Orthopedic Board Review MCQs: Trauma, Adult Reconstruction & Upper Extremity | Part 151

Key Takeaway
This page offers Part 151 of a comprehensive AAOS/OITE Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs, replicating actual exam formats. Designed for orthopedic residents and surgeons, this quiz is crucial for mastering topics like Arthroplasty and Hip, ensuring robust preparation for board certification.
About This Board Review Set
This is Part 151 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 151
This module focuses heavily on: Arthroplasty, Dislocation, Elbow, Fracture, Hip, Ligament, Osteoporosis, Tendon, Wrist.
Sample Questions from This Set
Sample Question 1: Rupture of the distal biceps tendon is predictably identified by the hook test, which is performed by bringing a finger from lateral to medial across the antecubital fossa of a flexed elbow, feeling for a cord-like structure on which the ex...
Sample Question 2: A 35-year-old skiier presents with pain in the left buttock and proximal posterior thigh after a fall. His clinical appearance is shown in Figure A. He is enrolled in 8 weeks of physical therapy after 2 weeks of rest, icing and NSAIDS. He r...
Sample Question 3: The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?...
Sample Question 4: A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved ...
Sample Question 5: A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Rupture of the distal biceps tendon is predictably identified by the hook test, which is performed by bringing a finger from lateral to medial across the antecubital fossa of a flexed elbow, feeling for a cord-like structure on which the examiner can "hook" a finger. Bringing the finger from medial to lateral can cause a false-negative result, hooking the lacertus fibrosus, which can remain intact even with a ruptured distal biceps tendon. The Yergason test (option 3) and the Speed test (option 4) are used to assist in diagnosing proximal, not distal, biceps and labral pathology. Even if the distal biceps tendon is ruptured, the supinator remains intact. Although supination weakness may be present, an inability to supinate should not be observed. When treating a closed long finger central slip tendon rupture conservatively, what is the most appropriate plan of care?
Explanation
Closed central slip injuries treated nonsurgically require extension splinting of the PIP joint. DIP joint active range of motion is allowed during this time period. This allows the connections between the lateral bands and the central slip to pull the central slip distally with DIP joint active motion, minimizing the gap
across the central tendon injury and keeping the DIP joint from getting stiff as well.
Question 2
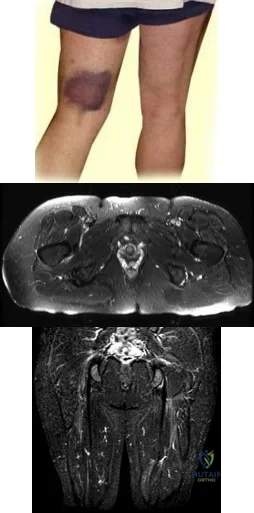
A 35-year-old skiier presents with pain in the left buttock and proximal posterior thigh after a fall. His clinical appearance is shown in Figure A. He is enrolled in 8 weeks of physical therapy after 2 weeks of rest, icing and NSAIDS. He returns for follow-up 6 months after his injury and has persistent ischial tuberosity pain with running. Examination confirms focal ischial tuberosity tenderness. MRI images are seen in Figures B and C. Which surgical option is most appropriate? Review Topic
Explanation
Untreated partial hamstring ruptures may present with residual pain, weakness and hamstring dysfunction. The mechanism is eccentric lengthening (sprinting or cutting) A proposed treatment algorithm is: (1) Nonoperative management for single tendon avulsion with <2cm retraction. The ruptured tendon scars to intact tendons. (2) Repair for acute 3-tendon rupture (semitendinosus, semimembranosus, biceps femoris) with retraction >= 2cm. (3) Surgery for young (<50y) patients with 2 tendon avulsion and retraction >= 2cm.
Bowman et al. examined the outcomes of operative management of partial hamstring tears in 17 patients. They found no postoperative difficulties with ADLs, and no recurrent surgery was required. All patients returned to their preoperative level of activity. They concluded that surgery can lead to good function with low complications and is reserved for patients who have failed nonoperative management.
Hofmann et al. retrospectively reviewed 19 patients with nonoperatively managed complete hamstring avulsions. They found diminished SF-12 scores, diminished hamstring strength at 45° and 90° of flexion (62% and 66%, respectively) compared with the normal side. They concluded that nonsurgical management leads to both subjective functional and objective strength deficits.
Figure A shows pronounced bruising from hematoma tracking following the injury. Figures B and C are coronal and axial images showing partial avulsion of the right hamstring insertion. The images correspond with Illustration B, with arrows pointing to the "sickle sign" . Illustration A shows the origins of the hamstring tendons. Illustration C shows the origins of the hamstring group (bf, biceps femoris; st, semitendinosus; sm, semimembranosus; qf, quadratus femoris; am, adductor magnus)
Incorrect Answers:
Question 3
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 4
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of “weeping” serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
REFERENCE: Killewich LA, Bedford GR, Black KW, et al: Diagnosis of deep venous thrombosis: A prospective study comparing duplex scanning to contrast venography.
Circulation 1989;79:810.
Question 5
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Paprosky WG (ed): Revision Total Hip Arthroplasty. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 64-69.
Question 6
03 A patient with carpometacarpal joint arthritis of the thumb undergoes trapezium excision and interposition arthroplasty. One year after treatment, radiographs reveal that there has been 25% subsidence of the thumb metacarpal compared with its preoperative height. This degree of subsidence will have what effect on the surgical outcome?
Explanation
pinch stress causes a large amount of axial compressive force through the CMC joint. They also compared preoperative and postoperative functional measurements, including key pinch strength, tipto-tip pinch strength, grip strength, and thumb ROM. Their findings were that postoperatively the first metacarpal subsided 21% at rest (p=0.001). and it subsided another 10.5% during maximal lateral key pinch. Even with this degree of subsidence, the patients experienced increases in pinch strength and grip strength. Also, all patients except for one who had bony impingement reported that they were subjectively much better and more functional.
Lin et. al. also studied trapezium excision and interposition arthroplasty and found no significant differences between results in patients with varying degrees of subsidence. Thus, subsidence does not affect the results of interposition arthroplasty for basal thumb arthritis.
back to this question next question
Question 7
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o’clock position? Review Topic
Explanation
Question 8
Which of the following body positions is associated with the highest intradiskal pressure?
Explanation
REFERENCES: Nachemson A, Morris JM: In vivo measurements of intradiscal pressure.
J Bone Joint Surg Am 1964;46:1077-1092.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 547-556.
Question 9
Which of the following statements best describes the location of the nerve that is at risk in a direct posterior approach to the Achilles tendon?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Fletcher MD, Warren PJ: Sural nerve injury associated with neglected tendo Achilles ruptures. Br J Sports Med 2001;35:131-132.
Question 10
Moderate distance running has what effect on knee articular cartilage in asymptomatic distance runners?
Explanation
Question 11
Nerve conduction velocity is slowed by
Explanation
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no association between hand dominance and nerve conduction velocity.
Question 12
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain?

Explanation
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 13
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
REFERENCES: Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 14
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of
Explanation
REFERENCES: Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-76.
Question 15
-The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the
Explanation

Question 16
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Explanation
REFERENCES: Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225.
Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Kerr CD, Sybert DR, Albarracin NS: An analysis of the flexor synovium in idiopathic carpal tunnel syndrome: Report of 625 cases. J Hand Surg Am 1992;17:1028-1030.
Question 17
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 18
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?
Explanation
REFERENCES: Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 19
A 77-year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 20
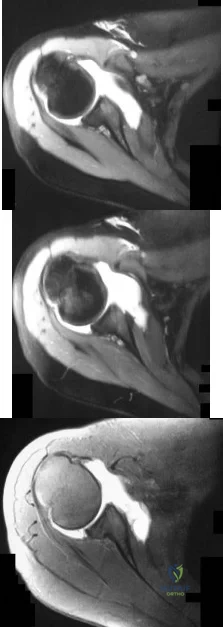
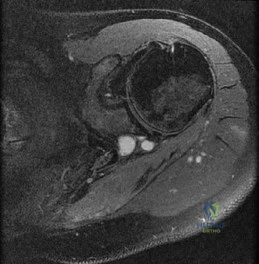
-Figures a through c are the MRI scans of a 21-year-old woman with recurrent shoulder instability and pain after an open anterior stabilization procedure. Positive belly-press test findings were positive.At surgery she was found to have an irreparable tear of the tendon injury identified preoperatively. The procedure to address the dynamic stabilizer deficit places which nerve at most risk?
Explanation
Question 21
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
REFERENCES: Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Post WR: Clinical evaluation of patients with patellofemoral disorders. Arthroscopy 1999;15:841-851.
Question 22
The Musculoskeletal Infection Society (MSIS) has adopted a definition of periprosthetic joint infection (PJI). This definition includes 2 major criteria and 5 minor criteria. Infection is present if 1 of 2 major criterions or 3 of 5 minor criterions are met. These criterions are
Explanation
In 2014, the MSIS published its revised PJI definition for clinical and research use. If 1 of 2 major criterions is met (phenotypically identical organisms obtained from 2 separate cultures or a draining sinus tract), then PJI is diagnosed. Alternatively, if 3 of 5 minor criterions are met, PJI is diagnosed.

Question 23
An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to
Explanation
Young age is a risk factor for early failure of cementless femoral components. Surgeons could consider cementing for patients older than 80 years of age. The Dorr classification has been shown to favor a cemented femoral stem in Dorr type C bone. Dorr type B bone can potentially sustain a proximally porous ingrowth stem. Osteoporosis is a risk factor for early failure of cementless femoral components.
Earlier designs for cemented femoral stems used microtexture to interlock the stem into the cement mantle. If these stems became loose, they would abrade the cement and loosen the stem further. Successful cemented femoral components are polished and have smooth edges with tapered bodies. Collars do not add to the design of femoral stems.
Patients are at risk for hypotension during the femoral pressurization process. With that in mind, the surgeon should make sure the anesthesiologist is ready to respond to hypotension. The FiO2 should be increased. The IV fluid rate also should be increased, and the anesthesiologist should be prepared with phenylephrine to support the patient’s blood pressure if he or she becomes hypotensive.

Question 24
In a fracture such as the one shown in Figure 16 (Salter-Harris type I fracture of the distal femur), which of the following best describes the location of the fracture?
Explanation
REFERENCES: Smith DG, Geist RW, Cooperman DR: Microscopic examination of a naturally occurring epiphyseal plate fracture. J Pediatr Orthop 1985;5:306-308.
Jaramillo D, Kammen BF, Shapiro F: Cartilaginous path of physeal fracture separations: Evaluation with MR
imaging: An experimental study with histologic correlation in rabbits. Radiology 2000;215:504-511. Question 17
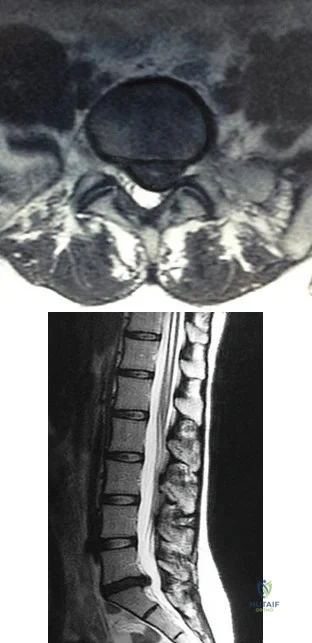
A 14-year-old boy has had a 3-month history of low back pain with no known trauma. The pain is worse with activity and relieved by rest, although he does report difficulty with prolonged sitting in school.
The patient was on the football team but stopped participating because of the back pain during football practice. He reports no history of radicular pain and denies any numbness, tingling, or weakness in the legs.
Neurologic examination is normal. Back examination reveals slight tenderness over the lower back area but no swelling or skin defects. Strength testing is 5 over 5 in the lower extremities and the straight leg raise test is negative. Back range of motion is nearly full, but back extension is painful. The hamstrings are slightly tight. Initial radiographs, including AP, lateral and oblique views, are negative. What is the best test to determine the patient’s diagnosis?
Flexion and extension lateral radiographs
MRI
Myelogram
Diskogram
Bone scan with SPECT PREFERRED RESPONSE: 5
DISCUSSION: A bone scan with SPECT is very sensitive and specific for spondylolysis not seen on initial
radiographs. MRI can sometimes visualize spondylolysis, but it is not as sensitive nor as specific as a bone scan with SPECT. Flexion and extension views have no role in the evaluation of the patient who presents with classic spondylolysis-type symptoms. The most sensitive physical examination finding is pain with back extension. Oblique radiographs can be obtained, but they are not as sensitive or specific as a bone scan with SPECT. The patient does not have any signs of a disk problem; therefore, an evaluation of the disk is not helpful.
REFERENCES: Hu SS, Tribus CB, Diab M, et al: Spondylolisthesis and spondylolysis. J Bone Joint Surg Am 2008;90:656-671.
Lawrence JP, Greene HS, Grauer JN: Back pain in athletes. J Am Acad Orthop Surg 2006;14:726-735.
Figure 18a Figure 18b
Question 25
A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm 3 (normal 3,500 to 10,500/ mm 3 ) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 26
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 27
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 28
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
REFERENCES: Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Bergsma JE, de Bruijn WC, Rozema FR, et al: Late degradation tissue response to poly
(L-lactide) bone plates and screws. Biomaterials 1995;16:25-31.
Question 29
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 30
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 31
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
Question 32
A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
the radial tuberosity.
Question 33
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
Explanation
REFERENCES: Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475.
McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement: Surgical technique. J Bone Joint Surg Am 2005;87:41-50.
Question 34
Which of the following best characterizes the injury shown in Figure 53? Review Topic

Explanation
Question 35
The patient is at highest risk for which complication?
Explanation
The quality of femoral neck fracture reduction was the key outcome factor in a number of studies. Capsulotomy is performed when achieving open reduction of the femoral neck. In rare cases in which acceptable closed reduction is achieved capsulotomy has been advocated, but poor anatomic reduction is more likely to negatively influence the outcome. Although some biomechanical data suggest that fixed-angle implants may be advantageous, this has not been demonstrated in well-controlled clinical studies. If reduction is not achieved, protecting postoperative weight bearing is not likely to improve outcomes.
Failure to achieve anatomic reduction of the femoral neck frequently leads to nonunion and varus collapse. Postoperative infection and/or heterotopic ossification are not typically seen in closed reduction and percutaneous stabilization of femoral neck fractures. Nonunion is more common than malunion of displaced femoral neck fractures.
RECOMMENDED READINGS
Duckworth AD, Bennet SJ, Aderinto J, Keating JF. Fixation of intracapsular fractures of the femoral neck in young patients: risk factors for failure. J Bone Joint Surg Br. 2011 Jun;93(6):811-6. doi: 10.1302/0301-620X.93B6.26432. PubMed PMID: 21586782. View
Abstract at PubMed
Yang JJ, Lin LC, Chao KH, Chuang SY, Wu CC, Yeh TT, Lian YT. Risk factors for nonunion in patients with intracapsular femoral neck fractures treated with three cannulated screws placed in either a triangle or an inverted triangle configuration. J Bone Joint Surg Am. 2013 Jan 2;95(1):61-9. doi: 10.2106/JBJS.K.01081. PubMed PMID: 23283374. View Abstract at
PubMed
Question 36
A 22-year-old man has mild hip pain bilaterally and multiple skeletal lesions. Based on the pelvic radiograph shown in Figure 30, what is the inheritance pattern for his disorder?
Explanation
REFERENCES: Stieber JR, Dormans JP: Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 2005;13:110-120.
Hilton MJ, Gutierrez L, Martinez DA, et al: EXT1 regulates chondrocyte proliferation and differentiation during endochondral bone development. Bone 2005;36:379-386.
Question 37
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
Explanation
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and paresthesias, are not supported by the evidence.
Question 38
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
REFERENCES: Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Lee S, James WC, Cohen BE, et al: Evaluation of hallux alignment and functional outcome after isolated tibial sesamoidectomy. Foot Ankle Int 2005;26:803-809.
Question 39
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0° to 125° of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of
Explanation
REFERENCES: Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133.
Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Smith GR, Altchek DW, Pagnani MJ, Keeley JR: A muscle-splitting approach to the ulnar collateral ligament of the elbow: Neuroanatomy and operative technique. Am J Sports Med 1996;24:575-580.
Question 40
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 241.
Question 41
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 42
A 29-year-old male sustained a mid-shaft femur fracture in a motor cycle accident. Even if asymptomatic, what additional radiographs must be obtained either preoperatively or intraoperatively before performing intramedullary nailing of the femoral shaft fracture?

Explanation
Question 43
The brachialis muscle is innervated by what two nerves?
Explanation
REFERENCES: Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
King A, Johnston GH: A modification of Henry’s anterior approach to the humerus. J Shoulder Elbow Surg 1998;7:210-212.
Question 44
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 45
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
Explanation
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.
REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.
Question 46
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?
Explanation
REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.
Question 47
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 48
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 49
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 50
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 51
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.
Question 52
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.
Neviaser RJ, Neviaser TJ, Neviaser JS: Anterior dislocation of the shoulder and rotator cuff rupture. Clin Orthop Relat Res 1993;291:103-106.
Question 53
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
REFERENCES: Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Malicky DM, Kuhn JE, Frisancho JC, et al: Nonrecoverable strain fields of the anteroinferior glenohumeral capsule under subluxation. J Shoulder Elbow Surg 2002;11:529-540.
Question 54
Which of the following is the only nonreversible effect of anabolic steroids? Review Topic
Explanation
Question 55
After the patient's wound has healed, which intervention is critical to prevent future ulceration?
Explanation
The most common etiology for plantar ulcers in patients with diabetes is neuropathy; 80% of these patients have adequate vascularity. The pathobiology is increased pressure applied on skin that lacks protective sensation (detected by lack of sensation to Semmes-Weinstein monofilament 5.07). The presence of sensation to light touch is not predictive of ulcer risk, but absent Semmes-Weinstein sensation at 5.07 carries a 30% risk for developing an ulcer. Intact light touch sensation does not rule out loss of protective sensation, and, therefore, does not rule out sensory neuropathy. The grading of an ulcer primarily depends on the existence of deep infection, either an abscess or osteomyelitis. In the presence of deep infection, formal surgical debridement is required. The surgery should be limited to the tissues
that are compromised, without an attempt at primary closure (which increases risk for recurrent infection). Negative-pressure dressings are a significant advance in postsurgical treatment by permitting delayed healing without further surgical intervention. Once healed, the key to preventing recurrent ulceration is the use of orthopaedic shoes with custom-molded soft inserts that accommodate the contours of the feet. This is particularly true when surgery has removed a portion of the foot; the foot otherwise will shift in a shoe that does not include a custom molded insert incorporating a filler that occupies the space left by the surgical resection.
RECOMMENDED READINGS
Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicenter trial. Diabetes Care. 2000 May;23(5):606-11. PubMed PMID: 10834417. View Abstract at PubMed Pinzur MS, Slovenkai MP, Trepman E, Shields NN; Diabetes Committee of American Orthopaedic Foot and Ankle Society. Guidelines for diabetic foot care: recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005 Jan;26(1):113-9. PubMed PMID: 15680122. View Abstract at PubMed Chantelau E. Effectiveness of diabetic therapeutic footwear in preventing reulceration: response to Maciejewski et al. Diabetes Care. 2004 Dec;27(12):3024-5; author reply 3025-
Question 56
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
Question 57
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
REFERENCES: Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 58
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 59
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 60
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 61
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include

Explanation
Question 62
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 63
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
Explanation
REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.
Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 64
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 65
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Johnson T, Steinbach L (eds): Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 44.
Question 66
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 67
- Work-related injuries to the lower back are most often related to which of the following risk factors?
Explanation
Question 68
Figure 4 shows the MRI scan of a patient who has had bilateral leg pain, weakness, diffuse numbness, and urinary retention for the past week. Examination reveals that motor strength is diffusely decreased, although it may be secondary to pain. The patient is numb throughout both legs, and reflexes in the lower extremities are absent. Rectal examination shows decreased tone, but voluntary tightening is present. Management should consist of
Explanation
REFERENCES: Kostuik JP, Harrington I, Alexander D, Rand W, Evans D: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, et al (eds): The Spine, ed 4. Philadelphia, PA,WB Saunders, 1992, vol 1,
pp 613-679.
Question 69
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
Explanation
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. View Abstract at PubMed
Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
A B
Question 70
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?
Explanation
REFERENCES: Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Ritter MA, Keating EM, Faris PM: Closed wound drainage in total hip or total knee replacement: A prospective, randomized study. J Bone Joint Surg Am 1994;76:35-38.
Question 71
A college athlete on a scholarship has a medical condition that you feel presents a life-threatening risk to him with participation in athletics. Because of the gravity of this decision and the potential effect it can have on the student/athlete's future, the college asks for your guidance. As the team physician for the college, what is your ethical obligation?
Explanation
Question 72
What method of spinal fixation requires the largest force to disrupt the bone-implant interface?
Explanation
Question 73
The arrow in Figure 39 is pointing to which of the following ligaments?
Explanation
REFERENCES: Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998,
pp 73-105.
Adams BD, Divelbiss BJ: Anatomy of the wrist ligaments, in Trumble TE (ed): Carpal Fracture-Dislocatons. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 1-5.
Question 74
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Explanation
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 75
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
REFERENCES: Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2001;83:661-667.
Question 76
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Explanation
Question 77
-A 14-year-old girl has a painless deformity of the right tibia. A radiograph from 2 years ago is seen in Figure a; nothing was done at that time. Her current radiograph is seen in Figure b. She has no pain, fever, or drainage. What is the most likely diagnosis?

Explanation
Question 78
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
REFERENCES: Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321.
Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 79
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 80
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
Explanation
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
Sclerosis of the proximal femoral epiphysis with subchondral lucency
Abnormal femoral head-neck junction offset
Widening of the proximal femoral physis with normal femoral head-neck junction offset
Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
Question 81
Figures 114a and 114b are the radiographs of a 5-year-old girl who fell from monkey bars. What is the first consideration regarding treatment for this injury? Review Topic

Explanation
Question 82
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic

Explanation
Question 83
A 19-year-old man was in a motorcycle accident. He sustained a grade IIIB open tibia fracture with a wide zone of injury to the surrounding soft tissue and a closed-head injury. The patient was treated emergently with irrigation, debridement, and external fixation. What is the most accurate statement regarding long-term functional and financial outcomes?
Explanation
Lower Extremity Assessment Project data suggest that long-term functional outcomes and patient satisfaction at 7 years are equivalent between those
who undergo limb-salvage and primary amputations. Return to work is essentially the same between the 2 groups. The projected lifetime healthcare cost for patients treated with amputation is nearly 3 times higher than costs for those who are treated with limb-salvage procedures.
RECOMMENDED READINGS
Busse JW, Jacobs CL, Swiontkowski MF, Bosse MJ, Bhandari M; Evidence-Based Orthopaedic Trauma Working Group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. J Orthop Trauma. 2007 Jan;21(1):70-6. PubMed PMID: 17211275. View Abstract at PubMed
MacKenzie EJ, Jones AS, Bosse MJ, Castillo RC, Pollak AN, Webb LX, Swiontkowski MF, Kellam JF, Smith DG, Sanders RW, Jones AL, Starr AJ, McAndrew MP, Patterson BM, Burgess AR. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007 Aug;89(8):1685-92. PubMed PMID: 17671005. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 85 THROUGH 88
Figures 85a and 85b are the plain radiographs of a 38-year-old man who fell off the roof of a 2-story house and sustained an isolated injury to his right knee. Examination reveals a swollen leg with a knee effusion. The skin is intact, but there are some abrasions and an obvious deformity. His neurovascular examination reveals active dorsiflexion and plantar flexion with some pain and symmetric palpable pulses

85A

B
Question 84
A 14-year-old boy has had a 3-month history of low back pain with no known trauma. The pain is worse with activity and relieved by rest, although he does report difficulty with prolonged sitting in school. The patient was on the football team but stopped participating because of the back pain during football practice. He reports no history of radicular pain and denies any numbness, tingling, or weakness in the legs. Neurologic examination is normal. Back examination reveals slight tenderness over the lower back area but no swelling or skin defects. Strength testing is 5 over 5 in the lower extremities and the straight leg raise test is negative. Back range of motion is nearly full, but back extension is painful. The hamstrings are slightly tight. Initial radiographs, including AP, lateral and oblique views, are negative. What is the best test to determine the patient's diagnosis? Review Topic
Explanation
have no role in the evaluation of the patient who presents with classic spondylolysis-type symptoms. The most sensitive physical examination finding is pain with back extension. Oblique radiographs can be obtained, but they are not as sensitive or specific as a bone scan with SPECT. The patient does not have any signs of a disk problem; therefore, an evaluation of the disk is not helpful.
(SBQ13PE.79) A 17-year-old male American football lineman presents with low back pain of insidious onset that is somewhat worse with activity. He has no neurologic complaints, night pain or fevers. His symptoms have been present for a few years but this is the first time he has sought medical attention. What physical examination finding is most likely to be found in this clinical scenario? Review Topic
Popliteal angle of 5 degrees
Heel cord tightness
Increased femoral anteversion
Pain with lumbar extension in single leg stance
Numbness of the skin of the anterolateral calf and dorsum of the foot
The patient demographics and clinical presentation are consistent with lumbar spondylolysis. Pain with lumbar extension is the most common physical exam finding.
Office assessment of the patient with spondylolysis should note pertinent negatives that would signify other causes of back pain. The history is most commonly negative for neurologic symptoms such as weakness or numbness, although patients will occasionally have radicular pain. On exam, patients may have localized spasm or tenderness, step off (if there is spondylolisthesis), hamstring tightness. The most common finding is pain with lumbar extension.
McCleary et al. review the diagnosis and treatment of spondylolysis in athletes. They identify three types of patients with spondylolysis: (1) female dancer or gymnast who is hyperlordotic, with increased motion and flexibility, (2) male weightlifter or football player undergoing a growth spurt, with decreased motion and flexiblity, especially of the spinal erectors, and (3) a novice athlete undergoing vigorous preparation for a new sport, with poor core strength and flexibility.
Incorrect
Question 85
Using methylmethacrylate to fill a biopsy hole in the diaphysis of a femur theoretically achieves what purpose?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 55-65.
Simon MA: Biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1982;64:1253-1257.
Question 86
Plate fixation without bone grafting
Explanation
Which of the following stress fractures most often requires internal fixation:
Question 87
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Explanation
REFERENCES: Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554.
Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 88
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?
Explanation
REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.
Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Tharani R, Nakasone C, Vince KG: Periprosthetic fractures after total knee arhtroplasty.
J Arthroplasty 2005;20:27-32.
Question 89
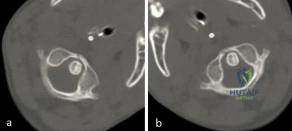
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 90
Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?

Explanation
Question 91
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 92
A 26-year-old elite female swimmer underwent a left medial meniscal allograft transplantation. She returns to clinic 3 years later with knee pain. What is the most likely cause for late presenting knee pain in this patient population? Review Topic
Explanation
Meniscal allograft transplantation is considered a salvage treatment option for young patients (<50 years old) with symptomatic meniscal deficiencies. The overall complication rate ranges from 4-36%, which include meniscal tearing, acute immune rejection, superficial and deep infection, chronic knee pain, etc. Graft tears make up
>50% of these complications.
Rath et al. evaluated 18 of 23 patients who had underwent meniscal allograft transplantation. They showed that 8 of 22 allograft menisci (36%) tore during the 8-year study period. They believe the decreased biologic activity of the graft over time may be a major factor that contributes to the high frequency of graft re-tearing.
Sekiya et al. reviewed meniscal allograft transplantation. They concluded that meniscal allograft transplantation may partially restore native meniscal function. Data has also shown that the progression of degenerative arthritic changes in transplanted meniscus-deficient knee compartments is slowed with this procedure.
Illustration A shows a basic schematic of meniscal transplantation. Here the graft is secured by anterior + posterior bone plugs and sutures to secure the transplanted meniscus into its native anatomical position.
Incorrect
<1%.
Question 93
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 94
- A high school distance runner reports a 3-week history of heel pain while running. Examination elicits no pain with dorsiflexion or with palpitation of the plantar fascia; however, pain is evident with palpitation over the muscular origin of the abductor hallucis. What is the most likely etiology of the pain?
Explanation
Question 95
-is the photograph of a 2-month-old infant with a left leg deformity. The mother’s pregnancy and delivery were unremarkable, and the infant is otherwise healthy. What is the most appropriate course of action?
Explanation


Question 96
Figure 57 is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment? Review Topic
Explanation
construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
Question 97
A 62-year-old runner injured his right ankle 8 weeks ago. He has ongoing lateral ankle pain and swelling that did not improve with 4 weeks of immobilization and 4 weeks of physical therapy. MR images demonstrate a longitudinal tear of the peroneus brevis tendon. Treatment should involve
Explanation
Additional nonsurgical treatment is not beneficial for peroneal tendon tears. Early repair of longitudinal tears reduces risk for progression to a full-thickness tear that would necessitate peroneus brevis to peroneus longus tenodesis. Platelet-rich plasma has no role in peroneal tendon tears.
RECOMMENDED READINGS
Arbab D, Tingart M, Frank D, Abbara-Czardybon M, Waizy H, Wingenfeld C. Treatment of isolated peroneus longus tears and a review of the literature. Foot Ankle Spec. 2014 Apr;7(2):113-8. doi: 10.1177/1938640013514273. Epub 2013 Dec 30. Review. PubMed
PMID: 24381076.View Abstract at PubMed
Coughlin MJ, Schon LC. Disorders of tendons. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014: 1188-1291.
RESPONSES FOR QUESTIONS 71 THROUGH 75
Lapidus procedure
First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
Proximal first metatarsal osteotomy
Distal first metatarsal chevron osteotomy
Biplanar distal first metatarsal osteotomy
Match the appropriate surgical procedure listed above with the clinical scenario described below.
Question 98
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 99
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 100
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
