not significantly different from each other.
Illustration A shows the zones of flexor tendon injury. Note that zone II injuries occur between the FDS insertion and the distal palmar crease. Illustration B shows the anatomy of the flexor tendons in detail. Video V shows a technique for repair of zone II injuries.
Incorrect Answers:
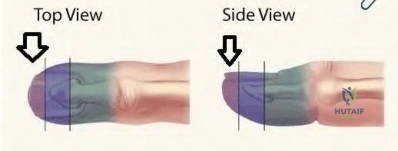
A 6-year-old girl sustains transverse amputations through her long and ring fingertips after getting her hand caught in a lawn mower. She presents to the emergency room 30 minutes after the injury with the amputated tissue which was placed on ice in a waterproof bag. On physical exam the amputation levels are found to be 6 millimeters distal to the lunula. The wounds are noted to be fairly
contaminated with no evidence of exposed bone. Skin defects are less than 1 centimeter. Which of the following is the most appropriate management at this time?
Emergent replantation of the amputated parts
Revision amputation through the distal interphalangeal joint
Thorough irrigation and debridement followed by elective Moberg advancement flaps
Thorough irrigation and debridement followed by elective Z-plasty reconstruction
Thorough irrigation and debridement, soft dressing application, and followup within 1 week
Distal fingertip amputations can be successfully managed with local wound care and healing by secondary intention if no bone is exposed and the soft tissue defects are minimal. This is especially true in the pediatric population.
Distal fingertip amputations are common injuries seen in the emergency department. If bone is not exposed, the wounds can be successfully treated with local wound care and dressing changes, followed by soaks in a hydrogen-peroxide solution after 7-10 days. Some controversy exists in the pediatric population if the soft tissue loss is > 1 cm, with options for management including a V-Y advancement flap or conservative management with dressing changes.
Quell et al. review the results of 82 patients with fingertip amputations treated conservatively; 31 of the digits were treated with primary closure with or without shortening of bone and 54 digits were treated with semiocclusive dressings. No complications were observed, and all healed fingertips were well padded and painless.
Tupper et al. review sixteen patients with twenty fingertip injuries who underwent V-Y plasty for transverse fingertip amputations. Sensitivity was 73% of normal, with eight patients reporting hypersensitivity. Contrary to popular belief, they believe normal sensation following a V-Y plasty is not a reasonable expectation.
Illustration A shows the three levels of fingertip amputations. Zone I is distal to the phalanx; Zone II is distal to the lunula; and Zone III is proximal to the lunula.
Incorrect Answers:
Which of following malformations is most commonly associated with Poland's syndrome?

Figure E CORRECT ANSWER: 4
Figure D demonstrates symbrachydactyly which is most commonly associated with Poland's syndrome.
Poland's syndrome is a rare birth defect characterized by underdevelopment or absence of the chest muscle in conjunction with ipsilateral symbrachydactyly. Poland syndrome most often affects the right side of the body, and occurs more often in males than in females.
Ireland et al. reviewed 43 consecutive cases of Poland's syndrome, and reviewed the relevant literature up to that point. The authors state that the clinical features are variable but always include congenital aplasia and syndactyly, and the right side is affected more than the left. They also note that although the hand remains hypoplastic and functional capacity is limited by the inherent skeletal anomalies, surgical treatment improves functional capacity and cosmetic appearance in the majority of patients.
Van Heest summarizes normal formation and growth of the upper limb as a basis for understanding malformation, with the goal of providing a basic understanding of the evaluation necessary for appropriate counseling and referrals for treatment of the child with hand and upper extremity congenital deformities.
Incorrect Answers:
A 55-year-old male laborer comes in with a chief complaint of clumsiness with his right hand for the past 3 months including difficulty using a hammer while at work. He has had no injury to the right upper extremity. On physical examination, he has persistent small finger abduction/extension with finger extension and active adduction. An EMG is performed and demonstrates ulnar nerve conduction velocities of 31 m/sec (normal >52m/sec). The patient symptoms are most accurately described as:
Axonotmesis with ischemia origin
Axonotmesis with myelin disruption
Neurapraxia with ischemia origin
Neurapraxia with endoneurium disruption
Neurotmesis CORRECT ANSWER: 3
The history and clinical presentation are consistent with ulnar entrapment neuropathy at the level of the cubital tunnel. This would be classified as a neuropraxia with ischemia origin.
Compression injuries to the peripheral nerves are often the result of microvascular dysfunction as the nerves traverse a high to low pressure gradient. Peripheral nerve injury can be classified as neuropraxia, axonotmesis, and neurotmesis. Compressive neuropathies are typically neuropraxias, with local myelin damage but not compromise of the major components of the nerve. In axonotmesis, there is Wallerian degeneration and myelin loss distal to the site of injury. The most severe type is that of neurotmesis. Neurotmesis is composed of a spectrum of injury in which the endoneurium is always disrupted (perineurium or epineurium may be intact). The worst form of neurotmesis is that of nerve transection.
Elhassan et al. review the pathophysiology of cubital tunnel syndrome. They report nerve dysfunction results from ischemic changes secondary to compression. Compressive effects on the nerves can last greater than 24 hours, even after the source of compression has been removed.
Rempel et al. review the pathophysiology of peripheral nerve compression syndromes. The authors indicate that deforming pressures to nerves are often the result of stenotic soft tissue canal boundaries. This leads to interference with local microvasculature of the nerve itself.
Illustration A demonstrates the Wartenberg sign, where the patient has persistent small finger abduction/extension resulting from weakness of the 3rd palmar interosseous/small finger lumbrical.
Illustration B reveals clawing which results from overpowering of the intrinsic muscles by the extrinsic muscles; a tenodesis effect results in flexion of the PIP/DIP joints. This is more severe in ulnar nerve compression at Guyon’s canal. Illustration C shows the Froment sign, where the FPL attempts to compensate for a deficient pinch, because of weakness of the adductor pollicis. Illustration D demonstrates atrophy of the 1st dorsal webspace from chronic compressive changes. Illustration E demonstrates atrophy of the thenar compartment which is consistent with carpal tunnel syndrome.
Incorrect Answers:
Which of the following hand injuries seen in Figures A-E is most appropriately treated with a first dorsal metacarpal artery flap?

Figure E CORRECT ANSWER: 3
Figure C shows a dorsal thumb laceration with exposed tendon that would be most appropriately treated with a first dorsal metacarpal artery (FDMA) flap.
The first dorsal metacarpal artery is a branch of the radial artery that supplies the dorsal hand skin from the thumb metacarpal to the long metacarpal, as well as the skin on the dorsal surfaces of the thumb and index to the proximal interphalangeal joint. The flap is raised distal to proximal as an island flap containing the FDMA, branches of the radial nerve, fascia of the underlying interosseous muscle of the first web space, and skin overlying the MP joint and proximal phalanx of the finger. It is an excellent option for large soft tissue defects on either side of the thumb. In this case, skin grafting is contraindicated because of exposed tendon without paratenon.
Sherif et al. detail the anatomy of the first dorsal metacarpal artery. They found three consistent branches, including the radial, ulnar, and intermediate branch. In part II of their study, they review the results of 23 patients where the FDMA flap was used as a fasciocutaneous or fascial flap for the coverage of soft tissue hand defects.
Illustration A shows a FDMA flap being raised for coverage of a thumb defect. Incorrect Answers:
bone can be allowed to heal through secondary intention.

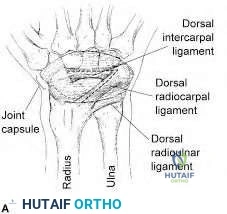
Figure A is a radiograph of a 35-year-old women who sustained an isolated left wrist injury after a fall onto an outstretched hand. She has been complaining of left dorsal wrist pain since the fall. Examination reveals a positive Watson's scaphoid shift test. What ligamentous structure is an important secondary stabilizer to prevent dorsal intercalated segment instability (DISI) deformity in this patient?

Transverse carpal ligament
Dorsal intercarpal ligaments
Triangular fibrocartilage complex
Dorsal lunotriquetral ligament
Volar lunotriquetral ligament
The integrity of the dorsal intercarpal ligaments is important in preventing dorsal intercalated segment instability (DISI) deformity and persistent scapholunate instability.
Scapholunate instability is the most common carpal instability. The primary stabilizing structure of the scaphoid and lunate bones is the scapholunate ligament, which is commonly injured with a fall on an outstretched hand.
Secondary stabilizers of the scaphoid and lunate include the dorsal intercarpal ligaments and the dorsal radiocarpal ligaments. Failure to recognize injury of these structures can cause persistent dorsal intercalated segment instability (DISI). This can predispose patients to a SLAC wrist and early wrist osteoarthritis.
Mitsuyasu et al. examined the role of dorsal intercarpal ligaments (DIC) in scapholunate instability. They showed that the DIC had an important role in stabilizing the scaphoid and lunate bones with static and dynamic movements. The authors of this study suggest that the DIC ligament should be assessed intraoperatively and consideration should be given to repair and/or reconstruction with surgical management of scapholunate ligament tears.
Viegas et al. showed that the dorsal intercarpal and the dorsal radiocarpal ligaments form a lateral V configuration over the dorsal wrist. This configuration acts as an indirect dorsal stabilizing effect on the scaphoid
throughout the range of motion of the wrist. Their integrity acts to ensure normal wrist kinematics.
Figure A shows an AP and lateral radiograph of the left hand. There is significant gapping between the scaphoid and lunate articulation. This is indicative of a complete scapholunate dissociation, however both wrists should be imaged as this deformity may exist without injury. Illustration A shows the anatomy of the dorsal intercarpal and the dorsal radiocarpal ligaments.
Incorrect Answers:
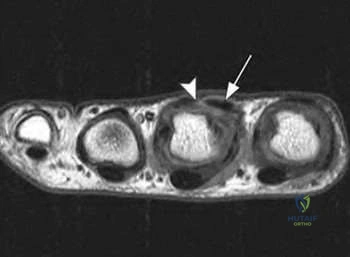
A 50-year-old patient presents with stiffness in her hand. A clinical photo is shown in Figure A. During surgical exposure, the neurovascular bundle is identified and dissected. What is the clinically most important pathologic structure to identify and what is its location relative to the neurovascular bundle in the digit?

Spiral cord which is central and superficial to the neurovascular bundle
Central cord which is midline and superficial to the neurovascular bundle
Retrovascular cord which is central and superficial to the neurovascular bundle
Spiral cord which is lateral and deep to the neurovascular bundle
Central cord which is lateral and deep to the neurovascular bundle
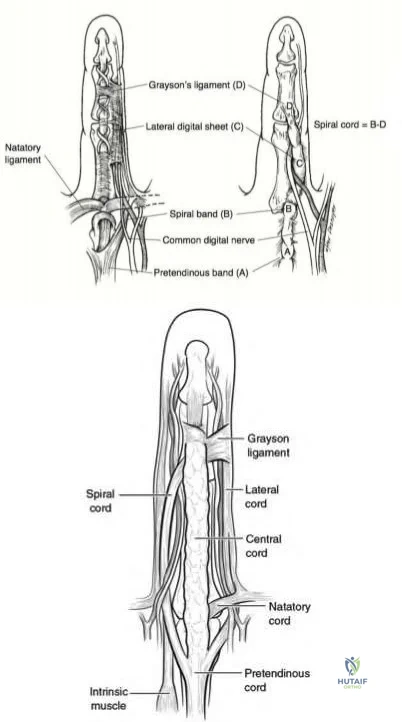
Based on clinical findings, the patient has evidence of Dupuytren’s contracture affecting her ring finger. Relative to the neurovascular bundle, the spiral cord will lie lateral and deep.
Dupuytren’s disease is a benign hand condition characterized by pathologic nodules and cords of existing fascial bands. The most clinically relevant structure in Dupuytren's disease, is the spiral cord. The spiral cord is the result of pathology of 4 structures: the middle layer of the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. The spiral cord is found predominantly at the palmodigital transition. The spiral cord displaces the neurovascular bundle centrally and superficially.
Benson et al. review the etiology, pathophysiology and treatment options for Dupuytren’s contracture. They highlight that while the pretendinous band is located volar and central to the neurovascular bundle in the palm, the spiral band and lateral digital sheath cause the neurovascular bundle to be displaced superficially and volarly as they become pathologically affected.
Black et al. review the pathoanatomy, diagnosis and management of Dupuytren's disease. They note that the spiral cord lies superficial to the neurovascular bundle proximal to the MCP joint. Distal to the MCP joint it passes deep to the bundle. At that location, the spiral cord lies lateral to the
neurovascular bundle as the lateral digital sheet becomes involved
Figure A demonstrates the cord formation that is characteristic of the pathologic Dupuytren’s condition. It is the central cord that causes contracture of the MCP, whereas the retrovascular and spiral cords cause contractures of the DIP and PIP respectively. Illustration A shows the relationship of spiral cord formation in Dupuytren's disease relative to the normal anatomy of the palmar fascia. The structures implicated in the formation of the spiral cord are the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. Cleland's ligament, more dorsally located, is spared in Dupuytren's disease. The neurovascular bundle is displaced superficially and towards the midline, as the pathological cord spirals around. Illustration B shows the presence of other affected structures, including the natatory ligament and the central band. The central band is an extension of the pretendinous cord and attaches to the base of the middle phalanx. It may insert onto the tendon sheath of the flexor tendon at this level. Formation of natatory cords cause webspace contractures. Formation of central cords lead to flexion contractures of the PIP. Illustration V is a video that provides an educational overview of Dupuytren's.
Incorrect Answers:
An infant is brought to your office for evaluation of his hands. Clinical photos are shown in Figures A and B. The clinical features are most consistent with a genetic mutation in which of the following:

Sonic Hedgehog (SHH)
FGFR2
FGFR3
PMP22
COL1A1 CORRECT ANSWER: 2
Based on the clinical features seen in the figures provided, the most likely syndrome is that of Apert syndrome, which is consistent with a mutation in FGFR2.
Apert syndrome is an autosomal dominant condition that gives rise to facial dysmorphism and complex syndactyly of the hands. The craniosynostosis that develops causes flattening of the skull and facial features.
Goldberg et al review congenital hand conditions and the malformations associated with them. They indicate that not only does identification allow for natural history to be better elucidated, but also timing of surgical intervention can be better gauged.
Figures A and B demonstrate clinical features consistent with Apert Syndrome. The “rosebud” hand is a complex syndactyly that affects the index, middle and ring fingers most commonly. Hypertelorism is exemplified with increased distance between the eyes; additionally, acrocephaly is noted with forehead broadening and skull flattening.
Incorrect Answers
1: Mutation in sonic hedgehog gene (SHH) is associated with a longitudinal deficiency of the radius. This is seen in conditions like TAR, Holt-Oram and VACTERL syndromes.
3: Mutation in FGFR3 leads to achondroplasia
4: Mutation in PMP22 gives rise to Charcot Marie Tooth syndrome 5: Mutation in COL1A leads to osteogenesis imperfecta
A 45-year-old patient presents with recurrence of radial sided wrist pain after undergoing a first dorsal compartment release about 3 months ago. The surgery was completed by one of your partners; operative reports indicate that the sheath was incised on the dorsal edge. On physical exam she is found to have normal appearing skin, a negative Tinel’s sign, and a positive Finklestein test. What is the most likely cause of the recurrence of her symptoms?
Development of neuroma
Complex regional pain syndrome
Failure to decompress the EPB sub-sheath
Failure to decompress the EPL sub-sheath
Failure to decompress the APB sub-sheath
Based on the history and clinical findings this patient has de Quervain’s tenosynovitis. The recurrence of her symptoms can be attributed to a failure to recognize and decompress the EPB sub-sheath.
De Quervain’s tenosynovitis is a stenosing inflammatory condition of the first dorsal compartment of the wrist (APL/EPB). Surgical release of the compartment is indicated after conservative measures have failed. At the time of the operation, the incision is made on the dorsal side of the sheath to prevent volar subluxation of the tendons. Failure to identify and release a distinct EPB sub-sheath or a separate fibro-osseous compartment of the APL can lead to a recurrence of symptoms.
Alegado et al. report a case of a patient with dysesthesias in the superficial radial nerve distribution 3 months after undergoing first dorsal compartment release for de Quervain’s tenosynovitis. They found a persistent fibrous remnant of the dorsal aspect of the sheath causing elevation of the superficial radial nerve. They recommend sheath excision or incision of the sheath at its dorsal attachment to avoid this complication.
Ashurst et al. report a case of a patient presenting with bilateral de Quervain’s tenosynovitis secondary to excessive text messaging. Conservative measures
afforded the patient complete symptomatic recovery. They recommend limitation of texting, in conjunction with other standard treatments, to treat text messaging- associated de Quervain’s tenosynovitis
Ilyas et al. review the etiology, diagnosis and management of De Quervain’s tenosynovitis. Non-surgical management is largely successful and includes splinting and cortisone injections. In refractory cases, surgical release of the first dorsal compartment is completed. They recommend meticulous care of the radial sensory nerve and identification of all separate sub-sheaths.
Illustration A shows an operative photo in a patient with multiple APL slips and an EPB that is hidden within a sub-sheath. Video V gives a brief overview of de Quervain’s tenosynovitis.
Incorrect Answers

A 28-year-old NFL running back complains of continued hand pain three days following an injury sustained while being tackled. He was splinted on the field. He has tenderness over the long finger metacarpal head, with subluxation of the extensor tendon into the intermetacarpal area during active metacarpophalangeal joint flexion. A representative MRI is shown in Figure A. What is the next best step in management of this patient?
Observation alone
Continued splinting in flexion
Continued splinting in extension
Open repair of the disrupted junctura tendinae
Open repair of the disrupted sagittal band
Based on the history and physical exam findings this patient has sustained a traumatic rupture of the sagittal band. In this professional athlete, the next best step would be to perform an open repair of the sagittal band. This will allow for earlier aggressive rehabilitation and a quicker return to sport.
Sagittal band ruptures may be traumatic (as in this case) or attritional in nature (as in rheumatoid arthritis). A direct blow to the MCP leads to forced flexion of the digit and subsequent stretching/rupture of the affected structure. On physical exam the tendons are most unstable with the wrist flexed; MCP flexion will lead to dislocation of the tendon into the intermetacarpal gutter.
Acute injuries may be treated with extension bracing for 4-6 weeks, but in professional athletes, direct open repair of the sagittal band is indicated.
Catalano et al. review sagittal band injuries treated with a thermally molded
plastic splint that held the MCP in ~25-35 degrees of hyperextension. Patients were evaluated over 14 months; out of 11 sagittal band injuries, splinting was successful in eight of them. They recommend initial nonsurgical management with custom splinting.
Hame et al. review the results of the management of sagittal band injuries in the professional athlete. The lesion commonly found was the disruption of the extensor mechanism with predictable sagittal band tears. In their series, all patients regained full range of motion and returned to their respective sports. They recommend surgical intervention in elite athletes in the form of extensor tendon centralization and sagittal band repair.
Figure A shows a T1 weighted axial cut of the affected hand; subluxation of the tendon (arrow) can be identified with disruption of the sagittal band (arrowhead).
The video provided briefly reviews injury to the sagittal band. Incorrect Answers
Compressive injury to the posterior interosseous nerve will lead to EMG fibrillations in which of the following muscles?
Extensor Carpi Radialis Longus/Extensor Carpi Radialis Brevis/Brachoradialis
Extensor Carpi Radialis Longus/Supinator/Abductor Pollicis Longus
Extensor Pollicis Longus/Supinator/Abductor Pollicis Longus
Brachoradialis/Supinator/Extensor Pollicis Longus
Extensor Pollicis Longus/Supinator/Abductor Pollicis Brevis
Based on the choices above, fibrillations will be seen in the extensor pollicis longus, supinator and abductor pollicis longus muscles.
The radial nerve splits into the superficial radial branch and the posterior interosseous nerve (PIN) at the anterior aspect of the radiocapitellar joint, just proximal to the supinator muscle. The PIN innervates the EDC, EDM, ECU,
EPB, EPL, EIP, APL and sometimes the ECRB. Compressive neuropathy of the PIN leads to motor dysfunction, namely weakness with wrist and finger extension.
Lubhan et al. review uncommon compression neuropathies affecting the upper extremity. They indicate that PIN syndrome may be caused by rheumatoid arthritis and compressive ganglion cysts. Depending on which nerve branch is affected, partial lesions may develop. They recommend use of conservative measures (rest, activity modification and splinting) first. Decompressive procedures may be indicated in symptoms lasting greater than 3 months.
Illustration A shows the course of posterior interosseous nerve from proximal to distal along the course of the supinator. This proximal edge of the supinator (Arcade of Froshe), the fibrous edge of the ECRB and the leash of Henry are three main points of compression of the PIN.
Incorrect Answers

Figure A shows a traumatic laceration of the distal forearm with a 5cm segmental median nerve defect. Which of the following repair or reconstruction techniques would allow for the best recovery of motor function?

Autogenous venous nerve conduit
Collegen synthetic nerve conduit
Biodegradable polyglycolic acid
Processed nerve allograft
Nerve autograft CORRECT ANSWER: 5
Figure A shows a traumatic laceration with 5cm of median nerve defect. The use of nerve autograft for this size defect has been shown to have the best recovery of motor function.
The optimal surgical treatment of nerve laceration is direct tension-free repair. In segmental nerve defects this approach cannot be achieved. The use of interposed autologous nerve grafting remains the gold standard of repair in this setting. The use of alternative techniques, such as processed allografts and synthetic conduits, have not shown to have equivalent recovery of motor function as compared to nerve autograft.
Giusti et al. used a rat model to examine techniques of peripheral nerve repair. They showed that nerve autograft resulted in better motor recovery than did the use of processed allograft or a collagen conduit.
Deal et al. discussed tubular interposition substitutes, or nerve conduits, as an alternative to nerve autograft in segmental nerve defect. Nerve conduits can include autogenous nerve conduits (venous or arterial) and synthetic nerve conduits (collagen, PGA, or caprolactone). In general, there is an upper limit of 3-cm when using nerve conduit.
Figure A is an image of the volar forearm. There is a traumatic laceration to
the anterior compartment tendons as well as the median nerve.
Incorrect Answers:
A 45-year-old man presents with a three-month history of unilateral symptoms in his right wrist and hand. He first noticed a palpable nodule over the volar aspect of his wrist about three months ago. The nodule would become painful after weekends of heavy drinking at which time he noticed tingling sensation in his index and middle fingers. He notes that ibuprofen has helped improve the pain in the past. On clinical examination, he has a palpable, nontender, solid nodule over the volar aspect of his wrist. He has no motor or sensory deficits and negative carpal tunnel provocative tests. An axial CT and MRI image are provided in figures A and B. What would be the most appropriate next step in the management of his symptoms?
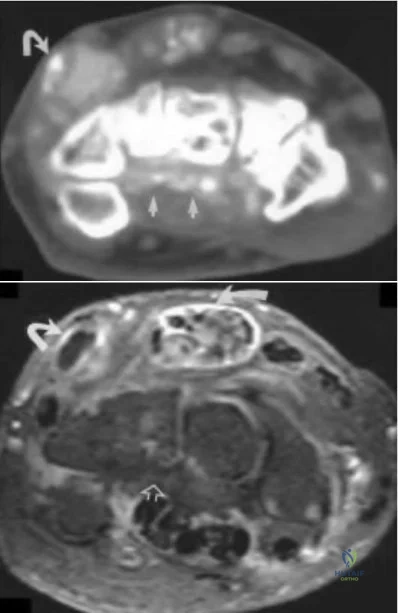
Fine needle aspiration
Chemotherapy
Night splints
Establish a tissue diagnosis and referral to a rheumatologist
Surgical excision CORRECT ANSWER: 4
The clinical presentation is consistent with carpal tunnel syndrome caused by an atypical space occupying lesion - in his case, gout. The most appropriate next step in the management of his symptoms would be establishing a tissue diagnosis and referral to a rheumatologist where medical therapy, such as prophylaxis with colchicine, could be initiated.
Carpal tunnel syndrome is the most common compressive neuropathy, affecting up to 10% of the general population. Risk factors include female sex,
advanced age, obesity, and repetitive motion activities. Typically, patients will develop symptoms of median nerve compression including thenar muscle atrophy, numbness in the radial 3.5 digits, night pain, and positive Tinel's and Phalen tests. First line management is non-operative, including NSAIDs, night splints, and activitiy modification. Carpal tunnel release surgery is indicated for those who have failed conservative management.
Chen et al. described 23 unusual cases of CTS in which space-occupying lesions were responsible for the symptoms and signs of median nerve compression. In patients with an atypical presentation, such as male gender, non-middle-aged, or unilateral involvement, space-occupying lesions such as gout, synovial sarcoma, lipoma, and ganglions should be investigated as a cause.
Fitzgerald et al. discussed gout affecting the hand and wrist. The medical treatment of gout includes NSAIDs such as indomethacin or ibuprofen for acute flares, and colchicine and allopurinol for chronic prophylaxis.
Figures A and B represent axial CT and MRI images showing calcification and gouty tophi deposition in the carpal tunnel floor.
Incorrect Answers:
Which statement most accurately describes the physiology of peripheral nerve regeneration following an axonotmesic lesion?
The proximal nerve segment undergoes Wallerian degeneration
Axon growth occurs from the distal segment to proximal segment
Neurotrophic factors direct phagocytic activity
Proximal axon budding allows for antegrade (or distal) axon migration
Axoplasm and myelin are degraded distally predominantly by Schwann cells for the first 12 months following injury
Axonomesis is a disruption of the nerve axon following injury. Repair/regeneration of the nerve occurs via proximal budding, followed by antegrade (or distal) axon migration.
The peripheral nerve regeneration process begins with the distal segment undergoing Wallerian degeneration (axoplasm and myelin are degraded distally by phagocytes). Existing Schwann cells proliferate and line-up along the basement membrane. Proximal budding occurs after a one-month delay. This is followed by sprouting axons that migrate in an antegrade fashion to connect to the distal tube. Repair of the nerve can take months, and often have poor outcomes.
Lee et al. reviewed peripheral never injury and repair. They commented that Wallerian degeneration (i.e., breakdown of the axon distal to the site of injury) is initiated 48 to 96 hours after transection. The Schwann cells then align themselves longitudinally, creating columns of cells called Büngner bands. At the tip of the regenerating axon is the growth cone.
Illustration A shows a chart of peripheral nerve injury. The two main classification systems are Seddon and Sunderland. Video V is a lecture discussing peripheral nerve injury and management.
Incorrect Answers:
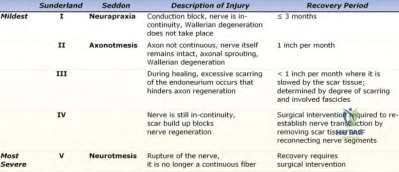
A 28-year-old male injures his hand while playing basketball and presents to the emergency room. Closed reduction is performed and is stable. Post-reduction rehabilitation is discussed with the patient.
Which of the following radiographs demonstrates an injury that would be treated best by dorsal extension block splinting?

Figure E CORRECT ANSWER: 2
Dorsal extension-block splinting is the treatment of choice for dorsal proximal interphalangeal joint (PIPJ) fracture dislocations that are stable following reduction and have less than 40% articular surface fracture involvement.
Dorsal PIPJ dislocations are a common injury, often resulting from jamming or hyperextending the finger. In the absence of an associated fracture or presence of a small volar plate avulsion, dorsal PIPJ dislocations are often
treated with closed reduction and buddy-taping to the adjacent digit. Injuries that are unstable following reduction or those associated with an intra-articular fracture of the middle phalanx are stabilized with a dorsal extension-block splint to maintain reduction. It is important to initiate early range of motion exercises within the constraints of the splint to minimize scar formation and subsequent PIPJ contracture.
Elfar et al. reviewed fracture-dislocations of the PIPJ. Dorsal PIPJ fracture-dislocations can be categorized as avulsion or impaction shear injuries.
Avulsion fractures result from hyperextension of the PIPJ, tensioning the volar plate (VP) with eventual VP rupture or avulsion of the volar lip of the middle phalanx. Axial load applied to the digit in PIPJ flexion drives the head of the proximal phalanx across the middle phalangeal base, resulting in a shear fracture or comminuted impaction fracture of the middle phalanx, depending on the amount of energy imparted and the bone quality.
Morgan et al. reviewed hand injuries in athletes. Dorsal PIPJ dislocations without associated fracture that are stable following successful reduction are treated by buddy taping the injured digit to the non-injured digit adjacent to the compromised collateral ligament. Buddy taping with active motion should be continued for 6 weeks. Unstable injuries and those with an intra-articular fracture of the middle phalanx should be treated with dorsal extension-block splinting with incremental extension of the splint on a weekly basis for 4 weeks, followed by buddy-taping for 3 months during sports activities.
Figure A shows a simple dorsal PIPJ dislocation. Figure B shows a dorsal PIPJ fracture dislocation. Figure C shows a simple volar PIPJ dislocation. Figure D shows a volar PIPJ fracture dislocation. Figure E shows a dorsal avulsion fracture at the base of the distal phalanx (bony mallet injury). Illustration A depicts an dorsal extension-block splint that blocks extension of the digit past a set point while allowing full active flexion of the digit. Illustration B is a lateral radiograph of a digit showing a small minimally displaced volar plate avulsion fracture at the PIPJ with minimal intra-articular involvement (as compared to Figure B). This injury may be managed with buddy taping and active range of motion as tolerated.
Incorrect Responses:
extension for 6-8 weeks to limit flexion of the digit and therefore fracture displacement.
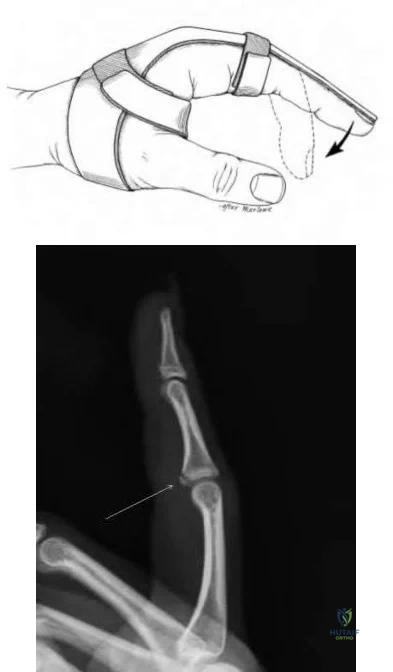
A 35-year-old mixed martial arts fighter and recreational cocaine user presents with symptoms concerning for hypothenar hammer syndrome (HHS). Significant ischemia is found on physical exam. Arteriography is shown in Figure A. What is the most appropriate next step in treatment?

Conservative treatment with cocaine abstinence
Conservative treatment with activity modifications and medical management with calcium channel blockers
Therapeutic endovascular fibrinolysis
Excision of involved segment and reconstruction with or without a vein graft
Medical management with coumadin for 6 months
Figure A shows a bilobed aneurysm overlying the ulnar artery with normal appearing distal vasculature. Hypothenar hammer syndrome (HHS) can be associated with an aneurysm and is most appropriately treated with resection of the involved segment and either reconstruction with a primary anastomosis or vein graft.
HHS syndrome consists of two separate entities, thrombosis and aneurysm. In the setting of thrombosis without aneurysm, conservative management is preferred. If the thrombosis is acute (<2 weeks), endovascular fibrinolysis has shown good results. In patients with an HHS and an aneurysm, surgery is required for resection to prevent distal embolization and remove the often painful aneurysmal mass.
Yuen et al. review HHS. In patients with HHS and aneurysms, resection of the involved segment of the ulnar artery prevents distal embolic events, eliminates the painful mass, relieves ulnar nerve compression, and removes the thrombus which initiated the reflex vasospasm and closed off the collateral
vessels in the region.
Lifchez et al. review the long-term outcomes of 11 patients with HHS treated with ulnar artery reconstruction. 2 of the patients underwent excision and direct ulnar artery repair, and the rest underwent reconstruction with a vein graft. All patients had a mean improvement in digital brachial index, decrease in pain and dysesthesia symptoms, and decrease in cold intolerance compared with preoperatively.
Nitecki et al. review a case series of 6 patients with HHS. They state that the treatment of thrombosis should be largely conservative, but thrombolytic treatment could be considered if the event happened <2 weeks prior to presentation.
Illustration A shows an excised ulnar artery aneurysm in a patient with HHS. Note the typical "corkscrew" appearance of the distal segment.
Incorrect Answers:
A 36-year-male was using a high-pressure paint gun when he suffered the injury shown in Figure A. Which of the following variables would have the worst impact on his prognosis?

Delay in surgical treatment
Injected solvent was grease
Injected solvent was water-based paint
An entry wound of greater than 3 cm
Injected solvent was at room temperature
The clinical presentation is consistent for a high-pressure injection injury. Delays in surgical treatment are associated with serious sequelae.
High-pressure injection injuries are characterized by extensive soft tissue damage associated with a benign high-pressure entry wound. They should be treated with irrigation & debridement, foreign body removal and broad-spectrum antibiotics. There is a higher rates of amputation when surgery is delayed.
Bekler et al. looked at the results of 14 surgically treated high-pressure injection injuries of the hand with a minimum of two years follow-up. Ten of the injuries required formal operative debridement and foreign body removal. Six required reconstructive microsurgical procedures and one underwent digital tip amputation. They concluded that high-pressure injection injury to the hand is a significant problem, which can easily lead to serious sequelae and, even, amputation.
Rosenwaser et al. report wide débridement of all involved tissues, decompression of tissue compartments, exploration and incision of tendon sheaths, removal of injected material, and saline irrigation are critical in the management of high-pressure injection injuries to the hand. They emphasize
delayed surgery has been associated with increased incidence of morbidity and amputation.
Figure A shows a typical high-pressure injection injury. Notice the benign looking entry wound.
Incorrect Answers:
A healthy 50-year-old secretary is about to undergo an open carpal tunnel release. Which of the following peri-operative steps will have the greatest influence on minimizing the risk of a surgical site infection in this patient?
Administration of cefazolin within 1 hour before incision
Administration of cefazolin within 1 hour before incision followed by 5 days of cephalexin post-op
Cleanse with bacitracin solution immediately before skin incision
Standard sterilization and prepping
Administration of one dose of cephalexin within 1 hour before incision
The patient is undergoing a clean, elective hand surgery. Prophylactic antibiotics, systemic or local, are not indicated for these procedures.
Carpal tunnel syndrome is the most common compressive neuropathy. Individuals who fail medical management (night splints, NSAIDs, activity modification) are candidates for carpal tunnel release surgery (CTS). The surgery may be performed open or endoscopically. The reported incidence of post-operative infections following CTS varies between studies from 0% to 8%.
Whittaker et al. performed a prospective, randomized, double-blinded, placebo
controlled trial investigating the use of antibiotic prophylaxis in clean, incised hand injuries. They found no significant difference in infection rates between patients who received IV flucloxacillin, IV followed by oral flucloxacillin, and an oral placebo (13% vs. 4% vs. 15%, p=0.19). They did not support the use of routine antibiotic prophylaxis prior to clean hand surgery.
Bykowski et al. retrospectively reviewed 8,850 outpatient elective hand surgeries and found no significant difference in the rate of surgical site infection, including patients with diabetes or history of smoking. They concluded that antibiotics should not be routinely administered prior to clean, elective hand surgeries.
Harness et al. found no statistical difference in the incidence of surgical site infection following CTS without prophylactic antibiotic compared with patients who received prophylactic antibiotics (0.7% vs. 0.4%, p=0.354). They did not recommend routine antibiotic prophylaxis.
Illustration A reviews the anatomic components of the carpal tunnel. Incorrect Answers:
infection in clean, elective hand surgery. Surgeons should consider the potential risks of antibiotics prior to administration, including Clostridium difficile colitis, antibiotic allergies, bacterial resistance, and so on.
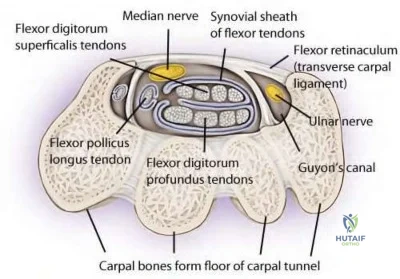
A 30-year-old male laborer sustained a right wrist injury 9 months ago. He continues to have symptoms of recurrent ulnar-sided wrist pain that impairs his ability to work. An MRI is performed and
shows a triangular fibrocartilage complex (TFCC) injury. Which of the following is an indication to combine a Wafer procedure with arthroscopic TFCC debridement?
Ulnar styloid fracture
Radial styloid fracture
2 mm of positive ulnar variance and ulnocarpal impingment
2 mm of negative ulnar variance and radiocarpal joint arthritis
Scapholunate ligament injury
A Wafer procedure is indicated for positive ulnar variance and symptomatic ulnocarpal impingement associated with degenerative TFCC tears.
Ulnar impaction syndrome and triangular fibrocartilage complex (TFCC) injuries are relatively common causes of ulnar-sided wrist pain. Positive ulnar variance causes increased contact pressures between the lunate and the ulnar head. The Wafer procedure removes 2-4 mm of distal ulnar head to reduce ulnar variance to neutral or negative. This is thought to reduce ulnar impaction and decrease pain.
Faber et al. examined the role of MRI in wrist injuries. They showed that the sensitivity and specificity to detect TFCC tears using MRI is approximately 80%. They conclude that there is no supporting evidence for routine MRI's for patients with non-specific ulnar-sided wrist pain.
Illustration A is a coronal view MRI (without arthrogram) of the right wrist that shows a TFCC tear (blue arrow) with positive ulnar variance. Illustration B shows a series of images showing a TFCC tear on MRI and intra-operatively.
Incorrect Answers:

A 27-year-old male sustains the injury shown in Figure A. He is taken to the operating room and the lesion is repaired primarily. Two months later, he feels a "pop" while using his hand and is no longer able to flex the distal phalanx of the involved digit. He is taken to the operating room for surgical exploration where 1.8 cm of scar tissue between the tendon ends is identified. The tendon sheath is found to be intact and allows smooth passage of a pediatric urethral catheter. What is the next step in management?

Resection of scar and primary repair of tendon ends.
Resection of scar and adjacent 1cm of tendon, placement of Hunter rod for staged reconstruction.
Debulking of scar, partial excision of 25% of the A2 and A4 pulleys.
Resection of scar, harvest of ipsilateral palmaris longus tendon for tendon reconstruction.
Resection of scar and proximal tendon, tendon transfer from adjacent digit.
This patient sustained an FDP laceration that was treated initially with primary repair. He subsequently re-ruptured the tendon 2 months later. With scar >1 cm, tendon grafting is indicated and primary tendon grafting with palmaris longus is commonly performed as it is the most accessible tendon in the operative field.
Flexor tendon lacerations commonly result from volar lacerations. Concomitant neurovascular injury is common. Partial lacerations <60% of tendon width are treated with debridement and early range of motion. With partial lacerations, the least amount of gliding resistance can be obtained with debridement alone. Lacerations >60% of tendon width are treated with flexor tendon repair and controlled mobilization. Failed primary repair and chronic untreated injuries are indications for flexor tendon reconstruction and intensive postoperative rehabilitation.
Lilly et al. reviewed complications after flexor tendon injuries. Common complications include adhesions, joint contracture, tendon rupture, triggering, pulley failure and bowstringing, quadrigia, swan-neck deformity and lumbrical plus deformity.
Figure A shows a zone II laceration of the left index finger FDP.
Incorrect Answers:
A 55-year-old female patient presents with pain along the thumb ray and increasing deformity of her right hand. Key pinch causes her pain. The appearance of her hand is seen in Figure A. Range of motion of her thumb is seen in Figure B. What is the most likely cause of her deformity?
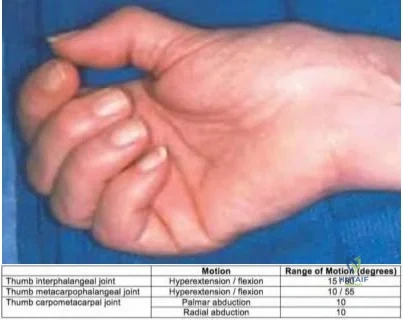
Type II hypoplastic thumb
Median nerve neuropathy
Lupus thumb deformity
Extensor tendon rupture
Osteoarthritis of the trapeziometacarpal joint
The patient has 1st carpometacarpal (CMC) arthritis.
With 1st CMC arthritis, the patient avoids painful thumb abduction and an adduction deformity gradually develops, with 1st webspace contracture. With progressive 1st CMC stiffness, the thumb metacarpophalangeal joint (MCP) develops hyperextension deformity to compensate for the loss of motion, leading to a secondary "Z" deformity.
Rozental et al. reviewed hand and wrist reconstruction. They believe that arthrosis arises from loss of the anterior oblique ("beak") ligament.
Compensatory MCP hyperextension should be treated with MCP capsulodesis or arthrodesis.
Van Heest et al. reviewed thumb CMC arthritis. Treatment for Eaton stage I/II arthritis is open/arthroscopic debridement, volar ligament reconstruction (with APL or FCR tendons), or metacarpal extension osteotomy. For stage III/IV arthritis, treatment options include implant arthroplasty or resection arthroplasty +/- LRTI (with APL, FCR or palmaris longus), and fusion (young patients).
Figure A shows adduction contracture of the 1st webspace, with hyperextension deformity of the 1st MCP joint. Figure B illustrates decreased thumb abduction because of adduction contracture with decreased palmar abduction (normal, 45deg) and decreased radial abduction (normal, 60deg). Illustration A is a radiograph showing thumb CMC arthritis with Z deformity. Illustration B shows lupus thumb deformity ("hitchhiker thumb"). Illustration C shows hand changes in inflammatory arthritis.
Incorrect Answers:
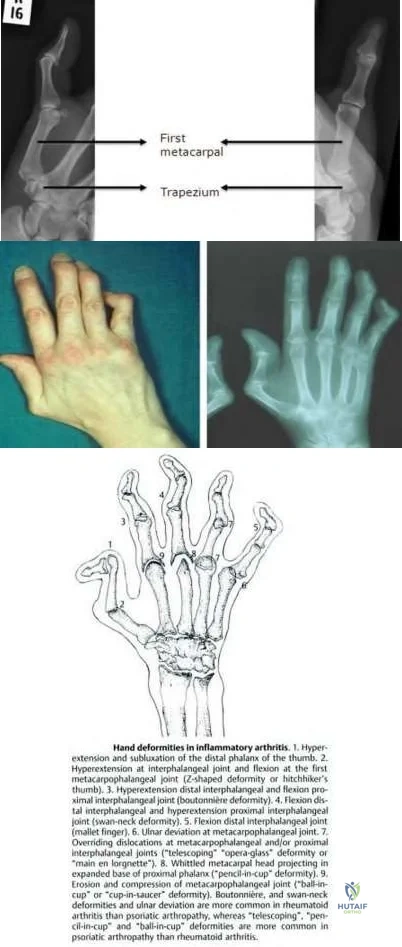
A 26-year-old man presents with chronic hand weakness. The clinical appearance of his hand, and radiographs are shown in Figures A through C. Surgical exploration and decompression is performed. Besides addressing thumb interphalangeal and index distal interphalangeal joint flexion, which is the most appropriate treatment to restore thumb opposition?

Ring flexor digitorum superficialis transfer to the abductor pollicis brevis
Extensor indicis proprius transfer to the abductor pollicis brevis
Neurotization of thenar muscles
Camitz palmaris longus transfer to the abductor pollicis brevis
Thumb carpometacarpal joint arthrodesis
This patient has a high median nerve neuropathy because of a supracondylar spur and ligament of Struthers. Reconstruction is best performed with extensor indicis proprius (EIP) transfer to the abductor pollicis brevis (APB).
In low median nerve palsy, the primary concern is restoration of thumb opposition. In high median nerve palsy, thumb opposition and IP flexion, and index and middle finger flexion have to be addressed. The four common opposition transfers include (1) ring or long FDS, (2) EIP, (3) Camitz palmaris longus (PL), or the Huber abductor digiti minimi (ADM).
Anderson et al. reviewed EIP transfer vs FDS transfer. They found a higher percentage of excellent results in the EIP group. In their series, complications included index finger extensor lag (EIP transfer if the extensor expansion was not repaired) and limited donor finger extension because of lateral band damage or adhesions between the remaining FDS tendon and flexor sheath (FDS transfer).
Cawrse et al. modified the Huber ADM opponens transfer by releasing the proximal end to prevent compression of the ulnar nerve in Guyon's canal by the rotated ADM belly. They found that this technique successfully restored
opposition and thenar bulk.
Figure A shows thenar wasting. Figures B and C show a supracondylar spur. The ligament of Struthers attaches from this spur to the medial epicondyle, under which median nerve and brachial artery pass. Illustration A shows EIP transfer. Illustration B shows FDS transfer. Illustration C shows Camitz PL transfer. Illustration D shows Huber ADM transfer.
Incorrect Answers:
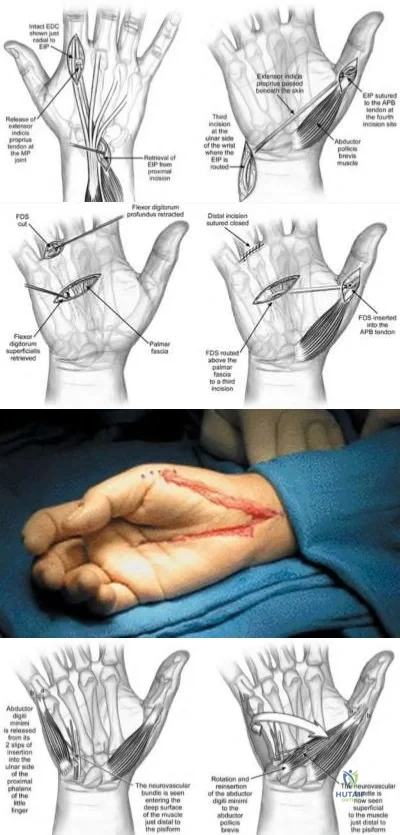
A 2-year-old child is referred by her pediatrician for fixed flexion deformity of the left thumb. She has been wearing a splint for the last 6 months. She has ventricular septal defect and left renal agenesis. The interphalangeal joint does not extend past 40 degrees of flexion as seen in Figures A and B. There is no triggering. There is a firm, nontender nodule overlying the metacarpophalangeal joint as outlined in blue in Figure C. What is the diagnosis and most appropriate treatment?

Thumb camptodactyly. Therapy including passive stretching exercises.
Congenital clapsed thumb. Percutaneous release of the A1 pulley.
Pediatric trigger thumb. Open release of the A1 pulley.
Pediatric trigger thumb. Open release of the A1 pulley and resection of the tendon nodule.
Blauth Type I hypoplastic thumb. Open release of the A1 pulley and volar plate, and resection of the tendon nodule.
This child has pediatric trigger thumb (PTT). The potential for spontaneous resolution beyond the age of 2 years is limited. Surgical release of the A1
pulley is indicated.
Pediatric trigger thumb presents as fixed flexion at the interphalangeal joint (IPJ) rather than triggering. It is likely to be acquired (rather than congenital). It is associated with the presence of Notta's nodule, a thickening of the FPL tendon and overlying tendon sheath. Treatment involves A1 pulley release.
The role of non-surgical management (splinting/stretching) remains unclear. The duration of non-surgical treatment is long (up to 30 months) and compliance can be difficult.
Shah et al. reviewed pediatric trigger thumb. The condition is associated with MCP hyperextension. The authors note no advantage to percutaneous release as general anesthetic is required anyway.
Marek et al. performed a retrospective review and survey response review of surgery for pediatric trigger thumb. They found that age at the time of surgery influences residual flexion contracture and rate of recovery. They found surgery to be safe and effective, and recommend: (1) surgery for a 2-year-old child with a locked thumb for 6 months, (2) observation for a child <1 year if the thumb is triggering (not locked), and (3) a 6-month observation period if observation is advocated.
Figures A and B show a fixed flexion deformity of the thumb and an attempt at thumb extension. Figure C shows the outlined Notta nodule.
Incorrect Answers:
A 48-year-old hairdresser presents with pain and swelling of his ring finger for 4 days. On examination, there is generalized tenderness along the entire digit. Passive extension of the digit triggers
excruciating pain. The clinical appearance of the digit is shown in Figure A. What is the most appropriate next step in management?

Acyclovir
Intravenous antibiotics, splinting and elevation
Closed tendon sheath irrigation from the level of the A1 pulley (proximal) to the distal interphalangeal joint (distal)
Continuous closed tendon sheath irrigation from the wrist (proximal) to the distal interphalangeal joint (distal)
Open irrigation and debridement
This patient has advanced pyogenic flexor tenosynovitis (PFT) with visible ischemia/necrosis. Open irrigation and debridement is necessary.
Pyogenic flexor tenosynovitis is usually caused by a puncture wound (although it may infrequently arise from hematogenous spread). The most common organism is Staphylococcus aureus. Kanavel signs help differentiate this disease from herpetic whitlow, septic arthritis, gout/pseudogout, and other hand infections such as paronychia, felons, cellulitis, and deep space infections.
Draeger et al. reviewed the treatment of pyogenic flexor tenosynovitis (PFT). They recommend open irrigation and debridement for advanced PFT and atypical or chronic tenosynovial infections where tenosynovectomy may be
indicated. Both midaxial and volar zigzag incisions can be used.
Pang et al. reviewed factors affecting the prognosis of PFT. Of the 4 Kanavel signs, they found that fusiform swelling was most often present (97% of patients), followed by pain on passive extension (72%), semiflexed digit posture (69%), and tenderness along the flexor tendon sheath (64%).
Figure A shows advanced PFT demonstrating subcutaneous purulence and local ischemia in addition to fusiform digital swelling. Illustration A shows the Nevasier technique of closed tendon sheath irrigation. Illustration B shows the setup for continuous tendon sheath irrigation using nested catheters.
Illustration C shows the incision for open irrigation and debridement.
Incorrect Answers:

Madelung's deformity of the distal radius is caused by which of the following?
Premature fusion of the distal radial ulnar joint
Physeal growth mismatch between the distal radius and ulna
Nutritional deficiency affecting the physeal zone of provisional calcification
Impaired growth of the volar and ulnar aspect of the distal radial physis
Unrecognized trauma CORRECT ANSWER: 4
Madelung's deformity is that of excessive ulnar/palmar angulation of the distal radius caused by impaired growth of the volar and ulnar aspect of the distal radial physis. It may be caused by either a bony lesion in the palmar/ulnar corner of the distal radial physis or an abnormal radial-carpal ligament (Vicker's ligament). The other answers do not cause Madelung's deformity.
Leri-Weill dyschondrosteosis is a rare genetic disorder caused by mutation in the SHOX gene that causes mesomelic dwarfism with associated Madelung's defomity of the forearm.
Illustration A is a radiographic example of Madelung's deformity.

A 17-year-old boy presents with pain in his right elbow for 2 years and limitation in elbow motion bilaterally. He denies any pain or discomfort in his left elbow. He reports no history of trauma to either elbow. He has had two courses of physical therapy, but has noted no noticeable improvement in pain or motion. Examination demonstrates no elbow tenderness on palpation, and there are no neurological deficits. Manual reduction is unsuccessful. The range of motion of both elbows is shown in Figure A. Radiographs of left and right elbow are shown in Figure B and C respectively. What is the most appropriate treatment plan for the right and left elbow?

Bilateral open reduction and application of a hinged external fixator to both elbows
Radial head resection of the right elbow and non-operative management of the left elbow.
Bilateral radial head arthroplasty
Physical therapy and splinting to both elbows
Radial head resection and interposition arthroplasty for the right elbow and radial head resection alone for the left elbow
This patient has bilateral congenital radial head dislocation (CRHD). The right side is symptomatic with significant loss of motion. The left is asymptomatic with minimal loss of active motion. Therefore the most appropriate treatment is radial head resection of the right elbow and non-operative management of the left elbow.
It is important to differentiate CRHD from traumatic dislocation. Clinical features of CRHD include bilateral involvement, presence at birth, other congenital anomalies, familial occurrence, irreducible by closed methods, and
lack of a history of trauma. Radiological features include dome-shaped radial head and hypoplastic capitellum, relatively short ulna or long radius, deficient trochlea, prominent medial epicondyle, grooving of the distal radius, and anterior curvature of the posterior outline of the ulna.
Bengard et al. reviewed 10 surgically treated and 6 nonsurgically treated CRHD patients. They found no change in flexion-extension and carrying angle postoperatively, but forearm rotation was improved. Surgically treated patients had significant improvement in elbow pain. Ultimately, >25% of patients had wrist pain postop and this must be weighed in the decision process of treatment. They recommend radial head excision as an effective intervention in selected patients with significant elbow pain.
Figure A is a table showing moderately diminished ROM of the right elbow, and minimally reduced ROM of the left elbow. Figures B and C both show posterior dislocation of the radial head (a line along the long axis of the radius should intersect the capitellum in all views).
Incorrect Answers:
Which of the following muscles provide the primary deforming forces to Bennett and Rolando fractures (base of the 1st metacarpal fractures)?
Pronator quadratus
Flexor pollicis longus
Extensor pollicis longus
Adductor pollicis longus and abductor pollicis
Abductor pollicis longus and adductor pollicis
The primary deforming forces in Bennett and Rolando fractures are the Abductor pollicis longus and adductor pollicis.
In a Bennet's or Rolando fracture-dislocation the volar-ulnar fracture fragment is held reduced by the anterior oblique ligament while strong deforming forces pull the remaining metacarpal shaft proximally and dorsally, angulate the shaft ulnarly and supinate the shaft. Most important in these deforming forces are the abductor pollicis longus (APL) inserting on the base of the metacarpal which pulls the metacarpal shaft proximally and dorsally and the adductor pollicis (AP) which inserts on the ulnar base of the proximal phalanx and angulates the metacarpal shaft ulnarly and supinates the shaft. Less important is the extensor pollicis longus (EPL) which inserts on the base of the distal phalanx and also adds to the ulnar angulation of the distal fragment.
Soyer reviews the diagnosis, pathoanatomy, and treatment for fractures at the base of the 1st metacarpal. Understanding the biomechanics, anatomical deforming forces, and the exact fracture pattern aids the treating surgeon in determining the most appropriate method of fixation. The most essential factor for obtaining a good functional result is anatomic restoration of the articular surface.
Elgafy et al. examined the terminal anatomy of the posterior interosseous nerve in their cadaver study - identifing six terminal branches and describing methods to avoid injury. They describe how treating surgeons can maximize function and recovery after base of the 1st metacarpal fractures by understanding these nervous branches and specific fracture pattern treatment to avoid iatrogenic injury to the PIN.
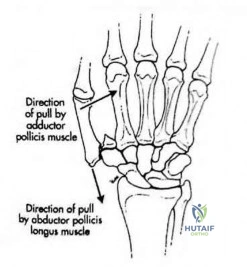
A 28-year-old man sustained a complete laceration of the flexor digitorum profundus of his index finger while cutting a watermelon 3 days ago. A clinical photograph is shown in Figure A. The surgeon plans to repair the tendon using a 4-strand core suture technique. Which method of tendon repair will give him the best results in terms of load to failure and gliding resistance?

Repair with core suture purchase 5mm from the cut edge only. No epitendinous suture
Repair with core suture purchase 10mm from the cut edge only. No epitendinous suture
Repair with core suture purchase 5mm from the cut edge. Circumferential
simple running epitendinous suture.
Repair with core suture purchase 10mm from the cut edge. Circumferential Silfverskiold epitendinous suture.
Repair with core suture purchase 10mm from the cut edge. Circumferential simple running epitendinous suture.
Repair with core suture purchase 10mm from the cut edge, coupled with circumferential simple running epitendinous suture will give him the best load to failure and gliding resistance.
The strength of tendon repairs depend on the number of strands crossing the repair site. Ideally, repairs should have 4-6 strands to allow for early active motion. A running epitendinous suture is recommended to improve tendon gliding and repair strength.
Gulihar et al. compared 3 different epitendinous suture techniques. They found that compared with an intact tendon, gliding resistance increased 100% with the Halsted repair, 80% with the Silfverskiold repair and 60% with a running suture. They thus recommend a simple running suture when an epitendinous suture is needed.
Lee et al. compared core suture purchase at 3, 5, 7 and 10mm from the cut edge. The 10mm-repair group had the highest 2-mm gap force and ultimate failure load. They recommend 10-mm suture purchase for optimal performance and to allow early active motion.
Figure A shows a laceration to the volar aspect of the index finger in flexor zone II. Illustration A shows a core suture purchase distance from the cut edge (represented by "X", where 10mm is the ideal distance). Illustration B shows 3 different epitendinous suture techniques (A, simple running; B, Silfverskiold; C, Halsted).
Incorrect Answers:

A 28-year-old professional baseball player injures his middle finger sliding into the catchers shin guard at home plate. He complains of pain and deformity of the middle finger. A radiograph is provided in figure A. All of the following are true EXCEPT:
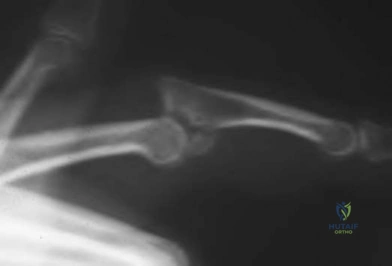
Anatomic reconstruction of the articular surface is prognostic of clinical function
Proximal interphalangeal joint subluxation precludes a normal gliding flexion arc
Hinging at the fracture site must be avoided
Early motion should be initiated in postoperative therapy
Early degenerative arthritis can be expected if the joint is not adequately reduced.
The radiograph demonstrates a dorsal fracture dislocation of the proximal interphalangeal joint of the middle finger. Kiefhaber and Stern review the presentation, evaluation, and treatment of PIP fractures. Congruent reduction of the joint to allow the middle phalanx to glide around the proximal phalangeal head is paramount to prevent joint subluxation and instability.
Anatomic reconstruction of the articular surface is desirable but not necessary for successful clinical outcome.
A 30-year-old male sustains a 3.5 cm long thumb pulp injury seen in Figure A. He undergoes a procedure to restore the soft tissue envelope. Which treatment option is contraindicated because of increased risk of interphalangeal joint stiffness?

Moberg volar advancement flap
Foucher first dorsal metacarpal artery flap
Littler neurovascular island flap
Free great toe pulp transfer
Holevich first dorsal metacarpal artery flap
This patient has a large thumb pulp defect measuring 3.5 cm in length, extending proximal to the interphalangeal joint (IPJ) crease. Inset of a Moberg flap large enough to cover the defect would necessitate IPJ flexion >45 degrees, increasing the risk of IPJ stiffness.
Thumb pulp defects may be resurfaced by different means, depending on size. The Moberg flap is suited for medium (1.8-3 cm) defects. For defects >1.5 cm, there is increased risk of wound dehiscence, parrot beak nail deformity, and decreased soft tissue padding. Modifications such as V-Y flaps, bilateral Z-plasties, Burrow triangles, 2 lateral triangular flaps at the proximal edge of the flap, or advancement of an island flap with skin grafting of the secondary defect (O’Brien modification), are recommended.
Baumeister et al. reviewed the functional outcome of Moberg flaps. These flaps do not cause marked impairment of active ROM and any reduction in the AROM of the IP joint is because of a loss of hyperextension.
Horta et al. reviewed the use of multiple flaps (Moberg, radial innervated cross-finger, Venkataswami-Subramanian, Foucher, Tezcan, and Littler). They recommended the Foucher flap because of good sensibility, single-stage surgery, and no need for cortical reintegration (unlike the Littler flap)
Figure A shows a large thumb pulp defect. Illustration A shows the options for resurfacing thumb pulp defects of different sizes. Illustration B is a diagram of these options. Illustrations C and D depict the Holevich dorsal metacarpal artery flap (with overlying skin strip). Illustrations E and F depict the Foucher dorsal metacarpal artery flap (islanded).
Incorrect Answers:
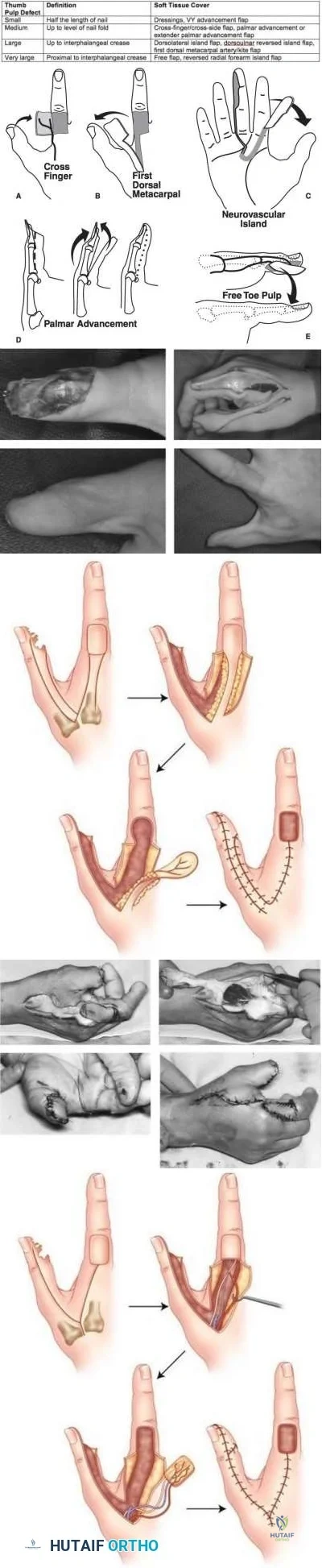
Percutaneous screw fixation for non-displaced scaphoid waist fractures has been shown to have which of the following differences compared to closed treatment?
Increased direct and indirect cost
Slower return to work
Higher union rates
Reduced time to fracture union
Improved motion and grip strength after 2 years
Fixation of non-displaced scaphoid fractures with a percutaneous screw has resulted in a shorter time to union (6-7 weeks versus 10-12 weeks) and faster return to work or sports.
Arora et al found the indirect cost reduction by a quicker return to work was shown to offset the direct costs of surgical intervention.The operatively treated group had a better mean DASH-score than the conservative group. Fracture
union was seen in the screw fixation group at a mean of 43 days and in the cast immobilization group at a mean of 74 days.
Bond et al found in active military personnel there was faster healing but no difference in ultimate union rates or final grip strength or range of motion between percutanous screw fixation and non-operative groups. The average time to fracture union in the screw fixation group was seven weeks compared with twelve weeks in the cast immobilization group. There was no significant difference in the range of motion of the wrist or in grip strength at the two-year follow-up evaluation.
Constriction ring syndrome, also known as amniotic band syndrome, is a congenital disorder associated with which paediatric foot condition?
Equinovalgus foot
Clubfoot (Congenital talipes equinovarus)
Tarsal coalition
Congenital vertical talus
Polydactyly CORRECT ANSWER: 2
Constriction ring syndrome is a congenital disorder that is most commonly associated with clubfeet (congenital talipes equinovarus). The reported incidence of clubfeet with concomitant constriction bands ranges from 12-56%.
Constriction ring syndrome is a collection of congenital malformations that occur as a result of intrauterine rings or bands that constrict fetal tissue. The etiology of constrictive ring syndrome remains elusive, though Streeter postulated in 1930 that a germline developmental abnormality is responsible for the development of amniotic constriction bands, hence one of the synomonous terms used to describe the disorder, Streeter’s dysplasia. Normal anatomy is found proximal to the band. Distally, a constrictive band can cause compression of lymphatic and neurovascular structures and result in lymphedema, altered circulation and neuropathy. In severe cases congenital amputation can occur. In terms of other orthopaedic conditions, constrictive ring syndrome is associated with clubfeet, acrosyndactyly and pseudoarthrosis. With respect to clubfeet, surgical treatment is commonly required, which consists of z-plasty releases of the constricted bands, in addition to surgical correction of the clubfoot deformity.
Gomez reviewed 35 children with clubfeet associated with constriction ring syndrome. In this cohort there was a poor response to casting, as 77% of the children required surgical corrections. Z-plasty releases of the deep bands were performed before the clubfoot correction.
Allington et al. examined the outcome of treatment of clubfeet distal to a lower extremity band in 18 patients (21 feet). Sixteen children (88.9%) underwent surgical treatment after manipulation and serial casting were unsuccessful.
Mild initial foot deformities and constriction bands located in the distal aspect of the lower leg were associated with the best outcomes.
Incorrect Answers:
You are consulted on a newborn male inpatient who presents with the clinical sign shown in Figure A. All of the following are commonly associated with this syndrome EXCEPT?

Bronchopulmonary dysplasia
Cardiac defects
Cleft palate
Encephalocele
Rigid talipes equinovarus
Question 67
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
Explanation
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Small SA, Perron AD, Brady WJ: Orthopedic pitfalls: Cauda equina syndrome. Am J Emerg Med 2005;23:159-163.
Question 68
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?
Explanation
and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular
angle. Correction of both of these abnormalities requires a proximal and distal first
metatarsal osteotomy.
REFERENCES: Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Peterson HA, Newman SR: Adolescent bunion treated with double osteotomy and longitudinal pin fixation of the first ray. J Pediatr Orthop 1993;13:80-84.
Question 69
What is the relative amount of type II collagen synthesis in disease-free adult articular cartilage compared to developing teenagers?
Explanation
the matrix.
REFERENCES: Lippiello L, Hall D, Mankin HJ: Collagen synthesis in normal and osteoarthritic human cartilage. J Clin Invest 1977;59:593-600.
Nelson F, Dahlberg L, Laverty S, et al: Evidence for altered synthesis of type II collagen in patients with osteoarthritis. J Clin Invest 1998;102:2115-2125.
Question 70
Physiologic bowing of the lower extremities should spontaneously correct by what age?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 7.
Salenius P, Vankka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am
J V :
Question 71
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 72
An acetabular fracture with all segments of the articular surface detached from the intact posterior ilium is defined as what fracture pattern?

Explanation
radiographic findings consistent with a both column acetabular fracture can be seen in Illustration A (AP), Illustration B (obturator oblique), and Illustration C (iliac oblique).
Question 73
Which of the following preoperative findings is a predictor of poor outcome following arthroscopic debridement for glenohumeral arthritis? Review Topic
Explanation
Question 74
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic

Explanation
Question 75
A 65-year-old man has had “catching” in front of his knee since he had a total knee arthroplasty 9 months ago. Examination reveals a palpable and audible snap in the anterior aspect of the knee at about 40 degrees of flexion as the knee is being actively extended. A radiograph of the prosthetic knee will most likely show
Explanation
Pathologically, the clunk is produced by a suprapatellar fibrous nodule seen superior to the patellar component at re-operation. This nodule has been seen to catch in the intercondylar notch in primarily first generation TKAs. Current component designs have decreased this phenomenon through better engineering of femoral components. Treatment is by arthroscopic debridement or open arthroplasty resection. The nodule may be recurrent.
Question 76
What is a known risk factor for wound infection after spinal fusion for neuromuscular scoliosis? Review Topic
Explanation
<1500 cells/µL (reference range, 1000-4800/µL) has been associated with increased postoperative wound infections.
Question 77
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 78
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Explanation
REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.
Question 79
Figures 115a and 115b are the radiograph and intraoperative view of the femoral taper junction of a 68-year-old man who has left groin pain 8 years after undergoing total hip arthroplasty (THA). He has a mild limp and mild pain with active and passive range of motion. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. His serum cobalt level is 5.3 ppb and serum chromium level is 3.4 ppb. In addition to exchanging the acetabular insert, what is the best surgical procedure for this patient?
Explanation
This patient has symptomatic severe pelvic and femoral osteolysis occurring after a metal-on-metal bearing THA. Bearing surface wear and taper wear (corrosion) are debris sources contributing to osteolysis, and both sources should be addressed at surgery. Current recommendations are to not remove a stable cementless femoral component unless the taper is damaged so badly that a new ball will not lock on the taper. There have been reports of repeat local tissue reactions when a new cobalt chromium ball is placed on a taper with corrosion damage. The current recommendation is to minimize the amount of cobalt at the taper junction, and this can be done by avoiding a cobalt chromium ball in favor of a titanium taper sleeve on the damaged taper with a ceramic ball on the new sleeve. Use of a ceramic head on a previously used trunnion poses risk for fracture of the ceramic head.
Question 80
Figures 12a through 12c show the radiographs of a 28-year-old professional baseball player who has ulnar-sided wrist pain and numbness and tingling in the fourth and fifth digits for the past 6 weeks. Management should consist of
Explanation
REFERENCES: Parker RD, Berkowitz MS, Brahms MA, et al: Hook of the hamate fractures in athletes. Am J Sports Med 1986;14:517-523.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 113-128.
Question 81
-are the anteroposterior (AP) and lateral radiographs of the right elbow of a 7-yearold boy who fell off the monkey bars onto his outstretched right hand. Immediate pain and swelling were noted around his elbow; there were no other injuries. His hand was neurovascularly intact. What is the best treatment for this fracture?

Explanation

Question 82
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Poehling GG, Whipple TL, Sisco L, Goldman B: Elbow arthroscopy: A new technique. Arthroscopy 1989;5:222-224.
Question 83
A 7-year-old boy sustained a 2-cm laceration to the anterior aspect of his left knee after falling on a rock. Examination reveals that the joint surface is not visible through the wound. Radiographs show no evidence of a foreign body or free air in the joint. Management should consist of
Explanation
REFERENCES: Voit GA, Irvine G, Beals RK: Saline load test for penetration of periarticular lacerations. J Bone Joint Surg Br 1996;78:732-733.
Leffers D: Dislocations and soft tissue injuries of the knee, in Browner BD (ed): Skeletal Trauma, ed 1. Philadelphia, PA, WB Saunders, 1992, pp 1717-1743.
Question 84
Which muscles are responsible for the displacement of the proximal fragment of the fracture shown in Figure 75?

Explanation
(SBQ12TR.39) A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
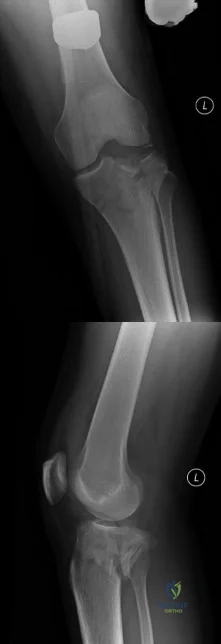
Popliteus and pes anserine
Lateral head of the gastrocnemius and pes anserine
Politeus and lateral head of the gastrocnemius
Iliotibial band and medial head of the gastrocnemius
Pes anserine and medial head of the gastrocnemius
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the
authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
Question 85
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70° of the right knee. The active arc of motion is from 70° to 90°, and the opposite knee has a flexion contracture of 10°. Both hips are dislocated with flexion contractures of 10°, passive hip motion is from 10° to 90° of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
REFERENCES: Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469.
DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Sells JM, Jaffe KM, Hall JG: Amyoplasia, the most common type of arthrogryposis: The potential for good outcome. Pediatrics 1996;97:225-231.
Question 86
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60 degrees F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis? Review Topic
Explanation
Question 87
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. This knee injury is best described as a

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 88
Figure 25 shows the radiograph of an 84-year-old woman who has pain and is unable to extend her knee. History reveals that she underwent total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss should consist of
Explanation
REFERENCES: Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241.
Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Clatworthy MG, Ballance J, Brick GW, et al: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 89
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
Question 90
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?
Explanation
REFERENCES: Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Blaha JD: Well-fixed acetabular component retention or replacement: The whys and the wherefores. J Arthroplasty 2002;17:157-161.
Question 91
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Explanation
REFERENCES: Kaplan FS, Singer FS: Paget’s disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Siris ES: Paget’s disease of bone, in Favus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. New York, NY, Raven Press, 1993, pp 375-384.
Question 92
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 93
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 94
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 95
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic
Explanation
Question 96
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
REFERENCES: Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 97
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
Question 98
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
Explanation
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996- 1002.
Question 99
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
Explanation
Question 100
Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be most appropriate for which of the following patients? Review Topic
Explanation
Combining a latissimus dorsi tendon transfers with reverse total shoulder arthroplasty (R-TSA) helps to restore control of active external rotation. Dysfunction with external rotation can be determined clinically with external rotation lag sign, a positive Hornblower's sign, and radiographically with fatty degeneration of the teres minor classified as stage 2 or greater according to the system of Goutallier et al. or Fuchs et al.
Gerber et al. found that R-TSA with combined lat dorsi transfer yielded minimal improvements in external rotation ROM (13 deg to 19 deg) compared to increases in shoulder ROM in flexion (94 deg to 137 deg) and abduction (87 deg to 145 deg), with this procedure.
Boileau et al. examined 17 consecutive patients treated with reverse shoulder arthroplasty and latissimus dorsi and teres major transfer (L'Episcopo). They found
that external rotation increased from -21 degrees to 13 degrees (+34 degrees ). They recommend transferring both the LD and TM, rather than the LD alone as it results in better active external rotation.
Illustration A is a radiograph showing a right reverse total shoulder replacement. Illustration B shows a cadaveric image of the positioning of the latissimus dorsi tendon transfer prior to implantation of the reverse total shoulder components.
Incorrect Answers
