Orthopedic Board Review MCQs: Elbow & Fracture Management | Part 125

Key Takeaway
This page offers an interactive MCQ quiz for orthopedic surgeons preparing for their AAOS and ABOS board certification exams, including OITE. It features 100 verified, high-yield questions modelled on actual exams, with detailed explanations and literature references to enhance board preparation.
About This Board Review Set
This is Part 125 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 125
This module focuses heavily on: Elbow, Fracture.
Sample Questions from This Set
Sample Question 1: A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed...
Sample Question 2: A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain....
Sample Question 3: 1 to 1 micron...
Sample Question 4: -A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with internation...
Sample Question 5: A 72-year-old male sustains the injury shown in Figure A as a result of a fall from a ladder. Which of the following factors has been shown to be associated with increased collapse or sliding displacement?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
REFERENCES: Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Sarhadi NS, Korday SN, Bainbridge LC: Radial tunnel syndrome: Diagnosis and management. J Hand Surg Br 1998;23:617-619.
Question 2
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis? Review Topic

Explanation
Question 3
1 to 1 micron
Explanation
For many years, it was believed that large particles incited the histiocytic response. It is now well established that submicron-size particles stimulate this response.
Question 4
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 5
A 72-year-old male sustains the injury shown in Figure A as a result of a fall from a ladder. Which of the following factors has been shown to be associated with increased collapse or sliding displacement?

Explanation
Palm et al showed that 22% of patients with a fractured lateral femoral wall underwent reoperation for collapse of fracture compared to 3% with an intact lateral femoral wall. Interestingly, 74% of the lateral proximal femoral wall fractures were iatrogenic during the procedure itself.
Gotfried et al reported on 24 patients with postoperative intertrochanteric hip fracture collapse and noted that this complication followed fracture of the lateral wall in every instance and resulted in a protracted period of disability until fracture healing. They recommend care when drilling at the base of the lateral wall intraoperatively.
Lindskog et al review the diagnosis, treatment, as well as biomechanical reviews of treatment options for unstable intertrochanteric hip fractures.
Incorrect Answers:
OrthoCash 2020
Question 6
A football player injures his knee when he is tackled and falls awkwardly. He does not note any discreet “pop,” but pain prevents him from returning to the game. An effusion is noted the following day and an MRI scan is ordered. Selected images are shown in Figures 1 through 3. Based on these images, physical examination findings likely include

Explanation
Question 7
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 8
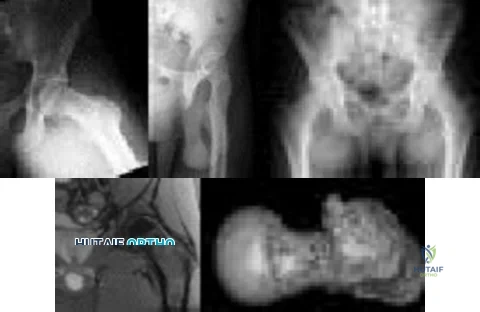
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 9
A 50-year-old man undergoes revision total knee arthroplasty (TKA). The tibial component shown in Figure 153 was retrieved at the time of revision. The wear damage demonstrated on the backside of the tibial component is most likely related to which wear mechanism(s)?
Explanation
Pitting and delamination seen in tibial component retrievals on the bearing surface of a TKA is related to fatigue wear. Backside wear is shown in the photograph; this is where the lot numbers usually are present, but now they are not distinguishable because of backside wear. This wear mechanism is attributable to adhesive and abrasive wear. The nanometer-size particles created by this wear mechanism account for the higher prevalence of osteolysis associated with modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 154 AND 155
Five weeks ago, an 82-year-old man underwent revision total knee arthroplasty (TKA). Three weeks after surgery he had a dental cleaning. The patient now reports 2 days of worsening pain following a long physical therapy session. His C-reactive protein (CRP) level is 15.0 mg/L (reference range, 0.08-3.1 mg/L). Upon examination, there is no drainage and slight effusion, and he has a passive range of motion to 110 degrees. Radiographs are unremarkable.
Question 10
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 11
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 12
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of Review Topic
Explanation
Question 13
A 10-month-old infant has a deformity of the right foot. Radiographs, including simulated weight-bearing AP and lateral views and a maximum plantar flexion lateral view, are shown in Figures 57a through 57c. Initial management of the foot should consist of Review Topic

Explanation
Question 14
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
Explanation
Question 15
A year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 16
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 17
Which 2 tendons are identified in the dissection shown in Video 92?
Explanation
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 18
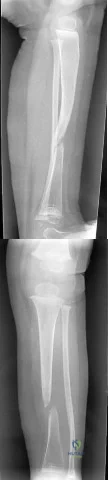
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient’s disorder?
Explanation
REFERENCES: Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236.
Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Cole WG: Etiology and pathogenesis of heritable connective tissue diseases. J Pediatr Orthop 1993;13:392-403.
Question 19
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 20
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. The athlete undergoes repair of the injury, and postsurgical radiographs are shown in Figures 1 and 2. At his first postsurgical visit, he reports no pain but describes weakness in his hand and decreased sensation over his lateral forearm. Upon examination, he has decreased 2-point discrimination over the lateral forearm and an inability to actively extend his thumb and fingers at the metacarpophalangeal joints. He can extend at the finger interphalangeal joints. He can extend his wrist weakly, and it deviates radially as he extends. His distal sensation is intact. Considering his examination findings, which two nerves are injured?

Explanation
elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
Question 21
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. Stress radiographs show a 2-mm medial physeal widening with valgus stress. What is the best initial treatment strategy for this patient?
Explanation
Question 22
2010 Pediatric Orthopaedic Examination Answer Book • 9 A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis?
Explanation
There is an asymmetry of the deformities that makes diastrophic dysplasia less likely.
REFERENCES: Goldberg MJ, Yassir W, Sadeghi-Nejad A: Clinical analysis of short stature. J Pediatr Orthop 2002;22:690-696.
Parmar VS, Stanitski DF, Stanitski CL: Interpretation of radiographs in a pediatric limb deformity practice: Do
radiologists contribute? J Pediatr Orthop 1999;19:732-734. Question 4
Patients with slipped capital femoral epiphysis are more likely to experience a delay in definitive diagnosis if they initially present to a physician reporting which of the following problems?
L Limp
Hip pain
Knee pain
Proximal thigh pain
Buttock pain
DISCUSSION: A delay in diagnosis of slipped capital femoral epiphysis (SCFE) can lead to significant worsening of the deformity or even progression from a stable to an unstable SCFE. Those patients that report knee pain as their primary complaint are most likely to experience significant delay. Other variables associated with this delay include Medicaid insurance and stable SCFE.
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis.
AL-Madena Copy
10 • American Academy of Orthopaedic Surgeons
Pediatrics 2004;113:e322-e325.
Rahme D, Comley A, Foster B, et al: Consequences of diagnostic delays in slipped capital femoral epiphysis. J Pediatr Orthop B 2006;15:93-97.
Question 23
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Lucas DR, Nascimento AG, Sim FH: Clear cell sarcoma of soft tissues: Mayo Clinic experience with 35 cases. Am J Surg Pathol 1992;16:1197-1204.
Question 24
A 21-year-old pregnant female arrives in the trauma bay with a closed head injury as well as an open ankle injury. During evaluation, what positioning is recommended to limit positional hypotension?

Explanation
reviews the appropriate physiological changes of pregnancy and covers the treatment of orthopedic trauma in the face of pregnancy.
Question 25
- A 12-year-old Little League pitcher has had pain in the dominant shoulder for the past week that prevents him from pitching. Examination reveals normal strength, full range of motion, normal stability, and mild tenderness about the proximal humerus. Radiographs with comparison views of the opposite shoulder show widening of the proximal humerus physis. Management should include
Explanation
Treatment requires cessation of repetitive physeal stress. There is no long-term sequelae. The athlete can return to same sports in the following season with emphasis on preseason conditioning.
Question 26
Figures 1 through 4 are the radiographs and MR images of a healthy 21-year-old woman who has had persistent dorsal wrist pain despite immobilization and no history of trauma. The surgical procedure associated with the best prognosis in this scenario is
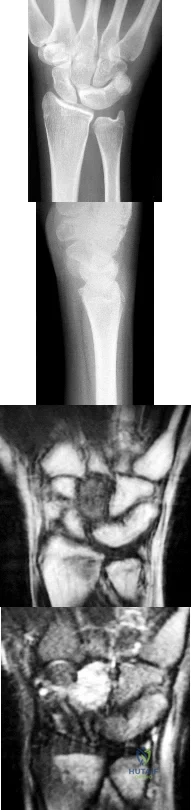
Explanation
This patient has osteonecrosis of the capitate. The MR images show evidence of osteonecrosis with decreased signal on the T1-weighted image. The radiographs are unremarkable, with the exception of lunotriquetral coalition, which does not necessitate treatment. The etiology of osteonecrosis of the capitate may be related to trauma, abnormal Interosseous vascular supply, and hypermobility. Surgery is an option for patients with persistent symptoms despite immobilization. Vascularized bone graft should be considered in this scenario because there is no evidence of capitate collapse or arthritic change about the wrist. Free and local vascularized bone grafts have produced satisfactory results. Capitate excision with interposition arthroplasty is indicated for patients with proximal pole capitate collapse. Total wrist fusion is a salvage procedure and would be considered if there were evidence of collapse and arthritic change. PRC would leave the capitate articulating with the radius and is not indicated.
Question 27
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?
Explanation
REFERENCE: Lansinger O, Bergman B, Korner L, et al: Tibial condylar fractures: A twenty-year follow-up. J Bone Joint Surg Am 1986;68:13-19.
Question 28
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include
Explanation
REFERENCES: Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Schleiermacher G, Peter M, Oberlin O, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Question 29
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Explanation
REFERENCE: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 30
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 31
What is the most appropriate treatment?
Explanation
A common postsurgical problem after TKA is a sudden increase of pain that typically occurs about 2 to 3 weeks after surgery. ESR findings are not reliable during the acute postsurgical period. A CRP level exceeding 100 mg/L during the acute postsurgical period is a joint aspiration indication. If the patient does not have sepsis, there is no emergency. This pain is likely attributable to too much activity during physical therapy. Observation is recommended for this patient.
Question 32
An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy? Review Topic
Explanation
Question 33
A 2-year-old girl has the fracture shown in Figures 5a and 5b. This fracture is most commonly associated with which of the following entities? Review Topic
Explanation
Question 34
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
Explanation
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and paresthesias, are not supported by the evidence.
Question 35
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 36
Radiographs of the femur are unremarkable. A radionuclide bone scan demonstrates abnormal uptake in the mid-femur. A radionuclide bone marrow scan demonstrates decreased uptake within the marrow. Which of the following is the best step in management?
Explanation
Skaggs et al reviewed 79 cases of acute extremity pain in sickle cell patients. Radionuclide bone marrow and bone scan was used to differentiate osteomyelitis from bone infarct. Four cases of infection were diagnosed by normal uptake on the bone marrow scan and abnormal uptake on the bone scan. These cases were confirmed osteomyelitis by positive culture. Seventy cases were diagnosed as bone infarct by decreased uptake on the bone marrow scan and abnormal uptake bone scan.
Chambers et al reviewed the charts of 2000 known sickle cell patients. Fourteen patients had an episode of osteomyelitis or septic arthritis. Radiographs and bone scans were not helpful in differentiating infection from an acute bone infarct. Salmonella was the most frequent organism cultured from the osteomyelitis cases. The authors recommend bone aspiration or biopsy in an sickle cell patient with extremity pain, swelling, and a fever greater than 38.2 degrees C.
An otherwise healthy, 65-year-old male undergoes a right total knee arthroplasty without complications. Which of the following statements is recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty?
Administer aspirin one week pre-operatively
Use elastic compressive stockings for 10 days pre-operatively
Obtain a post-operative duplex ultrasound of the patient for screening purposes
Administer Coumadin to maintain the patient’s INR between 1.5 and 2.5 during the post-perative period
Use mechanical compressive devices in the postoperative period
Use of mechanical compressive devices and aspirin during the postoperative period is
recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines.
In 2011, the American Academy of Orthopaedic Surgeons published their Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. A summary of those guidelines provide general recommendations for venous thromboembolic disease in patients with and without bleeding disorders. These recommendations range from strong (recommending against the use of routine post-operative duplex ultrasonography), to moderate (using mechanical compressive devices or a pharmacologic agent for prophylaxis in the post- operative period), to inconclusive (they are unable to recommend for or against specific pharmacologic prophylaxis agents). Additionally, there are recommendations based on consensus agreement of the authors (the recommendation of early mobilization in the post-operative period).
These guidelines are now much closer to in agreement with the American College of Chest Surgeons (ACCS) 2012 guidelines for VTE prophylaxis. One of the differences between the guidelines is that the AAOS guidelines do not state a specific amount of time that a pharmacologic agent should be given post- operatively while the ACCS recommends such agents for a minimum of 10-14 days.
Incorrect answers:
The definition of effect size is best described as which of the following?
Likelihood that a statistically significant difference would be found between 2 groups given that a difference truly did exist
Estimated magnitude of the difference in the means between two groups
Average of the squares of each value's deviation from the mean
Range within which it is probable that the true value lies for the whole population of patients
Probability of obtaining a result equal to or more extreme than what was actually observed assuming the null hypothesis is true
The effect size is best defined as the magnitude of the difference in the means of the control and experimental groups in a study with respect to the pooled standard deviation. Effect sizes are normally used for continuous variables in contrast to relative risk reduction which is used for dichotomous variables. Power (1), variance (3), confidence interval (4), and P value (5) are the other options provided.
Which of the following patients are at greatest risk of having a future vertebral fragility fracture?
Elderly female with prior hip fragility fracture
Elderly female with prior distal radius fragility fracture
Elderly female with prior T6 compression fragility fracture
Elderly female with a T-score of -3.0
Elderly female currently on hormone replacement therapy
History of a prior vertebral fragility fracture is the strongest predictor of a future fragility fracture. A meta-analysis by Klotzbuecher et al examined risk factors for fragility fractures and found an association between prior and subsequent fragility fractures. The strongest associations were observed between prior and subsequent vertebral fractures. They found women with preexisting vertebral fractures had an approximately 4 times greater risk of subsequent vertebral fractures than those without prior fractures. They also found this risk increases with the number of prior vertebral fractures. Other combinations of prior and future fracture sites, such as the hip or wrist, were also strongly associated, but none so high as vertebral fractures.
A 79-year-old female falls onto her right hip at home and sustains the injury shown in Figure A. She undergoes an uncemented unipolar hemiarthroplasty. During insertion of the stem into the femoral canal, the patient becomes hypotensive and hypoxic. Which of the following has most likely occurred?
Femoral shaft fracture
Inadequate fluid resuscitation during surgery
Acute myocardial infarction
Pulmonary embolism caused by dislodging of deep venous thrombosis during hip exposure
Intramedullary fat and marrow embolization
During insertion of the femoral stem, the intramedullary pressures are increased. Fat and marrow elements can become embolized into the bloodstream at this point resulting in ventilation perfusion mismatch in the lungs.
Kim et al prospectively followed 156 total hip arthroplasties including bilateral and unilateral procedures as well as cemented and uncemented procedures. They found no difference in fat embolization amongst any of the groups. However, they did find that if patients had evidence of bone marrow cells in the right atrium on the first postoperative day, they developed diffuse encephalopathy with confusion and agitation that lasted for about twenty-four hours.
Which of the following investigative studies is most useful in the definitive diagnosis of Amyotrophic Lateral Sclerosis (ALS)?
Genetic testing
MRI brain and spinal cord
Muscle biopsy
Serum protein electrophoresis and immunoelectrophoresis
Electrodiagnostic studies
The diagnosis of ALS requires a period of clinical observation to document the progressive loss of upper and lower motor function. Electrodiagnositic studies are required to make a definitive diagnosis.
Amyotrophic lateral sclerosis (ALS) is the most common degenerative disease of the motor neuron system. Nerve conduction studies and needle electromyography (EMG) are useful for confirming the diagnosis of ALS and for excluding peripheral conditions that resemble ALS. Hallmark findings in the electrodiagnosis of ALS are abnormal motor nerve conduction studies, with normal sensory nerve conduction studies. UMN signs are mild weakness, spasticity, and abnormally brisk reflexes; LMN signs are progressive weakness, wasting, and loss of reflexes and muscle tone.
Brooks et al. developed a diagnostic algorithm for the diagnosis of ALS. The algorithm is based on the degree of certainty of diagnosis, which is increased by the number of body segments that demonstrate upper motor neuron (UMN) and lower motor neuron (LMN) abnormalities. Clinical and electrophysiologic findings in 3 or more body segments is definitive of the diagnosis.
Incorrect Answers:
Radiographic changes suggestive of osteopetrosis in children are a known complication of which of the following types of medications?
TNF-alpha inhibitors
Bone morphogenic proteins
Bisphosphonates
Fluoroquinolones
RANKL antibiodies
Radiographic changes suggestive of osteopetrosis (marble bone disease) are a known complication of bisphosphonate usage. The common cellular pathway in this process is the osteoclast. Bisphosphonates target and inhibit the osteoclast, and these cells are not functioning in patients with osteopetrosis.
Whyte et al describe a case report of a 12-year-old child with idiopathic hyperphosphatasia treated with bisphosphonates who developed osteopetrosis.
Falk et al report on their small case series which showed the beneficial effects and known complications in the treatment of osteogenesis imperfecta with bisphosphonate therapy.
Marini presents a perspective article describing the off-label use of bisphosphonates in children.
What function does computerized physician order entry have on medication monitoring?
Reduces the rate of medication errors
Improves physician satisfaction
Decreases narcotic requirements by patients
Increases rates of allergy related medication errors
Improves physician knowledge about the drugs they are prescribing
Computerized physician order entry has greatest impact on reducing medication errors.
Bobb et al. studied medication errors averted by pharmacists at a 700-bed academic center and concluded that 65% of them would likely have been prevented with computerized physician order entry.
Upperman et al. reviewed medication errors at a pediatric hospital before and after implementation of a computerized physician order entry system. They found a significant decrease in adverse drug events following establishment of the computerized system.
Incorrect Answers:
2: Physician satisfaction has not been correlated with computer entry for medications.
3: Narcotic requirements are related to injury or patient characteristics, not computerized entry.
4: Allergy-related errors are decreased with use of computerized entry.
5: Physician knowledge is not necessarily increased with computerized entry.
What is the cellular mechanism of action for non-nitrogen containing bisphosphonates (such as clodronate and etidronate) to induce osteoclast apoptosis?
Inhibiting caspase
Inhibiting matrix metalloprotease
Inhibiting reverse transcriptase
Targeting of farnesyl diphosphate synthase
Creating toxic analog of adenosine triphosphate that targets mitochondria
Bisphosphonates work by one of two mechanisms. Non-nitrogren containing bisphosphonates (such as etidronate and clodronate) work by creating a toxic analog of ATP which inhibits ATP and leads to osteoclast apoptosis. Nitrogen containing bisphosphonates (such as alendronate, risedronate, and zoledronate) inhibit the enzyme farnesyl diphosphate synthase which prevents protein geranylgeranylation and prevents osteoclastic bone resorption.
Reska et. al. specifically discuss the difference between the two pathways. Non-nitrogen containing compounds inhibit ATP production and cause osteoclast apoptosis. Nitrogen containing bisphophonates inhibit protein synthesis by interrupting the cholesterol biosynthetic pathway, which prevents osteoclastic resorption.
Which class of antibiotics inhibit early fracture healing through toxic effects on chondrocytes?
cephalosporins
quinolones
penicillins
macrolides
sulfonamides
Animal models have shown that quinolones inhibit early fracture healing through a toxic effect on chondrocytes. The study by Perry et al demonstrated that fracture calluses in the animals treated with quinolones showed a lower histologic grade as compared with control animals representing a less mature callus with the presence of more cartilage and less woven bone. The study by Huddleston et al demonstrated fracture calluses in the animals treated with ciprofloxacin showed abnormalities in cartilage morphology and endochondral bone formation and a significant decrease in the number of chondrocytes compared with the controls. None of the other antibiotics listed are known to have toxic effects on chondrocytes.
A mutation of the retinoblastoma gene RB-1 leads to the development of malignancies such as retinoblastoma and osteosarcoma. Which term best characterizes the RB-1 gene?
growth factor
retro-oncogene
proto-oncogene
oncogene
tumor suppressor
A tumor suppressor is a gene whose presence normally prevents neoplasia and whose absence leads to unregulated cell growth. Two well-studied tumor suppressor genes include p53 and RB-1. P53 normally suppresses cell division by blocking the cell cycle if genetic damage is present. If it is absent or mutated, the p53 suppressing effect no longer regulates cell growth and neoplasm results. In a similar fashion, a mutation in RB-1, or the retinoblastoma gene, may leads to retinoblastoma and osteosarcoma.
Youarecounseling ayoungfemalepatientabout herfuturerisk of osteoporosis. Which of the following regarding peak bone mass (PBM) is true?
PBM is consistently attained by the end of the second decade of life in both men and women.
PBM is independent from environmental factors.
PBM correlates strongly with post-menopausal bone mineral density
Timing of PBM varies based on anatomic site.
Women attain PBM prior to men, regardless of anatomic site. Corrent answer: 4
The timing and magnitude of PBM varies based on anatomic site. PBM is often reached in the appendicular skeleton earlier than in the axial skeleton.
PBM is defined as the greatest amount of bone an individual will attain in his or her lifetime. Controversy has surrounded the timing of PBM due to significant anatomical variations as well as strong gender-based, genetic, geographic, environmental, and mechanical influences. While women may reach PBM
earlier than men in the hip, the converse has been found to be true of the spine. Furthermore, the age at which each is obtained varies widely. Though the PBM of the hip is most often achieved by the end of the second decade of life, PBM of the spine may not occur until the third or fourth decade of life. Interestingly, PBM has been found to correlate poorly with post-menopausal bone mineral density, likely a result of these strong confounding influences.
Bonjour et al. reviewed the controversy behind peak bone mass. The authors note that the gender-based difference in bone mass becomes expressed during puberty and that there is a large variability in normal values of bone mineral density between anatomic sites.
They conclude that bone mass accumulation can be completed by the end of the second decade at both the lumbar spine and femoral neck, but that this may be significantly influenced by a number of variables during growth such as genetics, diet, endocrine and mechanical factors.
Berger et al. more recently evaluated trends in peak bone mass from longitudinal data in the Canadian Multicentre Osteoporosis Study (CaMos). The authors found that peak bone mass was highly variable between the axial and appendicular skeleton. Specifically, lumbar spine PBM was reached in women
at 33-40 years, but much earlier in men at 19-33 years. Conversely, hip PBM was reached earlier in women at 16-19 years and later in men at 19-21 years. Furthermore, there was a lack of concordance between PBM and BMD over age
Question 37
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Patel CK, Fischgrund JS: Complications of anterior cervical spine surgery. Instr Course Lect 2003;52:465-469.
Question 38
Etanercept modifies the natural history of inflammatory arthropathies through what mechanism?
Explanation
Question 39
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, pp 956-957.
Wheeless’ Textbook of Orthopaedics: Acetabular Protrusio. www.wheelessonline.com/ortho/acetabular_protrusio
Question 40
Which of the following is true regarding intimate partner violence (IPV)?

Explanation
Interdisciplinary collaboration among healthcare workers was a predictor of positive treatment outcomes. Included were more accurate assessments of past history, more descriptive emotional symptoms as displayed by victims and written documentation of recommendations concerning intervention and linkage to community resources.
Bhandari et al performed a cross-sectional study of 282 women who presented to fracture clinic at two Level-I trauma centers in Canada. The prevalence of abuse was found to be 32% while 8.5% were found to have a history of previous abuse in the past 12 months. Ethnicity, socioeconomic status, and injury patterns were not associated with abuse.
Shields et al reviewed 153 cases of domestic violence victims who presented to two Emergency departments. They determined that positive treatment outcomes were correlated to the degree of interdisciplinary collaboration among treating health care providers.
Question 41
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 42
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 43
- Which of the following radiographic findings would be characteristic of the knee joints of a patient with neuropathic osteoarthropathy of the knee?
Explanation
The loss of sensation to the joint is followed by severe degenerative changes, osteophyte formation, articular and subchondral fractures, and often calcification of surrounding soft tissues. In the knee, this is a tricompartmental disease and will not selectively affect one compartment over another.
Question 44
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of
Explanation
REFERENCES: Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 45
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 46
Figure 1 shows the radiograph obtained from a 78-year-old woman who has a recent history of increasing thigh pain 12 years after undergoing total hip arthroplasty. Figure 2 depicts the radiograph obtained after she fell and was unable to ambulate. What is the most appropriate treatment?
Explanation
The surgical treatment of periprosthetic fractures of total hip replacement with a loose implant and progressive bone loss is associated with a high complication rate. The recent literature would favor the use of long "Wagner-type" stems, which have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic, because the intramedullary stem limits the ability to use screws with the plate. Using long distally fixed stems circumvents this problem by enhancing
fracture healing and creating a long-term prosthetic solution in these most difficult cases.
Question 47
An acetabular reinforcement cage is most often indicated for which of the following conditions?
Explanation
REFERENCES: Berry DJ, Lewallen DG, Hanssen A, Cabanela ME: Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am 1999;81:1692-1702.
Whaley AL, Berry DJ: Extra-large uncemented hemisphere acetabular components for revision THA. J Bone Joint Surg Am 2001;83:1352-1357.
Question 48
Which of the following statements best describes the anatomic considerations of the popliteal artery posterior to the knee joint?
Explanation
90 degrees of flexion.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 151.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-53.
Question 49
When performing a saline load test to evaluate for a traumatic arthrotomy of the knee, a mininum of how much saline should be utilized?

Explanation
The study by Nord et al found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were 110, 145, 155, and 175 mL, respectively.
The other referenced study by Keese et al found that 50 mL of saline successfully identified only 46% of known knee arthrotomies and that 194 mL was needed to reach a 95% identification rate.
Question 50
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient? Review Topic
Explanation
Question 51
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 52
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 53
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
REFERENCES: Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751.
Glassman SD, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
Raney EM, Bennett JT: Pediatric Chance fracture. Spine 1992;17:1522-1524.
Question 54
A Canale view best visualizes which of the following structures?
Explanation
REFERENCES: Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Bruden B: Roentgen examination of the subtaloid joint in fractures of the calcaneus. Acta Radiol 1949;31:85-91.
Question 55
A 16-year-old competitive female swimmer has a 1-year history of left shoulder pain. She denies any specific injury to her shoulder. She reports that the pain is worse with swimming but also has pain with daily activities. She also notes similar occasional symptoms in her right shoulder. Examination reveals symmetric range of motion and rotator cuff strength. Examination of the left shoulder reveals 2+ anterior and posterior translation with pain in both directions and a 2-cm sulcus sign. The right shoulder also has 2+ anterior and posterior translation and a 2-cm sulcus sign with no pain. She also has hyperextension of the elbows and the ability to touch the radial border of her thumb to her forearm. What is the next step in management? Review Topic
Explanation
Question 56
Which of the following conditions is transmitted by an autosomal dominant trait?
Explanation
REFERENCES: Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 1627.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 107.
Question 57
Rickets can be best characterized by which of the following radiographic changes in children?
Explanation
Question 58
Figures 51a and 51b show subluxation of the
Explanation
REFERENCES: Rowland SA: Acute traumatic subluxation of the extensor carpi ulnaris tendon at the wrist. J Hand Surg Am 1986;11:809-811.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1026-1027.
Question 59
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 60
A 45-year-old man has a draining sinus and recurrent infection of his right total knee arthroplasty. He has had two prior revision surgeries after the primary procedure and three other surgeries before his initial replacement, including a proximal tibial osteotomy and subsequent hardware removal. On clinical examination, he has a draining sinus in the mid portion of his surgical scar and a range of motion of 5° to 85°. AP and lateral radiographs of the right knee are shown in Figures below. During surgery, the femoral component is found to be grossly loose, but the tibial component is well fixed. What is the most appropriate extensile approach that would provide adequate exposure and aid in tibial component extraction?
Explanation
Extended tibial tubercle osteotomy is an extensile approach to revision total knee arthroplasty that affords excellent exposure and can facilitate removal of tibial sleeves and cones. This patient has had multiple surgeries, including a proximal tibial osteotomy, as well as poor range of motion, patella baja, and a well- fixed metaphyseal sleeve component. Classically, an extended tibial tubercle osteotomy provides outstanding exposure for component removal in the setting of prior high tibial osteotomy and patella baja. For this patient, it is important to recognize the patella baja on the radiographs, as well as the tibial sleeve. In many of these cases the osteotomy provides access to the sleeve to help with extraction, because the stem will not pull through the sleeve or detach from the tray to allow visualization of the sleeve. The extended medial parapatellar approach is just a long medial approach that typically yields good exposure
but would not help with the patella baja or extraction of the tibial sleeve. The quadriceps snip would give good exposure to the knee but would not aid in tibial component removal. Lastly, the medial epicondyle osteotomy could help with exposure and tensioning of the medial complex of the knee but would not help
with tibial component extraction.
Question 61
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 62
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 63
below shows the standing AP radiograph obtained from a year-old man who has a year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 64
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
REFERENCES: Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:1038-1047.
Question 65
When placing a percutaneous retrograde pubic rami screw for fixation of an acetabular fracture, which of the following radiographic views can best ensure that the screw does not exit the posterior aspect of the superior pubic ramus?

Explanation
Question 66
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 67
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
Explanation
Question 68
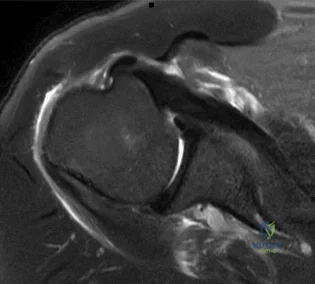
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis? Review Topic

Explanation
Question 69
- Figures 59a and 59b show the plain radiographs, and Figures 59c and 59d show the CT scan of a 77-year-old woman who has had pain in her back and both buttocks for the past 6 months. She reports that the pain radiates down her right thigh and leg when she is standing. What is the most likely diagnosis?
Explanation
Question 70
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 71
Which of the following best characterizes the antigenicity of allograft bone?
Explanation
REFERENCES: Crawford MJ, Swenson CL, Arnoczky SP, et al: Lyophilization does not inactivate infectious retrovirus in systemically infected bone and tendon allografts. Am J Sports Med 2004;32:580-586.
Stevenson S, Li XQ, Davy DT, et al: Critical biological determinants of incorporation of non-vascularized cortical bone grafts: Quantification of a complex process and structure. J Bone Joint Surg Am 1997;79:1-16.
Simon SR (eds): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 277-320.
Question 72
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 73
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 74
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.View Abstract at PubMed
Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. View Abstract at PubMed
Question 75
What approach should be chosen for the injury seen in Figure 67? Review Topic

Explanation
Innervates the medial aspect of the proximal thigh
Originates from the dorsal roots of L4-L5
Course runs medial to the femoral artery
Courses along the medial border of the psoas muscle
Courses under the inguinal ligament PREFERRED RESPONSE 5
Question 76
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
Explanation
REFERENCES: Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Beals RK, Bryant RE: The treatment of chronic open osteomyelitis of the tibia in adults.
Clin Orthop Relat Res 2005;433:212-217.
Question 77
Residual end-organ hypoperfusion in a polytraumatized patient is shown by which of the following?

Explanation
Question 78
Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when
Explanation
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
Question 79
A 45-year-old male auto mechanic presents to your office with left lateral elbow pain for 6 weeks. On physical exam he has tenderness to palpation over the lateral epicondyle and pain with resisted wrist extension. An MRI is shown in figures A and B. After failing non-surgical treatment modalities, he undergoes arthroscopic surgical management. At 3 months post-operatively, the patient reports persistent left elbow pain and an audible clicking since surgery which occurs when he lifts heavy objects and when he pushes himself up out of a chair. What is the best surgical treatment option? Review Topic
Explanation
PLRI is the result of an incompetent lateral ulnar collateral ligament (LUCL), a component of the elbow lateral collateral ligament complex. The LUCL originates on the lateral epicondyle of the humerus and inserts upon the supinator crest of the ulna. When deficient from acute trauma or from repetitive microtrauma, the elbow becomes rotationally unstable with elbow extension, supination, and an applied valgus force. In this case, the patient has had iatrogenic damage to the LUCL from an arthroscopic release of the extensor carpi radialis brevis (ECRB) for treatment of lateral epicondylitis. This patient exhibits an important manifestation of this: a positive chair pushup test. This test is positive when pushing off of a chair with a supinated forearm causes pain and instability. Due to the chronicity of the injury (3 months) and his persistent symptoms of instability (pain and clicking) the patient would benefit from surgical reconstruction of the damaged LUCL using either palmaris longus or gracilis allograft.
Kelly et. al. reviewed the known major and minor complications of elbow arthroscopy among 473 consecutive cases at their institution from 1980-1998. The most common complications were transient nerve palsies in 10 patients. Among them, the major
nerves involved included the anterior interosseous nerve, posterior interosseous nerve, ulnar nerve, superficial radial nerve, and medial antebrachial cutaneous nerve. The risk of iatrogenic nerve injury was increased among patients with rheumatoid arthritis. The most frequent complication was prolonged drainage from the portal sites.
Calfee et. al. reviewed the management of lateral epicondylitis. The authors suggest open or arthroscopic surgical debridement of the common extensor origin after failure of rest, orthoses, nonsteroidal drugs, physical therapy, cortisone and platelet-rich plasma injections. They do acknowledge that excessive debridement may compromise lateral elbow stability and cause PLRI.
O'Brien et. al. described the surgical techniques for managing PLRI, including an open technique for chronic injuries or revision treatment. In this setting, the authors suggest use of palmaris or gracilis allograft for reconstruction.
Figures A and B are an axial and coronal T2 weighted MRI of an elbow demonstrating signal intensity in the origin of the ECRB, consistent with lateral epicondylitis.
Incorrect Answers:
Question 80
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Explanation
Question 81
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical management has failed to provide relief. What is the treatment of choice?
Explanation
REFERENCES: Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.
Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.
Question 82
Which of the following is true regarding changes in the vascularity of the adult intervertebral disc with age? Review Topic
Explanation
The intervertebral disc is composed of an outer structure called the annulus fibrosis and an inner structure called the nucleus pulposus. The annulus fibrosis is composed
of type 1 collagen, water, and proteoglycans. The inner nucleus pulposus is composed of type 2 collagen, water, and proteoglycans. Intervertebral discs are avascular with capillaries terminating at the end plates. The nucleus pulposus receives nutrition primarily through diffusion through blood vessels within the endplate.
Roberts et al. review the histology and pathology of the intervertebral disc. They note that at birth, the cartilagenous end plates have large vascular channels through them as well as vascular channels through the annulus. Soon after birth, these vascular channels close with none remaining at the end of the first decade of life. However, with age, more blood vessels grow into the disc from the outer annulus fibrosis in response to degenerative changes.
Illustration A is a diagram of the vascular supply in an adult intervertebral disc. Incorrect Answers:
Question 83
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 84
Figures 42a through 42c show the MRI scans of a 56-year-old woman with progressively worsening low back and bilateral lower extremity pain. Based on these images, what muscle or muscle group would be expected to be weak on physical examination? Review Topic

Explanation
with L5-S1 spondylolisthesis. Many patients with spondylolisthesis report hamstring tightness; however, these structures are not usually weak. Quadriceps and tibialis anterior weakness is seen with L4 nerve root irritation. The gastrocnemius is generally weak in S1 nerve root syndromes.
Question 85
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Question 86
Figure 62 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks? Review Topic
Explanation
Question 87
A 17-year-old cross country athlete runs 7 miles per day, 6 days per week. She has new-onset right groin pain. Passive flexion of her hip is normal, but internal rotation of the hip, resisted hip flexion, and knee extension reproduce the pain. Hip radiograph findings are normal. What is the best next step?
Explanation
A stress fracture of the femoral neck or pelvis should be ruled out in this patient. She should be placed on crutches and not allowed to run. The consequences of missing such a diagnosis can be devastating. Superior cortical femoral neck stress fractures are tension injuries and can progress to a complete fracture and avascular necrosis. Surgical fixation may be indicated. Plain radiographic findings often do not appear until late in the clinical course. MRI is more accurate, more specific, and is superior to radionuclide bone scanning for the diagnosis of stress fracture in young endurance athletes. MRI detects early changes in osseous
stress injury and allows precise definition of the anatomy and extent of injury. This patient may have the female athletic triad: disordered eating, amenorrhea, and osteoporosis. However, the workup for this condition (including a possible DEXA scan) may be delayed until after the stress fracture is diagnosed and treated.

CLINICAL SITUATION FOR QUESTIONS 87 THROUGH 90
Figures 87a and 87b are the clinical photograph and radiograph of a 14-year-old high school football player who fractured his dominant right clavicle. The skin is closed and vascular and neurologic examination findings are normal.
Question 88
Immobilization with a sling
Explanation
Radiographically Active Cyst (age 4 to 8 years old with pathologic fracture)
Align and immobilize
Observe for spontaneous healing
Reassess after 2 to 4 months and if recurrent, follow procedure for pathological fracture of radiographically active cysts described in the article above.
Question 89
Second-impact syndrome following a concussion
Explanation
According to several consensus statements, no child or adolescent athlete with a concussion should be allowed to return to play on the same day, regardless of severity. Second-impact syndrome refers to a second traumatic head injury that occurs while an athlete is still experiencing symptoms from the first injury. Young athletes are particularly vulnerable to second-impact syndrome. The mechanism by which this syndrome occurs likely is disruption of cerebral autoregulation, which may result in cerebral vascular congestion, diffuse brain swelling, and death.

RESPONSES FOR QUESTIONS 2 THROUGH 6
Curettage and/or grafting
Radiofrequency ablation
Intravenous (IV) antibiotics
Incision, drainage, and IV antibiotics
Neoadjuvant chemotherapy followed by surgical reconstruction
Observation alone
For each clinical vignette seen in the figures, select the best initial treatment from the list above.
Question 90
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
REFERENCES: Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 91
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 92
Among patients with lumbar degenerative disk disease and low back pain, what factor is most predictive of clinical outcomes after surgical management? Review Topic
Explanation
Question 93
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?
Explanation
REFERENCES: Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212.
Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
Root MC, Orien WP, Weed JH: Normal and Abnormal Function of the Foot. Los Angeles, CA, Clinical Biomechanics Corporation, 1977, vol 2, pp 29-33.
Question 94
A 47-year-old woman has a right bunion that has been symptomatic despite modifications in shoe wear. She requests surgical correction. An AP radiograph is shown in Figure 37. Treatment should consist of
Explanation
REFERENCES: Coughlin MJ, Carlson RE: Treatment of hallux valgus with an increased distal metatarsal articular angle: Evaluation of double and triple first ray osteotomies. Foot Ankle Int 1999;20:762-770.
Coughlin MJ: Hallux valgus. Instr Course Lect 1997;46:357-391.
Question 95
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 96
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
REFERENCE: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 97
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann’s sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
REFERENCES: Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745.
Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 98
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 99
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
Explanation
metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller
and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations.
REFERENCES: Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements.
J Bone Joint Surg Am 2005;87:18-27.
Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.
Question 100
In addition to radiographs of the primary lesion and chest, MRI of the primary lesion, and CT of the chest, staging studies for Ewing’s sarcoma should include which of the following?
Explanation
REFERENCES: Schleiermacher G, Peter M, Oberlin O, Philip T, Rubie H, Mechinaud F, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Daldrup-Link HE, Franzius C, Link TM, Laukamp D, Sciuk J, Jurgens H, et al: Whole-body MR imaging for detection of bone metastases in children and young adults: Comparison with skeletal scintigraphy and FDG PET. Am J Roentgenol 2001;177:229-236.
