Orthopedic Surgery Board Exam MCQs: Shoulder, Nerve, & Spine | Part 121
Key Takeaway
This page presents Part 121 of a high-yield interactive MCQ bank for orthopedic surgeons preparing for AAOS and ABOS board certification. It offers 100 verified questions in OITE/AAOS format, covering Nerve and Shoulder topics, with detailed explanations and references to maximize exam preparation effectiveness.
About This Board Review Set
This is Part 121 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 121
This module focuses heavily on: Nerve, Shoulder.
Sample Questions from This Set
Sample Question 1: A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective...
Sample Question 2: After performing an open distal clavicle excision and resecting 15 mm of distal clavicle, which potential concern for shoulder function could result?...
Sample Question 3: A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusi...
Sample Question 4: -A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the ...
Sample Question 5: What is the function of the rotator cuff during throwing?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
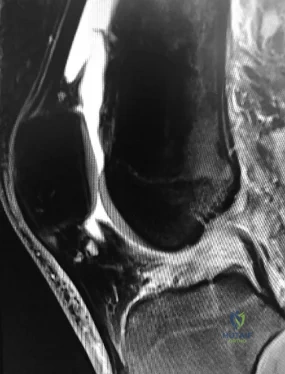
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 2
After performing an open distal clavicle excision and resecting 15 mm of distal clavicle, which potential concern for shoulder function could result?
Explanation
AC joint arthritis often is marked by pain along the anterior and superior aspects of the shoulder. It can occasionally radiate into the trapezius and the anterolateral neck region. A patient may have tenderness to palpation directly at the AC joint or pain with the cross-body adduction stress test and the O'Brien active compression test. During the cross-body adduction test, this patient has pain when the examiner lifts his arm in 90 degrees of forward flexion and maximally adducts it across his body. Although the cross-body adduction test is the most sensitive provocative test for AC joint osteoarthritis at 77%, the O’Brien active compression test has been shown to be most specific at 95%.
Physical therapy, rest, activity modification, and other nonsurgical treatments might not reverse osteoarthritis changes at the AC joint, but these interventions can often help improve pain, range of motion, and function. A corticosteroid injection into the AC joint may be an option if nonsurgical treatments do not work, although Wasserman and associates demonstrated that only 44% of AC joint injections accurately entered the joint.
Persistent pain is the most common complication following distal clavicle excision. Although the exact amount of distal clavicle that should be resected is a topic of debate, resection of 10 mm or more of the distal clavicle may lead to instability of the AC joint, especially if the AC capsule is sectioned.
Question 3
A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusion across the atlanto-axial junction?
Explanation
C1-C2 transarticular screw fixation is 10-fold stiffer than wiring constructs, particularly in rotation; eliminates the need for postsurgical halo use; and is associated with reported fusion rates to a maximum of 100% for bilateral screws and 95% for unilateral fixation. All of the other fusion techniques mentioned are associated with a pseudarthrosis rate of at least 30%.
RECOMMENDED READINGS
Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. View Abstract at PubMed
Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
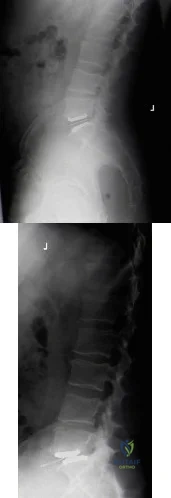
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
Question 4
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 5
What is the function of the rotator cuff during throwing?
Explanation
REFERENCES: Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 6
below show the radiographs obtained from a year-old woman with a year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 7
Treatment of a cruciate-retaining total knee that is unstable in flexion is best accomplished by
Explanation
REFERENCE: Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate-retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Question 8
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 9
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
(ie, the means and standard deviations).
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 10
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 11
03 A 13 y/o girl sustains the injury shown in Figures 69a and 69b in a fall. Examination reveals this to be an isolated injury, and the patient’s neurologic and vascular examinations are normal. Based on these findings, management should consist of
Explanation
pinning may be performed. If the articular surface shows that the fx line has extended into the joint and the articular surface is separated, open reduction and pinning are necessary. Once the fx is stabilized, the elbow is immobilized for 4 wks. The pins are then removed & motion is begun.
back to this question next question
Question 12
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?

Explanation
Question 13
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 14
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
Question 15
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.
Question 16
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 17
What is the most common complication associated with open reduction and internal fixation using a 90/90 plate configuration and olecranon osteotomy for an OTA type C2 distal humerus fracture?
Explanation
Question 18
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
Explanation
REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 19
A 46-year-old male sustains a patella fracture and is treated with cannulated screws and a tension band construct. Which of the following is correct regarding this treatment?
Explanation
Tension band constructs result in absolute stability when performed correctly. This technique works by converting tension from muscle pull into compressive force on the articular side of the fracture. Tension band constructs require a fracture pattern or bone that is able to withstand compression, an intact cortical buttress opposite to the tension band, and fixation that withstands tensile forces.
LeBrun et al. and associates evaluated functional outcomes of surgically isolated patella fractures. They reported that 52% of patients underwent surgery for hardware removal, and 38% of patients who retained their hardware reported pain at some time. They also found that nearly 20% had extensor lag, and almost 38% had restricted flexion. Extension power on testing showed significant mean deficits when compared to the contralateral side.
Bayar et al. evaluated 20 patients with patella fractures and found that articular incongruity of >1mm was the largest risk factor for quadriceps weakness at a mean of 30 months postoperatively. No significant differences were seen with sex, fracture pattern, or time from injury to surgery.
Illustration A shows patella fixation with plate/screw construct. Incorrect Answers:

OrthoCash 2020
Question 20
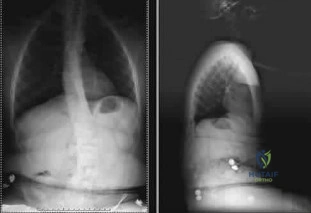
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic
Explanation
Question 21
Figure 24 shows the sitting AP and lateral spinal radiographs of a nonambulatory 12½-year-old boy with Duchenne muscular dystrophy who is being evaluated for scoliosis. The lumbar curve from T12 to L5 measures 36 degrees, and the thoracic curve from T3 to T12 measures 24 degrees on the AP radiograph. He has 5 degrees of pelvic obliquity. His forced vital capacity is 45% of predicted for height and weight. What is the most appropriate treatment for the spinal deformity? Review Topic
Explanation
Question 22
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 23
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 24
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
REFERENCES: Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int
2001;22:47-50.
Trnka HJ, Muhlbauer M, Zettl R, et al: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 25
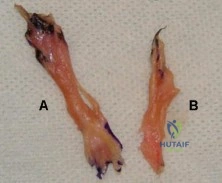
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true? Review Topic
Explanation
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle.
Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion
>30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect
Question 26
At the time of arthroscopy, a 9-year-old boy was found to have a Watanabe type II discoid lateral meniscus. What is the most appropriate treatment? Review Topic
Explanation
Question 27
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
REFERENCES: DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 28
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?
Explanation
REFERENCES: Weinstein JN, Kuo KN, Millar EA: Congenital coxa vara: A retrospective review. J Pediatr Orthop 1984;4:70-77.
Beaty JH: Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 409-425.
Question 29
BMP is FDA approved for well-defined medical conditions in limited patient populations. In which of the following clinical scenarios is use of rhBMP-2 FDA approved?
Explanation
rhBMP-2 is also FDA approved for use in open tibial shaft fractures stabilized with an IM nail and treated within 14 days of initial injury. rhBMP-7 has received FDA humanitarian device exemption approval as an alternative to autograft in recalcitrant long bone nonunions where use of autograft is unfeasible and alternative treatments have failed. It is also approved as an alternative to autograft in compromised patients (with osteoporosis, smoking or diabetes) requiring revision posterolateral/intertransverse lumbar fusion for whom autologous bone and bone marrow harvest are not feasible or are not expected to promote fusion.
Epstein reviewed the indications for rhBMP-2 use and its off-label use. She found that
anterior cervical surgery with BMP2 led to dysphagia and airway complications. With posterior lumbar spine surgery, complications included vertebral osteolysis (bone resorption) and ectopic bone formation/heterotopic ossifications, which made revision surgery difficult.
Burkus et al. prospectively compared 46 patients undergoing single-level ALIF with BMP-2 vs with autograft in an industry sponsored study. They found that patients receiving BMP-2 had higher rates of fusion and improvement in pain and neurologic status at 12 and 24 months compared with autograft, and there were no adverse events. They recommend rhBMP-2 in ALIF procedures to eliminate pain and scarring from iliac crest bone harvest.
Illustration A shows the FDA approved combination of INFUSE (rhBMP-2) and LT-CAGE device.
Incorrect Answers:
Question 30
A 42-year-old female with chronic discogenic back pain undergoes lumbar spine surgery via retroperitoneal approach. Figure A is the postoperative radiograph of her lumbar spine. Six weeks after the surgery the patient develops worsening low back pain. You obtain a radiograph of her lumbar spine, pictured in Figure B. What is the next best step in management? Review Topic
Explanation
Management of failed TDR is dictated by (1) patient symptoms and (2) radiographic implant position. Asymptomatic patients with implant subsidence without extrusion can be managed with close observation. Patients with persistent symptomatic back pain relating to facet joint or implant microinstability in the setting of an otherwise well-positioned TDR can be treated with posterior stabilization alone. Symptomatic patients with unacceptable implant position (i.e. complete dislodgement, fracture) require either revision arthroplasty or conversion to arthrodesis (anterior +/-
posterior).
Harrison et al. authored a report detailing a case of failed L5-S1 TDR with anterior dislocation of the polyethylene inlay and bilateral L5 pars fractures noted 2 weeks postoperatively. It is unclear whether the pars defect was missed following previous microdiscectomy, acquired during instrumentation, or acquired postoperatively due to abnormal endplate forces during rehabilitation. The patient underwent removal of TDR components and revision to anterior arthrodesis followed by percutaneous fixation of the bilateral L5 pars fractures.
Patel et al. published a review of the literature regarding revision lumbar TDR. Retroperitoneal revision procedures are complicated by higher risk of injury to vascular structures (16.7% versus 3.6% at primary surgery) and urogenital structures due to adhesions. Revision surgery should only be performed by surgeons familiar with the retroperitoneal approach to the spine. Alternative surgical approaches, such as the far lateral approach, should be considered to access the anterior spine at L4-L5 and above.
Madigan et al. reviewed the management of lumbar degenerative disc disease (DDD). They state that TDR is a motion-sparing surgical option designed to temper the problem of adjacent-segment disease. They report that long-term studies are limited, but point out that several short-term comparisons between TDR and ALIF show equivalent improvement in pain and function, equal complication rate, shorter hospitalization and lower rate of reoperation in the TDR group.
Figure A is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement. Figure B is a lateral radiograph of the lumbar spine showing L5-S1 total disc replacement with anterior dislocation of the polyethylene inlay.
Incorrect Responses:
Question 31
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50°. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
REFERENCES: Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe’s Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 32
An 8-year-old boy falls and injures his thumb. A radiograph is shown in Figure 23. Initial management should consist of
Explanation
REFERENCES: O’Brien ET: Part IV: Dislocations of hand and carpus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 429-431.
Bohart PC, Gelberman RH, Vardell RF, Solomon PB: Complex dislocations of the MCP joint. J Bone Joint Surg Am 1974;56:1459-1463.
Question 33
03 Figure 33 shows the radiograph of a 48-year-old man who sustained a fracturedislocation of his dominant arm and a significant head injury in a fall from a roof. Eight days after injury he is medically cleared for surgery. Treatment should consist of

Explanation
proximal humerus, with what appears to be a head-splitting component. Answer 1
(rotator cuff repair) is certainly not indicated yet – maybe as a secondary procedure
once the bone is healed, or as a subsequent procedure while dealing with the fracture.
Similar to question #109, there is no need to resurface the glenoid unless we have
evidence of significant degenerative changes, which we don’t. ORIF of head-splitting
fractures hasn’t had any promising results, and AVN is always an issue here. Both
articles referenced discuss the outcomes of acute hemiarthroplasty in the
treatment of 3- and 4-part proximal humerus fractures versus late replacement for
failed non-operative treatment, and the benefits of early management in regards
to difficulty of procedure, post-operative pain, and functional ROM/strength outcomes. Arthrodesis is a viable option, but not with the good results of hemiarthroplasty as evidenced here.
Goldman RT, Koval KJ, Cumom F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and four-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Norris TR, Green A, McGuigan FX: Late prosthetic shoulder arthroplasty for displaced proximal humerus fracture. J Shoulder Elbow Surg 1995;4:271-280.
back to this question next question
Question 34
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
corrective osteotomy.
REFERENCES: O’Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369.
Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Spinner RJ, O’Driscoll SW, Davids JR, et al: Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg 1999;24:718-726.
Question 35
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
Explanation
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If it were injured, the result would not be weakness of interphalangeal joint extension.
Question 36
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 37
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Explanation
REFERENCE: Hockenbury RT, Johns JC: A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990;11:67-72.
Question 38
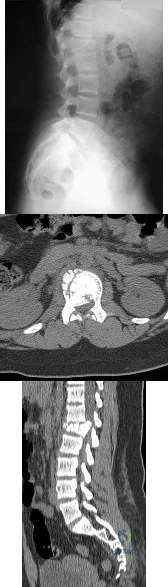
A B Figures 60a and 60b are the postmyelography CT images of a 62-year-old man who has had low-back and bilateral lower-extremity pain. His pain began approximately 1 year ago and there was no precipitating event. The location of the pain is in the lower lumbar region in the midline and it radiates into the buttocks and thighs bilaterally. The pain is exacerbated by standing and walking and relieved by forward spine flexion. He reports no pain while sitting or lying supine. Upright radiographs demonstrate 4 mm of anterolisthesis of L4 on L5. What is the most appropriate surgical procedure?

Explanation
This patient radiographically has L4-5 degenerative stenosis and a low-grade spondylolisthesis. The axial images demonstrate a gap in the facet joint, more on the left than the right, which is highly suggestive of dynamic instability. Thus, this patient would most benefit from a laminectomy and fusion of L4-5. A microdiskectomy would not be helpful as this patient does not have a disk herniation. Patients undergoing posterior decompression alone experience an unacceptably high rate of recurrent stenosis and/or progression of spondylolisthesis. Early studies demonstrated that adding an intertransverse process fusion to posterior decompression significantly improved clinical outcomes. Anterior interbody fusion likely will not decompress the spinal canal sufficiently, though there is some thought that indirect decompression can be effective in some cases.
RECOMMENDED READINGS
Frymoyer JW. Degenerative Spondylolisthesis: Diagnosis and Treatment. J Am Acad Orthop Surg. 1994 Jan;2(1):9-15. PubMed PMID: 10708989. Majid K, Fischgrund JS. Degenerative lumbar spondylolisthesis: trends in management. J Am Acad Orthop Surg. 2008 Apr;16(4):208-15. Review. PubMed PMID: 18390483. View Abstract at PubMed
Carlisle E, Fischgrund JS. Lumbar spinal stenosis and degenerative spondylolisthesis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006: 299-317.
Puschak TJ, Sasso RC. Spondylolysis-spondylolisthesis. In: Vaccaro AR, ed. Orthopaedic Knowledge Update 8. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2005:553-563.
Question 39
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle? Review Topic

Explanation
such as Parsonage-Turner syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
Question 40
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 41
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 42
Which of the following is a recognized consequence of hip fusion?
Explanation
REFERENCES: Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Sponseller PD, McBeath AA, Perpich M: Hip arthrodesis in young patients: A long-term follow-up study. J Bone Joint Surg Am 1984;66:853-859.
Question 43
Figure below shows the radiograph obtained from a 73-year-old woman who returns status post total hip arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis. This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis indefinite observation would not be appropriate. A foot drop develops 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MRI or CT may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be reduced by flexing the surgical knee and positioning the bed flat.
Question 44
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of
Explanation
REFERENCES: Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
Thompson CE, Larsen LJ: Recurrent hip dislocation in intermediate spinal atrophy.
J Pediatr Orthop 1990;10:638-641.
Question 45
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?
Explanation
REFERENCES: Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Chapman JR, Henley MB, Agel J: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Question 46
An active 65-year-old man has pain in the left shoulder 5 years after undergoing a hemiarthroplasty. He has a remote history of two previous instability operations. Examination reveals that forward elevation is 140 degrees and external rotation is 40 degrees. Serologic studies for infection are negative. AP and axillary radiographs are shown in Figures 7a and 7b. What surgical procedure will provide the most predictable pain relief and function? Review Topic

Explanation
Question 47
The modified Brostrom lateral ankle ligamentous reconstruction uses which of the following structures to provide supplementary stabilization?
Explanation
REFERENCES: Gould N, Seligson D, Gassman J: Early and late repair of lateral ligament of the ankle. Foot Ankle 1980;1:84-89.
Hamilton WG, Thompson FM, Snow SW: The modified Brostrom procedure for lateral ankle instability. Foot Ankle 1993;14:1-7.
Chrisman OD, Snook GA: Reconstruction of lateral ligament tears of the ankle: An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am 1969;51:904-912.
Evans DL: Recurrent instability of the ankle: My method of surgical treatment. Proc R Soc Med 1953;46:343.
Watson-Jones R: Fractures and Joint Injuries, ed 3. Baltimore, MD, Williams and Wilkins, 1946, p 234.
Liu SH, Baker CL: Comparison of lateral ankle ligamentous reconstruction procedures. Am J Sports Med 1994;22:313-317.
Brostrom L: Sprained ankles: VI. Surgical treatment of “chronic” ligament ruptures. Acta Chir Scand 1966;132:551-565.
Question 48
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of
Explanation
REFERENCES: Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289.
Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Damron TA, McBeath AA: Arthrodesis following failed total knee arthroplasty: Comprehensive review and meta-analysis of recent literature. Orthopedics 1995;18:361-368.
Question 49
In the Lauge-Hansen classification system, a pronation-abduction ankle fracture has what characteristic fibular fracture pattern?

Explanation
Question 50
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
Question 51
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
REFERENCE: Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 364.
Question 52
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
Marmor L, Bechtal CO: Paralysis of the serratus anterior due to electric shock relieved by transplantation of the pectoralis major muscle: A case report. J Bone Joint Surg Am 1983;45:156-160.
Question 53
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
REFERENCES: Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Sammarco GJ: How I manage turf toe. Phys Sports Med 1988;16:113-118.
Question 54
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
REFERENCES: Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels’ Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 55
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty? Review Topic
Explanation
Question 56
An athletic 55-year-old man reports a painless mass in the anterior aspect of the thigh that appeared 3 weeks ago and has not changed in size. The patient denies any history of trauma. Examination reveals a firm, well-defined nontender mass in the anterior thigh and no inguinal adenopathy or cutaneous changes. Plain radiographs are unremarkable. T1- and T2-weighted MRI scans are shown in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 57
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?
Explanation
REFERENCES: Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14.
Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 58
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 59
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 60
Which of the following best describes the mechanism of action of gentamycin?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-236.
Question 61
An year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 0 mg/L (reference range 08 to 1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly
difficult with activities of daily living and mobility.
Question 62
During an anterior approach to the bicipital 53 tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the

Explanation
The structure shown is the lateral antebrachial cutaneous nerve (LABC). It is the terminal sensory branch of the musculocutaneous nerve and runs superficial to the brachioradialis. It supplies sensation to the anterolateral surface of the forearm. The flexor pollicis longus is innervated by the anterior interosseous nerve. The extensor indicis proprius is innervated by the radial nerve. The LABC does not innervate the skin of the anteromedial forearm. Careful
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61

Please select the image that represents the most appropriate response to the question or statement below.
Question 63
A 25-year-old male is involved in an high-speed motor vehicle collision and sustains a closed femoral shaft fracture. During further evaluation, a CT scan of the chest/abdomen/pelvis reveals a non-displaced ipsilateral femoral neck fracture. Which of the following treatment options will most likely achieve anatomic healing of both fractures, mobilize the patient, and minimize the risk of complications?

Explanation
Question 64
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
REFERENCES: Dreese J, D’Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207.
Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Fuchs B, Jost B, Gerber C: Posterior-inferior capsular shift for the treatment of recurrent voluntary posterior subluxation of the shoulder. J Bone Joint Surg Am 2000;82:16-25.
Question 65
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 66
What type of nerve palsy is most common following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 67
A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the site of the tenderness, about 7 cm above the lateral heel, provided temporary relief of the pain. What is the recommended course of management for the persistent burning pain?
Explanation
Question 68
Which Morton neuroma histology is most common?
Explanation
Morton neuroma is a compressive neuropathy of the interdigital nerves of the forefoot that most commonly is noted in the third web space. Perineural fibrosis is commonly noted on microscopic examination of resected tissue. This accounts for the relatively higher failure rate of neuroma decompression by transection of the intermetatarsal ligament as opposed to resection. Wallerian degeneration is seen following axonal transection in the distal part of the nerve. Distal axonopathy is degeneration of the axon and myelin and is associated with "stocking-glove" distribution neuropathy. Segmental demyelination is characterized by breakdown of myelin with an intact axon
and is associated with lead poisoning and hereditary sensory motor neuropathy.
RECOMMENDED READINGS
Akermark C, Crone H, Saartok T, Zuber Z. Plantar versus dorsal incision in the treatment of primary intermetatarsal Morton's neuroma. Foot Ankle Int. 2008 Feb;29(2):136-41. doi: 10.3113/FAI.2008.0136. PubMed PMID: 18315967.View Abstract at PubMed
Ha'Eri GB, Fornasier VL, Schatzker J. Morton's neuroma--pathogenesis and ultrastructure. Clin Orthop Relat Res. 1979 Jun;(141):256-9. PubMed PMID: 477115. View Abstract at PubMed
Graham CE, Graham DM. Morton's neuroma: a microscopic evaluation. Foot Ankle. 1984 Nov-Dec;5(3):150-3. PubMed PMID: 6519606. View Abstract at PubMed
Question 69
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 70
Which of the following muscles has dual innervation?
Explanation
REFERENCE: Mahakkanukrauh P, Somsarp V: Dual innervation of the brachialis muscle.
Clin Anat 2002;15:206-209.
Question 71
In the absence of developmental dysplasia of the hip, what is the most common cause of osteoarthritis? Review Topic
Explanation
Question 72
A 40-year-old male who sustained an open pilon fracture 2 weeks ago is scheduled for a below-the-knee amputation (BKA). What laboratory value is the best predictor for wound healing?

Explanation
Question 73
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
REFERENCE: St Pierre P, Olson EJ, Elliott JJ, et al: Tendon healing to cortical bone compared with healing to a cancellous trough. J Bone Joint Surg Am 1995;77:1858-1866.
Question 74
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
Explanation
REFERENCES: Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Lowell TD, Errico TJ, Eskenazi MS: Use of steroids after discectomy may predispose to infection. Spine 2000;25:516-519.
Question 75
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 76
Figure 76 is the MR image of a 16-year-old high school football player who sustained a traumatic dominant shoulder dislocation during a game. On-field reduction was unsuccessful. The shoulder is reduced in the emergency department, and the player and his family followup in clinic. Which factor is most associated with failure of surgical treatment in this scenario?
Explanation
The MR image reveals a Bankart lesion. Arthroscopic Bankart repair failure likelihood is increased by numerous factors. Age, number of recurrences, and bony defects are most associated with failure of arthroscopic repair. Shoulder dominance, amount of periosteal
stripping, and difficulty of reduction do not correlate with increased recurrence risk following surgery.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
A 17-year-old volleyball player has a 3-month history of gradually worsening right shoulder pain. She describes a vague sensation of her shoulder “popping out of place” and weakness associated with overhead activities. She has intermittent generalized paresthesias in her right upper extremity, and she has discontinued participation in sports as a result of her symptoms. Glenohumeral range of motion is symmetric bilaterally. Empty can test findings are negative with full strength of the supraspinatus. An active compression test is negative, and sulcus sign findings are positive. An anterior apprehension test produces pain that is unrelieved with a relocation test. A cervical spine examination is unremarkable.
Question 77
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient’s symptoms?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 78
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
REFERENCES: Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531.
Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 79
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management? Review Topic
Explanation
Question 80
Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alleviated by rest. Examination reveals soft-tissue swelling, and tenderness and warmth in the region of the talonavicular and navicular cunieform joints. Management should consist of
Explanation
REFERENCE: Lutter LD: Sports-related injuries, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992.
Question 81
A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 82
Which of the following bones is most frequently involved in stress fractures in athletes? Review Topic
Explanation
Question 83
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 84
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
Question 85
A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
Explanation
REFERENCES: Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.
Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 1995;321:168-172.
Question 86
A 25-year-old male sustains the isolated injury shown in Figure A. Antegrade intramedullary nailing is planned for definite fixation within the next 12 hours. After obtaining lateral radiographs of the injury site, what would be the next best step in management of this patient?

Explanation
Femoral neck fractures are seen less than 10% of the time with femoral shaft fractures, but they are frequently missed on initial evaluation. The neck fracture line is almost vertical and nondisplaced, or minimally displaced. Therefore fine (2-mm) cut CT scan through the femoral neck should be ordered in the preoperative workup of these patients.
Tornetta et al. reported that they reduced the delay in diagnosis of concomitant femoral neck fractures by 91% by instituting a protocol that included: dedicated AP internal rotation plain radiograph, a fine (2-mm) cut CT scan through the femoral neck, an intraoperative fluoroscopic lateral radiograph prior to fixation, as well as postoperative AP and lateral radiographs of the hip in the operating room prior to awakening the patient.
Figure A shows a trauma view lower extremity radiograph with an isolated left midshaft femur fracture.
Incorrect Answers:
setting of fracture. Answer 5: The age, injury and fracture pattern are not consistent with a pathologic femur fracture.
Question 87
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?
Explanation
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon MA, Springfield DS, et al: Chondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 88
With comparison to a below the knee amputation, each of the following are disadvantages of a through the knee amputation EXCEPT:

Explanation
The cohort study by MacKenzie et al prospectively followed 161 patients that were part of the Lower Extremity Assessment Project (LEAP). These patients underwent an above-the-ankle amputation at a trauma center within 3 months following the injury and followed for 2 years. This study revealed that through-the-knee amputations had significantly worse scores for the objective performance measures of self-selected walking speed, independence in transfers, walking, and stair-climbing. Through-the-knee amputees also had worse SIP scores than AKA and BKA patients. Physicians were also less satisfied with both the clinical and the cosmetic recovery of the patients with a through-the-knee amputation. It should be noted that patients with a BKA had a faster walking speed than those with an AKA. Despite the worse SIP scores for through-the-knee amputations, patients actually reported less pain than those with an AKA or BKA, though this wasn't statistically significant.
(SBQ06.2) A 21-year-old male presents to the emergency department after sustaining a gun shot wound to his back. Subsequent radiographs reveal a bullet in the L2 vertebral body. Physical exam shows no neurologic deficits. He undergoes emergent laparotomy and is found to have a small bowel laceration. What would be the preferred treatment following his exploratory laparotomy and small bowel repair?

Intravenous antibiotic coverage for Gram negative bacteria for 7 days

Surgical decompression and bullet fragment removal

Observation

Broad-spectrum oral antibiotic coverage for 7 days
Broad-spectrum intravenous antibiotic coverage for 7 days
DISCUSSION: The clinical presentation is consistent with a GSW with bowel perforation and a retained bullet in the vertebral body. Because the patient is neurologically intact broad-spectrum intravenous antibiotic coverage for 7 days is the most appropriate treatment.
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the small bowel, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Indications for surgery include when a neurological deficit is present that correlates with imaging findings of neurological compression by the missile, or when the missile is in contact with the CSF posing a risk for metal toxicity.
Roffi et al performed a Level 4 study of 42 patients that sustained a gunshot wound that perforated the stomach or bowel and then entered the spinal column. They found that an extended regimen of broad spectrum antibiotics combined with bedrest appeared to significantly reduce the risk of spinal or paraspinal infection, whereas early bullet removal did not significantly prevent the occurrence of infection.
Velmahoos et al performed a Level 4 study including 24 patients that sustained a gunshot wound to the spine with associated colonic injury. They found that the incidence of sepsis was 8.4% (compared to 5% in non-bowel injuries) and concluded that retainment of the bullet did not increase the rate of sepsis.
Incorrect Answers:
Question 89
Which osseous landmark indicates the proximal border of the femoral insertion of the posterior cruciate ligament?
Explanation
The posterior cruciate ligament is composed of the anterolateral and posteromedial bundles. The medial intercondylar ridge marks the proximal border of the femoral insertion. Occasionally, a medial bifurcate ridge will separate the anterolateral and posteromedial bundles, and a clear change in slope occurs between the bundles. Knowledge of these osseous landmarks may aid in anatomic reconstruction of the posterior cruciate ligament. The medial interfemoral and interfascicular ridges are not accepted nomenclature.
RECOMMENDED READINGS
Lopes OV Jr, Ferretti M, Shen W, Ekdahl M, Smolinski P, Fu FH. Topography of the femoral attachment of the posterior cruciate ligament. J Bone Joint Surg Am. 2008 Feb;90(2):249-55. doi: 10.2106/JBJS.G.00448. PubMed PMID: 18245582.
View Abstract at PubMed
Forsythe B, Harner C, Martins CA, Shen W, Lopes OV Jr, Fu FH. Topography of the femoral attachment of the posterior cruciate ligament. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:89-100. doi: 10.2106/JBJS.H.01514.
PubMed PMID: 19255202. View Abstract at PubMed
Question 90
Sudden cardiac death in the young athlete is most frequently caused by
Explanation
REFERENCES: Burke AP, Farb A, Virmani R, Goodin J, Smialek JE: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991;121:568-575.
Maron BJ, Sharani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA
1996;276:199-204.
Question 91
Internal impingement is characterized by which of the following anatomic lesions? Review Topic
Explanation
Question 92
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Explanation
Question 93
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?
Explanation
REFERENCES: Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358.
Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Manifold SG, Kelly MA, Richardson L, et al: Osteotomies about the knee, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 947-961.
Question 94
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic

Explanation
Question 95
Figure 30 shows an axial T1-weighted MRI scan of a patient’s right shoulder. The arrows are pointing to what normal structure?
Explanation
REFERENCES: Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791.
Carrino JA, Chandnanni VP, Mitchell DB, et al: Pectoralis major muscle and tendon tears: Diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 2000;29:305-313.
Ohashi K, El-Khoury GY, Albright JP, et al: MRI of complete rupture of the pectoralis major muscle. Skeletal Radiol 1996;25:625-628.
Question 96
This medication, a factor Xa inhibitor, currently is not approved for venous thromboembolism (VTE) prophylaxis.
Explanation
Warfarin has a long clinical track record and is well known among most physicians. It is a vitamin K antagonist that can be monitored with prothrombin time (INR) testing and reversed with vitamin K and fresh frozen plasma if needed. Newer oral anticoagulants are becoming more common and offer the advantage of being rapidly active without a need for monitoring. These oral anticoagulants are not reversible, which can complicate the treatment of patients who present with bleeding or require surgery. Dabigatran (Pradaxa) is a direct thrombin inhibitor that is approved for stroke prevention in atrial fibrillation. It is not reversible, and a surgical delay of 24 to 48 hours is recommended for all but emergent surgeries. A longer delay is recommended with renal insufficiency. Rivaroxaban (Xarelto) is an oral factor Xa inhibitor that is approved for atrial fibrillation and the treatment of VTE and deep vein thrombosis prophylaxis. It offers the advantage of daily dosing. It
is not reversible and a surgical delay of 36 to 48 hours is recommended. Apixaban (Eliquis) is another factor Xa inhibitor for which twice-daily dosing is required. It is currently approved for stroke prevention in atrial fibrillation, and a surgical delay of 36 to 48 hours is recommended.
RECOMMENDED READINGS
Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013 May;88(5):495-511. doi: 10.1016/j.mayocp.2013.03.006. Review. Erratum in: Mayo Clin Proc. 2013 Jul;88(7):777. PubMed PMID: 23639500. View Abstract at PubMed Alquwaizani M, Buckley L, Adams C, Fanikos J. Anticoagulants: A Review of the Pharmacology, Dosing, and Complications. Curr Emerg Hosp Med Rep. 2013 Apr 21;1(2):83-97. Print 2013 Jun. PubMed PMID: 23687625. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 100 AND 101
A 55-year-old woman slipped on ice while getting out of her car and sustained the injury shown in Figure 100.

Question 97
What structure has been described as having a risk of injury with retractor placement on the sacrum during combined acetabular-pelvic ring surgery using the Stoppa approach with a lateral window?

Explanation
Question 98
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
Explanation
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-
Question 99
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 100
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
