Orthopedic Board Review MCQs: Shoulder, Trauma & Spine | Part 117
Key Takeaway
This page offers Part 117 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. It features 100 high-yield MCQs on dislocation, shoulder, and trauma, meticulously verified and formatted for exam prep. Designed for orthopedic residents and surgeons, this interactive quiz facilitates effective study and exam mode practice for certification.
About This Board Review Set
This is Part 117 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 117
This module focuses heavily on: Dislocation, Shoulder, Trauma.
Sample Questions from This Set
Sample Question 1: What is the most likely complication after surgical treatment in this scenario?...
Sample Question 2: What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?...
Sample Question 3: A 20-year-old girl reports a shoulder dislocation while reaching for a high shelf. Her history reveals multiple past dislocations with spontaneous reduction and no obvious traumatic event at onset. A photograph of her hand is shown in figur...
Sample Question 4: A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan ...
Sample Question 5: What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
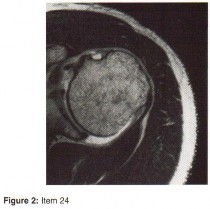
Question 1
What is the most likely complication after surgical treatment in this scenario?
Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, and internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through as seen in this patient.
The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The 4 muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the 4 rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation.
This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Brighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion, a posterior opening-wedge osteotomy is appropriate.
The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability and degenerative joint disease.
Question 2
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
REFERENCES: Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67.
Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Kwong LM, Jasty M, Harris WH: High failure rate of bulk femoral head allografts in total hip acetabular reconstructions at 10 years. J Arthroplasty 1993;8:341-346.
Question 3
A 20-year-old girl reports a shoulder dislocation while reaching for a high shelf. Her history reveals multiple past dislocations with spontaneous reduction and no obvious traumatic event at onset. A photograph of her hand is shown in figure
Explanation
The first line of treatment for shoulder dislocations in patients with MDI should consist of physical therapy aimed at strengthening the rotator cuff and scapular stabilizers. For those who fail to respond to 3 to 6 months of nonsurgical treatment, surgical intervention can be considered with inferior capsular shift being the procedure of choice for multidirectional instability. Good results have been achieved with surgical procedures for posterior and multidirectional instability, but results have been less predictable than those achieved with procedures for traumatic anterior instability.
Ide et al. evaluated the results of an 8-week rehabilitation program with shoulder-strengthening exercises and a novel scapular-stabilizing shoulder orthosis in 46 patients with MDI. There was a significant increase in mean total scores on the modified Rowe grading system and mean torque of internal and external rotation with a normalization of mean external/internal torque ratios at the completion of the program. The authors concluded that shoulder strengthening exercises represent a
useful treatment option for patients with MDI.
Levine et al. reviewed treatments of multidirectional shoulder instability in athletes. Nonoperative management remains the initial treatment of choice. Open capsular shifts remain the operative treatment of choice, however, arthroscopic electrothermal capsulorrhaphy has become increasingly used as an alternative to an open approach.
Beasley et al. reviewed multidirectional instability in the shoulder of female athletes. The authors note that women tend to have greater ligamentous laxity than men and female athletes have a greater risk of converting laxity to symptomatic instability.
Figure A demonstrates metacarpophalangeal hyperextension, which is a sign of generalized ligamentous laxity.
Incorrect Answers:
Question 4
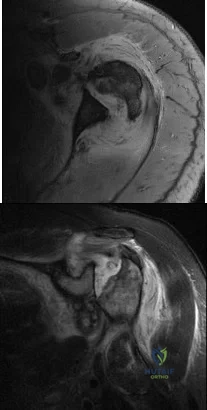
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
Question 5
What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic
Explanation
Question 6
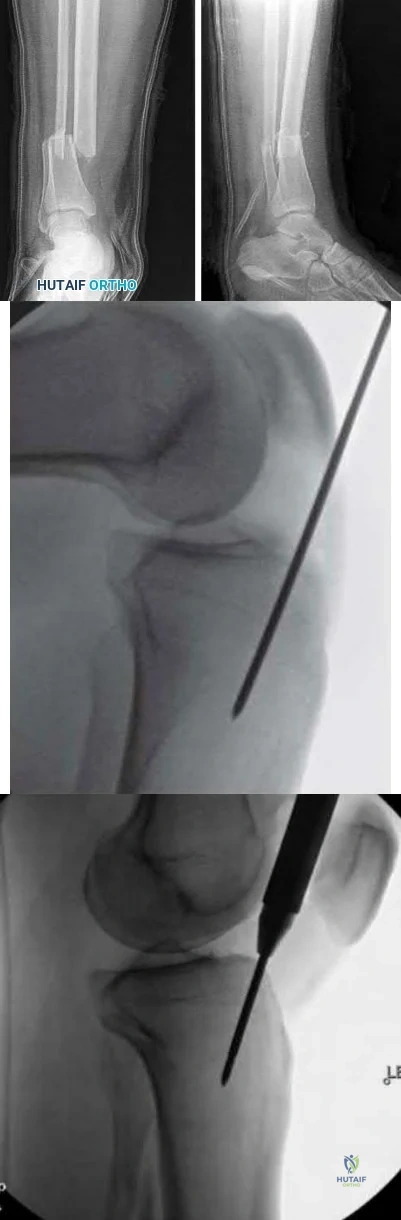
Figure 109 is the radiograph of an 11-year-old boy who felt a snap in his right hip while jumping hurdles during track practice yesterday. He complains of pain to his right groin region and is walking with a limp. What physical examination test will cause the patient to experience the most discomfort?

Explanation
Question 7
For a patient with a type II odontoid fracture, which of the following factors best predicts the development of a nonunion with nonsurgical management? Review Topic
Explanation
Question 8
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.
Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.
Question 9
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
REFERENCES: Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880.
Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
Hadjipavlou AG, Mader JT, Necessary JT, et al: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000;25:1668-1679.
Question 10
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 11
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Explanation
REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 12
In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
Explanation
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 13
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
Explanation
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
Question 14
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Howard FM: Fracture of the basal joint of the thumb. Clin Orthop 1987;220:46-51.
Question 15
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14-year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Question 16
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient’s ability to heal the wound postoperatively?
Explanation
A transcutaneous oxygen level should be greater than 40 mm Hg for healing.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Pinzur MS, Stuck R, Sage R: Benchmark analysis on diabetics at high risk for lower extremity amputation. Foot Ankle Int 1996;17:695-700.
Question 17
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation? Review Topic

Explanation
Question 18
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 19
What is the most common malignant tumor of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.
Bos GD, Ester RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 20
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis? Review Topic

Explanation
Question 21
A 40-year-old man underwent an ankle arthroscopy 6 months ago for a talus osteochondral defect. He continues to have pain and burning on the lateral portal but states that the pain is now more superficial than his original pain. Examination reveals that he has shooting pain to his medial foot and ankle when his lateral portal is tapped. A previous injection around the lateral portal gave him relief for about 2 weeks. What treatment will best eliminate his pain?
Explanation
REFERENCES: Jobe MT, Wright PE: Peripheral nerve injuries, in Canale ST (ed): Campbell’s Operative Orthopaedics. St Louis, MO, Mosby, 1998, pp 3839-3844.
Saito A, Kikuchi S: Anatomic relations between ankle arthroscopic portal sites and the superficial peroneal and saphenous nerves. Foot Ankle Int 1998;19:748-752.
Question 22
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 23
Figures 63a and 63b show the radiographs of a 38-year-old man who reports low back and bilateral lower extremity pain. The spondylolisthesis is best classified as which of the following? Review Topic

Explanation
Question 24
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 25
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 26
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 27
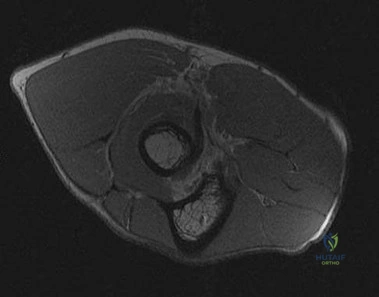
Rupture of the structure shown in the axial cross and the sagittal sections in Figures 100a and 100b causes weakness in

Explanation
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. View Abstract at PubMed
Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. View Abstract at PubMed
Question 28
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 29
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Explanation
Question 30
A skeletally mature GMFCS V child with spastic quadriplegic cerebral palsy presents with progressive scoliosis and inability to sit upright in a wheelchair. Radiographs are shown in Figures A and B, depicting a long C-shaped 75 degree curve with pelvic obliquity. Which is the most appropriate treatment option? Review Topic

Explanation
Scoliosis in CP differs from adolescent idiopathic scoliosis. Curves can be classified into double curves (thoracic and lumbar) with minimal pelvic obliquity (Weinstein Group I) and large curves (lumbar/thoracolumbar) with marked pelvic obliquity (Group II). In the presence of pelvic obliquity (>15°), caudal instrumentation should end at the pelvis to reduce the risk of pseudoarthrosis and late loss of correction. Cephalad instrumentation should end high in the thoracic spine (T2) to decrease proximal junctional kyphosis.
Imrie et al. reviewed the management of spinal deformity in CP. They advocate posterior-only pedicle screw fusion for curves <100° that bend down to 50% on traction films, from T2-3 to the pelvis, using iliac screws. They advocate single-stage anterior release and posterior fusion for curves >120° with poor flexibility, or associated severe pelvic obliquity or sagittal deformity.
McCarthy et al. reviewed scoliosis in CP. They advocate proximal fixation to the upper thoracic spine (T1-2), and distal fixation to L4-5 (pelvic obliquity <15°) or to the pelvis (pelvic obliquity >15°). They add anterior release for larger, rigid curves that do not bend out to <60°, and in skeletally immature children.
Figures A and B are PA and lateral scoliosis radiographs demonstrating 75° of thoracolumbar scoliosis and severe pelvic obliquity, and progressive lumbar hyperlordosis. Illustrations A and B are PA and lateral scoliosis radiographs demonstrating correction of curve and pelvic obliquity using the Galveston Technique with segmental fixation utilizing sublaminar wires.
Incorrect Answers:
(SBQ12SP.26) Figure A is a lateral cervical spine radiograph of a 70-year-old female who presents with two months of posterior midline neck pain that is worse with motion. She has no history of trauma. She denies any symptoms of arm pain, gait instability, or dexterity problems with her hands. Physical exam of the lower extremities shows 2+ patellar reflexes and flexion of the great toe with a Babinski test. What should the patient be told regarding these radiographic findings? Review Topic

She requires surgical decompression to prevent progressive neurologic deterioration
85% of individuals over the age of 60 years of age demonstrate these findings
She is indicated for MRI to rule out cervical radiculopathy
She would benefit from modalities such as heat, cold, and transcutaneous electrical stimulation
She has <10% chance of having symptomatic improvement with non-operative treatment
The patient has symptomatic cervical spondylosis. She should be told that 85% of asymptomatic individuals over the age of 60 demonstrate these radiographic findings.
Cervical spondylosis is defined as age-related degenerative changes within the cervical spinal column. It can present as axial neck pain, cervical radiculopathy, cervical myelopathy, or as a combination of each. Radiographs demonstrate loss of disc height, arthrosis of the facet and uncovertebral joints, and endplate sclerosis. Imaging such as cervical spine radiographs and MRI should be interpreted carefully and correlated with clinical symptoms, as radiographic evidence of spondylosis is frequently seen in asymptomatic patients.
Boden et. al. reviewed the cervical MRI of 63 asymptomatic volunteers with no history of cervical spine symptoms. Of those, 19% were interpreted as having an abnormality. These findings included herniated nucleus pulposus, bulging disc, and foraminal stenosis. 60% of patients over 40 years demonstrated disc degeneration or narrowing at one level.
Rao et al. reviewed the presentation, pathogenesis, and management of cervical spondylosis. In this review, they report that 85% of patients older than 60 years demonstrate cervical spondylosis on radiography.
Figure A is a lateral cervical spine radiograph demonstrating spondylosis at multiple levels. There is disc height loss, facet sclerosis, and anterior osteophyte formation.
Incorrect Answers:
Question 31
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 32
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
Explanation
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
Question 33
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 34
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 35
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 36
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Beredjiklian PK, Nalbantoglu U, Potter HG, et al: Prosthetic radial head components and proximal radial morphology: A mismatch. J Shoulder Elbow Surg 1999;8:471-475.
Question 37
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
REFERENCES: Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 19-27.
Question 38
- A 50-year-old alcoholic man has erythema and swelling in his entire dominant upper extremity. He has a WBC of 15,000/mm3, a temp of 101 oF (38.3 oC), and a blood pressure of 90/60 mm Hg. After hemodynamic stabilization, the cellulitic forearm is longitudinally incised dorsally and volarly. The forearm muscles are normal in appearance; however, the subcutaneous fat is necrotic. A culture will most likely reveal
Explanation
Question 39
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
REFERENCES: Cain JE Jr, Rosenthal HG, Broom MJ, Jauch EC, Borek DA, Jacobs RR: Quantification of leakage pressures after durotomy repairs in the canine. Spine 1990;15:969-970.
Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 40
Which of the following statements is true regarding articular cartilage?
Explanation
Proteoglycans, the most common of which is aggrecan, are produced by chondrocytes and give articular cartilage its hydrophilic properties. Multiple glycosaminoglycans (GAGs), such as chondroitin and keratin can attach to core proteins to form aggrecans. Link proteins then help aggrecans interact with hyaluronic acid. The negative charge of this complex helps create a strong osmotic gradient, which attracts water and increases tissue pressures. Normal aging involves a decrease in the water content of the extracellular matrix while osteoarthritis is associated with increased water content, which leads to loss of strength and elasticity.
Chen et al. evaluated the strain and depth related properties of articular cartilage in bovine models. They found that the zero-strain permeability, zero-strain equilibrium confined compression modulus, and deformation dependence constant differed among the layers of cartilage. They suggest that the complex strain-dependent properties of articular cartilage of different thickness and location have clinical implications for tissue engineering.
Illustration A is a diagram depicting the extracellular matrix of articular cartilage. Incorrect Answers:
Question 41
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?
Explanation
REFERENCES: Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573.
Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Pinzur M: Surgical versus accommodative treatment for Charcot arthropathy of the midfoot.
Foot Ankle Int 2004;25:545-549.
Question 42
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
Explanation
REFERENCES: Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A
meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.
Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 43
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.
Question 44
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
Question 45
78A B Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?

Explanation
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. View Abstract
at PubMed
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
PMID: 18207430. View Abstract at PubMed
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
Question 46
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
REFERENCES: Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34.
Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 47
A 62-year-old woman has loss of function of her left shoulder and dull pain. She denies any history of trauma, and there were no previous surgical procedures. MRI scans are shown in Figures 42a and 42b. The etiology of this pathology is most likely confirmed by Review Topic
Explanation
Question 48
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 49
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 50
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
Explanation
REFERENCES: Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22.
Question 51
What is the most common mechanism of injury that produces turf toe?
Explanation
REFERENCES: Clanton TO, Ford JJ: Turf toe injury. Clin Sports Med 1994;13:731-741.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsophalangeal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 52
Poor outcomes with necrotizing fasciitis have been associated with which of the following factors?

Explanation
Question 53
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 54
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of
Explanation
REFERENCE: Clarke CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Question 55
What is the most common type of malalignment after intramedullary nailing of distal 1/3 tibia fractures?

Explanation
McKee et al randomized 85 patients undergoing intramedullary tibial nailing using manual traction with the leg draped free versus standard fracture table positioning and traction. They found that manual traction is an effective technique that can save a significant amount of time without sacrificing the quality of reduction or fixation of tibial shaft fractures.
Question 56
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 57
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 58
Examination of a 7-year-old girl with myelomeningocele reveals calcaneal deformities of both feet. She ambulates on both extremities wearing ankle-foot orthoses and has no upper extremity aids. She has grade 5/5 motor strength to the tibialis anterior muscles and absent motor strength to the triceps surae. There is no varus or valgus deformity of the hindfoot, and the skin over the heels is intact; however, mild callosities are present. Management should consist of
Explanation
REFERENCES: Stott NS, Zionts LE, Gronley JK, Perry J: Tibialis anterior transfer for calcaneal deformity: A postoperative gait analysis. J Pediatr Orthop 1996;16:792-798.
Georgiadis GM, Aronson DD: Posterior transfer of the anterior tibial tendon in children who have a myelomeningocele. J Bone Joint Surg Am 1990;72:392-398.
Question 59
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
REFERENCES: McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Vegso JJ: Field evaluation and management of head and neck injuries. Post Grad Adv Sport Med 1987;10:2-10.
Question 60
Which of the following statements is true regarding the superomedial fragment of an intra-articular calcaneus fracture?

Explanation
Question 61
The implant shown in Figures 47a and 47b is introduced submuscularly employing a minimally invasive technique. A percutaneous method of screw insertion is used distally. What nerve is most at risk?

Explanation
Question 62
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
REFERENCES: Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
Question 63
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
Question 64
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?
Explanation
REFERENCES: Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2,
pp 2391-2409.
Dameron TB Jr: Fractures of the proximal fifth metatarsal: Selecting the best treatment option.
J Am Acad Orthop Surg 1995;3:110-114.
Question 65
You are evaluating a patient with recurrent patellar instability who has failed conservative management. MRI demonstrates articular cartilage loss in the patella. In addition to a cartilage restoration procedure, you recommend the procedure depicted in Figures A and B. Which of the following imaging findings best supports your decision? Review Topic

Explanation
Recurrent patellar instability is often associated with chondral lesions of the patellofemoral joint. In addition to managing the cartilage injury, the underlying etiology of the instability must also be addressed to ensure a successful outcome. Patellar instability may arise from coronal or rotational malalignment, patella alta, trochlear dysplasia or damage to soft tissue restraints including the medial patellofemoral ligament (MPFL). Rotational malalignment, defined by a TT-TG distance > 20mm, can be addressed by AMZ. Medialization of the tubercle restores a normal TT-TG distance while anteriorization of the tubercle unloads patellofemoral contact forces.
Beck et al performed a cadaveric study measuring patellofemoral contact pressures on the trochlear surface following AMZ. They found that anteromedialization decreased the mean contact pressures and shifted contact pressures to the medial trochlea. The authors concluded that while this procedure successfully unloads the lateral trochlea, it likely has minimal benefit for central chondral defects and may be detrimental for medial chondral defects where contact pressures are increased.
Strauss et al authored a review article detailing the surgical treatment options for patellofemoral cartilage lesions, including concomitant realignment/unloading procedures. AMZ is designed to correct rotational malalignment while unloading the patellofemoral compartment in the setting of cartilage restoration surgery. While AMZ has demonstrated good outcomes for lesions located in the lateral facet or distal
pole of the patella, poor outcomes have been seen with medial facet or central trochlear lesions.
Figures A and B are the AP and lateral radiographs, respectively, of a knee s/p AMZ, also know as a Fulkerson procedure. Illustration A is an algorithm detailing the approach to recurrent patellar instability in both skeletally immature and mature patients. Illustration B demonstrates how to measure the TT-TG distance, the distance between two lines drawn perpendicular to the posterior condylar axis to the tibial tubercle and deepest portion of the trochlear groove (normal 8-10mm). Illustration C depicts the measurement of the femoral trochlear angle or sulcus angle (normal 137°
+/- 8°). Illustration D shows how to measure lateral patellar tilt (normal < 5°). Illustration E is a postoperative radiograph after AMZ. A long (> 5cm) and thick (> 0.75cm) osteotomy cut is required to allow adequate fixation with two screws.
Incorrect Responses:
Question 66
below depicts the radiograph obtained from a year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 67
-A 30-year-old man sustained the injury seen in Figure 261. According to the Lauge-Hansen Classification System, the fracture should be classified as
Explanation

Question 68
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
Explanation
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.

CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
Question 69
Figure 20 shows the resting and stress radiographs of a patient who has had pain and feelings of instability after undergoing a total knee arthroplasty 1 year ago. Which of the following ligaments is not functional and is therefore responsible for the patient’s symptoms?
Explanation
REFERENCE: Incavo SJ, Churchill DL: The role of the posterior cruciate ligament in total knee arthroplasty. Techniques Orthop 1999;14:267-273.
Question 70
A 17-year-old basketball player has a soft-tissue abscess over the anterior aspect of his left knee. The team physician prescribes amoxicillin and the infection resolves. The next week the patient develops fevers and significantly increased pain at the site of the previous infection. What is the most likely diagnosis? Review Topic
Explanation
Question 71
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?
Explanation
REFERENCES: Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Spiegel PG, Mast JW, Cooperman DR, et al: Triplane fractures of the distal tibial epiphysis.
Clin Orthop Relat Res 1984;188:74-89.
Question 72
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
REFERENCE: Bingol H, Cingoz F, Yilmaz AT, et al: Vascular complications related to lumbar disc surgery: J Neurosurg 2004;100:249-253.
Question 73
- Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Explanation
Question 74
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a “bedding in” phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component.
REFERENCES: Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.
Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of
ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.
Question 75
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
REFERENCES: Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 76
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of
Explanation
REFERENCES: Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Pelligrini VD Jr, Konski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 77
An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?
Explanation
REFERENCES: Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Schneider RC, Thompson JM, Rebin J: The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
Question 78
A 56-year-old woman presents with left hip pain and diminishing range of motion. Examination reveals pain with range of motion of the hip. Radiographs reveal multiple calcific lesions within the hip and well-preserved joint space. MRI scan shows thickened synovium nodular loose bodies with decreased signal on T1 and T2. What is the best next step?
Explanation
Question 79
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 80
7 weeks from injury at a union rate of 94.5%. They concluded that functional bracing has many known benefits and remains a reliable treatment however certain parameters such as functional outcome, residual deformity, and loss of joint motion remain unclear and require further research.
Explanation
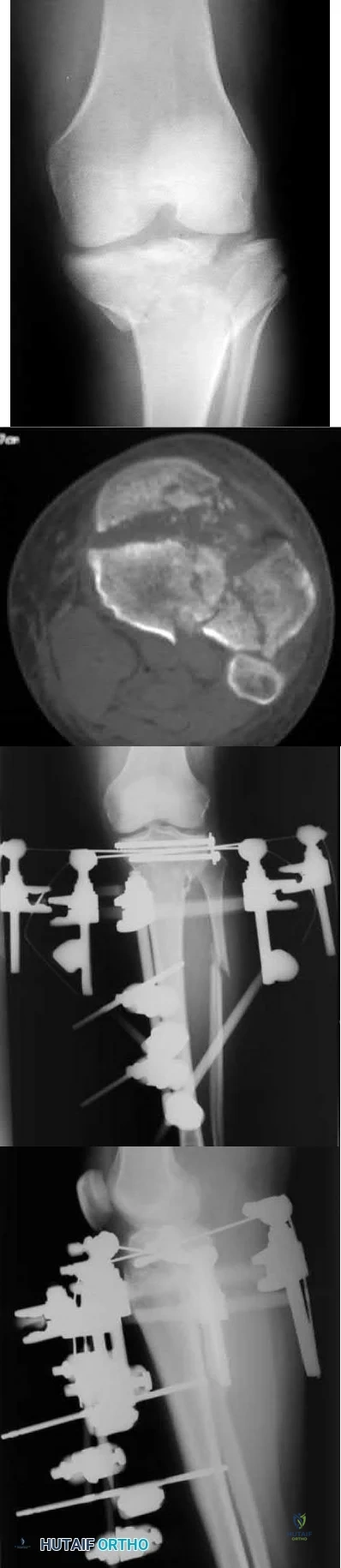
A patient presents with the injury shown in figures A and B. What has been associated with the technique depicted in figures C and D?
Longer operative times
Increased deep surgical infection rates
Unacceptably high malunion/nonunion rates
Slower early return to function
Longer hospital stays Corrent answer: 3
Treatment of Shatzker V and VI tibial plateau fractures with hybrid external fixation is associated with increased malunion and nonunion rates.
Hybrid external fixation for treating tibial plateau fractures involves the use of an external fixator to achieve reduction through ligamentotaxis. Additional fracture reduction is achieved through limited open incisions with fixation augmented through percutaneous cannulated screws. Definitive treatment with this technique avoids soft tissue complications that have been associated with traditional open reduction and internal fixation with bicondylar plating.
However, studies have reported high malunion and nonunion rates due to a lack of rigid fixation.
Bertrand et al. performed a prospective cohort study of patients undergoing either open reduction and internal fixation versus hybrid external fixation for Schatzker V and VI tibial plateau fractures. Hybrid external fixation was associated with significantly shorter operative times but insignificantly increased complication rates. They concluded that there were limited statistically differences between these techniques, but further studies are required before advising hybrid external fixation for higher Schatzker tibial plateau fractures.
Gross et al. performed a retrospective study of patients treated with hybrid external fixation for Shatzker V and VI tibial plateau fractures. The authors found there was an 80% union rate, a 70% satisfactory reduction rate, and a 52% rate of malunion. The development of osteoarthritis was associated with plateau widening, articular comminution, articular step-off, and incorrect mechanical alignment. The authors concluded that hybrid external fixation is an effective means for the treatment of tibial plateau fractures that minimizes tissue dissection, with decreased blood loss, and shorter operative times, but associated with a very high malunion rate.
Hall et al. performed a multicenter randomized controlled trial comparing the treatment of Schatzker V and VI fractures with open reduction and internal fixation with hybrid external fixation. Patients with hybrid external fixation had less intraoperative blood loss, fewer unanticipated secondary procedures, slightly faster return to pre-injury activity at 6 months and 1 year, and shorter
hospital stay. They concluded that both hybrid external fixation and open reduction and internal fixation provide effective means for fracture treatment, but hybrid external fixation avoids soft tissue complications with deleterious consequences.
Figure A is an AP radiograph of the right knee with a Schatzker VI tibial plateau fracture. Figure B is an axial CT slice of the articular surface of the tibia with extensive comminution. Figures C and D are the AP and lateral radiographs of the knee with a hybrid external fixation construct for a tibial plateau fracture
Incorrect answers:
OrthoCash 2020
An 89-year-old female sustained the injury shown in Figure A and underwent a hemiarthroplasty. Which of the following has been associated with increased rates of post-operative dislocation?

Posterior approach
Anterior approach
Anterolateral approach
Use of a bipolar implant
Use of a monopolar implant
The incidence of dislocation after hemiarthroplasty is highest when using a posterior approach.
Elderly femoral neck fractures are one of the most common fractures encountered by orthopaedists and will only become more common as the population continues to age. The displacement of the femoral head is associated with delayed union or nonunion, an increased risk of femoral head necrosis due to disrupted blood flow at the femoral neck, and failure of internal fixation devices. For this reason, displaced femoral neck fractures in older patients are often treated with hemiarthroplasty. Three approaches to hemiarthroplasty have been described: a lateral approach, a posterior approach, and an anterior approach. The posterior approach has been used more historically; however, its use has been called into question as it has been associated with increased dislocation rates.
Parker performed a trial on all patients with intracapsular femoral neck fractures being treated with hemiarthroplasty. Patients were randomized to surgery using either a lateral or posterior approach. They found that there were no statistically significant differences observed for any of the outcome measures including mortality, degree of residual pain and regain of walking ability. They concluded that both surgical approaches appear to produce comparable functional outcomes.
van der Sijp et al. performed a meta-analysis to compare the outcomes based on approaches for hemiarthroplasty in the treatment of proximal femur fractures. They found 21 studies and found that the posterior approach poses an increased risk of dislocation and reoperation compared to the lateral approach and anterior approaches. They conclude that there are no evident advantages of the posterior approach and its routine use for fracture-related hemiarthroplasty should be questioned.
Figure A is an AP pelvis radiograph demonstrating a displaced right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 50-year-old male sustained a humeral shaft fracture treated operatively 6 months ago. He denies medical problems but smokes 10 cigarettes per day. His current radiograph is shown in Figure A. He continues to have pain in his arm that is affecting his quality of life. On physical examination, there is motion at the fracture site. C-reactive protein and erythrocyte sedimentation rate are within normal limits. Which is the most appropriate definitive treatment for this fracture?

Exchange humeral nailing
Augmentative plating
Nail removal with open reduction compression plating
Smoking cessation and medical optimization
Nail removal with open reduction and compression plating with bone grafting
This patient has sustained an atrophic nonunion of a humeral shaft fracture treated with an intramedullary nail. The most appropriate definitive treatment is nail removal with open reduction and compression plating with bone grafting.
Most diaphyseal humeral fractures can be managed non-operatively with functional bracing. Operative treatment is indicated under a number of circumstances including open fractures, associated neurovascular injury, proximal and distal articular extension of the fracture, and in patients with other multiple injuries. Surgical stabilization can be accomplished with different implants and techniques. The two most common are plate and screw fixation and intramedullary nailing. Plate fixation has the advantages of potential absolute stability and sparing the rotator cuff from an incision. Intramedullary nailing has to be inserted proximally with potential damage to the rotator cuff. It, however, can be inserted with small incisions. If a nonunion develops after intramedullary nailing, nail removal and compression plating is the preferred treatment choice.
Heineman et al. performed a metanalysis on plate fixation or intramedullary nailing of humeral shaft fractures. They performed a literature search from 1967-2007 comparing nails and plates in patients with humeral shaft fractures that reported complications due to surgery. They found that the risk of a complication is lower when plating a fracture of the humeral shaft than when using an intramedullary nail.
Gerwin et al. performed an anatomical study to define the course of the radial nerve in the posterior aspect of the arm, with particular reference to its relationship to operative exposures of the posterior aspect of the humeral diaphysis. They found that the radial nerve crosses the posterior aspect of the humerus from an average of 20.7 +/- 1.2 centimeters proximal to the medial epicondyle to 14.2 +/- 0.6 centimeters proximal to the lateral epicondyle. They found the approach to permit the most visualization was the triceps reflecting approach.
Figure A is a lateral radiograph of an atrophic nonunion of a humeral shaft being stabilized with an intramedullary nail.
Incorrect Answers:
OrthoCash 2020
A 45-year-old man is struck while crossing a major highway and sustains the injury depicted in Figure A. Which of the following statements comparing the techniques in Figure B and C is most accurate?
Technique depicted in Figure B is associated with an increased risk of septic arthritis
Technique depicted in Figure B is associated with increased rate of anterior knee pain
Technique depicted in Figure B is associated with improved postoperative fracture alignment
Technique depicted in Figure C is associated with an increased risk of septic arthritis
Technique depicted in Figure C is associated with improved postoperative fracture alignment
Compared to infrapatellar tibial nailing, suprapatellar tibial nailing is associated with improved postoperative fracture alignment.
While antegrade tibial nailing results in postoperative anterior knee pain in approximately 20% of patients, there is no significant difference in the incidence of anterior knee pain when the conventional infrapatellar approach is compared to suprapatellar approaches. In open tibial shaft fractures, no difference has been observed in the incidence of knee sepsis with either approach. However, several studies have demonstrated that intramedullary nail fixation through a suprapatellar approach is associated with a more accurate entry position and a more accurate fracture reduction when compared with an infrapatellar technique, particularly in more proximal and distal shaft
fractures, without evidence of a functional impact on the patellofemoral joint. Lastly, intraoperative radiography is generally less cumbersome with suprapatellar nailing.
Marecek et al. performed a multicenter comparison study of suprapatellar and infrapatellar approaches and the risk of knee sepsis after treatment of open tibia fractures. They reported no differences in the rates of infection, deep infection, or reoperation between suprapatellar and infrapatellar nailing groups. They concluded that the risk of knee sepsis after suprapatellar nailing of open fractures is low.
Avilucea et al. performed a retrospective cohort study comparing postoperative alignment after suprapatellar versus infrapatellar nailing for distal tibial shaft fractures. They reported a significantly increased rate of primary angular malalignment of greater than 5 degrees in the infrapatellar compared to the suprapatellar nailing cohort. They concluded that in the treatment of distal tibial fractures, suprapatellar nailing results in a significantly lower rate of malalignment compared with the infrapatellar nailing.
Jones et al. performed a study comparing the radiologic outcome and patient-reported function after suprapatellar and infrapatellar intramedullary nailing. They reported no difference in anterior knee pain, however, found a more accurate fracture reduction, both in terms of angulation and translation in the coronal plane, with the use of the suprapatellar technique. They concluded that when compared with infrapatellar nailing, the suprapatellar technique was not associated with more anterior knee pain, yet more accurate nail insertion and fracture reduction.
Figure A depicts a displaced distal third tibial shaft fracture. Figure B depicts the infrapatellar tibial nailing technique. Figure C depicts the suprapatellar tibial nailing technique.
Incorrect Answers:
OrthoCash 2020
A 56-year-old woman sustains the closed injury depicted in Figures A-B. On examination, her wrist is mildly swollen and she is unable to actively oppose her thumb. She also complains of some paresthesias in her thumb and index finger. The patient undergoes closed reduction and splinting; however, her paresthesias worsen significantly in the next 12 hours. What is the likely mechanism of her paresthesias and what is the most appropriate treatment?

Nerve compression; open reduction internal fixation with open carpal tunnel release
Nerve laceration; open reduction internal fixation with primary nerve repair or grafting
Decreased arterial inflow; fasciotomy with open reduction internal fixation
Reflex sympathetic dystrophy; vitamin C
Nerve compression; repeat closed reduction Corrent answer: 1
This patient is presenting with signs of acute carpal tunnel syndrome (CTS) in the setting of a displaced distal radial fracture. The pathogenesis of acute CTS is nerve compression, requiring urgent open carpal release with open reduction internal fixation (ORIF).
Acute CTS is a well-recognized phenomenon after distal radial fractures. Risk factors include ipsilateral upper extremity fractures, translation of the fracture fragments, and articular distal radius fractures (DRFs). Acute CTS can manifest with paresthesias in the median nerve distribution and opponens pollicis weakness. Acute CTS is an indication for urgent surgical decompression of the median nerve.
Odumala et al. performed a study to evaluate the role of carpal tunnel decompression in the prevention of median nerve dysfunction after buttress plating of DRFs. They reported that prophylactic decompression of the carpal tunnel results in twice the relative odds of developing median nerve dysfunction, which routinely self-resolved. They concluded that prophylactic median nerve decompression does not alter the course of median nerve dysfunction and may actually increase postoperative morbidity.
Medici et al. performed a case-control study to investigate whether carpal tunnel release (CTR) during fixation DRFs improves outcomes. They reported no statistically significant difference between the groups in VAS and Mayo Wrist Scores, however, an increased risk of subsequent CTR in the group who underwent ORIF with no CTR at the index procedure. They concluded that the release of the transverse carpal ligament during ORIF may reduce the incidence of postoperative median nerve dysfunction.
Niver et al. reviewed CTS after DRFs. They reported that acute CTS noted at the time of DRF warrants urgent surgical release of the carpal tunnel and fracture fixation, and that delayed CTS presenting after a distal radius fracture has healed may be managed in the standard fashion for CTR. They concluded that there is no role for prophylactic CTR at the time of distal radius fixation in a patient who is asymptomatic.
Figures A and B depict a displaced apex volar DRF and a mildly displaced ulnar styloid fracture.
Incorrect Answers:
OrthoCash 2020
Figures A and B depict the closed injury radiograph of a 79-year-old right-hand-dominant woman who fell on her left wrist. According to meta-analysis and systematic reviews, which of the following statements is most accurate regarding her injury?

Improved functional outcomes with open reduction internal fixation (ORIF) through FCR approach vs. closed treatment
No difference in radiographic outcomes after ORIF vs. closed treatment
No difference in functional outcomes after ORIF vs. closed treatment
Improved functional outcomes with closed treatment vs. ORIF
Improved functional outcomes with external fixation and K wire fixation vs. ORIF
This elderly patient has sustained a closed intra-articular and shortened distal radial fracture (DRF). Many studies have reported no difference in functional outcomes when patients aged 60 and over are treated in a closed manner versus operatively for unstable fractures.
The treatment of DRFs in the elderly population is controversial. A variety of nonoperative and operative treatments are available, including closed reduction and splinting/casting, K wire stabilization, external fixation, and ORIF. While conservative management of DRFs in the elderly is common,
recent systematic reviews and meta-analyses have demonstrated that despite worse radiographic outcomes after closed treatment of unstable fractures, functional outcomes were no different between patients treated closed versus surgically in patients over the age of 60 years.
Ju et al. published a systematic review and meta-analysis comparing treatment outcomes between nonsurgical and surgical treatment of unstable DRFs in the elderly. They reported no significant differences in DASH score, VAS pain score, grip strength, wrist extension, pronation, supination, and ulnar deviation between the groups. They concluded that operative and nonoperative treatments result in similar outcomes in the treatment of unstable DRFs in the elderly, with no impact on subjective function outcome and quality of life with closed treatment.
Diaz-Garcia et al. published a systematic review of the outcomes and complications after treating unstable DRFs in the elderly, comparing various treatment techniques. They reported significant differences in wrist motion, grip strength, DASH score, although these findings may not be clinically meaningful. They concluded that although the operatively treated group had improved radiographic outcomes, functional outcomes were no different when compared to the group treated in a closed manner.
Figure A depicts an unstable intra-articular and shortened DRF. Incorrect Answers:
no difference in functional outcomes between operative and closed treatment modalities for DRF.
OrthoCash 2020
An active 60-year-old woman falls from her attic and presents with the injury in Figure A. She undergoes successful closed reduction and sling immobilization. At follow up, she is unable to move her shoulder. New radiographs are depicted in Figures B and C. What is the next best step?
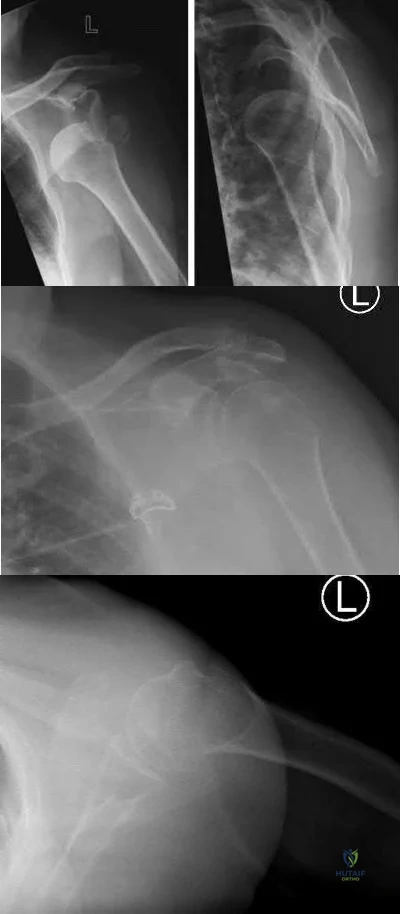
Continued sling immobilization
Closed reduction percutaneous pinning
Open reduction internal fixation
Hemiarthroplasty
Reverse total shoulder arthroplasty Corrent answer: 3
This active patient presents with a greater tuberosity fracture dislocation. Open reduction internal fixation (ORIF) is indicated, particularly when the greater tuberosity fragment is displaced greater than 5mm.
Many proximal humerus fractures are minimally displaced and respond acceptably to nonoperative management. Isolated greater tuberosity fractures or rotator cuff injuries are associated with shoulder dislocations in the elderly population. The greater tuberosity fragment undergoes deforming forces by the supraspinatus and infraspinatus muscles. In active patients, it is well-accepted that greater tuberosity fracture displacement greater than 5mm is an indication for ORIF to restore their ability to perform overhead activities and prevent impingement.
Schumaier et al. published a review article on the treatment of proximal humerus fractures in the elderly. They highlighted that while bone density was a predictor of reduction quality, social independence was a better predictor of outcome. They concluded that although the majority of minimally displaced fractures can be treated successfully with early physical therapy, treatment for displaced fractures should consider the patient's level of independence, bone quality, and surgical risk factors. They emphasized that there was no clear evidence-based treatment of choice, and the surgeon should consider their comfort level during their decision-making.
George et al. published a review article on greater tuberosity humerus fractures. They reported that these fractures may occur in the setting of anterior shoulder dislocations or impaction injuries against the acromion or superior glenoid, with surgical fixation recommended for fractures with greater than 5 mm of displacement in the general population or greater than 3 mm of displacement in active patients involved in frequent overhead activity. They recommended close followup and supervised rehabilitation to increase successful outcomes.
Figure A depicts a greater tuberosity fracture dislocation of the left shoulder. Figures B and C depict reduction of the glenohumeral joint with residual displacement of the greater tuberosity. Illustrations A and B depict radiographs after ORIF.
Incorrect Answers:

OrthoCash 2020
A 21-year-old football player is tackled as he falls onto an outstretched arm. He sustains the injury shown in Figure A. He undergoes successful operative treatment of his injury. In which order did his injury occur?

MCL > LCL > anterior capsule
MCL > anterior capsule > LCL
anterior capsule > MCL > LCL
LCL > anterior capsule > MCL
LCL > MCL > anterior capsule Corrent answer: 4
The patient sustained a terrible triad injury of the elbow, which progresses from the LCL to the anterior capsule and then the MCL.
Terrible triad injuries of the elbow are traumatic injuries that occur after a fall on an extended arm that results in a combination of valgus, axial, and posterolateral rotatory forces. The key features of a terrible triad injury include a radial head fracture, a coronoid fracture, and an elbow dislocation. Disruption of the structures in the elbow characteristically occurs from lateral to medial, affecting the LCL first, followed by the anterior capsule and MCL. Outcomes following terrible triad injuries have historically been poor; however, more recent literature has shown that good outcomes can be achieved with surgical stabilization of the elbow followed by an early rehabilitation protocol. Some authors use temporary immobilization, but range-of-motion exercises are typically initiated by 48 hours postoperatively. Active range of motion is particularly important, as it recruits muscles that act as dynamic stabilizers of the elbow. Depending on the injury, method of fixation, and stability that is achieved, the range of motion may be limited to 30° of extension during the early postoperative period but should allow full flexion.
Giannicola et al. (2013) performed a study to determine the critical time period for recovery of functional range of motion after surgical treatment of complex elbow instability (CEI). They found that the first 6 months after surgery represent the critical rehabilitation period to obtain a functional elbow and that elbow flexion recovered at a rate slower than that of the other elbow movements. They recommend that, following CEI surgical treatment, a rehabilitation program should be started promptly and should be continued for at least 6 months because a significant improvement of ROM occurs in this period.
Giannicola et al. (2015) performed a study analyzing the predictability of outcomes of terrible triad injuries (TTI) treated according to current diagnostic and surgical protocols. They found that the current diagnostic and therapeutic protocols allow for satisfactory clinical outcomes in a majority of cases but a high number of major and minor unpredictable complications still persist. Low compliance, obesity, and extensive soft elbow tissue damage caused by high-energy trauma represented negative prognostic factors unrelated to surgery.
McKee et al. performed a review on their standard surgical protocol for the treatment of elbow dislocations with radial head and coronoid fractures. Their surgical protocol included fixation or replacement of the radial head; fixation of the coronoid fracture, if possible; repair of associated capsular and lateral ligamentous injuries; and, in selected cases, repair of the medial collateral ligament and/or adjuvant-hinged external fixation. They found that their surgical protocol restored sufficient elbow stability to allow early motion postoperatively, enhancing the functional outcome. They recommend early operative repair with a standard protocol for these injuries.
Figure A is a lateral radiograph of the elbow demonstrating a terrible triad injury with a comminuted radial head/neck fracture, displaced coronoid fracture, and posterior elbow dislocation. Illustration A is a rendered image of the radiograph shown in Figure A with the components labeled.
Incorrect Answers:
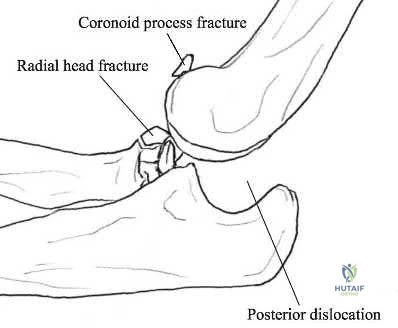
OrthoCash 2020
An 82-year-old female sustains the fracture shown in Figure A as the result of a ground level fall. Which of the following has been shown to be a reliable predictor of postoperative lateral wall fracture for this injury after treatment with a sliding hip screw?
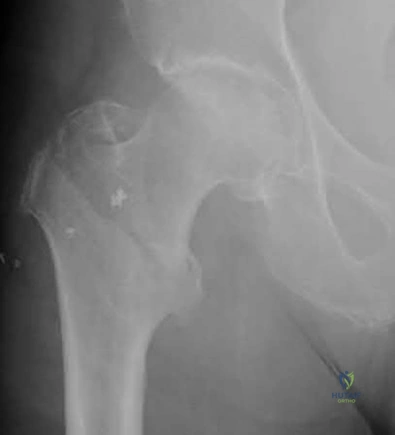
Reverse obliquity fracture pattern
Lateral wall thickness
Previous contralateral hip fracture
DEXA T-score <-2.0
Calcar comminution
Lateral wall thickness has been shown to be a predictor of postoperative lateral wall fracture. As the lateral wall thickness decreases, there is an increased chance of fracture.
Lateral wall fracture creates an unstable fracture pattern and increased screw sliding/collapse. This shortens the neck and abductors, leading to worse patient outcomes (radiographic and clinical). Recognition of a thin wall should lead toward the use of an intramedullary device or adjunct use of a trochanteric stabilizing plate with a sliding hip screw device.
Baumgaertner et al. reported that the failure of peritrochanteric fractures that have been treated with a fixed-angle sliding hip-screw device is frequently related to the position of the lag screw in the femoral head. They established the tip-apex distance as the sum of the distance from the tip of the lag screw to the apex of the femoral head on an anteroposterior radiograph and this distance on a lateral radiograph, after controlling for magnification. Upon reviewing their series, none of the 120 screws with a tip-apex distance of twenty-five millimeters or less cut out, but there was a very strong statistical relationship between an increasing tip-apex distance and the rate of cutout, regardless of all other variables related to the fracture.
Socci et al. performed a literature review of relevant papers and appropriate clinical databases and concluded that fixation of AO 31A1 fractures was best achieved with a sliding hip screw device and that all other types of intertrochanteric hip fractures be fixed with an intramedullary device.
Utrilla et al. reported no difference in outcome in stable fractures, but better mobility at one year following intramedullary fixation of unstable fractures.
Hsu et al. measured the thickness of the lateral wall of patients with AO/OTA 31-A1 and 31-A2 type intertrochanteric hip fractures. They found that the lateral wall thickness was a reliable predictor of postoperative lateral wall fracture for unstable AO Type A2 fractures and concluded that the lateral wall thickness threshold value for risk of developing a secondary lateral wall fracture was found to be 20.5 mm.
Figure A shows a standard obliquity intertrochanteric hip fracture.
Illustration A from the Hsu article demonstrates the measurement of the lateral wall thickness. The distance is measured along a 135-degree angle, between a point 3cm distal to the innominate tubercle of the greater trochanter and the fracture line (midway between the two cortical lines).
Incorrect Answers:
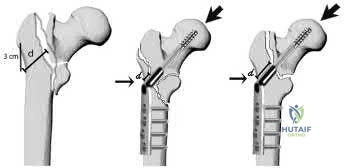
OrthoCash 2020
A 78-year-old patient presents with right hip pain and inability to bear weight after an unwitnessed fall at a nursing home. Figures A and B are the radiographs of the hip and pelvis. Which statement is true regarding the treatment of these injuries?

Smaller lateral wall thickness favors sliding hip screw constructs
Unstable fractures are best treated with sliding hip screw constructs
Avoiding distal locking screws in intramedullary implants protects against refracture
Stable fractures have no differences in outcomes between sliding hip screws and intramedullary implants
Implant stability has a greater impact on outcomes rather than reduction quality
Studies have shown that in stable intertrochanteric femur fractures there are no differences in outcomes between sliding hip screws and intramedullary implants.
Intertrochanteric femur fractures are one of the most common fractures in the geriatric population. Implant selection has been a great topic of research with most studies reporting minimal to no differences in outcomes between intramedullary and sliding hip screw constructs in stable fracture patterns.
Unstable fractures, however, are reportedly better treated with a distally locked intramedullary implant. The quality of fracture reduction has a greater impact on the overall outcome than implant selection.
Hsu et al. performed a retrospective study of risk factors for postoperative lateral wall fractures in patients treated with sliding hip screws for intertrochanteric femur fractures. They found that fracture classification and lateral wall thickness, which is measured from 3 cm distal from innominate tubercle and angled 135 degrees to the fracture line, were associated with postoperative lateral wall fracture. They recommended not treating intertrochanteric femur fractures with sliding hip screws if the lateral wall thickness is less than 20.5 mm.
Socci et al. reviewed the literature regarding the treatment of intertrochanteric femur fractures. Based on the literature, they recommend treatment of AO/OTA type 31A1 fractures with sliding hip screws, type 31A2 fractures with short intramedullary implants, and 31A3 fractures with long intramedullary implants. Simple basicervical fractures of the femoral neck can be treated with sliding hip constructs whereas comminuted fractures treated with intramedullary devices due to the inherent instability of the pattern. The most import aspect in fracture healing is the quality of the reduction rather than the choice of implant.
Lindvall et al. performed a retrospective study of refracture rates in patients treated with either long or short cephalomedullary nails. The authors found a 97% union rate with both implant types and refracture not associated with either long or short implants. Rather, refracture was associated with the lack of a distal locking screw. The authors recommended locking intramedullary implants to avoid refracture.
Utrilla et al. performed a randomized control trial of elderly patients treated
with compression hip screw or Trochanteric Gamma Nail for intertrochanteric femur fractures. They reported the only differences between the two implants were quicker operating time, less fluoroscopy use, and better walking with unstable fractures treated with intramedullary implants. The authors recommended either construct for stable fractures, but intramedullary implants for unstable fractures.
Figures A and B are the AP and lateral radiographs of the right hip radiographs demonstrating a simple and minimally displaced intertrochanteric femur fracture, classified as an AO/OTA 31A1 fracture. Illustration A depicts the AO/OTA classification system for proximal femur fractures.
Incorrect answers:
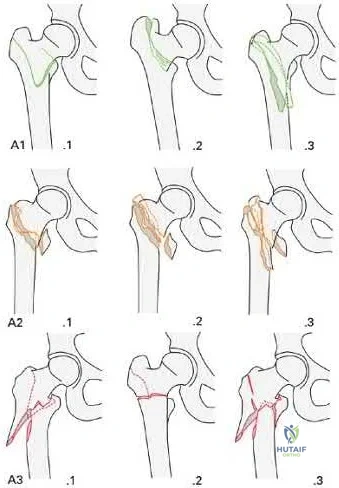
OrthoCash 2020
A 28-year-old male that sustained a closed left femoral shaft fracture 12 months ago and underwent intramedullary nailing presents with persistent pain in the right thigh. The patient walks with an antalgic gait. He denies any fevers or chills. His surgical sites are well healed and there are no signs of drainage. Serum ESR and CRP are 12 mm/hr (reference <20 mm/hr) and 0.9 mg/L (reference <2.5 mg/L), respectively. Figures A and B are the AP and lateral radiographs of the left femur. Which treatment option offers the highest chance of union and enables immediate weight-bearing?

Nail removal with compression plating and open bone grafting
Closed reamed exchange nailing
Nail dynamization
Nail retention with plate augmentation and bone grafting
Electrical bone stimulator Corrent answer: 4
The patient is presenting with a hypertrophic nonunion of the femur below the isthmus, which studies have shown to have a higher union rate when treated with plate augmentation. Retention of the nail allows for full weight-bearing postop.
Hypertrophic nonunion of the femur is the result of fracture site hypermobility with sufficient biology for healing. This is demonstrated with abundant callus formation without bridging trabeculae. Traditionally, this is treated with closed reamed exchange nailing which increased construct stiffness with a larger diameter nail, improved isthmic fit, and extrusion of reaming contents to the nonunion site. However, studies have demonstrated a higher union rate with open plate augmentation, bone grafting, and nail retention. This is due to the ability to correct nonunion site deformity, provide added compression at the nonunion site, and increase fracture site biology with bone graft.
Lynch et al. reviewed the literature regarding the treatment options for femoral nonunions. The literature suggests high union rates when hypertrophic nonunions are treated with exchanged reamed nailing. However, the use of augmentative plate fixation allows for further deformity correction. The proposed mechanism by which exchange reamed nailing is increased construct stiffness with a large diameter nail, usually by 1-2 mm, increased isthmic fit, and autogenous bone graft extrusion into the nonunion site.
Somford et al. performed a systematic review of the surgical treatment of femoral nonunions. Results demonstrate that exchange nailing provides a 73% union rate compared to plate augmentation of 96%. They speculated that there were increased indications for exchange nailing for oligotrophic nonunions in many of the included studies, which may have reduced the union rate. Further, plate augmentation does allow for deformity correction, which can further improve the union rate.
Figures A and B are the AP and lateral radiographs of the femur with hypertrophic nonunion as suggested with the abundant callus formation and broken distal interlock screws. Illustration A and B are the AP and lateral radiographs of the distal femur subsequent plate augmentation and fracture healing.
Incorrect Answers:

OrthoCash 2020
A 25-year-old male sustains the injury depicted in Figure A. He is splinted in the field, but on arrival to the emergency room, he complains of painful "tightness" around the leg and severe uncontrolled pain despite maximum dose narcotics. His pain is exacerbated when the toes and ankle are passively stretched in flexion and extension. What is the most appropriate next step in treatment?

External fixation with serial doppler examinations
Intramedullary nailing
Open reduction internal fixation using plates and screws
Immediate 2-compartment fasciotomies and external fixation
Immediate 4-compartment fasciotomies and external fixation Corrent answer: 5
This patient has clinical symptoms and signs of leg compartment syndrome and should undergo immediate fasciotomies of all 4 leg compartments, followed by external fixation for fracture stabilization.
Tibial fractures are among the most common reasons for compartment syndromes of the leg. A clinical assessment is key in the diagnosis of acute compartment syndrome. If there is uncertainty, intracompartmental pressure measurement has been advocated to help confirm the diagnosis. An absolute
compartment pressure >30 mm Hg or a difference in diastolic pressure and compartment pressure (delta p) <30 mmHg may help to confirm the necessity for fasciotomy.
McQueen et al. published a report of 25 patients with tibial diaphyseal fractures which had been complicated by an acute compartment syndrome. They reported significant differences in any sequelae of acute compartment syndrome between patients who underwent compartment pressure monitoring and those who had not. They recommended that all patients with tibial fractures should have continuous compartment monitoring to minimize the incidence of acute compartment syndrome.
Mawhinney et al. reported on three cases of tibial compartment syndrome after closed intramedullary nailing of the tibia. They reported that the only predisposing factors for the development of compartment syndrome were the surgery and the fracture itself. They concluded that tibial compartment syndrome is a relatively rare but significant complication of tibial nailing.
Figure A is an AP and lateral radiograph of the leg with displaced, comminuted middle third tibia and fibula fractures.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male is brought to the ED after an MVC. He is found to have a closed comminuted segmental fibula fracture after a prolonged extraction from the vehicle. Several hours after arrival, the patient reports increasing pain and is noted to have an exacerbation of his pain with passive stretching of the ankle. He has a heart rate of 103 and a blood pressure of 141/87. Compartment pressures are obtained and are 27 mmHg in the anterior compartment, 47 mmHg in the lateral compartment, 28 mmHg in the superficial posterior compartment, and 27 mmHg in the deep posterior compartment. Which of the following correctly describes the initial pathophysiology of compartment syndrome and the neurologic deficit that would likely occur in this patient if left untreated?
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased arterial inflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Decreased arterial inflow; inability to dorsiflex his ankle
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the first webspace
Decreased venous outflow; decreased sensation on the dorsum of his foot involving the hallux, 3rd, and 4th toes
Compartment syndrome initially results from a decrease in venous outflow relative to arterial inflow. This patient has elevated pressures in the lateral compartment of the leg, which is where the superficial peroneal nerve runs to supply sensation to the dorsum of the foot including the hallux and 3rd and 4th toes.
Compartment syndrome results from compromised venous outflow from the leg relative to the arterial inflow. This venous congestion leads to elevated compartment pressures that ultimately lead to compromised arterial inflow without compartment release. There are 4 compartments in the leg: anterior, lateral, superficial posterior, and deep posterior. The anterior compartment contains the deep peroneal nerve, the lateral compartment of the leg contains the superficial peroneal nerve, and the deep posterior compartment contains the tibial nerve.
McQueen et al. performed a study to determine risk factors for acute compartment syndrome. They found that young patients, especially men, were most at risk of acute compartment syndrome after injury. They recommend that, when treating such injured patients, the diagnosis should be made early, utilizing measurements of tissue pressure.
Olson et al. published a review on acute compartment syndrome in lower extremity musculoskeletal trauma. They reported that acute compartment syndrome is a potentially devastating condition in which the pressure within an osseofascial compartment rises to a level that decreases the perfusion gradient across tissue capillary beds, leading to cellular anoxia, muscle ischemia, and death. They report that recognizing compartment syndromes requires having and maintaining a high index of suspicion, performing serial examinations in patients at risk, and carefully documenting changes over time.
Illustration A is a diagram depicting the compartments of the leg and its contents.
Incorrect Answers:

OrthoCash 2020
Which of the following amputations results in an approximate 40% increase in energy expenditure for ambulation?
Syme
Traumatic transtibial
Vascular transtibial
Traumatic transfemoral
Vascular transfemoral
The energy expenditure of a vascular transtibial amputation is approximately 40% greater.
The energy expenditure for ambulation increases with lower extremity amputation. Diabetics and vasculopathic patients who undergo amputation
have significantly increased energy requirements compared with nondiabetic patients undergoing amputations for trauma. The metabolic cost for a vascular transtibial amputation is 40% compared to a 25% increase in normal patients who sustain a traumatic amputation.
Huang et al. used a mobile instrument system to measure energy consumption by indirect calorimetry at rest and during ambulation in 25 unimpaired subjects, 6 unilateral below-knee (BK) amputee patients, 6 unilateral above-knee (AK) amputee patients and 4 bilateral AK amputee patients. They found that in comparison to unimpaired subjects, the mean oxygen consumption was 9% higher in unilateral BK amputee patients, 49% higher in unilateral AK amputee patients and 280% higher in bilateral AK amputee patients.
Pinzur et al. performed a study to measure cardiac function and oxygen consumption in 25 patients who underwent amputation for peripheral vascular disease (PVD), and in five similarly aged control patients without PVD. They found Normal walking speed and cadence decreased and oxygen consumption per meter walked increased with more proximal amputation. They conclude that peripheral vascular insufficiency amputees function at a level approaching their maximum functional capacity and more proximal amputation levels, the capacity to walk short or long distances is greatly impaired.
Incorrect Answers:
OrthoCash 2020
A 25-year-old man sustains the injury shown in Figures A-C. What is the primary advantage of using a trochanteric flip osteotomy (TFO) in treating this injury?

It may be performed in a minimally invasive manner
It involves minimal soft tissue stripping
It leads to higher union rates
It allows the surgeon to address all sites of injury through one approach
This patient has sustained a right hip fracture-dislocation with fractures of the femoral head and posterior wall. The TFO allows the surgeon to address all sites of injury through a single approach.
Femoral head fracture-dislocations are a result of high-energy trauma. Treatment ranges from closed reduction and conservative management to total hip arthroplasty. Intermediate options include open reduction and internal fixation or excision of fracture fragments. Complications of this injury include post-traumatic hip arthritis, avascular necrosis, and heterotopic ossification.
The injury is further complicated when a fracture of the acetabulum is concomitantly present. There has been no consensus treatment on this injury constellation as it presents quite rarely. The TFO is one approach that allows the surgeon to treat and stabilize both injuries concurrently. It should be noted that a surgical hip dislocation is performed in conjunction with the TFO to allow access to the femoral head.
Solberg et al. performed a retrospective study of patients sustaining Pipkin IV fracture/dislocations with a TFO. They had 12 patients over a 6 month period. They found that all patients healed radiologically and one patient developed osteonecrosis. 10 out of 12 patients had good to excellent outcomes. They concluded that using a surgical protocol with TFO rendered clinical results
comparable to previously reported outcomes in a series of isolated femoral head fractures.
Giannoudis et al. performed a systematic review to investigate data regarding femoral head fractures, particularly focusing on their management, complications and clinical results. They reported that fracture-dislocations were managed with emergent closed reduction, followed by definite treatment, aiming at an anatomic restoration of both fracture and joint incongruity. They concluded that neither the TFO nor an anterior approach seems to endanger femoral head blood supply compared to the posterior one, with the TFO possibly providing better long-term functional results and lower incidence of major complication rates.
Henle et al. reported on the result of 12 patients of femoral head fractures with associated posterior wall fractures treated with a TFO. They found good to excellent results in 10 patients. The two patients with poor outcome developed avascular necrosis of the femoral head and underwent total hip arthroplasty.
Heterotopic ossification was seen in five patients. They concluded that the TFO may lead to favorable outcomes in this injury constellation.
Figure A is an AP radiograph of the right hip demonstrating a femoral head fracture-dislocation. Figure B is an axial CT image demonstrating a posterior wall fracture. Figure C is an axial CT image demonstrating a femoral head fragment within the acetabulum. Illustration A is the Pipkin classification of femoral head fractures: Type I is below the fovea, Type II is above the fovea, Type III is associated with a femoral neck fracture, and Type IV is associated with an acetabular fracture.
Incorrect Answers:

OrthoCash 2020
A 30-year-old male is brought to your emergency department following a motor vehicle collision at high speed. He is intubated in the field for airway protection but is hemodynamically stable. Subsequent workup shows a displaced acetabular fracture, in addition to an intracranial bleed and liver laceration which do not require surgery. When placing an antegrade anterior column screw, what radiographic view should be used to avoid intra-pelvic screw penetration?
Iliac oblique view with hip and knee flexed
Iliac oblique inlet view
Obturator oblique view with hip and knee flexed
Obturator oblique outlet view
Obturator oblique inlet view Corrent answer: 2
The iliac oblique inlet view will best show the the anterior-posterior placement of an anterior column ramus screw.
Percutaneous and limited-open acetabular fixation is becoming increasingly common as it avoids the morbidity of extensile pelvic dissection and allows early mobilization. However, it relies heavily on a mastery of radiographic landmarks and ability to interpret these images to reduce fracture fragments without direct visualization. Slight deviations of the fluoroscopy beam and/or fracture displacement will distort the radiographic image. Without a facile ability to interpret these and make appropriate adjustments, percutaneous fixation will be extremely onerous.
Starr et al. described their early techniques for percutaneous and limited-open acetabular fixation. They first implemented this for minimally displaced fracture patterns but have expanded these to a wider range of pathology. They cite the benefit of earlier mobilization in the poly-traumatized patient as great use for this technique.
Mauffrey et al. reviewed radiograph utilization during acetabular fracture care. Though CT has added tremendously to demonstrating subtleties of acetabular fractures, they state the use of AP and orthogonal iliac and obturator oblique Judet views cannot be overlooked. Interpreting these radiographs allows the surgeon to recreate 2-dimensional images into a 3-dimensional fracture pattern and better understand the character of the injury.
Illustrations A and B demonstrate the iliac oblique inlet view and obturator oblique outlet views, respectively.
Illustration C demonstrates the relationship of the critical structures at risk of injury during anterior column screw placement. Illustrations D and E show the starting point with screw trajectory, and position of the hip during posterior column screw.
Incorrect Answers:
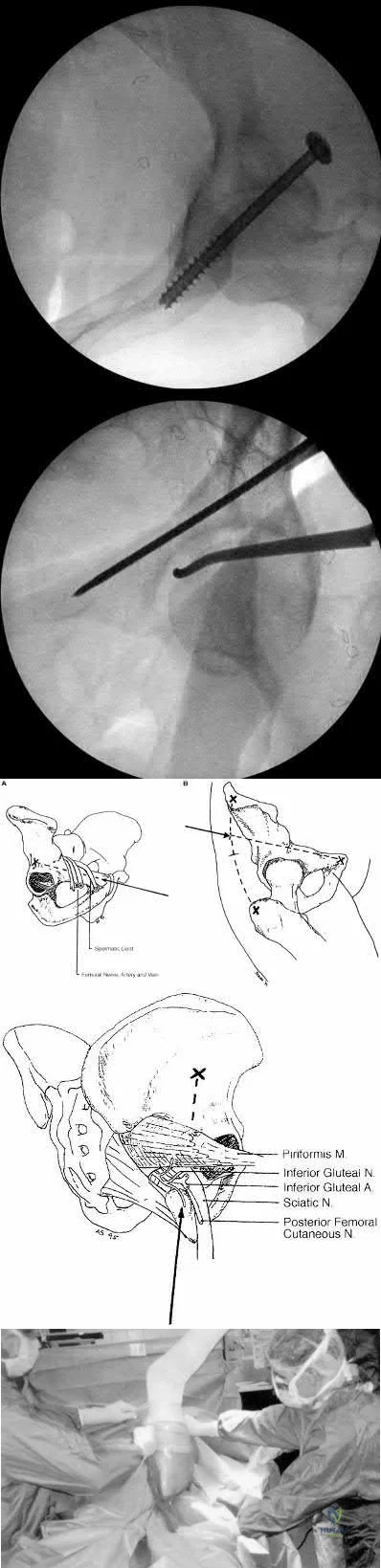
OrthoCash 2020
A 34-year-old male sustains the injury shown in Figures A and B. Which factor has been found to be elevated in the synovial fluid and contributes to post-traumatic arthritis?
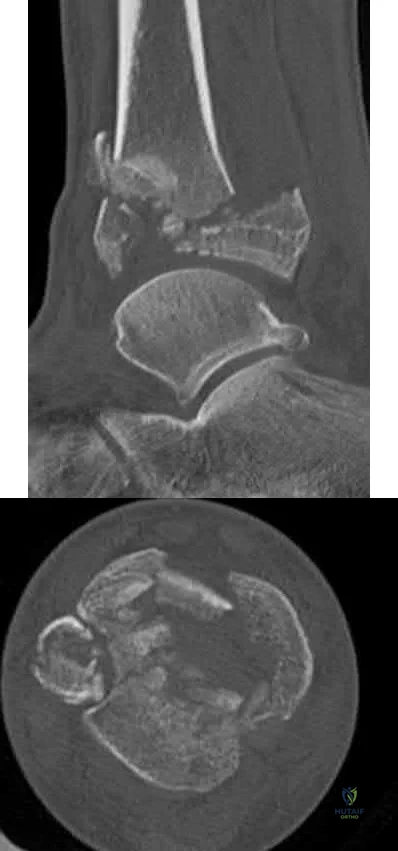
TGF-Beta
RANKL
IL-2
IL-6
cAMP
The patient has sustained a tibial plafond or pilon fracture as depicted in Figures A and B. IL-6 is one of many inflammatory molecules that has been found to be elevated in the synovial fluid following an intra-articular ankle fracture.
Post-traumatic arthritis following intra-articular fractures is a known complication. It commonly appears 1-2 years following injury and is related to chondrocyte death at the margins. There has not been shown to be any association between prolonged non-weight bearing, poor patient compliance with weight-bearing restrictions, and hardware reactions with the development of post-traumatic arthritis. However, literature has shown that the inflammatory molecules present in the synovial fluid can have a significant effect on the development of posttraumatic arthritis. Important inflammatory factors that have been found to be elevated include IL-6, IL-8, MMP-1, MMP-2, MMP-3, MMP-9 and MMP-10.
Adams et al. looked at the synovial fluid of 21 patients with an intra-articular ankle fracture and used the un-injured ankle as a control. They found the inflammatory molecules of GM-CSF, IL-10, IL-1 beta, IL-6, IL-8, IL-10, IL-12p70, TNF-alpha, MMP-1, MMP-2, MMP-3, MMP-9, MMP-10 were all elevated. They concluded that these inflammatory molecules may play a role in posttraumatic arthritis development.
Adams et al. looked at the synovial fluid of 7 patients from his previous 21 patients that had intra-articular ankle fractures. They found that IL-6, IL-8, MMP-1, MMP-2, and MMP-3 were significantly elevated in comparison to the uninjured ankle. They concluded that the sustained elevated intra-articular inflammatory environment is a potential contributor to post-traumatic arthritis.
Figures A and B are sagittal and axial CT slices, respectively, that depict a tibial plafond or pilon fracture.
Incorrect Answers:
immune system.
OrthoCash 2020
A 29-year-old female presents to the trauma bay from the scene of a high-speed motor vehicle accident. She is found to have a closed intraarticular distal radius fracture with a concomitant ulnar styloid base fracture. She subsequently undergoes ORIF of the distal radius fracture with a volar locking plate. The ulnar styloid fracture is not addressed. Which of the following, if present, is least likely to affect functional outcomes?
Ulnar styloid nonunion
DRUJ instability
Articular step-off >3mm
Radial shortening
Workers compensation claim Corrent answer: 1
Ulnar styloid non-unions do not affect the overall outcome of hand or wrist function following ORIF of distal radius fractures.
Ulnar styloid base fractures can be associated with DRUJ disruption and TFCC rupture. The DRUJ should be independently evaluated following ORIF of the distal radius. Without instability, unlar styloid fractures do not need to be addressed. If instability exists, the DRUJ should be treated as a separate entity, typically cross-pinned using k-wires. The result of ulnar styloid nonunions are inconsequential to the overall outcome of patients undergoing distal radius ORIF.
Daneshvar et al review the effects of ulnar styloid fractures on patients sustaining distal radius fractures. They report that patients with a concomitant ulnar styloid fracture had a slower recovery of wrist flexion and grip strength compared to those with an isolated distal radius fracture. They conclude, however, that even the presence of an ulnar styloid nonunion did not significantly affect outcomes.
Buijze et al review the clinical impact of united versus non-united fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. They report no difference in motion, strength or outcome scores
between the united and non-united groups at 6 months follow up. They conclude that nonunion of the ulnar styloid does not have an effect on the overall outcome of hand or wrist function.
Incorrect Answers:
OrthoCash 2020
Which of the following proximal humerus fractures has the highest likelihood of developing humeral head ischemia?

Posteromedial calcar length of the humeral head less than 8 mm and a loss of medial hinge are among the most reliable predictors of ischemia in the surgical management of humeral head fractures.
Proximal humerus fractures are classified based on the Neer classification, in which 4 parts are described: greater tuberosity, lesser tuberosity, articular surface, and the shaft. A fragment is considered a part if it is greater than 45 degrees angulated or displaced >1cm. The posterior humeral circumflex artery is the main blood supply to the humeral head. Following ORIF, humeral head ischemia may occur and is associated with the initial fracture pattern. Several factors including <8mm of calcar length attached to the articular segment, disruption of the medial hinge, displacement >10mm and angulation >45 degrees have been associated with a disruption of the vascular supply to the humeral head.
Campochiaro et al review Hertel’s criteria of calcar length and medial hinge integrity and its reliability in predicting humeral head necrosis. They reported a 3.7% incidence of ischemia across all 267 fractures evaluated. In those patients that developed AVN, 30% had all of the predictors described by Hertel, however, in the non-AVN group, only 4.7% had these same findings.
They concluded that while Hertel’s criteria are helpful, they may not be sufficient and the authors recommended 3-dimensional evaluation of any fracture involving the calcar.
Xu et al reviewed avascular necrosis in patients with proximal humerus fractures who were treated surgically. They reported on 291 patients throughout 7 studies in which there was no difference in the incidence of AVN for those treated surgically or nonoperatively. However, they concluded through subgroup analysis looking at different fixation constructs that, plate fixation specifically was associated with a higher risk of AVN than conservative management of proximal humerus fractures.
Figure A demonstrates a proximal humerus fracture with a medial calcar length of >8mm attached to the articular segment. Figure B is a proximal humerus fracture with a displaced greater tuberosity fragment. Figure C demonstrates a proximal humerus fracture with a medial calcar length of <8mm attached to the articular segment. Figure D is a displaced metadiaphyseal proximal humerus fracture in a skeletally immature patient. Figure E is a radiograph of a metadiaphyseal proximal humerus fracture in a skeletally mature patient with a medial calcar length >8mm.
Incorrect Answers:
OrthoCash 2020
A 34-year-old man presents with the closed injury depicted in Figure A after a high energy twisting injury. Which of the other injuries below is most commonly associated with his known injury?

Nondisplaced medial malleolus vertical shear fracture
Nondisplaced Volkmann's fragment
Nondisplaced Chaput's fragment
Nondisplaced lateral wall talar fracture
Posterior inferior tibiofibular ligament disruption Corrent answer: 2
This patient has sustained a distal third tibial shaft spiral fracture, which is commonly associated with nondisplaced posterior tibial plafond fractures, with the classic Volkmann's fragment.
Prior to operative management, distal third spiral tibial shaft fractures should always be evaluated for intra-articular extension. As this commonly associated injury can be missed on plain radiographs, an ankle CT is often recommended. This is especially important when intramedullary fixation is used for definitive management of the tibial shaft fracture, as nail insertion can displace a
previously nondisplaced intraarticular fracture. Anterior to posterior lag screw fixation prior to nailing may be useful in these cases.
Sobol et al. investigated the incidence of concomitant posterior malleolar fractures (PMFs) in operative distal third spiral tibial shaft fractures. They reported that spiral distal third tibial shaft fractures were identified with an ipsilateral posterior malleolus fracture in 92.3% of cases. They recommended a preoperative ankle CT in all cases with this specific fracture morphology to properly diagnose this commonly associated injury.
Hou et al. investigated the posterior malleolar fracture association with spiral tibial shaft fractures. They reported that plain radiography (both preoperative and intraoperative) resulted in rare identification of these associated injuries, which resulted in missed injuries. They concluded that a CT or MRI ankle may be a higher yield method to detect these injuries.
Figure A demonstrates a distal third spiral tibial shaft fracture. Illustration A is a schematic demonstrating the Volkmann, Chaput, and medial malleoli intraarticular fragments of the distal tibia.
Incorrect Answers:
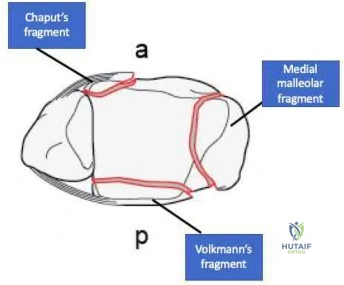
OrthoCash 2020
An 18-year-old male is admitted for a diaphyseal, open, tibial shaft fracture after falling off a motorcycle. He has a past medical history of nicotine dependence and obesity. He undergoes provisional splinting by the resident on call and is noted to be "neurovascularly intact" following splint placement. Throughout the evening, however, the patient has an increasing narcotic requirement and develops pain with passive stretch of his toes. What factor listed below is most associated with his progressive symptoms overnight?
Age < 20
Male gender
Body mass index >/ 30 kg/m^2
Open fracture
Nicotine use
The highest prevalence of compartment syndrome is found in patients aged 12-19 years, followed by 20-29 years.
One theory for the higher prevalence of compartment syndrome in younger patients is increased muscle mass in this cohort. If there is more muscle in a compartment, there is less room for swelling. On the flip side, elderly or deconditioned patients who have less muscle or fatty atrophy may be better able to accommodate muscle swelling. Additionally, a diaphyseal fracture location is associated with a higher risk of compartment syndrome. Again, this may be due to the fact that there is more muscle than tendon, and thus more swelling, in the proximal leg.
Shadgan et al. retrospectively reviewed 1,125 patients with diaphyseal tibia fractures to look for risk factors associated with the development of compartment syndrome. Compartment syndrome occurred in approximately 8% of patients with this injury. They concluded that younger patients were at a higher risk of developing compartment syndrome and that male gender, open fracture, and intramedullary nailing were not risk factors.
Beebe et al. set out to determine the correlation between the OTA/AO classification of tibia fractures and the development of compartment syndrome. they conducted a retrospective review of a prospectively collected database comprising 2,885 fractures. They concluded that age, sex, and the OTA/AO classification were highly predictive for the development of compartment syndrome in this cohort.
McQueen et al. similarly looked at predictors of compartment syndrome after tibial fractures in a retrospective cohort study. There were 1,388 patients in their study with ages ranging from 12-98; identical to the Shadgan study, 69% of patients were male. They concluded the strongest risk factor was age, with the highest prevalence in 12 to 19-year-olds.
Park et al. additionally analyzed 414 patients with tibia fractures in a retrospective cohort study. The main outcome measure of this study was the rate of clinically determined compartment syndromes requiring fasciotomy by anatomic region. The found that diaphyseal fractures were more frequently associated with the development of compartment syndrome than proximal (next most common site) and distal tibia fractures, specifically in younger patients.
Incorrect Answers:
OrthoCash 2020
Figure A is the radiograph of a 79-year-old female with elbow pain following a fall. Compared with a total elbow artrhoplasty, open reduction and internal fixation would most likely result in?

Greater Mayo Elbow Performance Score
Greater Disabilities of the Arm, Shoulder and Hand Score
Increased flexion-extension arc
Increased reoperation rate
Decreased complication rate Corrent answer: 4
This patient sustained a comminuted distal humerus fracture. Open reduction and internal fixation (ORIF) is found to have higher repoeration rates compared with total elbow arthroplasty (TEA) in the elderly: 27% versus 12%, respectively.
Distal humerus fractures account for approximately 30% of elbow fractures. There is often a low energy mechanism of injury in the elderly patient. While ORIF and TEA may be utilized in bicolumnar distal humerus fractures in the elderly patient, recent literature has demonstrated favorable outcomes with TEA in this aged cohort. TEA is indicated in the low demand osteoporotic patients with bicolumnar distal humerus fractures that are not amendable to ORIF. Utilization of TEA has demonstrated greater functional outcome scores, greater motion, less complications, and a lower revision rate.
Mckee et al. conducted a prospective, randomized, controlled trial comparing functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with ORIF or primary semiconstrained TEA. They reports that patients who underwent TEA had significantly better motion, performance and outcome scores, lower reoperation rates compared with the ORIF group. They concluded that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF and that TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation.
Githens et al. performed a systematic review and meta-analysis to analyze outcomes and complication rates in elderly patients with intra-articular distal humerus fractures being treated with either TEA or ORIF with locking plates. They report that TEA and ORIF for the treatment of geriatric distal humerus fractures produced similar functional outcome scores and range of motion.
However, they found a non-statistical trend toward a higher rate of major complications and reoperation after ORIF. They conclude that the quality of study methodology was generally weak and ongoing research including prospective trials and cost analysis is indicated.
Figure A is the AP radiograph of a comminuted bicolumnar distal humerus
fracture. Illustration A are the radiographs of a comminuted distal humerus fracture in an elderly patient treated with a TEA. Illustration B is the postoperative radiographs of a comminuted distal humerus fracture treated with ORIF.
Incorrect Answers:

OrthoCash 2020
Figure A is the postoperative radiograph of an 82-year-old female who was treated with a cephalomedually nail for a left intertrochanteric hip fracture. Which of the following is the most common complication following use of this device?

Anterior perforation of distal femur
Breakage of the screw
Implant cutout
Malunion
Nonunion
Intertrochanteric hip fractures are most commonly treated with a cephalomedullary nail. The most common complication following utilization of a cephalomedullary nail is implant failure and cutout.
Intertrochanteric hip fractures are extra-capsular injuries that are common in the elderly osteoporotic patient. These injuries carrry a 20-30% mortality rate in the first year following fracture. Femoral cephalomedullary nails are often used to treat these injuries. Often a helical blade or screw may be used to provide fixation within the femoral neck. Overall, the most common complication following use of this device is implant failure and cutout, which occurs most commonly within 3 months following surgery. A known risk factor of this complication is an increased tip-apex distance, with a 60% failure rate reported with a distance exceeding 45mm.
Gardner et al. reviewed the use of a helical blade device to stabilize
intertrochanteric hip fractures. They reported a mean telescoping in unstable and stable fractures of 4.3 mm and 2.6 mm, respectively. They also found that blade migration within the femoral head averaged 2.2 mm overall, with no difference between stable and unstable fractures. They concluded that position changes occurred within the first 6 weeks postoperatively, with no subsequent detectable migration or telescoping.
Haidukewych et al. reviewed patients with failed internal fixation of a hip fracture. They report that salvage options are dependent on the anatomic site of the nonunion, the quality of the remaining bone and articular surface, and patient factors such as age and activity level. They conclude that in younger patients with either a femoral neck or intertrochanteric fracture nonunion with a satisfactory hip joint, treatment typically involves revision internal fixation with or without osteotomy or bone grafting. Conversely, in older patients with poor remaining proximal bone stock or a badly damaged hip joint, conversion to hip arthroplasty is recommended.
Figure A is the AP radiograph of the right hip treated with a cephalomedullary nail. Illustration A demonstrates screw cutout.
Incorrect Answers:

OrthoCash 2020
Figure A is the radiograph of a 42-year-old female who presents to the trauma bay following a motor vehicle collision. She subsequently undergoes ORIF through a posterior approach. Iatrogenic injury to which nerve in Figure B is most likely with this approach?
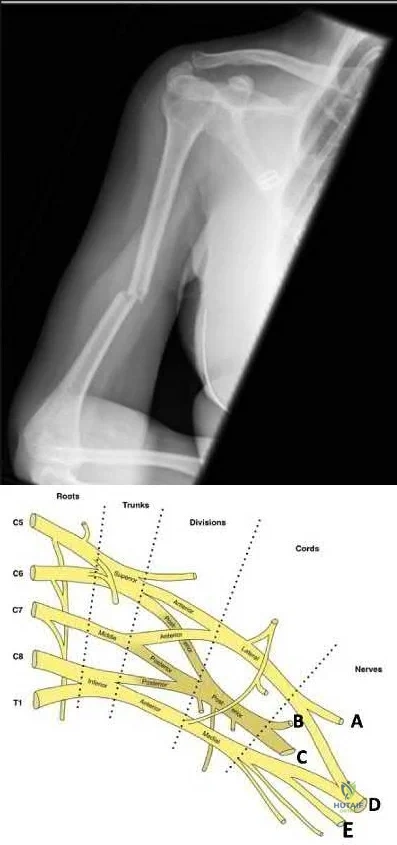
Question 81
- What is the primary immediate source of energy for muscle?
Explanation
Almost 90% of the total ATP formed by glucose metabolism is formed during oxidative phosphorylation. This is accomplished by a series of enzymatically catalyzed reactions in the mitochondria. When the body’s stores of carbohydrates decrease below normal, glucose can be formed from the breakdown of protein and fat via gluconeogenesis to yield more ATP.
Question 82
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?
Explanation
REFERENCE: Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 1057-1061.
Question 83
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 84
Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment? Review Topic
Explanation
patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20% of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid. Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss.
Incorrect Answers:
Question 85
Figures 233a through 233c are the radiographs and biopsy specimen of a 32-year-old woman who has had progressive ankle pain for 6 months. What is the most appropriate treatment option?

Explanation

Question 86
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
Question 87
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of
Explanation
the fracture.
REFERENCES: Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Banks AS, Cain TD, Ruch JA: Physeal fractures of the distal phalanx of the hallux. J Am Podiatr Med Assoc 1988;78:310-313.
Question 88
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
corrective osteotomy.
REFERENCES: O’Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369.
Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Spinner RJ, O’Driscoll SW, Davids JR, et al: Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg 1999;24:718-726.
Question 89
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
REFERENCE: Burkus JK, Gornet MF, Dickman CA, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 2002;15:337-349.
Question 90
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10° of residual dorsal tilt. What is the next step in management?
Explanation
REFERENCES: Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210.
McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417.
Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Roy DR: Completely displaced distal radius fractures with intact ulnas in children. Orthopedics 1989;12:1089-1092.
Question 91
03 A 64 year old man who underwent revision total knee arthroplasty 6 months ago has leg pain after walking. AP and lateral radiographs are shown in Figures 39a and 39b. The cause of pain is most likely related to

Explanation
back to this question next question
Question 92
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 93
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
Explanation
inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus
7% for infection and 7% for rotator cuff tearing.
Question 94
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 95
The fracture shown in Figure 32 is strongly indicative of what diagnosis?
Explanation
REFERENCES: Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Kleinman PK, Marks SC, Blackbourne B: The metaphyseal lesion in abused infants: A radiologic-histopathologic study. Am J Roentgenol 1986;146:895-905.
Question 96
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the most likely area of injury?
Explanation
Question 97
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Morrey BF, Adams RA: Capitellocondylar total elbow replacement in rheumatoid arthritis. J Bone Joint Surg Am 1992;74:479-490.
Question 98
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 99
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
Explanation
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
Sclerosis of the proximal femoral epiphysis with subchondral lucency
Abnormal femoral head-neck junction offset
Widening of the proximal femoral physis with normal femoral head-neck junction offset
Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
Question 100
Which of the following muscles has dual innervation?
Explanation
REFERENCE: Mahakkanukrauh P, Somsarp V: Dual innervation of the brachialis muscle.
Clin Anat 2002;15:206-209.
