Orthopedic Board Review MCQs: Ankle, Deformity, Fracture & Scoliosis | Part 113
Key Takeaway
This page offers Part 113 of a professional board review quiz for orthopedic residents and surgeons. It features 100 high-yield, verified MCQs specifically designed for OITE, AAOS, and ABOS board certification exam preparation. Utilize study and exam modes with detailed explanations to master core orthopedic concepts.
About This Board Review Set
This is Part 113 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 113
This module focuses heavily on: Ankle, Deformity, Fracture, Scoliosis.
Sample Questions from This Set
Sample Question 1: A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What...
Sample Question 2: -The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the...
Sample Question 3: A teenage female is referred to you for evaluation of curvature in her back that was discovered on routine school screening. She is diagnosed with adolescent idiopathic scoliosis. In which of the following scenarios is a bracing program the...
Sample Question 4: The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:...
Sample Question 5: Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Explanation
REFERENCES: Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: Review of a series of 25 cases. J Pediatr Orthop 1987;7:444-449.
Question 2
-The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the
Explanation

Question 3
A teenage female is referred to you for evaluation of curvature in her back that was discovered on routine school screening. She is diagnosed with adolescent idiopathic scoliosis. In which of the following scenarios is a bracing program the most appropriate treatment? Review Topic

Explanation
The treatment of adolescent idiopathic scoliosis (AIS) depends on the magnitude and location of curve as well skeletal maturity of the patient. For curves less than 20 degrees, observation is appropriate until skeletal maturity, with closer intervals during
times of peak growth. Curves between 20-25 and 45 degrees in patients who are Risser stage 0,1 or 2 are best treated with bracing to stop progression. Curves with an apex at T7 or below are typically treated with a Boston brace. Curves over 50 degrees generally warrant a discussion about surgery to prevent progression past maturity.
In a landmark study, Weinstein et al. evaluated both a randomized and preference based cohort of bracing versus observation. The trial was stopped early due to efficacy of bracing. The rate of treatment success was 72% after bracing and 48% after observation. Treatment success was strongly correlated to time of brace wear.
Schlenzka et al. reviewed indications, treatment, and complications associated with brace treatment of AIS. They state that further evidence is necessary to evaluate the efficacy of bracing in AIS.
Figure 1, 2, and 3 are radiographs depicting Risser stage 0, 1, and 4 respectively. Illustration B shows radiographs of all Risser stages. Illustration C is the Lenke classification system for idiopathic scoliosis.
Incorrect Answers:
Question 4
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:

Explanation
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Question 5
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 6
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
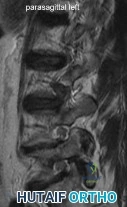
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 7
Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? Review Topic
Explanation
Question 8
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
Question 9
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
REFERENCES: Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 10
What is the most common cause of errors that harm patients? Review Topic
Explanation
Question 11
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 12
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
REFERENCES: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 13
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 14
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?
Explanation
REFERENCES: Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Lubowitz JH, Elson WS, Guttmann D: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86-92.
Question 15
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 16
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
Explanation
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin promotes nitric oxide activity to increase vasodilation.
Question 17
The nucleus pulposus of the intervertebral disk consists of chondrocyte-like cells that have a limited vascular supply and generate energy through which of the following?
Explanation
Question 18
A 75-year-old woman is undergoing a T10-S1 lumbar decompression and fusion for severe degenerative scoliosis. During the deformity corrective maneuver, intraoperative neuromonitoring revealed a sustained 80% decrease in somatosensory-evoked potential (SSEP) amplitudes. Appropriate lead placement and
Explanation
Question 19
What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates? Review Topic
Explanation
Question 20
During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?
Explanation
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary bone healing and secondary bone healing takes place at tissue strain of 2-10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40% or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
Question 21
The sublime tubercle of the elbow serves as the insertion site of the Review Topic
Explanation
Question 22
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 23
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
REFERENCES: Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Gelberman RH, Khabie V, Cahill CJ: The revascularization on healing flexor tendons in the digital sheath: A vascular injection study in dogs. J Bone Joint Surg Am 1991;73:868-881.
Question 24
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
REFERENCES: Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Ereth MH, Weber JG, Abel MD, et al: Cemented versus noncemented total hip arthroplasty: Embolism, hemodynamics, and intrapulmonary shunting. Mayo Clin Proc 1992;67:1066-1074.
Question 25
A 20-year-old male military recruit reports a 5-day history of progressive deep groin pain that is made worse with weight-bearing activities and running. His initial coronal T2-weighted MRI scan is shown in Figure 75. His initial treatment should consist of which of the following? Review Topic
Explanation
Question 26
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency?
Explanation
REFERENCES: Dunn AL, Busch MT, Wyly JB; et al: Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24:414-426.
Journeycake JM, Miller KL, Anderson AM, et al: Arthroscopic synovectomy in children and adolescents with hemophilia. J Pediatr Hematol Oncol 2003;25:726-731.
Question 27
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Langenskiold A, Ryoppy S: Treatment of paralysis of the trapezius muscle by Eden-Lange operation. Acta Orthop Scand 1973;44:383-388.
Romero J, Gerber C: Levator scapulae and rhomboid transfer for paralysis of trapezius: The Eden-Lange procedure. J Bone Joint Surg Br 2003;85:1141-1145.
Question 28
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist’s office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
Explanation
Question 29
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
REFERENCES: Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 30
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 31
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
Question 32
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
REFERENCES: McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Vegso JJ: Field evaluation and management of head and neck injuries. Post Grad Adv Sport Med 1987;10:2-10.
Question 33
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 34
Figures 1 and 2 are the radiographs of a 40-year-old woman who sustained a twisting injury to her lower extremity. What additional information or studies are important in determining treatment options?

Explanation
(SBQ12TR.24) In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?
Oligotrophic nonunion of a comminuted humeral shaft fracture
Oligotrophic nonunion of a transverse humeral shaft fracture
Oligotrophic nonunion of an oblique distal femur fracture
Oligotrophic nonunion of a comminuted tibial shaft fracture
Oligotrophic nonunion of an oblique tibial shaft fracture
Reamed exchange nailing is recommended for the management of aseptic nonunions of noncomminuted tibial shaft fractures. Union rates have been reported between 76-96% in large studies.
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
(SBQ12TR.79) A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2 weeks. Which of the following would be an indication for surgical management?
Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is
displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
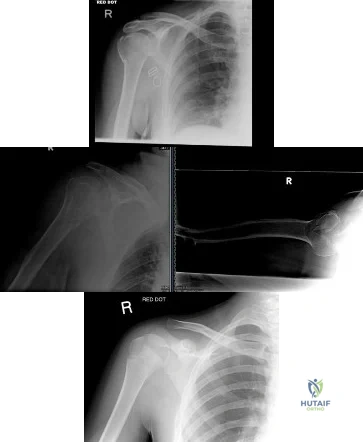
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Question 35
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
Explanation
REFERENCES: Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995.
Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Henderson RC: The long-term results of nonoperatively treated major pelvic disruptions. J Orthop Trauma 1989;3:41-47.
Question 36
03 A 35 year old man sustains a dislocation of his dominant shoulder in a fall. The shoulder is reduced and placed in a sling, but returns 6 hours later with shoulder dislocated again, despite use of a sling. A CT scan is shown in figure 36. Management should now consist of
Explanation
back to this question go to explanation
Question 37
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 38
What is the most common maxillofacial/dental injury in ice hockey?
Explanation
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
REFERENCES: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.
Question 39
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
REFERENCES: Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures:
A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170.
Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Cretnik A, Kosanovic M, Smrkolj V: Percutaneus versus open repair of the ruptured Achilles tendon: A comparative study. Am J Sports Med 2005;33:1369-1379.
Question 40
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701.
Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg
1997;5:240-248.
Bundschuh C, Modic MT, Kearney F, et al: Rheumatoid arthritis of the cervical spine: Surface-coil MR imaging. Am J Roentgenol 1988;151:181-187.
Question 41
A 30-year-old patient is indicated for distal femoral osteotomy. This procedure results in survivorship with
Explanation
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.

CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67
Figures 65a and 65b are the radiographs of an 80-year-old woman with long-standing knee pain who has failed nonsurgical treatment that includes a structured physical therapy program, nonsteroidal anti-inflammatory medications, and intra-articular steroid injections. Her radiographs reveal significant degenerative changes. She has experienced some cognitive decline during the last several years and poorly tolerates pain medications, but she remains very active.
Question 42
Figures A and B show the six-month follow-up radiographs of a 62-year-old woman who sustained a hip fracture in a fall. Prior to the fall, the patient was active and had no difficulty with ambulation. The patient underwent open reduction and internal fixation with a sliding hip screw device. She has difficulty with ambulation, continues to walk with a walker, and reports startup pain. What is the most appropriate management at this time? Review Topic
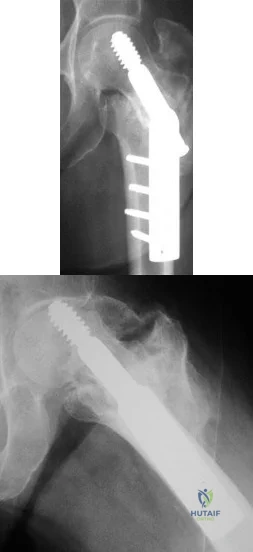
Explanation
Question 43
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
REFERENCES: Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861.
Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 44
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Explanation
REFERENCES: Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229.
Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.
Question 45
0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care? Review Topic
Explanation
Question 46
Synovitis of the MTP joints with eventual hyperextension deformity of the MTP is a common toe deformity seen with RA.
Explanation
Jin et al conducted a meta-analysis regarding polymorphisms in the 5' flank of COL1A1 gene and the conflicting results relating to osteoporosis. They found that the COL1A1 Sp1 polymorphism is associated with a modest reduction in BMD and an increased risk of fracture.
The attached review by Huang and Kung discusses the multiple genetic and environmental determinants of osteoporosis and illustration A (from a different review by these same authors) lists the known genes currently associated with osteoporosis.
The greatest biomechanical difference between unicortical and bicortical locking screws is seen when what force is applied?
Compression
Torsion
Distraction
Bending on the side of the plate
Bending on the surface perpendicular to the plate
Torsion force has the largest biomechanical difference between unicortical locked screws and bicortical locked screws.
The first referenced article by Roberts et al noted that by replacing the farthest unicortical
screws (3 per side of the fracture) with bicortical locking screws, torsion resistance was increased by over 50%.
The second referenced article by Fulkerson et al noted decreased resistance to all applied forces with unicortical screws in a comminuted fracture model, and recommended against their use in such a fracture.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
You are planning surgery on a 54-year-old female with the tibial plateau fracture seen in figures A and B. After reduction of the joint surface you plan to fill the void with a bone-graft substitute to prevent joint collapse. Which of the following bone-graft substitutes
disappears most quickly in vivo?
Collagen-based matrices
Calcium phosphate
Calcium sulfate
Synthetic calcium sulfate and tri-phosphate mixture
Coraline hydroxyapatite
Calcium sulfate disappears in vivo quickly, usually within 4-12 weeks. Calcium phosphate and coraline hydroxyapatite are resorbed slowly, somewhere between 1-10 years, depending on the manufacturer. Synthetics that combine calcium sulfate and phosphate
resorb quicker than calcium phosphate but slower than calcium sulfate. Collagen-based matrices show quick resorption of the collegen but slow resorption of their hydroxyapatite coating. Walsh et al. examined the in vivo response of calcium sulfate pellets alone or in combination with autogenous bone graft in a sheep model. They found excellent bone formation in defects filled with calcium sulfate pellets. Immunostaining for various cytokines (BMP-2, BMP-7, PDGF, or TGF-beta)
showed elevated levels in the newly formed bone. They proposed that the local environment acidity was responsible for breakdown of the calcium sulfate. Watson evaluated 8 patients with comminuted tibial metaphyseal fractures treated with an injectable calcium sulfate. They found that bone regrowth was observed in all patients and the bone substitute almost completely resorbed by
months. Bucholz reviewed the biochemical, biomechanical, and longevity characteristics of the common bone substitutes.
Which of the following Figures shows a fixation construct achieving absolute stability?
Figure A shows percutaneous pinning, Figure B shows locked bridge plating, Figure C shows intramedullary nailing, Figure D shows lag fixation and neutralization plating, and Figure E shows external fixation. All except Figure D show relative stability constructs.
Absolute stability is a construct seen in Figure D, where lag screws and a neutralization plate are shown in a postoperative clavicle. No micromotion is seen with this technique, and healing is by primary (Haversian) healing, as opposed to the other four constructs, which have relative stability and heal via callus formation. The first reference, the AO Principles textbook, covers this in depth.
The second reference by Claes et al notes that bone can still heal with bone (as opposed to fibrous union) with strain rates up to 15%.
Which immunoglobulin subtype does the rheumatoid factor target?
IgA
IgE
IgM
IgG
Rheumatoid factor does not target an immunoglobulin
Rheumatoid factor is an auto-antibody most commonly seen with rheumatoid arthritis. The presence of rheumatoid factor can also indicate generalized autoimmune activity unrelated to rheumatoid arthritis (e.g. tissue or organ rejection). Rheumatoid factor is itself an IgM antibody that is directed against the Fc portion of IgG antibody. Rheumatoid factor (IgM) attaches to IgG to form immune complexes which are deposited in tissues like the kidney and contribute to the overall disease process in rheumatoid arthritis.
James et al. assessed the occurrence and predictive factors for orthopaedic surgery in an cohort of patients with rheumatoid arthritis. Risk factors for surgery varied but the authors found that decreased inflammatory markers during the first year after diagnosis decreased the risk for subsequent surgery.
The positive predictive value is defined as which of the following?
True positives / (true positives + true negatives)
False negatives / (false negatives + true positives)
False positives / (false positives + false negatives)
(True positives + false positives) / (true negatives + false negatives)
True positives / (true positives + false positives) Corrent answer: 5
The positive predictive value is defined as the true positives divided by the sum of the positive results (true positive and false positive). It is also defined as the probability that a patient with a positive test actually has the disease; it is dependent on prevalence of disease.
The referenced articles by Wojtys and Kuhn et al are two of a series of medical statistics review papers.
An 85-year-old woman undergoes the treatment seen in Figure A for a displaced left femoral neck fracture. During wound closure, the patient becomes hypoxic and hypotensive. Despite aggressive resuscitation efforts, she passes away three hours later in the intensive care unit. The autopsy findings seen in
Figure B from the patient's lungs are most likely the result of which of the following
Reaming for the femoral component
Insertion of a femoral component after cement pressurization
Utilization of undersized broaches during canal preparation
Inadequate beta blockade
Use of spinal anesthesia
The clinical scenario is consistent with fat emboli syndrome. Figure A, shows a cemented bipolar hemiarthroplasty while Figure B shows marrow embolization into the lungs.
Studies have shown that intramedullary pressure and fat embolization are greatest during pressurization of cement and implant insertion.
Intramedullary pressure is influenced by size, shape, sharpness and insertion rate of an implant. Pressurization during cementing of a femoral component generates a large degree of pressure over a much wider surface area than in the other methods described of femoral canal instrumentation or preparation, as the entire femoral canal is
pressurized at one time. This results in the highest degree of marrow embolization to the lungs resulting in hypoxia.
Dobrjanski et al studied which variables affected intramedullary pressurization and found that lower implant insertion speed, lower hammering force, a
rubber- compared with steel-tipped hammer and a larger synthetic bone-to- implant radial gap reduced intramedullary pressure generated in a femur module.
Sustained compression applied to a growth plate under experimental conditions has what effect?
No effect
Accelerated longitudinal growth
Decelerated longitudinal growth
Decelerated apposition growth
Decreased bending strength of the bone
The Heuter-Volkmann Law states that compression across the growth plate slows longitudinal growth.
Stokes et al demonstrated that sustained compression across the growth plate can decrease longitudinal growth by 40%. Tension across the physis increases growth, but to a lesser degree.
A 13-year-old girl with a displaced proximal tibia fracture is brought into the emergency department by her adult cousin. The
fracture needs surgical management. The child is living with her cousin's family while her parents are in Germany. While the child speaks fluent English, her cousin and her parents are German-only speaking. How should you consent this patient?
No consent is needed given the urgent nature of the injury, proceed with surgery
Talk with the cousin, using the child as a translator
Talk with the cousin, using a German-translator
Call the parents in Germany, using the child as a translator over the phone
Call the parents in Germany, using a German-translator over the phone
This is an urgent (not emergent) clinical senario, and as such, the child needs to have
formal consent by speaking with her parents using a German- translator.
Wenger and Lieberman discuss the problems and potential solutions surrounding the process of informed consent in patients who either personally lack capacity to make decisions or in patients who require surrogates (like minors) to make treatment decisions.
Lindseth reviews the ethical issues encountered in pediatric orthopaedics and the problems associated with these decisions. Specifically pediatric consent is confounded because the person giving the consent is not the person who will bear the consequences of the treatment.
What is the primary mode of bisphosphonate excretion?
Renal
Gastrointestinal
Liver
Skin
Pulmonary
Bisphosphonates are a broad class of medicines used to treat osteoporosis and Paget's disease. They work by inhibiting osteoclast-mediated resorption after being absorbed into the inorganic phase of bone and taken up by osteoclasts. The paper by Lin et al provides a nice review of bisphosphonates and describe their appropriate use in enhancing bone density in patients with structurally
flawed bone. They describe the mechanism of action of bisphosphonates as pyrophosphate analogues and their renal mechanism of excretion, thus, prohibiting their use in patients with renal insufficiency. Rosier discusses the role of the orthopaedic surgeon in the diagnosis and treatment of patients with osteoporosis, now referred to as the "own the bone" initiative. Central to the treatment of osteoporosis are bisphosphonates and the anti-RANKL
monoclonal antibody, Denosumab.
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends classifying patients as having either a "standard" or "elevated" risk of bleeding complications. The presence of all of the following qualify a patient as having an "elevated" risk of major bleeding EXCEPT?
History of hemophilia
History of protein C deficiency
History of a recent gastrointestinal bleed
History of a recent hemorrhagic stroke
History of Von Willebrand's Disease
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends that all patients pre-operatively should be classified as either having an elevated or standard risk of bleeding and either an elevated or standard risk of pulmonary embolism.
A history of a bleeding disorder (e.g., hemophilia, Von Willebrand's Disease), recent GI bleed, or hemorrhagic stroke qualifies a patient as having an elevated risk of major bleeding.
A history of hypercoagulable state (such as protein C deficiency) or previous documented pulmonary embolism qualifies a patient as having an elevated risk of pulmonary embolism. Type of thromboembolism prophylaxis is recommended by weighing risk of major bleeding vs risk of PE. For those patients with a known contraindication to anticoagulation an IVC filter is considered. Mechanical prophylaxis is recommended across all risk (low to
high risk of either bleeding or pulmonary embolism) groups undergoing total hip or total knee arthroplasty. The detailed AAOS guidelines can be found on the AAOS website.
The evidence based clinical recommendations are presented in the reference by Johanson et al.
In consideration of a prosthetic knee, each of the following are advantages of choosing a polycentric knee with fluid control over a constant friction knee EXCEPT:
Allows variations in cadence
Flexes in a more controlled manner
Lighter in weight
Improved stance control allows less energy expenditure
Overall length of the limb is shortened during initiation of a step reducing the risk of stumbling
Single axis, constant friction knees function as a simple hinge. They are light, durable, and much cheaper prostheses making them ideal for growing children who will need multiple prostheses before reaching adulthood. This prosthesis allows only a single speed of walking, and relies solely on alignment for stance phase stability. Polycentric knees offer each of the advantages stated above making it a more ideal prosthesis for the active adult. Disadvantages of the polycentric knee include cost, weight, and more sophisticated maintenance.
Tang et al reviews the current prosthetic options for leg and foot amputees. Illustration A demonstrates a single axis knee prosthesis.
Illustration B demonstrates a polycentric knee prosthesis.
Which of the following biologic agents commonly used to treat rheumatoid arthritis (RA) DOES NOT target tumor necrosis factor- alpha (TNF-alpha)?
Infliximab
Rituximab
Etanercept
Golimumab
Adalimumab
Rituximab is a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of immune system B cells. Rituximab is used in combination with methotrexate to treat RA that has not responded to one or more types of treatment, including anti-tumor necrosis factor (TNF) blockers.
In rheumatoid arthritis, and other chronic inflammatory conditions, cytokines produced by activated T-cells/macrophages contribute to the pro-inflammatory state. TNF-alpha is thought to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat RA are directed towards blocking TNF-alpha or its receptors. These drugs are able to reduce inflammation and stop disease progression.
Elliot et al. evaluated the safety and efficacy of infliximab in 20 patients with active RA in an open phase I/II trial lasting 8 weeks. They found that treatment with anti-TNFa was safe, well tolerated and resulted in significant clinical and laboratory improvements.
Illustration A depicts five commonly used anti-TNF alpha biologic agents for the treatment of rheumatoid arhtirits with their usual dosing regimens.
Incorrect Answers:
Receptor activator of nuclear-factor kappa-B ligand (RANKL) is
an important regulator of bone resorption. Which of the following cells is the MAJOR source of RANKL in bone remodelling?
Osteoclasts
Osteoblasts
Integrins
T cells
Macrophages
RANKL, a key osteoclastogenic protein, is expressed by osteoblasts and binds to the RANK receptor on osteoclast precursor cells.
The binding of RANKL to RANK on osteoclast precursor cells drives their differentiation into mature osteoclasts (multinucleated giant cells). Mature osteoclasts bind to the bone surfaces via integrins and resorb bone via their ruffled border within Howship's lacunae. Osteocytes orchestrate bone resorption and bone deposition by controlling osteoclast and osteoblast activity. Osteoblasts release RANKL to induce osteoclast differentiation, while
osteoblasts release osteoprotegerin (OPG) to downregulate osteoclastogenesis. Osteocytes also release fibroblast growth factor-23 (FGF-23), BMPs and sclerostin to regulate osteoblast activity. Antibodies to RANKL and Sclerostin have both been shown to increase bone density.
Compton et al. reviewed osteocyte function and the emerging importance of sclerostin, which is a glycoprotein. Sclerostin is predominantly secreted by osteocytes under physiologic conditions to act as an important negative regulator of bone mass through inhibition of bone formation by osteoblasts.
Illustration A demonstrates local bone milieu. It depicts the interplay between osteocytes, osteoblasts, and osteoclasts via the factors described above.
Incorrect answers:
A 45-year-old woman with rheumatoid arthritis is being scheduled for a total knee athroplasty in 2 weeks. She is currently taking sulfasalazine, Penicillamine, and etanercept, a tumor necrosis factor inhibitor (aTNF-a). What changes should be made to her medication regimen prior to surgery?
Discontinuation of all three medications 1 weeks prior to surgery
Discontinuation of sulfasalazine 1 weeks prior to surgery, continuation of etanercept and penicillamine
Continuation of sulfasalazine, penicillamine, and etanercept
Continuation of sulfasalazine and penicillamine, discontinuation of etanercept 1 week prior to surgery
Continuation of penicillamine, discontinuation of sulfasalazine and etanercept 1 week prior to surgery
Anticytokine disease-modifying antirheumatic drugs (DMARD) have become increasingly popular in the treatment of RA. Immunosuppression and the risk of infection are potential complications for all anti-TNF-alpha medications. Current recommendations for cessation of immunosuppressive therapy are when the drug concentrations are at their lowest levels which include the following: 3 days after etanercept injection; 2 weeks prior to infliximab infusion; 10 days after adalimumab injection. Medications such as sulfasalazine and penicillamine may be continued during the pre and post- operative period. Recent evidence and guidelines such as those reviewed by Keith's paper, suggest that anti-TNF-alpha medications should be stopped 4 weeks prior to surgery.
Giles et al report in their case control series an increased infection rate of RA patients undergoing an orthopaedic procedure who were on TNF-a inhibitors as opposed to patients on more traditional treatment regimens like methotrexate and prednisone.
Which of the following supplements affects blood clotting through its effect on platelets?
Ginkgo
Vitamin D
Ephedra
St. John's Wort
Selenium
Ginkgo and ginseng are two common supplements used in the general population that have inhibitory effects of platelet function. Adverse peri- operative complications consisting of increased bleeding and hematoma formation have been reported with the use of these two herbal supplements. The most commonly used supplements that could have an effect in the peri- operative period include echinacea, ephedra, garlic, ginkgo, ginseng, kava, St John's wort, and valerian. Bleeding has been shown to be effected by garlic, ginkgo, and ginseng; cardiovascular instability from ephedra; and hypoglycemia from ginseng. Kava and valerian have pharmacodynamic herb- drug interactions that can increase the sedative effect of anesthetics. St John's wort has been shown to alter the metabolism of certain drugs used in the perioperative period.
Ang-Lee et al review common supplements used today and their potential anesthesia/operative effects. The article places emphasis on proper history taking of not only medications but also supplements which is often times left out of documentation.
The femur radiograph of a healthy 25-year-old female is compared to the femur radiograph of a healthy 85-year-old female. Which of the following best describes the 25-year-old's femur?
Increased cortical thickness and a smaller medullary canal volume
Decreased cortical thickness and a larger medullary canal volume
Equivalent cortical thickness and medullary canal volume
Increased cortical thickness and larger medullary canal volume
Decreased cortical thickness and a smaller medullary canal volume
As the human body ages the cortical thickness/area decreases and subsequently the diameter/volume of the medullary canal increases. Therefore, a young healthy 25- year-old woman should have thicker cortices and a smaller medullary canal volume than her counterpart at 85 years. A decreased cortical bone area is linked to increased fracture risk.
Stein et al studied femurs from subjects aged 21-92 years of age. They found that a reduction in cortical area was seen in older specimens and this change was more
pronounced in female specimens.
Wrong Answers:
Which of the following is NOT a described complication of corticosteroid injections?
Local flare in surrounding tissues
Apoptosis of myocytes
Skin pigmentation changes
Fat atrophy
Facial flushing
Corticosteroids have not been shown to cause apoptosis of myocytes when injected extra-articularly. Each of the other answers have been described.
Cole and Schumacher provide a review of current uses of corticosteroid injections, and emphasize that how accurately the injection is placed affects the outcome.
Kumar and Newman report prospectively on 672 patients who received 1147 intra- and extra-articular injections. Their overall complication rate was low (16%) with injection site pain (mild) and bleeding constituting the majority of cases. There were 4 instances of fat atrophy in the extra-articular group, and
cases of syncope or dizziness in the intra-articular group. They did not discuss the efficacy of their injections.
A surgeon chooses a periarticular locking plate with unicortical proximal locking screws for an extra-articular distal femur fracture as seen in Figure A. Compared to an identical construct with bicortical unlocked proximal screw fixation, the periarticular locking plate with unicortical locking screws has which biomechanical properties?
Greater torsional and axial fixation strength
Less torsional but greater axial fixation strength
Equal torsional and axial fixation strength
Greater torsional but less axial fixation strength
Less torsional and axial fixation strength
Unicortical locking plates have characteristically less torsional strength than bicortical locking plates and bicortical non-locking plates. Axial strength is improved with locking plate fixation.
Zlowodzki et al studied the LISS periarticular locking plate with unicortical proximal fixation in a distal femur model and found superior axial fixation strength (134%) but worse torsional strength (68%) compared to a fixed angle blade plate with non- locking bicortical screw fixation.
Locked plating was reviewed by Haidukewych and Ricci which highlighted the added cost, unique complications, and they recommended the use of locked plating only in situations when unlocked constructs have demonstrated poor outcomes.
In rat models looking at the effect of malnutrition on fracture healing, amino acid supplementation in a nutritionally deprived rat increases all of the following EXCEPT
Serum albumin
Body mass
Quadriceps total protein content
Fracture callus mineralization
Insulin-like growth factor 1 (IGF-1) mRNA expression
The study by Hughes et al found that essential amino acid supplementation (glutamine, arginine, and taurine) following femoral fracture in a protein- malnourished rat model increases serum albumin, body mass, quadriceps total protein content, and fracture callus mineralization. Expression of IGF-1 and
IGF-2, myosin, actin, and VEGF mRNA were all significantly decreased in the amino acid supplemented group compared to the malnourished group. The malnourished group is thought to have upregulation of mRNA expression in attempt to increase the amount of protein product that is translated, however the lack of amino acid building blocks in the malnutrition group was a barrier to appropriate protein synthesis.
The study by Day et al created a malnourished rat femur fracture model by administering a 6% protein diet. They found that administering a 20% protein diet in the post-fracture period yielded a greater cross-sectional area of the
fracture callus and callus stiffness compared to the 6% protein malnourished group.
The statistical power of a study is best defined by?
1 - probability of type-II (beta) error
True positive/(true positive + false negative)
True negative/(false positive + true negative)
1 - probability of type-I (alpha) error
[True positive/(true positive + false negative)] / false-positive rate
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists. The power is defined by
1 - probability of type-II (beta) error, and is often set at 80%. For example, a power of 80% means that if the intervention works, the study has an 80% chance of detecting this and a 20% chance of randomly missing it. A type-II or beta error occurs when one falsely concludes that there is no significant association when there actually is an association (resulting in a false-negative study that rejects a true alternative hypothesis). The type-II or beta error can be determined if Type I error rate and sample size are known. A type-I or alpha error occurs when a significant association is found when there is no true association (resulting in a false-positive study that rejects a true null hypothesis). The alpha level refers to the probability of a type-I (alpha) error and is usually set for most studies at 0.05. Answer 2 is the formula for sensitivity. Answer 3 is the formula for specificity. Answer 5 is the formula for the positive likelihood ratio. The references by
Kocher and Wojtys are excellent reviews of basic biostatistic principles.
A 55-year-old female with a history of metastatic breast cancer develops shoulder pain without any trauma. Which of the following is involved with the findings shown in Figures A and B?
IL-4
RANK
TNF-alpha
OPG
Sox-9
Osteoclastic bone resorption is the final common mechanism for osteolysis, whether due to a pathologic lytic lesion, macrophage activation in particle wear, or normal remodeling. The RANK-RANKL mechanism controls the coupling of osteoblast and osteoclast activation. Figures A and B show an osteolytic lesion in the humerus in a patient with known metastatic breast carcinoma.
RANKL is expressed from osteoblasts and bone-marrow stromal cells. When RANKL binds to the RANK receptor (receptor/activator of NF-[kappa]B) on the cell membrane of osteoclasts it stimulates differentiation from osteoclast progenitor cells to mature osteoclasts. Mature osteoclasts proceed with osteoclastic bone resporption.
Osteoprotegerin (OPG) acts as a decoy receptor by binding to RANKL and blocking the interaction between RANKL and the RANK-receptor and consequently inhibiting osteoclast formation and
activation.
Illustration A depicts the RANK/RANKL involvement in tumor metastatic spread.
Laboratory values of a normal serum calcium and parathyroid hormone can be found in which of the following disease states?
Primary hyperparathyroidism
Type I vitamin D deficient rickets
Type II vitamin D deficient rickets
X-linked hypophosphatemic rickets
Nutritional rickets
Hypophosphatemic rickets is caused by the inability of kidney proximal tubules to reabsorb phosphate due to a mutated PHEX gene, found on the X chromosome. PHEX is thought to protect extracellular matrix glycoproteins from proteolysis. Hypophosphatemic rickets shares many clinical similarities with nutritional rickets but shows PTH levels that are not elevated, even with calcium and phosphate abnormalities.
Pettifor reviews the advances in molecular genetics in the understanding and possible treatments in tumour-induced osteomalacia/rickets.
The review article by Carpenter discusses the X-linked disorder including its clinical manifestations, the wide spectrum of disease severity, and complications of the disease in adult patients.
Illustration A is a table that details the laboratory values associated with each type of rickets.
An 80 year-old female undergoes ORIF of her hip fracture without any complications. A hospitalist consult was obtained for medical clearance pre- operatively, and she was diagnosed with osteoporosis. Which of the following treatment scenarios will lead to the best management of the patient's osteoporosis?
Schedule a follow-up appointment with the patients primary care physician to initiate therapy
Order a physical therapy consult and initiate an exercise plan
Have the patient meet with a nutritionist to increase her calcium and vitamin D intake
Start bisphosphonates, and have the patient follow-up with her primary care physician
Perform a metabolic work-up as an inpatient, and set-up an appointment in an osteoporosis clinic
The initiation of appropriate osteoporosis treatment following hip fractures occurs at a surprisingly low rate. Physical therapy and dietary changes are not appropriate initial treatments for osteoporosis, and bisphosphonate therapy should be prescribed by the physician who will be following and managing the patient's osteoporosis.
Miki et al performed a prospective randomized trial where they compared the rates of osteoporosis treatment initiation. The percentage of patients who were on pharmacologic treatment at 6 months post-injury was 58% in the group whose treatment was directed by the orthopedic surgeon and osteoporosis clinic, and 29% when managed by the primary care physician alone.
The elements chromium, molybdenum, and cobalt are basic components of which of the following implant materials?
Aluminum oxide
Cobalt alloy
Stainless steel
PMMA
Tantalum
Cobalt alloys are extremely strong and are well-suited to applications requiring longevity. Strength of the implant is improved by the addition of molybdenum. Corrosion resistance is addressed by the addition of chromium, which also increases the hardness of the implant.
Incorrect Answers:
Which of the following scenarios of treatment of a humerus fracture best achieves low strain at the fracture site and high stiffness of the treatment construct?
Functional bracing of a transverse midshaft fracture
Comminuted midshaft fracture with locked bridge plating
Short oblique fracture with interfragmentary lag screw and locked neutralization plate
Uniplane external fixation of a spiral open fracture
Oblique fracture with intramedullary nail fixation
Strain in fractures is calculated by dividing the interfragmentary movement by the size of the fracture gap. Strain must be very low (2%) for primary bone healing to occur, and should be less than 10% for secondary bone healing to occur. Stiffness refers the ability of the construct to resist movement under applied loads. Answer 3 describes a situation where primary bone healing is
the goal. For this to occur, there must be no significant gapping at the fracture site, there must be low strain between fracture fragments, and the construct must be stiff.
None of the other answers would accomplish this. Functional bracing and intramedullary fixation both accomplish healing through formation of fracture callus, or secondary healing. A comminuted fracture treated with locked bridge plating relies on less stiffness to allow for secondary healing between fragments. However, since there are many fracture fragments, the strain is distributed among them and therefore remains low. A uniplane external fixator is very unlikely to accomplish low strain and high stiffness in this setting.
A 67-year-old man complains of low-grade fevers and calf pain 2 weeks following a total knee arthroplasty. What is the next appropriate step in management of this patient?
Plethysmography of lower extremity
MRI of lower extremity
CT angiography of lower extremity
Venous ultrasonography
Knee aspiration to evaluate for septic joint
Venous ultrasonography is the next best step in this patient's management, due to the clinical picture of a deep venous thrombosis. The most sensitive and specific recommended diagnostic procedure is a venous ultrasonography.
In their multi-center study, Haut et al. hypothesized that admission to trauma centers that use duplex ultrasound more frequently would independently predict increased DVT reporting for individual patients. They indeed found that trauma centers ultrasound practice was an independent predictor of DVT diagnosis for individual patients, controlling for patient-level risk factors, but concluded the elevated DVT rates at these centers were due to surveillance bias. As such, they recommend that surveillance for DVT should not be considered as a quality control measure in the care of trauma patients.
A patient undergoes closed reduction of a bimalleolar ankle fracture dislocation by the ER physician and is sent to your clinic for evaluation. You evaluate the patient and schedule him for surgery. According to the 2009 guidelines, which of the following scenarios would meet criteria for coding the encounter as a new patient?
You injected his knee in the office almost 3 years ago for osteoarthritis, and have not seen him since
He had an arthroscopic operation by your partner 4 years ago
You were consulted 1 year ago for shoulder pain when he was hospitalized for chronic renal failure
He was seen by your partner in clinic for a herniated disk 2 years ago, but had no procedures performed
You performed a hip replacement on him 12 years ago, and his last follow- up was 18 months ago at which time he was doing well
Only answer two is correct. The 2009 guidlines clarify that the patient can be defined as new only if he has not been seen by anyone in the physician's same group practice and of the same specialty in the past 3 years. Hand and sports medicine specialists with a CAQ, however, are an exception and are allowed to bill for patients already seen by other orthopedists in the same group as new
patients. This scenario would not qualify as a consultation, since the orthopedic surgeon
is taking over care of the patient's problem and is not merely offering advice to another physician who is already caring for the patient. Consultations do not have the same 3 year time qualification. However, Medicare and many other insurers no longer recognize consultation codes.
All the following medications binds reversibly to the enzyme COX-1 EXCEPT
Meloxicam
Diclofenac
Indomethacin
Naproxen sodium
Aspirin
Aspirin binds irreversibly to the cyclooxygenase enzyme. Aspirin acetylates platelet cyclooxygenase and permanently inhibits thromboxane (TX) A2 production leading to its antiplatelet effects. The other NSAID's listed above bind reversibly with COX-1.
Patrono et al discuss the pharmokinetics and platelet effect of both low dose and regular dose aspirin. Nonsteroidal anti-inflammatory drugs compete dose- dependently with arachidonate for binding to platelet cyclooxygenase.
In the treatment of patients with rheumatoid arthritis, TNF-alpha is blocked by which of the following agents?
Tocilizumab
Anakinra
Etanercept
Abatacept
Rituximab
Etanercept is a biochemically designed soluble p75 tumor necrosis factor receptor immunoglobulin G fusion protein, which blocks the downstream
effects of TNF.
Methotrexate is a chemotherapy agent used to inhibit lymphocytes. Gold inhibits monocytes, while sulfasalazine is an anti-inflammatory decreasing the production of
prostaglandins and leukotrienes. Rituximab inhibits B-cells as it
is a monoclonal antibody to CD20 antigen. Anakinra (Kineret) is a recombinant IL-1 receptor antagonist. Abatacept (Orencia) is a selective costimulation modulator that binds to CD-80 and CD-86 (inhibits T cells). Tocilizumab (Actemra)is an IL-6 receptor inhibitor (2nd line treatment for poor response to TNF-antagonist therapy).
Pisetsky wrote an editorial in NEJM discussing the development of TNF blockers through research, and the potential for the use of Etanercept in patients with juvenile RA through its inhibition of lymphotoxin-alpha.
Which of the following medications when combined with methotrexate has been shown to be more effective than methotrexate alone in the treatment of rheumatoid arthritis?
Nitrofurantoin
Rifampin
Azithromycin
Erythromycin
Doxycycline
Tetracycline was initially used in the treatment of rheumatoid arthritis (RA) because Mycoplasma was thought to be the causative agent. It was later found that tetracyclines have biologic effects on the inflammatory and immunologic cascade by inhibiting collagenase activity. Collagenase is an enzyme involved
in breaking down macromolecules in the connective tissue, contributing to the pathologic changes of RA.
In a prospective study, O'Dell et al found that initial therapy with methotrexate plus doxycycline was superior to treatment with methotrexate alone. Furthermore, similar results for low-dose and high-dose doxycycline suggested that antimetalloproteinase effects were more important than the antibacterial effects.
When using C-arm fluorocopy, patient radiation exposure will be increased with which of the following?
The extremity is positioned closer to the image intensifier
A larger body part is imaged compared to a smaller body part
Use of radiation beam collimation
Mini C-arm fluroscopy is used instead of large C-arm fluroscopy
Decreased duration of imaging
Patient radiation exposure will be increased if a larger body part is imaged compared to a smaller body part.
The first study by Giordano et al used radiation dosimeters for large and mini c-arm machines. They found that elevated exposure levels can be expected when larger body parts are imaged, when the extremity is positioned closer to the x-ray source, and when the large c-arm is used over the mini c-arm.
The second study by Giordano et al also used dosimeters for a mini c-arm and found that the surgical team is exposed to minimal radiation during routine
use of mini-c-arm fluoroscopy, except when they are in the direct path of the radiation beam. They list factors to decrease radiation exposure to patient and surgeon including: minimizing exposure time, reducing exposure factors, manipulating the x-ray beam with collimation, orienting the fluoroscopic beam in an inverted position relative to the patient, strategic positioning of the surgeon within the operative field, judicious use of protective shielding during imaging, and maximizing the distance of the surgeon from the radiation beam.
Illustration A shows that arrangement #1 has the body part half-way between the radiation source and image intensifier. Arrangement #2 has the the image intensifier acting as an arm table for the body part with the radiation source further away. Arrangement #1 has more radiation exposure than #2. The distance between the x-ray tube and the body part is doubled in arrangement
#2 compared to arrangement #1. This increased distance correlates to a reduction in exposure according to the inverse square law (reduction in radiation intensity with greater distance from the x-ray source).
You are seeing a 13-year-old girl for asymptomatic flat feet and recommend observation. In educating this patient/family about general bone health, you recommend what amount of daily dietary calcium for your patient?
Question 47
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 48
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?
Explanation
REFERENCES: Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449.
Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202.
Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Chan D, Aldridge MJ, Maffulli N, Davies AM: Chronic stress injuries of the elbow in young gymnasts. Br J Radiol 1991;64:1113-1118.
Question 49
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
REFERENCES: Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388.
Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
Mills WJ, Tejwani N: Heterotopic ossification after knee dislocation: The predictive value of the injury severity score. J Orthop Trauma 2003;17:338-345.
Question 50
A 17-year-old high school football player sustains a neck injury in a game. During the initial on-field assessment, the team physician removes his helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
Explanation
Complete immobilization of the cervical spine is critical for athletes with a suspected cervical spine or spinal cord injury. The spinal cord in the subaxial spine is especially sensitive to motion, and removal of protective gear such as the helmet and shoulder pads presents an unacceptable risk for progressive neurologic injury in the setting of a potentially unstable cervical spine injury. Removal of the face mask alone is typically performed to improve access to an athlete's airway. Protective equipment often prevents proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques
allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
Question 51
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Explanation
REFERENCES: Matava MJ: Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-296.
Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307.
Question 52
The use of nonsteroidal anti-inflammatory drugs following femoral nailing has been associated with which of the following?

Explanation
Giannoudis et al assessed factors which could affect union in 32 patients with nonunion of a fracture of the diaphysis of the femur and 67 matched patients whose fracture had united. They found that there was no relationship between the rate of union and the type of implant, mode of locking, reaming, distraction or smoking. They also concluded that there was a marked association between nonunion and the use of NSAIDs after injury and delayed healing was noted in patients who took NSAIDs and whose fractures had united.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Question 53
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 54
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms? Review Topic

Explanation
Question 55
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them?
Explanation
REFERENCES: Shea KG: ACL Injury: Epidemiology and Prevention Presented at Sports Related Injuries in the Skeletally Mature Athlete. POSNA: One Day Course, 2008.
Millett PJ, Willis AA, Warren RF: Associated injuries in pediatric and adolescent anterior cruciate
ligament tears: Does a delay in treatment increase the risk of meniscal tears? Arthroscopy 2002; 18:955-959.
Question 56
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?
Explanation
REFERENCES: Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.
Filan SK, Herbert TJ: Herbert screw fixation of scaphoid fractures. J Bone Joint Surg Br 1996;78:519-529.
Question 57
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Post M: Diagnosis and treatment of suprascapular nerve entrapment. Clin Orthop 1999;368:92-100.
Question 58
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 59
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286, 339-365.
Question 60
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?
Explanation
REFERENCES: Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Renshaw TS: Sacral agenesis: A classification and review of twenty-three cases. J Bone Joint Surg Am 1978;60:373-383.
Question 61
Which of the following is considered the most accurate test to determine the amount of limb-length discrepancy in a patient with a knee flexion contracture of 35°?
Explanation
REFERENCES: Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Tachdjian MO: Pediatric Orthopedics. Philadelphia, Pa, WB Saunders, 1990, pp 2867-2870.
Question 62
A 10-year-old boy who plays baseball reports acute pain after throwing a softball from the outfield to second base. A radiograph is shown in Figure 26. Management should consist of
Explanation
REFERENCE: Yandow SM, Lundeen GA, Scott SM, Coffin C: Autogenic bone marrow injections as a treatment for simple bone cyst. J Pediatr Orthop 1998;18:616-620.
Question 63
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
Explanation
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.

Video 8a
Video 8b
Question 64
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
Toe is fused too straight (plantar flexed)
Toe is fused in too much valgus
Toe is fused in too much dorsiflexion
There is a nonunion of the fusion
Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 65
A 58-year-old woman underwent a left total knee arthroplasty 6 years ago. She initially did well after surgery but sustained a fall 2 months ago while at work. She now describes left knee pain and instability and an inability to straighten her knee since the fall. She has been using a hinged knee brace, which provides partial support. On examination, she has passive range of motion of 0° to 115° and active range of motion of 80° to -115°. Her radiographs are shown in Figures below. What is the best option for the restoration of her function?
Explanation
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
Question 66
A 39-year-old man presents with back pain radiating to the left lower extremity for the past 6 weeks. Magnetic resonance images of the pathology are
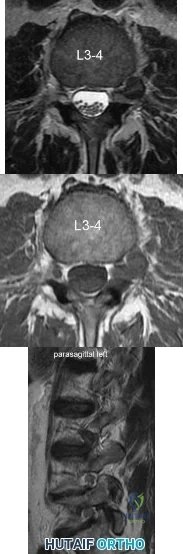
Explanation
Far lateral disc herniations constitute approximately 5-10 percent of disc hernations in the lumbar spine. Given the more vertical anatomy of lumbar nerve roots, at a given disc level, a central or paracentral herniation will affect the traversing nerve root (e.g. nerve root of level below) and a far lateral herniation will affect the exiting nerve root (e.g. nerve root of the level above). Similar to the more common central and paracentral herniations, approximately 90% of patients will improve without surgical intervention. When surgical intervention is needed, the paraspinal approach of Wiltse is utilized.
Marquadt et al. reported long term outcomes of surgical management of far lateral disc herniations. At an average of 146 months follow up, 56.3% of patients had complete relief of symptoms and 27.6% had permanent residual symptoms. Over 75% of patients subjectively rated their outcomes as excellent.
Figure A and B are T2 and T1 axial MRI images, respectively, showing the L3-L4 disc space with a left far lateral disc herniation. Figure C is a left parasagittal T2 MRI image showing impingement on the L3 nerve root. Structures are labeled in illustration A. Illustration B shows the dermatomes of the lower extremity.
Incorrect Answers:
Question 67
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
REFERENCES: Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Kapp S, Cummings D: Transtibial amputation: Prosthetic management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 453-478.
Question 68
A 62-year-old man slips on ice and sustains an elbow dislocation. Post-reduction imaging reveals a highly comminuted radial head fracture and coronoid fracture through its base. What is the most appropriate treatment?

Explanation
Pugh et al reported their experiences with this difficult population. Their protocol consisted of ORIF or replacement of the radial head, ORIF of the coronoid fracture, repair of the LCL and capsule, and repair of the MCL and/or hinged external fixation. Of the 36 cases, the outcome was graded as 28 excellent to good, 7 fair, and 1 poor. 8 cases required re-operation. The authors concluded that their surgical protocol restored sufficient elbow stability to allow early motion post-op, thereby enhancing the functional outcome. In fracture dislocation of the elbow with radial head
and coronoid fracture, the radial head must be fixed or replaced to restore stability. The ORIF of coronoid fracture and radial head restores some valgus stability therefore MCL repair may not be needed. However, the varus stability must be restored by LCL repair.
Question 69
An 83-year-old woman with a long history of her foot slowly and progressively “turning out” now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
Question 70
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
Explanation
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22- mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Question 71
A year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 72
Avascular necrosis
Explanation
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Question 73
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as
Explanation
REFERENCE: Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 74
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Explanation
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 75
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 76
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
REFERENCES: Allan DG, Lavoie GJ, Rudan JF, et al: The use of allograft bone in revision total hip arthroplasty, in Friedlaender GE, Goldberg VM (eds): Bone and Cartilage Allografts: Biology and Clinical Applications. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1991, pp 263-264.
Gross AE, Lavoie MV, McDermott P, Marks P: The use of allograft bone in revision of total hip arthroplasty. Clin Orthop 1985;197:115-122.
Head WC, Berklacich FM, Malinin TI, Emerson RH Jr: Proximal femoral allografts in revision total hip arthroplasty. Clin Orthop 1987;225:22-36.
Question 77
A resident arrives to the operating room late for a LEFT carpal tunnel release procedure. The patient is prepped and draped under general anaesthesia, and the attending surgeon and assistant are about to make an incision to the RIGHT carpal tunnel. The resident mentions to the attending surgeon that surgery was booked for the opposite limb, but he ignores the residents confers by saying the surgical mark is under the drape. What would be the most appropriate course of action for the resident at this time? Review Topic
Explanation
Wrong-site surgery is completely preventable by having the surgeon, in consultation with the patient when possible, place his or her initials on the operative site using a permanent marking pen and then operating through or adjacent to his or her initials. The intended site should be marked such that the mark will be visible after the patient has been prepped and draped. A "time-out" procedure should be done before the initiating of any surgical procedure to confirm the type of procedure, site, and side with all operating room personnel including residents.
Haynes et al. reviewed the effect of surgical safety checklists before surgery on the morbidity and mortality in a global population. They found the rate of death was 1.5% before the checklist was introduced and declined to 0.8% afterward (P=0.003). Inpatient complications occurred in 11.0% of patients at baseline and in 7.0% after introduction of the checklist (P<0.001).
Incorrect Answers:
Question 78
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 79
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management?
Explanation
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
Question 80
What is the most common problem seen following epiphysiodesis for limb-length discrepancy?
Explanation
REFERENCES: Blair VP III, Walker SJ, Sheridan JJ, Schoenecker PL: Epiphysiodesis: A problem of timing. J Pediatr Orthop 1982;2:281-284.
Raney ER: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
Question 81
A 33-year-old female with generalized ligamentous laxity is diagnosed with spontaneous atraumatic subluxation of the sternoclavicular joint. She notes mild, intermittent pain and a small amount of prominence to that area. What is the most appropriate treatment at this time?

Explanation
Question 82
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results? Review Topic

Explanation
Question 83
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? Review Topic

Explanation
(SBQ12SP.9) A 62-year-old male underwent posterior spinal instrumented fusion for degenerative lumbar spondylolithesis one year ago. He presents to office complaining of persistent lower back pain. The pain initially improved but over the last 6 months he has had recurring pain at the site of the surgery primarily with activity. He denies back pain at rest or night pain. Physical examination reveals a well healed wound and no physical abnormalities. He has no tenderness to palpation to the thoracic or lumbar spine. He has no neurological deficits. His laboratory results show an erythrocyte sedimentation rate (ESR) = 8 mm/h and C-reactive protein (CRP) = 3 mg/L at the last visit which are both within normal limits. Figure A shows a series of radiographs from his pre-operative, 3 month post-operative and 1 year post-operative clinic visits, respectively. Which of the following investigations would best confirm the suspected underlying diagnosis? Review Topic
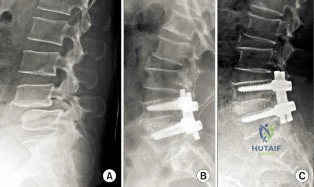
MRI of lumbar spine
Repeat ESR/CRP and whole body bone scan
CT of lumbar spine
Dynamic flexion/extension plain film radiographs
Dynamic lateral bending plain film radiographs
This patient has clinical and radiographic features of failed spinal arthrodesis. CT scan have been shown to be the most relable method for assessing spinal fusion postoperatively.
Reported rates of nonunion following posterior spinal fusion range from 0-70%. Rates are variable due to the various operative techniques, underlying diagnoses as well as asymptomatic patients. Non-union may lead to changes in alignment, spinal instability and potential neurological injury. Static radiographs have long been used as a practical method of fusion assessment, but these tend to significantly overestimate the presence of a solid fusion. Lack of movement at a fused segment, on dynamic views, does not confirm fusion. CT offers excellent bony resolution and are less affected by metal artifact compared to MRI.
Patel et al. showed that tobacco use, malnutrition, oral anti-inflammatory use, multilevel fusion, prior spine surgery, and sagittal imbalance are all risk factors for spinal nonunion.
Mok et al. looked at erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels after spinal surgery and compared their usefulness as predictors of infectious complications in the early postoperative period. They found that CRP is more applicable, predictable, and responsive in the early postoperative period compared with ESR. Using a second rise or failure to decrease as expected for CRP is sensitive for infection.
Shelby et al. reviewed the radiological assessment of spinal fusion. They comment that fine-cut imaging, multiplanar reconstruction, and metal artifact reduction have increased the ability to assess fusion on CT.
Figure A shows a series of lateral radiographs of the lumbar spine with posterior spinal instrumentation. Illustration A shows a lateral CT scan image of multi-level pseudoarthrosis after posterior spinal instrumented fusion. Illustration B shows an
intra-operative
view
of
spinal
pseudoarthrosis
(white
arrow).
Incorrect
(SBQ12SP.19) A 41-year-old male presents with acute onset of low back pain that started when he was trying to lift a heavy box while helping his brother move apartments two days ago. The pain has been severe enough to cause him to miss work yesterday. He has no neurologic deficits. What are the chances he will return to work within 6 weeks? Review Topic
1 80 to 90%
2 70 to 80%
3 60 to 70%
4 50 to 60%
5 40 to 50%
Most adults (up to 80%) will experience an episode of low back pain in their lifetime. In those whose pain is severe enough to cause them to miss work, 60 to 70% will return by 6 weeks, and 80 to 90% will return by 12 weeks.
Low back pain is common in adults. Most patients experience resolution of symptoms quickly and have no lasting loss of function. However, 5 to 10% develop chronic pain. Recurrence of pain is common, and is part of the natural history, occurring in 20 to 72% of patients. After 12 weeks, return to work rates are slow.
Shen et al. review the nonoperative management of acute and chronic low back pain. The authors note that none of the available interventions has been proven by high quality large randomized controlled trials. The authors believe that low dose oral
steroids are safe in the short term and that injection therapy should not be used without a reasonable presumptive diagnosis.
Madigan et al. review the management of lumbar degenerative disease. The authors emphasize that the majority of patients improve within 6 weeks with or without treatment. For patients that do not, the authors do not recommend epidural injection, as there are no good studies to support their use in the treatment of discogenic back pain. When surgical treatment is indicated they state that arthrodesis is the gold standard, although the long term results of total disk arthroplasty are being elucidated.
Illustration A shows a table of available non-operative treatment modalities for back pain. Illustration B shows a list of possible diagnoses associated with acute low back pain, with those associated with neurogenic pain italicized. Illustration C shows a list of 'red flag' symptoms indicating serious/emergent causes of low back pain.
Incorrect
2:
Longer
to than
90%
Question 84
Which of the following factors is associated with improved outcomes following surgery for hip fractures?
Explanation
Question 85
Prescribing touch (10 to 15 kg) weight-bearing would be most appropriate in the following scenario?
Explanation
The definition of touch weight bearing (also known as touch-down weight bearing) is ill-defined in the literature. Published data suggest touch weight bearing to be 10 to 15 kg of load applied to ground by the affected limb or less than 20% of body weight. In contrast, partial weight bearing is reported as 20 to 25 kg or 30% to 50% of body weight. Joint reaction forces across the hip have been shown to be lowest with touch weight-bearing. In this scenario, the foot should be flat against the ground so the flexor and extensor musculature that cross the hip are relaxed. With non-weight bearing restrictions, the musculature across the hip will be contracted, which increases contact pressures and joint reaction forces.
Rubin et al. looked at the validity of touch weight-bearing and partial weight bearing regimens. They found that most patients overload the limb up to 50% more than the target weight prescribed.
Lewis et al. showed that maintaining non-weight-bearing position of the involved leg produces increased compressive forces across the hip joint due to activation of the hip flexors compared to restricted weight-bearing.
Incorrect Answers:
Question 86
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. Which type of contraction of the involved muscle most likely resulted in this lineman's injury?
Explanation
followed by the ECU, EDQ, and, finally, the EIP.
Question 87
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 88
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 89
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 90
When compared with a conventional ultra-high molecular weight polyethylene (UHMWPE) -bearing surface in total hip arthroplasty, a highly cross-linked polyethylene (XLPE) -bearing surface is associated with
Explanation
A. a functional result for at least 20 years.
B. a functional result that deteriorates within the first 10 years.
C. an eventual conversion to a constrained knee arthroplasty.
D. an eventual need for arthrodesis.
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.
Question 91
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
REFERENCES: Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531.
Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 92
A 69-year-old female sustains the injuries seen in Figures A and
Explanation
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
Question 93
271 Which of the following factors has been shown to contribute to poor results after anatomic reduction of posterior wall acetabulum fractures?
Explanation
Complications can include sciatic nerve injury (incidence, 3% to 18%), heterotopic ossification (7% to 20%), and osteonecrosis of the femoral head (5% to 8%). Despite the relative simplicity of this acetabular fracture, unsatisfactory outcomes after surgical repair of the posterior wall occur in at least 18% to 32% of cases, results that are worse than for most of the other more complex acetabular fracture patterns.
Moed BR, et al. Results of operative treatment of fractures of the posterior wall of the acetabulum. JBJS AM 2002:84:752-758
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. JBJS Am 1996;78:1632-1645
back to this question next question
Question 94
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
REFERENCES: Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 95
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 96
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
REFERENCES: Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342.
Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Bylski-Austrow DI, Grood ES, Hetzy MS, et al: Anterior cruciate ligament replacements: A mechanical study of femoral attachment location, flexion angle at tensioning, and initial tensioning. J Orthop Res 1990;8:522-531.
Question 97
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?

Explanation
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A identifies the location of the incision for the anterolateral acromial exposure , and Illustration B shows the position of the axillary nerve in relation to the approach.
Question 98
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 99
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm P 3 P , an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
REFERENCES: Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Kocher MS, Zurakowski D, Kasser JR: Differentiating between septic arthritis and transient synovitis of the hip in children: An evidence-based clinical prediction algorithm. J Bone Joint Surg Am 1999;81:1662-1670.
Question 100
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
