Orthopedic Board Review MCQs: Spine, Hip, & Shoulder | Part 123

Key Takeaway
This page offers Part 123 of a comprehensive Orthopedic Surgery Board Review MCQ bank. Designed for orthopedic residents and surgeons, it features 100 high-yield, verified multiple-choice questions mimicking OITE and AAOS exam formats. Utilize study and exam modes to master critical topics like Deformity, Foot, Hip, and Shoulder for board certification success.
About This Board Review Set
This is Part 123 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 123
This module focuses heavily on: Deformity, Foot, Hip, Shoulder, Tumor.
Sample Questions from This Set
Sample Question 1: A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicatedleft primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A ra...
Sample Question 2: The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?...
Sample Question 3: Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her sympto...
Sample Question 4: A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of...
Sample Question 5: What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 2
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
(TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene).
REFERENCES: Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Roodman GD: Mechanisms of bone metastasis. N Engl J Med 2004;350:1655-1664.
Question 3
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 4
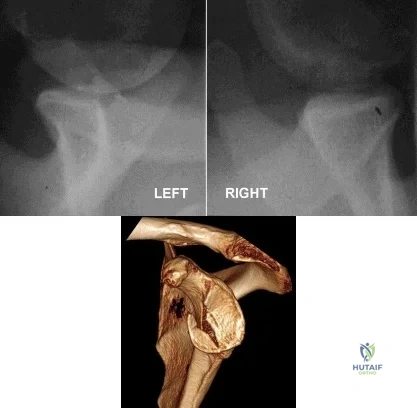
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 5
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 6
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 7
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular
Explanation
Question 8
An orthopaedic surgeon is counseling a patient regarding risk for complications following lumbar fusion via a direct lateral approach. Surgery at which level is most likely to injure the lumbosacral plexus?
Explanation
During the direct lateral approach, interbody fusion devices are inserted through a lateral window in the psoas muscle. To accomplish this, dilators and retractors are positioned at the posterior half of the disk space, and it must be noted that the lumbosacral plexus lies within the psoas muscle between the transverse process and vertebral body and departs distally at the medial edge of the psoas. Consequently, lateral interbody fusion poses risk for injury to the lumbosacral plexus. A cadaveric study demonstrated that the lumbosacral plexus progressively migrates from dorsal to ventral in the lumbar spine. Therefore, the plexus is most likely to be injured during an L4-L5 fusion because at this level the lumbosacral plexus is closest to the location at which dilators and retractors are placed.
A 2013 retrospective study by Le and associates followed 71 patients who underwent minimally invasive fusion via a lateral interbody approach. In this study, 54.9% (39/71) had immediate postsurgical ipsilateral iliopsoas or quadriceps weakness. Of these patients, the majority had resolution by 3 months (92.3%), and all had complete resolution by 2 years.
RECOMMENDED READINGS
Le TV, Burkett CJ, Deukmedjian AR, Uribe JS. Postoperative lumbar plexus injury after lumbar retroperitoneal transpsoas minimally invasive lateral interbody fusion. Spine (Phila Pa 1976). 2013 Jan 1;38(1):E13-20. doi: 10.1097/BRS.0b013e318278417c. PubMed PMID: 23073358.
View Abstract at PubMed
Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009 Feb;10(2):139-44. doi: 10.3171/2008.10.SPI08479. PubMed PMID: 19278328. View Abstract
at PubMed
Knight RQ, Schwaegler P, Hanscom D, Roh J. Direct lateral lumbar interbody fusion for degenerative conditions: early complication profile. J Spinal Disord Tech. 2009 Feb;22(1):34-
Question 9
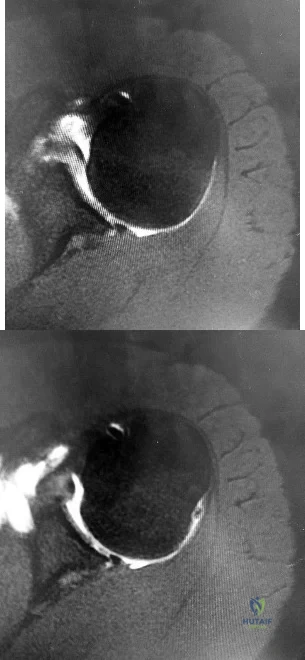
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
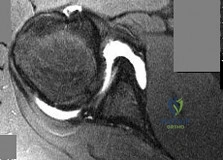
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
Toe is fused too straight (plantar flexed)
Toe is fused in too much valgus
Toe is fused in too much dorsiflexion
There is a nonunion of the fusion
Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 10
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Explanation
Question 11
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option? Review Topic
Explanation
Patients with glenoid bone defects >20-30% have a high recurrence rate (>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost
complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders. Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss. Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
Question 12
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 13
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
REFERENCES: Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Meding JB, Ritter MA, Keating ME, Faris PM: Impaction bone-grafting before insertion of a femoral stem with cement in revision total hip arthroplasty: A minimum two-year follow-up study. J Bone Joint Surg Am 1998;79:1834-1841.
Question 14
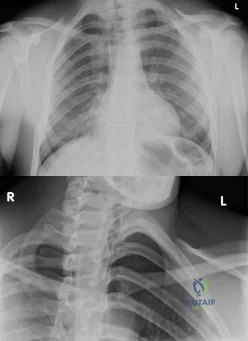
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is Review Topic
Explanation
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and
(3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
Question 15
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 16
Bacitracin is a topical antibiotic agent that may be added to solutions and used for intraoperative lavage. What is this agent effective against?
Explanation
REFERENCES: Rosenstein BD, Wilson FC, Funderburk CH: The use of bacitracin irrigation to prevent infection in postoperative skeletal wounds: An experimental study. J Bone Joint Surg Am 1989;71:427-430.
Brooks GF, Butel JS, Morse SA (eds): Jawetz, Melnick, and Adelberg’ s Medical Microbiology: Antimicrobial Chemotherapy. New York, NY, McGraw-Hill, 1995, pp 187-188.
Question 17
The spread of malignant cells to the vertebrae is often through
Explanation
REFERENCE: Batson OV: The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-149.
Question 18
A 70-year-old man with primary osteoarthritis undergoes a primary cementless total hip arthroplasty (THA). His history includes pelvis irradiation for prostate carcinoma (6000 rads). He is at increased risk for which complication?
Explanation
The complication associated with pelvic radiation prior to cementless THA is loosening of the acetabular component or postsurgical noningrowth of the component. Although scarring from radiation may put the hip at increased risk for arterial or nerve damage or infection, this risk has not been associated with pelvic radiation. Cementless acetabular components with porous metal surfaces such as trabecular metal should be considered.
Question 19
- Which of the following injuries is most commonly associated with a fracture of the scapular body?
Explanation
Question 20
A year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 21
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation? Review Topic

Explanation
Question 22
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively? Review Topic
Explanation
Question 23
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240.
Question 24
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
REFERENCES: Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Alleyne CH, Cawley CM, Shenglaia GC, et al: Microsurgical anatomy of Adamkiewicz’s artery. J Neurosurg 1998;89:791-795.
Question 25
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
REFERENCES: Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 26
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 27
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 28
A patient reports changes in vocal quality after undergoing a right-sided anterior cervical approach to C6. Which of the following nerves has most likely been injured?
Explanation
Question 29
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 30
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
REFERENCES: Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
Question 31
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs. New York, NY, Harper & Row, 1969.
Question 32
A 55-year-old man is about to undergo right total hip arthroplasty. A preoperative AP pelvis radiograph is shown in Figure below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?
Explanation
The radiograph shows that this patient has a high offset varus femoral morphology of both hips. Preoperative templating would identify this, and the surgeon should choose an implant system that has extended offset options to help match the native anatomy and biomechanics and minimize the risk of instability. Trialing a high offset neck, rather than a standard offset neck, is the next most appropriate step. Depending on the design of the implant system, this step can be accomplished by direct medialization of the femoral head, which would not affect leg length, or by lowering the neck angle, which would affect the leg length and would require a longer femoral head, because the leg lengths had previously been equal. Placement of a longer femoral head would likely improve hip stability but would also make the leg length uneven, which is a common cause of dissatisfaction after total hip arthroplasty. An offset acetabular liner also increases the leg length and does not correct the issue, which is on the femoral side. Trochanteric
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
Question 33
A 32-year-old laborer reports left ankle pain and deformity. History reveals that he sustained a left ankle fracture 2 years ago and was treated with closed reduction and casting. Radiographs are shown in Figures 25a through 25c. What is the most appropriate management?
Explanation
REFERENCES: Weber D, Friederich NF, Muller W: Lengthening osteotomy of the fibula for post-traumatic malunion: Indication, technique and results. Int Orthop 1998;22:149-152.
Lloyd J, Elsayed S, Hariharan K, et al: Revisiting the concept of talar shift in ankle fractures. Foot Ankle Int 2006;27:793-796.
Offierski CM, Graham JD, Hall JH, et al: Later revision of fibular malunion in ankle fractures. Clin Orthop Relat Res 1982;171:145-149.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
Question 34
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
REFERENCES: Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248.
Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Barber FA: Coplaning of the acromioclavicular joint. Arthroscopy 2001;17:913-917.
Question 35
-Figures 14a through 14d are the radiographs and sagittal T1- and T2-weighted MRI scans of an otherwise healthy 10-year-old girl who has experienced 3 weeks of worsening pain with weight bearing and is now refusing to bear weight to either of her lower extremities. She denies any history of injury or trauma.She has not had any fevers or recent illnesses. She denies any numbness or parasthesias. She has had no bowel or bladder incontinence. In the emergency department she is afebrile and tender to palpation over the midlumbar spine. She has pain with hyperextension and flexion of her back. Her white blood cell count is 11.4 (reference range, 4.5-11.0 x109/L), erythrocyte sedimentation rate is 40 mm/h (reference range, 0-20 mm/h), and C-reactive protein is 2.6 mg/L (reference range, 0.08-3.1 mg/L). What is the most appropriate course of action at this time?

Explanation

Question 36
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of
Explanation
REFERENCES: Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Pelligrini VD Jr, Konski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 37
What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?
Explanation
REFERENCES: Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
Question 38
A 38-year-old female with a grade IIIB open tibia fracture is scheduled to undergo definitive fixation and subsequent flap coverage with the orthopaedic and plastic surgery teams. She is met in the pre-operative area by the surgical intern and paperwork is completed per institutional protocol. She is then brought back to the operating room. Which of the following is true regarding the pre-surgical timeout?
Explanation
The WHO pre-surgical safety checklist involves assessment at three points during an operative procedure: before induction of anesthesia, before skin incision, and before the patient leaves the operating room. Some components of the checklist include
confirming IV access and allergies, administration of antibiotic prophylaxis, and surgical site verification. The surgeon has been shown to be the most effective team member at reducing complications when using the checklist.
Haynes et al. evaluated the effects of the WHO pre-surgical checklist on perioperative complication rates at eight international sites. They found a significant reduction in rates of complications and death in patients over the age of 16 undergoing noncardiac procedures after implementation of the checklist.
Illustration A shows the WHO pre-surgical checklist Incorrect Answers:
present for the timeout. Answer 2: The implant representative is not necessary for the timeout. Answer 4: The attending surgeon needs to be present in the same OR for the timeout. Answer 5: The timeout has been shown to decrease rates of complication and death.
Question 39
Which of the following indicates resolution of a postoperative wound infection? Review Topic
Explanation
Question 40
All of the following techniques can help to prevent apex-anterior angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
Question 41
Figures 5a and 5b show the clinical photograph and radiograph of a patient who has difficulty wearing shoes and has persistent symptoms medially and laterally at the first and fifth metatarsophalangeal joints. Because shoe modifications have failed to provide relief, management should now consist of
Explanation
REFERENCES: Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 415-435.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Question 42
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 43
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
Explanation
Question 44
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 45
A 14-year-old male sustains the injuries shown in Figures A and B after a fall off the roof of his house. What is the most appropriate management? Review Topic

Explanation
Pediatric femoral neck fractures are classified into transphyseal, transcervical, cervicotrochanteric and intertrochanteric (Delbets I-IV) respectively. Fixation type varies by author, but generally speaking, Types I-III can be treated with smooth wires for patients 0-3yrs of age, 4.5-6.5 mm cannulated screws 4-10yrs of age, or l 6.5-
Question 46
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Walch G, Nove-Josserand L, Boileau P, et al: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 47
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
Explanation
and degenerative joint disease.
Question 48
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
REFERENCES: Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 49
Figure 38 shows the radiograph of a 40-year-old woman who reports severe groin pain and lack of motion of the right hip. History reveals that the patient underwent a femoral osteotomy for hip dysplasia approximately 30 years ago. Treatment should include
Explanation
REFERENCE: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 789-802.
Question 50
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
REFERENCES: Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 51
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 52
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 53
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
at risk.
REFERENCES: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 281-289.
Question 54
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 55
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
Question 56
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Moskowitz A, Trommanhauser S: Surgical and clinical results of scoliosis surgery using Zielke instrumentation. Spine 1993;18:2444-2451.
Question 57
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?
Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 58
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
REFERENCES: Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 59
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
REFERENCES: Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
Question 60
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of Review Topic
Explanation
Question 61
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 62
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
REFERENCES: Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 63
A 23-year-old man was a restrained backseat passenger in a head-on motor vehicle collision. Examination revealed extensive bruising diagonally across his chest and abdominal areas and extreme pain at the thoracolumbar junction posteriorly. The lateral chest radiograph showed splaying of the spinous processes and increased disk height at the level of the injury, but no fracture of the vertebral bodies. He underwent a posterior spine fusion with instrumentation to stabilize the spine after a full trauma workup revealed the spine to be his only injury. Where is the center of rotation for this injury? Review Topic
Explanation
Question 64
What prosthetic factor has the most impact on decreasing the rate of scapular notching in a Grammont-style reverse total shoulder arthroplasty? Review Topic
Explanation
Question 65
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 66
What vessel is marked with an asterisk in Figure 44?
Explanation
REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.
Question 67
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 68
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 69
Currently, what is the most common clinical study type in the orthopaedic literature?
Explanation
Question 70
A 48-year-old man undergoes arthroscopy to repair a rotator cuff tear. During the arthroscopy, the tear is characterized and found to involve the entire supraspinatus and a majority of the infraspinatus tendons. After mobilization, the posterior rotator cuff can reach the greater tuberosity. However, the supraspinatus tendon cannot reach its insertion point at the greater tuberosity. What is the most appropriate treatment? Review Topic
Explanation
release, reverse acromioplasty, and tenotomy of the biceps tendon may improve shoulder pain. If these procedures fail, then a muscle transfer procedure can also be considered in select patients. If, however, a portion of the rotator cuff can be repaired, even partial repair can balance the coronal and axial forces about the shoulder to restore the kinematics of the joint. Reverse total shoulder arthroplasty is not appropriate for this relatively young patient.
Question 71
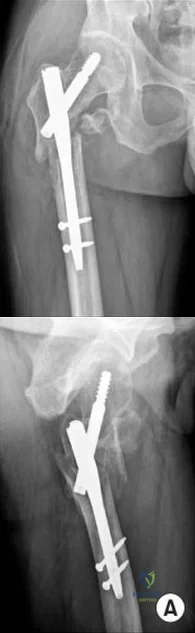
An 80-year-old patient presents 8 months postoperatively with right groin pain. Examination reveals a leg length discrepancy of 1.5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?
Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
(SBQ12TR.48) A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation
as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?

Age less than 30
Marijuana use
Use of negative pressure wound therapy
Male gender
Ability to return to work
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or
limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
1-4: These options are not as strong of a factor of patient satisfaction in long-term follow up after trauma-induced lower extremity amputation.
Question 72
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 73
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 74
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient’s pain. Treatment should now consist of
Explanation
REFERENCE: Delgado ED, Schoenecker PL, Rich MM, Capelli AM: Treatment of severe torsional malalignment syndrome. J Pediatr Orthop 1996;16:484-488.
Question 75
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
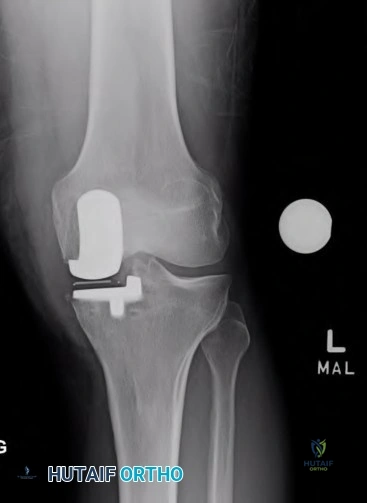
Explanation

OrthoCash 2020
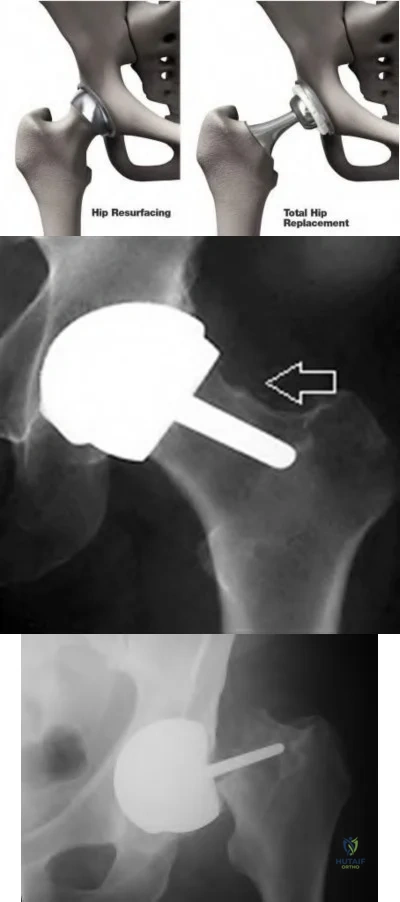
Which of the following is the most common cause of early revision surgery (<20 weeks) following a hip resurfacing arthroplasty?
Periprosthetic fracture
Rupture of abductors
Dislocation
Heterotopic ossification
Post-operative stiffness
Periprosthetic fracture, specifically femoral neck fracture, is the most common cause of early revision less than 20 weeks following surgery.
The rate of femoral neck fractures following hip resurfacing varies, but most literature reports a rate of 1%. A majority of these fractures happen in the early post-operative period and are the most frequent cause of revision surgery within several months following surgery. The cause is usually multifactorial, but placing the femoral implant in varus, osteonecrosis, and notching have been proven risk factors for fracture.
Little el al. report on 377 patients undergoing hip resurfacing. 13 required revision including 8 for fracture of the femoral neck and 3 for loosening of a component. Evidence of osteonecrosis was seen in two of these cases, leading the authors to believe it may contributed to fracture.
Illustration A shows a comparison of a typical total hip replacement and a hip resurfacing arthroplasty. Illustration B shows notching of the femoral neck, a known cause of femoral neck fracture following hip resurfacing. Illustration C shows a femoral neck fracture in a patient with a hip resurfacing.
OrthoCash 2020
A 55-year-old male undergoes a revision total knee arthroplasty of an implant that is only 3 years old. At the time of surgery, the tibial polyethylene liner shows catastrophic delamination and cracking. What is the most likely cause of this extensive, accelerated wear of the polyethylene liner?
Sterilization in ethylene oxide
Gamma irradiation of the polyethylene liner in the presence of air
Gamma irradiation of the polyethylene liner with vacuum packaging
Gamma irradiation of the polyethylene liner in nitrogen
Gamma irradiation of the polyethylene liner in argon Corrent answer: 2
Irradiation of polyethylene in air (i.e. oxygen present) has been shown to be a risk factor for catastrophic failure after total knee replacement.
Free radicals are generated when polyethylene is irradiated in the presence of air. Initially, these free radicals result in cross-linking. However, if the polyethylene is exposed to these free radicals for an extended period of time, delamination, cracking, and catastrophic failure may ensue. The industry has completely abandoned this method of sterilization as a result. Currently, the standard of care is irradiation of polyethylene in an inert gas (e.g. argon, nitrogen or vacuum packaging). The amount of oxidative products when polyethylene is sterilized in the absence of oxygen is much less and does not lead to catastrophic failure.
Sterilization without irradiation is another option (ethylene oxide). When this occurs, there is no cross-linking and thus the increased wear properties are lost. However, since there is no oxidization, you do not have the risk of catastrophic failure as seen in those liners irradiated in the presence of oxygen.
The cited reference by McNulty et al. from Orthopedics discusses the influence of sterilization methods on wear performance. They found that gamma irradiation and storage of the polyethylene components in an essentially oxygen-free environment imparted by gamma irradiation in a vacuum foil pouch (GVF) protects the components from oxidization.
Illustration A shows a polyethylene liner that has undergone catastrophic wear as a result of irradiation in the presence of oxygen.
Incorrect Answers:
catastrophic wear, although wear properties are less than gamma irradiation in the absence of air.

OrthoCash 2020
Which of the following interventions reduces osteolysis around distal portion of the femoral stem when performing a total hip arthroplasty?
Use of an extended offset femoral neck component
Use of a proximal circumferentially coated ingrowth stem
Use of a collared stem
Use of a long femoral stem
Ensuring that the stem fills the diaphysis of the femur Corrent answer: 2
Osteolysis of the femur is caused by activation of macrophages by microscopic polyethylene particles within the "effective joint space", defined as any area where joint fluid can come into contact with bone. This can occur above the acetabular cup, through screw holes, and down the femoral shaft around the prosthetic stem. Ideally, with a cementless stem, both the proximal and metaphyseal femur are well filled by the prosthesis. Collared stems are used to augment poor calcar bone quality or bone loss.
Sinha et al showed in a retrospective review of 101 hips with cementless circumferentially coated femoral stems no distal femur osteolysis occurred, but 82% showed “evidence of proximal femur stress shielding”, though only 38% showed proximal femoral osteolysis.
OrthoCash 2020
During a minimally invasive approach to total hip arthroplasty a femoral periprosthetic fracture occurs. Which of the following steps is crucial to properly treat this complication?
Transitioning to an extensile approach to adequately visualize and reduce the fracture
Limiting post-operative weight bearing
Switching to a cemented femoral stem to avoid the stresses created during press-fit fixation
Delaying the arthroplasty until the fracture has healed
Supplementing the fracture with autograft Corrent answer: 1
Proper treatment of an intraoperative femoral fracture during total hip arthroplasty involves adequate exposure, anatomic reduction, and bypassing the fracture site by 2 cortical diameters of the femur with a long stem. This may involve repositioning the patient on the table if the arthroplasty is performed in the supine position. Minimally invasive surgical techniques have been developed to insert the components through smaller exposures and less soft tissue dissection. The purported advantages include faster rehabilitation, less blood loss, shorter hospital stays, and better cosmesis. However, complications an arise if the surgeon sacrifices surgical exposure and visualization.
Fehring et al review 3 cases of total hip arthroplasty performed through minimally invasive techniques with catastrophic outcomes. Intra-operative fracture, chronic instability, and death were all identified.
OrthoCash 2020
A 70-year-old man underwent total hip arthroplasty 4 months ago and has experienced 3 dislocations. Radiographs reveal no failure of the hardware and an acetabular component that has an abduction
angle of 40 degrees and a version of 10 degrees retroverted. What is the most appropriate treatment for the recurrent dislocations?
hip abduction brace
revision of the acetabular liner to a constrained type
revision of the entire acetabular component
revision of the femoral head to a larger size
revision to an extended offset prosthesis Corrent answer: 3
Per Dorr et al: post-operative hip instability can be caused by several factors: soft tissue imbalance, component malposition, or position. Component malposition, as in this case, should be treated with revision of the offending component. In this case the acetabulum was placed in retroversion when it should have been 15-20 degrees anteverted. None of the other options addresses the cause of the instability. According to Morrey, the most signficant risk factors to instability are prior hip surgery, trochanteric nonunion, and posterior surgical approach. He wrote that the most reliable way to correct instability is to reorient a retroverted acetabular cup.
OrthoCash 2020
In patients with sickle cell disease and asymptomatic osteonecrosis of the femoral head identified with magnetic resonance imaging, what percentage will eventually go on to femoral head collapse?
Question 76
below shows the abdominal radiograph obtained from a year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to the administration of
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.
Question 77
Figures below show the AP and lateral radiographs obtained from a 54-year-old woman who has worsening groin pain 18 months after a primary left total hip arthroplasty. The pain is worst when climbing stairs, when rising from a seated position, and during resisted hip flexion. Her pain improved early after surgery but did not completely resolve. Her C-reactive protein and erythrocyte sedimentation rate results of less than 1 mg/dL and 10 mm/hr, respectively, were obtained in the office. What is the best next step?
Explanation
Iliopsoas impingement is a potential cause of persistent groin pain after a total hip arthroplasty. This patient’s history gives groin pain with resisted hip flexion and during activities that require this level of function. The radiographs depict an acetabular component with substantial retroversion. Typical options for the management of iliopsoas tendon impingement include injections, tenotomy, and acetabular revision. Recently, Chalmers and associates reported more predictable groin pain resolution with 8 mm or more of anterior acetabular component when overhang was revised. The radiographs clearly show more retroversion, with a cup prominence of more than 8 mm anteriorly. MRI with MARS could potentially help in the diagnosis of this impingement but would not help in management (option A). An ultrasound- guided injection would need to be administered into the iliopsoas tendon sheath to be of help and, in this case, would likely be performed for diagnostic purposes due to the extreme anterior overhang (option C). Option D would be useful for mild cases of iliopsoas impingement but likely would not help much in this more extreme case.
Question 78
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 79
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 80
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Skalley TC, Myerson MS: The operative treatment of acquired hallux varus. Clin Orthop 1994;306:183-191.
Question 81
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 82
Ulnar collateral ligament (UCL) reconstruction using a modified Jobe technique
Explanation
Certain complications are more strongly associated with the approach and surgical procedure for elbow pathology. With a 2-incision distal biceps repair, heterotopic ossification
with a radial-ulnar synostosis is a concern. This complication can be minimized through irrigation of bone debris and care to avoid dissection between the radius and ulna. With a single-incision distal biceps repair, the lateral antebrachial cutaneous nerve is retracted during the procedure. Numbness on the lateral side of the forearm is common, although often temporary. During arthroscopic debridement for lateral epicondylitis, injury to the radial UCL can occur, leading to posterolateral rotatory instability of the elbow. The modified Jobe technique for UCL reconstruction typically involves an ulnar nerve transposition during the procedure. Numbness and tingling in the fourth and fifth digits are concerns when this procedure is performed.
Question 83
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?
Explanation
REFERENCES: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lee JK, Yao L: Stress fractures: MR imaging. Radiology 1988;169:217-220.
Question 84
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate Review Topic

Explanation
Question 85
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 86
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 87
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of
Explanation
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
Question 88
The initiating cellular event in development of posttraumatic osteoarthritis is attributed to which of the following?
Explanation
Question 89
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 90
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
Explanation
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
Question 91
Figures below show the radiographs, and the MRIs obtained from a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 92
In the United States, groups at risk for community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) within the pediatric and adolescent populations include
Explanation
CA-MRSA is a growing problem in the United States. Groups at risk for CA-MRSA include athletes in contact sports and children in daycare. Tennis players, golfers, and runners are at lowest risk because their sports do not require close contact with teammates or competitors. Outbreaks have been noted in Alaskan native, Native American, and Pacific Islander minority populations.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 68
Figures 64a through 64d are the radiographs of an 11-year-old boy with a prolonged history of activity-related ankle pain. An examination is notable for restricted subtalar motion and moderate pes planovalgus.
Question 93
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
REFERENCES: Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed):
Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 94
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
REFERENCES: Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton- Century-Crofts, 1976, pp 249-254.
Question 95
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely
Explanation
REFERENCES: Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am
1993;75:1282-1297.
Question 96
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
Explanation
REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.
Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 97
What is the most likely explanation for the change between the initial intraoperative radiograph (Figure 11a) and the radiograph taken 4 weeks after surgery (Figure 11b) in an 87-year-old man who underwent primary hip replacement for osteoarthritis?

Explanation
The image demonstrates subsidence of the femoral implant. The implant subsided because it did not have good initial stability. The tapered femoral implant was placed after initial preparation for an anatomic femoral stem. A limited, nondisplaced femoral neck fracture was encountered during the procedure and treated. Two advantages of tapered stems are the efficient transfer of stress to the proximal femur and the ability to accommodate some subsidence to achieve enhanced stability. Although subsidence of a tapered stem to a more stable position can produce a good result, quality of metaphyseal bone should be considered. Attention to surgical technique remains important to optimize component stability for biological fixation.
RECOMMENDED READINGS
Savory CG, Hamilton WG, Engh CA Sr, Della Valle CJ, Rosenberg AG, Galante JO. 15 Hip designs. In: Barrack RL, Booth RE Jr, Lonner JH, McCarthy JC, Mont MA, Rubash HE, eds. Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:345-368.
Blaha JD, Borus TA. Press-fit femoral components. In: Callaghan J, Rosenberg A, and Rubash H, eds The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:1036-1043.
Question 98
Figure A is a pelvic radiograph of a healthy 20-month old girl with a limb leg discrepancy. A hip arthrogram under general anesthesia reveals concentric reduction of the left hip ONLY when the hip is positioned in 70 to 80 degrees of abduction. The next best step in treatment would be: Review Topic

Explanation
capsulorrhaphy, +/- femoral osteotomy +/- pelvic osteotomy
In children older than 18 months, open reduction is the preferred treatment for hip dysplasia. Open reduction is also considered when concentric closed reduction cannot be achieved or when excessive abduction (>60 degrees) is required to maintain reduction (due to increasing risk of avascular necrosis). The goal of open reduction is to remove the blocks to reduction and to increase stability by preforming soft-tissue or bone procedures.
Wenger et al. reviewed the surgical treatment of DDH. They say that the impediment to congruent reduction are the iliopsoas muscle, joint capsule, ligamentum teres, pulvinar, labrum, and transverse acetabular ligament. The most commonly used approaches are anterior and medial/anteromedial to the hip.
Gholve et al. reviewed DDH and the factors that contribute to secondary procedures. In their study, neither age nor unilateral vs bilateral dislocation had a direct influence on the outcome or the need for secondary procedures. The variable that significantly influenced the need for a secondary procedure was the concomitant use of a femoral osteotomy during initial surgical treatment. Of the 27 patients who did not have concurrent femoral osteotomy at index surgery, 19/27 (73%) required a secondary procedure (P<0.001).
Figure A shows an AP pelvic radiograph of an infant. Focusing on the left hip, there is lateral and superior subluxation of the femoral head, with the femoral head lateral to Perkin's line. The medial joint space is increased. The acetabular index is increased
>30 degrees. Shenton's line is disrupted. These are all features of DDH.
Incorrect Answers:
Question 99
- Which of the following factors is used to determine torsional rigidity of a long bone fracture under internal or external fixation?
Explanation
quantity having a magnitude and direction. Torsion involves shear and tensile stresses that cause deformation. Thus torsional rigidity is related to bone rotation and the torque applied to it.
Question 100
A 32-year-old recreational basketball player underwent a successful anterior cruciate ligament (ACL) reconstruction using hamstring autograft approximately 15 months ago. His chart notes that he has good functional knee outcome scores as tested by his physical therapist. However, he has not returned to play despite being cleared by his physician 3 months ago. After successful ACL reconstruction, which of the following factors has shown to contribute the greatest influence on a player's decision to return to sport? Review Topic
Explanation
The return to their preinjury level of sport is frequently expected within 1 year after anterior cruciate ligament (ACL) reconstruction, yet many athletes do not achieve this milestone. Having a previous ACL reconstruction to either knee, poorer hop-test symmetry and subjective knee function, and more negative psychological responses were associated with not returning to the preinjury level sport. Fear of reinjury is considered one of the most common reasons cited for a postoperative reduction in or
cessation of sports participation.
Tjong et al. conducted a qualitative study of 31 patients, aged 18 to 40 years, to understand the factors influencing a patient's decision to return to his or her preinjury level of sport after ACL reconstruction. They found 3 overarching factors what largely influenced their decision to return to the preinjury sport: fear, lifestyle changes, and innate personality traits. This highlighted the importance of recognizing and addressing the psychological factors and lifestyle changes that significantly contribute to a patient's postoperative decision to return to sport.
Ardern et al. investigated the return-to-sport rates at 2 years after ACL reconstruction in athletes. At 2 years after surgery, 66% were playing sport, with 41% playing their preinjury level of sport and 25% playing a lower level of sport. Demographics, physical function, and psychological factors were supported as the most important influencing factors for the return to their preinjury level of sport.
Incorrect Answers:
