Question 1
A 20-year-old woman with a history of subtotal meniscectomy has a painful knee. What associated condition is a contraindication to proceeding with a meniscal allograft?


Explanation
Patients with significant joint malalignment place increased stresses on the allograft, and this malalignment must be corrected to decrease the likelihood of meniscal allograft failure. None of the other options would lead to failure of the allograft.
Question 2
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?

Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
Question 3
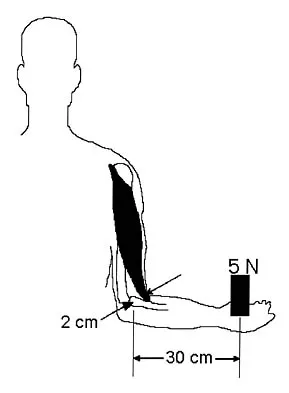
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Question 4
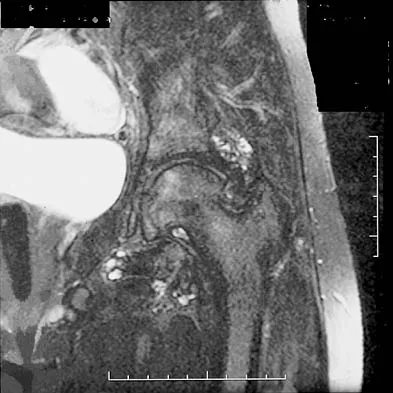
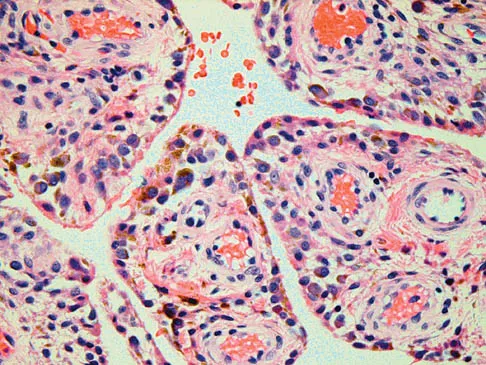
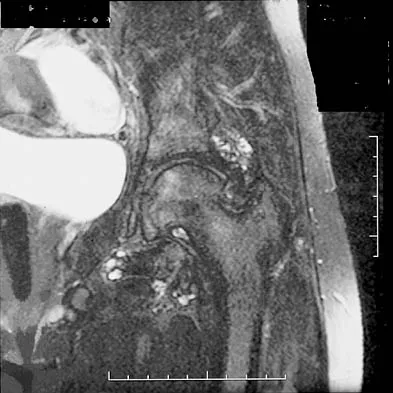
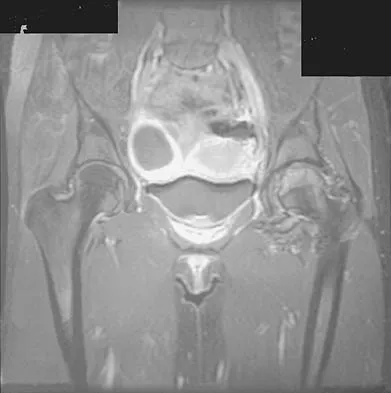
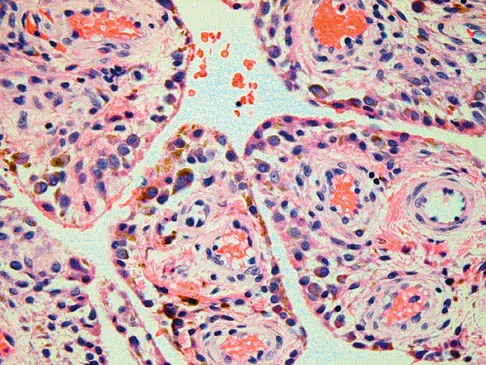
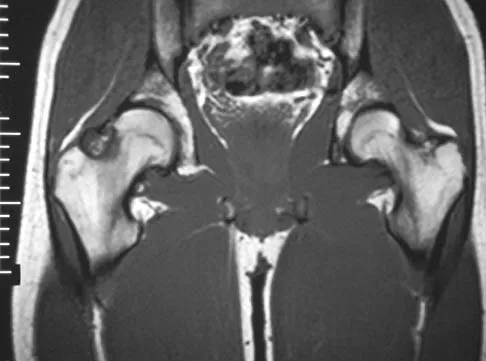
Figures 1a through 1c show the radiograph and MRI scans of a 16-year-old patient who has a painful hip. Examination reveals a significant limp, limited abduction and internal rotation, and severe pain with internal rotation and adduction. A biopsy specimen is shown in Figure 1d. What is the deposited pigment observed in this condition?



Explanation
1b 1c 1d Pigmented villonodular synovitis (PVNS) is a synovial proliferative disorder that remains a diagnostic difficulty. The most common clinical features are mechanical pain and limited joint motion. On radiographs, the classic finding is often a large lesion, associated with multiple lucencies. Other findings may include a normal radiographic appearance, loss of joint space, osteonecrosis of the femoral head, or acetabular protrusion. MRI is the imaging modality of choice and will show the characteristic findings of a joint effusion, synovial proliferation, and bulging of the hip. The synovial lining has a low signal on T1- and T2-weighted images, secondary to hemosiderin deposition. Copper deposition occurs in patients with Wilson's disease, which mainly affects the liver. Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 5
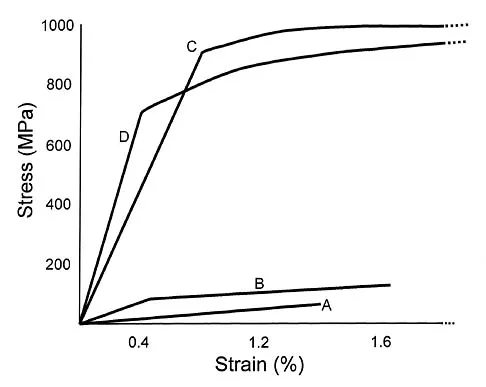
Titanium and its alloys are unsuitable candidates for which of the following implant applications?

Explanation
Titanium alloy is highly biocompatible, has higher strength than stainless steel, and is highly resistant to corrosion. It is particularly suited for use in fracture plates, bone screws, and intramedullary nails because of its low modulus of elasticity (low stiffness), which can reduce stress shielding. It is also widely used for porous-ingrowth coatings. However, clinical experience has shown that titanium alloy bearing surfaces such as a femoral ball are highly susceptible to severe metallic wear, particularly in the presence of third-body abrasive particles (PMMA fragments, bone chips, metal debris, etc). McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517. Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Question 6
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 7
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Explanation
Organisms may develop resistance to antibiotics by production of specific enzymes. S aureus develops methicillin resistance by production of penicillin-binding protein 2a (PBP2a). The strains of S aureus that have acquired the mecA gene for PBP2a are designated as methicillin-resistant S aureus (MRSA). The enzyme manifests resistance to covalent modification by beta-lactam antibiotics at the active-site serine residue in two ways. First, the microscopic rate constant for acylation (k2) is attenuated by three to four orders of magnitude over the corresponding determinations for penicillin-sensitive PBPs. Second, the enzyme shows elevated dissociation constants (Kd) for the noncovalent preacylation complexes with the antibiotics, the formation of which ultimately would lead to enzyme acylation. The two factors working in concert effectively prevent enzyme acylation by the antibiotics in vivo, giving rise to drug resistance. Catalase and oxidase are enzymes produced by some bacteria that confer virulence to the organism but do not make the organisms methicillin resistant. Glycocalix is the pericellular layer produced by bacteria that serves many functions including attachment to surfaces. Beta-lactam describes a class of antibiotics. Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806. Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
Question 8
A 30-year-old man reports pain and weakness in his right arm. Examination reveals grade 4 strength in wrist flexion and elbow extension, decreased sensation over the middle finger, and decreased triceps reflex. These symptoms are most compatible with impingement on what spinal nerve root?
Explanation
Motor impulses to the triceps, wrist flexion and elbow extension, and sensation to the middle finger are associated most commonly with the C7 root. Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 125.
Question 9
Why is tendon considered an anisotropic material?
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Question 10
What does Dual Energy X-ray Absorptiometry (DEXA) testing, as a technique, measure?
Explanation
DEXA can provide data on bone mineral content and soft-tissue composition, and requires cross-sectional dimension for accuracy. DEXA provides a quantitative, not qualitative, measurement of bone mineral content and is incapable of differentiating between trabecular and cortical bone. Osteoarthritis falsely elevates the values, especially in the AP spinal analysis. Genant HK, Faulkner KG, Gluer CC: Measurement of bone mineral density: Current status. Am J Med 1991;91:49S-53S. Genant HK, Engelke K, Fuerst T, et al: Review: Noninvasive assessment of bone mineral density and stature: State of the art. J Bone Miner Res 1996;11:707-730.
Question 11
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
Autologous chondrocyte implantation was first reported by Brittberg in 1994 and has resulted in predominantly type II collagen (hyaline-like articular cartilage) in the repair tissue. The extracellular matrix in articular cartilage is made up primarily of type II collagen, proteoglycans, and water. Arthroscopic chondroplasty, microfracture, drilling, and abrasion arthroplasty all result eventually in fibrocartilage fill of the defect (predominantly type I collagen). Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Question 12
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
The term 'spinal shock' applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
Question 13
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
BMPs signal through the activation of a transmembrane serine/threonine kinase receptor that leads to the activation of intracellular signaling molecules called SMADs. There are currently eight known SMADs, and the activation of different SMADs within a cell leads to different cellular responses. The other mediators are not believed to be directly involved with BMP signaling. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 14
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 15
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
Evidence implicates an association, albeit unexplained, between Clostridium septicum infection and malignancy, particularly hematologic or intestinal malignancy. The malignancy is often at an advanced stage, compromising survival of the patients. A bowel portal of entry is postulated for most patients. In the absence of an external source in the patient with clostridial myonecrosis or sepsis, the cecum or distal ileum should be considered a likely site of infection. Increased awareness of this association between Clostridium septicum and malignancy, and aggressive surgical treatment, may result in improvement in the present 50% to 70% mortality rate. Other organisms associated with malignancy include group Clostridium streptococci that are occasionally associated with upper gastrointestinal malignancies. Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Question 16
Immobilization of human tendons leads to what changes in structure and/or function?
Explanation
Recent in vivo and in vitro experiments demonstrate that immobilization of tendon decreases its tensile strength, stiffness, and total weight. Microscopically, there is a decrease in cellularity, overall collagen organization, and collagen fibril diameter.
Question 17
Human menisci are made up predominantly of what collagen type?
Explanation
Type I collagen accounts for more than 90% of the total collagen content. Other minor collagens present include types II, III, V, and VI. Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, p 41.
Question 18
Type II collagen in nondiseased adult human articular cartilage has a half-life that is generally
Explanation
Type II collagen in articular cartilage is amazingly stable. This is important to know because matrix homeostasis generally is associated with minimal synthesis and degradation of type II collagen. Passive glycation has a consistent rate and occurs over decades. The relative amount of glycation in cartilage with age has been used as a measure of stability. Also, the rate of racemization of aspartic acid from the L to D form occurs spontaneously at a very slow rate. The relative stability of collagen can be estimated by calculating the percentage of D aspartic acid per dry weight of type II collagen. Maroudas A, Palla G, Gilav E: Racemization of aspartic acid in human articular cartilage. Connect Tissue Res 1992;28:161-169.
Question 19
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
Muscle fibers can be categorized grossly into two types. Type I muscle, also known as slow-twitch muscle, is responsible for aerobic, oxidative muscle metabolism. It has a much lower strength and speed of contraction than fast-twitch type II muscle but is significantly more fatigue resistant. With training for endurance sports, the type I muscle undergoes adaptive changes to the increased stress. Increases in capillary density, oxidative capacity, mitochondrial density, and subsequent fatigue resistance are all observed changes. Hypertrophy of type IIb muscle is seen in strength training. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Question 20
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 21
A 24-year-old man who works at a local oyster and clam farm sustained a laceration on his hand at work. Examination reveals a cellulitic index finger without evidence of tenosynovitis. After appropriate irrigation and debridement, what antibiotic is most appropriate?
Explanation
Injuries involving brackish water and shellfish can have devastating consequences caused by Vibrio vulnificus infections. Patients may have a severe invasive infection, with three main clinical features: primary septicemia, wound infection, and gastroenteritis. Antibiotic administration is crucial because mortality rates of up to 50% have been observed with Vibrio septicemia. The current recommendation is to give a third-generation cephalosporin such as ceftazadime. Chiang SR, Chuang YC: Vibrio vulnificus infection: Clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 2003;36:81-88.
Question 22
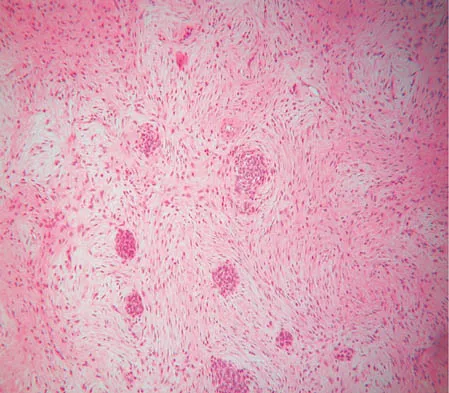
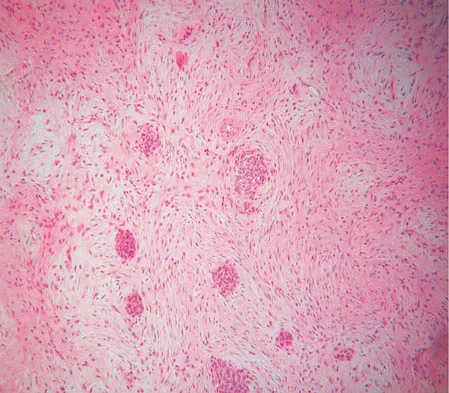
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?

Explanation
2b The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 23
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 24
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 25
What assay most directly assesses gene expression at the posttranslational level?
Explanation
Gene expression at the posttranslational level refers to proteins, as opposed to DNA or RNA. The only assay above that targets protein expression directly is the Western blot. Standard PCR is amplification of targeted DNA segments, regardless of whether or not they are actively expressed. Real-time PCR, Northern blot, and microarray expression profile analysis all quantify RNA as a means to determine posttranscriptional gene expression. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Finish Exam?
You cannot change answers after submitting.
