Orthopedic Surgery Board Review MCQs: Foot, Fracture, Knee, Shoulder | Part 133
Key Takeaway
This Orthopedic Surgery board review quiz (Part 133) offers 100 high-yield MCQs for orthopedic residents and surgeons. Mimicking OITE/AAOS exam format, it covers Foot, Knee, Shoulder, and Fracture. Its purpose is to enhance professional certification preparation for AAOS and ABOS exams.
About This Board Review Set
This is Part 133 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 133
This module focuses heavily on: Foot, Fracture, Knee, Shoulder.
Sample Questions from This Set
Sample Question 1: Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?...
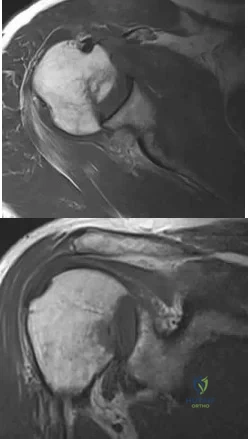
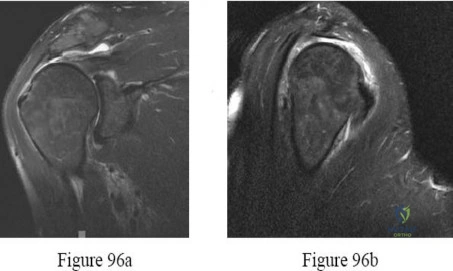
Sample Question 2: A 61-year-old man reports right shoulder pain and loss of external rotation since having a seizure 5 months ago. MRI scans are shown in Figures 82a and 82b. What is the most appropriate treatment? Review Topic...
Sample Question 3: To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?...
Sample Question 4: A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45° of valgus laxity at the metac...
Sample Question 5: A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tendernes...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 2
A 61-year-old man reports right shoulder pain and loss of external rotation since having a seizure 5 months ago. MRI scans are shown in Figures 82a and 82b. What is the most appropriate treatment? Review Topic
Explanation
Question 3
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 4
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45° of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25° of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
REFERENCE: Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg 1997;5:224-229.
Question 5
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 6
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 7
A 12-year-old girl has had increasing left knee pain for the past 3 months. A radiograph is shown in Figure 75a, and low- and high-power photomicrographs are shown in Figures 75b and 75c. What is the most appropriate treatment?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 203-209.
Papagelopoulos PJ, Galanis EC, Sim FH, et al: Clinicopathological features, diagnosis, and treatment of malignant fibrous histiocytoma of bone. Orthopedics 2000;23:59-65.
Question 8
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Explanation
REFERENCES: Matava MJ: Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-296.
Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307.
Question 9
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
corrective osteotomy.
REFERENCES: O’Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369.
Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Spinner RJ, O’Driscoll SW, Davids JR, et al: Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg 1999;24:718-726.
Question 10
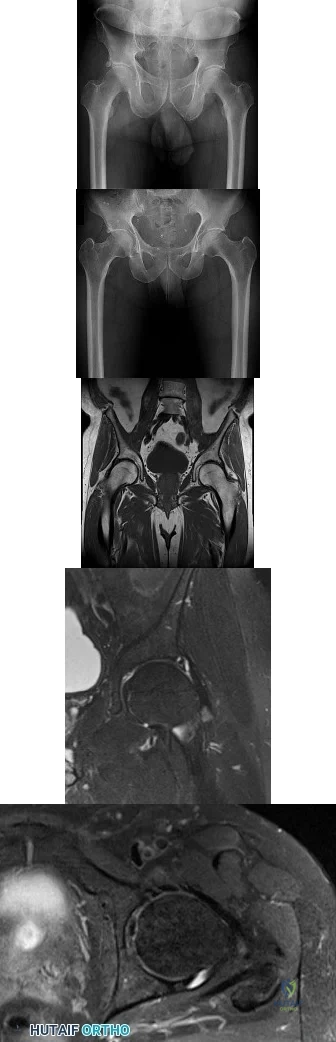
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. Images from an MRI scan of this patient's left hip are shown in Figures 3 through 5. What is the most likely cause of his acute pain?
Explanation
standing groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a
periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 11
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?
Explanation
REFERENCES: Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 12
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 13
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time? Review Topic

Explanation
(SBQ13PE.82) A renal ultrasound should be obtained in a patient with which of the following diagnoses? Review Topic
Congenital pseudoarthrosis of the clavicle
Accessory navicular
Congenital scoliosis
Charcot-Marie-Tooth Disease
Congenital curly toe
A renal ultrasound should be obtained in a patient with congenital scoliosis.
Congenitial scoliosis has a prevalence that is estimated at 1% to 4% in general population. It is associated with systemic anomalies in up to 61% of cases. The most common anomalies are cardiac defects, genitourinary defects and spinal cord malformations. As such, additional imaging of these systems should be considered in the initial work-up of these patients.
Ruf et al. retrospectively investigated 56 consecutive operative cases of congenital scoliosis. The average age at surgery was 9.9 years (1.5–17 years). There was one wound complication, 2 hardware failures, 1 revision and no neurological complications. They concluded that one-stage posterior hemivertebra resection and instrumentation was safe in this population.
Xu et al. examined the efficacy of selective partial hemivertebra excision via posterior-only approach in 17 adolescent patients with congenital kyphoscoliosis. There were no postoperative infections and no neurological complications. They concluded that this approach may be most successful in patients aged 9 to 14 years old, with the Risser sign grades from 0–3 and Cobb angles <60°.
Illustration A from Erol et al (UPOJ, Vol 15, 2002;37-42) shows a diagram of 'types' of congenital scoliosis based on the morphology of the vertebrae.
Incorrect Answers:
Question 14
Which nerve is most commonly injured after total knee arthroplasty?
Explanation
The tibial or peroneal nerves usually are not injured during total knee arthroplasty. Incidence of peroneal nerve damage is highest in knees with a valgus deformity and an associated flexion contracture attributable to nerve stretch. This nerve injury occurs in as many as 9% of patients undergoing knee arthroplasty. Tibial nerve injury is a rare occurrence and usually an iatrogenic transection injury. The infrapatellar branch of the saphenous nerve and its nerve plexus is commonly injured after the medial parapatellar approach, and altered sensation attributable to injury is reported in up to 70% of cases. Injury typically manifests as numbness inferior to the patella. The sartorial branch of the saphenous nerve provides sensation distal to the knee and is uncommonly injured with a medial parapatellar approach. These concepts are illustrated in video 57, “Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition.”
RECOMMENDED READINGS
Clarke HD, Bush-Joseph CA, Wolf BR. Selective Exposures in Orthopaedic Surgery: The Knee, 2nd Edition [DVD]. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2012.
Hunter LY, Louis DS, Ricciardi JR, O'Connor GA. The saphenous nerve: its course and importance in medial arthrotomy. Am J Sports Med. 1979 Jul-Aug;7(4):227-30. PubMed PMID: 474860.View Abstract at PubMed
Mistry D, O'Meeghan C. Fate of the infrapatellar branch of the saphenous nerve post total knee arthroplasty. ANZ J Surg. 2005 Sep;75(9):822-4. PubMed PMID: 16174002.View Abstract at PubMed
Schinsky MF, Macaulay W, Parks ML, Kiernan H, Nercessian OA. Nerve injury after primary total knee arthroplasty. J Arthroplasty. 2001 Dec;16(8):1048-54. PubMed PMID: 11740762.View Abstract at PubMed
Question 15
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include
Explanation
REFERENCES: Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Aprin H, Bowen JR, MacEwen GD, et al: Spinal arthrodesis in patients with spinal muscle atrophy. J Bone Joint Surg Am 1982;64:1179-1187.
Question 16
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
REFERENCES: Blazina ME, et al: Jumper’s knee. Orthop Clin North Am 1973;4:665.
Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper’s knee. Am J Sports Med 1984;12:375-380.
Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Rows J, et al: Patella tendinitis (jumper’s knees). Am J Sports Med 1978;6:362.
Question 17
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes an uncomplicated closed reduction under sedation in the emergency department. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, the patient has persistent pain at rest and forward elevation and external rotation weakness, but the remaining motor function in the extremity and sensation are intact. What is the best next step?
Explanation
modalities do not adequately address the concern over his potential for having sustained a rotator cuff tear.
Question 18
Decreased risk of shoulder and elbow injury in a throwing athlete has been demonstrated with which of the following? Review Topic
Explanation
Question 19
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?

Explanation
DISCUSSION: A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
Question 20
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Explanation
REFERENCES: Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87.
Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63.
Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
Kayanja M, Evans K, Milks R, et al: The mechanics of polymethylmethacrylate augmentation. Clin Orthop Relat Res 2006;443:124-130.
Question 21
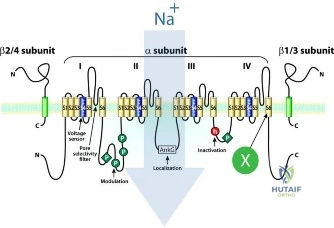
Figure A demonstrates the molecular structure of a cell membrane protein important in propagating the action potential of a neuron. Which of the following medications acts by binding to the location marked with an X in the illustration?
Explanation
Local anesthetics of the amide family (lidocaine, bupivacaine) bind to the intracellular portion of voltage-gated sodium channels to block sodium influx. This prevents depolarization and the initiation or conduction pain. Lidocaine and bupivacaine have a duration of action of 2 and 4 hours, respectively (4 and 8 hours with epinephrine), and maximum doses are 4.5mg/kg and 2.5mg/kg, respectively (7mg/kg and 3mg/kg with epinephrine respectively). Both are metabolized in the liver, and excreted by the kidneys.
Phillips et al. review specific analgesics. Agents used to manage chronic pain include tricyclic antidepressants, anticonvulsants, GABA agonists, local anesthetic analogs, and NMDA antagonists. Opiates may trigger tolerance and lack of efficacy may develop. In those with refractory chronic pain, centrally administered analgesics may be considered, including opiates, dilute local anesthetic, NMDA receptor antagonists, clonidine, midazolam, baclofen, or calcium channel blockers. Single agents may be less effective than analgesic combinations.
Scholz discussed the function of local anesthetics and sodium channels. There are 3 states to sodium channels: (1) The closed state at potentials below -70mV. In this state, Na+ ions cannot pass from 1 side to another. (2) The open state, initiated by depolarization of the membrane to above -40mV. The channel opens to allow Na+ ions to diffuse through the pore, causing an inward current, depolarizing the membrane further. (3) The inactivated state follows activation during prolonged depolarization. In this state, inactivation is seen in macroscopic currents.
Figure A shows the voltage gated sodium channel. Local anesthetics such as lidocaine and bupivacaine act at the binding site marked "X".
Incorrect Answers:
Question 22
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of
Explanation
REFERENCES: Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 449-458.
Hozack WJ, Goll SR, Lotke PA, Rothman RH, Booth RE Jr: The treatment of patellar fractures after total knee arthroplasty. Clin Orthop 1988;236:123-127.
Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 23
Calcitonin acts as an antiresorptive agent by
Explanation
REFERENCE: Lane JM, Nydick M: Osteoporosis: Current modes of prevention and treatment. J Am Acad Orthop Surg 1999;7:19-31.
Question 24
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 25
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 26
Which of the following enzymes is used to resorb bone by mature osteoclasts?
Explanation
Question 27
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 28
Decreased sun exposure leads to decreased bone health via what mechanism?
Explanation
Question 29
- A consecutive series of 50 patients is randomized to receive either treatment A or treatment B. At a 10-year follow up, patient satisfaction with treatment is measured. Which of the following statistical calculations will provide the most information regarding the magnitude of possible differences between the two groups of patients?
Explanation
Question 30
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 334.
Question 31
Figures below represent the radiographs obtained from a 37-year-old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?
Explanation
This patient has severe, uncorrectable varus deformity and pain from end-stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is
not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds
constraint to the knee to provide balance.
Question 32
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 33
The newborn foot deformity seen in Figures 64a and 64b should initially treated with Review Topic

Explanation
Question 34
The patient undergoes hip arthroscopy and the image of the right hip is shown in Figure 39. Repair of the injured structure would be expected to improve
Explanation
The radiographic studies reveal both acetabular dysplasia and cam-type femoroacetabular impingement. The MR image shows an acetabular labral tear. Structural abnormalities of the hip, including femoroacetabular impingement, have commonly been identified in association with labral tears. Disruption of the ligamentum teres is not associated with impingement conditions in the absence of trauma.
The patient has acetabular dysplasia with a decreased lateral center-edge angle and also has visible cam-type femoroacetabular impingement. The common pathway for joint degeneration in hips with cam-type femoral head anatomy includes the development of cartilage damage in the anterior or superolateral aspects of the acetabular cartilage. Paralabral cysts may be seen more commonly in association with acetabular dysplasia, although the patient’s radiographs did not demonstrate substantial cystic changes. Osteochondral loose bodies and ligamentum teres ruptures can be seen at arthroscopy in a small number of cases.
There are several proposed roles of the acetabular labrum. It can increase the depth of the acetabular socket by as much as 21% to 28%. Roles of the acetabular labrum include joint lubrication, shock absorption, and pressure distribution. Recent studies assessing the effects of loading on joint stability for both normal and dysplastic hips did not demonstrate a substantial role of the labrum in differences in loading. Although joint stability might be improved following surgical repair, acetabular dysplasia is not likely to be resolved with acetabular labral repair alone.
RECOMMENDED READINGS
Tibor LM, Leunig M. The pathoanatomy and arthroscopic management of femoroacetabular impingement. Bone Joint Res. 2012 Oct 1;1(10):245-57. doi: 10.1302/2046-3758.110.2000105.PubMed: 23610655. View Abstract at PubMed
Peelle MW, Della Rocca GJ, Maloney WJ, Curry MC, Clohisy JC. Acetabular and femoral radiographic abnormalities associated with labral tears. Clin Orthop Relat Res. 2005 Dec;441:327-33. PubMed PMID: 16331022. View Abstract at PubMed
Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011 Jul;39 Suppl:72S-8S. doi: 10.1177/0363546511412320.
PubMed PMID: 21709035. View Abstract at PubMed
James SL, Ali K, Malara F, Young D, O'Donnell J, Connell DA. MRI findings of 37
femoroacetabular impingement. AJR Am J Roentgenol. 2006 Dec;187(6):1412-9. PubMed PMID: 17114529. View Abstract at PubMed
Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17. doi: 10.1007/s12178-009-9052-9. Epub 2009 Apr 7. PubMed PMID: 19468871. View Abstract at PubMed
Henak CR, Ellis BJ, Harris MD, Anderson AE, Peters CL, Weiss JA. Role of the acetabular labrum in load support across the hip joint. J Biomech. 2011 Aug 11;44(12):2201-6. doi: 10.1016/j.jbiomech.2011.06.011. Epub 2011 Jul 14. PubMed PMID: 21757198. View Abstract at PubMed
Question 35
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 36
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
Explanation
Cauda equina syndrome, typically the result of severe central canal stenosis in the lower lumbar region, often is caused by a large central disk herniation. Symptoms include severe back or leg pain, perineal numbness, possible motor weakness, and initial urinary retention followed by an overflow incontinence. When bowel or bladder deficits are present, this is considered a surgical emergency because successful recovery is most likely if decompression occurs within the first 48 hours.
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. View Abstract at PubMed
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
View Abstract at PubMed
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 37
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 38
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 39
A 76-year-old woman has longstanding right shoulder pain affecting overhead function. Figures A and B are her original radiographs. She undergoes reverse total shoulder arthroplasty (rTSA) with iliac crest bone grafting behind the baseplate and is discharged from the hospital the following day. She returns for follow-up at 2 weeks. The incisions have healed and she has minimal pain, which is improving. What is the most accurate description for the cause of failure? Review Topic

Explanation
Glenoid complications are the primary concern of rTSA. Historically, rTSA fail at the glenoid interface because of inadequate fixation. The Grammont-style prosthesis has a medialized center of rotation to circumvent this, but this lead to inferior scapular notching. Newer prosthesis include locking peripheral screws and 15° inferior tilt of the base plate. Further, changing the neck-shaft angle from 155 deg to 143 deg or 135 deg has reduced notching and instability, and reduced the need to for subscapularis repair.
Boileau et al. examined revision surgery for rTSA. They found that the most common cause for revision was prosthetic instability (48%). Humeral complications (loosening/derotation/fracture) were 2nd most common and infection was 3rd most common. Underestimation of humeral shortening and excessive medialization were common causes of recurrent prosthetic instability. Proximal humeral bone loss was found to be a cause for humeral loosening or derotation.
Holcomb et al. reviewed failure of the rTSA glenoid baseplate in 14 patients, which was defined as shift of the baseplate with or without screw breakage. Strategies for success include: (1) Incorporating increased inferior baseplate tilt in post-revision prosthesis-scapular neck angle (PSNA) compared to pre-failure PSNA because inferior tilt maximizes compressive force across the baseplate-glenoid interface. (2) Locking peripheral 5.0mm screws (rather than non-locking 3.5mm screws). (3) Using larger glenospheres to tighten the patulous soft tissue envelope and secure the glenoid allograft. Four patients required structural allograft (2 iliac crest, 2 femoral head).
Figures A shows Hamada 4A cuff tear arthropathy. Figure B shows severe static posterior instability of the humeral head and posterior Walch B2 erosion of the glenoid. Figure C shows the same patient treated with rTSA and iliac crest bone graft. Because of technical error, the central peg was not implanted in the native glenoid. Illustration A shows catastrophic failure of the glenoid baseplate. Illustration B shows the PSNA, with increase in the PSNA from initial rTSA to revision rTSA. Illustration C shows baseplate-glenosphere dissociation. Illustration D shows correction of technical error/too short peg with exchange to a baseplate with a longer peg. Illustration E shows and algorithm for treating unstable rTSA.
Incorrect Answers:
Question 40
.Figures 89a and 89b are the radiographs of an 18-year-old woman who has had elbow pain after falling on an outstretched hand. She is evaluated 5 days after the injury. Examination reveals the wrist is normal and her elbow has a limited arc of motion of 30 to 90 degrees of flexion/extension and 20 to 20 degrees of pronation and supination, with tenderness isolated to the lateral side of the elbow. What is the most appropriate treatment option?
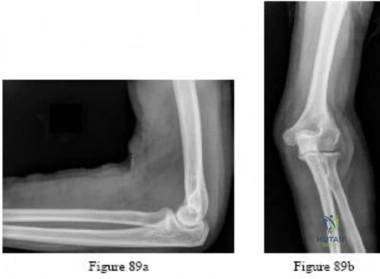
Explanation
Question 41
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?
Explanation
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non-neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.

Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Question 42
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them?
Explanation
REFERENCES: Shea KG: ACL Injury: Epidemiology and Prevention Presented at Sports Related Injuries in the Skeletally Mature Athlete. POSNA: One Day Course, 2008.
Millett PJ, Willis AA, Warren RF: Associated injuries in pediatric and adolescent anterior cruciate
ligament tears: Does a delay in treatment increase the risk of meniscal tears? Arthroscopy 2002; 18:955-959.
Question 43
A year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 44
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Morrey BF, Adams RA: Capitellocondylar total elbow replacement in rheumatoid arthritis. J Bone Joint Surg Am 1992;74:479-490.
Question 45
What part of the glenoid labrum has the least vascularity?
Explanation
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 46
A 69-year-old woman is seen in the emergency department with a bilateral C5-6 facet dislocation and complete quadriplegia after falling down a flight of stairs. After initial evaluation and treatment by the trauma service, she is moved to the intensive care unit. Examination reveals a blood pressure of 90/50 mm/Hg, a pulse rate of 50/min, a respiration rate of 12/min, and urine output of 1 mL/kg/h. Her hemodynamic status should be addressed by
Explanation
output suggests proper fluid resuscitation. Instead, she is bradycardic, possibly indicating neurogenic shock and loss of sympathetic tone to the heart. A Swan-Ganz catheter should be used to help differentiate these problems and guide appropriate fluid resuscitation and use of vasopressor agents.
REFERENCES: Hadley MN: Management of acute spinal cord injuries in an intensive care unit or other monitored setting. Neurosurgery 2002;50:S51-S57.
Vaccaro AR, An HS, Betz RR, et al: The management of acute spinal trauma: Prehospital and in-hospital emergency care. Instr Course Lect 1997;46:113-125.
Question 47
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 48
Which of the following statements best describes the typical early presentation of osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 49
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
Explanation
Question 50
What would be the advantage of surgery for the patient described in this scenario?
Explanation
The MR image of the lumbar spine postgadolinium contrast shows a ring-enhancing fluid collection. Ring-enhancing lesions within the spinal canal on postgadolinium MR images are indicative of epidural abscess. It is important to obtain a culture-specific diagnosis to inform the choice of antibiotics and educate patients regarding the likelihood of failure for standalone antibiotic therapy. Infection with MSSA, age younger than 65 years, the absence of neurologic deficit, and lumbar abscess location are all factors that point toward a patient being a reasonable candidate for a trial of culture-specific IV antibiotics. In this case, nafcillin is a suitable treatment for MSSA. The antibiotic should be initiated and closely observed with serial labs (WBC, ESR, CRP, repeat blood cultures) to ensure that the patient responds appropriately to therapy and that neurologic deficits do not develop. In the setting of epidural abscess, surgery is performed to evacuate the abscess and reverse or prevent neurologic deterioration. In the current scenario in which sepsis is not an issue, scant high-quality evidence shows that surgical intervention influences risk for mortality or chronic pain following epidural abscess.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
PubMed PMID: 24359002.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 51
03 A 13 y/o girl sustains the injury shown in Figures 69a and 69b in a fall. Examination reveals this to be an isolated injury, and the patient’s neurologic and vascular examinations are normal. Based on these findings, management should consist of
Explanation
pinning may be performed. If the articular surface shows that the fx line has extended into the joint and the articular surface is separated, open reduction and pinning are necessary. Once the fx is stabilized, the elbow is immobilized for 4 wks. The pins are then removed & motion is begun.
back to this question next question
Question 52
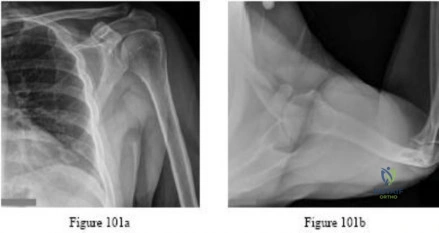
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?
Explanation
REFERENCES: Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23.
Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Oreck SL, Burgess A, Levine AM: Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption. J Bone Joint Surg Am 1984;66:758-763.
Question 53
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Rosenthal DI, Hornicek FJ, Wolfe MW, Jennings LC, Gebhardt MC, Mankin HJ: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 54
A 23-year-old man who is a competitive overhead athlete has shoulder pain. Based on the pathology shown in Figure 47, what treatment option would yield the highest satisfaction and return to overhead sports?
Explanation
REFERENCES: Snyder SJ, Karzel RP, Del Pizzo W, et al: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Altchek DW, Warren RF, Wickiewicz TL, et al: Arthroscopic labral debridement: A three-year follow-up study. Am J Sports Med 1992;20:702-706.
Question 55
Figures 28a and 28b show the posteroanterior and lateral radiographs of a 38-year-old woman with adult idiopathic scoliosis. She reports symptoms of long-standing lower back pain, progressive loss of height, and the inability to stand upright at the end of the day. What radiographic finding has been found to most closely correlate with symptoms of lower back pain? Review Topic

Explanation
Question 56
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended? Review Topic
Explanation
surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery.
Question 57
- Figures 42a and 42b show the sagittal and axial MRI scans of a 24-year-old patient who has sciatia. Which of the following combinations of physical findings is most consistent wit the MRI studies?
Explanation
Question 58
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 59
A 32-year-old male electrical worker complains of isolated left shoulder pain after a fall from 6 feet. Radiographs of the shoulder are seen in Figures A and B. The radiology technician was unable to obtain a good axillary view due to significant pain and muscle spasm. What would be the next most appropriate step in management? Review Topic
Explanation
Risk factors for posterior shoulder dislocation include epilepsy, electrocution and high-energy trauma. To make a diagnosis, standard views of the shoulder are required. These include an anteroposterior (AP) view, lateral scapular view and an axillary view. The axillary view is essential for diagnosis, but this requires the arm to be positioned in 20 - 30 degrees of abduction. If pain and muscle spasm restrict arm movement, the next most appropriate view would include a modified axially view,
such as a Velpeau view.
Robinson et al. reviewed posterior shoulder dislocations and fracture-dislocations. They state that apical oblique, Velpeau, or modified axial radiographs are preferable to other alternative axillary views, as they can be obtained with the arm in a sling. When an osseous injury is suspected, a CT scan and three-dimensional reconstruction can be useful in planning operative management.
Millet et al. wrote a JAAOS article on recurrent posterior shoulder instability. They state that 5 radiographic views, or advanced imaging, is essential to evaluate the shoulder. Characteristics to consider include, joint location, humeral head position, glenoid morphology (e.g., retroversion, hypoplasia, posterior glenoid rim), and impaction fracture of the humeral head.
Figure A and B show a normal shoulder radiograph with the shoulder positioned in internal rotation and external rotation. Illustration A shows the correct positioning of a patient to obtain a Velpeau view of the shoulder. Illustration B shows the correct positioning of a patient to obtain a Stryker notch view of the shoulder. This is used to asses for humeral head defects.
Incorrect Answers:
Question 60
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California
Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 61
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 62
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time? Review Topic
Explanation
Question 63
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 64
What is the most common behavioral effect of anabolic steroid use in athletes?
Explanation
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;19:667-689.
Question 65
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 66
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 67
A 22-year-old woman sustains the injury seen in Figure 12 as a result of a motor vehicle crash. What factor is most closely associated with development of osteonecrosis?

Explanation
(SBQ12TR.90) A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management? Review Topic

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam.
An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
30 mm Hg or persistently elevated absolute compartment pressures.. Answer 3: It would not be appropriate to leave this patient with impending compartment syndrome.
(SBQ12TR.57) A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on the available imaging, which of the following fracture characteristics best justifies this fixation choice?

Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on inter-fragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
congruity but does not dictate implant selection. Answer 3. Extension distal to the coronoid is an indication for plate fixation but there is no evidence of such extension on the radiograph shown Answer 4. This fracture is comminuted, without a distinct fracture line.
Question 68
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
REFERENCES: Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 69
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
REFERENCE: Johnson DC, Damiano DL, Abel MF: The evolution of gait in childhood and adolescent cerebral palsy. J Pediatr Orthop 1997;17:392-396.
Question 70
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
REFERENCES: Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Malicky DM, Kuhn JE, Frisancho JC, et al: Nonrecoverable strain fields of the anteroinferior glenohumeral capsule under subluxation. J Shoulder Elbow Surg 2002;11:529-540.
Question 71
A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?
Explanation
REFERENCES: Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Weigelt JA: Resuscitation and initial management. Crit Care Clin 1993;9:657-671.
Question 72
-What is the most appropriate next treatment step?
Explanation
Based on the patient’s signs and symptoms, the most likely diagnosis is osteomyelitis of the spine. The imaging studies do not reveal a herniated disk, which would be unusual in someone of this age. Aneurysmal bone cysts would involve the posterior elements with a more expansive lesion of bone, whereas this lesion involves primarily the body and anterior column. Hemangioma would likely not be present with systemic signs or symptoms and has a more characteristic coarse trabecular pattern on radiographs and scans. Given the likelihood that this patient has osteomyelitis of the spine, blood cultures may yield an organism about 50% of the time. If cultures are negative, an image-guided biopsy is warranted. A diagnosis needs to be established before treatment such as extension casting or bracing is rendered. Open biopsy may still be needed if needle biopsy is not diagnostic, but this is not the first treatment option. A chest CT scan is not appropriate as a first step when a tumor is presumed and a diagnosis has not been established.
Question 73
A 40-year-old man sustains a scapular body fracture after an all-terrain vehicle accident. Which of the following is the most commonly associated injury?
Explanation
Question 74
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic

Explanation
Question 75
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 76
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 77
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Rodriguez Merchan EC: Displaced fractures of the head and neck of the radius in children: Open reduction and temporary transarticular internal fixation. Orthopedics 1991;14:697-700.
Question 78
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of
Explanation
REFERENCES: DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994,
vol 3, pp 406-432.
Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Torg JS, Pavlov H, Morris VB: Salter-Harris type III fracture of the medial femoral condyle occurring in the adolescent athlete. J Bone Joint Surg Am 1981;63:586-591.
Question 79
In the arthroscopic photograph shown in Figure 5, the structure labeled “A” functions primarily as a restraint to translation of the humeral head in what direction?
Explanation
REFERENCES: Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Owen MD, Kregel KC, Wall PT, Gisolfi CV: Effects of ingesting carbohydrate beverages during exercise in the heat. Med Sci Sports Exerc 1986;18:568-575.
Question 80
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 81
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no

Explanation
Question 82
A 35-year-old construction worker continues to have weakness with lifting overhead 2 years after he was treated with physical therapy for a "chest muscle" tear. An obvious deformity noted in his axilla worsens with resisted extension and adduction. A clinical photograph and MRI scan are shown in Figures 119a and 119b. What is the most appropriate treatment? Review Topic
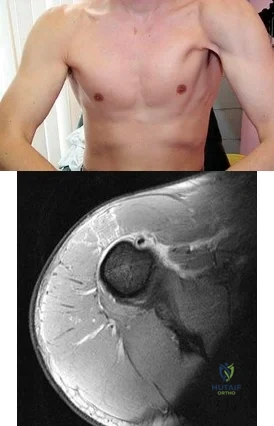
Explanation
Question 83
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 84
Endurance training primarily involving aerobic activities results in which of the following muscular adaptations? Review Topic
Explanation
Question 85
Which of the following injuries is most likely associated with the fracture seen in Figure A?

Explanation
Soft tissue pathology is common in tibial plateau fractures. In general, fractures that are largely displaced and/or a result of high energy trauma are more likely to have associated soft tissue pathology. A majority of meniscal injuries that occur in the setting of tibial plateau fractures are meniscocapsular detachments. This has important implications for healing (more reliable healing in the vascular zone). Additionally, the meniscus usually remains in close contact with the femoral condyle, while the tibial plateau widens around it. It is generally agreed upon that meniscal tears should be repaired, if possible, at the time of internal fixation to decrease the likelihood of
postraumatic arthritis.
Gardner et al. review 62 patients with Schatzker II tibial plateau fractures that had an MRI preoperatively. For displaced fractures, the incidence of lateral meniscal tears was 83%, while the incidence of lateral collateral and posterior cruciate ligament injuries was 30%.
Ringus et al. attempted to determine if the degree of lateral tibial plateau fracture depression on computed tomography (CT) images predicted the presence of lateral meniscus tears. Fractures with > 9mm depression had an eight-fold increase in lateral meniscal tears, and those younger than 48 years-old had a four-fold increase in lateral meniscal tears.
Illustration A shows an MRI of a Schatzker II tibial plateau fracture with a lateral meniscal detachment and a medial meniscal tear. Illustration B shows the Schatzker Classification, I-VI.
Incorrect Answers:
Question 86
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
Question 87
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 88
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 89
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
REFERENCES: Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Berenson JR, Lichtenstein A, Porter L, et al: Efficacy of pamidronate in reducing skeletal events in patients with advanced multiple myeloma: Myeloma Aredia Study Group. N Engl J Med 1996;334:488-493.
Question 90
A 35-year-old man with a history of spine surgery 5 years ago reports the recent development of frequent low back pain radiating to the legs. The patient blames a low-energy fall that occurred 9 months ago for the recent symptoms. Radiographs reveal previous interbody fusions of L4-L5 and L5-S1, with hardware present. The vertebrae appear well-fused and stable. What is the most likely cause of the low back pain? Review Topic
Explanation
Question 91
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 92
A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of
Explanation
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 93
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
Explanation
REFERENCES: Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 94
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 95
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
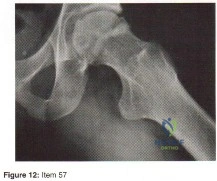
Explanation
Question 96
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies? Review Topic
Explanation
Question 97
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Explanation
REFERENCES: Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
McHenry CR, Piotrowski JJ, Pentrinic D, Malangoni MA: Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995;221:558-563.
Question 98
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 99
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
REFERENCES: Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Jobe CM: Gross anatomy of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 49-66.
Question 100
- An otherwise healthy 65-year-old man has had chronic pain in his prosthetic knee for the past 9 months. Repeated aspirations reveal a coagulase-negative staphylococcus infection. To eradicate the infection while maintaining the best possible joint function, management should consist of
Explanation
Present recommendations are to avoid a one-stage reconstruction in a patient in whom a glycocalyx elaborating microorganism has been isolated. In one study 52% of the isolates of S. epidermidis and 28% of the isolates of S. aureus elaborated glycocalyx. The microbiology laboratory can be asked to determine if the microorganisms elaborate glycocalyx. In the present case it should be assumed that the staphylococci elaborate glycocalyx and are resistant to antibiotics. A two-stage procedure is indicated for these reasons alone.
Antibiotic therapy alone has been used for a select group of patients who could not medically tolerate either a one-stage or a two-stage arthroplasty. The patient in this case is listed as otherwise healthy.
The decision to perform a resection arthroplasty as a definitive procedure without reimplantation is based on the bacteria’s resistance to antibiotics, quality of the local soft tissues, the complexity of the reconstruction, the patient’s refusal to have another operation, the patient’s overall health, or a combination of these factors. None of which appear to be present in this case.
