Orthopedic Board Review MCQs: Arthroplasty, Fracture & Tumor | Part 137

Key Takeaway
This page offers Part 137 of a comprehensive Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs by Dr. Mohammed Hutaif, modeled after OITE and AAOS exams. Ideal for orthopedic surgeons and residents preparing for certification, it includes interactive study and exam modes for effective preparation.
About This Board Review Set
This is Part 137 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 137
This module focuses heavily on: Arthroplasty, Deformity, Elbow, Foot, Fracture, Hip, Knee, Shoulder, Tumor.
Sample Questions from This Set
Sample Question 1: Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?...
Sample Question 2: During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the...
Sample Question 3: A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?...
Sample Question 4: A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindf...
Sample Question 5: Preoperative chemotherapy and wide excisionTumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, plate 4-46.
Question 2
During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the
Explanation
REFERENCES: Wasielewski RC, Cooperstein LA, Kruger MP, et al: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508.
Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws.
J Bone Joint Surg Am 1990;72:509-511.
Question 3
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Explanation
REFERENCES: Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA,
JB Lippincott, 2003, vol 2, pp 1265-1271.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy:
A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 4
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1422-1464.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Chandler JT, Bonar SK, Anderson RB, Davis WH: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
Question 5
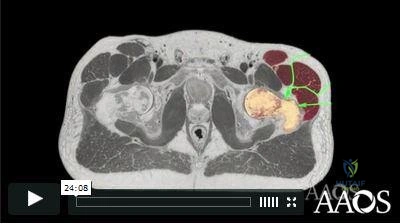
Preoperative chemotherapy and wide excision Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
A 20-year-old woman has a large mass over the right hip. An anteroposterior and oblique radiographs are shown in Slides 1 and
Question 6
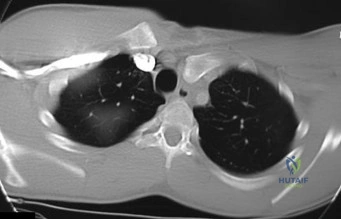
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step?
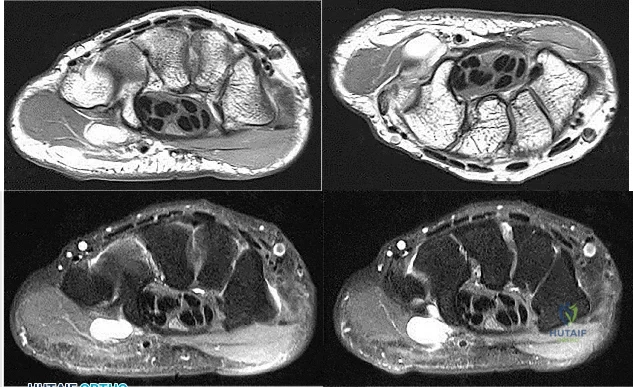
Explanation
Question 7
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 8
- A patient who had previously undergone a salvage pelvic (Chiari) osteotomy now requires a total hip arthroplasty. The most frequent complication of this procedure is
Explanation
Question 9
A coach of 3 football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on 1 team are different from those on the other teams?
Explanation
Data collected in research studies fall into 1 of 2 categories—continuous or discrete. Continuous data can be displayed on a curve. Examples include height, weight, and time recorded in a 40-yard dash. Discrete data represent data that fall into specific categories such as gender or the presence or absence of a risk factor.
ANOVA is used to determine statistical significance in mean values of continuous data when there are more than 2 independent samples. The 2-sample t test compares mean values of continuous data between 2 independent groups. The Chi-square test and Fisher's exact tests are tests used to analyze discrete data.
RESPONSES FOR QUESTIONS 58 THROUGH 61
Paresthesias in the fourth and fifth digits
Numbness on the lateral side of the forearm
Heterotopic ossification
Posterolateral rotatory instability of the elbow
Medial antebrachial cutaneous neuroma
For each surgical case described below, match the most likely related complication listed above.
Question 10
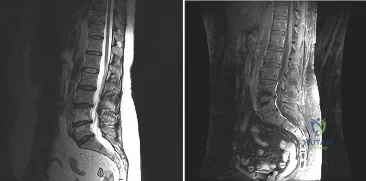
- A 31-year-old man who is a recent immigrant from Guatemala has had pain in his back and thighs for the past 12 months. History notes a recent diagnosis of gout, and the patient reports falling a distance of 3 feet on his buttocks immediately before the pain began. Examination reveals that he is neurologically intact. Plain radiographs are shown in Figures 44a and 44b, and T2-weighted MRI scans are shown in Figures 44c and 44d. The most likely cause of the pathologic fracture is
Explanation
The MR demonstrates involvement of L1 and adjacent disc spaces. With peri-vertebral edema and mass involving the posterior aspect of the vertebral body, placing pressure on the spinal cord. There is also involvement of the L2-3 disc with early signal changes.
The slow clinical course of the patients symptoms, being from a third world country and the findings on imaging studies, with an anterior wedge compression fracture. The level most commonly involved with TB is lower thoracic and upper lumbar. The anterior wedging results in the classic “Gibbus”.
Some of the MR findings are also consistent with metastatic disease, but with the localized mass, peri-vertebral abscess make this choice more unlikely.
The usual findings on MR found with TB are: Confluently decreased signal intensity of the vertebral bodies associated interspace with poor distinction between these on short TR/short TE images: Abnormal increased signal of the disk on long TR/long TE images with an abnormal configuration (i.e., absent intranuclear cleft): Increased signal of the vertebral endplates at the abnormal disk level on long TR/long TE images.
Question 11
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 12
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
REFERENCE: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 458.
Question 13
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413.
Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
O’Driscoll SW: Elbow arthritis: Treatment options. J Am Acad Orthop Surg 1993;1:106-116.
Question 14
A year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 15
A 54-year-old man undergoes revision surgery for loosening and osteolysis of a cementless acetabular component. The membrane obtained from behind the component at the time of surgery is analyzed for particulate debris particle size. Which particle size is most likely responsible for the membrane formation?
Explanation
A. Excessive femoral component flexion
B. Excessive anterior slope of the proximal tibia
C. Excessive tibial component varus
D. Excessive valgus resection of the distal femur
Question 16
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
Explanation
Plantar distal phalanges to medial navicular
Medial navicular to dorsal lateral cuneiform
Plantar 1st metatarsal to dorsal lateral cuneiform
5th metatarsal base to dorsal medial cuneiform
Plantar distal phalanx of the hallux to dorsal distal phalanx of hallux
Dynamic tendon transfer to restore active dorsiflexion of the foot involves transferring the posterior tibial tendon (PTT) insertion on the medial navicular to the dorsal lateral cuneiform.
Common peroneal nerve (CPN) injuries following traumatic knee dislocation are common, with an incidence of 25-40%. CPN palsy is characterized by foot drop due to loss of ankle dorsiflexors with a steppage gait and eventual development of a supinated equinovarus foot secondary to the unopposed pull of the PTT. Nonsurgical management involves use of an ankle-foot orthosis and physical therapy. Surgical
options include acute primary repair, nerve grafting with either autologous sural nerve or nerve conduits and dynamic tendon transfer. The PTT is harvested from its insertion at the navicular, passed through the interosseous membrane (IOM) and anchored to the lateral cuneiform (see Illustration A). The classic bridle procedure involves concomitant anastamosis of the PTT to the tibialis anterior (TA) and peroneus longus (PL) tendons.
Garozzo et al reported a case series of 62 patients with post-traumatic CPN palsy who underwent a one-stage procedure consisting of nerve repair and PTT transfer. Nerve repair combined with PTT transfer improved postoperative outcomes compared to nerve repair alone. At 2-year follow up, neural regeneration was demonstrated in 90% of patients. The authors hypothesized that poor outcomes following nerve repair alone are due to force imbalance between the functioning flexors and paralyzed extensors, which is somewhat equalized by performing a PTT transfer at time of repair.
Niall et al reviewed 55 patients with traumatic knee dislocation and reported a 41% incidence of CPN injury, exclusively associated with dislocations involving disruption of the posterior cruciate ligament (PCL) and posterolateral corner (PLC). Complete neurologic recovery was found in only 21% of patients. The best prognosis was found with lesions in continuity, less than 7cm of nerve involvement, and short conduction block and muscle activity on nerve conduction and EMG studies.
Vigasio et al described a dynamic tendon transfer technique for traumatic complete CPN injury, involving transfer of the PTT to the TA rerouted to a new origin at the lateral cuneiform to restore ankle dorsiflexion and flexor digitorum longus (FDL) to the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) to restore digit dorsiflexion. Rerouting the TA towards the transferred PTT ensures the PTT harvest length is sufficient. This avoids excessive tensioning of the PTT, which may limit tendon excursion and result in a static tenodesis rather than dynamic function, as well as the need for PTT lengthening which may decrease strength of the transfer
Illustration A is a series of intraoperative photographs demonstrating PTT transfer from Garg et al. An incision is made distal to the medial malleolus and the PTT is harvested subperiosteally (A). The PTT is delivered through a second incision ~15cm proximal to the medial malleolus (B-C). The PTT is then passed through the interosseous membrane and out a third incision over the anterior fibula (D). Lastly, the PTT is passed through a fourth incision over the dorsal midfoot and anchored to the lateral cuneiform (E).
Incorrect Responses:
nerve and therefore would not be functional. Answer 5: Transferring the flexor hallucis longus (FHL; insertion = plantar distal phalanx of the hallux) to the insertion of the EHL (dorsal distal phalanx of hallux) is recommended for correction of claw toe deformity and would not help restore foot dorsiflexion in this patient.
Question 17
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 18
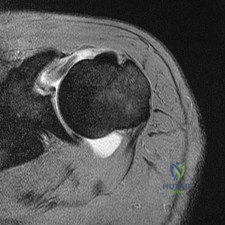
The MRI scan shown in Figure 33 reveals the sequelae of an acute traumatic anteroinferior shoulder dislocation. The image reveals the typical separation of what two commonly injured structures? Review Topic

Explanation
Question 19
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?

Explanation
well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 20
Figure 59 shows properties of a material being tested for use as an implant. What is represented by the portion of the stress-strain curve from point A to point B?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 45-46.
El-Ghannam A, Ducheyne P: Biomaterials, in Mow VC, Huiskes R (eds): Basic Orthopaedic Biomechanics and Mechano-Biology, ed 3. Philadelphia, PA, Lippincott-Raven, 2005, pp 501-503.
Question 21
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 22
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
REFERENCES: Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 23
A study was conducted in 500 patients to measure the effectiveness of a new growth factor in reducing healing time of distal radial fractures. The authors reported that average healing time was reduced from 9.2 to 8.9 weeks (P < 0.0001). Because the difference was highly statistically significant, they recommended routine clinical use of this drug despite its high cost. A more appropriate interpretation of these results is that they are
Explanation
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 24
Which of the following activities can improve posterior capsular contractures?
Explanation
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 25
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 26
Figure 89a is the radiograph of a 24-year-old man who was involved in a motor vehicle accident. A closed reduction is performed and a post-reduction CT scan is shown in Figure 89b. What is the next most appropriate step in management?

Explanation
Question 27
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 28
A 32 yr old man with oxalosis is scheduled for a surgical treatment of spinal stenosis. Which of the following organs is most likely to show signs of systemic oxalosis during a preoperative assessment?
Explanation
Question 29
All of the following are considered contraindications to the use of functional bracing of a humeral shaft fracture EXCEPT:

Explanation
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), segmental fractures, injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
The article by Rutgers and Ring found that proximal one-third oblique humeral shaft fractures had an unacceptably high 29% rate of nonunion treated with a functional brace.
The article by Sarmiento et al found a 97% rate of union, a radial nerve palsy incidence of 11%, and no contraindication to the use of functional braces in humeral shaft fractures associated with radial nerve palsy.
The review article by Defranco and Lawton states that 70% of these radial nerve injuries recover spontaneously. They note that it "seems reasonable, however, to consider surgical intervention (radial nerve exploration) between 4 and 6 months based on the patient’s clinical course."
Question 30
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
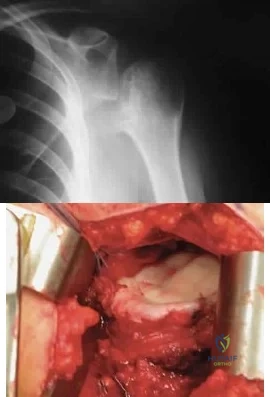
Explanation
Question 31
What is the most likely diagnosis? Review Topic
Explanation
Question 32
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
Explanation
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22- mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Question 33
During stabilization of a slipped capital femoral epiphysis, the screw penetrates into the joint. The screw is repositioned so that it is within the femoral head. This transient penetration of the hip joint will most likely lead to
Explanation
REFERENCES: Zionts LE, Simonian PT, Harvey JP Jr: Transient penetration of the hip joint during in situ cannulated-screw fixation of slipped capital femoral epiphysis. J Bone Joint Surg Am 1991;73:1054-1060.
Vrettos BC, Hoffman EB: Chondrolysis in slipped upper femoral epiphysis: Long-term study of the etiology and natural history. J Bone Joint Surg Br 1993;75:956-961.
Question 34
Following irrigation and debridement, what is the preferred method of fixation for a displaced open tibia fracture with a 16-cm clean wound?
Explanation
Question 35
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
REFERENCES: Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 36
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 2-49.
Question 37
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?
Explanation
REFERENCE: Millis MB, Murphy SB, Poss R: Osteotomies about the hip for the prevention and treatment of osteoarthritis. Instr Course Lect 1996;45:209-226.
Question 38
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity include a

Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
View Abstract at PubMed
Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 39
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 40
Anteromedial approach (Ludloff)
Explanation
The lateral femoral cutaneous nerve can be injured during a direct anterior approach to the hip. The superior gluteal nerve enters the gluteus medius from posterior to anterior approximately 5 cm above the greater trochanter. This nerve can be injured during the direct lateral and anterolateral approaches to the hip. Branches of the inferior gluteal nerve as well as the sciatic nerve can be injured during the posterior approach, and the obturator nerve can be damaged when performing a medial approach to the hip.

Question 41
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of
Explanation
REFERENCES: Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
Lotke PA, Abend JA, Ecker ML: The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop 1982;171:109-116.
Question 42
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
REFERENCES: Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 43
In total hip arthroplasty, increasing the perpendicular distance from the center line of the femur to the center of rotation of the femoral head (femoral offset) results in
Explanation
include an increased range of motion, better mechanical advantage for the abductors and decreased instability because of better soft tissue tension. According to Charnley,
increasing the femoral offset should improve the abductor lever arm which should decrease the abductor force required for walking, and therefore decrease the energy requirement for gait as well as the overall joint reactive force. The largest possible disadvantage of increasing the femoral offset is increasing the out of plane bending moment which puts stress on the prosthetic stem. Poly wear is a direct effect of surface area contact which is not changed with femoral Offset.
Question 44
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 45
The mother of a 3-month-old infant states that she has difficulty positioning the infant’s legs during diaper changes. Examination reveals limited abduction of both hips and a negative Ortolani sign. A radiograph reveals bilaterally dislocated hips. Initial management consists of guided reduction in a Pavlik harness, with weekly follow-up. Figures 57a and 57b show the radiograph and CT scan obtained after 6 weeks in the harness. Management should now consist of
Explanation
REFERENCES: Jones GT, Schoenecker PL, Dias LS: Developmental hip dysplasia potentiated by inappropriate use of the Pavlik harness. J Pediatr Orthop 1992;12:722-726.
Atar D, Lehman WB, Grant AD: Pavlik harness pathology. Isr J Med Sci 1991;27:325-330.
Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 46
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
REFERENCES: Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84.
Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Ganz R, Krushell RJ, Jacob RP, Kuffer J: The antishock pelvic clamp. Clin Orthop 1991;267:71-78.
Question 47
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of
Explanation
REFERENCE: Brassard MF, Insall JN, Scuderi GR: Complications of total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1801-1844.
Question 48
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Lee D, Ferlic R, Neviaser R: Hand infections, in Berger R, Weiss AP (eds): Hand Surgery. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 1784-1785.
Question 49
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of
Explanation
REFERENCE: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1077-1135.
Question 50
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 51
A 51-year-old male 2-pack per day smoker presents with a hyperkeratotic light brown plaque on the dorsum of his left ring finger that has been present for 7 years. It measures 14 mm by 13 mm. Initially, it responded to topical wart treatments, but has failed to do so recently so he sought evaluation by a dermatologist who biopsied the lesion. The results revealed squamous cell carcinoma (SCC) in situ, and he was referred for further surgical management. He has no other skin lesions, no history of SCC and no axillary lymphadenopathy. What is the next step in management?
Explanation
SCC in situ is a low-grade malignancy that typically presents as painless lesions on areas of high sun exposure such as the dorsum of the hand and fingers. The recommended treatment for lesions smaller than 100 mm is wide excision with 4 mm margins to a depth 1 layer below the tumor, along with any adjacent area of induration. Sentinel lymph node biopsy is typically not indicated in the setting of a low-grade tumor such as this one and in the absence of axillary lymphadenopathy.
Question 52
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 53
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?

Explanation
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds
Question 54
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic
Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 55
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Sun TC, Swee TC: Chondrosarcoma in Maffucci’s syndrome. J Bone Joint Surg Am 1985;67:1214-1219.
Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Began WB: Dyschondroplasia and hemangiomata (Maffucci’s syndrome). Arch Intern Med 1958;102:544.
Question 56
A 12-year-old child with L4 myelomeningocele who is schedules for foot surgery has a functioning ventriculoperitoneal shunt and has no history of allergies. Management should include
Explanation
Question 57
A 32-year-old male hockey player who is right-hand dominant was checked from behind and landed with full force into the boards. In the emergency department he reports shortness of breath. Figure 113 shows a 2-D CT scan. What is the best initial treatment for this injury?
Explanation
Question 58
Figure 163 is the radiograph of an 81-year-old man who had primary total hip arthroplasty 12 years ago and now has a 3-month history of left hip weight-bearing thigh pain. The appropriate treatment at this time is
Explanation
This patient has a loose cemented femoral component. The implant has subsided and the femur has remodeled into a varus position. Although the component may be removable without an extended trochanteric osteotomy, the varus bow of the femur will not allow distal fixation without use of an extended trochanteric osteotomy. The acetabular component appears
to be well fixed, and, as a result, should be retained in this older patient. An evaluation of stability could lead to possible revision of the acetabulum, and implants should be available.
Question 59
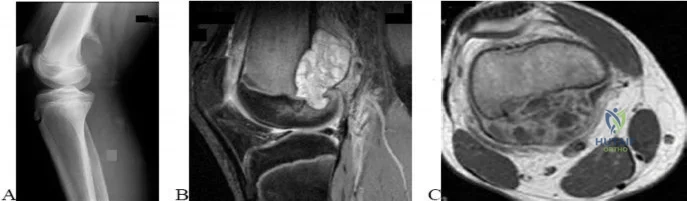
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
Explanation

Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
Question 60
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by Review Topic
Explanation
Question 61
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 62
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 63
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of
Explanation
REFERENCES: Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Stover S, Niemann K, Tullos J: Experience with surgical resection of heterotopic bone in spinal cord injury patients. Clin Orthop 1991;263:71-77.
Question 64
Parosteal osteosarcoma
Explanation
Question 65
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 66
A 52-year-old man with a BMI of 40 and primary osteoarthritis undergoes total hip arthroplasty through a posterolateral approach. To retract the femur anteriorly when exposing the acetabulum, the surgeon places a sharp curved retractor over (anterior to) the anterior inferior iliac spine. Pulsatile bleeding is encountered. A branch of which artery has been injured?
Explanation
Video 182 for reference
The femoral artery crosses the hip joint anterior to the anterior hip capsule. The medial femoral circumflex artery enters the joint along the route of the obturator externus. The obturator artery enters the hip joint beneath the transverse acetabular ligament. The iliac circumflex vessel arises superior to the hip joint.

RESPONSES FOR QUESTIONS 183 THROUGH 188
For each clinical scenario described below, identify the corresponding anteroposterior pelvic radiographic image shown above.
Question 67
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
REFERENCES: Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 68
A 2-year-old child refused to walk 3 days prior to being seen because of pain in the left hip. The pain has gradually subsided and the child is now walking. He is afebrile and has full motion of the hips. Laboratory studies show a normal CBC with differential and C-reactive protein. An ultrasound shows a joint effusion in the right hip. What is the most likely diagnosis?
Explanation
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2068-2070.
Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between
2010 Pediatric Orthopaedic Examination Answer Book • 11
septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004:86:1629-1635.
AL-Madena Copy
12 • American Academy of Orthopaedic Surgeons

Figure 7a Figure 7b
Question 69
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 70
A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal flexion, and normal pronation and supination. Radiographs reveal a 3- x 7-mm radiolucency of the capitellum. A T1-weighted MRI scan reveals a single solitary lesion, and T2-weighted images show no signal around the lesion. There are no intra-articular loose bodies. Appropriate management should include which of the following? Review Topic
Explanation
Question 71
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 72
Figure 36 shows the radiograph of a 28-year-old man who injured his shoulder in a motocross race. Management should consist of
Explanation
REFERENCES: Jupiter JB, Ring D: Fractures of the clavicle, in Ianotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott, Williams and Wilkins, 1999, pp 709-736.
Kona J, Bosse MJ, Staehli JW, Rosseau RL: Type II distal clavicle fractures: A retrospective review of surgical treatment. J Orthop Trauma 1990;4:115-120.
Question 73
The primary function of structure “A” in Figure 29 is to limit
Explanation
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 74
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
Explanation
REFERENCES: Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Beals RK, Bryant RE: The treatment of chronic open osteomyelitis of the tibia in adults.
Clin Orthop Relat Res 2005;433:212-217.
Question 75
Which treatment is associated with decreased complications related to femoral nerve blocks for TKA?
Explanation
TKA among elderly patients can be problematic, considering their potential for complex comorbidities including diminished cognitive function. As patients age, their tolerance for certain medications diminishes. Regional anesthesia is an important adjunct to a multimodal pain program, which can reduce narcotic pain medication use and improve cognitive function through less reliance on systemic medications. With regional pain management such as femoral nerve blocks comes potential for an increase in complications such as falls. Femoral nerve blocks improve pain but also have a large impact on quadriceps and motor function, which places patients at higher risk for falls.
Question 76
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T 1 -weighted, T 2 -weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-194.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 3897-3904.
Question 77
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Explanation
REFERENCES: van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437.
Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 78
-A 16-year-old girl was seen after a motor vehicle collision. Imaging studies including plain radiographs,MRI scans, and CT scans confirm bilateral jumped facets at C5-6 without disk herniation. She is alert,oriented, and neurologically intact. What is the most appropriate next step?
Explanation
Question 79
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
Explanation
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
Question 80
A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always "feels loose." Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization? Review Topic
Explanation
Question 81
A 23-year-old male college quarterback presents with acute left shoulder pain after being tackled. A radiograph of the injury is shown in figure A. After successful closed reduction, what shoulder position should be avoided in order to minimize the risk of a repeat injury? Review Topic

Explanation
Shoulder stability is achieved through the both dynamic and static stabilizers. The static stabilizers include the bony morphology of the joint, glenoid labrum, capsule, and glenohumeral ligaments. The contributions of the glenohumeral ligaments to shoulder stability are dependent upon the position of the humerus relative to the glenoid. Posterior stability is afforded to the joint by the superior glenohumeral ligament (SGHL) and the posterior band of the inferior glenohumeral ligament (IGHL). The SGHL specifically is taught and provides posterior stability with the shoulder in flexion, adduction, and internal rotation.
Kim et. al. reviewed their experience treating 27 athletes diagnosed with traumatic posterior shoulder instability and treated with arthroscopic posterior labral repair and capsular shift. Most patients were found to have an incompletely stripped posterior capsulolabral complex. After arthroscopic repair and shift, all 26 of the 27 patients treated had improved shoulder function and objective scores, a stable shoulder, and were able to return to sport.
Millett et. al. reviewed posterior shoulder instability. They describe the static restraints of the posterior shoulder as the SGHL, posterior band of IGHL, and the coraohumeral ligament (CHL). The SGHL and CHL are both taught in the position of flexion, adduction, and internal rotation, whereas the posterior band of the IGHL is taught in abduction. They describe posterior instability occuring secondary to overhead sports due to repetitive microtrauma causing gradual capsular failure.
Figure A is an axillary radiograph of the left shoulder demonstrating a posterior dislocation and an engaging reverse Hill-Sachs lesion.
Incorrect Answers:
Question 82
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 83
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 84
A 55-year-old woman fell and sustained an elbow dislocation with a coronoid fracture and a radial head fracture. The elbow is reduced and splinted. What is the most common early complication?
Explanation
REFERENCES: Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Ring D, Jupiter JB: Fracture-dislocation of the elbow. J Bone Joint Surg Am 1998;80:566-580.
Question 85
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon MA, Springfield DS, et al: Chondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 86
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 87
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 88
Figure 77 shows the clinical photograph of a 21-year-old male ice hockey player who sustained a blow to the jaw from another player’s hockey stick. Examination reveals an unstable jaw, mild bleeding with exposed bone, and malocclusion. What is the most serious acute complication of this injury?
Explanation
The mandible suspends the tongue anteriorly. When the mandible is fractured and the patient is supine, the tongue falls posteriorly and obstructs the airway. Soft-tissue swelling around the injured oronasal structures can also result in a loss of airway patency. Endotracheal or nasotracheal intubation is often impossible and a surgical airway may often have to be created to prevent death by asphyxiation. Other injuries that may require immediate attention include head or cervical spine injury and hemorrhage. A cerebrovascular accident is also less common but is associated with injury to the common carotid artery or its branches. Periodontal disease is generally a long-term complication from dental injuries. Hearing loss is not a common complication of dental and facial trauma.
REFERENCES: Seyfer AE, Hansen JE: Facial trauma, in Moore EF, Feliciano DV, Maddox KL (eds): Trauma, ed 5. New York, NY, McGraw-Hill, 2004, pp 423-444.
Rohrich RJ, Shewmake KB: Evolving concepts of craniomaxillofacial fracture management. Clin Plast
Surg 1992;19:1-10.
Question 89
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled “A” in Figure 45?
Explanation
REFERENCES: Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Sobel M, Levy ME, Bohne WH: Congenital variations of the peroneus quartus muscle: An anatomic study. Foot Ankle 1990;11:81-89.
Question 90
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 91
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?
Explanation
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 92
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 93
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 94
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of
Explanation
REFERENCES: Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Angermann P, Hougaard D: Chronic Achilles tendinopathy in athletic individuals: Results of nonsurgical treatment. Foot Ankle Int 1999;20:304-306.
Question 95
-Figures 156a and 156b are the radiographs of a 38-year-old man with diabetes mellitus who fell 8 feet from a ladder and sustained an isolated closed injury of his leg. Examination revealed swollen but soft compartments. His neurovascular examination was unremarkable. A damage-control fixator was initially applied, and his soft-tissue envelope is now amenable to further intervention. What is the most appropriate treatment?
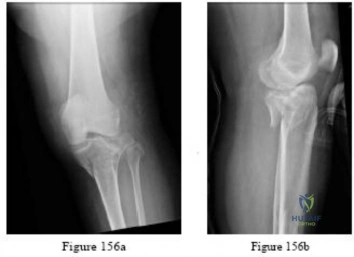
Explanation

Question 96
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to
Explanation
REFERENCE: El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 97
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
Question 98
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of Review Topic

Explanation
Question 99
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
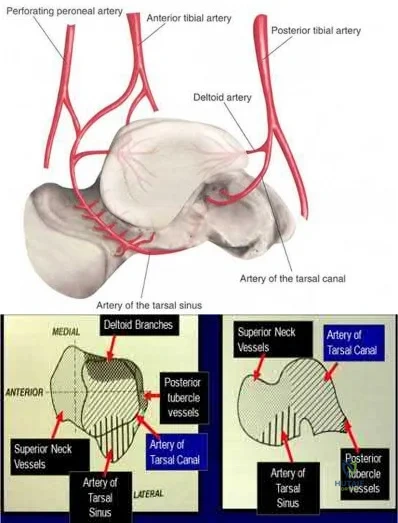
OrthoCash 2020
Question 100
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 965-981.
