Orthopedic Board Review MCQs: Knee Arthroplasty, Revision & Spine - Part 147

Key Takeaway
This page offers Part 147 of a high-yield orthopedic surgery board review MCQ bank for AAOS and OITE exam preparation. Authored by Dr. Mohammed Hutaif, it contains 100 verified questions in both study and exam modes, focusing on Arthroplasty, Knee, and Revision topics for orthopedic residents and surgeons.
About This Board Review Set
This is Part 147 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 147
This module focuses heavily on: Arthroplasty, Knee, Revision.
Sample Questions from This Set
Sample Question 1: Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?...
Sample Question 2: Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the excep...
Sample Question 3: Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic...
Sample Question 4: During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?...
Sample Question 5: Figures 21a and 21b show a transverse MRI scan at L4/5 and a lateral radiograph of a 75-year-old man with a 2-year history of worsening low back and bilateral leg pain that occurs with ambulation beyond approximately a half a block. Managem...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 2
Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the exception of an erythrocyte sedimentation rate (ESR) of 90 mm/h. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beatty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 3
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic

Explanation
Question 4
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
Question 5
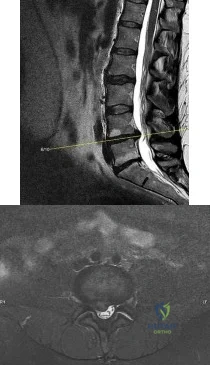
Figures 21a and 21b show a transverse MRI scan at L4/5 and a lateral radiograph of a 75-year-old man with a 2-year history of worsening low back and bilateral leg pain that occurs with ambulation beyond approximately a half a block. Management consisting of physical therapy, anti-inflammatory medications, and muscle relaxants has failed to successfully resolve his symptoms. He has minimal medical comorbidities. What is the best treatment approach for this patient? Review Topic

Explanation
Question 6
What is the most appropriate management at this time? Review Topic

Explanation
Question 7
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Fehring TK: Revision TJA corrects flexion extension gap imbalance. Orthop Today 2002;22:44.
Question 8
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of
Explanation
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
Question 9
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 10
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 11
You are staffing the prison clinic in a large public hospital when a 55-year-old African American male presents complaining of severe right hip pain. His pain has been ongoing for the past five years and limits his ambulation. He has never used medications for pain control or physical therapy. A radiograph is shown in figure
Explanation
healthcare delivery.
Physician bias, prejudice, discrimination, and clinical uncertainty are all factors that contribute to health care disparities in the United States. Implicit and explicit attitudes are cognitive traits that influence physician delivery of care, and sometimes these attitudes do not perfectly correspond. It is important for a physician to understand that his implicit attitudes about a patient may unintentionally influence care despite his explicit attitudes. Physicians should be aware of their implicit biases in order to provide more effective decision-making and quality of care.
Stone et al. write about the issue of culturally competent delivery of care and the avoidance of unconscious bias in medical decision making. They argue that because unconscious stereotypes and prejudices can trigger biased medical decisions against specific groups, leading to the creation of differential diagnoses, disparities in treatment, and causing minorities to feel uncomfortable with seeking or complying with treatment plans. The authors suggest the integration of cultural competency training into medical education in order to help understand the perspective of the minority group patient.
Sabin et. al. compared the implicit and explicit biases of physicians with respect to race, gender, and age. They found that medical doctors showed an implicit bias of preferentially caring for White Americans relative to Black Americans, independent of the doctors’ self-report (explicit biases). Doctors'implicit biases exceeded their explicit biases in all race groups studied, except for African American physicians, who did not show an implicit bias toward patients.
Figure A demonstrates an AP pelvis x-ray with severe arthrosis of the right hip. The left hip demonstrates moderate disease.
Incorrect Answers:
Question 12
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 13
A 12-year-old girl has painless bowing of the tibia. Radiographs and a biopsy specimen are shown in Figures 35a through 35c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 14
Soft-tissue sarcomas most commonly metastasize to the
Explanation
REFERENCES: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Enzinger FM, Weiss SW, Goldblum F: Soft Tissue Tumors, ed 4. Washington, DC, Mosby/AFIP, 2001.
Question 15
-The World Health Organization Fracture Risk Assessment Tool (FRAX) calculates which fracture risk?
Explanation
Question 16
A year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 17
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 18
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 19
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Evans D: Calcaneo-valgus deformity. J Bone Joint Surg Br 1975;57:270-278.
Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot: Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995;77:500-512.
Question 20
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
Question 21
A 70-year-old man is experiencing neck pain, progressive weakness, and numbness in his arms and legs without bowel or bladder dysfunction or dysphagia. Upon examination, he has atrophy of his upper extremities but normal muscle bulk in his legs. Strength is diffusely 4/5 throughout. Cervical spine radiographs show spondylosis. Electromyography (EMG) reveals fibrillations with increased amplitude in the extensor carpi radialis and pronator teres. Nerve conduction studies demonstrate slowing conduction diffusely in the sural, peroneal, and ulnar nerves, and severe slowing in the median nerve. Testing of the tongue and thoracic paraspinal muscles does not show fibrillations or positive short waves. What is the most likely diagnosis? Review Topic
Explanation
Question 22
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hgb is 8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?

Explanation
prolonged, invasive surgery. Upper extremity fractures are best managed acutely with splints in this clinical setting. Definitive fracture fixation should be delayed until the patient is adequately resuscitated.
Question 23
The CT scan shows the involvement area is approximately 30% of the posterior facet. What is the most appropriate treatment?
Explanation
Radiographs reveal a talocalcaneal coalition. The incidence of tarsal coalition in the general population ranges between 2% and 13%. The incidence of tarsal coalition among patients with FGFR-related craniosynostosis syndromes is much higher than among the general population. Tarsal coalitions have been noted in FGFR-1-, FGFR-2-, and FGFR-3-related craniosynostosis syndromes of Apert, Pfeiffer, Crouzon, Jackson-Weiss, and Muenke, but not in Beare-Stevenson or Crouzonodermoskeletal syndromes. The FGFR genes are involved in cell proliferation, differentiation, migration, apoptosis, and pattern formation.
Additionally, nonsyndromic familial coalitions have been described with autosomal-dominant patterns of inheritance.
Cross-sectional imaging should always be obtained prior to resection of a radiographically evident coalition to define the extent of the coalition and determine the coexistence of an additional coalition. CT scan is the gold standard test; however, MRI can be helpful to define a suspected fibrous coalition if a CT scan is nondiagnostic. A bone scan may be useful if pain or history is atypical for a symptomatic coalition. Laboratory tests such as CBC, ESR, CRP, ANA, and RF may be indicated if the imaging evaluation does not confirm a tarsal coalition and if there is concern for malignancy, infection, or inflammatory arthritis.
Investigators have suggested that larger talocalcaneal coalitions with surface areas larger than 33% to 50% of the size of the posterior facet are unsuitable for resection and primary arthrodesis should be considered. However, a study by Koshbin and associates found that with long-term follow-up, favorable functional outcomes were seen even with resections of large talocalcaneal coalitions occupying more than 50% of surface area.
Question 24
A 35-year-old physical therapist presents with right-sided back and leg pain. For the last 4 months, he has taken anti-inflammatory medications and performed exercises on his own. While his back pain has improved slightly, his leg pain remain severe and interferes with his ability to sleep and work. Examination reveals positive ipsilateral and contralateral straight leg raise at 30 degrees. He has mildly diminished big toe dorsiflexion strength on the right side. There is a small patch of diminished sensation on the dorsum of the foot. MRI scans are shown in Figures A and B. What is the most appropriate next step in treatment? Review Topic
Explanation
For lumbar disc herniation, the first line of treatment is rest, physical therapy and oral medications (NSAIDs, gabapentin, steroids). The second line of treatment is selective nerve root corticosteroid injections. The last line in treatment is laminotomy and discectomy.
Pearson et al. determined which individuals (as opposed to groups) in the SPORT (Spine Patients Outcomes Research Trial) would benefit from surgery. They found that disc herniation patients improved more with surgery than without.
Lurie et al. reviewed the 8 year outcomes of the SPORT. In patients with HNP on imaging and leg symptoms persisting for at least 6 weeks, surgery was superior to nonoperative treatment in relieving symptoms and improving function.
Figures A and B are sagittal and axial T2-weighted MRI images showing a large L4/L5 herniated disc causing neural foramina narrowing and impinging on the right L5 root.
Incorrect Answers:
Question 25
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
Explanation
REFERENCES: Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
McCarty EC, Warren RF, Deng XH, et al: Temperature along the axillary nerve during radiofrequency-induced thermal shrinkage. Am J Sports Med 2004;32:909-914.
Question 26
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 27
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
REFERENCES: Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 28
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
REFERENCE: O’Connell SJ, Moore MM, Strickland JW, Frazier GT, Dell PC: Results of zone I and zone II flexor tendon repairs in children. J Hand Surg Am 1994;19:48-52.
Question 29
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
REFERENCE: Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
Question 30
Which of the following is a significant risk factor for airway complications after anterior cervical surgery? Review Topic
Explanation
Question 31
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?
Explanation
REFERENCES: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Simon MA, Karluk MB: Skeletal metastases of unknown origin: Diagnostic strategy for orthopedic surgeons. Clin Orthop Relat Res 1982;166:96-103.
Question 32
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 33
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 34
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed
Explanation
REFERENCE: Murphy SB: Tibial osteotomy for genu varum: Indications, preoperative planning, and technique. Orthop Clin North Am 1994;25:477-482.
Question 35
- The Magnetic resonance imaging signal characteristics of a high-grade soft-tissue sarcoma are best described as
Explanation
other characteristics, such as size, pattern of growth, integrity of natural boundaries, and homogeneity.
Intravenous contrast agents are not necessary to evaluate neurovascular structures. Both the T1 & T2 weighted images are essential to detect and characterize soft tissue lesions.
Most Tumors have long T1 and T2 relaxation times, therefore, in most instances signal intensity alone is of limited benefit. Exceptions are lipoma, hematoma, intra-lesional hemorrhage.
Hemorrhage may occur in some soft tissue lesions, especially sarcomas, leading to the low T1 and high T2 intensity sound on MR. Miller, indicates that Water, CSF, acute hemorrhage and soft tissue tumors appear dark on T1 and light on T2.
Question 36
A 66-year-old female presents to your clinic complaining of back pain, difficulty standing-up straight, weakness in her legs, and neurogenic claudication. On upright thoracolumbar radiographs, there is a 75 degree thoracolumbar curve with the apex at L2, and the C7 plumb line falls 12 cm anterior to the posterosuperior corner of S1. Aside from a decompression of the stenotic levels, which of the following choices will lead to the MOST reliable decrease in overall disability? Review Topic
Explanation
Spinal malalignment in Adult Spinal Deformity (ASD) challenges balance mechanisms used for maintenance of an upright posture to achieve the basic human needs of preserving level visual gaze and retaining the head over the pelvis. Severe malalignment can result in greater muscular effort and energy expenditure to maintain the erect posture as well as use of compensatory mechanisms. As such, surgical correction of these deformities are aimed at achieving proper spinopelvic alignment.
Glassman et al. performed a multi-center retrospective study of 298 adults with spinal deformity. Regardless of operative (129 patients) or non-operative care (172 patients) a positive sagittal balance was the found to be the most reliable predictor of clinical symptoms in both patient groups.
Schwab et al. published a current concepts review on operative management for adult spinal deformities and identified three major goals of surgery: (1) Correct the SVA to
within 5 cm of neutral, (2) Ensure the pelvic tilt is less than 20 degrees, (3) Ensure the lumbar lordosis is within 9 degrees of the pelvic incidence.
Illustration A demonstrates how to measure the SVA. Illustration B depicts the realignment objectives in the saggital plane as described by Schwab et al.
Incorrect
Question 37
A 24-year-old man sustained a bilateral C5-6 facet dislocation in a car accident and was intubated at the scene. He remains sedated in the intensive care unit
Explanation
Question 38
Dorsal intercalated segment instability (DISI) describes which carpal deformity?
Explanation
Question 39
preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Explanation
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Central space
Hypothenar space
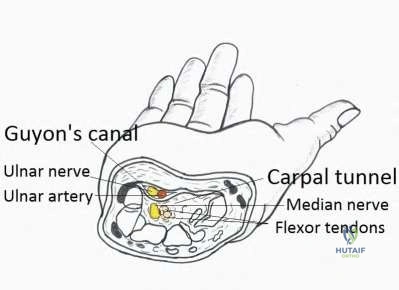
Carpal tunnel
Posterior adductor space
Thenar space CORRECT ANSWER: 5
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection.
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Medial antebrachial cutaneous
Lateral antebrachial cutaneous
Posterior antebrachial cutaneous
Medial brachial cutaneous
Dorsal antebrachial cutaneous
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure
Question 40
The placement of supplemental screw fixation with acetabular component fixation is a typical adjunct measure but carries the greatest risk of vascular injury if placed in which of the following positions?
Explanation
REFERENCES: Lavemia CJ, Cook CC, Hernandez RA, et al: Neurovascular injury in acetabular reconstruction cage surgery: An anatomical study. J Arthroplasty 2007;22:124-132.
Wasielewski RC, Galat DD, Sheridan KC, et al: Acetabular anatomy and transacetabular screw fixation at the
high hip center. Clin Orthop Relat Res 2005 ;43 8:171 -176.
Question 41
A 65-year man has right hip pain after a fall. Radiographs reveal a reverse oblique intertrochanteric femoral fracture. Treatment consists of reduction and internal fixation. Which of the following implants is most commonly associated with nonunion and hardware failure?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DB: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Baumgaertner MR, Chrostowski JH, Levy RN: Intertrochanteric hip fracture, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1833-1881.
Question 42
- A patient who had previously undergone a salvage pelvic (Chiari) osteotomy now requires a total hip arthroplasty. The most frequent complication of this procedure is
Explanation
Question 43
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 44
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 45
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
REFERENCE: Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 46
Which of the following is an advantage of using blocking screws for tibial nailing?

Explanation
Krettek found that medial and lateral blocking screws can increase the primary stability of distal and proximal metaphyseal fractures after nailing and can be an effective tool for selected cases that exhibit malalignment and/or instability by decreasing mechanically measured deformation.
In a later clinical study, Krettek found that after using blocking screws, tibial healing was evident radiologically at a mean of 5.4 months with a decreased rate of malunions.
Ricci also found that blocking screws are effective to help obtain and maintain alignment of fractures of the proximal third of the tibial shaft treated with intramedullary nails.
Question 47
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 48
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
REFERENCES: Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Clanton TO, Coupe KJ: Hamstring strains in the athlete: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 49
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic

Explanation
Question 50
Figure 1 is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?

Explanation
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A "V sign" (Figure 2) is evident, indicating dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress. Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 3 through 5.






Question 51
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
REFERENCES: Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 52
Which stress fracture location is reported most frequently among ballet dancers?
Explanation
Stress fractures are a frequent overuse injury among professional ballet dancers. The most common location is at the proximal metaphyseal-diaphyseal junction of the second metatarsal. Repetitive stress injuries and fractures of the tibial sesamoid, tarsal navicular, and base of the fifth metatarsal occur among other athletes.
RECOMMENDED READINGS
O'Malley MJ, Hamilton WG, Munyak J, DeFranco MJ. Stress fractures at the base of the second metatarsal in ballet dancers. Foot Ankle Int. 1996 Feb;17(2):89-94. PubMed PMID: 8919407. View Abstract at PubMed
Micheli LJ, Sohn RS, Solomon R. Stress fractures of the second metatarsal involving Lisfranc's joint in ballet dancers. A new overuse injury of the foot. J Bone Joint Surg Am. 1985 Dec;67(9):1372-5. PubMed PMID: 4077907. View Abstract at PubMed
Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int. 2006 Sep;27(9):750-7. Review. PubMed PMID: 17038292. View Abstract at PubMed
Question 53
A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm 3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
Explanation
REFERENCES: Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Leslie BM, Harris JM, Driscoll D: Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
Question 54
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 55
A 2-year-old boy has been referred for musculoskeletal evaluation. Examination reveals shortened proximal limbs, hip and knee flexion contractures, an abducted thumb, and ear abnormalities. His parents are concerned about his deformed feet. What is the most common foot deformity associated with this patient’s diagnosis?
Explanation
REFERENCES: Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
Bussett GS: The osteochondrodysplasias, in Morrissy RT, Weinstein S (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, p 219.
Question 56
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 57
A 17-year-old football player is unable to flex the distal interphalangeal (DIP) joint of his ring finger. He states that he injured the finger 6 weeks ago while attempting to tackle another player who pulled free from his grip, but he did not inform his coach at the time of the injury. Current radiographs show an observable fleck of bone volar to the base of the proximal phalanx. Treatment should consist of
Explanation
REFERENCES: Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin
1985;1:77-83.
Kiefhaber TR: Closed tendon injuries in the hand. Oper Tech Sports Med 1996;4:227-241.
Question 58
The failure of the acetabular component shown in Figure 15 is most likely the result of the use of a 32-mm head and
Explanation
REFERENCE: Astion DJ, Saluan P, Stulberg BN, Rimnae CM, Li S: The porous-coated anatomic total hip prosthesis: Failure of the metal-backed acetabular component. J Bone Joint Surg Am 1996;78:755-766.
Question 59
The main blood supply to the lateral two thirds of the talar body is provided by the
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1465-1518.
Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115-1120.
Question 60
You have been waiting to enroll a patient into your recent institutional review board (IRB)-approved clinical research protocol. A patient is admitted who, upon initial screening, meets all inclusion criteria. However, he has late-stage dementia, and you are told by your research coordinator that this condition is an exclusionary criterion. This scenario demonstrates the need for which aspect of proper informed consent?
Explanation
Question 61
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
REFERENCES: Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 62
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?

Explanation
Question 63
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Explanation
REFERENCES: Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554.
Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 64
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Explanation
REFERENCE: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 65
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Kamineni S, Hirahara H, Pomianowski S, et al: Partial posteromedial olecranon resection:
A kinematic study. J Bone Joint Surg Am 2003;85:1005-1011.
Question 66
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 67
What is the most common turf toe mechanism of injury?
Explanation
Turf toe, or capsuloligamentous injury to the first MTP joint, most commonly is caused by an axial load being applied to a fixed, dorsiflexed great toe with the heel off the ground. The external force causes further dorsiflexion of the great toe, leading to injury to the capsuloligamentous complex. A less common mechanism of turf toe is hyperplantarflexion of the great toe with valgus stress, which is seen in beach volleyball players.
RECOMMENDED READINGS
Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. View Abstract at PubMed
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
Question 68
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
Explanation
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Kitaoka HB, Holiday AD Jr: Lateral condylar resection for bunionette. Clin Orthop 1992;278:183-192.
Question 69
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
REFERENCES: DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.
Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.
Question 70
Physiologic bowing of the lower extremities should spontaneously correct by what age?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 7.
Salenius P, Vankka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am
J V :
Question 71
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?

Explanation
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette of the shoulder and is a stabilizer of the humeral head.
Question 72
Figures 1 and 2 are the radiographs of a 55-year-old woman homemaker with a 1-year history of insidious onset left wrist pain. She has failed conservative treatment and desires surgery. Her medical history is complicated by a smoking history of 1.5 packs of cigarettes per day. At the time of surgery her capitate articular surface is normal in appearance. The best procedure for her would be

Explanation
This patient has Lichtman stage 3B Kienbock disease. She is 55 years old and is a "low-demand" patient; however, she is a heavy smoker. Based on her condition and her current smoking status, salvage treatment that does not require bone healing such as a proximal row carpectomy is likely the best treatment option. A radial shortening osteotomy and a capitate shortening osteotomy may be helpful in offloading the lunate, but both procedures require bone healing and are better options in earlier stages of Kienbock disease. A scaphoid excision and four-corner fusion is typically performed for scapholunate advanced collapse or scaphoid nonunion advanced collapse wrist arthritis and would not be recommended in this scenario, as the lunate is avascular.
Question 73
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 74
A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?
Explanation
REFERENCES: Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Weigelt JA: Resuscitation and initial management. Crit Care Clin 1993;9:657-671.
Question 75
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
REFERENCES: Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA
2003;290:2549-2555.
Question 76
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following? Review Topic
Explanation
Question 77
82 • American Academy of Orthopaedic Surgeons A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 78
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
REFERENCES: Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 79
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 80
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 81
A 12-year-old girl is seen after tripping and twisting her ankle earlier in the morning. She had immediate pain and swelling and was unable to bear weight. Radiographs are shown in Figures 80a through 80c. Appropriate treatment should consist of which of the following? Review Topic

Explanation
Question 82
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option? Review Topic

Explanation
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion.
Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty.
Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position.
Incorrect Answers:
Question 83
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 84
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?

Explanation
Question 85
-A 75-year-old woman fell at home and sustained the injury seen in Figures 249a through 249c. What is the most appropriate treatment option?
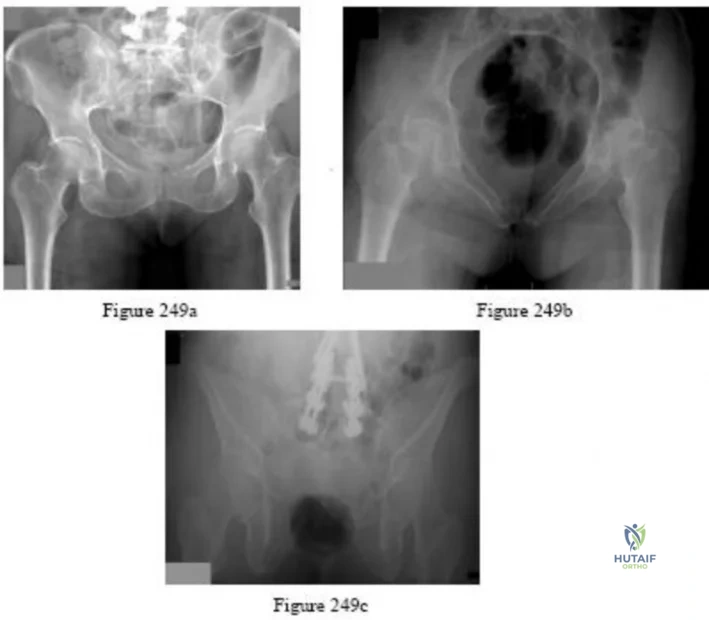
Explanation

Question 86
While performing a total shoulder arthroplasty, excessive retraction is placed on the "strap muscles" (short head of biceps and coracobrachialis). Neurovascular examination would reveal weakness of which of the following? Review Topic
Explanation
this area. Excessive traction on the musculocutaneous nerve could lead to a neurapraxia with resultant weakness of elbow flexion and forearm supinaton because of the loss of biceps function.
Question 87
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
REFERENCE: Schmade GA, Conrad EV III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
Question 88
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Explanation
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 89
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of Review Topic

Explanation
Question 90
A 10-month-old infant has no flexion at the elbows, mild flexion contractures at the wrist, a rigid clubfoot deformity on the left foot, and a rigid rocker bottom deformity on the right foot. Examination of the patient's hips reveals limited
Explanation
Question 91
During the implantation of a cementless acetabular component in total hip arthroplasty, placement of a screw in the anterior superior quadrant puts which of the following structures at risk for damage?
Explanation
REFERENCES: Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws. J Bone Joint Surg Am 1990;72:509-511.
Wasielewski RC, Cooperstein L, Kruger MP, Rubash HE: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am
1990;72:501-508.
Question 92
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include Review Topic
Explanation
(SBQ13PE.60) If a child develops dynamic supination after treatment of idiopathic clubfoot with Ponseti casting, at what age would it be appropriate to consider transfer of the tibialis anterior tendon to the lateral dorsum of the foot? Review Topic
In the first six months of life, immediately following failed cast treatment
12 months
4 years
12 years
15 years
Tibialis tendon transfer to the dorsum of the foot should be performed to address dynamic supination when the lateral cuneiform has ossified. This is typically after at least 2 years of age and usually not before age 3.
Question 93
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 94
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Herscovici D Jr, Sanders RW, Scaduto JM, et al: Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma 2003;17:683-688.
Question 95
Figure 49 shows the radiograph of a 3-year-old child with progressive bowlegs. Laboratory studies show a calcium level of 9.5 mg/dL (normal 9.0 to 11.0 mg/dL), a phosphorus level of 4.2 mg/dL (normal 3 to 5.7 mg/dL), and an alkaline phosphatase level of 305 IU/L (normal 104 to 345 IU/L). What is the most likely diagnosis?
Explanation
REFERENCES: Lachman RS, Rimoin DL, Spranger J: Metaphyseal chondrodysplasia - Schmid type: Clinical and radiographic delineation with a review of the literature. Pediatr Radiol 1988;18:93-102.
Warman ML, Abbot M, Apte SS, et al: A type X collagen mutation causes Schmid metaphyseal chondrodysplasia. Nat Genet 1993;5:79-82.
Question 96
Which of the following assessment tools most accurately reflects outcomes of well-being, daily function, and general health in a patient treated for cervical myelopathy?
Explanation
REFERENCES: Albert TJ, Mesa JJ, Eng K, McIntosh TC, Balderston RA: Health outcome assessment before and after lumbar laminectomy for radiculopathy. Spine 1996;21:960-963.
Swiontkowski MF, Buckwalter JA, Keller RB, Haralson R: The outcomes movement in orthopaedic surgery: Where we are and where we should go. J Bone Joint Surgery Am 1999;81:732-740.
Ludwig SC, Albert TJ: Measuring outcomes in cervical myelopathy and radiculopathy.
Instr Course Lect 1999;48:417-421.
Question 97
Figure 53 is the radiograph obtained at the time of transfer to the trauma center of a 41-year-old man who was involved in a motor vehicle accident. What is the most appropriate initial management?

Explanation
Question 98
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;109:15-18.
Question 99
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 100
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
REFERENCES: Allan DG, Lavoie GJ, Rudan JF, et al: The use of allograft bone in revision total hip arthroplasty, in Friedlaender GE, Goldberg VM (eds): Bone and Cartilage Allografts: Biology and Clinical Applications. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1991, pp 263-264.
Gross AE, Lavoie MV, McDermott P, Marks P: The use of allograft bone in revision of total hip arthroplasty. Clin Orthop 1985;197:115-122.
Head WC, Berklacich FM, Malinin TI, Emerson RH Jr: Proximal femoral allografts in revision total hip arthroplasty. Clin Orthop 1987;225:22-36.
