Orthopedic Board Review MCQs: Hip, Shoulder & Spine Surgery | Part 115

Key Takeaway
This page offers Part 115 of a comprehensive orthopedic surgery board review. It features 100 verified, high-yield MCQs mirroring OITE and AAOS exam formats, focusing on Hip, Shoulder, and Spine. Designed for orthopedic residents and surgeons, it's an essential tool for board certification exam preparation, enhancing clinical knowledge.
About This Board Review Set
This is Part 115 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 115
This module focuses heavily on: Hip, Shoulder, Spine.
Sample Questions from This Set
Sample Question 1: Thoracic disk herniations most typically occur at what level of the thoracic spine? Review Topic...
Sample Question 2: A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh...
Sample Question 3: A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and...
Sample Question 4: A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm P 3 P . What is the m...
Sample Question 5: An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Thoracic disk herniations most typically occur at what level of the thoracic spine? Review Topic
Explanation
Question 2
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
REFERENCES: Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Morrissy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 579-624.
Question 3
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and

Explanation
Question 4
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm P 3 P . What is the most common organism in this scenario?
Explanation
REFERENCES: Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Mills WJ, Mosca VS, Nizet V: Orthopaedic manifestations of invasive group A streptococcal infections complicating primary varicella. J Pediatr Orthop 1996;16:522-528.
Question 5
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 6
Which examination finding points toward a brachial plexus injury rather than root avulsion?
Explanation
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus injury.
Question 7
Figure 92 is the radiograph of a 45-year-old man who was thrown from his horse and now reports groin pain. Which of the following is the most common long-term sequelae of this injury?

Explanation
Question 8
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?
Explanation
REFERENCE: Gerber C, Myer DC, Schneeberger AG, et al: Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: An experimental study in sheep. J Bone Joint Surg Am 2004;86:1973-1982.
Question 9
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 10
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?
Explanation
REFERENCES: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lee JK, Yao L: Stress fractures: MR imaging. Radiology 1988;169:217-220.
Question 11
Figures below show the radiograph and the MRI scan obtained from a 37-year-old woman with a 2-month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
Question 12
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
Explanation
REFERENCES: Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Uribe J, Moza K, Jimenez O, et al: Delayed postoperative spinal epidural hematomas. Spine J 2003;3:125-129.
Question 13
A patient sustains a severe lower extremity injury. What can be said about his outcome at 2 years if he chooses reconstruction over amputation?

Explanation
Bosse et al found that at 2 years the SIP score and return to work were not statistically signficantly different between amputation and reconstruction groups. Reconstruction patients had a higher risk of rehospitalization. The psychosocial subscale of SIP did not improve with time. Risk factors for poorer SIP score were: rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), smoking, and involvement in disability-compensation litigation.
MacKenize et al evaluated factors influential in returning to work (RTW) after severe lower extremity injury. Characteristics that correlated with higher rates of RTW included younger age, higher education, higher income, the presence of strong social support, and employment in a white-collar job that was not physically demanding. Receipt of disability compensation had a strong negative effect on RTW.
Question 14
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 15
In the absence of developmental dysplasia of the hip, what is the most common cause of osteoarthritis? Review Topic
Explanation
Question 16
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
Explanation
Question 17
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?
Explanation
REFERENCES: Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45.
Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Lins RE, Simovitch RW, Waters PM: Pediatric elbow trauma. Orthop Clin North Am 1999;30:119-132.
Question 18
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. View Abstract at PubMed
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
Question 19
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management?
Explanation
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
Question 20
Staged open reduction and internal fixation with free flap soft tissue reconstruction is the most appropriate definitive treatment method for which of the following tibial injuries?

Explanation
Typically, treatment of Type IIIB tibial shaft fractures should be staged. Initially tetanus prophylaxis, antibiotics with gram negative and positive coverage, and application of an external fixator with repeat I&D’s are employed for immediate fracture care. Plating is usually required in the presence of significant intra-articular fracture involvement.
Incorrect Answers: Typically, proximal third tibia fractures requiring soft tissue coverage can be treated with a gastrocnemius rotation flap and middle third tibia fractures with soft tissue defects can be reliably covered with a soleus rotation flap. Therefore, a free flap is rarely indicated in the proximal and middle tibia.
Question 21
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
Cortical thickening in the region of the lesion
Erosive metaphyseal lesion with loss of cortical integrity
Normal bony anatomy on radiographs
Diffuse articular erosion with loss of joint space
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 22
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 23
A patient undergoes a proximal tibial resection that is reconstructed with a fresh frozen osteoarticular allograft. Eleven months later, the graft is retrieved. Histologically, the articular cartilage and subchondral bone retrieved would be expected to show evidence of
Explanation
REFERENCES: Enneking WF, Campanacci DA: Retrieved human allografts:
A clinicopathological study. J Bone Joint Surg Am 2001;83:971-986.
Enneking WF, Mindell ER: Observations on massive retrieved human allografts.
J Bone Joint Surg Am 1991;73:1123-1142.
Question 24
Plate fixation of olecranon fractures is recommended over tension band wire fixation when
Explanation
Question 25
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? Review Topic

Explanation
Question 26
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?
Explanation
REFERENCES: Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63.
White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
McCarty EC, Mencio GA, Walker LA, Green NE: Ketamine sedation for the reduction of children’s fractures in the emergency department. J Bone Joint Surg Am 2000;82:912-918.
Question 27
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 28
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 29
A 45-year-old recreational tennis player underwent arthroscopic decompression and mini-open repair of a small supraspinatus tendon tear 3 weeks ago after nonsurgical management failed to provide relief. He now has pain, swelling about the wound, erythema, and purulent drainage. The patient is returned to the operating room for irrigation, debridement, and cultures. What is the most common organism causing this infection?
Explanation
REFERENCES: Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Settecerri JJ, Pitner MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5.
Question 30
A 47-year-old male with a history of a Putti-Platt procedure 20 years ago presents with right shoulder pain with decreased range-of-motion. Radiograph is shown in Figure A. What is the most accurate diagnosis? Review Topic

Explanation
Post-stabilization procedure arthritis is thought to occur due to changes in contact loading in the shoulder joint due to fixing the joint in an incongruent posistion. It can be severe and debilitating, and lead to arthroplasty as a salvage procedure. The Putti-Platt procedure involves a division of the subscapularis tendon and anterior capsule, and realignment of the lateral tendon stump and capsule sewn into the anterior glenoid neck capsular insertion. The "pants-over-vest" style of repair is then finished by sewing the medial tendon stump into the tuberosity, so that external rotation is significantly limited by the soft tissue imbrication. There is no coracoid transfer for this stabilization procedure.
Bigliani et al. reported on a series of similar patients who developed arthritis following surgery for recurrent glenohumeral dislocation. Authors have theorized that instability repair may excessively tighten the joint in one direction and cause a fixed subluxation in the direction opposite from the side of repair, leading to severe degenerative arthritis due to inappropriate contact loading. 77% of patients following arthroplasty after post-capsulorrhaphy arthropathy had an excellent or satisfactory outcome, with improved pain and range of motion.
Figure A demonstrates severe osteoarthrosis of the affected shoulder, with significant joint space narrowing, periarticular osteophyte formation, and subchondral sclerosis.
Incorrect Answers:
performed for traumatic dislocation, but the best answer choice for this stem is Answer 2.
Question 31
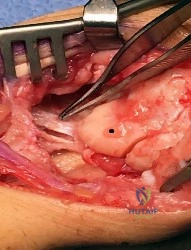
Figure 1 depicts an intraoperative photograph obtained following proximal row carpectomy. The black dot denotes the capitate. The top of the figure is radial and the bottom of the figure is ulnar. Surgical disruption of the structure identified by the forceps would result in
Explanation
The structure identified by the forceps is the radioscaphocapitate ligament. During a proximal row carpectomy, it is very important to identify and protect this ligament. Compromise of the ligament would result in ulnar translocation of the carpus and early failure of the proximal row carpectomy procedure. If the ligament is injured during surgery, immediate repair should be performed. Green and associates discuss the importance of the radioscaphocapitate ligament in stabilizing the carpus after this procedure is performed. Nakamura and associates compared 3-mm, 6-mm, and 10-mm radial styloidectomies, and only the 3-mm styloidectomy subsequently preserved carpal stability. Compromise of the radioscaphocapitate ligament occurred when larger portions of the radial styloid were excised. Distal radioulnar joint instability would result only from the disruption of the distal radioulnar joint stabilizers. Avascular necrosis would not occur, because the capitate receives its blood supply mainly from the palmar vessels. Finally, loss of active thumb IP flexion would not occur, because the flexor pollicis longus tendon would remain intact even if ligament compromise were to occur.
Question 32
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, www.aaos.org/research/guidelines/ PEguide.asp
Question 33
A 45-year-old male presented to the trauma department 10 hours after sustaining a fracture-dislocation of his ankle. The patient underwent an attempted closed reduction of his ankle which can be seen in Figures A and B. The splint was removed, and the appearance of the leg is shown in Figure C. Regarding the best next step in management and the intended goals, which of the following is most accurate?

Explanation
Patients with high-energy periarticular fractures in the lower extremity are at risk for surgical wound complications due to compromised soft tissues. As in this case, joint dislocations can place harmful tension on the skin that leads to blistering and/or skin necrosis. An urgent reduction is indicated, and if it cannot be obtained with a closed manipulation alone, percutaneous or open treatment is indicated. Staged joint-spanning external fixation can both hold a reduction and allow access for skin or wound care prior to a definitive open reduction of an articular fracture. Fracture healing during external fixation occurs by enchondral ossification by way of the relative stability.
Strauss et al. developed a treatment protocol for the treatment of fracture blisters. They used silver sulfadine to minimize soft tissue complications by promoting re-epithelialization. After providone-iodine prep, each blister was unroofed by removing the overlying epithelium of the fracture. Once the blister was unroofed, silver sulfadiazine was applied and covered with dry gauze. They would then perform bid dressing changes. Extremities were deemed operable when skin wrinkles were visible on the overlying skin of the injured extremity.
Anglen et al. in a review of external fixation, report that fractures of the lower extremity are frequently associated with soft tissue trauma that precludes safe surgical treatment in the early period. They present a technique of temporary joint-spanning external fixation which allows stabilization of length and alignment while awaiting resolution of soft tissue swelling. They report no differences between patients who had a temporary external fixator and those who did not with respect to healing time, time to partial or full weight bearing, or clinical score.
Figures A and B demonstrate a pronation-external rotation type fracture with disruption of the syndesmosis. Figure C demonstrates fracture blisters.
Illustration A demonstrates an ankle-spanning external fixator. Illustration B demonstrates skin wrinkling to indicate that the skin is safe to incise.
Incorrect Answers:

OrthoCash 2020
Question 34
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
Explanation
REFERENCES: Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
Wright JL, Nathans AB, Rivara FP, et al: Specific fracture configurations predict sexual and excretory dysfunction in men and women 1 year after pelvic fracture. J Urol 2006;176:1540-1545.
Question 35
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?
Explanation
Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents.
The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve.
REFERENCES: Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Salter RB, Harris WR: Injuries involving the epiphyseal plate. J Bone Joint Surg Am 1963;45:587-622.
Question 36
A 22-year-old man sustained a cervical fracture-dislocation of the C5-6 level in a motor vehicle accident along with an associated spinal cord injury. Six months after his injury, he has 4 out of 5 biceps on the left, with 5 out of 5 biceps on the right. Deltoid is graded at 5 out of 5 bilaterally. There is 0 strength in the triceps, wrist flexors, wrist extensors, and digital extensors. He has neurogenic bowel and bladder with absent perianal sensation and no voluntary motor in the lower extremities. The patient's neurologic deficit is best categorized as which of the following? Review Topic
Explanation
Question 37
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 38
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
REFERENCES: Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000.
Question 39
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 40
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 41
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
REFERENCES: Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998,
pp 724-727.
McDowell GS, Cammisa FP, Eismont FJ: Hyperextension injuries of the cervical spine, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA,
WB Saunders, 1998, pp 372-374.
Question 42
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
Question 43
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time.
REFERENCES: Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.
Question 44
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 45
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis?
Explanation
REFERENCES: Schantz K, Reigels-Nielsen P: The anterior interosseous nerve syndrome.
J Hand Surg Br 1992;17:510-512.
Seror P: Anterior interosseous nerve lesions: Clinical and electrophysiological features. J Bone Joint Surg Br 1996;78:238-241.
Question 46
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 47
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 48
Emergent management of acute tooth displacement (luxation) includes
Explanation
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
Question 49
A patient wakes up with a foot drop following open reduction internal fixation of a posterior wall/posterior column acetabular fracture. What position of the leg causes the highest intraneural pressure in the sciatic nerve?

Explanation
Question 50
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?
Explanation
REFERENCE: Jebson PJ, Engber WD: Proximal row carpectomy. Tech Hand Up Extrem Surg 1999;3:32-36.
Question 51
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 52
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH: Scoliosis in pediatric spinal cord injured patients. J Pediatr Orthop 1990;10:214-218.
Question 53
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Boyd JB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon. J Bone Joint Surg Am 1961;43:1041-1043.
Morrey BF, Askew LJ, An KN, Dobyns JH: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418-421.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 54
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
Explanation
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.
Question 55
03 5.
Explanation
The radiograph here shows the typical Paget’s lesion in the right iliac wing with mixed lytic and sclerotic areas.
Question 56
- A patient who had previously undergone a salvage pelvic (Chiari) osteotomy now requires a total hip arthroplasty. The most frequent complication of this procedure is
Explanation
Question 57
Which of the following best describes heat stroke?
Explanation
[41 degrees C]), central nervous system dysfunction, and cessation of sweating with hot, dry skin. It is a medical emergency that results from failure of the thermoregulatory mechanisms of the body. It has a high death rate and requires rapid reduction in body core temperature. Heat syncope is characterized by a transient loss of consciousness with peripheral vasodilation and decreased cardiac output with normal body temperature. Heat cramps involve painful contractions of large muscle groups because of decreased hydration and a decrease of serum sodium and chloride. Heat exhaustion is distinguished by a core temperature of less than
Question 58
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92?
Explanation
REFERENCES: Vellet AP, Marks PH, Fowler PJ, et al: Occult posttraumatic osteochondral lesions of the knee: Prevalence, classification, and short-term sequelae evaluated with MR imaging. Radiology 1991;178:271-276.
Cone R: Imaging sports-related injuries of the knee, in DeLee J, Drez D, Miller M (eds): DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 2, pp 1595-1652.
Question 59
A 58-year-old male presents after a motor vehicle accident with severe pain and point tenderness over his lumbar spine. He is hemodynamically stable and full neurologic examination reveals no deficits. Radiographs showed no evidence of fracture. A CT was performed and is shown in Figure A. What is the most appropriate treatment of his injury. Review Topic

Explanation
In patients with ankylosing spondylitis (AS), the rigid spine creates a long lever arm that makes even minimally displaced fractures potentially unstable. Thus, despite being minimally displaced in a neurologically intact patient, most fractures in AS warrant a posterior instrumentation and fusion, typically of three levels above and three levels below the fracture.
Caron et al. present a retrospective review of patients with ankylosed spines (due to AS or DISH) and characterize their fractures and outcomes of treatment. Cervical fractures were most common (55%) and rates of occurrence decreased as they progressed down the spine, with lumbar fractures seen only 8% of the time. They found the most common successful surgical intervention was multilevel posterior instrumentation and fusion (with decompression when necessary for neurologic compromise).
Wang et al. reviewed 12 cases of patients with AS who presented with traumatic spinal injuries. They reviewed clinical histories and available imaging. They found that MRI was the most sensitive test for identifying occult fractures of the spine, and recommend using MRI to rule out occult fractures as well as better characterize fractures seen on radiographs or CT imaging for patients with AS.
Werner et al. present a review of spinal fractures in patients with AS. They note that non-operative treatment of these fractures is reserved only for patients who have an unacceptably high risk of undergoing surgery. For three column thoracolumbar fractures they recommend surgical stabilization with a long posterior construct.
Figure A is a sagittal CT image of the lumbar spine with marginal syndesmophytes consistent with AS. The white arrow highlights a minimally displaced fracture that extends through all three columns on the spine. Illustration A are radiographs comparing DISH (on the left) with non-marginal syndesmophytes, and AS (on the right) with marginal syndesmophytes.
Incorrect Answers:
Question 60
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
Lateral femoral circumflex
Medial femoral circumflex
Superior gluteal
Inferior gluteal
Obturator
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419-424.
Question 61
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
REFERENCES: Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Blotter RH, Connolly E, Wasan A, Chapman MW: Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int 1999;20:687-694.
Question 62
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Explanation
Question 63
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 64
Which of the following actions best enhances performance when an athlete is participating in a 10K race?
Explanation
REFERENCES: Newmark SR, Toppo FR, Adams G: Fluid and electrolyte replacement in the ultramarathon runner. Am J Sports Med 1991;19:389-391.
Noakes T: Fluid replacement during marathon running. Clin J Sports Med 2003;13:309-318.
Question 65
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?
Explanation
REFERENCE: Nielson JH, Sallis JG, Potter HG, et al: Correlation of interosseous membrane tears to the level of the fibular fracture. J Orthop Trauma 2004;18:68-74.
Question 66
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 67
A 25 year-old-male sustains a closed injury shown in Figure A. If a tibial intramedullary nail is placed with the starting points shown (arrows), what subsequent alignment will occur?

Explanation
There are several tips and tricks to avoid subsequent deformity following tibial IMN of a proximal third fracture. One way to avoid deformity is to use a more lateral starting point than normal to ensure nail placement in the true center of the canal, which is more lateral when compared to the tibial plateau.
Walker et al. studied 12 cadaveric tibias and inserted a Kirschner wire depending on rotated views of the knee. In order obtain a perfect starting point, a perfect anteroposterior as well as lateral of the knee must be obtained; otherwise, the authors noted that malrotation is bound to occur. With a perfect view, a more lateral starting point correlated with the center of the tibial canal.
McConnell et al. studied cadaveric and subsequent radiographic correlation on a lateral knee x-ray to determine the ideal 'safe zone' for the starting point of a tibial nail. This safe zone is more lateral and posterior, when looking at the axial cut of the plateau.
Figure A exhibits a proximal third tibia fracture with starting points that are not lateral enough, and too distal (on the lateral view), which will result in apex anterior and valgus deformity.
Incorrect answers:
Question 68
Which of the following hip fracture patterns is at increased risk of proximal fragment flexion malreduction with dynamic hip screw fixation?

Explanation
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Question 69
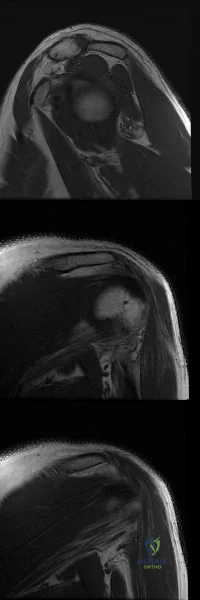
Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervates the affected muscles?
Explanation
Quadrilateral space syndrome is a condition defined by axillary nerve, +/- posterior humeral circumflex artery compression in the quadrilateral space. It most commonly affects the dominant shoulder in overhead movement athletes (e.g. basketball players) or other throwing athletes. Physical examination may reveal weakness with the arm positioned in abduction and external rotation. In situations of long-standing compression, there may also be atrophy of the teres minor and deltoid muscle.
Chafik et al. dissected thirty-one cadaveric human shoulders to describe the neuromuscular anatomy of teres minor. They showed that the primary nerve branch to teres minor travelled in a fascial sling 44 mm medial to the muscular insertion. This
area may be the potential site of greatest compression and tethering of this nerve in patients with isolated teres minor atrophy.
Friend et al. performed a cadaveric dissection of nine shoulder specimens to look at the anatomical variability in course, length and branching pattern of both the teres minor nerve and the axillary nerve. These were compared to a case-based study of these two male patients with isolated atrophy of teres minor. They concluded that there is no good anatomical predictor of nerve compression outside the quadrilateral space as there is considerable anatomical variation in its origin and course, as well as potential site of compression.
Figure A-C are MRI images that show atrophy of the teres minor muscle and possibly deltoid muscle. The rotator cuff muscles are labeled in Illustration A. The teres minor muscle is labeled in Illustration B. Illustration C shows a diagram of the brachial plexus.
Incorrect
1:
This
describes
the
musculocutaneous
nerve.
3:
This
describes
the
suprascapular
nerve.
4:
This
describes
the
long thoracic
nerve.
Question 70
The dominant arterial blood supply to the patella enters at which anatomical location?
Explanation
The arterial blood supply to the patella is made up of branches of six main arteries: the descending genicular, the superior medial and lateral genicular, the inferior medial and lateral genicular, and the anterior genicular. Several of these branches contribute to the anastomotic network that surround the patella. From the ring, there are two main interosseous blood supply systems to enter the patella, known as the midpatellar and polar vessel systems. The distal pole of the patella is considered to be the largest arterial contribution to the peripatellar ring and the polar vessel system.
Lazaro et al. used twenty matched pairs of fresh-frozen cadaveric knees to isolate the dominant blood supply to the patella. After cannulating the superficial femoral artery, anterior tibialis artery, and posterior tibialis artery and performing magnetic resonance imaging, they found that the largest arterial contribution to the patella entered at the inferior pole in 100% of the specimens. In sixteen specimens (80%), the dominant artery entered the medial aspect of the distal pole. In three specimens (15%), it entered the lateral aspect of the distal pole.
Illustation A shows the arterial supply system to the patella. The dominant arterial supply enters at the distal (inferior) pole of the patella, with the dominant geniculate arteries entering inferomedially (labelled with a green star). Illustration B shows an anatomical illustration of the patellar blood supply. Note the dominant distal pole blood supply (arrow).
Incorrect Answers:
Question 71
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 72
Which factor increases the success rate associated with all-inside lateral meniscal repair?
Explanation
Decreased patient age, neutral alignment, and a concomitant ACL tear are associated with improved success rates of meniscal repair. Meniscus tears on the contralateral side of the knee and articular cartilage defects are not associated with improved healing rates.
RESPONSES FOR QUESTIONS 5 THROUGH 6
Physical therapy and a home exercise program
Corticosteroid injection
Arthroscopic debridement
Microfracture
Osteochondral autograft transplantation (OAT)
Match the treatment above with the clinical scenario below
Question 73
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 74
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following? Review Topic
Explanation
Question 75
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
REFERENCES: Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
Gisolfi CV, Duchman SM: Guidelines for optimal replacement beverages for different athletic events. Med Sci Sports Exerc 1992;24:679-687.
Question 76
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 77
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.
Question 78
An 18-year-old man recently underwent an uncomplicated arthroscopic partial medial meniscectomy that was complicated by reflex sympathetic dystrophy (RSD), also termed “sympathetically maintained pain” (SMP). What is the most common finding of this condition?
Explanation
REFERENCES: Lindenfeld TN, Bach BR Jr, Wojtys EM: Reflex sympathetic dystrophy and pain dysfunction in the lower extremity. Instr Course Lect 1997;46:261-268.
O’Brien SJ, Ngeow J, Gibney MA, Warren RF, Fealy S: Reflex sympathetic dystrophy of the knee: Causes, diagnosis, and treatment. Am J Sports Med 1995;23:655-659.
Question 79
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
REFERENCES: Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Campbell DG, Masri BA, Garbuz DS, Duncan CP: Acetabular bone loss during revision total hip replacement: Preoperative investigation and planning, in Zuckerman J (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 43-56.
Question 80
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter “A”?
Explanation
REFERENCES: Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 400, 405, 407, 450.
Question 81
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
Explanation
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006. Question 74
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
Discoid meniscus
Posterolateral comer injury
Vertical meniscal tears
Middle third lateral meniscal tears
Popliteus tendon tears
DISCUSSION: Lateral meniscal cysts often arise from myxoid degeneration that progresses from the meniscal center and then outside the meniscus. Horizontal cleavage tears are commonly associated with the condition.
Cysts of the lateral meniscus are most commonly the consequence of a tear located in the medial third. If the
tear communicates with the joint, arthroscopic partial meniscectomy and cyst decompression are indicated. If the tear does not open into the joint, arthroscopy should be followed by an open cystectomy.
REFERENCES: Hulet C, Souquet D, Alexandre P, et al: Arthroscopic treatment of 105 lateral meniscal cysts with 5-year average follow-up. Arthroscopy 2004;20:831-836.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part I. Macroscopic and histologic findings. Clin Orthop
Relat Res 1980;146:289-300.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part II. Horizontal cleavages and lateral cysts. Clin Orthop Relat Res 1980:146:301-307.
Question 82
A 16-year-old female with adolescent idiopathic scoliosis undergoes posterior spinal fusion with instrumentation. The thoracic pedicle screws were placed using a tap 1 mm smaller than the screw diameter and a straightforward trajectory that runs parallel to the superior endplate. This techniques allows for which of the following: Review Topic
Explanation
Contemporary segmental pedicle screw placement used in the treatment of scoliosis deformity offer significantly higher screw pullout and deformity correction than prior hook and wire constructs. Additionally, screw insertional torque has been found in numerous studies to correlate with resistance to screw pullout. Several factors have been found to increase maximum screw insertional torque, including tapping 1mm smaller than the screw diameter and using the straightforward trajectory. It is important to note that while undertapping makes for a stronger screw, there are some studies that suggest not tapping at all makes for an even stronger screw.
Lehman et al. performed a biomechanical study evaluating maximum insertional torque when tapping line to line, undertapping by 0.5mm, and undertapping by 1mm in 34 fresh frozen cadavers. They found undertapping the thoracic pedicle by 1mm increased maximum insertional torque by 47% when compared to undertapping by 0.5mm and by 93% when compared to line to line tapping.
Kuklo et al. performed a biomechanical study on thirty cadavers using the straightforward technique (sagittal trajectory of the screws parallels the superior endplate of the vertebral body) versus anatomic trajectory (22 degrees in the cephalo-caudad direction in the sagittal plane). They found maximum insertional torque to be
Question 83
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 84
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function. A pathognomonic radiographic feature of this injury is a

Explanation
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 85
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 86
- What is the most important surface geometry design parameter associated with decreased contact stress and wear reduction in total knee prostheses?
Explanation
Question 87
After the athlete undergoes the appropriate treatment of the postsurgical complication and recovers without further incident, which muscle most likely will be last to experience return of function?
Explanation
This patient sustained an eccentric contracture (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest
potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed.
The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared to the 2-incision technique. The most troubling complication for most surgeons is the development of a PIN palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABC nerve injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button.
Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The EIP is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC followed by the ECU, EDQ, and, finally, the EIP.
RESPONSES FOR QUESTIONS 26 THROUGH 27
Anterior tibial artery
Posterior tibial artery
Superficial peroneal nerve
Deep peroneal nerve
Match the neurovascular structure at risk (listed above) with the compartment undergoing fasciotomy (listed below).
Question 88
What medication has been shown to decrease osteolysis after total joint replacement surgery?
Explanation
Aseptic loosening and osteolysis are the primary causes of implant failure in total
joint arthroplasty. Early findings indicate that bisphosphonates upregulate bone morphogenetic protein-2 production and stimulate new bone formation, leading to decreased osteolysis in total joint replacement surgery. While further investigation is required, bisphosphonates may play a future role in improving the long-term duration of joint arthroplasties.
Shanabhag et al. reviewed the use of bisphosphonates and reported that they had the potential to enhance bone ingrowth into implant porosities, prevent bone resorption under adverse conditions, and dramatically extend the long-term durability of joint arthroplasties. They recommended further investigation into the subclasses to determine which ones are most beneficial.
Arabmotlagh el al. performed a prospective study on use of alendronate after total hip arthroplasty. They reported that the alendronate-treated patients had significantly less periprosthetic bone loss on DXA scans after 6 years.
Illustration A shows evidence of osteolysis (arrows) around a total hip arthroplasty. Incorrect Answers:
2-5: These medication classes do not decrease osteolysis after total joint arthroplasty.
Question 89
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?

Explanation
DISCUSSION: A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
Question 90
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 91
A 50-year-old man undergoes revision total knee arthroplasty (TKA). The tibial component shown in Figure 153 was retrieved at the time of revision. The wear damage demonstrated on the backside of the tibial component is most likely related to which wear mechanism(s)?
Explanation
Pitting and delamination seen in tibial component retrievals on the bearing surface of a TKA is related to fatigue wear. Backside wear is shown in the photograph; this is where the lot numbers usually are present, but now they are not distinguishable because of backside wear. This wear mechanism is attributable to adhesive and abrasive wear. The nanometer-size particles created by this wear mechanism account for the higher prevalence of osteolysis associated with modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 154 AND 155
Five weeks ago, an 82-year-old man underwent revision total knee arthroplasty (TKA). Three weeks after surgery he had a dental cleaning. The patient now reports 2 days of worsening pain following a long physical therapy session. His C-reactive protein (CRP) level is 15.0 mg/L (reference range, 0.08-3.1 mg/L). Upon examination, there is no drainage and slight effusion, and he has a passive range of motion to 110 degrees. Radiographs are unremarkable.
Question 92
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
REFERENCES: Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS: DeQuervain’s syndrome: Surgical and anatomical studies of the fibro-osseous canal. Orthopedics 1991;14:545-549.
Question 93
A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability. Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-to-moderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain? Review Topic
Explanation
Question 94
A nonambulatory verbal 6-year-old child with spastic quadriplegic cerebral palsy has progressive bilateral hip subluxation of more than 50%. There is no pain with range of motion, but abduction is limited to 20 degrees maximum. An AP radiograph is seen in Figure 34. Management should consist of
Explanation
REFERENCES: Presedo A, Oh CW, Dabney KY, et al: Soft-tissue releases to treat spastic hip subluxation in children with cerebral palsy. J Bone Joint Surg Am 2005;87:832-841.
Miller F, Bagg MR: Age and migration percentage as risk factors for progression in spastic hip disease. Dev Med Child Neurol 1995;37:449-455.
Question 95
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Olney BW: Tarsal coalition, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 169-181.
Question 96
Figure 13 is the photograph of 18-month-old triplets with a lower-limb condition. What is the best initial treatment? Review Topic

Explanation
(SBQ13PE.56) A 22-month-old female is hospitalized with a fever and malaise. She is found to be bacteremic, and blood cultures grow methicillin-sensitive Staphylococcus aureus (MSSA). During her hospitalization, the pediatrician notices her arm is slightly swollen and appears painful to use. MRI is obtained and demonstrated in figure A. Which feature of the MRI suggests the need for surgical management? Review Topic

Brodie's Abscess
Osteomyelitis of the humeral metaphysis
Subperiosteal abscess of the humerus
Presence of subcutaneous air
High risk of proximal humeral growth arrest
This patient has osteomyelitis of the humerus with a large subperiosteal abscess. The presence of subperiosteal abscess necessitates surgical intervention for irrigation and debridement (I&D).
The diagnosis of acute osteomyelitis in children is made based upon a constellation of findings including pain, systemic signs of infection, elevated serum inflammatory markers, and imaging studies demonstrative of osseous infection. It is most commonly hematogenously spread to the metaphysis of immature bone, which is highly vascular prior to skeletal maturity. Treatment involves obtaining specimen for culture, empiric antibiotic treatment, and surgical irrigation and debridement of known abscesses. The end-point of treatment is return of pain-free functionality and the resolution of local/systemic signs of infection.
Conrad reviewed the management of acute hematogenous osteomyelitis and emphasized that surgical intervention in the presence of abscess can be both therapeutic and diagnostic: I&D can obtain culture and narrow the antibiotic plan.
Jones et. al. reviewed chronic pediatric osteomyelitis and report that surgery is the mainstay of treatment because removal of dead bone is essential for resolution of infection. This may be performed with sequestrectomy and curettage, with an emphasis on prevention of pathologic fracture, growth disturbances, bone loss, joint involvement, and permanent loss of function.
Figure A is a coronal STIR MRI image of the humerus demonstrating osteomyelitis
with extensive subperiosteal abscess.
Incorrect Answers:
Brodie's abscess is a type of subacute osteomyelitis which remains indolent and creates a focal intra-osseous abscess. This is not demonstrated in the clinical image.
The patient does have osteomyelitis of the humeral metaphysis, but this alone is not the indication for surgery. Uncomplicated osteomyelitis may be treated effectively with antibiotics alone.
Presence of subcutaneous air is suggestive of necrotizing fasciitis, which is a surgical emergency. The MRI however does not demonstrate this finding.
The infection and its surgical management both increase risk of injury to the proximal humeral physis and has the potential for growth arrest or angular deformity.
(SBQ13PE.3) Figure A demonstrates a physical examination maneuver in a 1 month old infant. What is this maneuver? Review Topic

Ortolani Test
Barlow Test
Galeazzi Sign
Patrick test
Teratologic Sign
Figure A shows a schematic image of the Ortalani test.
The Ortolani test, or Ortolani maneuver, is part of the physical examination for developmental dysplasia of the hip. It is used alongside the Barlow test to detect subluxated hips that are either reducible or irreducible. A positive sign is a distinctive 'clunk' which can be heard and felt as the femoral head relocates anteriorly into the acetabulum.
Guille et al. showed that the use of Pavlik harness has become the mainstay of initial treatment for the infant who has not yet begun to stand. If concentric reduction of the hip cannot be obtained, surgical reduction of the dislocated hip is the next step before they are able to stand.
Video V is a lecture discussing the hip examination of the infant. Incorrect Answers:
pressure on the knee, directing the force the femoral head posteriorly. A positive Barlow test would result in posterior subluxation/dislocation of the hip. Answer 3: Galeazzi test is performed by flexing an infant's knees in the supine position so that the ankles touch the buttocks. If the knees are not level then the test is positive, which indicates a potential congenital hip issue (e.g. DDH). Answer 4: Patrick or Faber test (flexion, abduction, external rotation) has been described both for stressing the SI joint and for isolating symptoms to the hip Answer 5: Teratologic dislocation of the hip is a term used to imply that the hip joint did not develop normally in utero, thus the hip is in a fixed dislocated position at birth.
Question 97
Figures below depict the AP and lateral radiographs obtained from a 64-year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
Question 98
What is the most common causative bacteria in septic arthritis in children?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, p 2109.
Jackson MA, Nelson JD: Etiology and medical management of acute suppurative bone and joint infections in pediatric patients. J Pediatr Orthop 1982;2:313-323.
Question 99
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129.
Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Thompson JE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309-316.
Question 100
A 75-year-old woman has a 1-year history of right hip pain and a right total hip arthroplasty (THA) performed in 1999. Her left THA, performed in 2002, is asymptomatic. Plain radiographs show that all of the components appear well fixed and in good position. There is evidence of eccentric polyethylene wear of the right hip with focal osteolysis of the calcar and great trochanter (with none of these findings on the left hip). What is the most likely explanation for her right hip pain?
Explanation
This patient likely has 1 conventional polyethylene hip (1999) and 1 hip with highly cross-linked polyethylene (HXLPE) (2002); most centers transitioned to HXLPE around 2001 to 2002. This explains the clear difference in the clinical and radiographic performance of the 2 hips during the second decade. There is clear evidence of decreased wear and osteolysis and clinical benefits (ie, decreased revision rate) during the second decade following the introduction of HXLPE for THA. Acute infection is unlikely considering the chronicity of symptoms. The radiographs show no obvious evidence of cup loosening. A pseudotumor attributable to trunnionosis, while reported, remains an infrequent clinical issue.
