Orthopedic Board Review MCQs: Ankle, Foot, Hip & Knee | Part 139

Key Takeaway
This page offers Part 139 of a comprehensive orthopedic surgery board review. Featuring 100 high-yield MCQs, it's designed for orthopedic surgeons and residents preparing for AAOS, ABOS, and OITE exams. Utilize interactive study and exam modes with detailed explanations to master key topics and ensure certification success.
About This Board Review Set
This is Part 139 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 139
This module focuses heavily on: Ankle, Foot, Hip, Knee.
Sample Questions from This Set
Sample Question 1: A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?...
Sample Question 2: Failure of posterolateral corner repair or reconstruction of the knee may be associated with which of the following? Review Topic...
Sample Question 3: A study is being designed to compare the effectiveness of an antibiotic. The choice of the number of patients (ie, the sample size) depends on several factors. What type of calculation assesses the potential of the study to successfully add...
Sample Question 4: A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?...
Sample Question 5: Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history ofprogressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examinatio...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Explanation
Question 2
Failure of posterolateral corner repair or reconstruction of the knee may be associated with which of the following? Review Topic
Explanation
Question 3
A study is being designed to compare the effectiveness of an antibiotic. The choice of the number of patients (ie, the sample size) depends on several factors. What type of calculation assesses the potential of the study to successfully address the effectiveness of the antibiotic?
Explanation
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 4
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
REFERENCES: Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 5
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 6
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 7
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?
Explanation

Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
Question 8
A 65-year-old woman with rheumatoid arthritis is involved in a motor vehicle accident. Her injuries include a right displaced femoral neck fracture, a left open tibial pilon fracture, a left open tibial plateau fracture, multiple rib fractures, and bilateral pulmonary contusions. Her vitals signs on admission are a heart rate of 115 bpm and a systolic blood pressure of 90 mm Hg. Laboratory studies show a hemoglobin of 10.0 g/dL and a delta base of -6.0 mmol/L. What finding in this patient is most significantly associated with increased mortality? Review Topic
Explanation
Question 9
During stabilization of a slipped capital femoral epiphysis, the screw penetrates into the joint. The screw is repositioned so that it is within the femoral head. This transient penetration of the hip joint will most likely lead to
Explanation
REFERENCES: Zionts LE, Simonian PT, Harvey JP Jr: Transient penetration of the hip joint during in situ cannulated-screw fixation of slipped capital femoral epiphysis. J Bone Joint Surg Am 1991;73:1054-1060.
Vrettos BC, Hoffman EB: Chondrolysis in slipped upper femoral epiphysis: Long-term study of the etiology and natural history. J Bone Joint Surg Br 1993;75:956-961.
Question 10
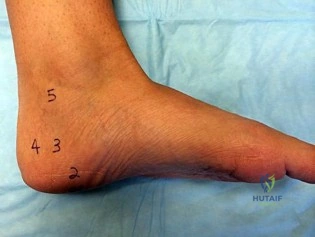
A B Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?

Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. View Abstract at PubMed
Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. View Abstract at PubMed Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87

Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 11
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, chapter 2.
Flynn TB: Neurologic complication of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 12
What is the most common benign bone tumor in childhood?
Explanation
REFERENCES: Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 13
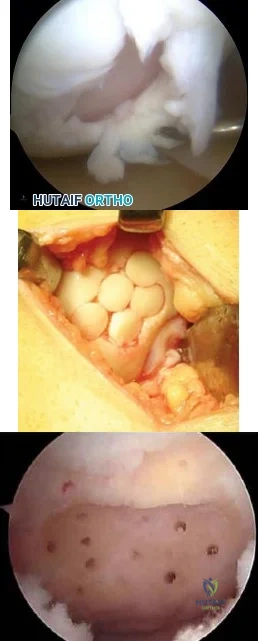
A 35-year-old man presents with mechanical knee pain after a fall. An arthroscopic picture taken during diagnostic arthroscopy is shown in Figure A. His surgeon considers treatment with Technique B and Technique C, which are shown in Figures B and C, respectively. Which of the following statement is true with respect to Technique B and C? Review Topic
Explanation
The initial treatment for small articular cartilage defects is rest, NSAIDS and bracing. For larger defects (<2-4cm2), options include marrow stimulation procedures (abrasion chondroplasty, microfracture, osteochondral drilling) and autograft procedures (Mosaicplasty, a technique of osteochondral autograft transfer (OAT).
Alford et al. reviewed cartilage restoration. They defined a spectrum of treatment option ranging from (1) palliative (debridement/lavage), intended to reduce irritation
and inflammation, (2) reparative (marrow stimulation techniques), intended to recruit stem cells to proliferate fibrocartilage repair tissue, to (3) restorative (osteochondral grafting), designed to replace articular cartilage and subchondral bone as a single unit.
Magnussen et al. reviewed the treatment of cartilage defects in the knee. They compared autologous chondrocyte implantation (ACI), OATs, matrix-induced ACI, and microfracture. No one technique was superior to the rest. Outcomes for microfracture tended to be worse in larger lesions.
Figures A is an arthroscopic picture showing a grade IV chondral defect. Figure B shows microfracture. Figure C shows the multiple cylindrical plugs of mosaicplasty, a technique of osteochondral autograft transfer (OAT). Illustration A shows donor and recipient sites in mosaicplasty. Illustration B shows the spectrum of treatment options defined by Alford et al (MST = marrow stimulation; ACI = autologous chondrocyte implantation; OCG = osteochondral grafting with autograft/allograft).
Incorrect Answers:
Question 14
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 15
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 16
A B C Figures 64a through 64c are the MR images and radiograph of an active 30-year-old man who has been treated for pain in his subtalar joint for 6 months. He has had casting, physical therapy, and bracing but continues to have activity-limiting pain. An injection into the subtalar joint under fluoroscopic guidance temporarily relieved his pain. His best surgical option at this time is

Explanation
When contemplating the causes of subtalar joint degeneration in young patients, an unstable tarsal coalition should be considered in the absence of antecedent trauma. Initial treatment with casting is appropriate because this intervention can relieve symptoms for many patients. There are 2 surgical options for a symptomatic tarsal coalition: bar resection or completion fusion. Risk factors for a poor outcome after bar resection are adult age and a bar that encompasses more than 50% of the middle facet of the subtalar joint. Because this patient has both risk factors, the appropriate procedure is a subtalar fusion.
RECOMMENDED READINGS
Comfort TK, Johnson LO. Resection for symptomatic talocalcaneal coalition. J PediatrOrthop. 1998 May-Jun;18(3):283-8. PubMed PMID: 9600549. View Abstract at PubMed
Thorpe SW, Wukich DK. Tarsal coalitions in the adult population: does treatment differ from the adolescent? Foot Ankle Clin. 2012 Jun;17(2):195-204. doi: 10.1016/j.fcl.2012.03.004. Epub 2012 Apr 6. Review. PubMed PMID: 22541520. View Abstract at PubMed
Question 17
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 18
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic

Explanation
Question 19
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic
Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 20
A 73-year-old man presents to your clinic many years after undergoing total shoulder arthroplasty with pain and the radiographic findings demonstrated in Figure 56. The most likely cause of this patient’s pain is

Explanation
The radiograph shows proximal humeral migration and loosening of the glenoid component. Proximal migration of the humeral head may represent rotator cuff dysfunction and can lead to progressive failure of the glenoid component. Stress shielding will not cause lysis or loosening of the glenoid component. Humeral osteolysis is an uncommon finding and is not shown. Progressive glenoid arthrosis is not possible with a resurfaced glenoid.
RECOMMENDED READINGS
Hill JM, Norris TR. Long-term results of total shoulder arthroplasty following bone-grafting of the glenoid. J Bone Joint Surg Am. 2001 Jun;83-A(6):877-83. PubMed PMID: 11407796.View Abstract at PubMed
Fox TJ, Cil A, Sperling JW, Sanchez-Sotelo J, Schleck CD, Cofield RH. Survival of the glenoid component in shoulder arthroplasty. J Shoulder Elbow Surg. 2009 Nov-Dec;18(6):859-63. doi: 10.1016/j.jse.2008.11.020. Epub 2009 Mar 17. PubMed
PMID: 19297199.View Abstract at PubMed
Question 21
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
specific to this pathology.
Question 22
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
REFERENCES: Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84.
Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Ganz R, Krushell RJ, Jacob RP, Kuffer J: The antishock pelvic clamp. Clin Orthop 1991;267:71-78.
Question 23
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
REFERENCE: Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 24
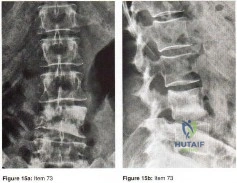
Figures 15a and 15b show the AP and lateral radiographs of the lumbar spine of a 51 year old woman who has had back pain that radiates into the right thigh for the past 3 months. Her medical history is unremarkable except for a mastectomy for breast cancer 12 years ago. What is the most likely diagnosis?
Explanation
Question 25
Figures 80a and 80b are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test result, trace effusion, and range of motion from 0 to 85 degrees of knee flexion. Which factor is most contributory to his examination findings?
Explanation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
CLINICAL SITUATION FOR QUESTIONS 81 THROUGH 84
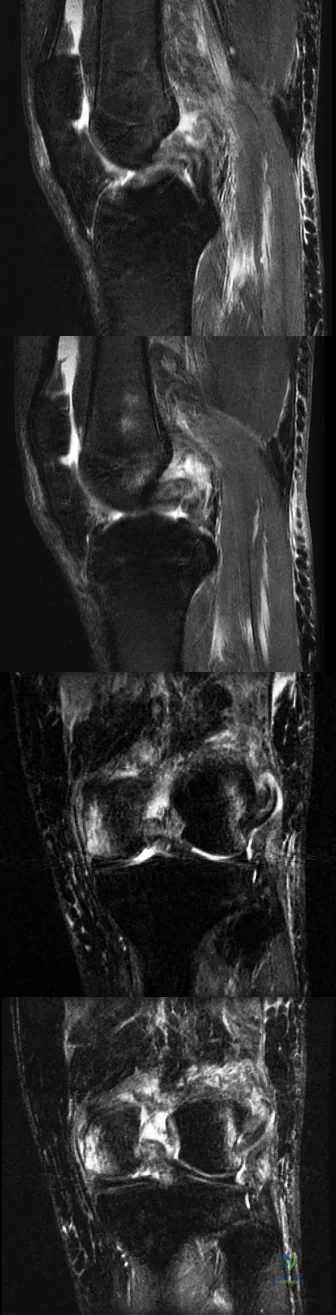
Figures 81a through 81d are the MR images of a 25-year-old man with left knee pain after a motorcycle collision. He has palpable pedal pulses with an ankle-brachial index of 0.95. Neurologic examination findings of the injured extremity are normal.
Question 26
Anterior perforation of the distal femur from antegrade femoral nailing has been attributed to what factor?

Explanation
The radius of curvature is generally smaller (114-120 cm) than many earlier generation femoral nails (up to 300 cm), and the referenced article by Ostrum et al describes a case series of 3 such patients with subtrochanteric fractures. He noted that the difference in femoral anteroposterior bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Illustration A shows an example of a nail penetrating the anterior femoral cortex.
Question 27
Which of the following is most important to acheive a good outcome following a Syme amputation?

Explanation
Question 28
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
Explanation
REFERENCES: Fritz GR, Stern PJ, Dickey M: Complications following mucous cyst excision. J Hand Surg Br 1997;22:222-225.
Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 29
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
REFERENCES: Werner A, Mueller T, Boehm D, et al: The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval: A histoanatomic study. Am J Sports Med 2000;28:28-31.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 165-189.
Question 30
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing’s sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 31
Figures 7a through 7d are the images of a 31-year-old obese woman who has a long history of low-back pain and intermittent bilateral lower extremity pain. Five days ago her symptoms increased markedly and she was given pain medications upon presentation to her primary care physician. Three days ago she noticed that her bed was wet upon awakening; she also had numbness and tingling in her peroneal area and lower extremities and weakness in her lower extremities. She is brought to your office in a wheelchair. Her examination reveals diminished sensation to light touch in the L4 to S4 dermatomes and 0-1/5 strength in all muscle groups in her bilateral lower extremities with the exception of her hip flexors, hip adductors, and quadriceps, which are 5/5 in strength. She has decreased sphincter tone on rectal examination. You recommend immediate decompressive laminectomy. What is the likelihood she will regain bladder function after surgery? A B C D

Explanation
This patient has congenital and acquired spinal stenosis with multilevel disk protrusions that have both chronic (calcified) and acute components, resulting is multilevel cauda equina compression and acute cauda equina syndrome of more than 48 hours duration. Most studies indicate that patients who undergo decompression within 48 hours of symptom onset have a better prognosis for neurologic recovery than those who undergo decompression after 48 hours. Among patients with urinary incontinence, 1 study indicated that 43% remained incontinent at follow-up visits, but this study included a mix of early and late surgical patients. In another series of 44 patients with acute cauda equina syndrome, chronic bowel and bladder dysfunction were issues for 63% of those for whom surgery was delayed for more than 48 hours after symptom onset.
RECOMMENDED READINGS
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 32
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 33
Examination of a 9-year-old boy reveals a right thoracic prominence on forward flexion. Neurologic examination is normal, and no other abnormalities are noted. AP radiographs reveal a 30-degree right thoracic curve. Initial management should consist of
Explanation
REFERENCES: Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 685-705
Nohria V, Oakes WJ: Chiari I malformation: A review of 43 patients. Pediatr Neurosurg 1990-91;16:222-227.
Goldberg CJ, Moore DP, Fogarty EE, Dowling FE: Left thoracic curve patterns and their association with disease. Spine 1999;24:1228-1233.
Question 34
- Analysis of which of the following proteins is used to establish the diagnosis of Becker muscular dystrophy?
Explanation
A 25-year-old woman with spastic diplegia has a painful progressive bunion deformity that has failed to respond to nonsurgical treatment. Examination reveals tenderness and erythema over the bunion prominence; however, the hallux metatarsophalangeal joint has full range of motion. A standing AP radiograph shows a hallux valgus angle of 30 degrees and a 1-2 intermetatarsal angle of 13 degrees. Treatment should now consist of
arthrodesis of the hallux metatarsophalangeal joint.
arthrodesis of the first tarsometatarsal joint.
excision of the medial eminence and medial capsular reefing of the metatarsophalangeal joint.
osteotomy of the distal first metatarsal.
proximal metatarsal osteotomy with distal soft-tissue realignment.
Treatment of hallux valgus in a patient with cerebral palsy is largely dependent on the degree of spasticity and the pattern of gait. The only way to adequately eliminate spastic deforming forces is with an arthrodesis of the MTP joint. Any other procedure will most likely lead to a high incidence of either hallux varus or recurrent hallux valgus.
The optimal arthrodesis angle is 25-30 degrees, and the metatarsal inclination angle should be 25-30 degrees also. Sagittal plane position should be checked intraoperatively and the proximal phalanx should clear the table by 5-10mm with simulated WB
Question 35
A 45-year-old male auto mechanic presents to your office with left lateral elbow pain for 6 weeks. On physical exam he has tenderness to palpation over the lateral epicondyle and pain with resisted wrist extension. An MRI is shown in figures A and B. After failing non-surgical treatment modalities, he undergoes arthroscopic surgical management. At 3 months post-operatively, the patient reports persistent left elbow pain and an audible clicking since surgery which occurs when he lifts heavy objects and when he pushes himself up out of a chair. What is the best surgical treatment option? Review Topic
Explanation
PLRI is the result of an incompetent lateral ulnar collateral ligament (LUCL), a component of the elbow lateral collateral ligament complex. The LUCL originates on the lateral epicondyle of the humerus and inserts upon the supinator crest of the ulna. When deficient from acute trauma or from repetitive microtrauma, the elbow becomes rotationally unstable with elbow extension, supination, and an applied valgus force. In this case, the patient has had iatrogenic damage to the LUCL from an arthroscopic release of the extensor carpi radialis brevis (ECRB) for treatment of lateral epicondylitis. This patient exhibits an important manifestation of this: a positive chair pushup test. This test is positive when pushing off of a chair with a supinated forearm causes pain and instability. Due to the chronicity of the injury (3 months) and his persistent symptoms of instability (pain and clicking) the patient would benefit from surgical reconstruction of the damaged LUCL using either palmaris longus or gracilis allograft.
Kelly et. al. reviewed the known major and minor complications of elbow arthroscopy among 473 consecutive cases at their institution from 1980-1998. The most common complications were transient nerve palsies in 10 patients. Among them, the major
nerves involved included the anterior interosseous nerve, posterior interosseous nerve, ulnar nerve, superficial radial nerve, and medial antebrachial cutaneous nerve. The risk of iatrogenic nerve injury was increased among patients with rheumatoid arthritis. The most frequent complication was prolonged drainage from the portal sites.
Calfee et. al. reviewed the management of lateral epicondylitis. The authors suggest open or arthroscopic surgical debridement of the common extensor origin after failure of rest, orthoses, nonsteroidal drugs, physical therapy, cortisone and platelet-rich plasma injections. They do acknowledge that excessive debridement may compromise lateral elbow stability and cause PLRI.
O'Brien et. al. described the surgical techniques for managing PLRI, including an open technique for chronic injuries or revision treatment. In this setting, the authors suggest use of palmaris or gracilis allograft for reconstruction.
Figures A and B are an axial and coronal T2 weighted MRI of an elbow demonstrating signal intensity in the origin of the ECRB, consistent with lateral epicondylitis.
Incorrect Answers:
Question 36
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
REFERENCES: Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 37
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
Explanation
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. View Abstract at PubMed
Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. View Abstract at PubMed
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.View Abstract at PubMed
Question 38
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 39
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 40
1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
Explanation
failure, hyperhomocystinemia, diseases that alter blood viscosity (eg, polycythemia, sickle cell disease, multiple myeloma), and inherited thrombophilias. In addition to the risk associated with embolization of PMMA, the patient has been immobile for 7 days and was ultimately diagnosed with multiple myeloma.
Which key factor that induces osteoclastogenesis is secreted by osteoblasts in response to inflammatory stimuli?
Osteoprotegerin (OPG)
Tumor necrosis factor (TNF)
Insulin growth factor-1 (IGF)
Bone morphogenetic protein (BMP)
Receptor activator of nuclear factor kappa-B ligand (RANKL) Corrent answer: 5
Osteoclasts are derived from cells of the monocyte/macrophage lineage. They are multinucleated and develop by fusion of mononuclear precursors, a process that requires receptor activator for nuclear factor kappa-B ligand (RANKL) and macrophage-colony stimulating factor (M-CSF). RANKL is secreted by osteoblasts in response to inflammatory signals and is a key component of inflammation-mediated osteolysis. OPG binds to and sequesters RANKL, thus inhibiting osteoclast differentiation and activity.
BMP and IGF-1 are potent regulators of osteoblast differentiation and activation. TNF is a cytokine secreted by macrophages and degranulating platelets infiltrated in the fracture site and impacts a variety of cells, not osteoclasts.
A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have preferences for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?
I
II
III
IV
V
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
The fracture seen in Figures A and B is most likely to occur in which of the following growth plate zones?
Resting zone
Proliferative zone
Zone of maturation
Zone of degeneration
Zone of provisional calcification
Physeal fractures typically occur through the zone of provisional calcification. Answers 3-5 are all part of the hypertrophic zone which is labeled "D" on the histologic illustration A. Illustration B shows the relationship of the physeal zones to the epiphysis and metaphysis of a growing bone. However, the stress concentration is greatest in the sub-layer where there is a transition from the soft cartilagenous physis to the harder calcific metaphysis.
As discussed in the review by Ballock and O'Keefe, the growth plate is a remarkable portion of the skeleton that requires precise coordination between multiple endocrine, paracrine, and autocrine signaling systems. While fractures can occur in any portion of the growth plate, the zone of provisional calcification is the most common.
Since the adoption by the American Academy of Orthopaedic Surgeons in 1997 of the presurgical protocol in which the surgeon signs the surgical site and the mandate for this protocol by the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO)
in 2003, the total number of wrong-site surgeries reported per year in the United States has
increased.
decreased.
decreased for orthopaedic surgery but stayed the same for other surgeries.
remained the same.
only improved for hospital-based surgery.
Despite the initiatives by the American Academy of Orthopaedic Surgeons and the
JCAHO, the number of reported cases of wrong-site surgery has continued to increase yearly since 1997. Because reporting of these events is not mandated by JCAHO, it is possible that the continued increase is due to a greater awareness of the problem and thereby a greater level of reporting. The U.S. estimates are 12.7 wrong-site surgeries per million cases performed. Orthopaedic surgery and podiatry are the most common specialties associated with wrong-site surgery (41%) followed by general surgery (21%), neurosurgery (14%), and urologic surgery (11%).
The use of evidence-based studies among professions associated with health care, including purchasing and management, is known as
decision analysis.
cost-utility analysis.
cost-benefit analysis.
cost-effectiveness analysis.
evidence-based health care.
Evidence-based health care extends the application of the principles of evidence-based medicine to all professions associated with health care. This concept is becoming more important because data will be used by the different parties for their decision making (policy makers, health insurances, hospitals, doctors, and the public). Cost-benefit analysis refers to the conversion of effects into the same monetary terms as the costs and compares them. Cost- effectiveness analysis refers to the conversion of effects into health terms and describes the costs for some additional health gain (eg, cost per additional event prevented). Cost-utility analysis refers to the conversion of effects into personal preferences (or utilities) and describes how much it costs for some additional quality gain (eg, cost per additional quality-adjusted life-year).
Decision analysis refers to the application of explicit, quantitative methods to analyze decisions under conditions of uncertainty.
All of the following medications have been associated with an increased risk of osteoporosis EXCEPT:
Selective serotonin reuptake inhibitors (SSRI)
Glucocorticoids
Non-steroidal anti-inflammatories (NSAIDs)
Phenytoin
Protease inhibitors
Numerous drugs are associated with an increased risk of osteoporosis in
adults, including oral corticosteroids, androgen-deprivation therapy, aromatase inhibitors, protease inhibitors, selective serotonin reuptake inhibitors,
prolactin-raising antiepileptic agents and many cytotoxic agents.
Additionally, a number of disease states are associated with osteoporosis, including endocrinopathies such as hyperparathyroidism, thyrotoxicosis and type I diabetes, hypogonadism, chronic glucocorticoid therapy, malnutrition, malabsorption states, chronic immobilization, rheumatoid arthritis, alcoholism, vitamin D deficiency, and multiple myeloma.
NSAIDs have not been shown to increase risk of osteoporosis.
A 65-year-old woman with rheumatoid arthritis is unable to actively extend her index, middle, ring, and little fingers secondary to tendon rupture. In performing a flexor digitorum sublimis (FDS) of the middle/ring finger to extensor digitorum communis (EDC) transfer to restore active metacarpophalangeal (MCP) joint extension, the FDS should be passed
ulnarly, around the ulna in a dorsal direction.
radially, around the radius in a dorsal direction.
through the interosseous membrane.
through the intermetacarpal spaces between the index, middle, ring, and little fingers.
through the lumbrical canals of the index, middle, ring, and little fingers. Corrent answer: 2
Although the early use of FDS as a transfer to restore finger extension in patients with radial nerve palsy was performed by passing the tendon through the interosseous membrane, Nalebuff and Patel later modified this procedure for the rheumatoid arthritis patient by passing the FDS radially, around the radius in a dorsal direction. They felt that this provided a number of advantages, including: 1. technical ease, 2. avoidance of synovial disease on the dorsum of the wrist, and 3. correction of ulnar deviation of the fingers through the line of pull from the radial side of the forearm.
Based on the clinical photograph, radiographs, and biopsy specimen shown in Figures 68a through 68d, what is the most likely diagnosis?
Calcium pyrophosphate deposition disease
Bacterial infection
Fungal infection
Gout
Giant cell tumor
The patient has gout. Unfortunately, gout may mimic several conditions affecting the small joints of the hand, including infection. The histologic specimen shows negatively birefringent intracellular rods consistent with gout. The histology rules out giant cell tumor and calcium pyrophosphate deposition disease.
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Continued observation and monitoring
Obtain arterial blood gas measurements
Obtain emergent spiral CT scan to assess for pulmonary embolism
Insertion of a chest tube
Airway control and, if necessary, endotracheal intubation
Because the phrenic nerve lies in close proximity to the site of anesthetic injection, temporary hemidiaphragmatic paresis is a very common side effect of interscalene brachial plexus block. Pulmonary function and chest wall mechanics may be slightly compromised, but can easily be compensated in a healthy patient. Therefore, with
sufficient oxygenation, aggressive assessments or treatments such as arterial blood gas measurements,
emergent spiral CT scans, chest tube insertions, or endotracheal intubation are not warranted. For this stable patient, continued monitoring with gradual withdrawal of oxygen is the most appropriate treatment.
A 67-year-old woman with rheumatoid arthritis has had a 3-year history of gradually progressive right elbow pain and limited function despite intra-articular injections and medical management. She previously underwent a rheumatoid hand reconstruction, and has no pain or dysfunction of the ipsilateral shoulder.
Radiographs are shown in Figures 93a and 93b. What is the most appropriate treatment?
Soft-tissue interposition arthroplasty with radial head resection
Arthroscopic synovectomy with radial head resection
Elbow arthrodesis
Total elbow arthroplasty
Resection arthroplasty
Total elbow arthroplasty is the treatment of choice. The patient has end-stage rheumatoid involvement of the ulnohumeral and radiocapitellar joints. Given the advanced nature of the disease and evidence of bony erosion, arthroscopic
synovectomy and interposition arthroplasty are unlikely to provide lasting benefit or functional improvement. Elbow arthrodesis and resection arthroplasty are considered salvage techniques and are generally not considered as a primary treatment method.
A 66-year-old woman with known poorly controlled rheumatoid arthritis reports that for the past 4 weeks she has been unable to extend the metacarpophalangeal (MCP) joints of her right hand index, middle, ring and little fingers. She cannot hyperextend the thumb interphalangeal joint. Active wrist extension is possible, but shows radial deviation. Examination reveals mild synovitis at the wrist and MCP joints of the affected hand. There is no ulnar deviation at the MCP joints with normal alignment. When the MCP joints are passively extended, the patient is unable to maintain them in this position.
There is no piano key sign at the distal ulna. Passive wrist motion shows a normal tenodesis effect. Which of the following would most likely confirm your diagnosis?
Radiographs of the hand
Radiographs of the cervical spine
Electrodiagnostic studies of the affected upper extremity
Surgical exploration of the extensor tendon ruptures
MRI of the elbow
There are many causes of inability to extend the MCP joints in a patient with rheumatoid arthritis. The most common cause is rupture of the extensor tendons. An intact tenodesis test suggests that the extensor tendons are intact, thus surgical exploration is not indicated and would not confirm the diagnosis. The patient has normal alignment of the fingers without ulnar deviation, suggesting that there are no MCP dislocations to account for the inability to extend the MCP joints; therefore, radiographs would not confirm the diagnosis. The most likely cause of inability to extend the fingers in this patient is posterior interosseous nerve (PIN) palsy. Electrodiagnostic studies would confirm the presence of PIN palsy. An MRI of the elbow may show synovitis at the radiocapitellar joint, which can cause the PIN palsy. This finding however, is nonspecific and many patients without PIN palsy would also demonstrate synovitis at the radiocapitellar joint.
Therefore, although an MRI would be helpful in localizing a potential cause of PIN compression, it would not in itself confirm the diagnosis.
What is the predominant type of collagen found in the nucleus pulposus of the intervertebral disk?
Type I
Type II
Type V
Type VI
Type XII Corrent answer: 2
Types I and II collagen are the predominant types of collagen found in the intervertebral disk. Type I collagen is present in the highest concentration in the annulus fibrosus and type II collagen in the nucleus pulposus. Type V collagen is present in small concentration in the annulus fibrosus. Type VI collagen is a non-fibrillar, short-helix collagen found in both the annulus and nucleus. Type XII is present in the annulus fibrosus only.
What complication is associated with the use of epidural morphine and steroid paste after laminectomy?
Surgical site infection
Arachnoiditis
Urinary retention
Disk space infections
Nerve irritation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. There is no evidence in the literature verifying the incidence of postoperative urinary retention and arachnoiditis.
Which of the following materials has the highest modulus of elasticity?
Cortical bone
Cobalt-chrome
Ceramic
Titanium
Stainless steel
Young's modulus of elasticity is a measure of the stiffness of a material and its ability to resist deformation. This is the slope of the stress/strain curve in the elastic range. The highest modulus is ceramic, followed by: cobalt-chrome alloy, stainless steel, titanium, and then cortical bone.
What medication has been shown to decrease osteolysis after total joint replacement surgery?
Bisphosphonates
NSAIDs
TNF-alpha inhibitors
Calcium and vitamin D supplementation
BMP-7
Bisphosphonates have been shown to decrease osteolysis after total joint replacement surgery.
Aseptic loosening and osteolysis are the primary causes of implant failure in total joint arthroplasty. Early findings indicate that bisphosphonates upregulate bone morphogenetic protein-2 production and stimulate new bone formation, leading to decreased osteolysis in total joint replacement surgery. While
further investigation is required, bisphosphonates may play a future role in improving the long-term duration of joint arthroplasties.
Shanabhag et al. reviewed the use of bisphosphonates and reported that they had the potential to enhance bone ingrowth into implant porosities, prevent bone resorption under adverse conditions, and dramatically extend the long- term durability of joint arthroplasties. They recommended further investigation into the subclasses to determine which ones are most beneficial.
Arabmotlagh el al. performed a prospective study on use of alendronate after total hip arthroplasty. They reported that the alendronate-treated patients had significantly less periprosthetic bone loss on DXA scans after 6 years.
Illustration A shows evidence of osteolysis (arrows) around a total hip arthroplasty.
Incorrect Answers:
5: These medication classes do not decrease osteolysis after total joint arthroplasty.
A 60-year-old woman has progressive neck pain, upper extremity pain, and paresthesias. A lateral cervical spine radiograph and an MRI scan are shown in Figures 52a and 52b. What is the most likely underlying diagnosis?
Osteomyelitis
Ankylosing spondylitis
Age-related degenerative changes
Rheumatoid arthritis
Previous cervical decompression Corrent answer: 4
The radiograph and sagittal T2-weighted MRI scan show multilevel degenerative changes and subaxial subluxations with anterolisthesis at C3-C4 and C4-C5 and retrolisthesis at C5-C6. In addition, there is evidence of midcervical kyphosis. Such findings are often seen in patients with rheumatoid arthritis. Patients with osteomyelitis typically show increased signal intensity in the disks and vertebral bodies. Patients with ankylosing spondylitis typically show ankylosis of the disks and vertebral bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single- level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
The use of lead glasses, thyroid shield, and a lead apron with a equivalent lead thickness of 0.25 mm
Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
Limiting the beam on time to only what is clinically important
The use of continuous fluoroscopy to ensure proper placement of implants
Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius from the fluoroscopy machine
Continuous fluoroscopy and cineradiography exposes the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray
tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Nicotine impairs osteoblast activity, thus interfering with bone remodeling.
The effects of smoking on bone healing are multifactorial and not yet fully understood.
The vasoconstrictive and platelet-activating properties of nicotine inhibit fracture healing.
Nicotine inhibits the function of fibroblasts, red blood cells, and macrophages.
Hydrogen cyanide inhibits oxidative metabolism at the cellular level. Corrent answer: 2
Tobacco smoking is now the leading avoidable cause of morbidity and mortality in the United States. The musculoskeletal effects of smoking have been implicated in osteoporosis, low back pain, degenerative disk disease, poor wound healing, and delayed fusion and fracture healing. A number of studies have demonstrated the relationship between smoking and development of pseudarthrosis. Numerous studies have been performed to
offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have
demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
In which of the following scenarios should a physician be relieved of their duties?
After 24 hours of continuous work
A significant error in care is noted
The physician appears fatigued
Physician is recovering from an ankle fracture
Chemical impairment is suspected
Impairment of a healthcare professional is the inability or impending inability to practice according to accepted standards as a result of substance use, abuse, or dependency (addiction). A surgeon (resident, fellow or attending) who discovers chemical impairment, dependence, or incompetence in a colleague or supervisor has the responsibility to ensure that the problem is identified and treated. Mechanisms exist for the proper identification and treatment of the impaired physician. Misconduct can be reported to state and local agencies. One must be sure to act in good faith with reasonable evidence when reporting such an incident. If a patient is at risk for immediate harm or injury by an impaired physician, one should assert authority and relieve the physician of the patient care and then address the problem with the senior hospital staff as soon as possible. The referenced article by Baldisseri is a review on the ethics of dealing with impaired healthcare professionals, with a focus on physicians.
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management?
DEXA scan
Brace treatment with a Jewett hyperextension brace
Anterior lumbar corpectomy and arthrodesis with instrumentation
Posterior lumbar decompression and fusion
Vertebral cement augmentation
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and
begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
Figure 10 is the radiograph of a middle-aged woman who has had midfoot pain for the past several years without antecedent trauma. What is the most likely etiology of her condition?
Osteomyelitis
Kohler disease
Rheumatoid arthritis
Primary osteoarthritis
Osteochondritis dissecans
The radiograph shows isolated degeneration in the talonavicular joint that is symmetric. The symmetry of the degeneration is characteristic of an inflammatory arthritis. In the absence of trauma, isolated arthritis in this joint is uncommon. The navicular is normal sized, ruling out Kohler disease (as well as the patient being in the wrong age group). There are no erosions indicative of osteomyelitis. Osteochondritis dissecans appears as focal osteochondral lesions, which are not present in the radiograph.
Figure 39 is the radiograph of a 67-year-old woman with rheumatoid arthritis who reports an 8-month history of increasing pain, swelling, and deformity. Anti- inflammatory drugs, orthotics, and extra-depth shoes have failed to provide relief. What is the next most appropriate step in treatment?
First metatarsophalangeal joint arthrodesis and lesser metatarsal head resections
First metatarsophalangeal joint replacement and lesser metatarsal head resections
Keller arthroplasty and lesser metatarsal head resections
Distal Chevron osteotomy and lesser metatarsal head resection
Lapidus procedure and Weil osteotomies
The patient has a severe rheumatoid forefoot deformity involving all metatarsophalangeal joints. Coughlin and Mann have found that 90% of patients have excellent and good results with combined first metatarsophalangeal fusion and lesser metatarsal head resection. Keller arthroplasty does not provide a stable platform for walking and is associated with recurrent deformity and pain. The first metatarsophalangeal joint replacement has not been shown to provide reliable long- term results. Osteotomies may be indicated in patients without erosive joint changes. The Lapidus procedure is an arthrodesis of the first tarsometatarsal joint, which would not address the patient's arthritic first metatarsophalangeal joint.
The operative report of a recent patient incorrectly documents the timing of peri-operative antibiotic administration. How should the
medical record be legally altered?
Obtain written approval from the hospital medical director
Obtain written approval from the risk management team
Obtain written approval from your lawyer and the senior partners of his law firm
No approval is needed, as you were the treating surgeon and have identified
the error
It is illegal to alter the medical record, but an addendum can be made
It is illegal to alter the medical record under any circumstance. If a documentation error has occurred, you may addend the medical record by identifying the error and noting the correction.
The review article by Bal discusses medical practice and highlights the four legal elements that must be proven in litigation: (1) a professional duty owed to the patient; (2) breach of such duty; (3) injury caused by the breach; and (4) resulting damages.
A 31-year-old woman underwent a left Kidner procedure 3 months ago. She now has pain overlying the medial column of the foot. She withdraws the foot when touching of the medial foot is attempted. Examination reveals allodynia, pain, hyperalgesia, and edema of the medial foot. What is the most likely diagnosis?
Shingles
Cellulitis
Charcot foot
Osteomyelitis
Reflex sympathetic dystrophy
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
Question 41
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively? Review Topic
Explanation
function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis.
Question 42
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 43
A 35-year-old man falls off of a roof and sustains an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed but was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is 40° to 100°. What is the next appropriate step in management?
Explanation
Question 44
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?

Explanation
Question 45
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 46
A 71-year-old woman has a failed revision hip arthroplasty and is undergoing a re-revision hip arthroplasty. Her last hip surgery was 4 years ago with revision of the acetabular component. Radiographs show a well-fixed extensively porous-coated femoral component and a failed acetabular component with proximal and medial migration through the floor of the acetabulum. Preoperative laboratory studies reveal an erythrocyte sedimentation rate (ESR) of 70 mm/h (normal 0-29 mm/h), a C-reactive protein (CRP) of 23.3 (normal 0.2-8.0), and a negative hip aspiration. At the time of surgery, tissues look inflamed and a frozen section shows 20 WBC per high power field; however, a Gram stain is negative. What is the most appropriate action at this point?
Explanation
REFERENCES: Sanzen L, Sundberg M: Periprosthetic low-grade hip infections: Erythrocyte sedimentation rate and C-reactive protein in 23 cases. Acta Orthop Scand 1997;68:461-465.
Spangehl MJ, Hanssen AD, Osman DR: Diagnosis and treatment of the infected hip arthroplasty, in Morrey BF(edA)L:-MJoaidnetnaRCeopplyacement Arthroplasty, ed 3. Philadelphia, PA, Churchill Livingstone, 2003, pp 856-874. Question 71
A 79-year-old patient has a history of peripheral vascular disease and reports chronic knee pain. She has had coronary artery disease treated with angiography and stents on two occasions. Peripheral pulses are absent in both lower extremities, but the patient is disabled by advanced chronic degenerative arthritis in her right knee and would like to proceed with a total knee arthroplasty. The next most appropriate evaluation should include which of the following?
Ankle-brachial index of the affected lower extremity
Femoral popliteal angiography
Venous Dopplers of both lower extremities
MRI of the popliteal fossa
Radiographs to identify calcified plaques in the femoral artery
DISCUSSION: This question is designed to draw attention to the fact that peripheral vascular disease carries an increased risk of complications for the patient and should be carefully evaluated. The vascular surgeon will make the choice of revascularization or surgical clearance for knee reconstruction based on the initial results of the ankle-brachial index.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9:253-257.
Question 47
Stability at the atlanto-occipital joint is provided mainly by
Explanation
REFERENCES: Werne S: Studies in spontaneous atlas dislocation. Acta Orthopaedica Scandinavica 1977;23(supplement).
Jarrett PJ, Whitesides TE Jr: Injuries of the cervicocranium, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 665-697.
Question 48
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? Review Topic

Explanation
(SBQ12SP.9) A 62-year-old male underwent posterior spinal instrumented fusion for degenerative lumbar spondylolithesis one year ago. He presents to office complaining of persistent lower back pain. The pain initially improved but over the last 6 months he has had recurring pain at the site of the surgery primarily with activity. He denies back pain at rest or night pain. Physical examination reveals a well healed wound and no physical abnormalities. He has no tenderness to palpation to the thoracic or lumbar spine. He has no neurological deficits. His laboratory results show an erythrocyte sedimentation rate (ESR) = 8 mm/h and C-reactive protein (CRP) = 3 mg/L at the last visit which are both within normal limits. Figure A shows a series of radiographs from his pre-operative, 3 month post-operative and 1 year post-operative clinic visits, respectively. Which of the following investigations would best confirm the suspected underlying diagnosis? Review Topic
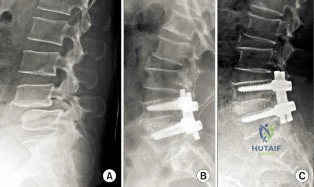
MRI of lumbar spine
Repeat ESR/CRP and whole body bone scan
CT of lumbar spine
Dynamic flexion/extension plain film radiographs
Dynamic lateral bending plain film radiographs
This patient has clinical and radiographic features of failed spinal arthrodesis. CT scan have been shown to be the most relable method for assessing spinal fusion postoperatively.
Reported rates of nonunion following posterior spinal fusion range from 0-70%. Rates are variable due to the various operative techniques, underlying diagnoses as well as asymptomatic patients. Non-union may lead to changes in alignment, spinal instability and potential neurological injury. Static radiographs have long been used as a practical method of fusion assessment, but these tend to significantly overestimate the presence of a solid fusion. Lack of movement at a fused segment, on dynamic views, does not confirm fusion. CT offers excellent bony resolution and are less affected by metal artifact compared to MRI.
Patel et al. showed that tobacco use, malnutrition, oral anti-inflammatory use, multilevel fusion, prior spine surgery, and sagittal imbalance are all risk factors for spinal nonunion.
Mok et al. looked at erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels after spinal surgery and compared their usefulness as predictors of infectious complications in the early postoperative period. They found that CRP is more applicable, predictable, and responsive in the early postoperative period compared with ESR. Using a second rise or failure to decrease as expected for CRP is sensitive for infection.
Shelby et al. reviewed the radiological assessment of spinal fusion. They comment that fine-cut imaging, multiplanar reconstruction, and metal artifact reduction have increased the ability to assess fusion on CT.
Figure A shows a series of lateral radiographs of the lumbar spine with posterior spinal instrumentation. Illustration A shows a lateral CT scan image of multi-level pseudoarthrosis after posterior spinal instrumented fusion. Illustration B shows an
intra-operative
view
of
spinal
pseudoarthrosis
(white
arrow).
Incorrect
(SBQ12SP.19) A 41-year-old male presents with acute onset of low back pain that started when he was trying to lift a heavy box while helping his brother move apartments two days ago. The pain has been severe enough to cause him to miss work yesterday. He has no neurologic deficits. What are the chances he will return to work within 6 weeks? Review Topic
1 80 to 90%
2 70 to 80%
3 60 to 70%
4 50 to 60%
5 40 to 50%
Most adults (up to 80%) will experience an episode of low back pain in their lifetime. In those whose pain is severe enough to cause them to miss work, 60 to 70% will return by 6 weeks, and 80 to 90% will return by 12 weeks.
Low back pain is common in adults. Most patients experience resolution of symptoms quickly and have no lasting loss of function. However, 5 to 10% develop chronic pain. Recurrence of pain is common, and is part of the natural history, occurring in 20 to 72% of patients. After 12 weeks, return to work rates are slow.
Shen et al. review the nonoperative management of acute and chronic low back pain. The authors note that none of the available interventions has been proven by high quality large randomized controlled trials. The authors believe that low dose oral
steroids are safe in the short term and that injection therapy should not be used without a reasonable presumptive diagnosis.
Madigan et al. review the management of lumbar degenerative disease. The authors emphasize that the majority of patients improve within 6 weeks with or without treatment. For patients that do not, the authors do not recommend epidural injection, as there are no good studies to support their use in the treatment of discogenic back pain. When surgical treatment is indicated they state that arthrodesis is the gold standard, although the long term results of total disk arthroplasty are being elucidated.
Illustration A shows a table of available non-operative treatment modalities for back pain. Illustration B shows a list of possible diagnoses associated with acute low back pain, with those associated with neurogenic pain italicized. Illustration C shows a list of 'red flag' symptoms indicating serious/emergent causes of low back pain.
Incorrect
2:
Longer
to than
90%
Question 49
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic

Explanation
Question 50
A total knee arthroplasty is recommended to a mentally competent 68-year-old woman who has disabling knee pain caused by degenerative arthritis. Her son has researched the procedure on the internet and prefers the Acme Female Knee for his mother. You have designed the Axis Woman's Knee, for which you receive royalties, and use it exclusively. Which of the following ethical principles takes precedence in guiding her treatment?
Explanation
Question 51
A 23-year-old man who is a competitive overhead athlete has shoulder pain. Based on the pathology shown in Figure 47, what treatment option would yield the highest satisfaction and return to overhead sports?
Explanation
REFERENCES: Snyder SJ, Karzel RP, Del Pizzo W, et al: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Altchek DW, Warren RF, Wickiewicz TL, et al: Arthroscopic labral debridement: A three-year follow-up study. Am J Sports Med 1992;20:702-706.
Question 52
The 73-year-old patient undergoes shoulder hemiarthroplasty. What is a risk factor for a poor outcome?
Explanation
Surgical treatment is favored for young, active patients with displaced proximal humerus fractures. Nonsurgical treatment is favored to treat fractures with minimal displacement among low-demand elderly patients. When ORIF is used, a number of strategies are employed to prevent failure, including restoration of medial cortical support (medial calcar), incorporation of the rotator cuff into the construct, and placement of screws of adequate length to gain purchase in the subchondral bone of the humeral head. Intramedullary allograft is not routinely required but is useful when dealing with osteoporotic bone. Cancellous allograft has not been shown to prevent
failure. Varus collapse and failure of fixation are more prevalent in patients with osteoporotic bone, and, in these cases, strategies for supplemental fixation are advisable. In cases of severe osteoporosis, comminution, or poor bone quality, shoulder arthroplasty may be a better choice. Without a functioning rotator cuff, as would happen with a tuberosity nonunion, outcomes after shoulder hemiarthroplasty and TSA are poor.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 53
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 54
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 55
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 56
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 57
Primary chondrosarcoma of bone most commonly occurs in which of the following locations?
Explanation
REFERENCES: Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Simon M, Springfield D, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 58
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
Question 59
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 60
A patient undergoing joint arthroplasty is put on a drug that competitively inhibits the activation of an enzyme that breaks down Factor Ia. The drug is
Explanation
Tranexamic acid competitively inhibits the activation of plasminogen to plasmin by binding to specific sites on both plasminogen and plasmin. Tranexamic acid has roughly eight times the antifibrinolytic activity of an older analogue, e-aminocaproic acid. It is used during joint replacement surgery to reduce blood loss and the need for transfusion.
Watts et al. review strategies for minimizing blood loss and transfusion. They recommend 1g of TXA prior to incision, and 1g at wound closure. They also recommend giving fluids for symptoms of anemia, rather than transfusion, as even high risk patients do well with sufficient intravascular volume even with low hemoglobin levels.
Imai et al. evaluated TXA in 107 patients undergoing THA. They found that intraoperative blood loss after preoperative TXA administration was lower than both control and postoperative TXA administration groups. They recommend using 1 g of TXA 10 minutes before surgery and 6 hours after the first administration to best reduce blood loss during THA.
Gillette et al. retrospectively reviewed 2046 patients receiving TXA for THA or TKA together with either aspirin, warfarin or dalteparin. They found that the rates of symptomatic DVT (0.35%, 0.15%, and 0.52%, respectively) and nonfatal PE were similar (0.17%, 0.43%, and 0.26%, respectively) for the 3 drugs respectively. They recommend TXA to decrease blood loss and transfusion.
Illustration A shows the role of tranexamic acid in the fibrinolytic cycle and the
clotting cascade.
Incorrect Answers:
Question 61
A 20-year-old man has a large soft-tissue mass behind his knee. MRI scans are shown in Figures 10a through 10c. Figure 10d shows a clinical photograph of his chest. The patient’s condition is most likely a result of a defect in what gene?
Explanation
REFERENCES: Theos A, Korf BR, American College of Physicians, et al: Pathophysiology of neurofibromatosis Type 1. Ann Intern Med 2006;144:842-849.
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Question 62
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
REFERENCES: Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Morrey BF: Difficult complications after hip joint replacement: Dislocation. Clin Orthop 1997;344:179-187.
Question 63
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of
Explanation
the fracture.
REFERENCES: Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Banks AS, Cain TD, Ruch JA: Physeal fractures of the distal phalanx of the hallux. J Am Podiatr Med Assoc 1988;78:310-313.
Question 64
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
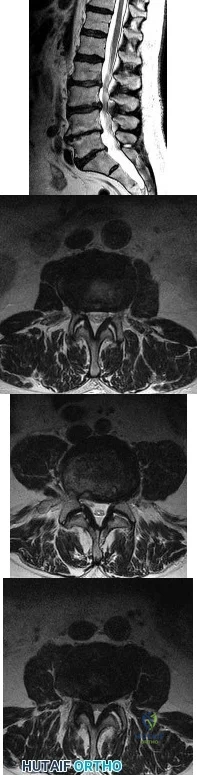
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 65
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 66
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
REFERENCES: Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 67
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 68
A 72-year-old male sustains the injury shown in Figure A as a result of a fall from a ladder. Which of the following factors has been shown to be associated with increased collapse or sliding displacement?

Explanation
Palm et al showed that 22% of patients with a fractured lateral femoral wall underwent reoperation for collapse of fracture compared to 3% with an intact lateral femoral wall. Interestingly, 74% of the lateral proximal femoral wall fractures were iatrogenic during the procedure itself.
Gotfried et al reported on 24 patients with postoperative intertrochanteric hip fracture collapse and noted that this complication followed fracture of the lateral wall in every instance and resulted in a protracted period of disability until fracture healing. They recommend care when drilling at the base of the lateral wall intraoperatively.
Lindskog et al review the diagnosis, treatment, as well as biomechanical reviews of treatment options for unstable intertrochanteric hip fractures.
Incorrect Answers:
OrthoCash 2020
Question 69
ORIF of the injury was chosen (as illustrated in Figure 27). Long-term results may include
Explanation
The injury mechanism describes axial loading to a plantar-flexed foot and is classic for Lisfranc injury. If the initial films are not diagnostic as in this case, weight-bearing films are a reasonable next step. Radiographic widening of 2 mm or more between the second metatarsal base and medial cuneiform (as
compared to the other side) is diagnostic; occasionally, a "fleck" sign (a small bony fragment noted in the Lisfranc joint) may indicate an avulsion fracture. Clinical signs include plantar ecchymosis, tenderness over the Lisfranc joint, and an inability to bear weight. Anatomic ORIF or fusion are the options for treatment, and results for ligamentous injuries are better when fusion is performed. Better AOFAS scores have been demonstrated with fusion, and a higher incidence of pain and arthritis have been noted with fixation. No significant difference has been seen regarding hardware failure, and hindfoot pain is not a consideration.
RECOMMENDED READINGS
Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816.View Abstract at PubMed
Kuo RS, Tejwani NC, Digiovanni CW, Holt SK, Benirschke SK, Hansen ST Jr, Sangeorzan BJ. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000 Nov;82-A(11):1609-18. PubMed PMID: 11097452. View Abstract at PubMed Rammelt S, Schneiders W, Schikore H, Holch M, Heineck J, Zwipp H. Primary open reduction and fixation compared with delayed corrective arthrodesis in the treatment of tarsometatarsal (Lisfranc) fracture dislocation. J Bone Joint Surg Br. 2008 Nov;90(11):1499-506. doi: 10.1302/0301-620X.90B11.20695. PubMed PMID: 18978273. View Abstract at PubMed
Question 70
A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable, she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
Explanation
Question 71
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management? Review Topic
Explanation
and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses.
Question 72
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
Explanation
REFERENCES: Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.
Buckley RE, Tough S: Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg 2004;12:172-178.
Question 73
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?
Explanation
REFERENCES: Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2,
pp 2391-2409.
Dameron TB Jr: Fractures of the proximal fifth metatarsal: Selecting the best treatment option.
J Am Acad Orthop Surg 1995;3:110-114.
Question 74
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 75
What percentage of bone weight is collagen?
Explanation
Question 76
Figures 20a and 20b show the radiographs of an obese 15-year-old boy who has severe left groin pain and is unable to bear weight following a minor injury. Treatment should consist of
Explanation
REFERENCES: Aronson DD, Loder RT: Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop 1996;322:99-110.
Karol LA, Doane RM, Cornicelli SF, Zak PA, Haut RC, Manoli A II: Single versus double screw fixation for treatment of slipped capital femoral epiphysis: A biomechanical analysis. J Pediatr Orthop 1992;12:741-745.
Stanitski CL: Acute slipped capital femoral epiphysis: Treatment alternatives. J Am Acad Orthop Surg 1994;2:96-106.
Question 77
.Figures 255a through 255c are the radiographs and MRI scan of a 73-year-old man who has severe pain and functional disability of the right shoulder despite receiving several cortisone injections and physical therapy. Examination reveals restricted shoulder range of motion in forward elevation and both internal and external rotation. There is moderately diminished strength and pain with resisted forward elevation.What is the best treatment option?

Explanation

Question 78
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 79
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, Churchill Livingstone, 1993, pp 1-13.
Question 80
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
Explanation
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
Question 81
-A likely candidate for treatment with a thoracic lumbosacral orthosis scoliosis brace is seen in
Explanation

Question 82
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 83
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?
Explanation
REFERENCES: Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Kasser JR (ed): Orthopedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 389-426.
Question 84
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Explanation
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 85
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 86
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 87
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 88
.Figures 89a and 89b are the radiographs of an 18-year-old woman who has had elbow pain after falling on an outstretched hand. She is evaluated 5 days after the injury. Examination reveals the wrist is normal and her elbow has a limited arc of motion of 30 to 90 degrees of flexion/extension and 20 to 20 degrees of pronation and supination, with tenderness isolated to the lateral side of the elbow. What is the most appropriate treatment option?
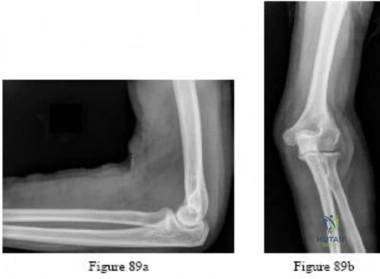
Explanation
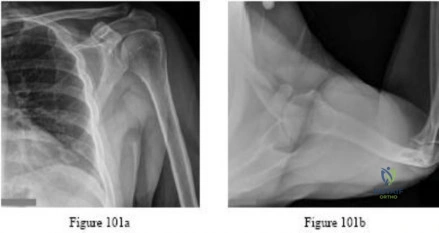
Question 89
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T 2 -weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 36.
Question 90
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?
Explanation
REFERENCE: Haentjens P, Autier P, Collins J, et al: Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women: A meta-analysis. J Bone Joint Surg Am 2003;85:1936-1943.
Question 91
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 92
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Miniaci A, Bailey WH, Bourne RB, McLaren AC, Rorabeck CH: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty. J Arthroplasty 1990;5:143-149.
Question 93
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?
Explanation
REFERENCE: Buckwalker JA, Einhorn TA, Simon SR (ed): Orthopedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 182-215.
Question 94
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 95
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 96
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.
Question 97
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle? Review Topic

Explanation
such as Parsonage-Turner syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
Question 98
On physical examination, he has no open wounds and is neurologically intact in both lower extremities. Imaging of the right femur (Figures A and B) and the left femur (Figures C and D) is shown. What is the next best step in treatment?

Explanation
OrthoCash 2020
Question 99
A healthy 39-year-old male presents to clinic with posttraumatic elbow stiffness after a minimally displaced radial head fracture. His injury occurred 4 months ago with no improvement in range of motion despite 10 weeks of supervised physiotherapy. Follow-up radiographs reveal normal osseous anatomy. What is the next best step in treatment?
Explanation
The goal of treatment in post-traumatic stiffness is to restore a functional range of elbow motion (30° to 130°). Non-operative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static or dynamic progressive elbow splinting with a turnbuckle has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Gelinas et al. treated 22 patients with an elbow contracture using a static progressive turnbuckle splint for a mean of 4.5 +/- 1.8 months. The mean range of motion improved from 32 - 108, to 26 - 127 degrees (p = 0.0001). Their results suggest that static progressive splinting is an effective modality for postoperative elbow stiffness.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12
month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Illustration A shows an image of a static progressive elbow splint. Incorrect Answers:
(SBQ12TR.94) A 60-year-old otherwise healthy female sustains the fracture in Figure
A. Immediate surgical treatment would most likely prevent which of the following complications?

Malunion.
Regional osteopenia.
Skin necrosis.
Posttraumatic arthritis.
Refracture.
The patient has a calcaneal tuberosity fracture. The Achilles tendon is attached to the displaced fragment, which can cause soft tissue compromise and skin necrosis if not treated promptly.
Displaced calcaneal tuberosity and tongue-type calcaneus fractures have a high incidence of wound complications if not treated urgently. Recommended management includes surgical fixation often performed percutaneously. Lag screws are typically directed from the posterior superior tuberosity inferiorly and distal. In cases of skin sloughing and skin necrosis, flaps may be needed.
Gardner et al. reviewed 139 tongue-type calcaneus fractures, and found that 21% had some degree of posterior skin compromise. Additionally, there was a statistically significant increase in posterior skin compromise with delayed presentations.
Hess et al. reviewed 3 cases of calcaneal tuberosity avulsion fractures that let to skin necrosis because of a delay in treatment.
Tornetta reviewed the indications for percutenaous treatment of calcaneus fractures, and found it was successful and most useful in tongue-type calcaneus fractures.
Figure A shows a lateral radiograph of a R ankle showing a calcaneal tuberosity fracture. Illustration A shows an AP radiograph of a R ankle following percutaneous reduction and internal fixation of the calcaneus fracture with two cannulated screws. Illustration B shows a lateral radiograph of a R ankle showing interval reduction and fixation of the calcaneus fracture. Illustration C shows a clinical photograph of posterior skin compromise associated with a calcaneal tuberosity fracture.
Incorrect Answers:
Malunion, regional osteopenia, posttraumatic arthritis, and refracture risk would not be significantly altered with immediate surgical intervention as opposed to operative management within a reasonable time frame.
Question 100
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the
Explanation
REFERENCE: Coleman SS, Chestnut WJ: A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop 1977;123:60-62.
