Orthopedic Surgery Board Review MCQs: Arthroplasty, Foot & Ankle, Trauma | Part 141

Key Takeaway
This page offers Part 141 of a professional orthopedic surgery board review. It contains 100 verified, high-yield MCQs for AAOS and OITE exam preparation. Designed for orthopedic residents and surgeons, it features study and exam modes with detailed clinical explanations to ensure comprehensive certification readiness.
About This Board Review Set
This is Part 141 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 141
This module focuses heavily on: Arthroplasty, Foot, Hip, Knee, Revision, Trauma.
Sample Questions from This Set
Sample Question 1: A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should...
Sample Question 2: Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of...
Sample Question 3: A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?...
Sample Question 4: A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?...
Sample Question 5: A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hi...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 2
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 3
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
REFERENCES: Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
Kibler WB (ed): ACSM’s Handbook for Team Physician. Philadelphia, PA,
Williams & Wilkins, 1996, p 151.
Question 4
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
REFERENCES: Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423.
Question 5
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 6
03 A patient with carpometacarpal joint arthritis of the thumb undergoes trapezium excision and interposition arthroplasty. One year after treatment, radiographs reveal that there has been 25% subsidence of the thumb metacarpal compared with its preoperative height. This degree of subsidence will have what effect on the surgical outcome?
Explanation
pinch stress causes a large amount of axial compressive force through the CMC joint. They also compared preoperative and postoperative functional measurements, including key pinch strength, tipto-tip pinch strength, grip strength, and thumb ROM. Their findings were that postoperatively the first metacarpal subsided 21% at rest (p=0.001). and it subsided another 10.5% during maximal lateral key pinch. Even with this degree of subsidence, the patients experienced increases in pinch strength and grip strength. Also, all patients except for one who had bony impingement reported that they were subjectively much better and more functional.
Lin et. al. also studied trapezium excision and interposition arthroplasty and found no significant differences between results in patients with varying degrees of subsidence. Thus, subsidence does not affect the results of interposition arthroplasty for basal thumb arthritis.
back to this question next question
Question 7
A 70-year-old female presents with right thigh ache for 6 months. Except for a history of osteoporosis, she is otherwise healthy. She has been on antiresorptive therapy for 8 years. Her radiograph is shown in Figure A. Four months later, she trips over a rug and falls, sustaining the injury shown in Figures B and C. Which of these statements is TRUE regarding surgical fixation of this fracture compared with conventional fractures?

Explanation
Subtrochanteric fractures are fractures extending from the lesser trochanter to 5cm distal to it. BP fractures are characterized by (1) focal lateral cortical thickening, (2) transverse fracture orientation, (3) medial spike and (4) lack of comminution. There is increased risk of iatrogenic fracture with IM nailing because BP fractures have thickened, brittle cortices and the mismatch between medullary diameter and increased proximal nail diameter results in iatrogenic fracture.
Weil et al. reviewed the outcome of surgically treated bisphosphonate fractures. IM nailing resulted in healing in 54% of bisphosphonate fractures with 98-99% of conventional fractures. In their study, 46% required revision procedures.
Prasarn et al. compared plate and nail treated bisphosphonate fractures with conventional fractures. They found that the bisphosphonate group had more major and minor complications (68%) than the conventional group (10%). The most common complications were intraoperative femoral shaft comminution (nail) and hardware failure (plate).
Figure A shows diffuse cortical thickening with an antero-lateral cortical ridge. Figure B shows a transverse subtrochanteric fracture extending through the middle of the cortical ridge seen previously. Note also healed fractures of the left superior and inferior rami. Figure C is a post-reduction radiograph showing the transverse fracture through the beak-shaped region of the previous insufficiency fracture. Illustration A shows a typical bisphosphonate-related fracture with transverse fracture orientation,
focal lateral cortical thickening (white arrows), medial beak (black arrow), and lack of comminution. Illustration B shows a conventional subtrochanteric fracture. Illustration C shows intraoperative iatrogenic fracture with anterolateral comminution during nailing. Illustration D shows fixation with a proximal femoral hook LCP Plate with late hardware failure at 3 months.
Incorrect Answers:
Question 8
Refers to the effectiveness of various antibiotics against a particular microorganism.
Explanation
Knowledge of the basic nomenclature of antibiotic use is important to effectively treat patients and communicate with colleagues. The effectiveness of an antimicrobial against an infecting organism is measured by the MIC, which refers to the concentration needed to prevent growth of a microorganism on culture medium, and MBC, which is the smallest concentration of the antibiotic necessary to kill the microorganism in culture. Typically, an antibiotic is considered bactericidal if the MBC is no more than 4 times the MIC. The spectrum of antimicrobial coverage refers to an agent’s effectiveness against a range of bacteria. An antibiogram refers to the tabulation of prevalence of different bacteria in a specific setting or specific patient population. Antibiotic susceptibility and resistance refers to the bacteria’s ability to be affected or unaffected by a given antibiotic.

Question 9
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
REFERENCES: Winiarsky R, Barth P, Lotke P: Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770-1774.
Stern SH, Insall JN: Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400-1404.
Griffin FM, Scuderi GR, Insall JN, Colizza W: Total knee arthroplasty in patients who were obese with 10 years follow-up. Clin Orthop 1998;356:28-33.
Question 10
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
REFERENCES: Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998,
pp 235-238.
Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Question 11
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 12
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 13
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the
Explanation
REFERENCE: Coleman SS, Chestnut WJ: A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop 1977;123:60-62.
Question 14
Patient-specific instrumentation (PSI) reliably demonstrates which benefit over conventional intramedullary guidance systems?
Explanation
Cost is usually increased with PSI because the theoretical decreased number of surgical trays and shortened surgical time do not offset cost of presurgical imaging and extra cost associated with the necessary jigs. Studies do not demonstrate a reliable improvement in functional outcomes or coronal alignment when PSI is compared to standard instrumentation. Evidence reveals that PSI necessitates fewer trays than standard instrumentation.
Question 15
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
REFERENCES: Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Raaymakers EL: Complications of talar fractures, in Tscherne H, Schatzker J (eds): Major Fractures of the Pilon, the Talus, and Calcaneus: Current Concepts of Treatment. Berlin, Springer-Verlag, 1993, pp 137-142.
Question 16
Figure 49 shows an acute axial MRI scan of a left knee. What is the most likely diagnosis?
Explanation
REFERENCES: Elias DA, White LM, Fithian DC: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 17
-The Coleman block test is used to test for
Explanation

Question 18
Which of the following statements is true regarding articular cartilage?
Explanation
Proteoglycans, the most common of which is aggrecan, are produced by chondrocytes and give articular cartilage its hydrophilic properties. Multiple glycosaminoglycans (GAGs), such as chondroitin and keratin can attach to core proteins to form aggrecans. Link proteins then help aggrecans interact with hyaluronic acid. The negative charge of this complex helps create a strong osmotic gradient, which attracts water and increases tissue pressures. Normal aging involves a decrease in the water content of the extracellular matrix while osteoarthritis is associated with increased water content, which leads to loss of strength and elasticity.
Chen et al. evaluated the strain and depth related properties of articular cartilage in bovine models. They found that the zero-strain permeability, zero-strain equilibrium confined compression modulus, and deformation dependence constant differed among the layers of cartilage. They suggest that the complex strain-dependent properties of articular cartilage of different thickness and location have clinical implications for tissue engineering.
Illustration A is a diagram depicting the extracellular matrix of articular cartilage. Incorrect Answers:
Question 19
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of
Explanation
REFERENCES: Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Parvizi J, Wade FA, Rapuri VR, et al: Revision hip arthroplasty for late instability secondary to polyethylene wear. Clin Orthop 2006, in press.
Question 20
-An infant was born with complex syndactyly involving all 4 fingers of both hands, short and deformed thumbs, and similar syndactyly involving both feet. In addition, an altered facial appearance was noted with protruding eyes, a towered cranium, and midface hypoplasia. This appearance is characteristic of which syndrome?
Explanation
Question 21
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 22
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
Explanation
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.

Figure 80a Figure 80b
Question 23
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 24
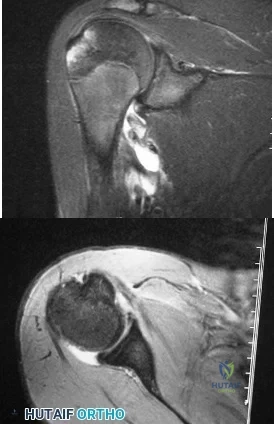
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 25
Clinical staging of osteomyelitis using the Cierney-Mader classification system takes into account which of the following factors?
Explanation
Question 26
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?
Explanation
REFERENCE: Bertoni F, Bacchini P: Classification of bone tumors. Eur J Radiol
1998;27:S74-S76.
Question 27
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 28
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
REFERENCES: Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
David TS, Drez DJ Jr: Electrothermally-assisted capsular shift. IEEE Eng Med Biol Mag 1998;17:102-104.
Question 29
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 30
A radiograph of a 27 month old child with bilateral genu valgum and internal tibial torsion shows the metaphyseal-diaphyseal angle of Levine and Drennen is 12 degrees on the right and 13 degrees on the left. Based on this finding, management should consist of
Explanation
Question 31
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion- extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior
surgery was not deemed a contraindication.
Question 32
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
Explanation
Question 33
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 34
What is the main function of collagen found within articular cartilage?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 35
Intermittent daily administration of recombinant parathyroid hormone (rhPTH) is an FDA-approved treatment for osteoporosis. Intermittent rhPTH treatment targets which of the following cells in osteoporotic patients?
Explanation
Question 36
Sciatic nerve
Explanation
The principal thrombogenic stimulus leading to the production of venous thromboembolic disease during total hip arthroplasty occurs at which time:
Question 37
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
REFERENCES: Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Sharrard J, Drennan JC: Osteotomy excision of the spine for lumbar kyphosis in older children with myelomeningocele. J Bone Joint Surg Br 1972;54:50-60.
Question 38
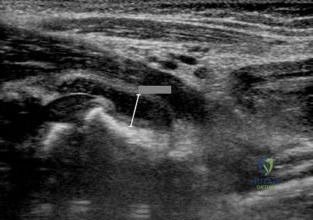
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 39
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 40
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 41
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
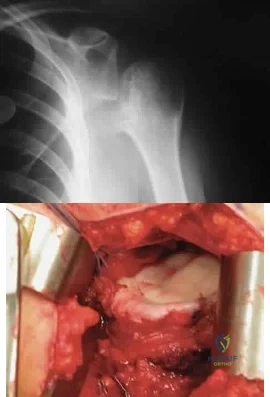
Explanation
Question 42
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 43
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 44
What structure is most at risk with anterior penetration of C1 lateral mass screws?
Explanation
REFERENCES: Currier BL, Todd LT, Maus TP, et al: Anatomic relationship of the internal carotid artery to the C1 vertebra: A case report of cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Spine 2003;28:E461-E467.
Grant JC: Grant’s Atlas of Anatomy, ed 6. Baltimore, MD, Williams & Wilkins, 1972.
Harms J, Melcher RP: Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine 2001;26:2467-2471.
Question 45
-A 3-year-old child with achondroplasia is hypotonic, and sleep studies reveal central apneic episodes. An initial workup should evaluate for what diagnosis?
Explanation
Borrelia titer
Calcium, phosporus, alkaline phosphatase, vitamin D
Human leukocyte antigen (HLA)-B27
Complete blood count, erythrocyte sedimentation rate, C-reactive protein
Rheumatoid factor
Antinuclear antibody
Uric acid
The laboratory studies listed above are needed to diagnose the disorders listed below. Match theappropriate laboratory studies with each of these disorders.
Question 46
A patient with a 5-cm synovial sarcoma located in the distal portion of the rectus femoris muscle undergoes excision of the mass. The procedure is performed through a 10-cm longitudinal incision. Only a portion of the rectus femoris is removed; the vast majority of the muscle is preserved. The plane of dissection is beyond the reactive zone, and the pathology reveals that the margins are negative. This procedure is classified as
Explanation
REFERENCES: Enneking WF: Staging of musculoskeletal neoplasms, in Current Concepts of Diagnosis and Treatment of Bone and Soft Tissue Tumors. Heidelberg, Germany, Springer-Verlag, 1984.
Simon MA, Springfield D: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998.
Question 47
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. The surgical approach for definitive reduction and stabilization of this pattern is

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 48
An 83-year-old woman with a long history of her foot slowly and progressively “turning out” now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
Question 49
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 50
A 16-year-old female gymnast reports a 2-month history of back pain since falling off the parallel bars, and she has been unable to return to gymnastics. She has no numbness or tingling. Examination reveals lower back tenderness, some paravertebral muscle spasm, range of motion of the lumbosacral spine is 20 degrees of flexion and 20 degrees of extension, and an equivocal straight leg raise. Lumbosacral spine radiographs demonstrate Schomorl’s nodes but no evidence of spondylolisthesis. What is the next best step in management?
Explanation
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
Question 51
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
REFERENCES: Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 115.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 119.
Question 52
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of
Explanation
REFERENCES: Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107.
Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Hove E, Sury B: Melorheostosis: Report on 5 cases with follow-up. Acta Orthop Scand 1971;42:315-319.
Question 53
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 54
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 55
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 56
Figures 113a and 113b are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step? Review Topic

Explanation
Question 57
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 58
A college athlete has a knee injury requiring surgery. He has acne, gynecomastia, and well-developed muscles related to the use of anabolic steroids. What association with steroid use is concerning for surgery and anesthesia? Review Topic
Explanation
Question 59
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
REFERENCES: Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Stambough JL, Davidson RS, Ellis RD, et al: Slipped capital femoral epiphysis: An analysis of 80 patients as to pin placement and number. J Pediatr Orthop 1986;6:265-273
Question 60
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 61
As a diaphyseal fracture heals, peripheral callus forms about the shaft axis, creating a structure with a substantially larger diameter than the original diaphyseal shaft. What biomechanical properties does this callus impart to the healing fracture site?
Explanation
The biomechanical role of the peripheral callus is to provide initial stability to the fracture and to act as a scaffold for gradual mineralization. Because the bending stiffness of a structure is proportional to the 4th power of the diameter, a peripherally located callus provides substantial stability to the fracture, despite the relatively low stiffness and strength of callus. For example, doubling the diameter of the callus increases the resistance to bending by a factor of 16. As mineralization progresses, the bending stiffness and strength of the healed fracture eventually may be substantially greater than that of the original, intact bone.
Augat et al. review the mechanical and biological aspects of fracture healing. They report that increased diameter of periosteal callus formation benefits healing by enlarging the cross-sectional area of area of the bridging tissue and reducing interfragmentary motion. Patients with osteoporosis are known to have decreased callus mineralization and biomechanical properties.
Incorrect Answers:
Question 62
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 63
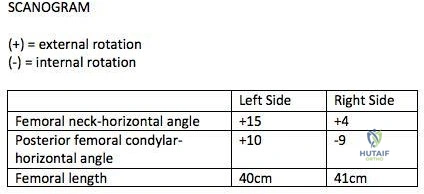
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 64
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin-resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was 21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 65
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 66
When counseling a patient with hypophosphatemic rickets, which of the following scenarios will always result in a child with the same disorder?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Greene WB, Kahler SG: Hypophosphatemic rickets: Still misdiagnosed and inadequately treated. South Med J 1985;78:1179-1184.
Question 67
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 68
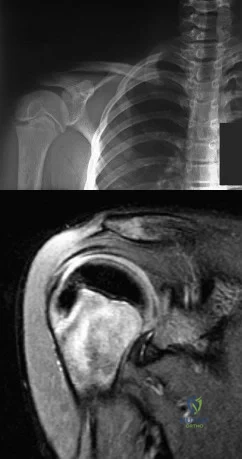
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder “slip out” when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?
Explanation
REFERENCES: Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Smith SP, Bunker TD: Primary glenoid dysplasia: A review of twelve patients. J Bone Joint Surg Br 2001;83:868-872.
Question 69
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 70
A favorable outcome following nonsurgical management of a partial tear of the posterior cruciate ligament (PCL) is best associated with
Explanation
REFERENCES: Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-38.
Griffin JR, Annunziata CC, Harner CD: Posterior cruciate ligament injuries in the adult, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2083-2106.
Question 71
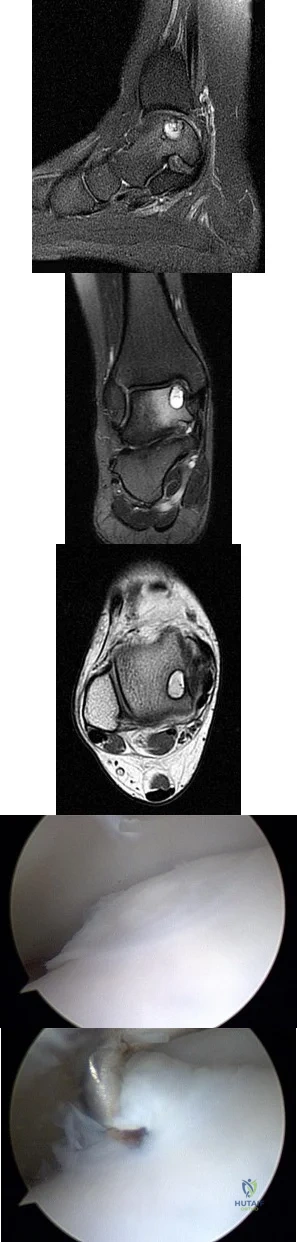
A B C D E Figures 45a through 45c are the MR images of a 22-year-old woman who has had 6 months of ankle pain related to activities of daily living. She recently completed a course of cast immobilization and protected weight bearing without symptom resolution. Figures 45d and 45e are the intraoperative arthroscopy images after minimal probing. What is the most appropriate treatment?
Explanation
The MR images reveal a large cystic medial talar dome osteochondral lesion (OCL) in a patient who has failed nonsurgical treatment. Ankle fusion is inappropriate because the patient has an otherwise normal ankle. Arthroscopic debridement and drilling are appropriate for smaller (< 1.5 cm sq) noncystic lesions. Retrograde drilling and bone grafting is an option in the treatment of cystic OCL if the cartilage surface is intact; however, intraoperative arthroscopy images show that this patient's cartilage surface is unstable. Osteochondral allografts and autografts are effective in the treatment of large cystic talar dome OCLs but are not appropriate for the initial surgical treatment of smaller lesions like this one.
RECOMMENDED READINGS
Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71. doi: 10.1302/0301-620X.96B2.31637. Review. PubMed PMID:
Question 72
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 28-29.
Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991,
pp 1255-1272.
Zancolli E: Reconstructive surgery in brachial plexus sequelae, in Gupta A, Kay S, Scheker L (eds): The Growing Hand. London, England, Mosby, 1999, p 807.
Question 73
Figure 71 is the MRI scan of a 2-year-old girl who has been febrile for 1 week and has refused to bear weight on her left lower extremity for 3 days. Her entire left lower extremity is markedly swollen. Doppler ultrasound shows a deep venous thrombosis of the internal iliac vein. Her white blood cell count is 19000/ µL (reference range, 4500-11000/ µL) and her C-reactive protein level is higher than 20 mg/L (reference range, 0.08-3.1 mg/L). If blood cultures yield positive results, what is the most likely organism? Review Topic

Explanation
Question 74
An year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 0 mg/L (reference range 08 to 1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly
difficult with activities of daily living and mobility.
Question 75
Figure below shows the abdominal radiograph obtained from a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 76
If the structure marked by the tip of the probe in Figure 94 is repaired to the bony glenoid with suture anchors during an arthroscopic stabilization procedure, what is the most likely result? Review Topic

Explanation
Question 77
Which of the following medications has been shown to improve skeletal muscle regeneration and decrease fibrosis following muscle injury in an animal model? Review Topic
Explanation
Skeletal muscle undergoes a natural process of healing and regeneration after injury. The formation of fibrous tissue in place of normal muscle is also part of this process. However, fibrous tissue in place of muscle can predispose the area to re-injury and impaired function. Administration of angiotensin II receptor blockade medications (e.g. losartan) after skeletal muscle injury has been shown to decrease the apoptotic cascade response and the formation of fibrous tissue. The mechanism of benefit is thought to be associated with blockade of insulin-like growth factor.
Terada et al. looked at the affect of platelet-rich plasma (PRP) and losartan on muscle healing after contusion injuries. They showed that PRP plus losartan combination
therapy improved overall skeletal muscle healing by enhancing angiogenesis and follistatin expression as well as reducing the expression of phosphorylated Smad2/3 and the development of fibrosis.
Bedair et al. used a rat model to investigate the effect of angiotensin receptor blockade on muscle fibrosis after injury. They found that angiotensin receptor blockade therapy significantly reduced fibrosis and led to an increase in the number of regenerating myofibers in acutely injured skeletal muscle.
Incorrect
Question 78
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures?

Explanation
Question 79
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 80
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 81
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include
Explanation
REFERENCES: Crossan JF, Wynne-Davies R, Fulford GE: Bilateral failure of the capital femoral epiphysis: Bilateral Perthes disease, multiple epiphyseal dysplasia, pseudoachondroplasia, and spondyloepiphyseal dysplasia congenita and tarda. J Pediatr Orthop 1983;3:297-301.
Sponseller PD: The skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 269-270.
Question 82
use of a true lateral to assess the DRUJ, 4) beginning early range of motion of the wrist after stable fixation and 5) use vitamin C to help mitigate intractable pain.
Explanation
A 26-year-old male sustains a fall from a ladder onto his outstretched right hand. He is evaluated in the emergency room and is found to have a closed injury to his elbow without evidence of neurovascular compromise. Plain radiographs are obtained and are shown in Figures A and B. During surgery a sequential approach is used to treat each element of this injury. Which part of the procedure is felt to add the most to rotatory stability?

Radial head replacement
Radial head ORIF
Capsular plication
Lateral collateral ligament complex repair or reconstruction
Medial collateral ligament complex reconstruction Corrent answer: 4
The essential lesion that results in the most instability in a terrible triad injury of the elbow is rupture of the lateral collateral ligament. Repair of this lesion
results in the greatest increase in elbow rotatory stability.
The key components of a terrible triad injury are a radial head fracture, coronoid fracture, dislocation of the ulnohumeral joint and disruption of the lateral collateral ligament complex. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
Forthman et al. reviewed 34 patients with an elbow dislocation, 22 of 34 of which were terrible triad injuries. Open reduction internal fixation or radial head replacement (as appropriate) along with LCL repair was completed; the MCL was not surgically addressed. Seventeen of 22 had good or excellent results, indicating that MCL repair is not necessary.
Pugh et al. discuss their surgical protocol for addressing terrible triad injuries with 28/36 of their patients obtaining good or excellent results. Their inside out protocol is described as follows: 1) coronoid fracture ORIF (capsular repair), 2) radial head fracture ORIF or replacement 3) LCL complex repair (isometric point is center of capitellum), 4) reevaluation of stability; MCL repair or hinged fixator application
Jensen et.al in cadaveric studies have demonstrated that radial head replacement alone decreases varus laxity and external rotatory laxity to 14.6 &
Question 83
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 84
Which of the following can be seen in the heart of a well-conditioned athlete? Review Topic
Explanation
Question 85
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function? Review Topic

Explanation
Question 86
- An MRI scan of the brain of a patient with spastic diplegia will most likely show
Explanation
Agnesis of the corpus callosum is a rare anomaly that is asymptomatic neurologically unless tests designed specifically to test the transfer of information from one cerebral hemisphere to another is employed. Additionally, the corpus callosum is intimately related to the development of the limbic system which governs major CNS roles as behavior, memory, and emotions. Therefore, this would not involve the neurologically challenged spastic diplegic individuals.
Question 87
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 88
An elderly woman with osteoporosis falls from a standing height, sustaining a low-energy fracture of the acetabulum. What structures are most likely fractured?
Explanation
may present as atypical fracture patterns not always conforming to classic injury patterns described by Judet and associates. This fracture pattern seen commonly in geriatric patients results from low-energy falls with force directly applied to the greater trochanter. Fractures involving the posterior column and/or wall and transverse fracture patterns involving both the anterior and posterior columns occur infrequently in this age group. They are, however, more commonly encountered in younger age groups as a result of higher energy trauma.
Question 89
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
REFERENCES: O’Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: “Dancer’s Fracture.” Am J Sports Med 1996;24:240-243.
DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Hamilton WG: Foot and ankle injuries in dancers, in Yokum L (ed): Sports Clinics of North America. Philadelphia, PA, Williams and Wilkins, 1988.
Question 90
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 14-15.
Question 91
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?
Explanation
and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular
angle. Correction of both of these abnormalities requires a proximal and distal first
metatarsal osteotomy.
REFERENCES: Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Peterson HA, Newman SR: Adolescent bunion treated with double osteotomy and longitudinal pin fixation of the first ray. J Pediatr Orthop 1993;13:80-84.
Question 92
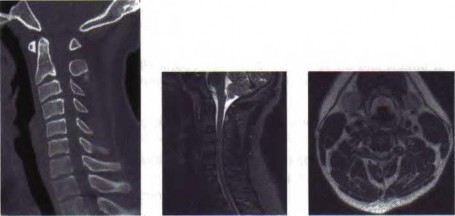
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Johnson T, Steinbach L (eds): Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 44.
Question 93
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
REFERENCES: Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
Guskiewicz KM, McCrea, Marshall SW, et al: Cumulative effects associated with recurrent concussion in collegiate football players: The NCAA Concussion Study. JAMA
2003;290:2549-2555.
Question 94
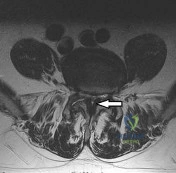
Figure 93 shows the axial T2-weighted MRI scan of the lumbar spine of a 70-year-old man. The arrow points to which of the following structures? Review Topic
Explanation
(SBQ12SP.14) A 36-year-old male presents with acute onset of right buttock and leg pain following lifting a heavy object. On physical exam he has weakness to knee extension, numbness over the medial malleolus, and a decreased patellar reflex. Which of the following would most likely explain this clinical presentation. Review Topic
Lumbar arachnoiditis
L4/L5 paracentral disc herniation
L3/L4 far lateral (foraminal) disc herniation
L4/L5 far lateral (foraminal) disc herniation
L5/S1 far lateral (foraminal) disc herniation
The clinical presentation is consistent with a L4 radiculopathy. A L4/L5 far lateral (foraminal) disc herniation would compress the exiting root (L4) and cause these symptoms.
The location of a prolapsed lumbar disc determines its symptoms. Central disc herniations may give rise to back pain or cauda equina syndrome. Paracentral disc herniations (90-95% of cases) affect the traversing nerve root. Far lateral disc herniations (5-10%) affect the exiting nerve root.
Gregory et al. summarize physical signs in lumbar disc herniation. They state that the straight-leg-raise is the most sensitive (73-98% sensitive) test and the crossed straight-leg-raise is the most specific (88-98% specific) test for lumbar disc herniation. Other specific tests include weak ankle dorsiflexion (89% specific), absent ankle reflex (89% specific), and calf wasting (94% specific, but a late finding).
Illustration A shows how a paracentral L4/L5 disc herniation affects the traversing L5 root, but a far lateral L4/L5 disc herniation affects the L4 root. Illustration B shows the dermatomal distribution of pain with root involvement from L3 to S1.
Incorrect Answers:
Question 95
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 96
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 97
Which structure is indicated by the arrow in Figure 33?

Explanation
The posterior position of the sciatic nerve in relation to the acetabulum and the lateral peroneal division makes the peroneal division of the sciatic nerve the portion of the nerve that is most likely to be injured in a posterior traumatic hip dislocation, accounting for up to 10% of concomitant nerve injuries with posterior hip dislocation. The corona mortis is an anatomic variant that results in vascular anastomosis between the obturator and either the external iliac or inferior epigastric arteries. This variant occurs in approximately 80% of patients and varies in its position, being located 4 cm to 9 cm lateral to the symphysis pubis. The obturator vascular bundle is situated in the fat medial to the obturator internus muscle and must be mobilized to access the quadrilateral plate. Dissection may be carried out both above and below this vascular leash. The Kocher-Langenbeck approach is indicated for fractures involving the posterior wall and/or posterior column of the acetabulum and for both column fractures that require direct posterior visualization. This approach is not indicated for direct reduction of the anterior wall or column when direct visualization is required anteriorly. The L5 nerve root is located on the anterior sacrum and is indicated by the arrow.
The position of this neural structure must be considered whether the surgeon is stabilizing 31 the sacroiliac (SI) joint with percutaneous iliosacral screws or with anterior SI plating through the lateral window of the ilioinguinal approach.
RECOMMENDED READINGS
Cornwall R, Radomisli TE. Nerve injury in traumatic dislocation of the hip. Clin Orthop Relat Res. 2000 Aug;(377):84-91. Review. PubMed PMID: 10943188. View Abstract at PubMed
Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007 May;20(4):433-9. PubMed PMID: 16944498. View Abstract at PubMed
Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. View Abstract at PubMed
Rommens P. The Kocher-Langenbeck approach for the treatment of acetabular fractures. Operat Orthop Traumatol 2004; 16:59-74.
Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management. J Am Acad Orthop Surg. 2013 Aug;21(8):458-68. doi: 10.5435/JAAOS-21-08-458. Review. PubMed PMID: 23908252.View Abstract at PubMed
Question 98
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the patient's symptoms? Review Topic
Explanation
Question 99
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 100
Figure 48a shows the full-leg standing radiograph of a patient with a prior femoral fracture. Figure 48b shows the lateral view of the same joint. The patient is scheduled to undergo total knee arthroplasty. Because the mechanical axis of the lower extremity in patients with a prior femoral fracture may be disrupted, which of the following should be used during surgery to restore the mechanical axis of the lower extremity in this patient?
Explanation
(3 degrees valgus), and the deformity at the healed fracture site (14 degrees) does not appear to affect the joint alignment and is acceptable. Use of a routine knee prosthesis will be possible in this patient. To avoid hardware removal, extramedullary jigs and/or computerized navigation may be used to measure and restore the long axis of the femur. The use of a hinged prosthesis does not influence the mechanical axis directly. Extra-articular osteotomy is occasionally needed to reverse severe deformities.
REFERENCES: Papadopoulos EC, Parvizi J, Lai CH, et al: Total knee arthroplasty following distal femoral fractures. Knee 2002;9:267-274.
Lonner JH, Siliski JM, Lotke PA: Simultaneous femoral osteotomy and total knee arthroplasty for treatment of osteoarthritis associated with severe extra-articular deformity. J Bone Joint Surg Am 2000;82:342-348.
