Question 51
What is the most common location of osteosarcoma?



Explanation
The most common location of osteosarcoma is the knee area (50% to 55%), followed by the proximal humerus and iliac wing. The most commonly involved long bone is the femur (40% to 45%), followed by the tibia (15% to 25%). Within these bones, tumors are typically adjacent to the epiphyses in most patients. The flat bones of the pelvis and spine are less frequently involved. Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
Question 52
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of

Explanation
The treatment of choice for pelvic chondrosarcoma is wide resection via an internal hemipelvectomy. Chondrosarcoma requires surgical resection for control and does not respond to traditional chemotherapy or external beam radiation. Hip arthroplasty with acetabular reconstruction and curettage and cementation of the lesion are intralesional procedures that result in a higher incidence of local recurrence of tumor. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 53
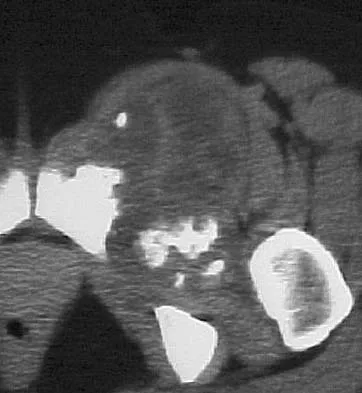
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of


Explanation
29b The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Question 54
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?


Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 55
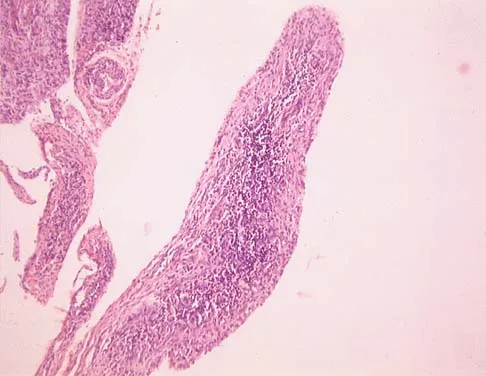
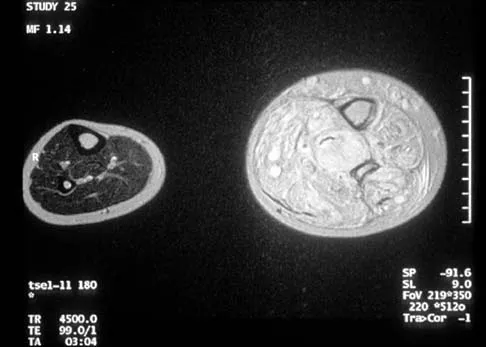
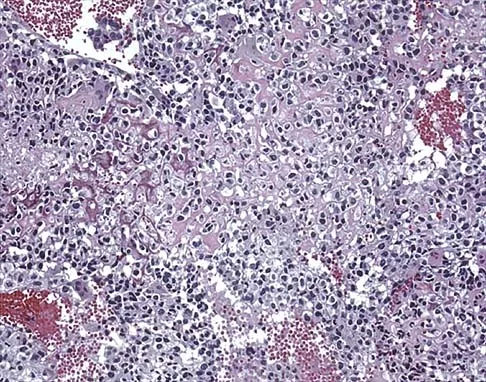
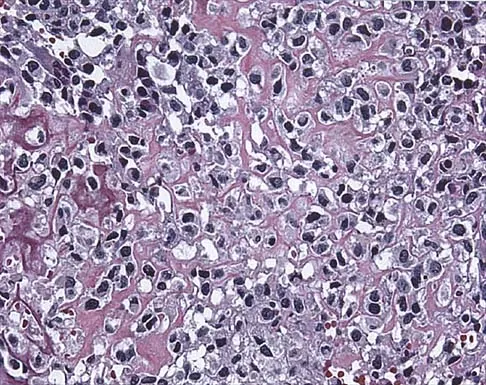
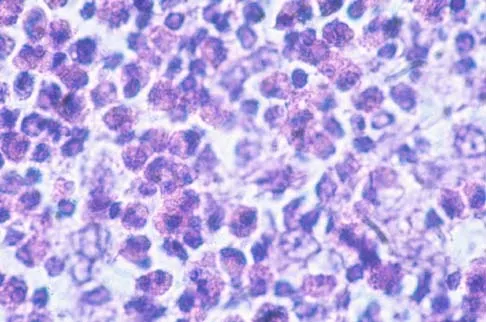
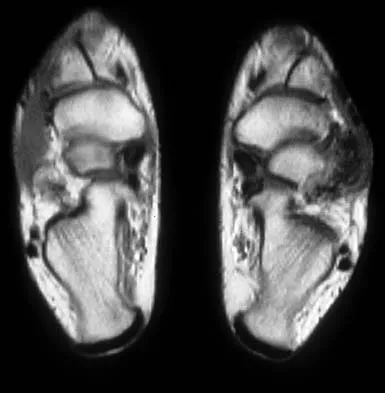
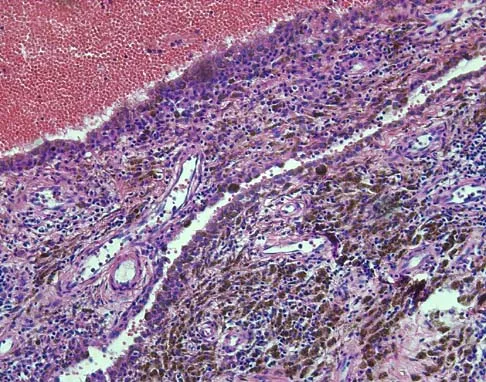
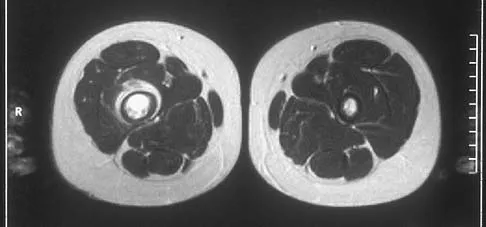
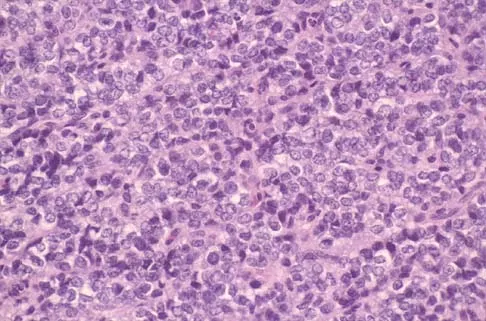
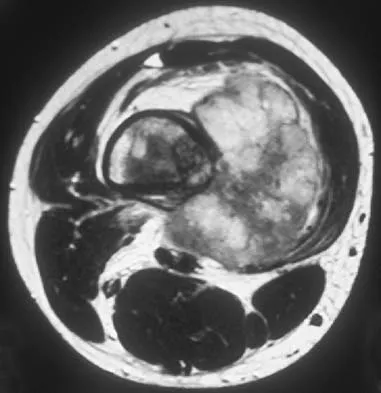
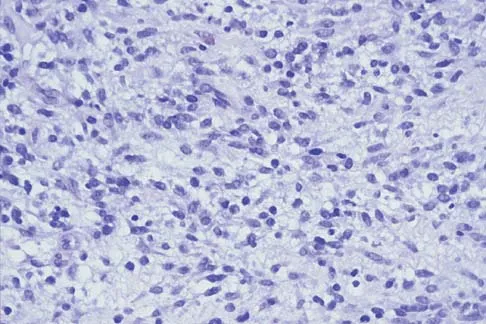
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of




Explanation
30b The histology shows small round blue cells that are uniform in appearance; these findings are consistent with Ewing's sarcoma. The MRI scan shows infiltration of the marrow and a large surrounding soft-tissue mass. Based on these findings, the management of choice is systemic chemotherapy. Local control of the primary lesion is addressed by either surgical resection or radiation therapy or a combination of the two after the patient receives systemic chemotherapy. The clinical, radiographic, and histologic presentation of Ewing's sarcoma often can be confused with osteomyelitis. The histology shows an absence of inflammatory cells. Grier HE: The Ewing family of tumors: Ewing's sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Question 56
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?



Explanation
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
Question 57
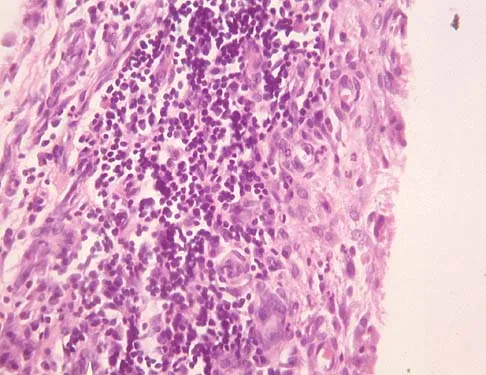
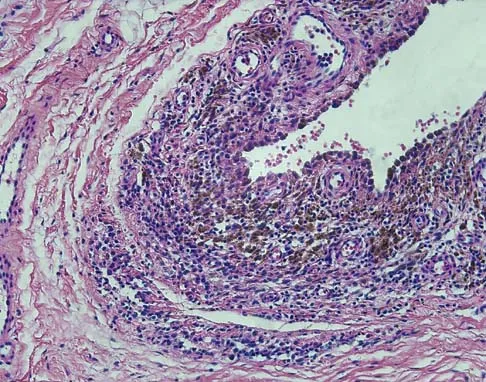
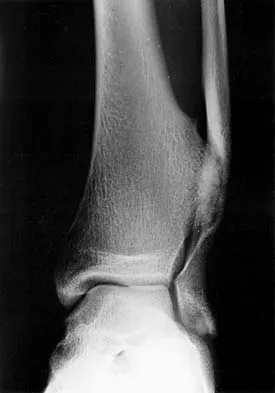
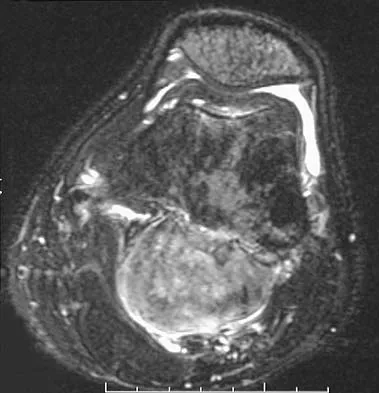
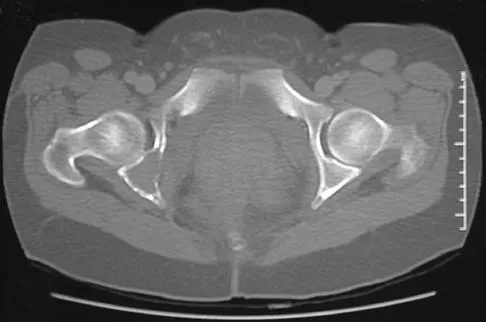
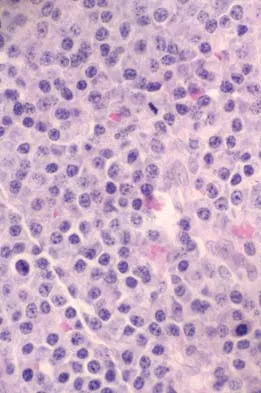
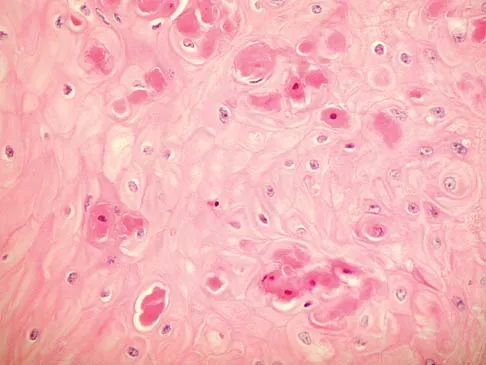
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?

Explanation
32b 32c 32d Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 58
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Question 59
A previously healthy 14-year-old boy now reports fatigue, and has a bilateral Trendelenburg gait, right hip pain, and bilateral knee and foot pain. Biopsy of a right sacral mass reveals intermediate grade osteosarcoma. There are no metastases. Laboratory studies reveal a serum calcium level of 7.7 mg/dL (normal 8.5 to 10.5), a phosphate level of 2.0 mg/dL (normal 2.7 to 4.5), a 1,25-dihydroxyvitamin D level of less than 10 pg/mL (normal 18 to 62), a parathyroid hormone level of 19 pg/mL (normal 10 to 60), and an alkaline phosphatase level of 428 U/L (normal 15 to 351). What is the most likely cause of the patient's symptoms?
Explanation
The laboratory findings are typical for rickets. Oncogenic rickets is a paraneoplastic syndrome that results from a substance secreted by the tumor that interferes with renal tubule reabsorption of phosphate. This substance previously had been called phosphatonin but recently has been identified as fibroblast growth factor 23. Nutritional rickets is rare in developed countries. Delayed onset familial hypophosphatemic rickets is possible, but the likelihood of having two rare diseases is unlikely. Osteosarcoma does not sequester calcium. Alkaline phosphatase levels can be elevated in osteosarcoma but does not cause muscle weakness. Tumor cachexia would occur only with advanced metastatic disease. A unilateral sacral mass would not cause a bilateral L5 neuropathy or the abnormal laboratory findings. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 29-2001. A 14-year-old with abnormal bones and a sacral mass. N Engl J Med 2001;345:903-908.
Question 60
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Question 61
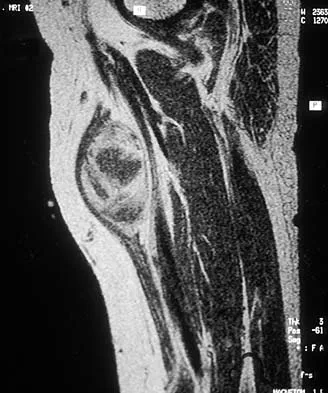
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?

Explanation
33b 33c 33d 33e The patient has parosteal osteosarcoma. The posterior aspect of the distal femur is the typical location for this variant of osteogenic sarcoma. The imaging studies indicate a surface lesion with no involvement of the adjacent intramedullary canal. The histologic appearance is that of a low-grade fibroblastic osteosarcoma, consisting of relatively mature bone and a bland fibroblastic stroma lacking cytologic atypia and mitotic activity. A cartilaginous component is also frequently seen. Classic osteosarcoma typically has a more aggressive radiologic and histologic appearance. Sessile osteochondromas, while common behind the knee, have a presence of hematopoietic marrow and fat. The cartilage found in the associated cartilaginous cap is oriented. Chondrosarcomas are more typical in an older age group and have a histologic pattern consisting of malignant chondroid. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
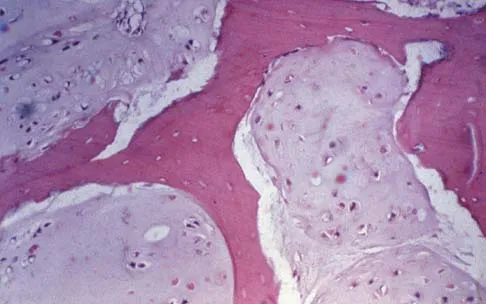
Question 62
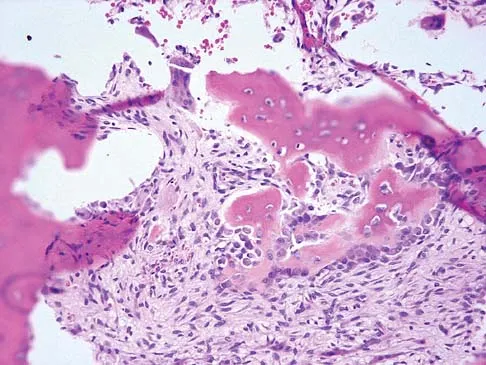
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?

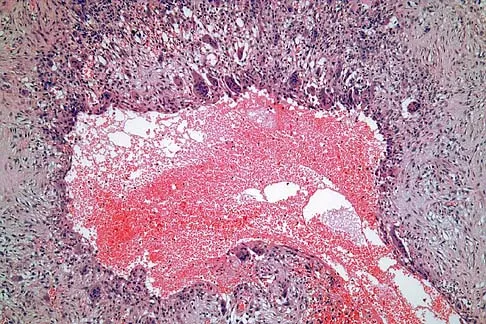
Explanation
34b Aneurysmal bone cysts typically present as radiolucent lesions with an expansile remodeled cortex. The histologic appearance consists of blood-filled lakes surrounded by a benign lining that contains fibroblasts, giant cells, and hemosiderin. Although the other lesions are in the radiographic differential diagnosis, these histologic findings indicate an aneurysmal bone cyst. Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Question 63
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
The mutation of the retinoblastoma gene has been associated with an increased prevalence of osteosarcoma. The mutation resulting in EWS-FLI1 is associated with Ewing's sarcoma. The other mutations are associated with tumor formation and proliferation but not necessarily with osteosarcoma formation. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4. Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Question 64
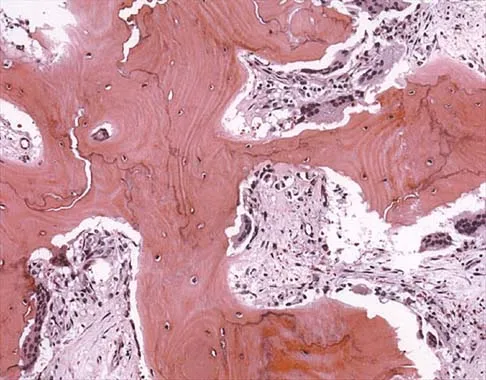
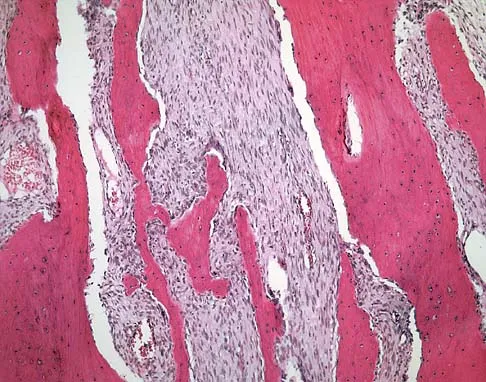
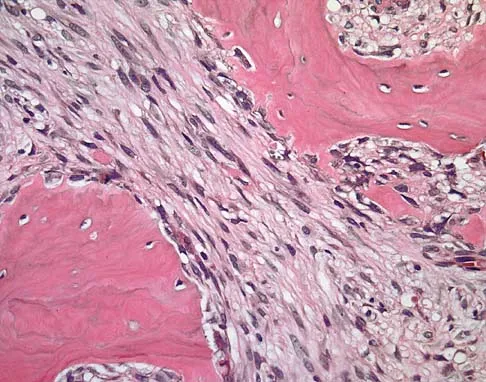
A 12-year-old girl has painless bowing of the tibia. Radiographs and a biopsy specimen are shown in Figures 35a through 35c. What is the most likely diagnosis?


Explanation
35b 35c The patient has osteofibrous dysplasia. The radiographic differential diagnosis includes osteofibrous dysplasia, fibrous dysplasia, and adamantinoma. Histology shows a fibro-osseous lesion with prominent osteoblastic rimming but a lack of epithelial nests. Adamantinoma is a low-grade malignancy that typically is located in the anterior tibial cortex and has a soap bubble appearance. Histologically, it is similar to osteofibrous dysplasia but includes epithelial nests of cells. Treatment requires resection. Fibrous dysplasia usually does not require biopsy; however, in this patient the radiographs do not distinguish it from adamantinoma. The radiographic findings are not typical of Ewing's sarcoma or osteosarcoma. Repeat biopsy should be considered if clinical or radiographic features change.
Question 65
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in

Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 66
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
Curettage and bone grafting typically are the preferred treatment of chondroblastoma, yielding acceptable local recurrence rates of less than 10%. Some surgeons advocate adjuvant therapies such as phenol, liquid nitrogen, or argon beam coagulation. Untreated, these lesions can destroy bone and invade the joint to a significant degree. Large intra-articular lesions may require major joint reconstruction. Wide local excision is rarely required to control the tumor. Radiation therapy is indicated only in unresectable lesions. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Question 67
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of


Explanation
37b 37c 37d The patient has Ewing's sarcoma. Management options for local tumor control include radiation therapy, resection, or a combination; however, in this patient wide resection is preferred over radiation therapy. Radiation therapy is associated with damage to the growth plate, pathologic fracture, radiation-induced sarcomas, and a local recurrence rate of approximately 10% to 12%. Radiation therapy is used for positive margins, unresectable tumors, or for tumors that have a poor response to chemotherapy. Amputation is not necessary since the tumor is resectable. Chemotherapy has improved overall survival rates to over 60% of patients. Sailer SL: The role of radiation therapy in localized Ewing' sarcoma. Semin Radiat Oncol 1997;7:225-235. Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing's sarcoma. United Kingdom Children's Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704. Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Question 68
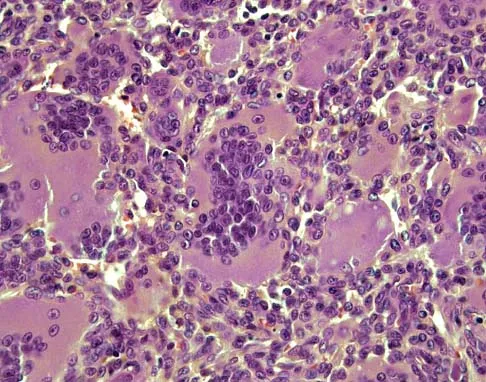
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?

Explanation
38b 38c The laboratory studies and histology are both consistent with myeloma. Infection should show white blood cells other than plasma cells on histology. Lymphoma would show lymphocytes, not plasma cells. The lack of bone formation on the imaging studies and the lack of osteoid on histology rule out osteosarcoma. The cells have too much cytoplasm and nuclear chromatin to be Ewing's sarcoma cells.
Question 69
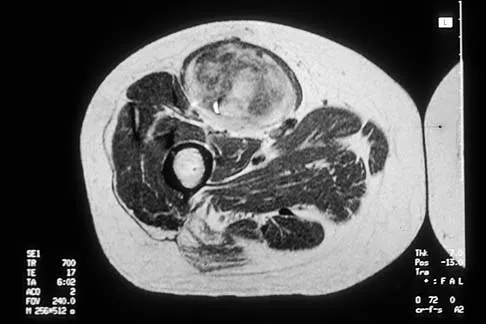
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include

Explanation
39b Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 70
A 60-year-old man has pain at the tip of the index finger. A radiograph and biopsy specimen are shown in Figures 40a and 40b. Management should consist of

Explanation
40b The radiograph and histology findings are most consistent with squamous cell carcinoma. This tumor is best treated with wide surgical resection margins alone in the absence of metastasis; in this patient, management should consist of amputation through the distal interphalangeal joint. The other treatments are not indicated. Soltani K, Krunic A: Non melanoma skin neoplasms, in Vokes E, Golomb H (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, pp 646-647.
Question 71
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

Explanation
41b The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 72
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
Paucytopenia is a common problem in patients with metastatic disease. Causes include chemotherapy, external beam radiation, marrow replacement by tumor, and anemia of chronic disease. There is no correlation with decreased calcium and a decrease in hematopoiesis. Supportive care with granulocyte-colony stimulating factor (G-CSF) and neupogen can stimulate hematopoiesis.
Question 73
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of

Explanation
42b 42c The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 74
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of


Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 75
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?


Explanation
44b The patient has multiple hereditary exostoses and a secondary chondrosarcoma arising from a proximal femoral exostosis. The radiograph of the knee shows multiple osteochondromas typical in a patient with multiple hereditary exostoses. Patients with this diagnosis are at an increased risk for malignant degeneration of an osteochondroma. The lateral radiograph of the hip shows a bony lesion emanating from the anterior aspect of the femoral neck that is not well defined in the surrounding soft tissues. There are punctate calcifications and a large soft-tissue mass. The most likely diagnosis is a secondary chondrosarcoma developing from a benign osteochondroma. An enchondroma is an intramedullary benign cartilage lesion. Ollier's disease and Maffucci's syndrome involve multiple enchondromas. Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Finish Exam?
You cannot change answers after submitting.
