Question 51
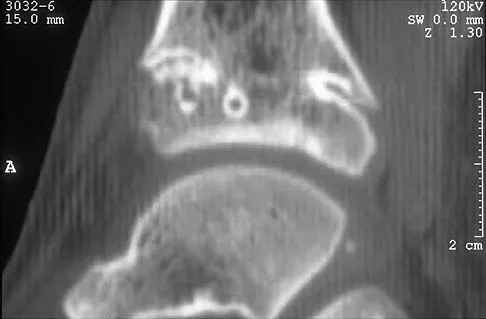
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 52
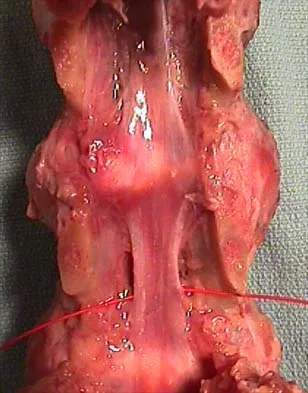
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 53
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 54
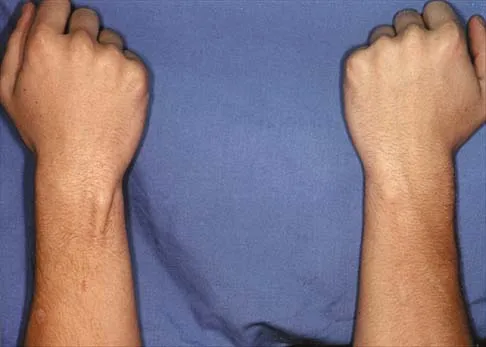
A positive Froment sign indicates weakness of which of the following muscles?


Explanation
Thumb adduction is powered by the adductor pollicis (ulnar nerve). Testing involves having the patient forcibly hold a piece of paper between the thumb and radial side of the index proximal phalanx. When this muscle is weak or nonfunctioning, the thumb interphalangeal joint flexes with this maneuver, resulting in a positive Froment sign. The paper is held by action of the thumb flexion (flexor pollicis longus and flexor pollicis brevis; median innervated).
Question 55
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?

Explanation
The patient's clinical signs (fever and flank, hip, and abdominal pain) suggest a primary iliopsoas abscess. With an increased patient population who abuse drugs and/or who are HIV-positive, iliopsoas abscess may be more prevalent because of systemic bacterial seeding and may be potentially unrecognized. Diagnostic imaging studies provide a better understanding of the anatomic magnitude of the infection, give concrete confirmation of the diagnosis, and may suggest an underlying cause. Neither standard abdominal radiographs nor ultrasound studies are sensitive enough to be diagnostic of this disease process. CT has been established as the standard study for identifying the underlying cause of this abscess. The hip infection has most likely developed as a result of hematogenous spread from an infected skin lesion from the patient's IV drug use. Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
Question 56
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?

Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Question 57
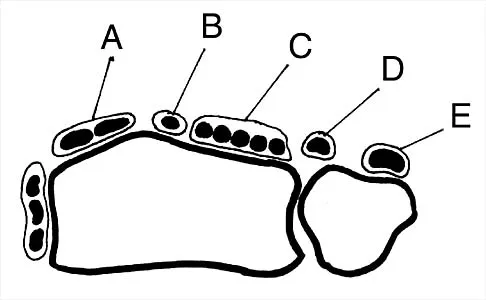
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?
Explanation
The posterior interosseous nerve in contained in the floor of the fourth dorsal compartment of the wrist, which is labelled C in this diagram. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 224.
Question 58
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?


Explanation
31b The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 59
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?

Explanation
An avulsion fracture from the lateral tibial margin carries the eponym Segond fracture and is pathognomonic for an anterior cruciate ligament (ACL) tear. The fragment is located posterior to Gerdy's tubercle and is superior and anterior to the fibular head. It represents an avulsion of the lateral capsular ligament of the knee and is caused by the same mechanism that causes the ACL tear. The pes anserinus is the insertion point of the medial hamstrings and would not be affected in a lateral avulsion injury. The posterior cruciate ligament may be seen on a lateral view if associated with an avulsion fragment, but a tear of the PCL generally cannot be diagnosed on an AP view. The insertion of the iliotibial band is broad and is unlikely to produce an avulsion injury such as that seen in the radiograph. This view is not consistent with the appearance of a lateral collateral ligament injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 60
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
The saphenous nerve is located on the posterior medial aspect of the knee and must be protected when performing an inside-out repair of the medial meniscus. The peroneal nerve is most at risk with lateral meniscal repairs. The other structures usually are not at risk with meniscal repair. Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Question 61
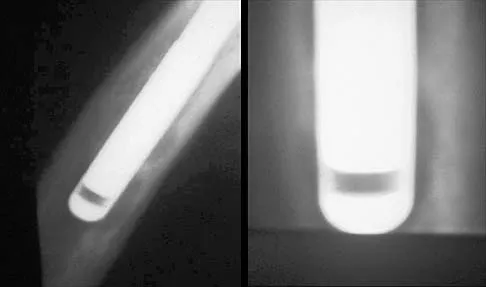
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
Osteolysis of an otherwise well-functioning total hip arthroplasty is a recognized complication, and its radiographic appearance is typical, as shown here. Distal osteolysis, such as that shown here, is more prevalent when there is noncircumferential sealing of the proximal femoral canal. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 62
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Question 63
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 64
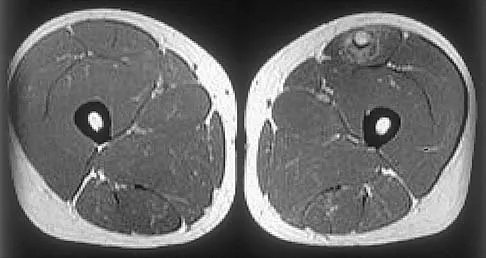
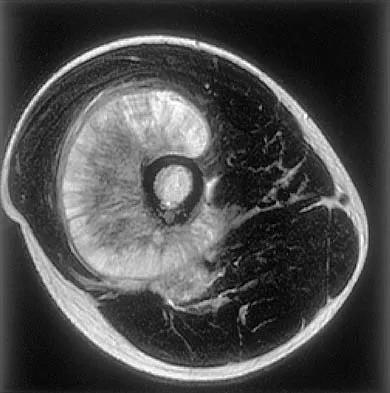
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?


Explanation
34b 34c The images reveal a region of increased signal within the rectus femoris muscle with mild, ill-defined surrounding edema. The presence of high intensity signal on the T1-weighted image favors acute blood, in this case associated with a rectus femoris muscle tear or fatty tissue. However, because of fat suppression, a fatty lesion or lipoma would be dark on STIR, rather than bright as in this image. Most foreign bodies are low intensity signal and if small, are difficult to evaluate with MRI. The lack of adjacent subcutaneous soft-tissue edema or surrounding fluid makes pyomyositis an unlikely diagnosis.
Question 65
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 66
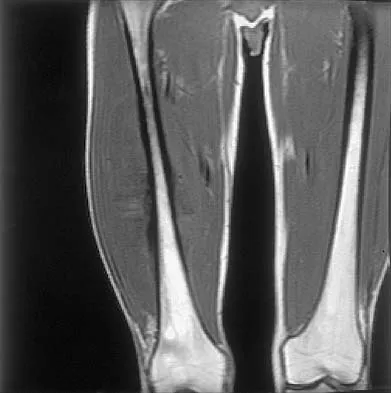
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
35b The images show a large, almost circumferential, mass surrounding the diaphysis of the femur. The intramedullary signal is normal with minimal cortical destruction, both findings that should be abnormal in conventional osteosarcoma and Ewing's sarcoma. There are very low-signal striations representing osteoid formation that would have a sunburst radiographic pattern. This indicates an osteogenic lesion. Myositis ossificans is not indicated because studies would reveal zonal ossification starting in the periphery rather than the more central pattern seen in this patient. This appearance is typical for periosteal osteosarcoma.
Question 67
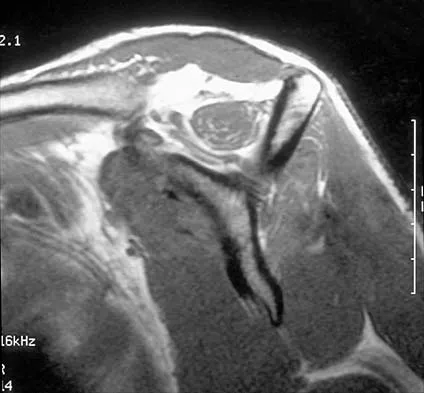
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

Explanation
36b The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 68
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
The obturator internus originates on the obturator membrane and adjacent bone, including the quadrilateral plate, and exits the lesser sciatic notch to insert on the posterior medial greater trochanter. The structure labeled C is the pectineus, B is the sartorius, and D is the gluteus medius. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Question 69
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
The great medullary artery originates as a direct or indirect branch of the left posterior intercostal artery, usually between T8 and T12. It becomes intradural and crosses over one to three disk spaces before turning to the midline where it anastomoses with the anterior spinal artery. Injury to this artery can result in devastating ischemia of the lower spinal cord. Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
Question 70
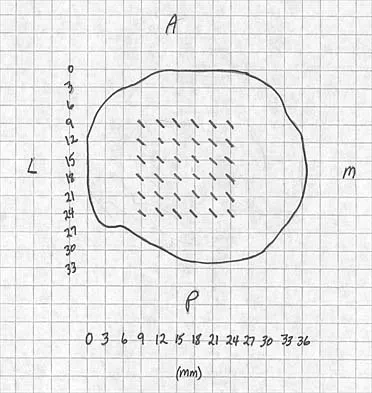
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?

Explanation
The saphenous nerve follows the saphenous vein, giving off the infrapatellar branch that crosses the knee anteriorly to supply the peripatellar skin. A longitudinal incision can interrupt the nerve, leaving the terminal distribution without sensation.
Question 71
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
The musculocutaneous nerve travels through the conjoined tendon approximately 8 cm distal to the tip of the acromion. The musculocutaneous nerve innervates the biceps muscle and the bracialis muscle, both of which are responsible for elbow flexion. Shoulder flexion is facilitated by the anterior fibers of the deltoid muscle (axillary nerve) and the supraspinatus muscle (suprascapular nerve). The subscapular muscle facilitates internal rotation of the shoulder (upper and lower subscapularis nerve). Shoulder abduction is performed by the deltoid muscle (axillary nerve), and forearm pronation is facilitated by the pronator teres (median nerve). Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Question 72
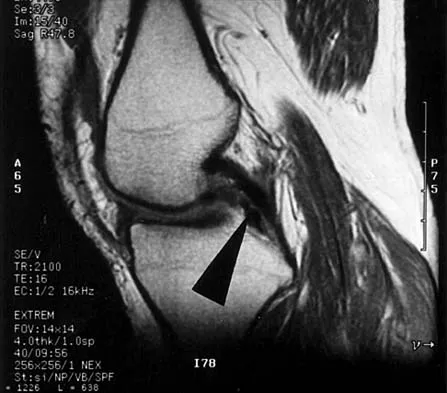
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
Question 73
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?

Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 74
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?

Explanation
The MRI scan shows near complete involvement of the femoral head with bone marrow changes and some collapse of the necrotic segment. This is most suggestive of osteonecrosis.
Question 75
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Finish Exam?
You cannot change answers after submitting.
