Orthopedic Board Review MCQs: Elbow, Hip, & Nerve | Part 127

Key Takeaway
This page offers Part 127 of a comprehensive Orthopedic Surgery Board Review series. It features 100 high-yield MCQs designed for orthopedic residents and surgeons preparing for their OITE and AAOS certification exams, ensuring optimal board exam readiness with verified content and detailed explanations.
About This Board Review Set
This is Part 127 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 127
This module focuses heavily on: Arthroscopy, Elbow, Hip, Nerve.
Sample Questions from This Set
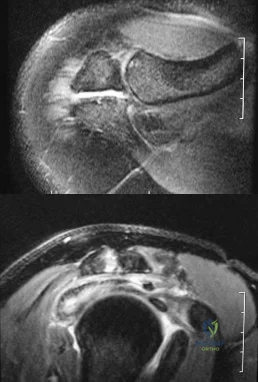
Sample Question 1: Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with amonth history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?...
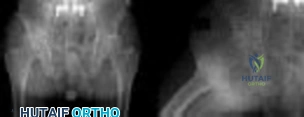
Sample Question 2: A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body...
Sample Question 3: Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with...
Sample Question 4: -An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 10...
Sample Question 5: In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 2
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
Question 3
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 4
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 5
In the most common condition causing a winged scapula, which of the following nerves is affected? Review Topic
Explanation
Question 6
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 7
-An absolute contraindication for closed management of a humeral shaft fracture in a fracture brace is
Explanation

Question 8
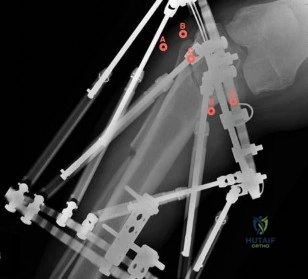
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 9
Anterior subluxation in a throwing athlete is most commonly the result of
Explanation
REFERENCES: Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
Question 10
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
Explanation
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
Question 11
A 19-year-old collegiate middistance runner has a 4-year history of bilateral leg pain. Pain begins within 10 minutes after starting to run and is described as a “tightness and cramping in the front of the legs.” Symptoms resolve within 15 to 20 minutes of running cessation. A presumptive diagnosis of exercise-induced compartment syndrome (EICS) is made, and the patient elects to undergo compartmental pressure testing. What is the strongest indication for elective fasciotomy of the anterior compartment?
Explanation
This clinical scenario describes a patient with EICS, marked by a nonphysiologic rise in muscle compartment pressure during exercise. Pressure testing is the best currently accepted method of diagnosis. Most physicians use the following criteria for diagnosis: resting pressure higher than 15 mm Hg, 1-minute postexercise pressure higher than 30 mm Hg, or 5-minute postexercise pressure higher than 20 mm Hg. Only 1-minute postexercise anterior compartment pressure of 42 mm Hg meets these criteria. Neurologic symptoms in the plantar foot would imply involvement of the posterior compartments and would not support the diagnosis of anterior compartment involvement.
Question 12
What is the second most common primary bone malignancy in children?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 13
A 9-year-old boy sustained a traumatic brain injury and right lower extremity trauma in an accident involving a motor vehicle and a pedestrian. Initial evaluation in the emergency department reveals an obtunded patient who is breathing spontaneously and withdraws appropriately to painful stimuli. After initial resuscitation and stabilization, a CT scan reveals a right parietal intracranial hemorrhage. Radiographs of the swollen right thigh are shown in Figures 32a and 32b. Management of the fractured femur should ultimately consist of
Explanation
35 patients with head injury. In one patient with hemiplegia and a urinary tract infection, a deep wound infection developed, necessitating nail removal. The remaining patients all healed without major complications. Heinrich and associates treated 78 diaphyseal femoral fractures with flexible intramedullary nails, including 14 with head injury. No major complications were reported and all fractures healed.
REFERENCES: Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996,
pp 83-95.
Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich MS, Drvaric DM, Darr K, et al: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatric Orthop 1994;14:501-507.
Canale ST, Tolo VT: Fractures of the femur in children. Instr Course Lect 1995;44:255-273.
Question 14
Which modality has the broadest application for the reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 15
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. Determining if a patient needs fasciotomies in the operating room while a patient is under anesthesia is complicated by the fact that obtaining a clinical exam is impossible, and that the diastolic blood pressure may be falsely decreased compared to normal pre- or postoperative measurements. Currently, it is recommended that intraoperative compartment pressures be compared to preoperative diastolic blood pressures, with delta p < 30 indicating the need for fasciotomies.
Kakar et al. review the preoperative, intraoperative, and postoperative diastolic blood pressure (DBP) in 242 patients with a tibia fracture treated operatively. They found the mean DBP was 18 points lower in the operating room compared to the preoperative measurement. In addition, they found the difference between preoperative and postoperative diastolic blood pressures to be within 2 points, indicating the decrease seen intraoperatively is likely a spurious value induced by anesthetic.
McQueen and Court-Brown prospectively review 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Incorrect Answers:
Question 16
A 47-year-old man undergoes a posterior cervical procedure for a benign tumor. Postoperatively, severe dysfunction with decreased forward elevation and abduction develops and he has lateral winging of the scapula. What is the recommended treatment to best restore motion and function? Review Topic
Explanation
Question 17
When performing hip arthroscopy, the hip should be placed in neutral to slight internal rotation to protect which of the following structures? Review Topic
Explanation
Question 18
Which of the following cannulated screw configurations used in the treatment of subcapital femoral neck fractures is optimal?

Explanation
Booth et al performed a cadaveric study comparing central versus calcar (cortical-adjacent) fixation. The results demonstrated significant improved stability, load, stiffness, and displacement in all tested parameters for the group with calcar-adjacent screw fixation.
Lindequist and Törnkvist performed a Level 4 study of 72 femoral neck fractures. They found that all 5 of their nonunions had screws placed greater than 3mm from the femoral calcar. Additionally, 16 of 18 fractures healed in the group of displaced fractures where both the fixating screws were placed within 3 mm from the femoral neck cortex.
Gurusamy et al performed a Level 4 study of 395 patients undergoing femoral neck fixation. They found a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture.
Illustration A depicts the optimal configuration of an inverted triangle with the single screw being inferior and all of the screws being cortical adjacent.
Question 19
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
REFERENCES: Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 20
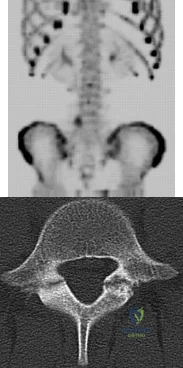
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 21
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?
Explanation
REFERENCE: Bertoni F, Bacchini P: Classification of bone tumors. Eur J Radiol
1998;27:S74-S76.
Question 22
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
REFERENCES: Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Tewes DP, Fischer DA, Fritts HM, et al: MRI findings of acute turf toe: A case report and review of anatomy. Clin Orthop 1994;304:200-203.
Question 23
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology? Review Topic
Explanation
Question 24
A 14-year-old male sustains the injuries shown in Figures A and B after a fall off the roof of his house. What is the most appropriate management? Review Topic

Explanation
Pediatric femoral neck fractures are classified into transphyseal, transcervical, cervicotrochanteric and intertrochanteric (Delbets I-IV) respectively. Fixation type varies by author, but generally speaking, Types I-III can be treated with smooth wires for patients 0-3yrs of age, 4.5-6.5 mm cannulated screws 4-10yrs of age, or l 6.5-
Question 25
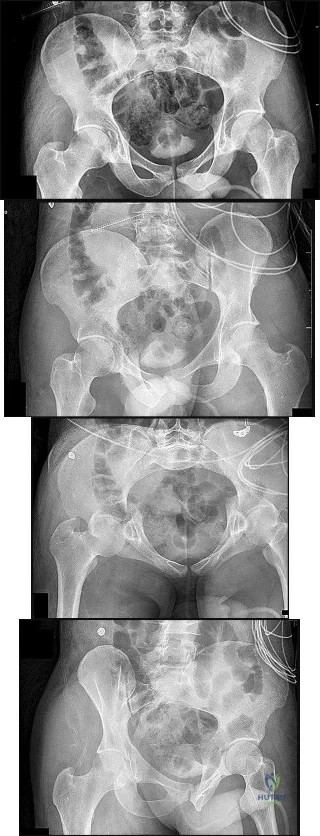
Figures 15a through 15d
Explanation
Plain radiographic imaging of a patient with an acetabular injury begins with 5 standard views of the pelvis (anteroposterior [AP], iliac oblique, obturator oblique, inlet, and outlet views). These views will show fractures of the acetabulum and help to evaluate for pelvic fractures and hip joint integrity. The obturator oblique view is taken with the injured side rotated 45 degrees forward with the beam centered on the patient’s affected hip. This shows the anterior column and posterior wall and will reveal if any posterior subluxation of the hip is present. The iliac oblique view is taken with the injured side of the patient rolled 45 degrees forward with the beam centered on the affected hip. This shows the posterior column and the anterior wall. Inlet and outlet pelvic radiographs may depict pelvic injuries such as sacroiliac joint fracture or widening.
Judet and Letournel have a classification system for acetabular fractures. The system consists of 5 elementary fracture patterns: anterior wall, anterior column, posterior wall, and posterior column fractures of the acetabulum and a transverse pattern. There are also 5 associated fracture patterns: posterior column/posterior wall, transverse/posterior wall, T-type, anterior column with hemitransverse fracture of the posterior column, and both-column fractures.
Figure 12b shows a fracture of the posterior column on the Iliac oblique, and Figure 12c shows a fracture of the posterior wall in the obturator oblique.
In Question 13, the figures only reveal a fracture of the posterior wall, and this is best appreciated in Figure 13c, the obturator oblique view.
The T-type fracture is a transverse fracture with a secondary fracture line extending inferiorly. This causes the anterior and posterior columns to be separated. The iliac oblique view, Figure 14b, shows a fracture extending through the posterior column. In the obturator oblique view (Figure 14c), the yellow arrow shows a fracture extending through the anterior column, and the red arrow shows a fracture extending inferiorly through the ischium.
Fractures extending through the anterior and posterior columns are seen, which represent a transverse fracture, but there is no extension inferiorly, which eliminates T-type as a possible correct response. The anterior column fracture is best seen on the inlet view (Figure 15b), but it also can be seen in Figure 15d, the obturator oblique view. Figure 15c shows the fracture through the posterior column. For this patient, a small fracture of the posterior wall is visualized on the AP view (Figure 15a).
RECOMMENDED READINGS
Dickson KF, Dowling RM. Treatment of pelvic and acetabular fractures in elderly patients. Orthopaedic Knowledge Online Journal. Volume 11, Number 8 August 2013.
Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. View Abstract at PubMed
Moed BR, Kregor PJ, Reilly MC, Stover MD, Vrahas MS. Current management of posterior wall fractures of the acetabulum. Instr Course Lect. 2015;64:139-59. Review. PubMed PMID: 25745901. View Abstract at PubMed
Question 26
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of
Explanation
REFERENCES: Lemos MJ: The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 1998;26:137-144.
Rockwood CA Jr, Green DP, Bucholz RW, et al: Fractures in Adults, ed 5. Philadelphia, PA, Lippincott-Raven, 2001, pp 1209-1240.
Question 27
A 9-year-old girl reports the immediate onset of severe groin pain and the inability to walk after tripping on a curb. Examination reveals marked hip pain with passive range of motion. A radiograph is shown in Figure 21. Regardless of treatment, what is the most common complication following this injury?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Rhoad RC, Davidson RS, Heyman S, et al: Pretreatment bone scan in SCFE: A predictor of ischemia and avascular necrosis. J Pediatr Orthop 1999;19:164-168.
Question 28
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of
Explanation
REFERENCES: Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Sharkey PF, Hozack WJ, Callaghan JJ, et al: Acetabular fracture associated with cementless acetabular component insertion: A report of 13 cases. J Arthroplasty 1999;14:426-431.
Question 29
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to surgery.
Question 30
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
Question 31
A 16-year-old competitive female swimmer has a 1-year history of left shoulder pain. She denies any specific injury to her shoulder. She reports that the pain is worse with swimming but also has pain with daily activities. She also notes similar occasional symptoms in her right shoulder. Examination reveals symmetric range of motion and rotator cuff strength. Examination of the left shoulder reveals 2+ anterior and posterior translation with pain in both directions and a 2-cm sulcus sign. The right shoulder also has 2+ anterior and posterior translation and a 2-cm sulcus sign with no pain. She also has hyperextension of the elbows and the ability to touch the radial border of her thumb to her forearm. What is the next step in management? Review Topic
Explanation
Question 32
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of
Explanation
REFERENCES: Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228.
Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Ziv I, Mosheiff R, Zeligowski A, Liebergal M, Lowe J, Segal D: Crush injuries of the foot with compartment syndrome: Immediate one-stage management. Foot Ankle 1989;9:185-189.
Question 33
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 34
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 35
Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
Explanation
REFERENCES: Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169.
Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Tornetta P III, Tiburzi D: Antegrade or retrograde reamed femoral nailing: A prospective, randomized trial. J Bone Joint Surg Br 2000;82:652-654.
Question 36
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
REFERENCES: Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 37
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension? Review Topic
Explanation
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
1-4: These structures are not primary restraints to internal tibial rotation in full extension.
Question 38
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 39
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 40
Which of the following is most commonly associated with an open clavicular fracture?
Explanation
REFERENCE: Taitsman LA, Nork SE, Coles CP, et al: Open clavicle fractures and associated injuries. J Orthop Trauma 2006;20:396-399.
Question 41
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?

Explanation
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette of the shoulder and is a stabilizer of the humeral head.
Question 42
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
REFERENCES: Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Itoi E, Kuelchle DK, Newman SR, Morrey BF, An KN: Stabilizing function of the biceps in stable and unstable shoulders. J Bone Joint Surg Br 1993;75:546-550.
Question 43
-What is the most likely deficit in elbow function resulting from an isolated lesion of the ulnar nerve above the elbow?
Explanation

Question 44
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
Explanation
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-
Question 45
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 46
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
Explanation
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.
REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.
Question 47
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
REFERENCE: Mont MA, Alexander N, Krackow KA, Hungerford DS: Total knee arthroplasty after failed high tibial osteotomy. Orthop Clin North Am 1994;25:515-525.
Question 48
A 56-year-old laborer sustained a subcoracoid dislocation of the shoulder as a result of falling off a scaffold 3 weeks ago. He now is unable to actively raise his arm and has constant pain. What is the most likely diagnosis?
Explanation
Question 49
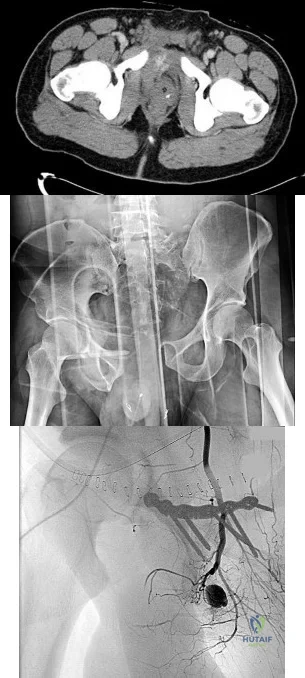
4A 4B 4C A 30-year-old man was involved in a high-speed motorcycle collision and sustained the injury shown in Figure 4a. Hypotension ensued shortly after arrival in the emergency department. Figure 4b is the initial contrast pelvic CT image with an unrecognized blush consistent with arterial bleeding. During surgical repair, the patient was noted to have active bleeding and an angiogram was obtained (Figure 4c). Which structure is the likely cause of his bleeding?
Explanation
Pelvic bleeding occurs predominantly from disruption of the posterior venous plexus and bleeding from the fractured bone. Occasionally arterial bleeding is seen, with injury to the superior gluteal artery most common. Anterior pelvic bleeding occurs from injury to the obturator artery (commonly from a pubic bone fracture laceration) and less frequently from the pudendal artery near the symphysis. The location of the bleeding on CT and angiography images does not correspond to the superior gluteal, external iliac, or femoral arteries.
RECOMMENDED READINGS
Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. 2009 Apr;40(4):343-53. Epub 2009 Mar 17. Review.PubMed PMID: 19278678. View Abstract at PubMed
Loffroy R, Yeguiayan JM, Guiu B, Cercueil JP, Krausé D. Stable fracture of the pubic rami: a rare cause of life-threatening bleeding from the inferior epigastric artery managed with transcatheter embolization. CJEM. 2008 Jul;10(4):392-5. PubMed PMID: 18652733. View Abstract at PubMed
White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures.Injury. 2009 Oct;40(10):1023-30. Epub 2009 Apr 16. Review. PubMed PMID:19371871. View Abstract at PubMed
RESPONSES FOR QUESTIONS 5 THROUGH 8

5A

5B
- Avascular necrosis, head collapse, and screw penetration
- Fixation failure and varus collapse
- Humeral stem loosening
- Glenoid component loosening
- Hardware failure (breakage of plate or screws)
- Shoulder dislocation
Please choose from the responses to identify the most likely complication in each scenario.
Question 50
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 51
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
REFERENCES: Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg
1992;1:238-245.
Question 52
03 A 26-year-old woman has chronic toe pain after hitting a bedpost 3 months ago. A radiograph is shown in Figure 27. Her injury represents an avulsion of the

Explanation
The EDB originates on the distal lateral and superior surface of the calcaneus and inserts on the
lateral aspect of the flexor digitorum longus tendon and also on to the base of the proximal phalanx of the first through fourth toes. There is no EDB tendon to the fifth toe. If an EDB laceration is easily identified at the time of an EDL repair, than it may be repaired as well, otherwise repair of the EDL alone is sufficient.
Heckman JD: Fractures and dislocation of the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds):Rockwood and Green’s Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 2166-2169.
Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 787-788.
back to this question next question
Question 53
Which of the following is the most relevant clinical factor in the maturation assessment of an adolescent female athlete contemplating anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Micheli LJ, Foster TE: Acute knee injuries in the immature athlete. Instr Course Lect 1993;42:473-481.
Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Fowler PJ: Anterior cruciate ligament injuries in the child, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2067-2074.
Question 54
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three- and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Robinson CM, Page RS, Hill RM, et al: Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am 2003;85:1215-1223.
Question 55
Figures 19a and 19b show the AP and lateral radiographs of an 18-year-old man who has had knee pain for 3 months. Figure 19c shows a histopathologic photomicrograph of the biopsy specimen. Which of the following factors is most likely to affect his survival?
Explanation
REFERENCES: Weis L: Common malignant bone tumors: Osteosarcoma, in Simon MA, Springfield DS (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlation. Philadelphia, PA, Lea and Febiger, 1989, pp 248-438.
Question 56
The humeral nonunion shown in Figure 27 is most likely to unite when using what method of treatment?
Explanation
REFERENCES: Pugh DM, McKee MD: Advances in the management of humeral nonunion.
J Am Acad Orthop Surg 2003;11:48-59.
McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 57
- What factor is most commonly associated with malignant transformation of a giant cell tumor?
Explanation
Question 58
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of
Explanation
REFERENCE: Peterson CA, Altchek DW, Warren RF: Shoulder arthroscopy, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 290-335.
Question 59
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
REFERENCES: Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44.
Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 60
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of
Explanation
REFERENCES: Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Lazar RD, Hall JE: Simultaneous anterior and posterior hemivertebra excision. Clin Orthop 1999;364:76-84.
Question 61
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?
Explanation
If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision.
REFERENCES: Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Bos GD, Esther RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 62
Which of the following is a true statement regarding thoracic disk herniations? Review Topic
Explanation
common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals.
Question 63
- A skeletal survey is more accurate than a bone scan for detecting skeletal involvement in which of the following neoplastic diseases?
Explanation
Question 64
A 75-year-old woman is undergoing a T10-S1 lumbar decompression and fusion for severe degenerative scoliosis. During the deformity corrective maneuver, intraoperative neuromonitoring revealed a sustained 80% decrease in somatosensory-evoked potential (SSEP) amplitudes. Appropriate lead placement and
Explanation
Question 65
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 66
Which of the following conditions is associated with palmoplantar pustulosis?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.
Question 67
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10° to 60°. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
REFERENCES: Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br
1989;71:498-500.
Ogilvie-Harris DJ, Saleh K: Generalized synovial chondromatosis of the knee: A comparison
of removal of the loose bodies alone with arthroscopic synovectomy. Arthroscopy
1994;10:166-170.
Question 68
Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population? Review Topic
Explanation
Question 69
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?
Explanation
REFERENCES: Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337.
Pichney GA, Derner R, Lauf E: Digital “V” arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 70
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. She has symmetric knee flexion, extension, and frontal alignment to her contralateral knee. She has a 1-cm limb-length discrepancy of the femur. She has always been in the 50th percentile for height and her skeletal age matches her chronologic age. She has a complete physeal closure of the right distal femur. What is the expected limb-length discrepancy at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
AL-Madena Copy
Question 71
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 72
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
Explanation
REFERENCES: Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Crockett HC, Gross LB, Wilk KE, et al: Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med 2002;30:20-26.
Question 73
A 74-year-old woman with rheumatoid arthritis has pain in the shoulder that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 24a and 24b. Active forward elevation is 120 degrees and external rotation is 30 degrees. At the time of surgery, a 1-cm rotator cuff tear is found, which is repairable. Which of the following treatment options will result in the most predictable pain relief and function? Review Topic

Explanation
Question 74
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 75
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 247-264.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 76
A patient undergoing joint arthroplasty is put on a drug that competitively inhibits the activation of an enzyme that breaks down Factor Ia. The drug is
Explanation
Tranexamic acid competitively inhibits the activation of plasminogen to plasmin by binding to specific sites on both plasminogen and plasmin. Tranexamic acid has roughly eight times the antifibrinolytic activity of an older analogue, e-aminocaproic acid. It is used during joint replacement surgery to reduce blood loss and the need for transfusion.
Watts et al. review strategies for minimizing blood loss and transfusion. They recommend 1g of TXA prior to incision, and 1g at wound closure. They also recommend giving fluids for symptoms of anemia, rather than transfusion, as even high risk patients do well with sufficient intravascular volume even with low hemoglobin levels.
Imai et al. evaluated TXA in 107 patients undergoing THA. They found that intraoperative blood loss after preoperative TXA administration was lower than both control and postoperative TXA administration groups. They recommend using 1 g of TXA 10 minutes before surgery and 6 hours after the first administration to best reduce blood loss during THA.
Gillette et al. retrospectively reviewed 2046 patients receiving TXA for THA or TKA together with either aspirin, warfarin or dalteparin. They found that the rates of symptomatic DVT (0.35%, 0.15%, and 0.52%, respectively) and nonfatal PE were similar (0.17%, 0.43%, and 0.26%, respectively) for the 3 drugs respectively. They recommend TXA to decrease blood loss and transfusion.
Illustration A shows the role of tranexamic acid in the fibrinolytic cycle and the
clotting cascade.
Incorrect Answers:
Question 77
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 78
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 79
As a baseball player dives to catch a line drive in the outfield, the ball strikes the tip of the player’s finger when extended, causing forcible flexion to avulse the extensor tendon from the distal phalanx. Following evaluation and normal radiographic findings, initial management should include
Explanation
6 weeks, followed by nighttime splinting for an additional 6 weeks. It must be emphasized to the patient that at no time during the initial 6 weeks of treatment should the DIP joint be allowed to fall into flexion or an additional 6 weeks of continuous splinting is required.
REFERENCES: Miller MD, Cooper DE, Warner JP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 255.
Rettig AC: Closed tendon injuries of the hand and wrist in the athlete. Clin Sports Med 1992;11:77-99.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 229-230.
Question 80
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
Explanation
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
Question 81
Figure 7 shows a sagittal T 1 -weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
REFERENCES: Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears.
J Shoulder Elbow Surg 2003;12:550-554.
Agur AM (ed): Grant’s Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.
Question 82
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 83
Figures 38a and 38b are the MRI scans of a 28-year-old man who reports progressively worsening severe back pain for the past 3 months. He denies fevers, chills, weakness, or neurologic dysfunction. Examination reveals tenderness to palpation over the lumbar spine but normal neurologic findings. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein; blood cultures are positive for methicillin-sensitive Staphylococcus aureus. In addition to intravenous antibiotics, what is the next step in management? Review Topic

Explanation
Question 84
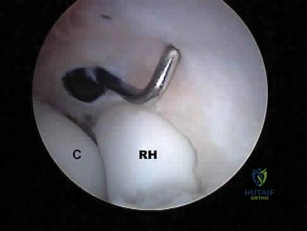
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic
Explanation
Question 85
Figure 26 is the radiograph of a 33-year-old woman who was involved in a high-speed motor vehicle crash. Her initial blood pressure is 80/50 mm Hg and she has a pulse rate of 120 bpm. After hemodynamic stabilization and temporizing measures have been performed, the patient is cleared for surgery. What is the most appropriate method of definitive fixation?

Explanation
Question 86
- Resurfacing the patella during a total knee replacement is strongly indicated when the diagnosis is
Explanation
Hence, chronic pain after TKA without resurfacing the patella was more common in knees affected by rheumatoid arthritis than in those affected by degenerative osteoarthritis. The authors of the study recommend that the patella be resurfaced when an unconstrained prosthesis is used in patients with a diagnosis of inflammatory arthritis and to a lesser degree osteoarthrosis.
Question 87
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 88
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90°, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of
Explanation
REFERENCES: Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193.
Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
Beals RK: Hemihypertrophy and hemihypotrophy. Clin Orthop 1982;166:199-203.
Question 89
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Dillin L, Hoaglund FT, Scheck M: Brachial neuritis. J Bone Joint Surg Am 1985;67:878-880.
Question 90
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 91
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
REFERENCE: Cooper JR, Dowson D, Fisher J, Jobbins B: Ceramic bearing surfaces in total articular joints: Resistance to third body damage from bone cement particles. J Med Eng Technol 1991;15:63-67.
Question 92
Figure below shows the radiograph obtained from a 73-year-old woman who returns status post total hip arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of

Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis. This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis indefinite observation would not be appropriate. A foot drop develops 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MRI or CT may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be reduced by flexing the surgical knee and positioning the bed flat.
Question 93
Which of the following fluoroscopic views is used to assess intra-articular screw penetration during volar fixation of a distal radius fracture?
Explanation
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
check for long distal screws.
OrthoCash 2020
Question 94
A 58-year-old man has a painful, warm, erythematous and fluctuant area over his left olecranon. An aspiration would be most likely to reveal
Explanation
Question 95
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Explanation
REFERENCES: Matava MJ: Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-296.
Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307.
Question 96
3 degrees Celsius and heart rate of 105 bpm. A clinical photograph, results of synovial fluid analysis, and a polarizing microscopy image are seen in Figures A through C. Synovial fluid gram stain and cultures are pending. What is the most appropriate next step in management?
Explanation
While the incidence of superimposed gout and septic arthritis is low (~1.5%),
it is reported. In the presence of crystals on aspiration, one should not rule out the possibility of septic arthritis. If there are other risk factors for infection, or the synovial WBC count is high (greater than 50,000), then empiric antibiotics should be initiated immediately after cultures are obtained. If the patient has other evidence supporting septic arthritis (positive Gram stain, purulence), emergent I&D is indicated. Even if the initial suspicion is lower, if they have
not respond to antibiotics after 24-48 hours they should undergo I&D.
Shah et al. investigated 265 crystal-positive joint aspirates in a 7-year retrospective study. They found the incidence of concomitant septic arthritis and crystal disease was 1.5% (4 cases including 2 knees, 1 hip, 1 ankle). All 4 patients that had superimposed infection had a WBC of > 50,000. They concluded that the presence of crystals in the synovial fluid cannot
conclusively rule out a septic joint.
Schuind et al. described a case report of concomitant septic arthritis and gout of the wrist. They found that cultures were positive for Staphylococcus aureus while pathological examination revealed aggregated crystals of monosodium urate.
Figure A shows tense, erythematous swelling of the right knee. Figure B is a table showing synovial fluid analysis with elevated WBC and PMN cell count characteristic of septic arthritis. Figure C shows needle-shaped negatively birefringent crystals on polarizing microscopy. Illustration A shows the synovial fluid characteristics in different disease conditions.
Incorrect Answers:
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Lead to lower patient satisfaction rates
Lead to higher patient satisfaction rates
Lead to higher likelihood the patient will take legal action against surgeon
Lead to higher likelihood the patient will change physicians
Prevent any legal action
The surgeon has provided all the elements of good communication with the patient and family. His actions will lead to improved patient satisfaction, compared to nondisclosure and attempting to push or shirk responsibility.
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise:
an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose
non-disclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
The acquired immune response mediated by the interaction between the T cell receptor and major histocompatibility complex requires which of the following first steps?
Antigen phagocytosis by T cells
Antigen processing and presentation to T cells
Antigen recognition by natural killer T cells
Antigen proliferation by polymerase chain reaction
T cell disulfide bond cleavage and enzymatic processing
The process of antigen processing and presentation is the first step of the acquired immune response. This is performed by the so called antigen presentation cells (APC) of which B cells and dentritic cells are two examples. The APC breaks down the protein antigen in a multitude of enzymatic reactions and presents key peptide sequences via the major histocompatibility complex
(MHC) receptors. Once presented on the surface of the APC, the T-cell receptor recognizes the MHC/antigen complex leading to T-cell activation. At no point in this process are antigens phagocytosed by T cells. Natural killer T cells are involved in this sequence, but not for antigen processing and presentation. Polymerase chain reaction is a laboratory tool used to amplify nucleic acid. Finally, disulfide bond cleavage is a step involved in the APCs antigen processing reaction and does not occur in T cells.
All of the following are true regarding a physician responding to a formal written complaint by a patient EXCEPT:
Complaint should be taken seriously
Written response by the physician is required
Physician mandated to retain an attorney to address the formal complaint
Patient should be supplied with contact information for the institution's patient representative department
Law mandates that the physician respond to the formal complaint
It is important for the surgeon to know how to manage a formal complaint. An attorney is not required to assist on behalf of the physician when addressing a formal complaint. All complaints must be taken seriously and the physician is required by law to respond to all formal complaints in writing. Verbal
responses to formal, written complaints are not sufficient. If a patient is filing a formal complaint it is advisable that the patient be supplied with contact information for the institution's patient representative department.
What laboratory findings would you expect to find in a patient newly diagnosed with renal osteodystrophy?
Decreased PTH secretion, hypophosphatemia, and hypocalcemia
Increased PTH secretion, hyperphosphatemia, and hypocalcemia
Decreased PTH secretion, hypophosphatemia, and hypercalcemia
Increased PTH secretion, hyperphosphatemia, and hypercalcemia
Hypophosphatemia and hypocalcemia
Renal osteodystrophy is characterized by bone mineralization deficiency due to the electrolyte and endocrine abnormalities associated with chronic kidney disease. The pathogenesis of renal osteodystrophy is multifactorial. Hypocalcemia occurs due to the inability of the damaged kidney to convert vitamin D3 into its active form, calcitriol. The hypocalcemia and lack of phosphate excretion by the damaged kidney causes hyperparathyroidism and secondary hyperphosphatemia.
Loss of function in the 25(OH) vitamin D1-alpha hydroxylase gene causes which of the following diseases?
Hyperphosphatemia
Vitamin D resistant rickets
Hereditary Vitamin D dependant rickets type I
Hereditary Vitamin D dependant rickets type II
Hypophosphatemic rickets
Loss of function mutations in the 25 (OH) vitamin D hydroxylase gene cause hereditary vitamin D dependant rickets type I. Hereditary vitamin D dependant rickets type II is caused by a defect in intracellular receptor for 1,25-(OH)2- vitamin D3. Both forms of
hereditary vitamin D dependent rickets show decreased serum calcium/phosphorous, elevated alkaline phosphatase/PTH,
but type I has a decrease in the 1,25(OH)2 vitamin D and type II shows a increase in 1,25(OH)2 vitamin D. Vitamin D resistant rickets (Familial Hypophosphatemic Rickets) is caused by a large deletion in the PHEX gene and results in low serum phosphorous, elevated alkaline phosphatase, and normal calcium. Hyperphosphatemia can be caused by mutation in the GALNT3 gene and results in elevated serum phosphate and decreased PTH/calcium.
Kato et al. describe the molecular physiology of vitamin D metabolism and the recognized gene mutations associated with various clinical manifestations of mutations in vitamin D homeostasis.
Figure A is a radiograph taken after an open reduction and internal fixation of a periprosthetic distal femur fracture. With this type of hybrid locked plate fixation, what is the difference between screw A and screw B?
Screw A can assist in fracture reduction while screw B provides a fixed angle support
Screw A provides improved axial stiffness while screw B provides a fixed angle support
Screw A can be used to reduce the plate to bone while screw B can be used to lag fracture fragments together
Screw A provides a fixed angle support while screw B can be used to reduce the plate to the bone
Screw A can be used to lag fracture fragments together and screw B increases the plate bone frictional stability
Locking screws provide a fixed angle support and can improve fixation in osteoporotic bone while nonlocking screws can be used to reduce the plate to the bone, lag fracture fragments together and increase the plate bone frictional stability. "Hybrid" locked plate fixation utilizes both screw types in order to assist with difficult fracture fixation such as when there is a short metaphyseal segment and osteoporotic bone.
Zura et al discusses the biomechanical and biological advantages offered by locked plate fixation.
Using levels of evidence in research studies, which of the following represents a level II study?
Retrospective case control study
Prospective cohort study
Case report of 3 patients with the same disease
High-quality randomized prospective clinical trial
The opinion of a review panel at the annual AAOS meeting
Level II Evidence includes prospective cohort studies. There are 5 levels of evidence in clinical research. Level I includes randomized clinical trials. Level II includes prospective cohort studies. Level III includes case control studies AND retrospective cohort studies. Level IV includes case series. Level V evidence includes expert opinion, case reports, and personal observation. The cited reference by Bernstein et al is an excellent review of Evidence Based Medicine (EBM) and describes the 5 step process of making medical decisions based on the available, and often limited, evidence. These steps include: 1) Formulate answerable questions. 2) Gather the evidence. 3) Appraise the evidence. 4) Implement the evidence. 5) Evaluate the process. The reference by Spindler et al is another review article that discusses the different levels of evidence for different study types.
All of the following are true regarding the assessment of bone mineral density EXCEPT?
Bone mineral density loss is not apparent on standard radiographs until 30% to 40% of mineral is lost
Dual energy x-ray absorbtiometry (DEXA) is only able to measure mineralization of the axial skeleton
Single photon absorbtiometry allows for the analysis of bone mineralization in the appendicular skeleton alone
Quantitative computed tomography (QCT) is associated with 10 times the radiation of a DEXA scan
MRI allows for accurate discrimination of normal bone from osteopenic bones
without exposing the patient to ionizing radiation
Dual energy x-ray absorbtiometry (DEXA) scans allow for accurate assessment of bone mineralization in both the axial and appendicular skeleton.
Over the last decade, DEXA has become a safe, cost-effective and reliable method to quantify bone mineral density. The World Health Organization (WHO) has adopted DEXA derived BMD measurements to define normal bone, osteopenia, and osteoporosis in the adult and paediatric population. The typical DEXA analysis therefore reports a Z-score, which is the number of standard deviations (SDs) that a patient's BMD is above or below the mean value for persons of the patient's age and sex. The T score is the number of SDs the patient's BMD is either above or below the mean value for young patients of the same gender.
Tortolani et al. provide an overview of the techniques used to assess bone mineral density, the pathophysiology of osteopenia, and the evaluation and treatment options for the general pediatric population as well as for patients with specific pediatric disorders. The authors encouraged orthopaedic surgeons to understand the problems of osteopenia in both otherwise healthy children and children with chronic disorders.
Binkovitz & Henwood provide a review of DEXA technique and interpretation with emphasis on the considerations unique to pediatrics. They found that changes in bone size over time, as occurs in normal pediatric development, confound DXA interpretation. This is one of the major limitations in the use of pediatric DXA. However, attempts to correct for or to circumvent this limitation have been proposed and show promise in improving DXA interpretation and
our understanding of bone physiology.
T-score according to the World Health Organization (WHO): A T- score of -1.0 or above is normal bone density.
A T-score between -1.0 and -2.5 means you have low bone density or osteopenia.
A T-score of -2.5 or below is a diagnosis of osteoporosis.
Incorrect Answers:
A mother brings her 4-year-old daughter to your clinic for evaluation of knocked knees and short stature. On exam, the patient ambulates with a circumduction gait pattern and frequently falls. Plain radiographs are displayed in Figure A. Laboratory data is obtained and notable for calcium 9.1 mg/dL (RR 8.5-
Question 97
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of
Explanation
REFERENCE: Davids JR, Glancy GL, Eilert RE: Fracture through the stalk of pedunculated osteochondromas: A report of three cases. Clin Orthop 1991;271:258-264.
Question 98
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.The most substantial functional deficit that may develop if no surgical treatment is provided is
Explanation
have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
Question 99
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1422-1464.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Chandler JT, Bonar SK, Anderson RB, Davis WH: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
Question 100
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.
