Orthopedic Surgery Board Review MCQs: Foot, Fracture, Hip, Infection, Shoulder | Part 129

Key Takeaway
This page offers Part 129 of an interactive MCQ set for orthopedic surgeons preparing for AAOS and ABOS board certification exams. Authored by Dr. Mohammed Hutaif, it features 100 high-yield, verified questions on Foot, Fracture, Hip, Infection, and Shoulder, designed for comprehensive board exam preparation.
About This Board Review Set
This is Part 129 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 129
This module focuses heavily on: Foot, Fracture, Hip, Infection, Shoulder.
Sample Questions from This Set
Sample Question 1: Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?...
Sample Question 2: Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The ...
Sample Question 3: Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to res...
Sample Question 4: A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsu...
Sample Question 5: Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
REFERENCES: Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 2
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?
Explanation
REFERENCES: Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.
Buckley RE, Tough S: Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg 2004;12:172-178.
Question 3
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 4
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 5
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 6
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 7
03 Fig 51c. What laboratory finding is most likely associated with this disease entity?
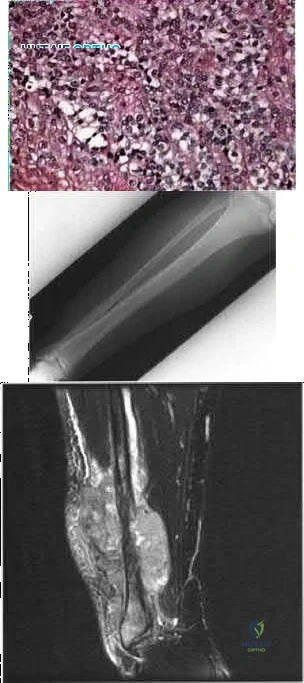
Explanation
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Inst Course Lect 2002;51:413-428
back to this question next question
Question 8
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
Question 9
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 10
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
Explanation
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Small SA, Perron AD, Brady WJ: Orthopedic pitfalls: Cauda equina syndrome. Am J Emerg Med 2005;23:159-163.
Question 11
A 30-year-old man has had leg pain for 6 months. A lesion is identified in the proximal femur and biopsy it taken. Histology is shown in Figure A and is consistent with a low-grade intramedullary osteogenic sarcoma. Additional imaging studies confirm that this is an isolated lesion with no metastasis. What is the standard treatment for this type of lesion?
Explanation
Choong et al. reviewed the long term follow-up of 20 patients diagnosed with low grade osteogenic sarcoma and found the 5 year survival rate was 90% and at 10 years was 85%. Local recurrence is a key feature in most cases and is typically the result of inadequate surgical margins frequently arising from initial misdiagnosis. Although amputation generally is successful for primary and recurrent tumors, limb salvage surgery is a definite option.
Kurt et al reviewed 80 well-differentiated osteosarcomas. They found local excision was almost always associated with recurrence. Wide excision was
almost never followed by recurrence. The recurrent tumor was a high-grade, conventional osteosarcoma in 15% of the patients, and this was associated with a poor prognosis. They recommend wide excision as the treatment of choice for this very rare variant of osteosarcoma.
A 32-year-old male sustains a the injury shown in Figure A after a high-speed motor vehicle collision. Which factor has been found to have the highest direct correlation with severe heterotopic ossification after traumatic knee dislocation?

Injury Severity Score (ISS )
Glascow Coma Scale (GCS )
Timing of knee reconstruction
Number of ligaments reconstructed
Open ligament reconstruction
Figure A shows a knee dislocation with cruciate ligament avulsion injuries. Development of significant heterotopic ossification (HO) formation has been shown to be most directly correlated to the ISS score.
Mills and Tejwani looked at multiple variables including injury severity score
( ISS), Glascow coma scale (GCS), closed head injury (CHI), timing of surgery (> or < 3 weeks) and type of surgery (open vs. arthroscopic, number of ligaments reconstructed) in its relation to the formation of HO following knee dislocation. In the final group the sensitivity and specificity of the ISS in relation to HO formation was 100%, while presence of CHI had a specificity of 97 %. Timing, type of surgery and approach did not influence HO formation.
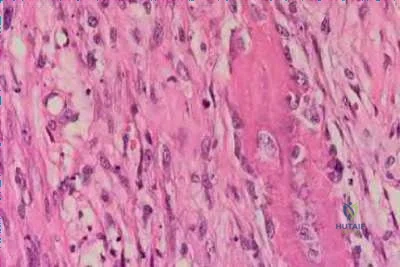
A 52-year-old male presents with 6 months of swelling and pain in his leg. He states the lesion has not changed in size for several months and doesn't bother him. He is otherwise healthy and has no other complaints. Representative photograph and MRI are shown in Figures A through C. What is the best initial step in his management?
Follow-up in 6 months with repeat radiographs
Biopsy
Marginal excision
Radiation therapy
Neoadjuvant chemotherapy and wide excision
The initial step in management of a patient presenting with a large soft tissue mass deep to the fascia is to obtain a tissue diagnosis, via biopsy. Initiation of treatment prior to tissue diagnosis is inappropriate and can result in significant patient morbidity and potential mortality. While some soft tissue sarcomas may benefit from chemotherapy, this cannot be initiated prior to diagnosis.
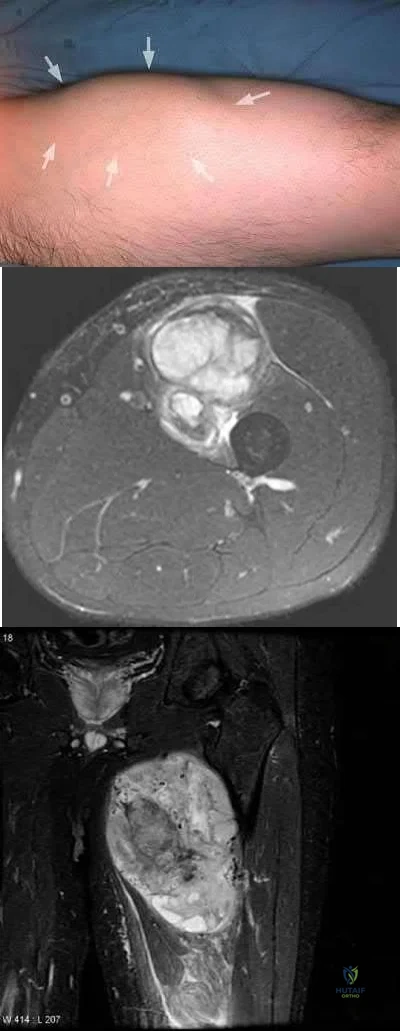
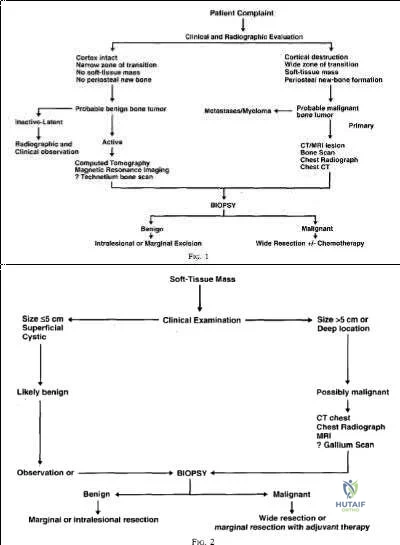
Radiation therapy is used in the treatment of soft tissue sarcoma, but again, only after tissue diagnosis. Peabody et al review the appropriate evaluation and staging for musculoskeletal neoplasms and present flow-charts useful in the work-up of bone (Illustration A) and soft tissue (Illustration B) neoplasms. Skrzynski et al performed a comparison of outpatient core-needle biopsy with open surgical biopsy for musculoskeletal tumors. They found the diagnostic accuracy of core-needle biopsy was only 84% with many samples yielding no or different histological samples when compared to final resected specimens. They conclude that while core-needle biopsy is significantly less expensive
than surgical biopsy ($1106 vs. $7234), there is higher concern for sampling error or general diagnostic inaccuracy associated with a core-needle biopsy compared to open biopsy, the "gold standard".
What is the appropriate treatment for a 10-year-old boy with Ewing's sarcoma isolated to the proximal femur?
Neoadjuvant chemotherapy and surgical excision
Neoadjuvant chemotherapy, surgical excision, and radiation therapy
Neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy
Neoadjuvant radiation therapy and surgical excision
Surgical excision and hormonal therapy
Ewing's sarcoma is a malignant small round blue cell neoplasm which has a predilection for long tubular bones, pelvis, and ribs. The radiographic appearance of "onion-skinning" seen in illustrations A and B is due to the body's periosteal reaction. Illustration C shows the large soft tissue extraosseous mass characteristic for Ewing's sarcoma. Finally, Illustration D shows the histology where the multiple small round blue neoplastic cells are seen.
Ewing's sarcoma is most commonly treated with neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy - in particular for tumors located in bones which can be easily resected and reconstructed. For large tumors in areas which either cannot be completely excised or where excision is associated with significant morbidity, some centers consider chemotherapy and radiation therapy without surgical excision. There is a current trend towards surgical resection and away from irradiation for Ewing's sarcoma even though it is radiosensitive, because of the risk of secondary malignancy and growth disturbance due to radiation.
Pierz et al review many of the common bone tumors including Ewing's sarcoma and discuss the relevant diagnostic factors as well as specific treatment protocols for each tumor.

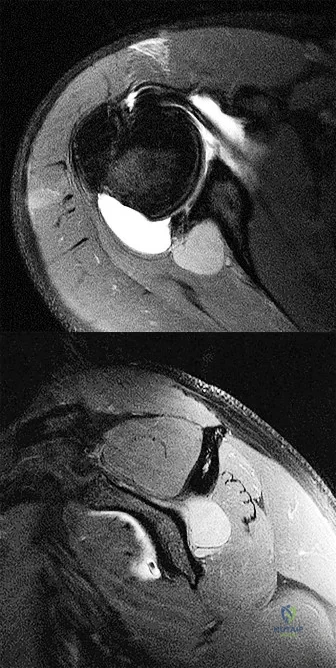
A 30-year-old female presents with a painful posterior knee mass. The mass gets larger and more painful with activity. Examination reveals a boggy soft tissue mass about her knee. Radiograph and MRI are shown in Figures A and B. What is the most likely diagnosis?

Synovial sarcoma
Hemangioma
Lipoma
Parosteal osteosarcoma
Pigmented villonodular synovitis (PVNS )
This patients history, physical exam, and imaging studies are suggestive of a hemangioma. Pain in hemangiomas is thought to occur due to vascular engorgement secondary to activity and increased blood flow to the lesion. The calcification on the plain radiograph and the fat of the T1 MRI are diagnostic for hemangioma. Current treatment for symptomatic hemangiomas includes some combination of sclerotherapy or vascular coiling, with surgical excision
reserved for few cases. The two attached reviews by Gilbert et al and Damron et al review the history, diagnosis, treatment, and controversial issues in soft tissue sarcomas and benign sarcoma like conditions such as hemangiomas.
Current treatment for soft tissue sarcomas includes radiotherapy and surgical excision. While many centers in the world use chemotherapy for soft tissue sarcomas, the data supporting its use is quite limited and likely too controversial to be tested. With regard to the other answer choices, synovial sarcoma and lipoma can show calcification on radiographs, but they are usually not painful and image differently on T1 MRI. Parosteal osteosarcoma typically occurs in this location (posterior distal femur) but occurs as a lesion stuck on the bone. PVNS can have a similar appearance on imaging, but doesn't cause this type of pain.
Question 12
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively
Explanation
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 13
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
Explanation
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
Question 14
What is the most likely contributory factor to this patient's problem?
Explanation
Proximal humeral epiphysiolysis (little leaguer’s shoulder) is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Factors that contribute to the condition include excessive throwing, improper throwing mechanics, and muscle-tendon imbalance. Radiographic findings typically are normal but may indicate subtle widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms. Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to throwing is implemented until the patient’s condition returns to baseline. This protocol has a long-term success rate exceeding 90%. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The most common cause of this condition is overuse, as is seen in pitchers who throw all year. Internal rotation deficit and internal impingement is typically a finding in older athletes without open physes. This patient had no evidence of rotation deficit upon examination, making this diagnosis unlikely.
Question 15
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
Schwend RM, Hennrikus W, Hall JE, et al: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 16
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 17
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 18
Elbow distraction interposition arthroplasty may be most appropriate treatment for which of the following patient profiles? Review Topic
Explanation
Question 19
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
REFERENCE: Wagner L, Archer B: Minimizing Risks from Fluoroscopic X-rays: A Credentialing Program for Anesthesiologists, Cardiologists, Surgeons, Radiologists, and Urologists, ed 3. The Woodlands, TX, Partners in Radiation Management, 2000.
Question 20
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 21
A 19-year-old linebacker for a collegiate football team has had two episodes of bilateral arm tingling and weakness after tackling; the symptoms resolved after 30 minutes of rest. Three follow-up neurologic examinations have been normal. Cervical spine CT and MRI scans are shown in Figures 13a through 13c. What is the next best step in management?
Explanation
REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
Question 22
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Explanation
Question 23
- A 32-year-old man has swelling of the knee as a result of falling with the knee flexed and his foot in plantar flexion. A Lachman’s test reveals an apparent increase in anterior translation. Passive external tibial rotation at 30 degrees and 90 degrees is equal to the contralateral side, and the quadriceps active test is positive on the affected side. The neurovascular examination is normal. Treatment should consist of
Explanation
Question 24
A patient sustains a severe lower extremity injury. What can be said about his outcome at 2 years if he chooses reconstruction over amputation?

Explanation
Bosse et al found that at 2 years the SIP score and return to work were not statistically signficantly different between amputation and reconstruction groups. Reconstruction patients had a higher risk of rehospitalization. The psychosocial subscale of SIP did not improve with time. Risk factors for poorer SIP score were: rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), smoking, and involvement in disability-compensation litigation.
MacKenize et al evaluated factors influential in returning to work (RTW) after severe lower extremity injury. Characteristics that correlated with higher rates of RTW included younger age, higher education, higher income, the presence of strong social support, and employment in a white-collar job that was not physically demanding. Receipt of disability compensation had a strong negative effect on RTW.
Question 25
A 50-year-old woman reports a burning sensation on the plantar aspect of her left forefoot, distal to the metatarsal heads between her third and fourth digits. Palpation of the third web space recreates her symptoms. Which of the following will most accurately aid in confirming a diagnosis?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 145-151.
Quinn TJ, Jacobson JA, Craig JG, et al: Sonography of Morton’s neuromas. Am J Roentgenol 2000;174:1723-1728.
Question 26
A 10-month-old boy has multiple skeletal lesions and a skin rash that he has had since he was a newborn. Based on the radiographs and biopsy specimens shown in Figures 79a through 79d, what is the most likely diagnosis?
Explanation
REFERENCES: Plasschaert F, Craig C, Bell R, et al: Eosinophilic granuloma: A different behaviour in children than in adults. J Bone Joint Surg Br 2002;84:870-872.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 857-876.
Question 27
Which of the following statements most accurately describes the layers of articular cartilage?
Explanation
REFERENCE: Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM (eds): Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995,
pp 95-101.
Question 28
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 29
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Explanation
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 30
A 40-year-old woman with history of intravenous drug abuse and ongoing Staphylococcus aureus septicemia is referred for intractable neck pain with radiation down her arm. She also complains of progressive hand weakness. Examination reveals long tract signs in the lower extremities. Her MRI scan is shown in Figure A. Besides intravenous antibiotics, what is the most appropriate next step in treatment? Review Topic
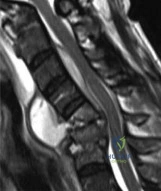
Explanation
Spinal epidural abscesses are more common in immunodeficient patients and IV drug abusers. They result in verebral body destruction and instability. In addition to draining the abscess and necrotic bone, the instability has to be addressed by instrumentation and fusion, even in the face of infection. Structural support can include cages with morselized bone graft, or structural allograft fixation of anterior and middle column and/or pedicle screw instrumentation of the posterior column.
Shousha et al. reviewed the treatment of cervical spondylodiscitis in 30 patients. They found an epidural abscess in 80% of patients, and noncontiguous discitis in 47% of cases. Thus, they recommend MRI of the entire spine in all cases, and surgery for intractable neck pain, septicemia, epidural abscess, neurological compromise, gross
kyphotic deformity with extensive destruction, and failure of conservative treatment.
Heyde et al. reviewed cervical spondylodiscitis in 20 patients. All cases had postoperative antibiotic therapy for 8–12 weeks. At 37 months (range 24–63), all cases went on to union and there were no recurrences of infection. There was improvement in preoperative neurological status in all cases, leading them to recommend early surgical intervention.
Figure A is an MRI scan showing spondylodiscitis C5–C7 with partial destruction of the vertebral bodies and epidural abscess formation. Illustration A shows the lateral xray (left) and MRI (right) of the same patient 9 months postoperatively after corpectomy C5 and C6 and posterior instrumentation.
Incorrect
Question 31
What is the most likely type of pathology seen in Figure 16?
Explanation
REFERENCES: McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Charlton OP, Martinez S, Gehweiler JA Jr: Pedicle thinning at the thoracolumbar junction: A normal variant. Am J Roentgenol 1980;134:825-826.
Question 32
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
REFERENCES: Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 33
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
REFERENCES: Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Question 34
A resident arrives to the operating room late for a LEFT carpal tunnel release procedure. The patient is prepped and draped under general anaesthesia, and the attending surgeon and assistant are about to make an incision to the RIGHT carpal tunnel. The resident mentions to the attending surgeon that surgery was booked for the opposite limb, but he ignores the residents confers by saying the surgical mark is under the drape. What would be the most appropriate course of action for the resident at this time? Review Topic
Explanation
Wrong-site surgery is completely preventable by having the surgeon, in consultation with the patient when possible, place his or her initials on the operative site using a permanent marking pen and then operating through or adjacent to his or her initials. The intended site should be marked such that the mark will be visible after the patient has been prepped and draped. A "time-out" procedure should be done before the initiating of any surgical procedure to confirm the type of procedure, site, and side with all operating room personnel including residents.
Haynes et al. reviewed the effect of surgical safety checklists before surgery on the morbidity and mortality in a global population. They found the rate of death was 1.5% before the checklist was introduced and declined to 0.8% afterward (P=0.003). Inpatient complications occurred in 11.0% of patients at baseline and in 7.0% after introduction of the checklist (P<0.001).
Incorrect Answers:
Question 35
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 36
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 37
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common source of surgical failure?
Explanation
Question 38
The optimal method with which to diagnose component malrotation in total knee arthroplasty (TKA) is
Explanation
The epicondylar axis and tibial tubercle can be used as references on CT scans to quantitatively measure rotational alignment of the femoral and tibial components. This technique has been used to determine whether rotational malalignment is present and whether revision of 1 or both components may be indicated. Although clinical assessment is useful, malrotation can occur as a result of deformities unrelated to the arthroplasty. Similarly, an isolated radiographic skyline view of the patella may indicate a problem with patellar maltracking, but cannot quantitatively assess malrotation of the components. MR imaging proves useful for evaluating painful TKA, but it is dependent on the center’s quality and has not yet been shown to quantify component malrotation.

CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 22
Figures 20a and 20b are the radiographs of an elderly woman who underwent total knee arthroplasty (TKA) several years ago. She now states that something is not right; her knee frequently swells and is diffusely painful, especially at the end of the day. She does not trust her knee, especially while going up and down stairs or getting up from a chair.
Question 39
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?
Explanation
REFERENCES: Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Samson IR, Springfield DS, Suit HD, Mankin HJ: Operative treatment of sacrococcygeal chordoma: A review of twenty-one cases. J Bone Joint Surg Am 1993;75:1476-1484.
Question 40
Deep anterior compartment
Explanation
Question 41
After performing a total hip arthroplasty through a posterolateral approach, an orthopaedic surgeon is unable to adequately externally rotate the leg and subsequently exposes the anterior capsule. When releasing the inferior aspect of the anterior capsule, pulsatile bleeding is encountered. A branch of which artery is most likely lacerated?
Explanation
Branches of the lateral femoral circumflex artery arise from the inferior aspect of the anterior hip capsule. They can be injured when removing the anterior capsule from any approach. The inferior gluteal artery supplies the gluteus maximus. The medial femoral circumflex artery enters the hip joint along the path of the obturator externus tendon. The femoral artery crosses the anterior hip joint in the superior-to-inferior direction and is located just medial to the hip joint.

Question 42
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
REFERENCE: Schmade GA, Conrad EV III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
Question 43
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of
Explanation
REFERENCES: Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-76.
Question 44
Deep posterior compartment
Explanation
The structures at risk are the anterior tibial artery and deep peroneal nerve in the anterior compartment, superficial peroneal nerve in the lateral compartment, sural nerve in the superficial posterior compartment, and posterior tibial nerve and posterior tibial and peroneal arteries and veins in the deep posterior compartment.
Question 45
Ceramic bone substitutes have which of the following properties?
Explanation
REFERENCES: Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 46
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 47
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 48
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 49
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 50
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 51
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 52
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 53
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
REFERENCES: Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Hawkins RJ, Switlyk P: Acute prosthetic replacement for severe fractures of the proximal humerus. Clin Orthop 1993;289:156-160.
Question 54
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
REFERENCES: Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 421-454.
Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 55
An 80-year-old patient presents 8 months postoperatively with right groin pain. Examination reveals a leg length discrepancy of 1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
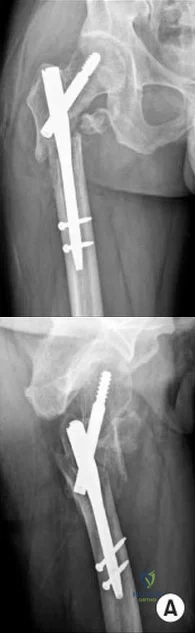
Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
(SBQ12TR.48) A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation
as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?

Age less than 30
Marijuana use
Use of negative pressure wound therapy
Male gender
Ability to return to work
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or
limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
1-4: These options are not as strong of a factor of patient satisfaction in long-term follow up after trauma-induced lower extremity amputation.
Question 56
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
Question 57
Figures 38a and 38b are the MRI scans of a 28-year-old man who reports progressively worsening severe back pain for the past 3 months. He denies fevers, chills, weakness, or neurologic dysfunction. Examination reveals tenderness to palpation over the lumbar spine but normal neurologic findings. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein; blood cultures are positive for methicillin-sensitive Staphylococcus aureus. In addition to intravenous antibiotics, what is the next step in management? Review Topic

Explanation
Question 58
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
Marmor L, Bechtal CO: Paralysis of the serratus anterior due to electric shock relieved by transplantation of the pectoralis major muscle: A case report. J Bone Joint Surg Am 1983;45:156-160.
Question 59
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as Review Topic
Explanation
Question 60
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
REFERENCES: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Question 61
- An infected total knee replacement with symptoms occurring within 4 weeks of surgery and no radiographic signs of osteomyelitis would be best managed with
Explanation
Arthroscopic debridement not recommended secondary to missing cutaneous tracks and soft tissue/muscle involvement.
Question 62
- A 13-year-old quarterback feels a “pop” in his knee while being tackled. Radiographs of the knee and results of a Lachman’s test are normal. Examination reveals tenderness over the distal femoral physis. To help confirm the diagnosis, management should first include
Explanation
Question 63
A 45-year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 64
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 65
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 66
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 67
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
Explanation
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
Sclerosis of the proximal femoral epiphysis with subchondral lucency
Abnormal femoral head-neck junction offset
Widening of the proximal femoral physis with normal femoral head-neck junction offset
Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
Question 68
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Chauveinc L, Mosseri V, Quintana E, Desjardins L, Schlienger P, Doz F, Dutrillaux B: Osteosarcoma following retinoblastoma: Age at onset and latency period. Ophthalmic Genet 2001;22:77-88.
Question 69
Figures 1 and 2 show the radiographs obtained from a 56-year-old man who has been experiencing progressive wrist pain since he felt a pop while throwing a 25-pound bag over his shoulder 6 months ago. Failure to address the injury surgically might lead to progressive arthritic changes in what order?

Explanation
This patient demonstrates scapholunate dissociation with an associated dorsal intercalated segment instability deformity. Chronic scapholunate ligament tears lead to scapholunate advanced collapse (SLAC) wrist. Watson and Ballet describe SLAC wrist as having a predictable progression of arthritic changes, starting at the radial styloid, progressing to the radioscaphoid joint, and advancing to the lunocapitate joint. Some authors have described the radiolunate joint as being affected in very late-stage SLAC wrist.
Question 70
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of Review Topic
Explanation
Question 71
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared to a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.

RESPONSES FOR QUESTIONS 58 THROUGH 62
Nerve palsy
Skin necrosis
Flexion instability
Patellar instability
Anterior knee pain
Malalignment
Total knee arthroplasty (TKA) is performed to address each condition shown in Figures 58 through 62b. Which complication is most commonly associated with each image?
Question 72
Which of the following is not a cause of childhood osteomalacia (rickets)?
Explanation
Question 73
A 58-year-old patient suddenly develops cardiac arrest while undergoing a routine total knee arthoplasty. He is resuscitated with 20% lipid emulsion. What was the most likely causative agent for cardiac arrest?
Explanation
Bupivacaine is a long acting local anesthetic. It acts on intracellular voltage-gated sodium channels to block sodium influx into nerve cells, which prevents depolarization. If administered systemically, bupivacaine can cause serious complications to the cardiovascular system. Side effects include hypotension, arrhythmia, bradycardia, heart block, and cardiac arrest. Treatment should involve urgent administration of intravascular lipid emulsion alongside standard ACLS protocols.
Rosenblatt et al. describe the successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Resuscitation involved a lipid emulsion bolus of 1 mL/kg given immediately, which was followed by a continuous infusion until the patient stabilized.
Corman et al. evaluated the use of lipid emulsion for reversal of local anesthetic-induced toxicity. They suggest that lipid emulsion may reverse local anesthetic toxicity by extracting lipophilic local anesthetics from aqueous plasma or tissues or by counteracting local anesthetic inhibition of myocardial fatty acid oxygenation.
Illustration A shows an ECG of a patient with clinical deterioration after systemic administration of bupivicaine. The ECG shows complete heart block with multifocal ventricular beats. The patient progressed to asystole.
Inncorrect Answers:
Question 74
A 66-year-old woman with known poorly controlled rheumatoid arthritis reports that for the past 4 weeks she has been unable to extend the metacarpophalangeal (MCP) joints of her right hand index, middle, ring and little fingers. She cannot hyperextend the thumb interphalangeal joint. Active wrist extension is possible, but shows radial deviation. Examination reveals mild synovitis at the wrist and MCP joints of the affected hand. There is no ulnar deviation at the MCP joints with normal alignment. When the MCP joints are passively extended, the patient is unable to maintain them in this position. There is no piano key sign at the distal ulna. Passive wrist motion shows a normal tenodesis effect. Which of the following would most likely confirm your diagnosis? Review Topic
Explanation
Question 75
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?

Explanation
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
Question 76
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Hays DM: Rhabdomyosarcoma. Clin Orthop 1993;289:36-49.
Question 77
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 78
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 79
For a patient with a type II odontoid fracture, which of the following factors best predicts the development of a nonunion with nonsurgical management? Review Topic
Explanation
Question 80
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 81
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
Explanation
REFERENCE: Opinions on ethics and professionalism, in Guide to The Ethical Practice of Orthopaedic Surgery, ed 6. American Academy of Orthopaedic Surgeons, Rosemont, IL, 2006, pp 38-42.
Question 82
The usual presentation of traumatic subscapularis tears is most often seen after forced Review Topic
Explanation
Question 83
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 84
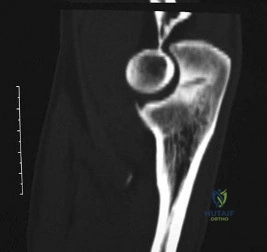
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room. Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present? Review Topic
Explanation
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3).
Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
Question 85
An adult patient with a grade I isthmic spondylolisthesis at L5-S1 is most likely to have weakness of the
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.
Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208.
Question 86
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries. Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
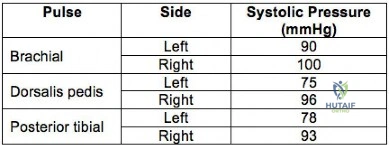
Explanation
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI
<0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Question 87
-A 14-year-old girl has a painless deformity of the right tibia. A radiograph from 2 years ago is seen in Figure a; nothing was done at that time. Her current radiograph is seen in Figure b. She has no pain, fever, or drainage. What is the most likely diagnosis?

Explanation
Question 88
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 89
After completion of bone cuts and ligament balancing of a severe valgus knee during primary total knee arthroplasty, there is a 5-mm increased medial gap that cannot be corrected. In this scenario, what is the most appropriate level of constraint?
Explanation
Cruciate-retaining implants are typically used in the presence of a functioning posterior cruciate ligament (PCL). A posterior stabilized insert improves anteroposterior stability in the absence of a PCL but does not account for imbalance of the collateral ligaments. An
uncorrectable laxity medially indicates insufficiency of the medial collateral ligament (MCL), which is best treated with a varus-valgus constrained component. A rotating hinge is generally reserved for complete absence of the MCL or both collateral ligaments.
Change of IV antibiotics and splinting
Arthroscopic irrigation and debridement
CT-guided needle aspiration
Open debridement
DISCUSSION
In an acutely febrile child with bone pain and elevated acute-phase reactants, osteomyelitis is suspected. Blood cultures will yield the offending organism in 30% to 60% of patients and are the most appropriate next step. Knee aspiration in the absence of an effusion likely will not be helpful. Although a bone scan may show an osteomyelitic focus, an indium-labeled WBC scan is unnecessarily complex and costly in this case. Pelvic radiographs would add little to the unremarkable femur films.
Initiating IV antibiotics after obtaining blood cultures is appropriate, even in the presence of an MRI with normal findings. Observation or discharge may be considered, but suspicion for infection should be strong in this clinical situation and delay is not warranted. A CT scan of the knee in the setting of normal MRI findings will not be helpful.
Most hematogenous osteomyelitis cases among children are attributable to S. aureus. In many areas of the country, MRSA is endemic, and initial coverage for resistance is appropriate. The other listed organisms would rarely be seen in this scenario.
The MR images show early abscess formation in the distal medial femoral metaphysis. Because the formation developed during antibiotic treatment, surgical drainage (rather than a change of antibiotic) is appropriate. Arthroscopy is not helpful because this is not an intra-articular process. Although aspiration prior to surgical debridement could be considered, the organism has already been identified from the blood culture, and CT guidance is not needed to locate this large abscess in such an accessible area.
Question 90
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
Explanation
REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.
Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.
McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.
Question 91
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 92
Nutritional rickets in the US occurs more frequently in infants older than 6 months of age who do not receive vitamin D supplementation and are Review Topic
Explanation
Question 93
A 22-year-old man has mild hip pain bilaterally and multiple skeletal lesions. Based on the pelvic radiograph shown in Figure 30, what is the inheritance pattern for his disorder?
Explanation
REFERENCES: Stieber JR, Dormans JP: Manifestations of hereditary multiple exostoses. J Am Acad Orthop Surg 2005;13:110-120.
Hilton MJ, Gutierrez L, Martinez DA, et al: EXT1 regulates chondrocyte proliferation and differentiation during endochondral bone development. Bone 2005;36:379-386.
Question 94
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 95
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
Explanation
REFERENCES: Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863.
Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 96
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 97
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
REFERENCES: Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Aronow MS, Diaz-Doran V, Sullivan RJ, et al: The effect of triceps surae contracture force on plantar foot pressure distribution. Foot Ankle Int 2006;27:43-52.
Question 98
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone? Review Topic
Explanation
Question 99
At which joint do degenerative changes occur first in a patient with chronic, untreated scapholunate dissociation?
Explanation
Stage I of scapholunate advanced collapse (SLAC) is characterized by the presence of radioscaphoid arthritis. A predictable pattern exists of the progression of degenerative changes for SLAC wrist, including stage I (radial styloid involvement at the scaphoid fossa), stage II (scaphoid and entire scaphoid facet involvement), stage III (degeneration between the capitate and lunate), and stage IV (pancarpal involvement). The radiolunate joint is often spared.
Question 100
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
