Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
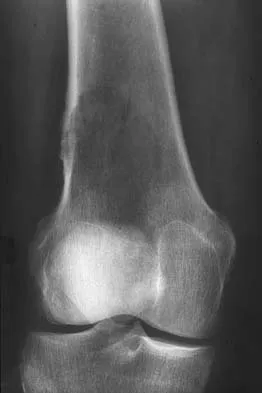
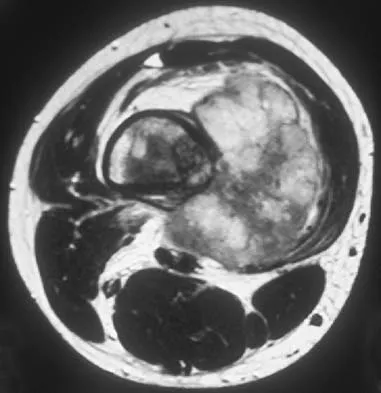
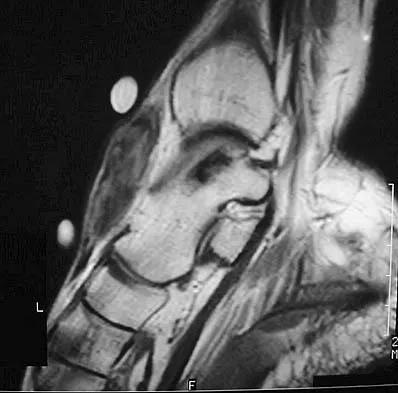
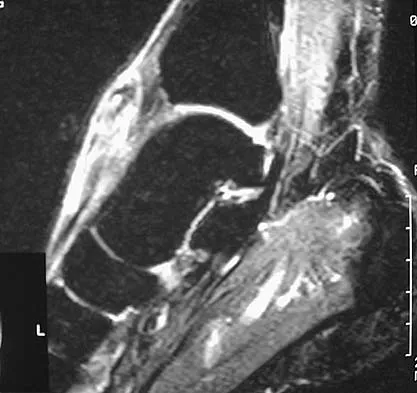
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?


Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 2
High Yield
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 3
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?

Explanation
The patient has symptomatic primary osteoarthritis of the elbow with multiple loose bodies. Given his age and occupation, an elbow arthroplasty is not an option. Arthroscopic debridement and removal of loose bodies has been shown to be effective for osteoarthritis of the elbow. Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Question 4
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
The pectoralis major insertion is just lateral to the long head of the biceps tendon. Medial to the biceps is the insertion for the teres major and latissimus dorsi. The short head of the biceps originates on the coracoid process. The subscapularis inserts on the lesser tuberosity just medial to the biceps.
Question 5
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?

Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 6
High Yield
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Detailed Explanation
The patient has patellar tendinitis (jumper's knee). It is a common overuse condition seen in runners, volleyball players, soccer players, and jumpers but can be seen in any activity in which repeated extension of the knee is required. In the acute setting, the pain is well localized and there is tenderness and sometimes swelling of the tendon. MRI is recommended for evaluating chronic cases and for surgical planning. In the acute phases, ice, rest, and avoidance of the offending activity are recommended. Weakness of the quadriceps and hamstring muscle are thought to contribute to this problem; therefore, stretching and isometric exercise in a limited range of motion are important. Complete rest and intratendinous injections of steroids are detrimental to tendon physiology. Stanish WD, Rubinovich RM, Curwin S: Eccentric exercise in chronic tendinitis. Clin Orthop 1986;208:65-68.
Question 7
High Yield
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 8
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?


Explanation
While difficult to appreciate on the AP radiograph of the shoulder, the increased physeal signal demonstrated on the axial MRI scan is consistent with a nondisplaced growth plate fracture. A comparison radiograph of the left shoulder also could be considered and the injured shoulder evaluated for physeal widening. Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents. The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve. Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Question 9
High Yield
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?


Explanation
Solitary bone lesions require biopsy, for there is the possibility that the lesion may represent a primary bone sarcoma, which will necessitate a different treatment plan. This is especially true in patients with remote histories of cancer. The most likely cause of a lytic bone lesion in a patient older than age 40 years is a metastatic lesion. Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 10
High Yield
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 11
Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
Explanation
The most important aspect in the decision for surgery in an acetabular fracture is the ability of the femoral head to remain concentrically reduced under the dome in AP and Judet oblique views of the pelvis. If this parameter is present, then the need for surgery is determined by other aspects such as fragmentation, age, incongruity, and displacement. If the head remains stable under the dome without traction, there is sufficient acetabular dome to provide stability, and nonsurgical treatment may be appropriate. Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354. Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Question 12
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?

Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 13
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the

Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 14
High Yield
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include

Detailed Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 15
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
A total hip arthroplasty using the posterior approach has resulted in hip dislocation under certain circumstances. Reconstruction of the external rotator/capsular complex is recognized as a stability-enhancing mechanism for the posterior approach. During the procedure, the acetabular component should be placed in 15 to 20 degrees of anteversion and approximately 45 degrees of abduction. Relative retroversion is a risk factor for posterior dislocation. High abduction angles result in edge loading of the polyethylene and possible early failure, as well as an increased risk of dislocation. Smaller diameter heads and skirted neck extensions used together decrease the range of motion that is allowed before impingement occurs, and this can result in dislocation. Shorter neck lengths generally result in soft-tissue envelope laxity. If laxity occurs, increased offset, neck length, or both can improve stability. Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Question 16
High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 17
High Yield
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
The most common cause of recurrent dislocation following total hip arthroplasty continues to be component malposition. Component malposition should be addressed prior to any other treatment options, such as increasing soft-tissue tension with increased femoral offset or greater trochanteric advancement. A larger femoral head size may help, but correcting the component malposition should give more predictable results. A retroverted acetabular component should be revised to 15 degrees to 20 degrees of anteversion, matching the patient's anatomy with an abduction angle close to 45 degrees. Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343. Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Question 18
High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?

Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 19
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?

Explanation
Posttraumatic osteolysis of the distal portion of the clavicle is a condition that can be a complication of acute or repetitive trauma. The distal end of the clavicle is frayed and resorbed. Resorption may occur after weeks or months. The end of the clavicle may reconstitute over a period of months, or the acromioclavicular joint may remain widened. The differential diagnosis for distal clavicular erosion also includes rheumatoid arthritis, hyperparathyroidism, neoplastic destruction, cleidocranial dysplasia, and pyknodysostosis. Acutely, a type 2 acromioclavicular joint injury does not result in erosion or resorption of the clavicle. Periosteal sleeve injuries radiographically mimic acromioclavicular joint dislocation. Rickets occurs only in childhood.
Question 20
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 21
High Yield
The dose of the chemotherapeutic agent doxorubicin (Adriamycin) is limited by which of the following factors?
Explanation
Doxorubicin is a chemotherapeutic agent that is best known for dose-limiting cardiotoxicity. This is related not only to the cumulative dose, but also the rate of infusion.
Question 22
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?


Explanation
The CT scans show a burst fracture that results from an axial load injury. The radiographic hallmark of a burst fracture is compression of the posterior cortex of the vertebral body with retropulsion of bone into the spinal canal. AP radiographs often show widening of the interpedicular distance with a fracture of the lamina. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 23
High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 24
High Yield
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Question 25
High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 26
High Yield
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of


Detailed Explanation
The complications of femoral neck fractures in children include osteonecrosis, malunion, nonunion, and premature physeal closure. It is presumed that the risk of osteonecrosis is directly related to the amount of displacement at the time of injury and is not affected by the type of treatment. The risk of the other complications can be decreased depending on the type of treatment. Anatomic reduction by either closed or open methods can reduce the risk of malunion. The addition of internal fixation allows for maintenance of the reduction. In young children who cannot comply with a partial or non-weight-bearing status, the addition of a spica cast gives added protection. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 27
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of

Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 28
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 29
High Yield
A 6-year-old boy with spastic diplegic cerebral palsy has a crouched gait. Examination reveals hip flexion contractures of 15 degrees and popliteal angles of 70 degrees. Equinus contractures measure 10 degrees with the knees extended. Which of the following surgical procedures, if performed alone, will worsen the crouching?

Detailed Explanation
Children with spastic diplegic cerebral palsy often have contractures of multiple joints. Because the gait abnormalities can be complex, isolated surgery is rarely indicated. To avoid compensatory deformities at other joints, it is preferable to correct all deformities in a single operation. Isolated heel cord lengthening in the presence of tight hamstrings and hip flexors will lead to progressive flexion at the hips and knees, thus worsening a crouched gait. Split posterior tibial tendon transfer is used for patients with hindfoot varus, which is not present in this patient. Gage JR: Distal hamstring lengthening/release and rectus femoris transfer, in Sussman MD (ed): The Diplegic Child. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 324-326.
Question 30
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?


Explanation
The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age. Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259. Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Question 31
High Yield
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of

Explanation
The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence. Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Question 32
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 33
High Yield
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?

Detailed Explanation
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Question 34
High Yield
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 35
High Yield
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 36
High Yield
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?

Explanation
The grading of response to chemotherapy for osteosarcoma was introduced by Huvos and associates. Patients with tumors that show more than 90% necrosis after neoadjuvant chemotherapy are considered to have had a good response and have better survival rates than those with less than 90% necrosis. However, it should be noted that survival rates for patients with a poor response are still better than in patients who do not receive neoadjuvant chemotherapy. More recently, similar results have been reported in patients with Ewing's sarcoma. Chemotherapy is not typically used for giant cell tumor of bone. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Question 37
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Creatine is currently used as a nutritional supplement in an attempt to enhance athletic performance. The physiologic basis for its use is based on its conversion by CK to PCr, which acts as an energy reservoir in muscle cells for the production of ATP. A number of studies that examined the effect of creatine supplementation on performance concluded that while creatine does not increase peak force production, it can increase the amount of work done in the first few anaerobic short duration, maximal effort trials. The mechanism for this enhancement of work is unknown, but it is most likely secondary to the increase in the available PCr pool. Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110. Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571. Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Question 38
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?

Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 39
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 40
High Yield
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include

Explanation
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 41
Linazolid exerts its antimicrobial action by inhibiting bacterial
Explanation
Linazolid is the first agent of the oxazolidinone group of antibiotics and is very active against methicillin-sensitive Staphylococus aureus, S epidermidis, and vancomycin-resistant enterococci. The drug has no gram-negative activity. Linazolid inhibits protein synthesis by blocking formation of the 70S ribosomal translation complex. This mechanism of action is unique to the oxazolidinones. Rybak MJ, Cappelletty DM, Moldovan T, et al: Comparative in vitro activities and postantibiotic effects of the oxazolidinone compounds eperezolid (PNU-100592) and linezolid (PNU-100766) versus vancomycin against Staphylococcus aureus, coagulase-negative staphylococci, Enterococcus faecalis, and Enterococcus faecium. Antimicrob Agents Chemother 1998;42:721-724.
Question 42
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 43
High Yield
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?

Explanation
The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Question 44
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 45
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of


Explanation
The radiographs show well-fixed components of a posterior cruciate-retaining total knee replacement. The relative position of the femoral component is anteriorly subluxated relative to the tibial component. The AP radiograph shows that the articular space is markedly asymmetric, indicating either failure or fracture of the polyethylene or subluxation of the femur relative to the tibia. The patient's symptoms suggest a failure of the posterior cruciate ligament that is consistent with the radiographic findings; therefore, the treatment of choice is revision to a posterior cruciate-substituting implant.
Question 46
Figures 43a and 43b show the AP and lateral radiographs of the radius and ulna of a 9-year-old patient. The fracture is manipulated and placed in a long arm cast with the elbow flexed to 90 degrees and the forearm to neutral rotation. Figures 43c and 43d show the alignment of the fracture after the manipulation. What is the next most appropriate step in management?




Explanation
By placing the forearm at neutral rotation, as shown in Figures 43c and 43d, the distal fragment has become malrotated by 90 degrees. This is evident by the fact that the bicipital tuberosity is rotated 90 degrees to the radial styloid. Normally, it should be directly opposite (180 degrees) to the radial styloid. The correct alignment was present in the original radiographs shown in Figures 43a and 43b. Another clue to the malrotation in the postreduction radiographs is the difference in the diameters of the opposing radial shafts. To correct this rotational malalignment, the distal fragment needs to be remanipulated into supination so that it is correctly aligned with the supinated proximal radius. Evans EM: Fractures of the radius and ulna. J Bone Joint Surg Br 1951;33:548-561.
Question 47
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?



Explanation
The patient has an AP I pelvic ring disruption with minimal symphyseal widening. The best treatment is nonsurgical management and weight bearing as tolerated. This will help close the anterior pelvic ring during the healing process. Pelvic binders are excellent for acute treatment of widely displaced pelvic fractures but are not recommended for long-term use. Open reduction and internal fixation is not indicated for this injury and furthermore, the posterior ring is not injured. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems SA, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 48
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?



Explanation
A destructive mixed lytic and blastic metaphyseal lesion with a large soft-tissue mass in an adolescent is most likely an osteosarcoma until proven otherwise. The epicenter of the tumor is on the surface of the bone, most likely involves the periosteum, and is more likely to be chondroblastic in nature. Parosteal osteosarcoma is a low-grade tumor, much more radiodense, usually smaller, and found in the posterior distal femur of middle-aged patients. Chondrosarcomas are distinctly rare in childhood.
Question 49
High Yield
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
Explanation
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation. Riegler HP, Routson T: Complications of deep puncture wounds of the foot. J Trauma 1979;19:18-22.
Question 50
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Explanation
The patient has an avulsion of the flexor digitorum profundus. Treatment should include surgical exploration and tendon reinsertion. This is not an avulsion of the flexor digitorum superficialis because the patient's deficiency is the inability to flex the distal interphalangeal joint, not the proximal interphalangeal joint. Surgical release of the anterior interosseous nerve is not indicated because the flexor digitorum profundus of the ring finger is innervated by the ulnar nerve. A median nerve contusion causes wrist pain and/or numbness and tingling in the median nerve distribution. Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 1851-1897.
Question 51
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of

Explanation
The radiograph shows a type IIa Hangman's fracture, and the classic treatment is halo vest immobilization. Traction should be avoided in type IIa injuries because of the risk of overdistraction. A lesser form of immobilization such as a hard collar or a Minerva jacket can be used for nondisplaced (type I) fractures. Surgery generally is reserved for type III fractures (includes C2-3 facet dislocation), or extenuating circumstances such as multiple trauma or other fractures of the cervical spine that require surgical stabilization. Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 52
High Yield
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?


Explanation
The patient has a rotational stress fracture of the proximal humeral physis (Little Leaguer's shoulder). The symptoms of increasing pain with activity and relief with rest are typical of a stress injury. Treatment should consist of cessation of throwing activity but rehabilitation of the shoulder girdle muscles. The pitching technique should be evaluated as well. Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 53
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 54
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 55
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of

Explanation
Infantile tibia vara is a developmental condition characterized by a varus angulation of the proximal end of the tibia that is caused by a growth disturbance of the proximal medial physis. In a study of 42 affected extremities in 24 children younger than age 3 years, it was found that daytime ambulatory brace treatment favorably altered the natural history of tibia vara. Another study of 27 patients with stage II Langenskiöld disease found a success rate of 70% (improved alignment without the need for osteotomy) using brace treatment. These authors also noted that children with unilateral disease were more likely to obtain correction of the deformity compared with those with bilateral disease. In this patient, observation is not warranted because untreated tibia vara has a significant risk for progressive worsening. Osteotomy is best reserved for those patients who, despite bracing, do not show satisfactory clinical and radiographic improvement by age 4 years. Elevation of the medial tibial plateau is a treatment option for older patients who have more advanced disease. An MRI scan would not provide any useful clinical information at this time. Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109. Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount's disease. J Pediatr Orthop 1998;18:374-380.
Question 56
Figure 10 shows the radiograph of an 18-year-old woman who sustained a spinal cord injury in a motor vehicle accident. Based on the radiographic findings, her injury is best described as

Explanation
The Allen and Ferguson mechanistic classification system is a useful tool for evaluating cervical spine injuries. Cervical fractures are classified as compressive extension, distractive extension, compressive flexion, distractive flexion, vertical compression, and lateral flexion. The patient has a distractive flexion injury.
Question 57
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
Both myeloma and lymphoma are more responsive to radiation therapy. The other types of tumors are relatively more resistant to radiation. Doses of 25 to 50 Gy (2,500 to 5,000 cGy) are usually sufficient for myeloma and lymphoma, while carcinomas frequently require a higher dosage. Large cell lymphoma of bone is usually of B-cell origin and is treated with chemotherapy and radiation therapy. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Question 58
High Yield
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?

Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 59
High Yield
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 60
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?


Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 61
High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?

Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 62
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
Advances in development of new tumor markers and techniques of antigen retrieval have enhanced the sensitivity and reliability of identifying the primary source of metastasis. New markers such as CK7, CK20, CA125, and thyroid transcription factor-1 (TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene). Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Question 63
High Yield
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of

Explanation
The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Question 64
High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 65
High Yield
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?

Explanation
The ulnar collateral ligament is often difficult to visualize during elbow arthroscopy. It can be seen clearly in only 10% to 30% of elbow arthroscopies. All of the other structures should be easily and thoroughly seen and palpated during elbow arthroscopy. Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Question 66
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?

Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 67
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 68
What is the most common primary malignant tumor of bone in childhood?
Explanation
Osteosarcoma is the most common primary malignant tumor of bone in childhood, followed by Ewing's sarcoma. Rhabdomyosarcoma is a soft-tissue sarcoma of childhood. Chondrosarcoma rarely occurs in childhood. Osteochondroma is a benign tumor of bone. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Question 69
High Yield
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Detailed Explanation
An inability to participate in athletics generally is considered an indication for continued symptomatic treatment only. All of the other answers suggest the possibility of more significant pathology that may require more urgent treatment. Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
Question 70
High Yield
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 71
High Yield
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of

Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 72
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?

Explanation
The work-up for a patient with an unknown primary lesion that is metastatic to bone includes a search for the primary tumor and other sites of metastasis. This involves conducting a thorough history and physical examination, appropriate laboratory studies, bone scan, chest radiograph, and CT of the chest, abdomen, and pelvis. In women, a mammogram may be indicated. CT of the brain is not necessary in the early stages of a metastatic work-up. Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Question 73
High Yield
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?


Detailed Explanation
The radiographs reveal a blastic lesion of the proximal tibial metaphysis with cortical destruction, mineralization extending into the soft tissue laterally, indistinct margins, and destruction of the normal trabecular pattern. In this age group, with this aggressive appearance, osteosarcoma is the most likely diagnosis. Chondroblastoma and giant cell tumor are generally geographic and lytic. Chondrosarcoma is rare in this age group and would likely be a secondary lesion from an underlying chondroid tumor that is not present here. Whereas infection can have a wide variety of appearances, it tends to be more lytic in the acute presentation. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 74
High Yield
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10 degrees of hip abduction on the left and 30 degrees on the right with the hips and knees extended. The Thomas test shows 20 degrees of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0 degrees on the left and -10 degrees on the right. The neck shaft angles are 170 degrees bilaterally. Which of the following procedures would offer the best results?
Detailed Explanation
The patient has bilateral subluxated hips, with nearly vertical neck shaft angles; therefore, the treatment of choice is varus derotation osteotomy. Shortening of the bone on one or both sides may be necessary to allow adequate range of motion postoperatively. In patients this age and with this degree of bony deformity, soft-tissue releases are not likely to lead to hip stability. Botulinum toxin has been shown to be effective in the treatment of ankle equinus, but its efficacy in other areas has not been demonstrated as yet. The indications for obturator neurectomy are unclear at present. Proximal femoral resection is a salvage procedure for long-standing hip dislocations that are symptomatic and not reconstructable. Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Question 75
A 10-year-old girl was thrown over the handlebars of her bicycle and landed directly on her left shoulder. She was treated with a figure-of-8 strap and analgesics. Follow-up examination 2 weeks later reveals that the lateral end of the clavicle is superiorly dislocated relative to the acromion. A radiograph of the shoulder shows calcification lateral to the coracoid process at the level of the acromion, and the clavicle is superiorly displaced. Management should consist of
Explanation
In adults, a direct blow on the acromion usually results in an acromioclavicular dislocation. In children, however, the usual injury from this mechanism is a physeal fracture of the lateral clavicle. The clavicular shaft fragment, analogous to the metaphyseal portion of a physeal fracture, herniates through the periosteum, leaving the distal periosteal sleeve in contact with the lateral (distal) physeal fragment. The treatment of choice is immobilization until the patient is pain-free. Falstie-Jensen S, Mikkelsen P: Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-369.
Question 76
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include


Explanation
Fractures through the cartilage on the inferior pole of the patella, the so-called sleeve fracture, are often difficult to diagnose because of the paucity of ossified bone visible on the radiographs. If the fracture is missed and the fragments are widely displaced, the patella may heal in an elongated configuration that may result in compromise of the extensor mechanism function. The treatment of choice is open reduction and internal fixation using a tension band wire technique to achieve close approximation of the fragments and restore full active knee extension. Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Question 77
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 78
High Yield
An acetabular reinforcement cage is most often indicated for which of the following conditions?
Explanation
An acetabular reinforcement cage is required infrequently except when there is pelvic discontinuity in which there is no posterior column support of the acetabular cup. A larger cup inserted with cement and morselized bone graft is an effective technique for contained cavitary and anterior wall defects. Zone 1 osteolysis and a medial wall defect are essentially the same as a contained cavitary defect and can be reconstructed using cementless cups. Berry DJ, Lewallen DG, Hanssen A, Cabanela ME: Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am 1999;81:1692-1702.
Question 79
High Yield
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of


Detailed Explanation
The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy. Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Question 80
High Yield
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of

Detailed Explanation
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis. Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Question 81
High Yield
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Detailed Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 82
High Yield
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 83
The additional risk of complications in organ transplant patients receiving a total joint arthroplasty is attributed to
Explanation
Tannenbaum and associates found that patients who had a joint replacement after an organ transplantation had a rate of infection of 19% (five of 27 joint replacements in 16 patients). They retrospectively reviewed the results of 35 joint (hip or knee) replacements in 19 patients who had an organ transplant. The patients received a standard immunosuppressive induction regimen at the time of the transplantation and were maintained on a combination of prednisone, azathioprine, and cyclosporin A. All patients received antibiotics perioperatively, but antibiotic-impregnated bone cement was not used for any procedure. Six joint replacements in three patients (median patient age of 48.2 years at the time of the arthroplasty) were performed before a renal transplantation. Twenty-four joint replacements in 14 patients (average patient age of 40.9 years at the time of the arthroplasty) were performed after an organ transplantation. Two patients, with an average age of 53.8 years at the time of the arthroplasty, each had a joint replacement both before and after a liver transplantation (a total of five joint replacements). The average duration of follow-up after the first joint replacement was 8.8 years (range, 1 to 23 years). An infection developed around the implant in five patients who had undergone the joint replacement after a transplantation. The average interval from implantation of the prosthesis until detection of the infection was 3.4 years (range, 1 to 6 years). Of two patients who underwent a liver transplant, one had Pseudomonas aeruginosa infection and the other Escherichia coli infection. Of three patients who underwent a renal transplantation, one was infected with Staphylococcus epidermidis, one with Enterococcus, and one with Serratia marcescens.
Question 84
High Yield
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?



Explanation
Congenital vertical talus is a fixed dorsal dislocation of the talonavicular joint with equinus of the ankle joint. The AP radiograph shows valgus of the midfoot and an increased talocalcaneal angle; the lateral radiograph shows a vertically positioned talus and equinus of the ankle joint, and the plantar flexion lateral view shows that the talonavicular joint does not reduce. A line drawn through the long axis of the talus passes below the long axis of the first metatarsal. Initial management should consist of serial casting to stretch the dorsal soft-tissue structures; surgery eventually will be required to reduce the talonavicular joint. The differential diagnosis of congenital vertical talus includes pes calcaneovalgus, flexible pes planus, and peroneal spastic flatfoot. Pes calcaneovalgus, flexible pes planus, congenital short Achilles tendon, and peroneal spastic flatfoot would not show resistent dorsal dislocation of the navicular on the plantar flexion view. Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 85
High Yield
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?

Detailed Explanation
The lateral cord terminates as the musculocutaneous nerve and also contributes sensory fibers to the median nerve. Involvement of the C6 root or upper trunk could potentially cause weakness of the infraspinatus and the brachioradialis. The middle trunk and the posterior cord do not contribute motor fibers to the thumb or sensory fibers to the thumb.
Question 86
High Yield
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 87
A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
Explanation
Traumatic brain injury is considered to be either primary or secondary. Primary injury is direct or impact damage to the brain, and secondary injury can have intracranial or systemic causes. While treatment has little impact on primary brain injury, secondary brain injury can be avoided. There are also many causes of intracranial secondary brain injury, including intracranial hypertension or cerebral edema. There are many causes of systemic secondary brain injury, but none has a greater impact on outcome than hypotension or hypoxia. In fact, the occurrence of hypotension postinjury causes a 10- to 15-fold increase in mortality. In a series by Pietropaoli and associates, the mortality rate for head-injured patients that were normotensive during surgery was 25%, but if they were hypotensive the mortality rate was 82%. In the same series, the number of patients with a Glasgow Coma Scale score of either 4 or 5 dropped from 58% in those patients that were normotensive during surgery to 6% in those patients that became hypotensive during surgery. Efforts to avoid hypotension postinjury and especially during surgery should be of primary importance. Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:216-222. Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J: The deleterious effects of intraoperative hypotension on outcome in patients with severe head injury. J Trauma 1992;33:403-407. Schmeling GJ, Schwab JP: Polytrauma care: The effect of head injuries and timing of skeletal fixation. Clin Orthop 1995;318:106-116.
Question 88
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of

Explanation
Because the patient's shoulders are overtensioned anteriorly, premature osteoarthritis may develop. This may create obligate translation posteriorly and increase the interarticular pressure of the humeral head against the glenoid. Patients should achieve 20 degrees to 30 degrees of external rotation with the elbow at the side. Late degenerative arthritis following a Putti-Platt procedure is associated with significant restriction of external rotation. This patient's shoulder has a reduced risk of anterior instability, rotator cuff tear, and internal impingement because of the limitation of motion. Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 89
High Yield
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of


Detailed Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 90
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 91
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 92
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured?
Explanation
The patient has sustained an iatrogenic injury to the lateral ulnar collateral ligament. This injury has been reported after lateral approaches to the elbow. The orbicular, annular, and lateral radial collateral ligaments have a much less important role in lateral elbow stability. The anterior band of the ulnar collateral ligament is on the medial side of the elbow and is important for valgus stability. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 93
High Yield
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?


Explanation
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit. Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
Question 94
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?


Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 95
Figures 48a through 48c show the lateral radiograph and MRI scans of a 60-year-old man who has had pain in his thigh for 1 month. The next most appropriate step in management should consist of



Explanation
The patient has a presumed metastatic bone tumor. The approach to evaluating a patient with a bone tumor of unknown primary origin is to obtain laboratory studies that include a CBC, an erythrocyte sedimentation rate, a serum protein electrophoresis, a calcium level, a urinalysis, and a prostate-specific antigen. In addition, a bone scan, a radiograph of the chest, and CT scans of the chest and abdomen should be obtained. These evaluations can identify the primary site in 85% of patients. GI studies rarely are of diagnostic value. Prophylactic stabilization is contraindicated until a diagnosis is confirmed by histology. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 96
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed "quadriceps avoidance." This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45 degrees of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability. Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20. Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Question 97
High Yield
A 55-year-old woman fell and sustained an elbow dislocation with a coronoid fracture and a radial head fracture. The elbow is reduced and splinted. What is the most common early complication?

Detailed Explanation
The patient has a dislocation of the elbow with displaced coronoid process and radial head fractures. The elbow is extremely unstable after this injury, and recurrent dislocation in a splint is the most common early complication. Skeletal stabilization of the fractures is required to restore stability of the joint. Characteristics of the fractures will determine the techniques required to restore stability. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 98
High Yield
A patient with a left-sided C6-7 herniated nucleous pulposis would likely have which of the following constellation of findings?
Detailed Explanation
A C6-7 herniation affects the C7 root. The C7 root has the middle finger as its predominant sensory distribution. Its motor function is the triceps, wrist extension, and finger metacarpophalangeal extension. The reflex is the triceps. Magee D: Principles and concepts, in Orthopedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 99
High Yield
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?



Explanation
Nonsurgical management of a symptomatic accessory navicular should be attempted prior to surgery. Good relief is often obtained with a semi-rigid orthosis with a medial arch support. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Question 100
High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
