Question 1
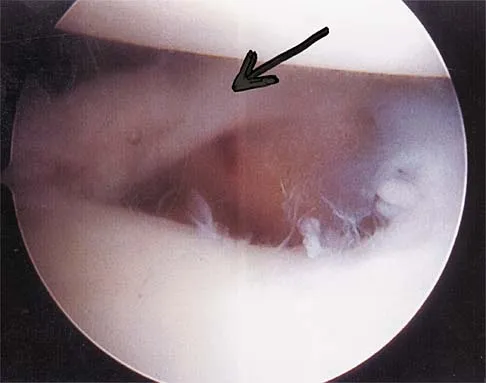
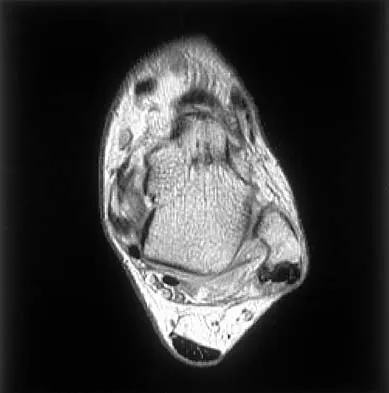
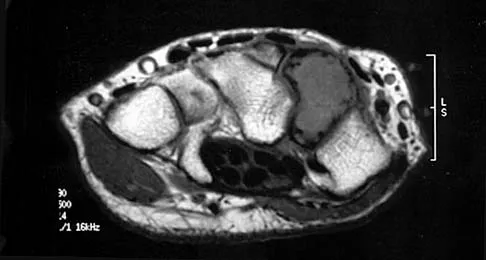
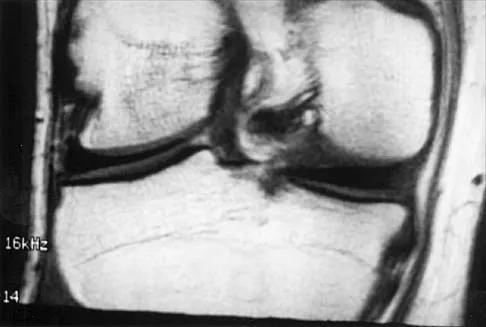
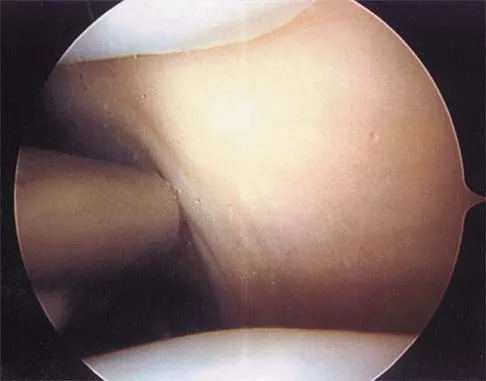
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?

Explanation
1b The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 2
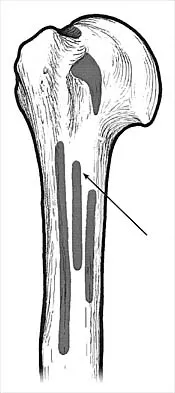
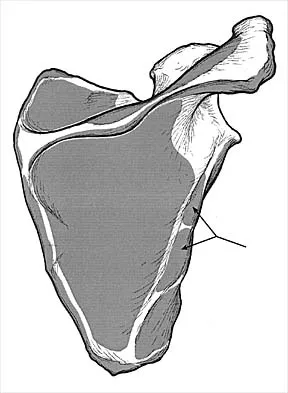
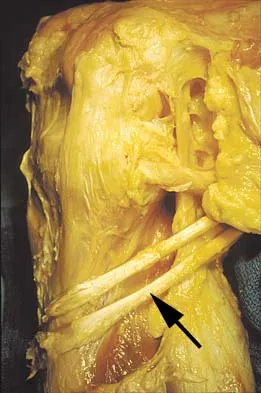
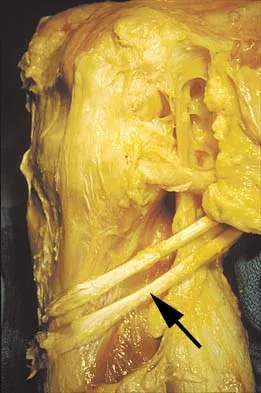
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
The latissimus dorsi inserts on the humerus metaphysis between the pectoralis major (posterior) and teres major (anterior). Teres minor inserts on the base of the greater tuberosity. Pectoralis minor does not insert on the humerus. Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Question 3
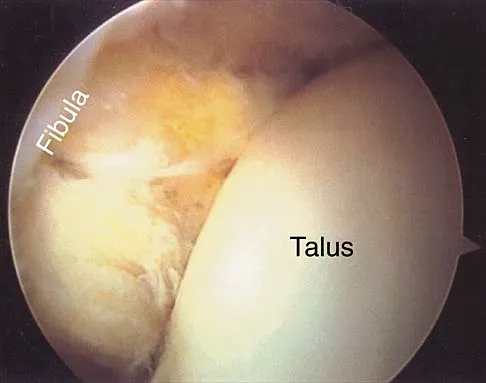
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
3b The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 4
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?

Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 5
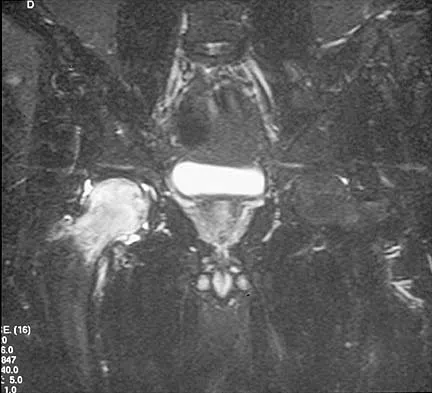
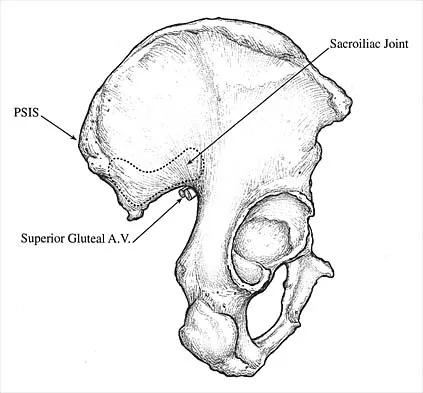
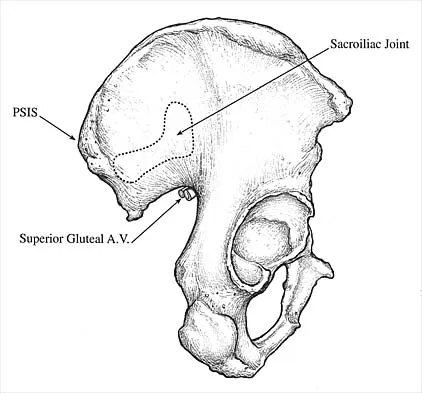
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?


Explanation
The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur. Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Question 6
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?
Explanation
Severely displaced acromioclavicular injuries disrupt the deltotrapezial fascia and muscular origin in addition to the ligaments (acromioclavicular and coracoclavicular or trapezoid and conoid). When the deltoid is still attached to the clavicle, an isometric shoulder shrug will tend to reduce the displacement. When the deltoid is detached but the trapezius is attached, this manuever will increase the deformity and surgery may be indicated.
Question 7
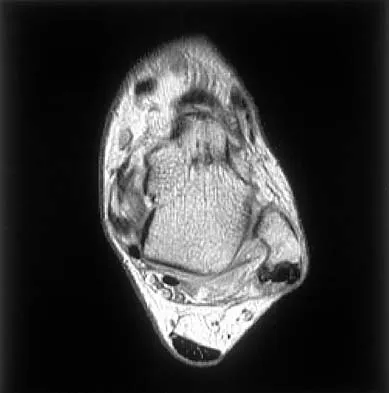
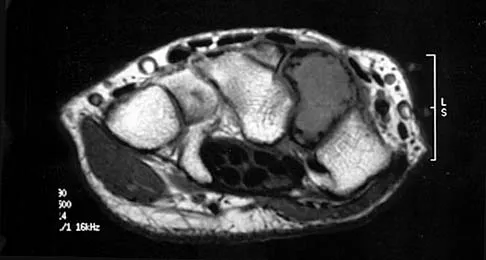
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?

Explanation
5b The figures show a longitudinal split within the peroneus brevis tendon as it courses posterior to the fibula. The peroneus longus tendon has been driven between the medial and lateral components of the peroneus brevis tendon. Peroneal split syndrome is a cause of lateral ankle pain but may be less asymptomatic in the elderly. It may be associated with tendon subluxation following a tear of the superior peroneal retinaculum.
Question 8
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?

Explanation
The ulnar collateral ligament is often difficult to visualize during elbow arthroscopy. It can be seen clearly in only 10% to 30% of elbow arthroscopies. All of the other structures should be easily and thoroughly seen and palpated during elbow arthroscopy. Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Question 9
The quadrilateral space in the shoulder contains which of the following structures?


Explanation
The quadrilateral or quadrangular space of the shoulder is formed laterally by the humerus, proximally by the subscapularis (and teres minor viewed from posterior), distally by the teres major, and medially by the long head of triceps. The posterior humeral circumflex artery and axillary nerve pass through it. The axillary artery is more proximal. The radial nerve and profunda brachii pass through a triangular space more inferior. The circumflex scapular artery passes through a triangular space more medial. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Question 10
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?


Explanation
The MRI scan reveals an abnormal signal in the trapezoid, which lies adjacent to the capitate in the distal carpal row. The tumor is a giant cell tumor of bone. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240. bar based on these measurements is shown in Figure 54d. Initial treatment should consist of 1- bony bar resection and distal fibula epiphysiodesis. 2- bony bar resection and corrective osteotomy. 3- bony bar resection and physiodesis of the opposite distal tibial physis. 4- corrective osteotomy and a limb-lengthening procedure. 5- corrective osteotomy and physiodesis of the opposite distal tibial physis. 2 54a 54b 54c 54d Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 11
The recurrent motor branch of the median nerve innervates which of the following muscles?
Explanation
The recurrent motor branch of the median nerve supplies the thenar muscles (abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis) that are primarily responsible for thumb opposition. The nerve can be injured in carpal tunnel release. A branch of the nerve also supplies the first lumbrical. The adductor pollicis and the interossei are supplied by the ulnar nerve. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 12
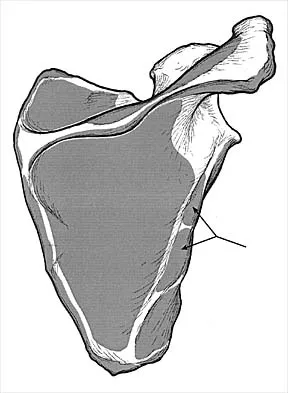
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?

Explanation
Teres minor originates from the middle third of the dorsal surface of the lateral border of the scapula. It is supplied by the axillary nerve (C5). Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
Question 13
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?

Explanation
Based on the MR arthrogram in which gadolinium (bright on T1-weighted images) was injected into the joint space prior to imaging, the study shows a tear of the anterior band of the ulnar collateral ligament (UCL). The disruption in the distal end of the UCL is outlined by contrast. A small collection of contrast extravasation into the flexor musculature further confirms the presence of a tear. The UCL has a broad-based attachment on the medial epicondyle and has a pointed or tapered attachment distally on the ulna. Most UCL tears occur distally at the ulnar (coronoid) attachment. MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 14
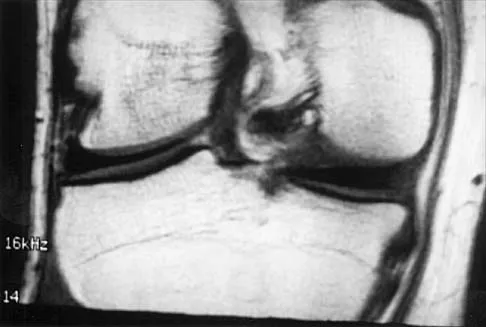
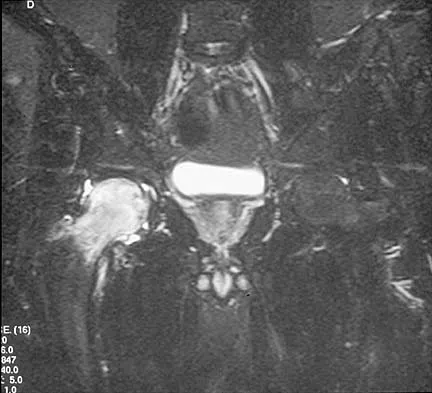
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?



Explanation
9b 9c A discoid meniscus is a large disk-like meniscus. It is seen in the lateral meniscus in 3% of the population; a discoid medial meniscus is much less common. It can be identified on the coronal view by noting meniscal tissue extending into the tibial spine at the intercondylar notch. The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 15
The gluteus maximus is innervated by which of the following nerves?

Explanation
The inferior gluteal nerve supplies the gluteus maximus muscle. The superior gluteal nerve supplies the gluteus medius, gluteus minimus, and tensor fascia lata muscles. The femoral nerve supplies the quadriceps, sartorius, and pectineus muscles. The pudendal nerve is primarily a sensory nerve.
Question 16
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 17
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 18
A purulent flexor tenosynovitis of the thumb may communicate with the small finger flexor through which of the following structures?

Explanation
Only the flexor sheaths of the thumb and small finger are continuous from the digit through the carpal canal and into the distal forearm. If one of the sheaths ruptures from synovitis, it may contaminate the other sheath through Parona's space in the distal forearm. This potential space lies superficial to the pronator quadratus and deep to the flexor tendons. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1044-1045.
Question 19
Which of the following nerves travels with the deep palmar arch?
Explanation
The ulnar nerve divides alongside the pisiform, and the deep branch supplies the three hypothenar muscles and crosses the palm with the deep palmar arch to supply the two ulnar lumbricals, all interossei, and finally the adductor pollicis. The superficial branch supplies the ulnar digital branches to the small and ring fingers. The median nerve branches are more superficial in the palm near the superficial palmar arch. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 20
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?


Explanation
10b 10c Transient osteoporosis is a self-limited painful but reversible disorder. Although first described in pregnant women, it is more common in young to middle-aged men. The radiograph shows loss of mineralization in the right hip relative to the left side. There is no osseous destruction or cortical expansion typical of metastasis or giant cell tumor. The process is confined to the femoral side of the joint unlike rheumatoid arthritis, which would be centered in the joint. Osteonecrosis is better defined with sharp but irregularly shaped margins, and there is no double-line sign. The MRI scans reveal diffuse edema in the femoral head and neck that is atypical for osteonecrosis. Transient osteoporosis may recur in the same or opposite hip.
Question 21
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
The semitendinosus and gracilis tendons lie beneath the superficial fascia and superficial to the medial collateral ligament. The semitendinosus is located more inferior to the gracilis tendon. The sartorius is more posterior and distal as is the medial collateral ligament. The semimembranosus is posterior. Pagnani MJ, Warner JJ, O'Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Question 22
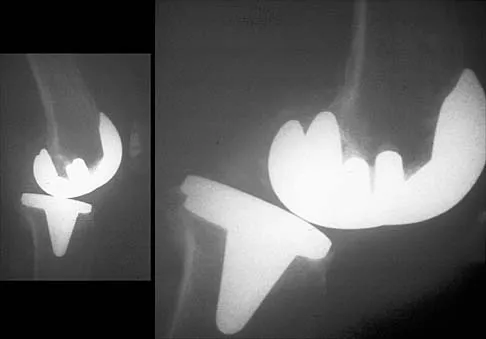
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?

Explanation
The figure shows a supracondylar process, which is a normal anatomic variant. An osteochondroma tends to occur more toward the end of bones, and the medullary space of the underlying bone extends into the base of the osteochondroma. The presence of a supracondylar process is usually asymptomatic. However, the ligament of Struthers that always extends from the supracondylar process to the medial epicondyle can result in median nerve entrapment secondary to trauma. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Question 23
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?

Explanation
The first branch of the lateral calcaneal nerve innervates the abductor digiti minimi. It is reported to be trapped at the interval between the abductor hallucis and the quadratus plantae muscles.
Question 24
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 25
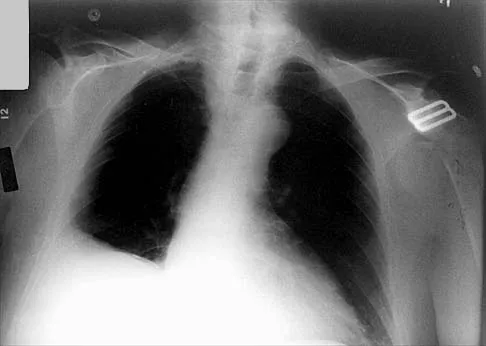
Which of the following findings is seen in the chest radiograph shown in Figure 13?
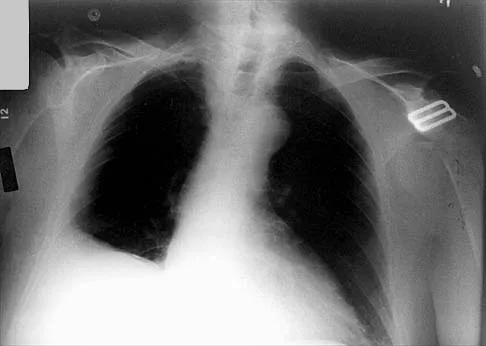

Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
Finish Exam?
You cannot change answers after submitting.
