Orthopedic Board Review MCQs: Arthroplasty, Trauma & Elbow | Part 119

Key Takeaway
This page offers Part 119 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review quiz. Designed for orthopedic residents and surgeons, it features 100 high-yield, verified MCQs in various modes. It's an essential tool for mastering complex clinical scenarios and excelling in board certification exams.
About This Board Review Set
This is Part 119 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 119
This module focuses heavily on: Arthroplasty, Elbow, Fracture, Hip, Infection, Knee.
Sample Questions from This Set
Sample Question 1: CLINICAL SITUATIONFigures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymo...
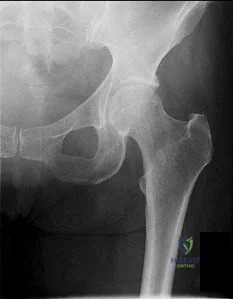
Sample Question 2: Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stagedebilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplas...
Sample Question 3: A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include...
Sample Question 4: In a patient with a major head injury and a femoral shaft fracture, intraoperative hypotension during femoral fixation has been associated with which of the following?...
Sample Question 5: A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. O...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 2
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 3
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics 2004;113:322-325.
Matava MJ, Patton CM, Luhmann S, et al: Knee pain as the initial symptom of slipped capital femoral epiphysis: An analysis of initial presentation and treatment. J Pediatr Orthop 1999;19:455-460.
Question 4
In a patient with a major head injury and a femoral shaft fracture, intraoperative hypotension during femoral fixation has been associated with which of the following?

Explanation
Question 5
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis (musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii (musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis (musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis (musculocutaneous nerve)
Question 6
A 78-year-old woman has had activity-limiting cervical pain and occipital headaches for the past 4 years. Management consisting of injections, analgesics, and part-time collar wear has provided temporary relief. Examination reveals that her neck pain seems to be primarily located immediately below the skull and is aggravated by long periods of sitting and rotation of her head. Plain radiographs are shown in Figures 36a through 36c. What is the best course of action?
Explanation
REFERENCES: Ghanayem AJ, Leventhal M, Bohlman HH: Osteoarthrosis of the atlanto-axial joints: Long-term follow-up after treatment with arthrodesis. J Bone Joint Surg Am 1996;78:1300-1307.
Star MJ, Curd JG, Thorne RP: Atlantoaxial lateral mass osteoarthritis: A frequently overlooked cause of severe occipitocervical pain. Spine 1992;17:S71-S76.
Question 7
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 8
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Explanation
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Question 9
By which mechanism can a true aneurysm of the ulnar artery result?
Explanation
Question 10
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14-year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Question 11
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What is the most likely diagnosis for the source of this patient's pain?

Explanation
Question 12
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Explanation
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Durrani AA, Crawford AH, Chouhdry SN, et al: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 13
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
REFERENCES: Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Rechtine GR II, Cahill D, Chrin AM: Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 1999;12:406-409.
Question 14
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 15
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 16
Plate fixation of olecranon fractures is recommended over tension band wire fixation when
Explanation
Question 17
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 18
Physiologic bowing of the lower extremities should spontaneously correct by what age?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 7.
Salenius P, Vankka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am
J V :
Question 19
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 20
Which of the following anatomic structures is labeled 6 in Figure 27?
Explanation
REFERENCES: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 309.
Question 21
A coach of 3 football teams—the B team, junior varsity team, and varsity team—wants to study the average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on 1 team are different from those on the other teams?
Explanation
Data collected in research studies fall into 1 of 2 categories—continuous or discrete. Continuous data can be displayed on a curve. Examples include height, weight, and time recorded in a 40-yard dash. Discrete data represent data that fall into specific categories such as gender or the presence or absence of a risk factor.
ANOVA is used to determine statistical significance in mean values of continuous data when there are more than 2 independent samples. The 2-sample t test compares mean values of continuous data between 2 independent groups. The Chi-square test and Fisher's exact tests are tests used to analyze discrete data.
RESPONSES FOR QUESTIONS 58 THROUGH 61
Paresthesias in the fourth and fifth digits
Numbness on the lateral side of the forearm
Heterotopic ossification
Posterolateral rotatory instability of the elbow
Medial antebrachial cutaneous neuroma
For each surgical case described below, match the most likely related complication listed above.
Question 22
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 23
In the treatment of thoracolumbar idiopathic scoliosis using an anterior single rod technique with interbody cages, which of the following variables has been associated with pseudoarthrosis. Review Topic
Explanation
In a prospective study, Sweet et al found anterior instrumented fusions using a single solid rod had good radiographic and clinical outcomes. In their treatment group they found common risk factors for pseudarthrosis were smoking, weight >70 kg, and T5-T12 hyperkyphosis of > 40 degrees. They recommend consideration should be given to alternate techniques in larger adolescents (>70 kg) with thoracic hyperkyphosis (>40 degrees ). The average coronal correction of thoracic curves was from 55 degrees to 29 degrees (47%). The average correction of thoracolumbar/lumbar curves was from 50 degrees to 15 degrees (70%). Neither of these variables were associated with pseudoarthrosis. In the sagittal plane, lordosis was maintained in thoracolumbar/lumbar fusions at -58 degrees (T12-sacrum). Improved maintenance of lumbar lordosis is considered one of the advantages of an anterior approach.
In an additional study from the same group at Wash U, Hurford et al designed a study to compare the results of anterior DUAL-rod instrumentation with their previous experience using single-rod constructs. They found the two technique were comparable in the amount of radiographic deformity correction obtained. However, they report the absence of any pseudarthroses in the 60 patients with dual-rod is a distinct advantage over the single rod technique.
Question 24
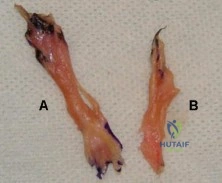
A 55-year-old man was injured when a large piece of sheet metal lacerated his medial elbow while working at a factory. He underwent primary repair of the lacerated structures shown in Figures 1 and 2 on the day of injury. In addition to this surgical treatment, what nerve transfer procedure should be considered during this primary operative intervention to improve his functional recovery?

Explanation
In adults, the repair of high ulnar nerve injuries typically yields incomplete motor recovery and disappointing functional results despite early surgical intervention and careful surgical technique. Early transfer of the terminal branch of the AIN to the deep ulnar motor fascicle can rapidly reinnervate distal targets and potentially preserve motor end plate function in the intrinsic musculature of the hand because of the proximity of the nerve transfer to the target muscle. Sensory deficits due to an ulnar nerve injury
can be restored through a transfer of median sensory fascicles to the distal ulna sensory fascicles. This procedure typically would not be considered at the time of the original surgery, because sensory recovery is more likely than motor recovery in the setting of a high ulnar nerve injury. For radial nerve injuries, wrist extension can be restored through an FDS branch of the median nerve transfer to the ECRB branch of the radial nerve. The FCU fascicle of the ulnar nerve can be transferred to the biceps branch of the musculocutaneous nerve to restore elbow flexion and supination.
Question 25
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
REFERENCES: Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears.
Am J Sports Med 2005;33:1405-1417.
Fukuda H: The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br 2003;85:3-11.
Question 26
A lO'/z-year-old boy sustained the injury shown in Figure 72 when he fell out of a tree. This is a closed, neurologically intact injury and the patient has no head injury or loss of consciousness. He weighs 115 pounds and is otherwise healthy. What is the optimal treatment option for this injury?
Explanation
REFERENCES: Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295-1301.
Figure 73a Figure 73b
Question 27
After performing a total hip arthroplasty through a posterolateral approach, an orthopaedic surgeon is unable to adequately externally rotate the leg and subsequently exposes the anterior capsule. When releasing the inferior aspect of the anterior capsule, pulsatile bleeding is encountered. A branch of which artery is most likely lacerated?
Explanation
Branches of the lateral femoral circumflex artery arise from the inferior aspect of the anterior hip capsule. They can be injured when removing the anterior capsule from any approach. The inferior gluteal artery supplies the gluteus maximus. The medial femoral circumflex artery enters the hip joint along the path of the obturator externus tendon. The femoral artery crosses the anterior hip joint in the superior-to-inferior direction and is located just medial to the hip joint.

Question 28
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 29
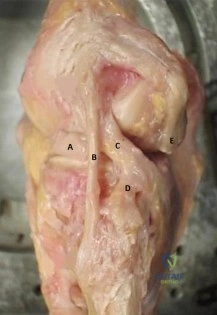
Figure A is the lateral view of a left knee cadaveric specimen that has the extensor mechanism removed. Which two structures labeled provide the most rotational stability in knee flexion? Review Topic
Explanation
extension.
The lateral knee is stabilized by 28 unique static and dynamic structures. These structures work in concert to resist varus gapping and rotational knee instability. The three primary stabilizers include the fibular or lateral collateral ligament (LCL), the popliteus tendon (PT) and the popliteofibular ligament (PFL). Injury to these ligaments results in increased forces seen on ACL and PCL ligament reconstruction grafts with combined posterolateral corner (PLC) injuries, which can result in graft failure if the PLC is not reconstructed as well.
James et al reviewed the anatomy and biomechanics of the lateral knee stabilizers, detailing the specific functional contributions of the individual structures. The LCL is the primary restraint to varus instability, the highest forces occurring at knee extension (0°-30°). The PT and PFL serve as restraints to rotational instability, the highest forces occurring at knee flexion (60°-90°).
LaPrade et al reviewed the anatomy and biomechanics of the medial knee stabilizers. The three key static stabilizers are the superficial medial collateral ligament (sMCL), the deep medial collateral ligament (dMCL), and the posterior oblique ligament (POL). The sMCL is the primary restraint to valgus instability (proximal sMCL) and secondary restraint to rotational instability (distal sMCL) at all knee flexion angles. The dMCL is a secondary restraint to valgus and rotational instability. The POL is the primary restraint to rotational instability.
Figure A depicts the lateral knee structures in a cadaver specimen (A = lateral meniscus, B = LCL, C = PT, D = PFL, E = lateral head of gastrocnemius). Illustration A is a labeled picture of the lateral knee structures. Illustration B is a table from James et al demonstrating the change in forces experienced by the different lateral stabilizers at varying degrees of knee flexion. You see the LCL resists rotation at 0°-30° (extension) while the PT and PFL resist rotation at 60°-90° (flexion).
Incorrect Responses:
Question 30
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 31
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
REFERENCES: Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Katzner M, Schvingt E: Operative treatment of bone metastases secondary to renal carcinoma: Basic research and treatment of renal cell carcinoma metastasis. Prog Clin Biol Res EORTC 1990;348:151-168.
Question 32
- A skeletal survey is more accurate than a bone scan for detecting skeletal involvement in which of the following neoplastic diseases?
Explanation
Question 33
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data?
Explanation
REFERENCES: Jones SC, Fernau R, Woeltjen BL: Use of somatosensory evoked potentials to detect peripheral ischemia and potential injury resulting from positioning of the surgical patient: Case reports and discussion. Spine J 2004;4:360-362.
Schwartz DM, Sestokas AK, Hilibrand AS, et al: Neurophysiological identification of position-induced neurologic injury during anterior cervical spine surgery. J Clin Monit Comput 2006;20:437-444.
Question 34
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 35
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 36
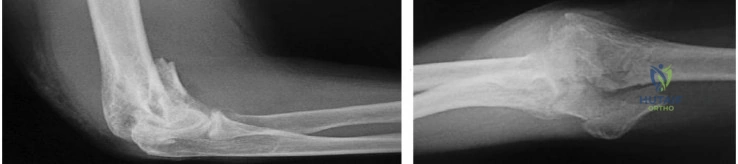
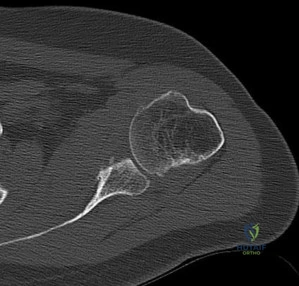
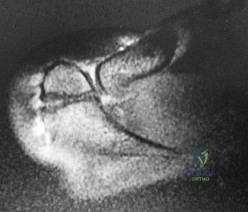
Figures 34a through 34c show the radiographs of a 51-year-old woman who injured her elbow in a fall from standing height. Examination reveals that elbow range of motion is limited by pain only. Management should consist of
Explanation
function and minimize stiffness. A long arm cast for any length of time will result in severe elbow stiffness.
REFERENCES: Morrey BF: Radial head fracture, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 341-364.
Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 37
..Figures 83a and 83b are the radiographs of a 53-year-old otherwise healthy homemaker who had a syncopal episode and sustained a ground-level fall and injury to her right elbow. She presently admits to right elbow pain, swelling, and an inability to bend her elbow. What is the best initial treatment for this injury?
Explanation
Figure 84 is the glenoid CT scan of a 20-year-old man who dislocated his shoulder anteriorly while playing football. He had persistent instability 2 months after the injury, but he did not have a sulcus sign or posterior instability. He underwent an arthroscopic Bankart repair with 4 bioabsorbable anchors with simple sutures through the labrum and capsule.
He did not have an engaging Hill-Sachs lesion, the rotator cuff was unremarkable, and the capsule was not torn from the humerus. After surgery, he did well for 6 months until he jumped into a lake and again dislocated his shoulder anteriorly. He says his shoulder no longer felt stable after his reduction.
Question 38
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?
Explanation
REFERENCES: Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Question 39
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 40
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
REFERENCES: Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 41
A 9-year-old boy has pain over the midfoot medially with activity. Based on the findings shown in Figures 26a and 26b, which of the following is considered the most effective short-term management?
Explanation
REFERENCES: Borges JL, Guile JT, Bowen JR: Köhler’s bone disease of the tarsal navicular.
J Pediatr Orthop 1995;15:596-598.
Williams GA, Cowell HR: Köhler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 42
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
REFERENCE: Bukata SV, Gelinas J, Wei X, et al: PGE2 and IL-6 production by fibroblasts in response to titanium wear debris particles is mediated through a Cox-2 dependent pathway. J Orthop Res 2004;22:6-12.
Question 43
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
Question 44
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Thometz J: Tarsal coalition. Foot Ankle Clin 2000;5:103-118.
Question 45
Which of the following best characterizes the antigenicity of allograft bone?
Explanation
REFERENCES: Crawford MJ, Swenson CL, Arnoczky SP, et al: Lyophilization does not inactivate infectious retrovirus in systemically infected bone and tendon allografts. Am J Sports Med 2004;32:580-586.
Stevenson S, Li XQ, Davy DT, et al: Critical biological determinants of incorporation of non-vascularized cortical bone grafts: Quantification of a complex process and structure. J Bone Joint Surg Am 1997;79:1-16.
Simon SR (eds): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 277-320.
Question 46
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder “slipped out” and “went back in.” The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?
Explanation
REFERENCES: Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 47
A 5-year-old boy complains of atraumatic foot pain that is aggravated by weight-bearing and an antalgic limp for a few days. He is splinted for 2 weeks by his pediatrician and referred to your office. Examination is unremarkable. Radiographs are shown in Figures A through C. What is the next best step? Review Topic

Explanation
Idiopathic avascular necrosis (AVN) of the navicular arises because the intraosseous blood flow of the navicular is centripetal, leaving a central watershed area. The primary blood supply is via perforating branches of the dorsalis pedis. Patients present with midfoot pain between 2-9 years of age. Navicular sclerosis, fragmentation, and flattening are noted radiographically.
Digiovanni et al. reviewed AVN in the foot. Nonsurgical management is routine. Cast immobilization will provide earlier resolution of symptoms. Weight-bearing will not affect outcome. The navicular will regain a normal appearance over time.
Aiyer and Hennrikus reviewed pediatric foot pain. That state that up to 25% of Kohler's disease is bilateral. They agree that casting for 4-6weeks will mitigate symptoms and increase the rate of symptom resolution.
Figures A through C are AP, oblique and lateral foot radiographs showing navicular flattening and sclerosis consistent with Kohler's disease.
Incorrect Answers:
(SBQ13PE.29) A 10-year-old girl presents to your office accompanied by her mother to discuss cosmetic concerns regarding her feet pictured in Figure A. They recently migrated to the U.S. and this is the first medical evaluation for this complaint. The father's feet apparently look similar. The remainder of the patient's physical
examination is normal. The parents should be counseled that children with this condition have: Review Topic

Delayed motor milestones, and cardiac and renal work up are necessary
Normal motor milestones, but cardiac and renal work up are necessary
Delayed motor milestones, but no further work up is necessary
Normal motor milestones, and no further work up is necessary
No chance of passing on this trait to children, as it results from a spontaneous genetic mutation
This patient has post-axial polydactyly of the feet. Children with this condition exhibit normal motor milestones. If the remainder of the physical examination is normal, no further work up is necessary.
Post-axial polydactyly is a common autosomal dominant trait. As such, there is usually a family history. In the absence of other physical exam abnormalities, this condition is not associated with systemic disorders. Normal motor development can be expected, though surgical treatment may be undertaken to facilitate cosmesis or shoe-wear.
Phelps et al. reviewed supernumerary digits in 61 patients at an average of 15 year follow up. They found 94% good to excellent results. Poor results were associated with pre-axial duplications and persistent hallux varus.
Figure A is a clinical photo showing bilateral post-axial polydactyly of the foot. Incorrect answers:
cardiac or renal conditions without any manifestations. Answer 5. This is an autosomal dominant condition.
Question 48
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.
Question 49
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include

Explanation
Rotator cuff and scapular stabilizer strengthening exercises
Diagnostic and therapeutic corticosteroid injection
Arthroscopic debridement
Completion of rotator cuff tear, repair, and biceps tenotomy
Acromioplasty
Repair of rotator cuff and superior labrum anterior to posterior (SLAP) repair
Repair of subscapularis tendon and biceps tenodesis
Question 50
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 51
Figures below demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is

Explanation
Question 52
Which of the following activities can improve posterior capsular contractures?
Explanation
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 53
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.
Question 54
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 55
A 55-year-old male returns for followup 3 months after reverse shoulder arthroplasty. He reports limited function of his right shoulder but no antecedent trauma. A radiograph of his shoulder is shown in Figure A. All of the following variables are associated with this complication EXCEPT: Review Topic
Explanation
RSA dislocation is a known complication of RSA. Risks include proximal humeral bone loss, chronic fracture sequelae with malunited/ununited tuberosities, failed previous arthroplasty, and fixed glenohumeral dislocation preoperatively. An irreparable subscapularis tears may be less of an issue with newer implant designs.
Trappey et al. studied instability and infection rates after RSA. They found that the rate of instability was similar in primary and revision surgery, but the rate of infection was higher in revision surgery. Instability was highest in the fracture sequelae group because of malunited tuberosities, contractures and proximal humeral bone loss.
Favre et al. examined the effect of component positioning on RSA stability. They found that humeral version was more important than glenoid version. Stability is improved with the humerus in neutral or slight anterversion. They recommend avoiding retroversion >10deg.
Edwards et al. examined subscapularis insufficiency and the risk of RSA dislocation. They found that of 138 RSA, all 7 dislocations occurred in patients with an irreparable subscapularis. Dislocation was also more likely in patients with complex diagnoses, including proximal humeral nonunion, fixed dislocation, and failed prior arthroplasty.
Figure A shows reverse shoulder arthroplasty dislocation. Incorrect Answers:
Question 56
A 56-year-old laborer sustained a subcoracoid dislocation of the shoulder as a result of falling off a scaffold 3 weeks ago. He now is unable to actively raise his arm and has constant pain. What is the most likely diagnosis?
Explanation
Question 57
Figure 93 shows the axial T2-weighted MRI scan of the lumbar spine of a 70-year-old man. The arrow points to which of the following structures? Review Topic
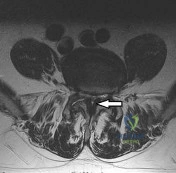
Explanation
(SBQ12SP.14) A 36-year-old male presents with acute onset of right buttock and leg pain following lifting a heavy object. On physical exam he has weakness to knee extension, numbness over the medial malleolus, and a decreased patellar reflex. Which of the following would most likely explain this clinical presentation. Review Topic
Lumbar arachnoiditis
L4/L5 paracentral disc herniation
L3/L4 far lateral (foraminal) disc herniation
L4/L5 far lateral (foraminal) disc herniation
L5/S1 far lateral (foraminal) disc herniation
The clinical presentation is consistent with a L4 radiculopathy. A L4/L5 far lateral (foraminal) disc herniation would compress the exiting root (L4) and cause these symptoms.
The location of a prolapsed lumbar disc determines its symptoms. Central disc herniations may give rise to back pain or cauda equina syndrome. Paracentral disc herniations (90-95% of cases) affect the traversing nerve root. Far lateral disc herniations (5-10%) affect the exiting nerve root.
Gregory et al. summarize physical signs in lumbar disc herniation. They state that the straight-leg-raise is the most sensitive (73-98% sensitive) test and the crossed straight-leg-raise is the most specific (88-98% specific) test for lumbar disc herniation. Other specific tests include weak ankle dorsiflexion (89% specific), absent ankle reflex (89% specific), and calf wasting (94% specific, but a late finding).
Illustration A shows how a paracentral L4/L5 disc herniation affects the traversing L5 root, but a far lateral L4/L5 disc herniation affects the L4 root. Illustration B shows the dermatomal distribution of pain with root involvement from L3 to S1.
Incorrect Answers:
Question 58
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true? Review Topic
Explanation
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle.
Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion
>30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect
Question 59
Which of the following conditions is associated with palmoplantar pustulosis?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.
Question 60
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity include a

Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
View Abstract at PubMed
Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 61
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 62
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
REFERENCES: Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 233-245.
Question 63
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
REFERENCES: Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
Mann RA, Mann JA: Keratotic disorders of the plantar skin. Instr Course Lect 2004;53:287-302.
Question 64
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of
Explanation
REFERENCES: An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-143.
Question 65
Figure 45 shows the current radiograph of an 11-year-old girl who sustained a simple nondisplaced fracture of the distal radius 4 weeks ago. Management at the time of injury consisted of application of a short arm cast but no manipulation. What is the major concern at this time?
Explanation
REFERENCES: Peterson HA: Physeal fractures: Part 2. Two previously unclassified types. J Pediatr Orthop 1994;14:431-438.
Peterson HA: Physeal and apophyseal injuries, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 108-109.
Question 66
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
Question 67
A 7-year-old boy presents to the ED with visible right elbow deformity after a fall on the playground. His injury films are shown in figures A and B. The injury is closed, and there is a palpable radial pulse with a well-perfused hand. He undergoes multiple attempts at closed reduction and percutaneous pinning with 3 lateral pins in the operating room. Final radiographs show some gapping at the fracture site. At the end of the case, the radial pulse is no longer palpable and the hand appears pale. What is the next best step in management? Review Topic

Explanation
The management of supracondylar humerus fractures is dictated significantly by the neurovascular examination. Loss of pulse and a pale, cool hand warrants emergent closed reduction and percutaneous pinning. If the vascular status does not change, open exploration is warranted. When a hand becomes pulseless and cool after reduction, it is typically due to the brachial artery being interposed in the fracture site. Undoing the reduction can often help. If there is still evidence of vascular compromise, open exploration is warranted. A pale (poorly perfused) hand or any change in neurovascular status requires urgent intervention. A pink, pulseless but well perfused hand can be observed.
Carter et al. surveyed over 300 pediatric orthopaedic surgeons on the management of type III supracondylar humerus fractures. They found an increasing trend toward lateral pin configuration and non-emergent delayed treatment.
Abzug et al. reviewed current concepts regarding management of supracondylar humerus fractures. They report an increased trend in surgical management of type II supracondylar humerus fractures. For the pink pulseless hand, they recommend admission for observation and splinting in 45 degrees of flexion.
Babal et al. reviewed nerve injuries in pediatric supracondylar humerus fractures. Anterior interosseous nerve palsy ranks highest, with ulnar nerve palsy highest with flexion type injuries. Medial pinning leads to risk of iatrogenic ulnar nerve injury.
Figures A and B are AP and lateral elbow radiographs showing a Gartland type III supracondylar humerus fracture.
Incorrect Answers:
Question 68
During the revision surgical procedure, thoracic pedicle screws are placed. Following placement, triggered electromyography (EMG) is performed by stimulating the pedicle screw heads. During testing the right T2 pedicle screw head returns a threshold of 2 mA. What does this reading indicate?
Explanation
This patient has developed a proximal junctional kyphosis following a long posterior fusion performed for treatment of degenerative lumbar scoliosis. Risk factors for proximal junctional kyphosis in the setting of instrumented fusions performed for degenerative scoliosis include advanced age, 360-
degree fusions, extension of fusion constructs to the sacrum, and upper instrumented vertebrae at the level of T1-3. The patient's junctional kyphosis is attributable to failure of the disk and ligamentous structures at T2-3 and would be graded as type I using the classification system of Yagi and associates. Most symptomatic proximal junctional kyphoses are treated with posterior extension of the fusion construct to a more proximal level spanning the kyphosed region. The use of orthoses or simple removal of instrumentation is unlikely to substantively impact symptoms or address the proximal kyphosis. Diabetes and obesity are known factors that increase risk for postsurgical infection following a spine fusion procedure. The most frequent complication following revision surgery for proximal junctional kyphosis, however, is the need for further surgery. In the study by Yagi and associates, 48% of patients who underwent revision surgery for proximal kyphosis developed further adjacent segment degeneration. In the proximal thoracic spine, where the pedicle may be narrow, triggered EMG testing of inserted pedicle screws may be used to assess for violation of the pedicle wall during insertion. In the setting of triggered EMG, thresholds exceeding 10 mA indicate a well-placed pedicle screw. Thresholds lower than 4 mA to 6 mA indicate that a screw is directly contacting a neural structure. Thresholds between 9 mA and 10 mA suggest that a breach of the pedicle may be present, but the screw is not contacting a neural structure.
RECOMMENDED READINGS
Yagi M, Rahm M, Gaines R, Maziad A, Ross T, Kim HJ, Kebaish K, Boachie-Adjei O; Complex Spine Study Group. Characterization and surgical outcomes of proximal junctional failure in surgically treated patients with adult spinal deformity.Spine (Phila Pa 1976). 2014 May 1;39(10):E607-14. doi: 10.1097/BRS.0000000000000266. PubMed PMID: 24525992. View
Abstract at PubMed
Cammarata M, Aubin CÉ, Wang X, Mac-Thiong JM. Biomechanical risk factors for proximal junctional kyphosis: a detailed numerical analysis of surgical instrumentation variables. Spine (Phila Pa 1976). 2014 Apr 15;39(8):E500-7. doi: 10.1097/BRS.0000000000000222. PubMed
PMID: 24480964. View Abstract at PubMed
Kim HJ, Lenke LG, Shaffrey CI, Van Alstyne EM, Skelly AC. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine (Phila Pa 1976). 2012 Oct 15;37(22 Suppl):S144-64. doi: 10.1097/BRS.0b013e31826d611b. PubMed PMID: 22885829. View Abstract at PubMed Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 69
When planning a research study, the power of the study may be increased by
Explanation
Question 70
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
intermediate-term follow-up.
Question 71
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient? Review Topic
Explanation
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
Question 72
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 73
A 74-year-old man underwent a hemiarthroplasty with acromioplasty for rotator cuff tear arthropathy 2 years ago. Despite continued therapy, he is still unable to elevate his arm beyond 40 degrees. Attempted elevation is painful and demonstrates bulging in the anterosuperior aspect of his shoulder. Radiographs show a well-positioned hemiarthroplasty without signs of loosening. What is the most appropriate treatment for this patient? Review Topic
Explanation
Question 74
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
Question 75
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
REFERENCE: Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 76
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 77
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist’s office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
Explanation
Question 78
A 6-year-old girl has never been able to crawl or walk and can sit only when propped. History reveals no complications during pregnancy or delivery. Examination reveals a 30-degree scoliosis from T4 to L3. Deep tendon reflexes are absent, but fasciculations are present. The most likely genetic defect is the result of an abnormality in
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
Thompson GH, Berenson FR: Other neuromuscular disorders, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 633-676.
Question 79
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of
Explanation
REFERENCES: Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Muldoon MP, Cofield RH: Complications of humeral head replacement for proximal humeral fractures. Instr Course Lect 1997;46:15-24.
Question 80
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic

Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 81
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
REFERENCES: Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 82
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of
Explanation
REFERENCES: Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 323-337.
Question 83
A skeletally mature GMFCS V child with spastic quadriplegic cerebral palsy presents with progressive scoliosis and inability to sit upright in a wheelchair. Radiographs are shown in Figures A and B, depicting a long C-shaped 75 degree curve with pelvic obliquity. Which is the most appropriate treatment option? Review Topic

Explanation
Scoliosis in CP differs from adolescent idiopathic scoliosis. Curves can be classified into double curves (thoracic and lumbar) with minimal pelvic obliquity (Weinstein Group I) and large curves (lumbar/thoracolumbar) with marked pelvic obliquity (Group II). In the presence of pelvic obliquity (>15°), caudal instrumentation should end at the pelvis to reduce the risk of pseudoarthrosis and late loss of correction. Cephalad instrumentation should end high in the thoracic spine (T2) to decrease proximal junctional kyphosis.
Imrie et al. reviewed the management of spinal deformity in CP. They advocate posterior-only pedicle screw fusion for curves <100° that bend down to 50% on traction films, from T2-3 to the pelvis, using iliac screws. They advocate single-stage anterior release and posterior fusion for curves >120° with poor flexibility, or associated severe pelvic obliquity or sagittal deformity.
McCarthy et al. reviewed scoliosis in CP. They advocate proximal fixation to the upper thoracic spine (T1-2), and distal fixation to L4-5 (pelvic obliquity <15°) or to the pelvis (pelvic obliquity >15°). They add anterior release for larger, rigid curves that do not bend out to <60°, and in skeletally immature children.
Figures A and B are PA and lateral scoliosis radiographs demonstrating 75° of thoracolumbar scoliosis and severe pelvic obliquity, and progressive lumbar hyperlordosis. Illustrations A and B are PA and lateral scoliosis radiographs demonstrating correction of curve and pelvic obliquity using the Galveston Technique with segmental fixation utilizing sublaminar wires.
Incorrect Answers:
(SBQ12SP.26) Figure A is a lateral cervical spine radiograph of a 70-year-old female who presents with two months of posterior midline neck pain that is worse with motion. She has no history of trauma. She denies any symptoms of arm pain, gait instability, or dexterity problems with her hands. Physical exam of the lower extremities shows 2+ patellar reflexes and flexion of the great toe with a Babinski test. What should the patient be told regarding these radiographic findings? Review Topic

She requires surgical decompression to prevent progressive neurologic deterioration
85% of individuals over the age of 60 years of age demonstrate these findings
She is indicated for MRI to rule out cervical radiculopathy
She would benefit from modalities such as heat, cold, and transcutaneous electrical stimulation
She has <10% chance of having symptomatic improvement with non-operative treatment
The patient has symptomatic cervical spondylosis. She should be told that 85% of asymptomatic individuals over the age of 60 demonstrate these radiographic findings.
Cervical spondylosis is defined as age-related degenerative changes within the cervical spinal column. It can present as axial neck pain, cervical radiculopathy, cervical myelopathy, or as a combination of each. Radiographs demonstrate loss of disc height, arthrosis of the facet and uncovertebral joints, and endplate sclerosis. Imaging such as cervical spine radiographs and MRI should be interpreted carefully and correlated with clinical symptoms, as radiographic evidence of spondylosis is frequently seen in asymptomatic patients.
Boden et. al. reviewed the cervical MRI of 63 asymptomatic volunteers with no history of cervical spine symptoms. Of those, 19% were interpreted as having an abnormality. These findings included herniated nucleus pulposus, bulging disc, and foraminal stenosis. 60% of patients over 40 years demonstrated disc degeneration or narrowing at one level.
Rao et al. reviewed the presentation, pathogenesis, and management of cervical spondylosis. In this review, they report that 85% of patients older than 60 years demonstrate cervical spondylosis on radiography.
Figure A is a lateral cervical spine radiograph demonstrating spondylosis at multiple levels. There is disc height loss, facet sclerosis, and anterior osteophyte formation.
Incorrect Answers:
Question 84
What molecules have been shown to promote fibrosis during muscle injury?
Explanation
Question 85
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
REFERENCES: DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.
Question 86
What clinical scenario is most consistent with the MR image of the L4-L5 disk level shown in Figure 14? Review Topic
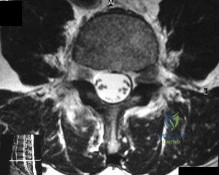
Explanation
Question 87
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 88
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?
Explanation
REFERENCES: Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001.
Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 89
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Explanation
REFERENCES: Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC: Charnley total hip arthroplasty with cement: Minimum twenty-five year follow-up. J Bone Joint Surg Am 2000;82:487-497.
Isaac GH, Wroblewski BM, Atkinson JR, Dowson D: A tribological study of retrieved hip prostheses. Clin Orthop 1992;276:115-125.
Question 90
Figure 48 shows the radiograph of a 17-year-old boy who sustained a gunshot wound to his forearm. There is a small entrance wound on the volar surface. The exit wound is dorsal and more than 15 cm in size, with loss of skin and an extensive amount of devitalized muscle hanging out of the wound. Vascular supply to the hand is excellent, the ulnar and median nerves are intact in the hand, but the radial sensory nerve function is absent. After repeated surgical debridements of the wound and bone, definitive treatment for the fracture would most likely be which of the following? Review Topic

Explanation
Question 91
No fractures were identified and the patient was treated nonsurgically in a range-of-motion brace. Two months later, he continued to experience elbow pain and was unable to return to sports. He regained motion and strength with physical therapy, there was no gross instability with varus or valgus testing, and he had a negative moving-valgus stress test. The orthopaedic surgeon performed an examination under anesthesia in the operating room (Video 54). Which anatomic structure is injured?
Explanation
Ninety percent of elbow dislocations occur in a posterolateral direction. O’Driscoll and associates described the mechanism of injury in posterolateral elbow dislocations in 1992, reporting that they occur most typically after a fall onto an outstretched arm. As the arm hits the ground it causes axial compression, forearm supination, and valgus load across the elbow. The triceps fires, pulling the olecranon posterior; the forearm supinates while simultaneous shoulder internal rotators fire; and the elbow falls into valgus. These 3 mechanisms cause the elbow to subluxate and dislocate posterolaterally. The elbow is most stable following posterolateral dislocation in a flexed and pronated position. The elbow is least stable in extension and supination. Simple dislocation often can be treated nonsurgically, while fracture dislocation will usually necessitate surgical intervention. The video shows the elbow pivot-shift test, which evaluates for posterolateral rotatory instability. A positive test finding elicits apprehension and, in this case, radial head subluxation and confirms an insufficient lateral UCL.
Question 92
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999,
pp 1422-1464.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Chandler JT, Bonar SK, Anderson RB, Davis WH: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
Question 93
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries
of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703.
Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Hasler CC, von Laer L: Prevention of growth disturbances after fractures of the lateral humeral condyle in children. J Pediatr Orthop B 2001;10:123-130.
Question 94
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns’s kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
REFERENCES: Lowe TG: Scheuermann’s disease. Orthop Clin North Am 1999;30:475-487.
Lenke LG: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patients: Prevention and treatment of surgical complications. Instr Course Lect 2004;53:501-510.
Question 95
The radiographic finding in Figure 58 is indicative of what type of acetabular fracture?

Explanation
(SBQ12TR.58) A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries? Review Topic

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Question 96
- Demyelination diseases as multiple sclerosis and Guillain-Barre $ create neurologic symptoms by
Explanation
Question 97
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 98
A 67-year-old female presents with shoulder pain for 3 months after falling down stairs. Imaging demonstrates a large rotator cuff tear involving multiple tendons. You perform an arthroscopic rotator cuff repair and biceps tenodesis. At her 2 month follow up, she reports worsening shoulder pain and decreased range of motion. Examination reveals active forward flexion to 80°. Passive range of motion is full. There is a positive external rotation lag sign. An MRI is performed and is pictured in Figure A. Which is the best treatment for this patient? Review Topic
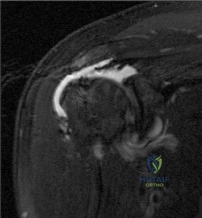
Explanation
Failed rotator cuff repair is multifactorial. Structural failure of repair is the result of both intrinsic and extrinsic factors. Intrinsic factors include advancing patient age, increasing tear size, poor tendon and muscle quality, systemic disease and smoking history. Extrinsic factors include inadequate biomechanical construct or repair configuration and overaggressive postoperative rehabilitation.
Denard et al authored a review article on revision rotator cuff repair. Indications for revision repair are persistent symptoms despite nonoperative management in whom infection and advanced degenerative changes have been ruled out. Satisfactory results have been reported following revision repair of recurrent rotator cuff tears, particularly with arthroscopic techniques. Female sex and preoperative forward flexion < 135° is associated with poorer outcomes.
Lambers Heerspink et al found that increasing age, larger tear size and additional biceps or acromioclavicular (AC) joint procedures have a negative influence on cuff integrity at follow up. Smoking, duration of symptoms, obesity and medical comorbidities were not found to influence cuff integrity in this study. Only AC procedures and workers’ compensation status were associated with worse functional outcomes.
Figure A is a coronal T2 MRI demonstrating a failed rotator cuff repair with retear. Incorrect Responses:
Question 99
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
McCarty EC, Tsairis P, Warren RF: Brachial neuritis. Clin Orthop Relat Res 1999;368:37-43.
Question 100
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
