Orthopedic Surgery Board Review MCQs: Spine, Deformity & Trauma | Part 131
Key Takeaway
This page offers Part 131 of a comprehensive Orthopedic Surgery board review. It features 100 high-yield, verified MCQs in OITE/AAOS format, designed for orthopedic surgeons and residents preparing for their certification exams. Utilize study and exam modes for effective preparation.
About This Board Review Set
This is Part 131 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 131
This module focuses heavily on: Deformity, Scoliosis, Spine, Trauma, Wrist.
Sample Questions from This Set
Sample Question 1: A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. Th...
Sample Question 2: Etanercept modifies the natural history of inflammatory arthropathies through what mechanism?...
Sample Question 3: A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of...
Sample Question 4: A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Sta...
Sample Question 5: Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.
REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.
Question 2
Etanercept modifies the natural history of inflammatory arthropathies through what mechanism?
Explanation
Question 3
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing’s sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon M, Springfield D, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 4
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 5
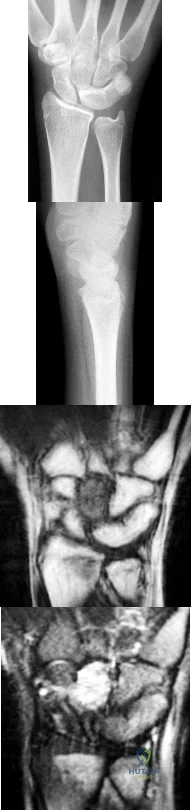
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 6
An 83-year-old woman with diabetes mellitus has a history of recurrent infection over the medial aspect of her great toe and has had a painless bunion for the past 45 years. Shoe wear modifications have failed to provide relief. Pedal pulses are palpable. Figures 30a and 30b show the clinical photograph and radiograph. Management should now consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 123-134.
Abidi NA, Conti SF: The clinical and radiographic anatomy of hallux valgus and surgical algorithm. Foot Ankle Clin 1997;2:599-626.
Question 7
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?
Explanation
Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents.
The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve.
REFERENCES: Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Salter RB, Harris WR: Injuries involving the epiphyseal plate. J Bone Joint Surg Am 1963;45:587-622.
Question 8
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter “A”?
Explanation
REFERENCES: Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 400, 405, 407, 450.
Question 9
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
REFERENCES: Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Morrissy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 579-624.
Question 10
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Explanation
REFERENCES: Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 11
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
REFERENCE: Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 12
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
Explanation
REFERENCES: Kreig JC, Mohr M, Ellis TJ, et al: Emergent stabilization of pelvic ring injuries by controlled circumferential compression: A clinical trial. J Trauma 2005;59:659-664.
Croce MA, Magnotti LJ, Savage SA, et al: Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg 2007;204:935-942.
Routt ML Jr, Falicov A, Woodhouse E, et al: Circumferential pelvic antishock sheeting:
A temporary resuscitation aid. J Orthop Trauma 2002;16:45-48.
Question 13
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of Review Topic

Explanation
Question 14
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
Explanation
REFERENCES: Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
Wright JL, Nathans AB, Rivara FP, et al: Specific fracture configurations predict sexual and excretory dysfunction in men and women 1 year after pelvic fracture. J Urol 2006;176:1540-1545.
Question 15
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
REFERENCES: Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury afterknee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 16
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 17
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks?

Explanation
Question 18
The spring ligament of the foot connects what two bones?
Explanation
REFERENCES: Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Davis WH, Sobel M, DiCarlo EF, et al: Gross, histological and microvascular anatomy and biomechanical testing of the spring ligament complex. Foot Ankle Int 1996;17:95-102.
Question 19
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 20
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 21
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 22
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management? Review Topic

Explanation
Question 23
Pedicle subtraction osteotomies (PSO) are commonly performed in the lumbar spine to treat sagittal imbalance. What is the most common complication following a PSO in the lumbar spine? Review Topic
Explanation
Question 24
A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 25
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?
Explanation
REFERENCES: O’Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118.
Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
McDaniel WJ Jr, Dameron TB Jr: The untreated anterior cruciate ligament rupture. Clin Orthop 1983;172:158-163.
Question 26
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
REFERENCES: Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Tohmeh AG, Mathias JM, Fenton DC, et al: Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine 1999;24:1772-1776.
Question 27
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Explanation
Question 28
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 29
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
Question 30
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH: Experience in the surgical mangement of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 1998;88:623-633.
Question 31
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
REFERENCES: Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 32
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 33
Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic
Explanation
Question 34
A 24-year-old professional male soccer player has lower abdominal pain on exertion. He has pain with resisted hip adduction and with sit-ups. There is no palpable inguinal hernia with a Valsalva maneuver. Nonsurgical management has failed to provide relief. After ruling out malignancies, what is the next most appropriate step in management? Review Topic
Explanation
Question 35
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 36
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?
Explanation
REFERENCES: Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Mimaston MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601.
Question 37
A 30-year-old man sustained an acute injury to his left shoulder while lifting weights. He reports pain with abduction and external rotation of the shoulder, and he has weakness with internal rotation. Inspection shows loss of contour of the axillary fold. Definitive management should consist of Review Topic
Explanation
Question 38
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
Explanation
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.

CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
Question 39
A 72-year-old female presents to your office with a 24-month old painful nonunion of a 3-part fracture of the proximal humerus. She has been treated conservatively with range of motion exercises but continues to complain of debilitating pain and dysfunction. Operative management should include:

Explanation
The referenced article by Cheung et al reviews treatment options for proximal humeral nonunions and reports successful use of arthroplasty in treating elderly osteoporotic proximal humeral nonunions as a pain relieving procedure.
Dines reported a case series of 20 chronic post-traumatic proximal humerus fractures including nonunions that were treated with shoulder arthroplasty achieving fair to excellent results in 90% at mid-term follow-up
Question 40
Anterior approach
Explanation
The nerve most commonly injured in the posterior approach to the hip is the sciatic nerve. Overall injury prevalence is 1% to 2%. This nerve is more commonly injured in cases of hip dysplasia with excessive leg lengthening. The superior gluteal nerve is at highest risk with the direct lateral approach to the hip. This nerve courses in the gluteus medius muscle and is
at risk when splitting the muscle 5 cm proximal to the greater trochanter. The lateral femoral 73
cutaneous nerve is commonly damaged with anterior total hip replacement surgery. Neuropraxia has been reported in 81% of patients. The inferior gluteal nerve travels from the greater sciatic notch and enters the gluteus maximus muscle. It is at risk when the posterior approach to the hip is used.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia.
PA: Lippincott Williams & Wilkins; 2003:365-453.
DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. View Abstract at PubMed
Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010 Sep;468(9):2397-404. doi: 10.1007/s11999-010-1406-5. PubMed PMID:
Question 41
Examination of a carpenter who hit his thumb with a hammer reveals that the nail plate is broken but in place, and there is a 100% subungual hematoma that covers 100% of the area under the nail plate. Radiographs reveal a comminuted distal phalangeal tuft fracture. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Zook EG, Guy RJ, Russell RC: A study of nail bed injuries: Causes, treatment, and prognosis. J Hand Surg Am 1984;9:247-252.
Question 42
One advantage of using onlay strut allograft in femoral revision surgery is that it can
Explanation
REFERENCES: Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44.
Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Head WC, Emerson RH Jr, Malinin TI: Structural bone grafting for femoral reconstruction. Clin Orthop 1999;369:223-229.
Question 43
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple times between 1 week and 2 years after surgery.
Question 44
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5° to 55° of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
REFERENCE: Esler CN, Lock K, Harper WM, Gregg PJ: Manipulation of total knee replacements: Is the flexion gained retained? J Bone Joint Surg Br 1999;81:27-29.
Question 45
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
REFERENCE: Cooper JR, Dowson D, Fisher J, Jobbins B: Ceramic bearing surfaces in total articular joints: Resistance to third body damage from bone cement particles. J Med Eng Technol 1991;15:63-67.
Question 46
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?
Explanation
REFERENCES: Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Chen BH, Natarajan RN, An H, Andersson GB: Comparison of biomechanical response to surgical procedures used for cervical radiculopathy: Posterior keyhole foraminotomy versus anterior foraminotomy and discectomy versus anterior discectomy with fusion. J Spinal Disord 2001;14:17-20.
Question 47
Figure 16 shows the MRI scan of a 43-year-old man who has had worsening low back pain for the past 4 months. What is the most likely diagnosis?
Explanation
REFERENCES: Boachie-Adjei O, Squillante RG: Tuberculosis of the spine. Orthop Clin North Am 1996;27:95-103.
Currier BL, Eismont FJ: Infections of the spine, in Rothman RH, Simeone FA (eds): The Spine. Philadelphia, PA, WB Saunders, 1992, p 2614.
Question 48
A 36-year-old woman reports vague right shoulder pain. She denies any previous shoulder problems or any recent trauma. MRI scans are shown in Figures 81a and 81b. Weakness of which of the following is the most likely finding in her physical examination? Review Topic
Explanation
Question 49
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 50
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
Explanation
REFERENCES: Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.
Matta JM: Operative treatment of acetabular fractures through the ilioinguinal approach:
A 10-year perspective. Clin Orthop Relat Res 1994;305:10-19.
Question 51
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1132-1133.
Question 52
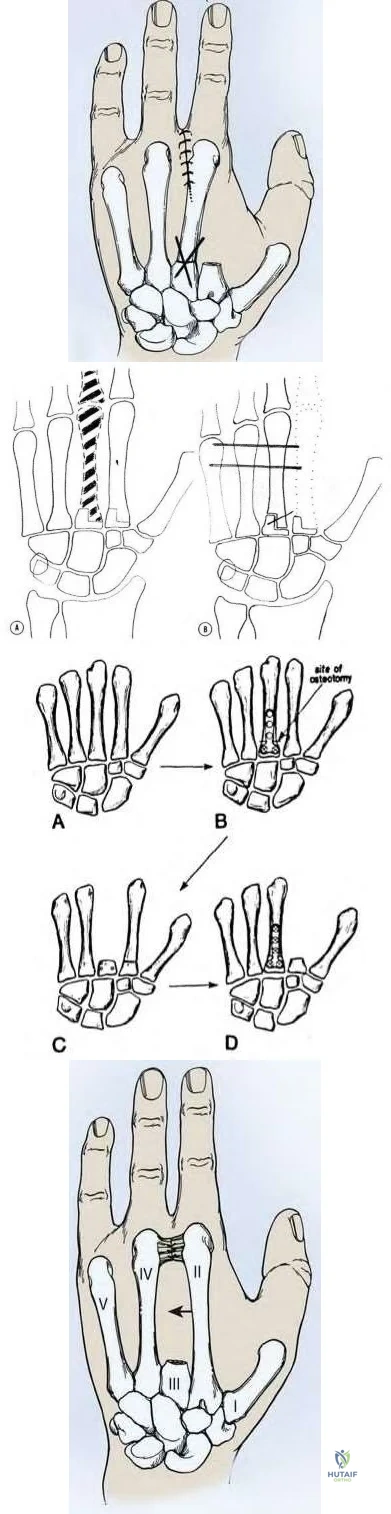
5cm from the carpometacarpal joint. The attached deep transverse intermetacarpal ligaments are sacrificed. To prevent scissoring of the remaining digits and small objects falling through the gap between index and ring fingers, which of the following procedures should be performed?

Explanation
With amputation of the middle or ring metacarpals, small objects fall through the gap and the adjacent fingers scissor. For single central ray defects, techniques to reduce the gap include transposition of the index finger (for middle ray amputation), small finger (for ring ray amputation), complete removal of the metacarpal (without leaving a proximal metacarpal base stump) to allow the bases of index and ring metacarpals to migrate together and reconstruction of the deep transverse metacarpal ligament. The technique of index transposition may vary depending on the osteotomy (straight vs step-cut) and fixation (K wires vs plate) as seen in the illustrations below.
Muramatsu et al. describe bony transposition for reconstruction after ray amputation for malignancy. The advantage is immediate closure of the space. The disadvantages include prolonged postoperative immobilization until union, malrotation (leading to scissoring), mal-tension of tendon (because of different metacarpal heights), and delayed or nonunion.
Lyall et al. advocate total middle ray amputation. They believe that leaving the metacarpal base behind leads to difficulty in aligning the adjacent rays as the index and ring must angulate over the bony obstruction to close the distal gap, leading to scissoring. They believe that index transposition leaves an abnormally wide 1st web space and a remnant 2nd metacarpal stump that can protrude dorsally.
Figure A is an AP radiograph of the right hand showing a destructive lesion of the proximal phalanx of the middle finger abutting the metacarpophalageal joint. Figure B is a STIR coronal MRI image showing the tumor mass extending into surround soft tissue. Illustration A is a diagram showing index transposition for middle ray amputation using a straight osteotomy and crossed K-wires. Illustration B is a diagram showing index transposition using a step-cut osteotomy and multiple K-wire fixation to the adjacent metacarpals. Illustration C is a diagram showing index transposition using a straight osteotomy and plate fixation. Illustration D is a diagram showing an alternative technique of suturing deep transverse metacarpal ligaments together to close the gap.
Incorrect Answers
A 65-year-old man fell and injured his right wrist. Radiographs taken in the emergency room are seen in Figure A. He was treated as a sprain and no further follow-up was planned. He sustained 2 minor falls over the next 6 years and his wrist pain recurred. Recent radiographs are seen in Figure B. Surgical treatment that will best address his symptoms and preserve wrist motion consists of

Anterior and posterior interosseous neurectomy
Scaphotrapezialtrapezoidal (STT) fusion
Complete wrist arthrodesis
Proximal row carpectomy
Four-corner fusion with scaphoidectomy
Four-corner fusion with scaphoidectomy is indicated for Stage III SLAC wrist.
Surgical treatment of SLAC wrist is stage dependent. Stage I disease (scaphoid-radial styloid arthritis) is treated with AIN/PIN neurectomy. This procedure can also be done in addition to other bony procedures for Stages II-III disease. Stage II (scaphoid-entire scaphoid facet) is treated with PRC or scaphoid excision with 4-corner fusion (4CF). Stage III (capitolunate arthritis with proximal migration of the capitate into the scapholunate interval) is treated with either scaphoidectomy with 4CF or total wrist fusion.
Some other conditions exist: If capitolunate arthritis exists, PRC is contraindicated and 4CF is performed. If radiolunate arthritis exists, both PRC and 4CF are contraindicated and total wrist fusion is performed. If both radiolunate and capitolunate surfaces are preserved, then either PRC or a 4CF may be performed.
Cohen et al. compare PRC with 4-corner fusion plus scaphoid excision. PRC is technically easier, but leads to shortening of the carpus with weakness and incongruity exists between the capitate and lunate fossa of the distal radius. Scaphoid excision and four-corner fusion maintains carpal height and preserves the radiolunate relationship, but is more technically demanding, there is risk of nonunion, and it requires longer postop immobilization. Pain relief is more reliable following 4-corner fusion.
Figure A shows scapholunate ligament disruption. Figure B shows late stage SLAC wrist. There is capitolunate arthritis but no radiolunate arthritis.
Illustration A shows an example of PRC. Illustration B shows an example of 4CF and scaphoidectomy.
Incorrect Answers

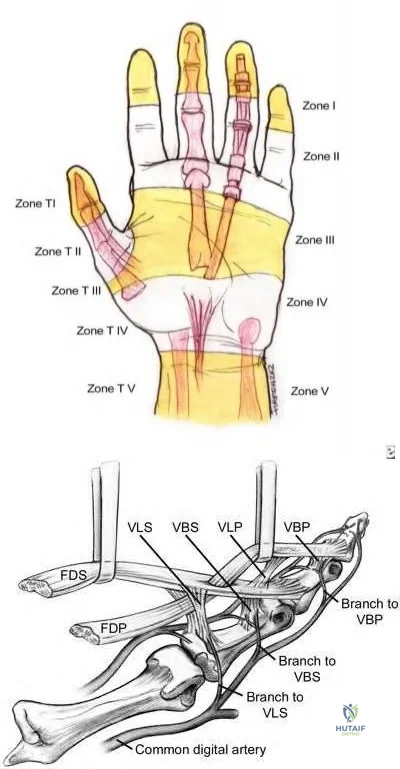
Which of the following statements is true regarding zone II flexor tendon injuries?
At this level, FDS and FDP are located within separate tendon sheaths
FDS repair has not been shown to improve outcomes
Improved gliding is seen with repair of 1 slip of FDS compared to repairing both slips
Repairing FDS does not affect post-operative digit strength
FDP repair has not been shown to improve outcomes
In zone II flexor tendon injuries, repairing only one slip of FDS has been shown to improve gliding when compared to repair of both slips.
Zone II flexor tendon injuries have notoriously had poor outcomes secondary to high rates of adhesion formation at the pulleys. However, new advances in post-operative rehabilitation have significantly improved outcomes to the point where it is no longer considered "no man's land." Management of the FDS has been a source of controversy. In the past, the FDS was occasionally excised to theoretically make more room for the FDP. This has now been largely abandoned and the FDS is repaired whenever possible. Whether or not to repair both slips of FDS remains controversial, with in vitro data suggesting that gliding resistance is improved if only one slip is repaired.
Zhao et al. review the effect of partial vs. complete FDS excision following repair of FDP for zone II flexor tendon injuries. Preserving the whole FDS resulted in a significantly larger increase in gliding resistance after FDP repair than did full or partial FDS removal, which were not significantly different from each other.
Illustration A shows the zones of flexor tendon injury. Note that zone II injuries occur between the FDS insertion and the distal palmar crease. Illustration B shows the anatomy of the flexor tendons in detail. Video V shows a technique for repair of zone II injuries.
Incorrect Answers:
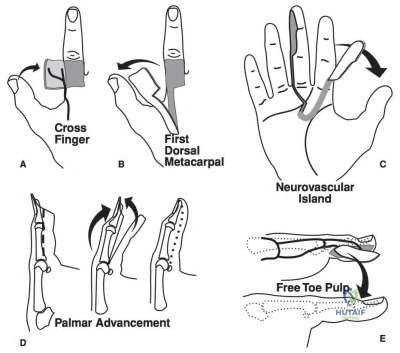
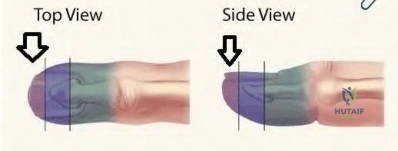
A 6-year-old girl sustains transverse amputations through her long and ring fingertips after getting her hand caught in a lawn mower. She presents to the emergency room 30 minutes after the injury with the amputated tissue which was placed on ice in a waterproof bag. On physical exam the amputation levels are found to be 6 millimeters distal to the lunula. The wounds are noted to be fairly
contaminated with no evidence of exposed bone. Skin defects are less than 1 centimeter. Which of the following is the most appropriate management at this time?
Emergent replantation of the amputated parts
Revision amputation through the distal interphalangeal joint
Thorough irrigation and debridement followed by elective Moberg advancement flaps
Thorough irrigation and debridement followed by elective Z-plasty reconstruction
Thorough irrigation and debridement, soft dressing application, and followup within 1 week
Distal fingertip amputations can be successfully managed with local wound care and healing by secondary intention if no bone is exposed and the soft tissue defects are minimal. This is especially true in the pediatric population.
Distal fingertip amputations are common injuries seen in the emergency department. If bone is not exposed, the wounds can be successfully treated with local wound care and dressing changes, followed by soaks in a hydrogen-peroxide solution after 7-10 days. Some controversy exists in the pediatric population if the soft tissue loss is > 1 cm, with options for management including a V-Y advancement flap or conservative management with dressing changes.
Quell et al. review the results of 82 patients with fingertip amputations treated conservatively; 31 of the digits were treated with primary closure with or without shortening of bone and 54 digits were treated with semiocclusive dressings. No complications were observed, and all healed fingertips were well padded and painless.
Tupper et al. review sixteen patients with twenty fingertip injuries who underwent V-Y plasty for transverse fingertip amputations. Sensitivity was 73% of normal, with eight patients reporting hypersensitivity. Contrary to popular belief, they believe normal sensation following a V-Y plasty is not a reasonable expectation.
Illustration A shows the three levels of fingertip amputations. Zone I is distal to the phalanx; Zone II is distal to the lunula; and Zone III is proximal to the lunula.
Incorrect Answers:
Which of following malformations is most commonly associated with Poland's syndrome?

Figure E CORRECT ANSWER: 4
Figure D demonstrates symbrachydactyly which is most commonly associated with Poland's syndrome.
Poland's syndrome is a rare birth defect characterized by underdevelopment or absence of the chest muscle in conjunction with ipsilateral symbrachydactyly. Poland syndrome most often affects the right side of the body, and occurs more often in males than in females.
Ireland et al. reviewed 43 consecutive cases of Poland's syndrome, and reviewed the relevant literature up to that point. The authors state that the clinical features are variable but always include congenital aplasia and syndactyly, and the right side is affected more than the left. They also note that although the hand remains hypoplastic and functional capacity is limited by the inherent skeletal anomalies, surgical treatment improves functional capacity and cosmetic appearance in the majority of patients.
Van Heest summarizes normal formation and growth of the upper limb as a basis for understanding malformation, with the goal of providing a basic understanding of the evaluation necessary for appropriate counseling and referrals for treatment of the child with hand and upper extremity congenital deformities.
Incorrect Answers:
A 55-year-old male laborer comes in with a chief complaint of clumsiness with his right hand for the past 3 months including difficulty using a hammer while at work. He has had no injury to the right upper extremity. On physical examination, he has persistent small finger abduction/extension with finger extension and active adduction. An EMG is performed and demonstrates ulnar nerve conduction velocities of 31 m/sec (normal >52m/sec). The patient symptoms are most accurately described as:
Axonotmesis with ischemia origin
Axonotmesis with myelin disruption
Neurapraxia with ischemia origin
Neurapraxia with endoneurium disruption
Neurotmesis CORRECT ANSWER: 3
The history and clinical presentation are consistent with ulnar entrapment neuropathy at the level of the cubital tunnel. This would be classified as a neuropraxia with ischemia origin.
Compression injuries to the peripheral nerves are often the result of microvascular dysfunction as the nerves traverse a high to low pressure gradient. Peripheral nerve injury can be classified as neuropraxia, axonotmesis, and neurotmesis. Compressive neuropathies are typically neuropraxias, with local myelin damage but not compromise of the major components of the nerve. In axonotmesis, there is Wallerian degeneration and myelin loss distal to the site of injury. The most severe type is that of neurotmesis. Neurotmesis is composed of a spectrum of injury in which the endoneurium is always disrupted (perineurium or epineurium may be intact). The worst form of neurotmesis is that of nerve transection.
Elhassan et al. review the pathophysiology of cubital tunnel syndrome. They report nerve dysfunction results from ischemic changes secondary to compression. Compressive effects on the nerves can last greater than 24 hours, even after the source of compression has been removed.
Rempel et al. review the pathophysiology of peripheral nerve compression syndromes. The authors indicate that deforming pressures to nerves are often the result of stenotic soft tissue canal boundaries. This leads to interference with local microvasculature of the nerve itself.
Illustration A demonstrates the Wartenberg sign, where the patient has persistent small finger abduction/extension resulting from weakness of the 3rd palmar interosseous/small finger lumbrical.
Illustration B reveals clawing which results from overpowering of the intrinsic muscles by the extrinsic muscles; a tenodesis effect results in flexion of the PIP/DIP joints. This is more severe in ulnar nerve compression at Guyon’s canal. Illustration C shows the Froment sign, where the FPL attempts to compensate for a deficient pinch, because of weakness of the adductor pollicis. Illustration D demonstrates atrophy of the 1st dorsal webspace from chronic compressive changes. Illustration E demonstrates atrophy of the thenar compartment which is consistent with carpal tunnel syndrome.
Incorrect Answers:
Which of the following hand injuries seen in Figures A-E is most appropriately treated with a first dorsal metacarpal artery flap?

Figure E CORRECT ANSWER: 3
Figure C shows a dorsal thumb laceration with exposed tendon that would be most appropriately treated with a first dorsal metacarpal artery (FDMA) flap.
The first dorsal metacarpal artery is a branch of the radial artery that supplies the dorsal hand skin from the thumb metacarpal to the long metacarpal, as well as the skin on the dorsal surfaces of the thumb and index to the proximal interphalangeal joint. The flap is raised distal to proximal as an island flap containing the FDMA, branches of the radial nerve, fascia of the underlying interosseous muscle of the first web space, and skin overlying the MP joint and proximal phalanx of the finger. It is an excellent option for large soft tissue defects on either side of the thumb. In this case, skin grafting is contraindicated because of exposed tendon without paratenon.
Sherif et al. detail the anatomy of the first dorsal metacarpal artery. They found three consistent branches, including the radial, ulnar, and intermediate branch. In part II of their study, they review the results of 23 patients where the FDMA flap was used as a fasciocutaneous or fascial flap for the coverage of soft tissue hand defects.
Illustration A shows a FDMA flap being raised for coverage of a thumb defect. Incorrect Answers:
bone can be allowed to heal through secondary intention.

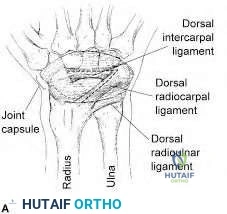
Figure A is a radiograph of a 35-year-old women who sustained an isolated left wrist injury after a fall onto an outstretched hand. She has been complaining of left dorsal wrist pain since the fall. Examination reveals a positive Watson's scaphoid shift test. What ligamentous structure is an important secondary stabilizer to prevent dorsal intercalated segment instability (DISI) deformity in this patient?

Transverse carpal ligament
Dorsal intercarpal ligaments
Triangular fibrocartilage complex
Dorsal lunotriquetral ligament
Volar lunotriquetral ligament
The integrity of the dorsal intercarpal ligaments is important in preventing dorsal intercalated segment instability (DISI) deformity and persistent scapholunate instability.
Scapholunate instability is the most common carpal instability. The primary stabilizing structure of the scaphoid and lunate bones is the scapholunate ligament, which is commonly injured with a fall on an outstretched hand.
Secondary stabilizers of the scaphoid and lunate include the dorsal intercarpal ligaments and the dorsal radiocarpal ligaments. Failure to recognize injury of these structures can cause persistent dorsal intercalated segment instability (DISI). This can predispose patients to a SLAC wrist and early wrist osteoarthritis.
Mitsuyasu et al. examined the role of dorsal intercarpal ligaments (DIC) in scapholunate instability. They showed that the DIC had an important role in stabilizing the scaphoid and lunate bones with static and dynamic movements. The authors of this study suggest that the DIC ligament should be assessed intraoperatively and consideration should be given to repair and/or reconstruction with surgical management of scapholunate ligament tears.
Viegas et al. showed that the dorsal intercarpal and the dorsal radiocarpal ligaments form a lateral V configuration over the dorsal wrist. This configuration acts as an indirect dorsal stabilizing effect on the scaphoid
throughout the range of motion of the wrist. Their integrity acts to ensure normal wrist kinematics.
Figure A shows an AP and lateral radiograph of the left hand. There is significant gapping between the scaphoid and lunate articulation. This is indicative of a complete scapholunate dissociation, however both wrists should be imaged as this deformity may exist without injury. Illustration A shows the anatomy of the dorsal intercarpal and the dorsal radiocarpal ligaments.
Incorrect Answers:
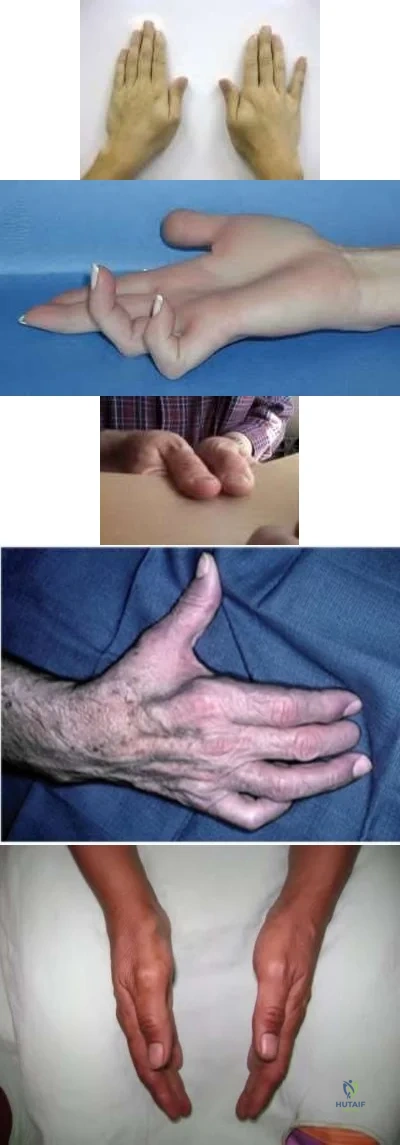
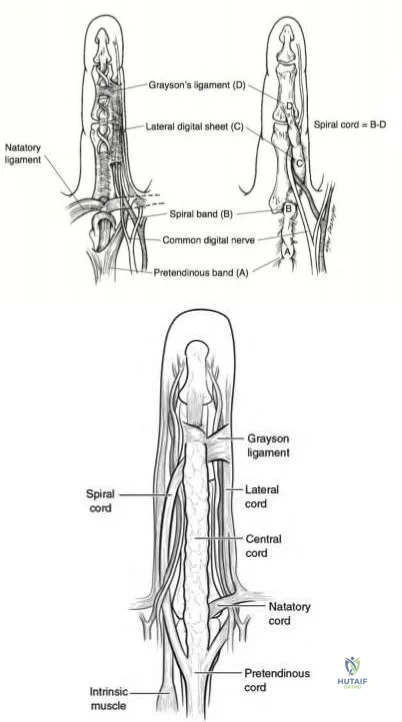
A 50-year-old patient presents with stiffness in her hand. A clinical photo is shown in Figure A. During surgical exposure, the neurovascular bundle is identified and dissected. What is the clinically most important pathologic structure to identify and what is its location relative to the neurovascular bundle in the digit?

Spiral cord which is central and superficial to the neurovascular bundle
Central cord which is midline and superficial to the neurovascular bundle
Retrovascular cord which is central and superficial to the neurovascular bundle
Spiral cord which is lateral and deep to the neurovascular bundle
Central cord which is lateral and deep to the neurovascular bundle
Based on clinical findings, the patient has evidence of Dupuytren’s contracture affecting her ring finger. Relative to the neurovascular bundle, the spiral cord will lie lateral and deep.
Dupuytren’s disease is a benign hand condition characterized by pathologic nodules and cords of existing fascial bands. The most clinically relevant structure in Dupuytren's disease, is the spiral cord. The spiral cord is the result of pathology of 4 structures: the middle layer of the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. The spiral cord is found predominantly at the palmodigital transition. The spiral cord displaces the neurovascular bundle centrally and superficially.
Benson et al. review the etiology, pathophysiology and treatment options for Dupuytren’s contracture. They highlight that while the pretendinous band is located volar and central to the neurovascular bundle in the palm, the spiral band and lateral digital sheath cause the neurovascular bundle to be displaced superficially and volarly as they become pathologically affected.
Black et al. review the pathoanatomy, diagnosis and management of Dupuytren's disease. They note that the spiral cord lies superficial to the neurovascular bundle proximal to the MCP joint. Distal to the MCP joint it passes deep to the bundle. At that location, the spiral cord lies lateral to the
neurovascular bundle as the lateral digital sheet becomes involved
Figure A demonstrates the cord formation that is characteristic of the pathologic Dupuytren’s condition. It is the central cord that causes contracture of the MCP, whereas the retrovascular and spiral cords cause contractures of the DIP and PIP respectively. Illustration A shows the relationship of spiral cord formation in Dupuytren's disease relative to the normal anatomy of the palmar fascia. The structures implicated in the formation of the spiral cord are the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. Cleland's ligament, more dorsally located, is spared in Dupuytren's disease. The neurovascular bundle is displaced superficially and towards the midline, as the pathological cord spirals around. Illustration B shows the presence of other affected structures, including the natatory ligament and the central band. The central band is an extension of the pretendinous cord and attaches to the base of the middle phalanx. It may insert onto the tendon sheath of the flexor tendon at this level. Formation of natatory cords cause webspace contractures. Formation of central cords lead to flexion contractures of the PIP. Illustration V is a video that provides an educational overview of Dupuytren's.
Incorrect Answers:
An infant is brought to your office for evaluation of his hands. Clinical photos are shown in Figures A and B. The clinical features are most consistent with a genetic mutation in which of the following:

Sonic Hedgehog (SHH)
FGFR2
FGFR3
PMP22
COL1A1 CORRECT ANSWER: 2
Based on the clinical features seen in the figures provided, the most likely syndrome is that of Apert syndrome, which is consistent with a mutation in FGFR2.
Apert syndrome is an autosomal dominant condition that gives rise to facial dysmorphism and complex syndactyly of the hands. The craniosynostosis that develops causes flattening of the skull and facial features.
Goldberg et al review congenital hand conditions and the malformations associated with them. They indicate that not only does identification allow for natural history to be better elucidated, but also timing of surgical intervention can be better gauged.
Figures A and B demonstrate clinical features consistent with Apert Syndrome. The “rosebud” hand is a complex syndactyly that affects the index, middle and ring fingers most commonly. Hypertelorism is exemplified with increased distance between the eyes; additionally, acrocephaly is noted with forehead broadening and skull flattening.
Incorrect Answers
1: Mutation in sonic hedgehog gene (SHH) is associated with a longitudinal deficiency of the radius. This is seen in conditions like TAR, Holt-Oram and VACTERL syndromes.
3: Mutation in FGFR3 leads to achondroplasia
4: Mutation in PMP22 gives rise to Charcot Marie Tooth syndrome 5: Mutation in COL1A leads to osteogenesis imperfecta
A 45-year-old patient presents with recurrence of radial sided wrist pain after undergoing a first dorsal compartment release about 3 months ago. The surgery was completed by one of your partners; operative reports indicate that the sheath was incised on the dorsal edge. On physical exam she is found to have normal appearing skin, a negative Tinel’s sign, and a positive Finklestein test. What is the most likely cause of the recurrence of her symptoms?
Development of neuroma
Complex regional pain syndrome
Failure to decompress the EPB sub-sheath
Failure to decompress the EPL sub-sheath
Failure to decompress the APB sub-sheath
Based on the history and clinical findings this patient has de Quervain’s tenosynovitis. The recurrence of her symptoms can be attributed to a failure to recognize and decompress the EPB sub-sheath.
De Quervain’s tenosynovitis is a stenosing inflammatory condition of the first dorsal compartment of the wrist (APL/EPB). Surgical release of the compartment is indicated after conservative measures have failed. At the time of the operation, the incision is made on the dorsal side of the sheath to prevent volar subluxation of the tendons. Failure to identify and release a distinct EPB sub-sheath or a separate fibro-osseous compartment of the APL can lead to a recurrence of symptoms.
Alegado et al. report a case of a patient with dysesthesias in the superficial radial nerve distribution 3 months after undergoing first dorsal compartment release for de Quervain’s tenosynovitis. They found a persistent fibrous remnant of the dorsal aspect of the sheath causing elevation of the superficial radial nerve. They recommend sheath excision or incision of the sheath at its dorsal attachment to avoid this complication.
Ashurst et al. report a case of a patient presenting with bilateral de Quervain’s tenosynovitis secondary to excessive text messaging. Conservative measures
afforded the patient complete symptomatic recovery. They recommend limitation of texting, in conjunction with other standard treatments, to treat text messaging- associated de Quervain’s tenosynovitis
Ilyas et al. review the etiology, diagnosis and management of De Quervain’s tenosynovitis. Non-surgical management is largely successful and includes splinting and cortisone injections. In refractory cases, surgical release of the first dorsal compartment is completed. They recommend meticulous care of the radial sensory nerve and identification of all separate sub-sheaths.
Illustration A shows an operative photo in a patient with multiple APL slips and an EPB that is hidden within a sub-sheath. Video V gives a brief overview of de Quervain’s tenosynovitis.
Incorrect Answers

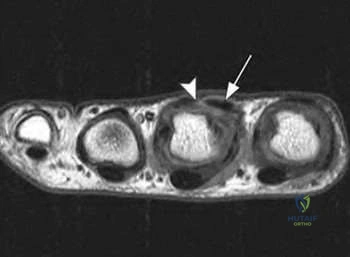
A 28-year-old NFL running back complains of continued hand pain three days following an injury sustained while being tackled. He was splinted on the field. He has tenderness over the long finger metacarpal head, with subluxation of the extensor tendon into the intermetacarpal area during active metacarpophalangeal joint flexion. A representative MRI is shown in Figure A. What is the next best step in management of this patient?
Observation alone
Continued splinting in flexion
Continued splinting in extension
Open repair of the disrupted junctura tendinae
Open repair of the disrupted sagittal band
Based on the history and physical exam findings this patient has sustained a traumatic rupture of the sagittal band. In this professional athlete, the next best step would be to perform an open repair of the sagittal band. This will allow for earlier aggressive rehabilitation and a quicker return to sport.
Sagittal band ruptures may be traumatic (as in this case) or attritional in nature (as in rheumatoid arthritis). A direct blow to the MCP leads to forced flexion of the digit and subsequent stretching/rupture of the affected structure. On physical exam the tendons are most unstable with the wrist flexed; MCP flexion will lead to dislocation of the tendon into the intermetacarpal gutter.
Acute injuries may be treated with extension bracing for 4-6 weeks, but in professional athletes, direct open repair of the sagittal band is indicated.
Catalano et al. review sagittal band injuries treated with a thermally molded
plastic splint that held the MCP in ~25-35 degrees of hyperextension. Patients were evaluated over 14 months; out of 11 sagittal band injuries, splinting was successful in eight of them. They recommend initial nonsurgical management with custom splinting.
Hame et al. review the results of the management of sagittal band injuries in the professional athlete. The lesion commonly found was the disruption of the extensor mechanism with predictable sagittal band tears. In their series, all patients regained full range of motion and returned to their respective sports. They recommend surgical intervention in elite athletes in the form of extensor tendon centralization and sagittal band repair.
Figure A shows a T1 weighted axial cut of the affected hand; subluxation of the tendon (arrow) can be identified with disruption of the sagittal band (arrowhead).
The video provided briefly reviews injury to the sagittal band. Incorrect Answers
Compressive injury to the posterior interosseous nerve will lead to EMG fibrillations in which of the following muscles?
Extensor Carpi Radialis Longus/Extensor Carpi Radialis Brevis/Brachoradialis
Extensor Carpi Radialis Longus/Supinator/Abductor Pollicis Longus
Extensor Pollicis Longus/Supinator/Abductor Pollicis Longus
Brachoradialis/Supinator/Extensor Pollicis Longus
Extensor Pollicis Longus/Supinator/Abductor Pollicis Brevis
Based on the choices above, fibrillations will be seen in the extensor pollicis longus, supinator and abductor pollicis longus muscles.
The radial nerve splits into the superficial radial branch and the posterior interosseous nerve (PIN) at the anterior aspect of the radiocapitellar joint, just proximal to the supinator muscle. The PIN innervates the EDC, EDM, ECU,
EPB, EPL, EIP, APL and sometimes the ECRB. Compressive neuropathy of the PIN leads to motor dysfunction, namely weakness with wrist and finger extension.
Lubhan et al. review uncommon compression neuropathies affecting the upper extremity. They indicate that PIN syndrome may be caused by rheumatoid arthritis and compressive ganglion cysts. Depending on which nerve branch is affected, partial lesions may develop. They recommend use of conservative measures (rest, activity modification and splinting) first. Decompressive procedures may be indicated in symptoms lasting greater than 3 months.
Illustration A shows the course of posterior interosseous nerve from proximal to distal along the course of the supinator. This proximal edge of the supinator (Arcade of Froshe), the fibrous edge of the ECRB and the leash of Henry are three main points of compression of the PIN.
Incorrect Answers

Figure A shows a traumatic laceration of the distal forearm with a 5cm segmental median nerve defect. Which of the following repair or reconstruction techniques would allow for the best recovery of motor function?

Autogenous venous nerve conduit
Collegen synthetic nerve conduit
Biodegradable polyglycolic acid
Processed nerve allograft
Nerve autograft CORRECT ANSWER: 5
Figure A shows a traumatic laceration with 5cm of median nerve defect. The use of nerve autograft for this size defect has been shown to have the best recovery of motor function.
The optimal surgical treatment of nerve laceration is direct tension-free repair. In segmental nerve defects this approach cannot be achieved. The use of interposed autologous nerve grafting remains the gold standard of repair in this setting. The use of alternative techniques, such as processed allografts and synthetic conduits, have not shown to have equivalent recovery of motor function as compared to nerve autograft.
Giusti et al. used a rat model to examine techniques of peripheral nerve repair. They showed that nerve autograft resulted in better motor recovery than did the use of processed allograft or a collagen conduit.
Deal et al. discussed tubular interposition substitutes, or nerve conduits, as an alternative to nerve autograft in segmental nerve defect. Nerve conduits can include autogenous nerve conduits (venous or arterial) and synthetic nerve conduits (collagen, PGA, or caprolactone). In general, there is an upper limit of 3-cm when using nerve conduit.
Figure A is an image of the volar forearm. There is a traumatic laceration to
the anterior compartment tendons as well as the median nerve.
Incorrect Answers:
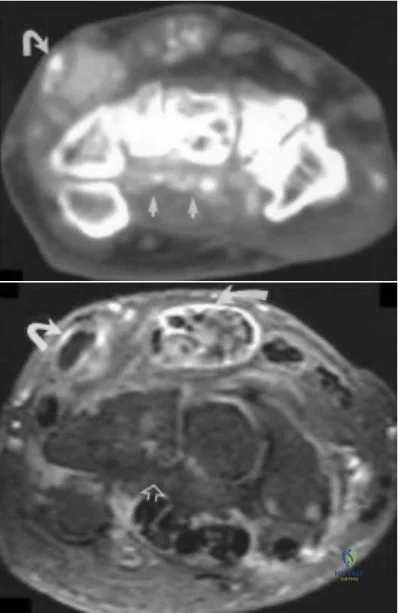
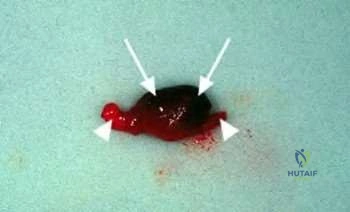
A 45-year-old man presents with a three-month history of unilateral symptoms in his right wrist and hand. He first noticed a palpable nodule over the volar aspect of his wrist about three months ago. The nodule would become painful after weekends of heavy drinking at which time he noticed tingling sensation in his index and middle fingers. He notes that ibuprofen has helped improve the pain in the past. On clinical examination, he has a palpable, nontender, solid nodule over the volar aspect of his wrist. He has no motor or sensory deficits and negative carpal tunnel provocative tests. An axial CT and MRI image are provided in figures A and B. What would be the most appropriate next step in the management of his symptoms?
Fine needle aspiration
Chemotherapy
Night splints
Establish a tissue diagnosis and referral to a rheumatologist
Surgical excision CORRECT ANSWER: 4
The clinical presentation is consistent with carpal tunnel syndrome caused by an atypical space occupying lesion - in his case, gout. The most appropriate next step in the management of his symptoms would be establishing a tissue diagnosis and referral to a rheumatologist where medical therapy, such as prophylaxis with colchicine, could be initiated.
Carpal tunnel syndrome is the most common compressive neuropathy, affecting up to 10% of the general population. Risk factors include female sex,
advanced age, obesity, and repetitive motion activities. Typically, patients will develop symptoms of median nerve compression including thenar muscle atrophy, numbness in the radial 3.5 digits, night pain, and positive Tinel's and Phalen tests. First line management is non-operative, including NSAIDs, night splints, and activitiy modification. Carpal tunnel release surgery is indicated for those who have failed conservative management.
Chen et al. described 23 unusual cases of CTS in which space-occupying lesions were responsible for the symptoms and signs of median nerve compression. In patients with an atypical presentation, such as male gender, non-middle-aged, or unilateral involvement, space-occupying lesions such as gout, synovial sarcoma, lipoma, and ganglions should be investigated as a cause.
Fitzgerald et al. discussed gout affecting the hand and wrist. The medical treatment of gout includes NSAIDs such as indomethacin or ibuprofen for acute flares, and colchicine and allopurinol for chronic prophylaxis.
Figures A and B represent axial CT and MRI images showing calcification and gouty tophi deposition in the carpal tunnel floor.
Incorrect Answers:
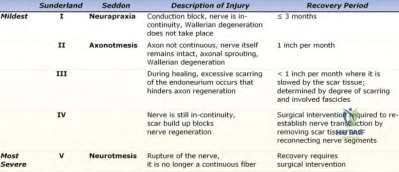
Which statement most accurately describes the physiology of peripheral nerve regeneration following an axonotmesic lesion?
The proximal nerve segment undergoes Wallerian degeneration
Axon growth occurs from the distal segment to proximal segment
Neurotrophic factors direct phagocytic activity
Proximal axon budding allows for antegrade (or distal) axon migration
Axoplasm and myelin are degraded distally predominantly by Schwann cells for the first 12 months following injury
Axonomesis is a disruption of the nerve axon following injury. Repair/regeneration of the nerve occurs via proximal budding, followed by antegrade (or distal) axon migration.
The peripheral nerve regeneration process begins with the distal segment undergoing Wallerian degeneration (axoplasm and myelin are degraded distally by phagocytes). Existing Schwann cells proliferate and line-up along the basement membrane. Proximal budding occurs after a one-month delay. This is followed by sprouting axons that migrate in an antegrade fashion to connect to the distal tube. Repair of the nerve can take months, and often have poor outcomes.
Lee et al. reviewed peripheral never injury and repair. They commented that Wallerian degeneration (i.e., breakdown of the axon distal to the site of injury) is initiated 48 to 96 hours after transection. The Schwann cells then align themselves longitudinally, creating columns of cells called Büngner bands. At the tip of the regenerating axon is the growth cone.
Illustration A shows a chart of peripheral nerve injury. The two main classification systems are Seddon and Sunderland. Video V is a lecture discussing peripheral nerve injury and management.
Incorrect Answers:
A 28-year-old male injures his hand while playing basketball and presents to the emergency room. Closed reduction is performed and is stable. Post-reduction rehabilitation is discussed with the patient.
Which of the following radiographs demonstrates an injury that would be treated best by dorsal extension block splinting?

Figure E CORRECT ANSWER: 2
Dorsal extension-block splinting is the treatment of choice for dorsal proximal interphalangeal joint (PIPJ) fracture dislocations that are stable following reduction and have less than 40% articular surface fracture involvement.
Dorsal PIPJ dislocations are a common injury, often resulting from jamming or hyperextending the finger. In the absence of an associated fracture or presence of a small volar plate avulsion, dorsal PIPJ dislocations are often
treated with closed reduction and buddy-taping to the adjacent digit. Injuries that are unstable following reduction or those associated with an intra-articular fracture of the middle phalanx are stabilized with a dorsal extension-block splint to maintain reduction. It is important to initiate early range of motion exercises within the constraints of the splint to minimize scar formation and subsequent PIPJ contracture.
Elfar et al. reviewed fracture-dislocations of the PIPJ. Dorsal PIPJ fracture-dislocations can be categorized as avulsion or impaction shear injuries.
Avulsion fractures result from hyperextension of the PIPJ, tensioning the volar plate (VP) with eventual VP rupture or avulsion of the volar lip of the middle phalanx. Axial load applied to the digit in PIPJ flexion drives the head of the proximal phalanx across the middle phalangeal base, resulting in a shear fracture or comminuted impaction fracture of the middle phalanx, depending on the amount of energy imparted and the bone quality.
Morgan et al. reviewed hand injuries in athletes. Dorsal PIPJ dislocations without associated fracture that are stable following successful reduction are treated by buddy taping the injured digit to the non-injured digit adjacent to the compromised collateral ligament. Buddy taping with active motion should be continued for 6 weeks. Unstable injuries and those with an intra-articular fracture of the middle phalanx should be treated with dorsal extension-block splinting with incremental extension of the splint on a weekly basis for 4 weeks, followed by buddy-taping for 3 months during sports activities.
Figure A shows a simple dorsal PIPJ dislocation. Figure B shows a dorsal PIPJ fracture dislocation. Figure C shows a simple volar PIPJ dislocation. Figure D shows a volar PIPJ fracture dislocation. Figure E shows a dorsal avulsion fracture at the base of the distal phalanx (bony mallet injury). Illustration A depicts an dorsal extension-block splint that blocks extension of the digit past a set point while allowing full active flexion of the digit. Illustration B is a lateral radiograph of a digit showing a small minimally displaced volar plate avulsion fracture at the PIPJ with minimal intra-articular involvement (as compared to Figure B). This injury may be managed with buddy taping and active range of motion as tolerated.
Incorrect Responses:
extension for 6-8 weeks to limit flexion of the digit and therefore fracture displacement.

A 35-year-old mixed martial arts fighter and recreational cocaine user presents with symptoms concerning for hypothenar hammer syndrome (HHS). Significant ischemia is found on physical exam. Arteriography is shown in Figure A. What is the most appropriate next step in treatment?

Conservative treatment with cocaine abstinence
Conservative treatment with activity modifications and medical management with calcium channel blockers
Therapeutic endovascular fibrinolysis
Excision of involved segment and reconstruction with or without a vein graft
Medical management with coumadin for 6 months
Figure A shows a bilobed aneurysm overlying the ulnar artery with normal appearing distal vasculature. Hypothenar hammer syndrome (HHS) can be associated with an aneurysm and is most appropriately treated with resection of the involved segment and either reconstruction with a primary anastomosis or vein graft.
HHS syndrome consists of two separate entities, thrombosis and aneurysm. In the setting of thrombosis without aneurysm, conservative management is preferred. If the thrombosis is acute (<2 weeks), endovascular fibrinolysis has shown good results. In patients with an HHS and an aneurysm, surgery is required for resection to prevent distal embolization and remove the often painful aneurysmal mass.
Yuen et al. review HHS. In patients with HHS and aneurysms, resection of the involved segment of the ulnar artery prevents distal embolic events, eliminates the painful mass, relieves ulnar nerve compression, and removes the thrombus which initiated the reflex vasospasm and closed off the collateral
vessels in the region.
Lifchez et al. review the long-term outcomes of 11 patients with HHS treated with ulnar artery reconstruction. 2 of the patients underwent excision and direct ulnar artery repair, and the rest underwent reconstruction with a vein graft. All patients had a mean improvement in digital brachial index, decrease in pain and dysesthesia symptoms, and decrease in cold intolerance compared with preoperatively.
Nitecki et al. review a case series of 6 patients with HHS. They state that the treatment of thrombosis should be largely conservative, but thrombolytic treatment could be considered if the event happened <2 weeks prior to presentation.
Illustration A shows an excised ulnar artery aneurysm in a patient with HHS. Note the typical "corkscrew" appearance of the distal segment.
Incorrect Answers:
A 36-year-male was using a high-pressure paint gun when he suffered the injury shown in Figure A. Which of the following variables would have the worst impact on his prognosis?

Delay in surgical treatment
Injected solvent was grease
Injected solvent was water-based paint
An entry wound of greater than 3 cm
Injected solvent was at room temperature
The clinical presentation is consistent for a high-pressure injection injury. Delays in surgical treatment are associated with serious sequelae.
High-pressure injection injuries are characterized by extensive soft tissue damage associated with a benign high-pressure entry wound. They should be treated with irrigation & debridement, foreign body removal and broad-spectrum antibiotics. There is a higher rates of amputation when surgery is delayed.
Bekler et al. looked at the results of 14 surgically treated high-pressure injection injuries of the hand with a minimum of two years follow-up. Ten of the injuries required formal operative debridement and foreign body removal. Six required reconstructive microsurgical procedures and one underwent digital tip amputation. They concluded that high-pressure injection injury to the hand is a significant problem, which can easily lead to serious sequelae and, even, amputation.
Rosenwaser et al. report wide débridement of all involved tissues, decompression of tissue compartments, exploration and incision of tendon sheaths, removal of injected material, and saline irrigation are critical in the management of high-pressure injection injuries to the hand. They emphasize
delayed surgery has been associated with increased incidence of morbidity and amputation.
Figure A shows a typical high-pressure injection injury. Notice the benign looking entry wound.
Incorrect Answers:
A healthy 50-year-old secretary is about to undergo an open carpal tunnel release. Which of the following peri-operative steps will have the greatest influence on minimizing the risk of a surgical site infection in this patient?
Administration of cefazolin within 1 hour before incision
Administration of cefazolin within 1 hour before incision followed by 5 days of cephalexin post-op
Cleanse with bacitracin solution immediately before skin incision
Standard sterilization and prepping
Administration of one dose of cephalexin within 1 hour before incision
The patient is undergoing a clean, elective hand surgery. Prophylactic antibiotics, systemic or local, are not indicated for these procedures.
Carpal tunnel syndrome is the most common compressive neuropathy. Individuals who fail medical management (night splints, NSAIDs, activity modification) are candidates for carpal tunnel release surgery (CTS). The surgery may be performed open or endoscopically. The reported incidence of post-operative infections following CTS varies between studies from 0% to 8%.
Whittaker et al. performed a prospective, randomized, double-blinded, placebo
controlled trial investigating the use of antibiotic prophylaxis in clean, incised hand injuries. They found no significant difference in infection rates between patients who received IV flucloxacillin, IV followed by oral flucloxacillin, and an oral placebo (13% vs. 4% vs. 15%, p=0.19). They did not support the use of routine antibiotic prophylaxis prior to clean hand surgery.
Bykowski et al. retrospectively reviewed 8,850 outpatient elective hand surgeries and found no significant difference in the rate of surgical site infection, including patients with diabetes or history of smoking. They concluded that antibiotics should not be routinely administered prior to clean, elective hand surgeries.
Harness et al. found no statistical difference in the incidence of surgical site infection following CTS without prophylactic antibiotic compared with patients who received prophylactic antibiotics (0.7% vs. 0.4%, p=0.354). They did not recommend routine antibiotic prophylaxis.
Illustration A reviews the anatomic components of the carpal tunnel. Incorrect Answers:
infection in clean, elective hand surgery. Surgeons should consider the potential risks of antibiotics prior to administration, including Clostridium difficile colitis, antibiotic allergies, bacterial resistance, and so on.
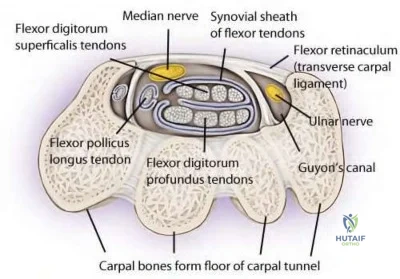
A 30-year-old male laborer sustained a right wrist injury 9 months ago. He continues to have symptoms of recurrent ulnar-sided wrist pain that impairs his ability to work. An MRI is performed and
shows a triangular fibrocartilage complex (TFCC) injury. Which of the following is an indication to combine a Wafer procedure with arthroscopic TFCC debridement?
Ulnar styloid fracture
Radial styloid fracture
2 mm of positive ulnar variance and ulnocarpal impingment
2 mm of negative ulnar variance and radiocarpal joint arthritis
Scapholunate ligament injury
A Wafer procedure is indicated for positive ulnar variance and symptomatic ulnocarpal impingement associated with degenerative TFCC tears.
Ulnar impaction syndrome and triangular fibrocartilage complex (TFCC) injuries are relatively common causes of ulnar-sided wrist pain. Positive ulnar variance causes increased contact pressures between the lunate and the ulnar head. The Wafer procedure removes 2-4 mm of distal ulnar head to reduce ulnar variance to neutral or negative. This is thought to reduce ulnar impaction and decrease pain.
Faber et al. examined the role of MRI in wrist injuries. They showed that the sensitivity and specificity to detect TFCC tears using MRI is approximately 80%. They conclude that there is no supporting evidence for routine MRI's for patients with non-specific ulnar-sided wrist pain.
Illustration A is a coronal view MRI (without arthrogram) of the right wrist that shows a TFCC tear (blue arrow) with positive ulnar variance. Illustration B shows a series of images showing a TFCC tear on MRI and intra-operatively.
Incorrect Answers:

A 27-year-old male sustains the injury shown in Figure A. He is taken to the operating room and the lesion is repaired primarily. Two months later, he feels a "pop" while using his hand and is no longer able to flex the distal phalanx of the involved digit. He is taken to the operating room for surgical exploration where 1.8 cm of scar tissue between the tendon ends is identified. The tendon sheath is found to be intact and allows smooth passage of a pediatric urethral catheter. What is the next step in management?

Resection of scar and primary repair of tendon ends.
Resection of scar and adjacent 1cm of tendon, placement of Hunter rod for staged reconstruction.
Debulking of scar, partial excision of 25% of the A2 and A4 pulleys.
Resection of scar, harvest of ipsilateral palmaris longus tendon for tendon reconstruction.
Resection of scar and proximal tendon, tendon transfer from adjacent digit.
This patient sustained an FDP laceration that was treated initially with primary repair. He subsequently re-ruptured the tendon 2 months later. With scar >1 cm, tendon grafting is indicated and primary tendon grafting with palmaris longus is commonly performed as it is the most accessible tendon in the operative field.
Flexor tendon lacerations commonly result from volar lacerations. Concomitant neurovascular injury is common. Partial lacerations <60% of tendon width are treated with debridement and early range of motion. With partial lacerations, the least amount of gliding resistance can be obtained with debridement alone. Lacerations >60% of tendon width are treated with flexor tendon repair and controlled mobilization. Failed primary repair and chronic untreated injuries are indications for flexor tendon reconstruction and intensive postoperative rehabilitation.
Lilly et al. reviewed complications after flexor tendon injuries. Common complications include adhesions, joint contracture, tendon rupture, triggering, pulley failure and bowstringing, quadrigia, swan-neck deformity and lumbrical plus deformity.
Figure A shows a zone II laceration of the left index finger FDP.
Incorrect Answers:
A 55-year-old female patient presents with pain along the thumb ray and increasing deformity of her right hand. Key pinch causes her pain. The appearance of her hand is seen in Figure A. Range of motion of her thumb is seen in Figure B. What is the most likely cause of her deformity?
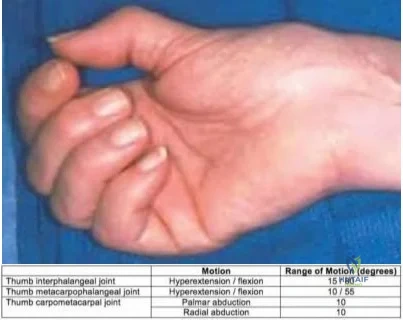
Type II hypoplastic thumb
Median nerve neuropathy
Lupus thumb deformity
Extensor tendon rupture
Osteoarthritis of the trapeziometacarpal joint
The patient has 1st carpometacarpal (CMC) arthritis.
With 1st CMC arthritis, the patient avoids painful thumb abduction and an adduction deformity gradually develops, with 1st webspace contracture. With progressive 1st CMC stiffness, the thumb metacarpophalangeal joint (MCP) develops hyperextension deformity to compensate for the loss of motion, leading to a secondary "Z" deformity.
Rozental et al. reviewed hand and wrist reconstruction. They believe that arthrosis arises from loss of the anterior oblique ("beak") ligament.
Compensatory MCP hyperextension should be treated with MCP capsulodesis or arthrodesis.
Van Heest et al. reviewed thumb CMC arthritis. Treatment for Eaton stage I/II arthritis is open/arthroscopic debridement, volar ligament reconstruction (with APL or FCR tendons), or metacarpal extension osteotomy. For stage III/IV arthritis, treatment options include implant arthroplasty or resection arthroplasty +/- LRTI (with APL, FCR or palmaris longus), and fusion (young patients).
Figure A shows adduction contracture of the 1st webspace, with hyperextension deformity of the 1st MCP joint. Figure B illustrates decreased thumb abduction because of adduction contracture with decreased palmar abduction (normal, 45deg) and decreased radial abduction (normal, 60deg). Illustration A is a radiograph showing thumb CMC arthritis with Z deformity. Illustration B shows lupus thumb deformity ("hitchhiker thumb"). Illustration C shows hand changes in inflammatory arthritis.
Incorrect Answers:
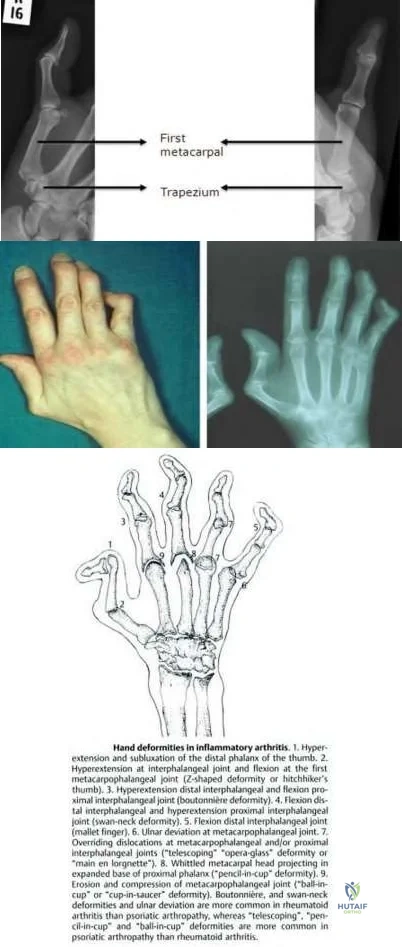
A 26-year-old man presents with chronic hand weakness. The clinical appearance of his hand, and radiographs are shown in Figures A through C. Surgical exploration and decompression is performed. Besides addressing thumb interphalangeal and index distal interphalangeal joint flexion, which is the most appropriate treatment to restore thumb opposition?

Ring flexor digitorum superficialis transfer to the abductor pollicis brevis
Extensor indicis proprius transfer to the abductor pollicis brevis
Neurotization of thenar muscles
Camitz palmaris longus transfer to the abductor pollicis brevis
Thumb carpometacarpal joint arthrodesis
This patient has a high median nerve neuropathy because of a supracondylar spur and ligament of Struthers. Reconstruction is best performed with extensor indicis proprius (EIP) transfer to the abductor pollicis brevis (APB).
In low median nerve palsy, the primary concern is restoration of thumb opposition. In high median nerve palsy, thumb opposition and IP flexion, and index and middle finger flexion have to be addressed. The four common opposition transfers include (1) ring or long FDS, (2) EIP, (3) Camitz palmaris longus (PL), or the Huber abductor digiti minimi (ADM).
Anderson et al. reviewed EIP transfer vs FDS transfer. They found a higher percentage of excellent results in the EIP group. In their series, complications included index finger extensor lag (EIP transfer if the extensor expansion was not repaired) and limited donor finger extension because of lateral band damage or adhesions between the remaining FDS tendon and flexor sheath (FDS transfer).
Cawrse et al. modified the Huber ADM opponens transfer by releasing the proximal end to prevent compression of the ulnar nerve in Guyon's canal by the rotated ADM belly. They found that this technique successfully restored
opposition and thenar bulk.
Figure A shows thenar wasting. Figures B and C show a supracondylar spur. The ligament of Struthers attaches from this spur to the medial epicondyle, under which median nerve and brachial artery pass. Illustration A shows EIP transfer. Illustration B shows FDS transfer. Illustration C shows Camitz PL transfer. Illustration D shows Huber ADM transfer.
Incorrect Answers:
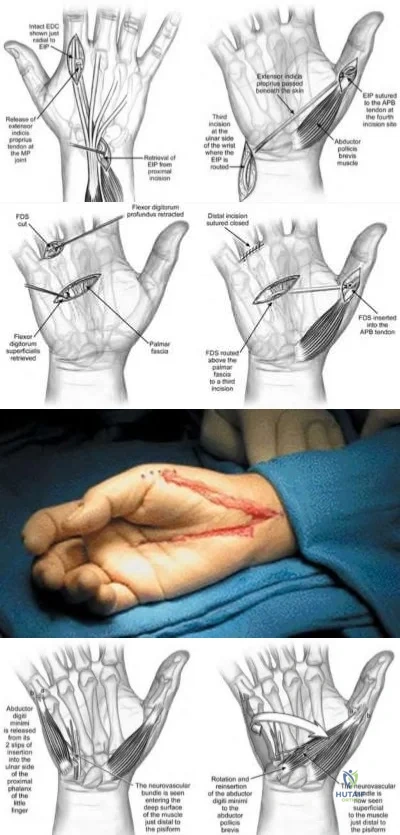
A 2-year-old child is referred by her pediatrician for fixed flexion deformity of the left thumb. She has been wearing a splint for the last 6 months. She has ventricular septal defect and left renal agenesis. The interphalangeal joint does not extend past 40 degrees of flexion as seen in Figures A and B. There is no triggering. There is a firm, nontender nodule overlying the metacarpophalangeal joint as outlined in blue in Figure C. What is the diagnosis and most appropriate treatment?

Thumb camptodactyly. Therapy including passive stretching exercises.
Congenital clapsed thumb. Percutaneous release of the A1 pulley.
Pediatric trigger thumb. Open release of the A1 pulley.
Pediatric trigger thumb. Open release of the A1 pulley and resection of the tendon nodule.
Blauth Type I hypoplastic thumb. Open release of the A1 pulley and volar plate, and resection of the tendon nodule.
This child has pediatric trigger thumb (PTT). The potential for spontaneous resolution beyond the age of 2 years is limited. Surgical release of the A1
pulley is indicated.
Pediatric trigger thumb presents as fixed flexion at the interphalangeal joint (IPJ) rather than triggering. It is likely to be acquired (rather than congenital). It is associated with the presence of Notta's nodule, a thickening of the FPL tendon and overlying tendon sheath. Treatment involves A1 pulley release.
The role of non-surgical management (splinting/stretching) remains unclear. The duration of non-surgical treatment is long (up to 30 months) and compliance can be difficult.
Shah et al. reviewed pediatric trigger thumb. The condition is associated with MCP hyperextension. The authors note no advantage to percutaneous release as general anesthetic is required anyway.
Marek et al. performed a retrospective review and survey response review of surgery for pediatric trigger thumb. They found that age at the time of surgery influences residual flexion contracture and rate of recovery. They found surgery to be safe and effective, and recommend: (1) surgery for a 2-year-old child with a locked thumb for 6 months, (2) observation for a child <1 year if the thumb is triggering (not locked), and (3) a 6-month observation period if observation is advocated.
Figures A and B show a fixed flexion deformity of the thumb and an attempt at thumb extension. Figure C shows the outlined Notta nodule.
Incorrect Answers:
A 48-year-old hairdresser presents with pain and swelling of his ring finger for 4 days. On examination, there is generalized tenderness along the entire digit. Passive extension of the digit triggers
excruciating pain. The clinical appearance of the digit is shown in Figure A. What is the most appropriate next step in management?

Acyclovir
Intravenous antibiotics, splinting and elevation
Closed tendon sheath irrigation from the level of the A1 pulley (proximal) to the distal interphalangeal joint (distal)
Continuous closed tendon sheath irrigation from the wrist (proximal) to the distal interphalangeal joint (distal)
Open irrigation and debridement
This patient has advanced pyogenic flexor tenosynovitis (PFT) with visible ischemia/necrosis. Open irrigation and debridement is necessary.
Pyogenic flexor tenosynovitis is usually caused by a puncture wound (although it may infrequently arise from hematogenous spread). The most common organism is Staphylococcus aureus. Kanavel signs help differentiate this disease from herpetic whitlow, septic arthritis, gout/pseudogout, and other hand infections such as paronychia, felons, cellulitis, and deep space infections.
Draeger et al. reviewed the treatment of pyogenic flexor tenosynovitis (PFT). They recommend open irrigation and debridement for advanced PFT and atypical or chronic tenosynovial infections where tenosynovectomy may be
indicated. Both midaxial and volar zigzag incisions can be used.
Pang et al. reviewed factors affecting the prognosis of PFT. Of the 4 Kanavel signs, they found that fusiform swelling was most often present (97% of patients), followed by pain on passive extension (72%), semiflexed digit posture (69%), and tenderness along the flexor tendon sheath (64%).
Figure A shows advanced PFT demonstrating subcutaneous purulence and local ischemia in addition to fusiform digital swelling. Illustration A shows the Nevasier technique of closed tendon sheath irrigation. Illustration B shows the setup for continuous tendon sheath irrigation using nested catheters.
Illustration C shows the incision for open irrigation and debridement.
Incorrect Answers:

Madelung's deformity of the distal radius is caused by which of the following?
Premature fusion of the distal radial ulnar joint
Physeal growth mismatch between the distal radius and ulna
Nutritional deficiency affecting the physeal zone of provisional calcification
Impaired growth of the volar and ulnar aspect of the distal radial physis
Unrecognized trauma CORRECT ANSWER: 4
Madelung's deformity is that of excessive ulnar/palmar angulation of the distal radius caused by impaired growth of the volar and ulnar aspect of the distal radial physis. It may be caused by either a bony lesion in the palmar/ulnar corner of the distal radial physis or an abnormal radial-carpal ligament (Vicker's ligament). The other answers do not cause Madelung's deformity.
Leri-Weill dyschondrosteosis is a rare genetic disorder caused by mutation in the SHOX gene that causes mesomelic dwarfism with associated Madelung's defomity of the forearm.
Illustration A is a radiographic example of Madelung's deformity.

A 17-year-old boy presents with pain in his right elbow for 2 years and limitation in elbow motion bilaterally. He denies any pain or discomfort in his left elbow. He reports no history of trauma to either elbow. He has had two courses of physical therapy, but has noted no noticeable improvement in pain or motion. Examination demonstrates no elbow tenderness on palpation, and there are no neurological deficits. Manual reduction is unsuccessful. The range of motion of both elbows is shown in Figure A. Radiographs of left and right elbow are shown in Figure B and C respectively. What is the most appropriate treatment plan for the right and left elbow?

Bilateral open reduction and application of a hinged external fixator to both elbows
Radial head resection of the right elbow and non-operative management of the left elbow.
Bilateral radial head arthroplasty
Physical therapy and splinting to both elbows
Radial head resection and interposition arthroplasty for the right elbow and radial head resection alone for the left elbow
This patient has bilateral congenital radial head dislocation (CRHD). The right side is symptomatic with significant loss of motion. The left is asymptomatic with minimal loss of active motion. Therefore the most appropriate treatment is radial head resection of the right elbow and non-operative management of the left elbow.
It is important to differentiate CRHD from traumatic dislocation. Clinical features of CRHD include bilateral involvement, presence at birth, other congenital anomalies, familial occurrence, irreducible by closed methods, and
lack of a history of trauma. Radiological features include dome-shaped radial head and hypoplastic capitellum, relatively short ulna or long radius, deficient trochlea, prominent medial epicondyle, grooving of the distal radius, and anterior curvature of the posterior outline of the ulna.
Bengard et al. reviewed 10 surgically treated and 6 nonsurgically treated CRHD patients. They found no change in flexion-extension and carrying angle postoperatively, but forearm rotation was improved. Surgically treated patients had significant improvement in elbow pain. Ultimately, >25% of patients had wrist pain postop and this must be weighed in the decision process of treatment. They recommend radial head excision as an effective intervention in selected patients with significant elbow pain.
Figure A is a table showing moderately diminished ROM of the right elbow, and minimally reduced ROM of the left elbow. Figures B and C both show posterior dislocation of the radial head (a line along the long axis of the radius should intersect the capitellum in all views).
Incorrect Answers:
Which of the following muscles provide the primary deforming forces to Bennett and Rolando fractures (base of the 1st metacarpal fractures)?
Pronator quadratus
Flexor pollicis longus
Extensor pollicis longus
Adductor pollicis longus and abductor pollicis
Abductor pollicis longus and adductor pollicis
The primary deforming forces in Bennett and Rolando fractures are the Abductor pollicis longus and adductor pollicis.
In a Bennet's or Rolando fracture-dislocation the volar-ulnar fracture fragment is held reduced by the anterior oblique ligament while strong deforming forces pull the remaining metacarpal shaft proximally and dorsally, angulate the shaft ulnarly and supinate the shaft. Most important in these deforming forces are the abductor pollicis longus (APL) inserting on the base of the metacarpal which pulls the metacarpal shaft proximally and dorsally and the adductor pollicis (AP) which inserts on the ulnar base of the proximal phalanx and angulates the metacarpal shaft ulnarly and supinates the shaft. Less important is the extensor pollicis longus (EPL) which inserts on the base of the distal phalanx and also adds to the ulnar angulation of the distal fragment.
Soyer reviews the diagnosis, pathoanatomy, and treatment for fractures at the base of the 1st metacarpal. Understanding the biomechanics, anatomical deforming forces, and the exact fracture pattern aids the treating surgeon in determining the most appropriate method of fixation. The most essential factor for obtaining a good functional result is anatomic restoration of the articular surface.
Elgafy et al. examined the terminal anatomy of the posterior interosseous nerve in their cadaver study - identifing six terminal branches and describing methods to avoid injury. They describe how treating surgeons can maximize function and recovery after base of the 1st metacarpal fractures by understanding these nervous branches and specific fracture pattern treatment to avoid iatrogenic injury to the PIN.
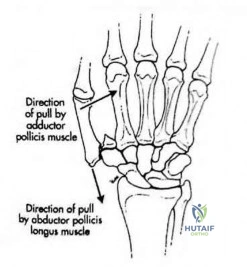
A 28-year-old man sustained a complete laceration of the flexor digitorum profundus of his index finger while cutting a watermelon 3 days ago. A clinical photograph is shown in Figure A. The surgeon plans to repair the tendon using a 4-strand core suture technique. Which method of tendon repair will give him the best results in terms of load to failure and gliding resistance?

Repair with core suture purchase 5mm from the cut edge only. No epitendinous suture
Repair with core suture purchase 10mm from the cut edge only. No epitendinous suture
Repair with core suture purchase 5mm from the cut edge. Circumferential
simple running epitendinous suture.
Repair with core suture purchase 10mm from the cut edge. Circumferential Silfverskiold epitendinous suture.
Repair with core suture purchase 10mm from the cut edge. Circumferential simple running epitendinous suture.
Repair with core suture purchase 10mm from the cut edge, coupled with circumferential simple running epitendinous suture will give him the best load to failure and gliding resistance.
The strength of tendon repairs depend on the number of strands crossing the repair site. Ideally, repairs should have 4-6 strands to allow for early active motion. A running epitendinous suture is recommended to improve tendon gliding and repair strength.
Gulihar et al. compared 3 different epitendinous suture techniques. They found that compared with an intact tendon, gliding resistance increased 100% with the Halsted repair, 80% with the Silfverskiold repair and 60% with a running suture. They thus recommend a simple running suture when an epitendinous suture is needed.
Lee et al. compared core suture purchase at 3, 5, 7 and 10mm from the cut edge. The 10mm-repair group had the highest 2-mm gap force and ultimate failure load. They recommend 10-mm suture purchase for optimal performance and to allow early active motion.
Figure A shows a laceration to the volar aspect of the index finger in flexor zone II. Illustration A shows a core suture purchase distance from the cut edge (represented by "X", where 10mm is the ideal distance). Illustration B shows 3 different epitendinous suture techniques (A, simple running; B, Silfverskiold; C, Halsted).
Incorrect Answers:

A 28-year-old professional baseball player injures his middle finger sliding into the catchers shin guard at home plate. He complains of pain and deformity of the middle finger. A radiograph is provided in figure A. All of the following are true EXCEPT:
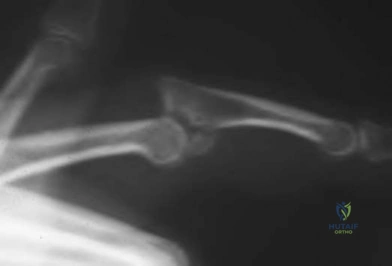
Anatomic reconstruction of the articular surface is prognostic of clinical function
Proximal interphalangeal joint subluxation precludes a normal gliding flexion arc
Hinging at the fracture site must be avoided
Early motion should be initiated in postoperative therapy
Early degenerative arthritis can be expected if the joint is not adequately reduced.
The radiograph demonstrates a dorsal fracture dislocation of the proximal interphalangeal joint of the middle finger. Kiefhaber and Stern review the presentation, evaluation, and treatment of PIP fractures. Congruent reduction of the joint to allow the middle phalanx to glide around the proximal phalangeal head is paramount to prevent joint subluxation and instability.
Anatomic reconstruction of the articular surface is desirable but not necessary for successful clinical outcome.
A 30-year-old male sustains a 3.5 cm long thumb pulp injury seen in Figure A. He undergoes a procedure to restore the soft tissue envelope. Which treatment option is contraindicated because of increased risk of interphalangeal joint stiffness?

Moberg volar advancement flap
Foucher first dorsal metacarpal artery flap
Littler neurovascular island flap
Free great toe pulp transfer
Holevich first dorsal metacarpal artery flap
This patient has a large thumb pulp defect measuring 3.5 cm in length, extending proximal to the interphalangeal joint (IPJ) crease. Inset of a Moberg flap large enough to cover the defect would necessitate IPJ flexion >45 degrees, increasing the risk of IPJ stiffness.
Thumb pulp defects may be resurfaced by different means, depending on size. The Moberg flap is suited for medium (1.8-3 cm) defects. For defects >1.5 cm, there is increased risk of wound dehiscence, parrot beak nail deformity, and decreased soft tissue padding. Modifications such as V-Y flaps, bilateral Z-plasties, Burrow triangles, 2 lateral triangular flaps at the proximal edge of the flap, or advancement of an island flap with skin grafting of the secondary defect (O’Brien modification), are recommended.
Baumeister et al. reviewed the functional outcome of Moberg flaps. These flaps do not cause marked impairment of active ROM and any reduction in the AROM of the IP joint is because of a loss of hyperextension.
Horta et al. reviewed the use of multiple flaps (Moberg, radial innervated cross-finger, Venkataswami-Subramanian, Foucher, Tezcan, and Littler). They recommended the Foucher flap because of good sensibility, single-stage surgery, and no need for cortical reintegration (unlike the Littler flap)
Figure A shows a large thumb pulp defect. Illustration A shows the options for resurfacing thumb pulp defects of different sizes. Illustration B is a diagram of these options. Illustrations C and D depict the Holevich dorsal metacarpal artery flap (with overlying skin strip). Illustrations E and F depict the Foucher dorsal metacarpal artery flap (islanded).
Incorrect Answers:
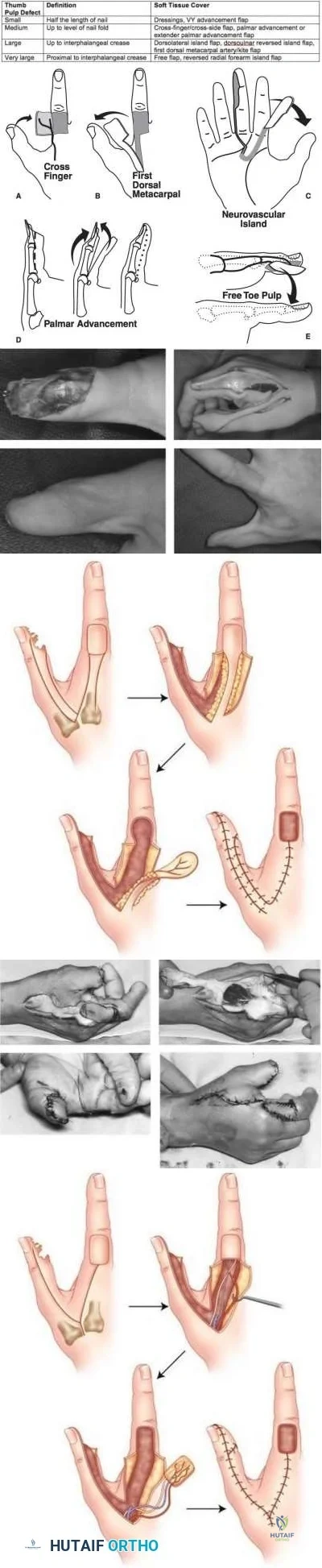
Percutaneous screw fixation for non-displaced scaphoid waist fractures has been shown to have which of the following differences compared to closed treatment?
Increased direct and indirect cost
Slower return to work
Higher union rates
Reduced time to fracture union
Improved motion and grip strength after 2 years
Fixation of non-displaced scaphoid fractures with a percutaneous screw has resulted in a shorter time to union (6-7 weeks versus 10-12 weeks) and faster return to work or sports.
Arora et al found the indirect cost reduction by a quicker return to work was shown to offset the direct costs of surgical intervention.The operatively treated group had a better mean DASH-score than the conservative group. Fracture
union was seen in the screw fixation group at a mean of 43 days and in the cast immobilization group at a mean of 74 days.
Bond et al found in active military personnel there was faster healing but no difference in ultimate union rates or final grip strength or range of motion between percutanous screw fixation and non-operative groups. The average time to fracture union in the screw fixation group was seven weeks compared with twelve weeks in the cast immobilization group. There was no significant difference in the range of motion of the wrist or in grip strength at the two-year follow-up evaluation.
Constriction ring syndrome, also known as amniotic band syndrome, is a congenital disorder associated with which paediatric foot condition?
Equinovalgus foot
Clubfoot (Congenital talipes equinovarus)
Tarsal coalition
Congenital vertical talus
Polydactyly CORRECT ANSWER: 2
Constriction ring syndrome is a congenital disorder that is most commonly associated with clubfeet (congenital talipes equinovarus). The reported incidence of clubfeet with concomitant constriction bands ranges from 12-56%.
Constriction ring syndrome is a collection of congenital malformations that occur as a result of intrauterine rings or bands that constrict fetal tissue. The etiology of constrictive ring syndrome remains elusive, though Streeter postulated in 1930 that a germline developmental abnormality is responsible for the development of amniotic constriction bands, hence one of the synomonous terms used to describe the disorder, Streeter’s dysplasia. Normal anatomy is found proximal to the band. Distally, a constrictive band can cause compression of lymphatic and neurovascular structures and result in lymphedema, altered circulation and neuropathy. In severe cases congenital amputation can occur. In terms of other orthopaedic conditions, constrictive ring syndrome is associated with clubfeet, acrosyndactyly and pseudoarthrosis. With respect to clubfeet, surgical treatment is commonly required, which consists of z-plasty releases of the constricted bands, in addition to surgical correction of the clubfoot deformity.
Gomez reviewed 35 children with clubfeet associated with constriction ring syndrome. In this cohort there was a poor response to casting, as 77% of the children required surgical corrections. Z-plasty releases of the deep bands were performed before the clubfoot correction.
Allington et al. examined the outcome of treatment of clubfeet distal to a lower extremity band in 18 patients (21 feet). Sixteen children (88.9%) underwent surgical treatment after manipulation and serial casting were unsuccessful.
Mild initial foot deformities and constriction bands located in the distal aspect of the lower leg were associated with the best outcomes.
Incorrect Answers:
You are consulted on a newborn male inpatient who presents with the clinical sign shown in Figure A. All of the following are commonly associated with this syndrome EXCEPT?

Bronchopulmonary dysplasia
Cardiac defects
Cleft palate
Encephalocele
Rigid talipes equinovarus
Question 53
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 54
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 55
A favorable outcome following nonsurgical management of a partial tear of the posterior cruciate ligament (PCL) is best associated with
Explanation
REFERENCES: Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-38.
Griffin JR, Annunziata CC, Harner CD: Posterior cruciate ligament injuries in the adult, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2083-2106.
Question 56
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 57
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 58
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
REFERENCES: Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547.
Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 297, 331-332.
Question 59
Lumbar instability may be surgically induced by
Explanation
REFERENCE: Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T, Crisco JJ: Biomechanical evaluation of lumbar spinal stability after graded facetectomies. Spine 1990;15:1142-1147.
Question 60
Figures 23a through 23h are the radiographs and MR images of a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability symptoms. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to decrease stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but, if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should only be performed at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
Question 61
All of the following techniques can help to prevent valgus angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
A final technical trick is the usage of blocking (Poller) screws - the referenced article by Ricci et al had 100% correction and maintenance of reduction with usage of blocking screws without other adjunct techniques. These should be placed in the lateral aspect of the proximal and distal fragments when needed.
The referenced study by Krettek et al is a biomechanical evaluation of blocking screws in a tibial model that showed significantly increased strength when they were utilized.
Question 62
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
Explanation
REFERENCES: Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.
Mathews V, Cabanela ME: Femoral neck nonunion treatment. Clin Orthop Relat Res 2004;419:57-64.
Question 63
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
REFERENCES: Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 64
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 65
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis? Review Topic
Explanation
Question 66
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 67
A 6-year-old girl sustains an ankle injury after falling on roller blades. An AP radiograph is shown in Figure 68. Treatment should consist of which of the following?
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 68
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 69
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement? Review Topic
Explanation
Question 70
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the “teardrop” in its original position and redirects the acetabulum?
Explanation
REFERENCES: Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Ninomija S, Tagwa H: Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am 1984;66:430.
Question 71
below depicts the radiograph obtained from a year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 72
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 73
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 74
Which of the following best describes the relationship of the median nerve to the flexor carpi radialis tendon just proximal to the carpal canal?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 75
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.The most substantial functional deficit that may develop if no surgical treatment is provided is
Explanation
have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
Question 76
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 77
A 29-year-old male rugby player presents for further evaluation and management of left shoulder instability. He initially dislocated his left shoulder six years ago while snowboarding. Since that time, he has sustained five dislocations requiring reduction. He has participated in multiple rounds of physical therapy without improvement. His CT scan and 3D reconstruction are pictured in Figures A and B. Which of the following is the most appropriate treatment for this patient? Review Topic
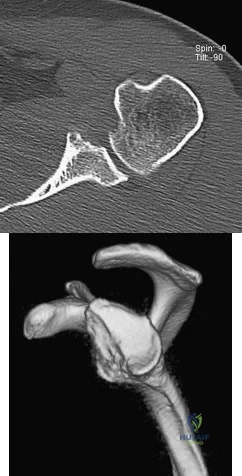
Explanation
Recurrent anterior shoulder instability occurs in 33-67% of patients who sustain an initial traumatic dislocation. Specific risk factors include age < 25 years, male gender, anterior glenoid (Bankart) and/or posterior humeral (Hill-Sachs) osseous defect(s) and participation in contact sports. Surgical management of recurrent instability depends on the presence or absence of glenohumeral bone loss. Patients with < 20% glenoid bone loss can be managed with arthroscopic Bankart repair. An engaging Hill-Sachs lesion, meaning the humeral head defect engages the glenoid rim in abduction (ABD) and external rotation (ER) [see Illustration B], in the setting of minimal glenoid bone loss can be managed with remplissage. Patients with > 20% glenoid bone loss require greater stabilization, mostly commonly in the form of an open coracoid transfer (Latarjet procedure).
Burkhart et al. (2000) found arthroscopic Bankart repairs equivalent to open Bankart repairs if no substantial bone defects were present. However, patients with an “inverted pear” glenoid secondary to significant anteroinferior bone loss or an engaging Hill-Sachs lesion of the humerus had a 67% recurrence rate overall and an 89% recurrence rate if they were contact athletes. Therefore, contact athletes with structural bone deficits require open surgery and often necessitate reconstruction with bone-block procedures.
Itoi et al. determined that an osseous defect with a width of >/= 21% of the glenoid length was associated with anteroinferior instability in ABD and internal rotation (IR), as well as loss of external rotation following Bankart repair. The authors concluded that while Bankart repair in the setting of a substantial bone loss conferred adequate stability in ABD and ER, it did so at the cost of overtightening the anterior structures which limited ER and did not affect stability in IR when the anterior capsuloligamentous structures are lax.
Burkhart et al. (2007) concluded that in the setting of significant glenohumeral bone deficiency, an open Latarjet procedure had only a 4.9% recurrence rate as compared to a 67% recurrence rate following arthroscopic Bankart repair. The Latarjet procedure works to extend the bony glenoid concavity, provide a dynamic sling from the conjoint tendon, preserve the lower third of the subscapularis and repair the capsule.
Figures A and B are the axial CT scan and 3D reconstruction en face view of the glenoid demonstrating significant anteroinferior glenoid bone loss of approximately 40%. Illustration A is an algorithm for the management of anterior shoulder instability based on pertinent risk factors and glenohumeral bone loss. Illustration B compares non-engaging and engaging Hill Sachs lesions. Size and depth of the Hill-Sachs lesion as well as glenoid bone deficiency both contribute to risk of engagement. Illustration C depicts a simplistic version of the Latarjet procedure.
Incorrect Responses:
Question 78
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 79
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
Question 80
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
REFERENCES: Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417.
D’Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Pearl ML, Bessos K, Wong K: Strength deficits related to distal biceps tendon rupture and repair: A case report. Am J Sports Med 1998;26:295-296.
Question 81
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.
Question 82
Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?

Explanation
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise pulley function.
Question 83
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
REFERENCES: Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, et al: Toddler’s fracture: Presumptive diagnosis and treatment. J Pediatr Orthop 2001;21:152-156.
Oudjihane K, Newman B, Oh KS, et al: Occult fractures in preschool children. Trauma 1988;28:858-860.
Question 84
What is the theoretical advantage of an open subpectoral technique of tenodesis of the long head of the biceps tendon compared to arthroscopic soft-tissue tenodesis techniques? Review Topic
Explanation
Question 85
During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the
Explanation
REFERENCES: Wasielewski RC, Cooperstein LA, Kruger MP, et al: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508.
Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws.
J Bone Joint Surg Am 1990;72:509-511.
Question 86
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 87
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
REFERENCES: Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 88
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 89
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 90
Which of the following techniques is most commonly used to classify tissue type in soft-tissue tumors?
Explanation
Question 91
When performing a Kocher approach to the radial head for open reduction internal fixation the forearm is held in pronation. What structure is this maneuver attempting to protect?

Explanation
Question 92
A 40-year-old woman is admitted to the hospital with a history of new-onset right lower extremity weakness resulting in frequent falls. She reports that a few weeks prior to the onset of the lower extremity symptoms, she experienced an episode of acute back pain, which has since resolved. Examination reveals 1-2/5 strength in the right hip flexors, abductors, and quadriceps. There is 0-1/5 strength

Explanation
(SBQ12SP.39) Which of the following is associated with increased risk of surgical site infection following lumbar spinal decompression? Review Topic
Use of intra-wound vancomycin powder
Hair removal by clipping at the time of surgery
Use of morphine nerve paste applied to the dura after spinal decompression
Skin preparation with an alcohol-based prep solution rather than povidone iodine
Failure to use chlorhexidine gluconate wash the night prior to surgery
The use of morphine nerve paste applied to the dura after decompressive spine surgery has been used in an effort to mitigate postoperative pain but has been associated with epidemic levels of surgical site infection.
Surgical site infection risk is modulated by a myriad of factors, both host factors and perioperative factors. Perioperative strategies to reduce infection that have been shown to be effective include: 1) hair removal by clipping (not shaving) at the time of surgery, 2) use of an alcohol based skin preparation agent, 3) use of perioperative prophylactic antibiotics, 4) limiting operating room traffic from OR personnel.
Kramer et al. did a retrospective analysis of 148 patients who underwent laminectomy in order to identify risk factors for infection in the context of a sudden increase in infections. Regression analysis showed that use of morphine paste resulted in an 18-fold increase in the risk of surgical site infection. 17 of 148 had developed infection during the epidemic period, compared to 15/995. Cultures were positive in 10 of 16 cases; 7 of these involved skin flora. Histological exam showed foreign body reaction.
Devin et al. did a multi-center analysis of patients undergoing spine surgery at seven spine centers to determine whether there was a difference in infection risk based on whether or not intra-wound vancomycin was used. They analyzed 2056 patients, of whom 47% had vancomycin used in their wounds. The risk of surgical site infection was higher in those patients that did not have vancomycin (relative risk 2.5).
Incorrect answers:
Question 93
A year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 94
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of
Explanation
REFERENCES: Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Cavolo DJ, Sherwood GF: Dupuytren’s disease of the plantar fascia. J Foot Surg 1982;21:12-15.
Question 95
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 96
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Explanation
REFERENCES: Levine AM: Traumatic spondylolisthesis of the axis (Hangman’s fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 97
Figures 15a and 15b are the radiographs of a 28-year-old man who fell from a height and sustained an isolated closed diaphyseal femur fracture that was treated with reamed antegrade femoral nailing 8 months ago. He now reports persistent pain during ambulation. He smokes one pack of cigarettes per day but is otherwise healthy. He denies any infectious history or symptoms, and laboratory studies show a normal WBC count, erythrocyte sedimentation rate, and C-reactive protein. What is the most appropriate treatment?

Explanation
Question 98
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Explanation
REFERENCES: Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasty. J Bone Joint Surg Am
1999;81:831-843.
Christie J, Burnett R, Potts HR, Pell AC: Echocardiography of transatrial embolism during cemented and uncemented hemiarthroplasty of the hip. J Bone Joint Surg Br 1994;76:409-412.
Question 99
14A 14B An 18-year-old man was involved in an altercation during which he sustained the injuries shown in Figures 14a and 14b. His Glasgow Coma Scale (GCS) score is 11 (a GCS score of 9-12 indicates moderate head injury). The neurosurgeons elect to not place an intracranial pressure (ICP) monitor. The patient responds appropriately to stimuli and is hemodynamically stable. What is the most appropriate initial treatment?

Explanation
Although management of femoral shaft fractures in patients with head injuries remains controversial, most practitioners agree that "damage-control principles" are appropriate for patients with evolving head injuries. This patient has a subarachnoid hemorrhage and a decreased GCS but is responding appropriately. The best treatment is a damage-control approach for the femur that will cause minimal blood loss and allow the brain injury (and swelling) to equilibrate. External fixation can be performed expeditiously and with minimal blood loss, which will reduce further injury to the brain. Special attention should be paid to maintaining cerebral perfusion pressure higher than 70 mmHg. Admission to the intensive care unit is recommended for monitoring of this injury. Knee immobilizers are not tolerated well by young muscular men with femur shaft fractures. A GCS score of 11 or higher can be observed without ICP monitoring.
RECOMMENDED READINGS
Flierl MA, Stoneback JW, Beauchamp KM, Hak DJ, Morgan SJ, Smith WR, Stahel PF. Femur shaft fracture fixation in head-injured patients: when is the right time? J Orthop Trauma. 2010 Feb;24(2):107-14. PubMed PMID: 20101135. View Abstract at PubMed
Roberts CS, Pape HC, Jones AL, Malkani AL, Rodriguez JL, Giannoudis PV.Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect. 2005;54:447-62. Review. PubMed PMID: 15948472. View Abstract at PubMed
Question 100
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?
Explanation
REFERENCES: Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135.
Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Galante A: Facial trauma, in Baker CL (ed): The Hughston Clinic Sports Medicine Book. Baltimore, MD, Williams & Wilkins, 1995, p 121.
