Question 26
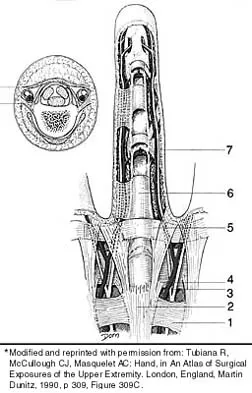
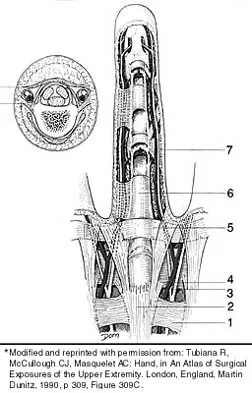
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?

Explanation
Full exposure of the volar plate of the proximal interphalangeal joint of the finger is best accomplished by incision of the distal C1, A3, and proximal C2 pulleys; followed by gentle retraction of the flexor digitorum superficialis and profundus tendons. Sacrifice of the A3 pulley, although associated with some biomechanic disadvantage, can be tolerated without causing functionally limiting bowstringing of the flexor tendon. Sacrifice of even a portion of the A2 or A4 pulleys can decrease the biomechanic leverage provided by the flexor tendon sheath, leading to bowstringing of the flexor tendons. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186. Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 1853-1855.
Question 27
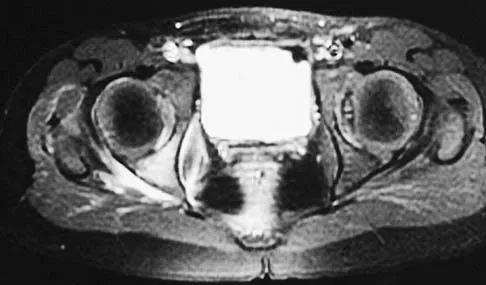
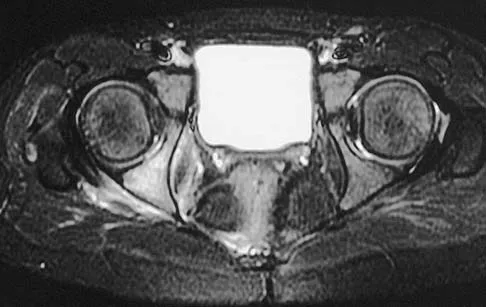
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?

Explanation
The CT scan reveals a left-sided psoas abscess. Irritation of the saphenous division of the femoral nerve can cause paresthesias along the medial aspect of the knee. Pain is usually improved with hip flexion. Cellier C, Gendre JP, Cosnes J, et al: Psoas abscess complication Crohn's disease. Gastroenterol Clin Biol 1992;16:235-238.
Question 28
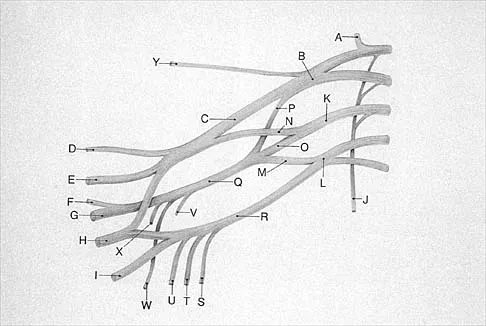
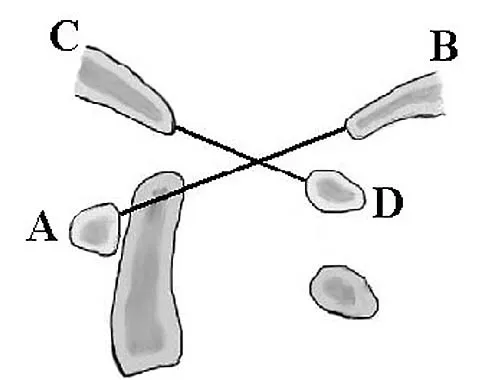
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter "A"?


Explanation
The nerve labeled A is the axillary nerve, a branch from the posterior cord. The posterior cord innervates the subscapularis, latissimus dorsi, teres major and minor, deltoid, triceps, anconeus, brachioradialis, and extensors of the forearm. The axillary nerve innervates the teres minor and deltoid. The pectoralis minor is innervated by the medial cord. The supraspinatus and the subclavius are innervated by the superior trunk. The brachialis is innervated by the lateral cord. Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Question 29
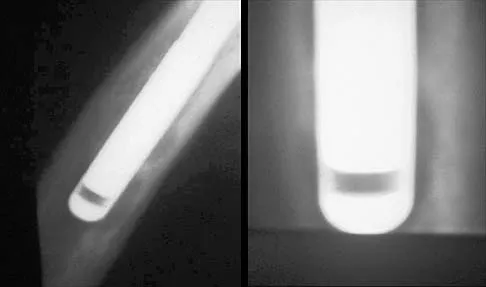
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?


Explanation
17b The major risk of performing a high tibial osteotomy is neurovascular injury. The new version of the high tibial osteotomy makes a transverse osteotomy at the level of the tibial tubercle. The osteotome is protected by the oblique belly of the popliteus muscle. The popliteal artery and vein and tibial nerve all lie posterior to the muscle. The soleus muscle originates below this level. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Question 30
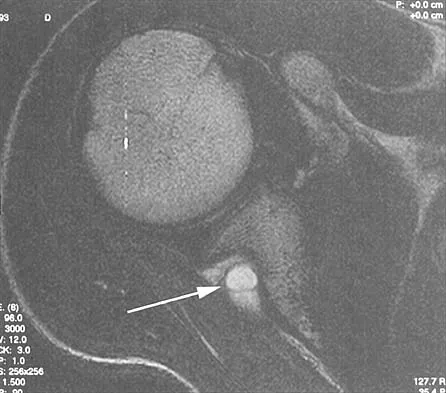
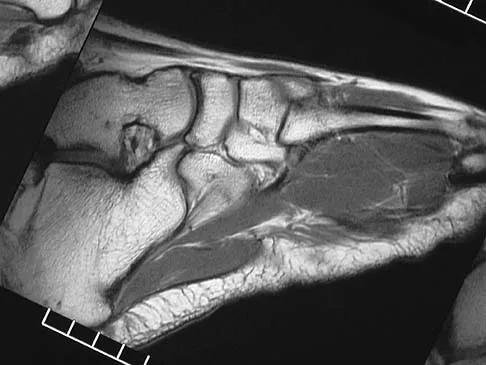
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?


Explanation
The arrow is pointing to the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long, beginning at the proximal extent of the transverse carpal ligament and ending at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches, with the deep branch of the ulnar nerve persisting distal to the canal. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel. The radial artery is on the radial side of the wrist. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Question 31
Osteonecrosis of the femoral head after intramedullary nailing in children is thought to be the result of injury to the
Explanation
All of these are possible explanations for the development of osteonecrosis following intramedullary nailing in children. However, the lateral ascending cervical artery, which supplies the epiphysis, is much more vulnerable to injury in children because it lies in the trochanteric fossa. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Question 32
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?


Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 33
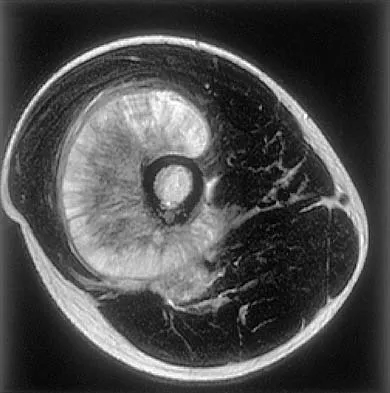
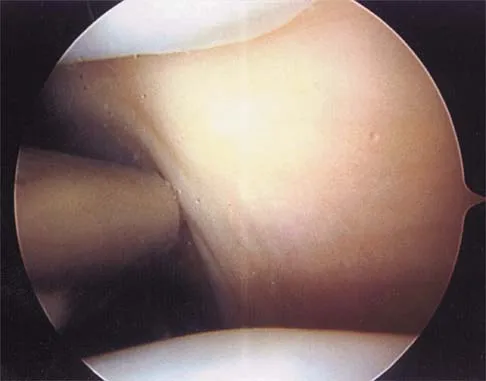
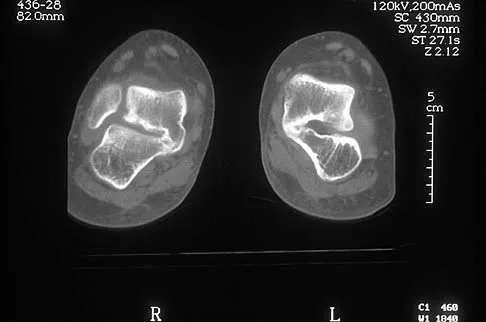
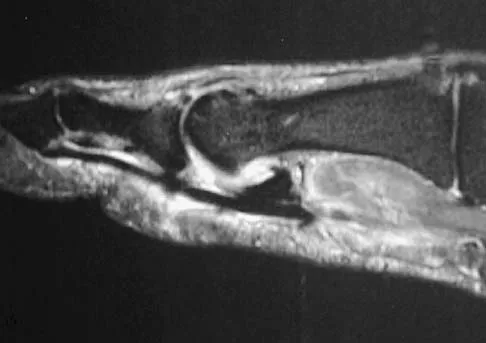
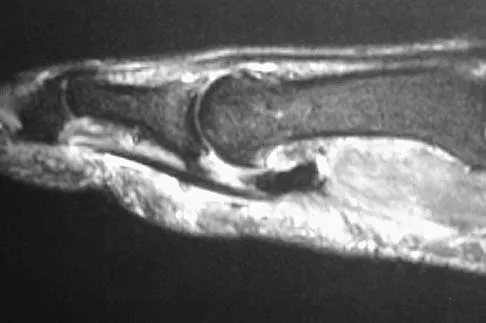
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient's left knee. Abnormal findings include

Explanation
20b The MRI scans show meniscal tissue extending across the entire lateral compartment, revealing a discoid lateral meniscus. The increased signal within the lateral meniscal tissue indicates a tear. Discoid lateral menisci are congenital variants that often present with mechanical symptoms in adolescents. The other structures in the knee are normal. Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Question 34
An ulnar nerve palsy at the level of the wrist is typically associated with deficits in the palmaris brevis, the hypothenar muscles, and what other groups of muscles?



Explanation
The intrinsic muscles innervated by the ulnar nerve include the palmaris brevis, hypothenar muscles, all of the interossei, adductor pollicis, and the deep head of the flexor pollicis brevis. The superficial head of the flexor pollicis brevis is innervated by the median nerve. Goldfarb CA, Stern PJ: Low ulnar nerve palsy. JASSH 2003;3:14-26.
Question 35
Figures 21a and 21b show the radiographs of a 22-year-old man who has had progressive pain and swelling about the knee for the past 6 weeks. Examination reveals limited range of motion and fullness about the knee. What is the most likely diagnosis?
Explanation
21b The radiographs reveal a destructive lesion in the metaphysis of the distal femur with periosteal changes and an associated soft-tissue mass with subtle mineralization. This suggests an aggressive malignant process. In this age group, the most likely diagnosis is osteosarcoma. Giant cell tumor, which usually is in a more subchondral location, is not typically so aggressive. Aneurysmal bone cyst is usually more geographic, with a well-marginated reactive rim. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 36
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the
Explanation
The Watson-Jones approach to the hip uses the intermuscular interval between the gluteus medius and the tensor fascia lata. This is not a true internervous plane, as both muscles are supplied by the superior gluteal nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 316-332.
Question 37
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the



Explanation
The flexor sheaths are in continuity with the deep spaces of the hand. The flexor sheaths of the thumb and little finger communicate with the radial and ulnar bursae, respectively, and these two bursae commonly communicate. The central digits do not communicate as readily with deep spaces of the hand but if flexor tendon sheath infection of the index, long, and right fingers is neglected, the potential exists for rupture into the deep midpalmar spaces. Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
Question 38
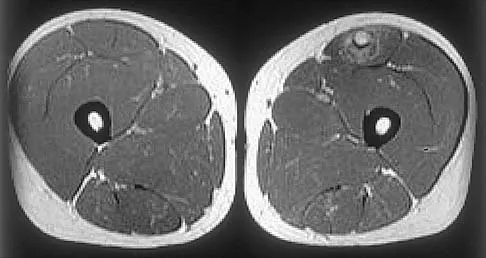
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?





Explanation
23b 23c 23d 23e The radiographs reveal a lytic subchondral lesion that has a poorly defined margin and lacks mineralization. The bone scan confirms an active lesion that has central photopenia, producing the characteristic doughnut configuration. The MRI scans confirm the presence of a subchondral lesion that is modestly expansile at the lateral plateau and has low signal intensity on the T1-weighted image and a mixed high signal on the T2-weighted image. These features strongly suggest giant cell tumor of bone, more than 50% of which appear around the knee. Simple cyst is excluded by the MRI characteristics. Fibrous dysplasia is unlikely to be in a subchondral location and typically does not show this intensity of uptake on bone scan. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Question 39
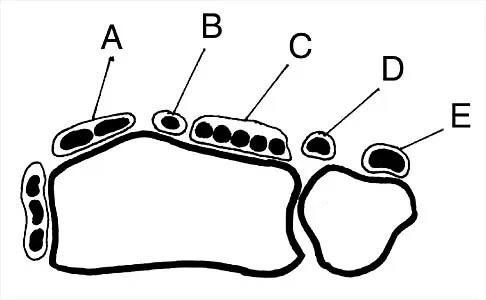
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?

Explanation
The peroneus brevis is easily identified by its location behind the fibula and its distal muscle belly. Axial MRI images provide a reliable guide even when one of the peroneals is completely ruptured, subluxated out of the peroneal groove, or absent. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
Question 40
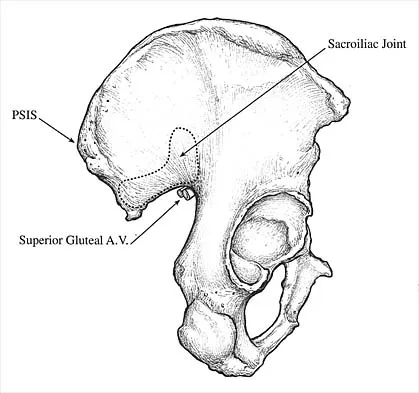
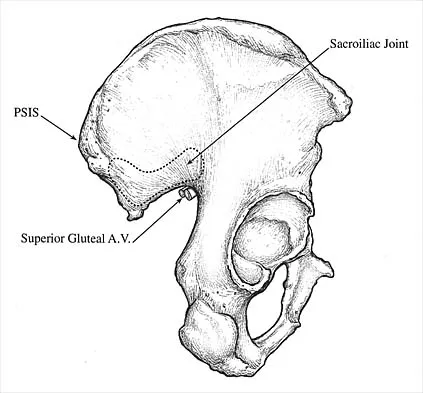
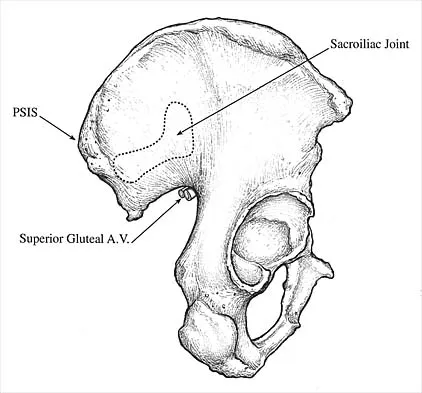
During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the


Explanation
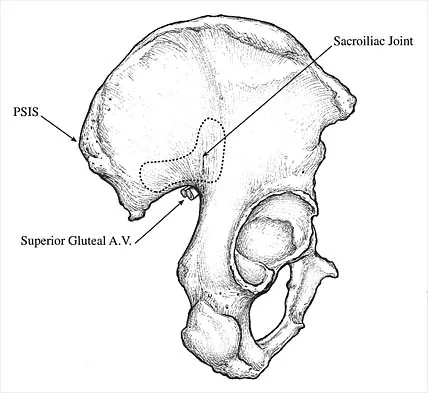
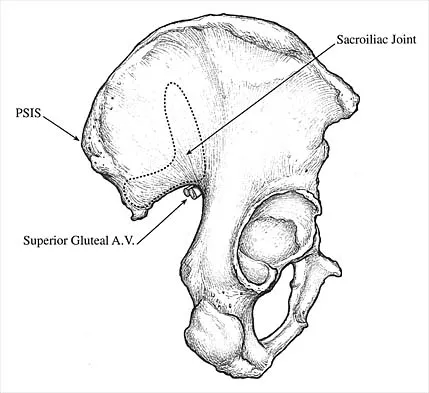
The acetabular quadrants are defined by two lines: one drawn from the anterosuperior iliac spine to the posterior fovea, forming acetabular halves, and a second drawn perpendicular to the first at the midpoint of the acetabulum, forming four quadrants. The anterior quadrants should be avoided because improper screw placement may injure the external iliac artery and vein, as well as the obturator nerve, artery, and vein. These structures lie close to the pelvic bone, with little protective interposition of soft tissue. Wasielewski RC, Cooperstein LA, Kruger MP, et al: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508.
Question 41
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 42
The brachialis muscle is innervated by what two nerves?

Explanation
The brachialis is innervated by two nerves: medially, the musculocutaneous nerve; laterally, the radial nerve. The muscle is split longitudinally to approach the humerus anteriorly. Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
Question 43
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?

Explanation
If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson's fracture. Patients with this type of injury usually require fusion. Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Question 44
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 45
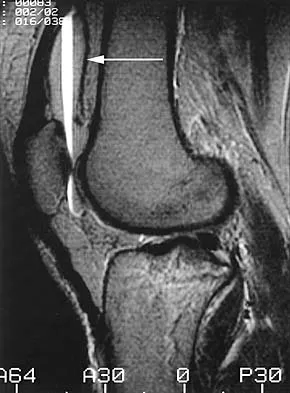
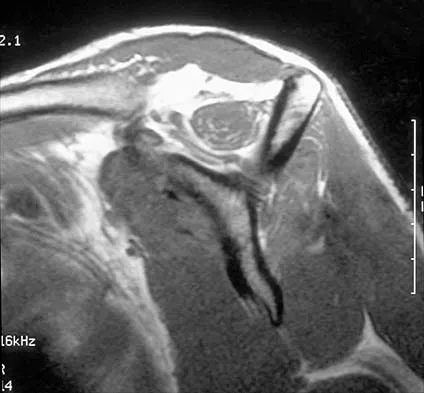
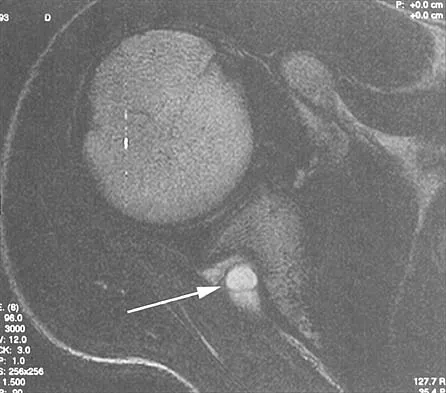
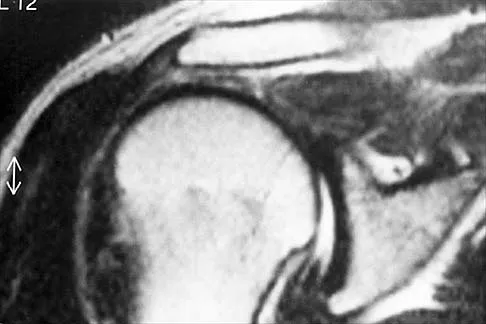
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?


Explanation
The gradient-echo MRI scan highlights the ulnar and radial arteries, as indicated by the arrow. This technique suppresses the signal of the surrounding fat and causes the stationary surrounding tissues to become intermediate in signal intensity. The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient's symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue. Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Question 46
In a postganglionic brachial plexus lesion at Erb's point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?

Explanation
In a postganglionic injury to the brachial plexus, the rhomboid muscle, innervated by the dorsal scapular nerve, would still be expected to function. This is a useful clinical sign that the brachial plexus lesion is postganglionic as opposed to preganlionic. The musculocutaneous, axillary, and suprascapular nerves are all located distal to Erb's point (the most common location of an upper nerve root brachial plexus injury), and all contain fibers from the C5 and C6 nerve roots. Therefore, these nerves are not expected to function normally following a postganglionic C5 and C6 nerve root injury. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
Question 47
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the


Explanation
The quadrangular space is bordered superiorly by the teres minor, medially by the long head of the triceps, laterally by the humerus, and inferiorly by the teres major. The posterior circumflex humeral artery and the axillary nerve lie in this space. Rockwood CA Jr, Matsen FA III: The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 70-71.
Question 48
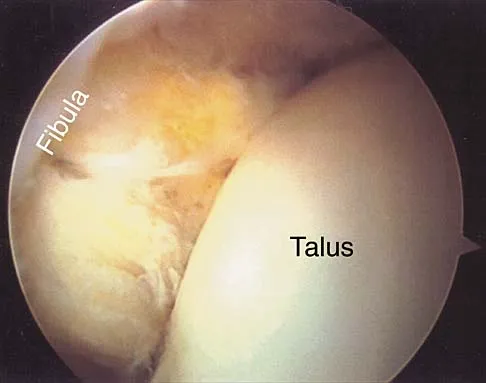
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?

Explanation
27b The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 49
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus and is subject to stretch injury if excessive retraction is applied. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal nerve and superior laryngeal nerve are both at risk during the exposure but are not located between the trachea and esophagus. An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, chapter 2.
Question 50
What is the first ossification center to appear radiographically in the pediatric elbow?

Explanation
The first ossification center to appear in the pediatric elbow is the capitellum. This ossification center generally appears between the first month and the 11th month in girls and between the first month and the 26th month in boys. The other ossification centers in the elbow appear in the following progression: radial head (3.8 to 4.5 years), medial epicondyle (5 to 6 years), olecranon (6 to 7 years), trochlea (9 to 10 years), and the lateral epicondyle (10 years). Wilkins KE, Beaty JH, Chambers HG, et al: Fractures and dislocation of the elbow region, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 657-662.
Finish Exam?
You cannot change answers after submitting.
