Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
The extensor carpi radialis brevis, supinator muscle, arcade of Frohse, and leash of Henry are potential sites of compression for the posterior interosseous nerve. The most common location of spontaneous entrapment is the arcade of Frohse. The lateral intermuscular septum is a site of compression for the radial nerve.
Question 2High Yield
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?

Explanation
Symptoms can persist following a rotator cuff repair for a variety of reasons. In the early postoperative period, infection is the primary concern. Stiffness and loss of motion can occur because of postoperative scarring. Complex regional pain syndrome can occur but is rare, and the diagnosis is not made with a plain radiograph. This radiograph shows a superiorly migrated humeral head that articulates with the acromion, indicating that the repair has failed. While large to massive tears may fail more commonly than once thought, the clinical outcome may be satisfactory in many patients. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Question 3High Yield
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
Pain secondary to an osteochondroma is usually from soft-tissue irritation and bursal formation. This is particularly common for proximal medial tibia osteochondromas that irritate the pes anserine tendons. Malignant degeneration into a chondrosarcoma rarely occurs, is usually associated with multiple hereditary exostoses, and usually occurs after skeletal maturity. Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Question 4
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 5 High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 6High Yield
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Question 7
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
Both the medial collateral ligament and the olecranon contribute to valgus stability of the elbow. Excessive olecranon resection increases the demand placed on the medial collateral ligament in resisting valgus forces during throwing. Bone removal from the olecranon should be limited to osteophytes. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Question 8
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Question 9
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
One of the most common complications of hemiarthroplasty is acetabular cartilage degeneration, resulting in increasing pain. Conversion total hip arthroplasty generally is successful with placement of an acetabular cup. Additionally, many patients with osteonecrosis already have degenerative changes of the acetabular cartilage even though radiographic findings may appear normal. Steinberg ME, Corces A, Fallon M: Acetabular involvement in osteonecrosis of the femoral head. J Bone Joint Surg Am 1999;81:60-65.
Question 10High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?

Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 11
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?



Explanation
The images show a lobulated, eccentric, well-marginated lesion that is typical of a nonossifying fibroma. The lesion is slightly expansile, and the CT scan findings show that the lesion is very well marginated and the cortex is disrupted, which is a common finding. None of the characteristics of this lesion is aggressive in nature. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 12
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of

Explanation
The CT scan shows an osteoblastic nidus pathognomic for an osteoid osteoma. Surgical treatment should include an en bloc excision of the lesion. Surgical treatment is not mandatory because the lesion often becomes asymptomatic over time. This lesion is not amenable to radiofrequency ablation due to its proximity to the spinal cord. A complete corpectomy is not necessary to adequately resect the lesion, as only the nidus needs to be removed. Radiation therapy and antibiotics are not appropriate treatments for an osteoid osteoma. Posterior C2-C3 fusion will not address the pathology. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 13High Yield
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the

Explanation
The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 14 High Yield
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of


Detailed Explanation
In a patient with known metastatic disease, the surgeon must rule out additional lesions throughout the femur prior to surgical management. Lesions located in the diaphysis or in the peritrochanteric region may influence the surgical procedure. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 15
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of


Explanation
Because the patient has sustained a tarsometatarsal injury with midfoot sag, the treatment of choice is a tarsometatarsal arthrodesis. The cause of his flatfoot deformity is secondary to the tarsometatarsal injury and not from posterior tibialis tendon deficiency. Lateral column lengthening, double arthrodesis, and calcaneal osteotomy are not indicated. Although open reduction and internal fixation may be performed late when arthritis is present, these procedures are less likely to succeed. Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 16
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?


Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 17 High Yield
What muscle is most often encountered during surgical approaches to C5-6?
Detailed Explanation
The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Question 18
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
For the parachute test, the examiner holds the child prone and then lowers the child rapidly toward the floor. The parachute reaction is normal or positive if the child reaches toward the floor. The Moro or startle reflex should not be present beyond age 6 months. Asymmetric tonic neck reflex, extensor thrust, and absent foot placement are abnormal findings at any age. Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Question 19
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of

Explanation
With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
Question 20High Yield
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Explanation
Several studies have shown that ultra-high molecular weight polyethylene liners used in total hip arthroplasties wear at a rate of 0.1 to 0.2 mm/yr. The orthopaedic surgeon performing total hip arthroplasties should be aware of the average wear rate so that potential problems can be identified when following patients postoperatively. Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC: Charnley total hip arthroplasty with cement: Minimum twenty-five year follow-up. J Bone Joint Surg Am 2000;82:487-497.
Question 21
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of



Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 22
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of




Explanation
The initial radiographs reveal a simple elbow dislocation without associated fractures. After successful closed reduction, the range of stability should be assessed. If the elbow is stable, nonsurgical management should consist of a short period of immobilization followed by range-of-motion exercises. Immobilization for more than 3 weeks results in significant elbow stiffness. Surgical repair is indicated for dislocations that are irreducible, have associated fractures, or where stability cannot be maintained with closed treatment. Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
Question 23
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 24
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 25 High Yield
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?

Detailed Explanation
In patients with flexion-distraction injuries of the thoracolumbar spine, 50% have associated, potentially life-threatening, visceral injuries that occasionally are diagnosed hours or even days after admission. Based on these findings, consultation with a general surgeon is recommended. Blunt and penetrating injuries to the cardiopulmonary system or aorta sometimes can be seen with this type of injury, but they are no more common than with other types of thoracolumbar fractures because of the relatively mild bony injury anteriorly. Neurologic trauma with this type of fracture is also somewhat rare. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Question 26High Yield
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
The genitofemoral nerve and the sympathetic plexus consistently lie on the ventral surface of the psoas muscle. The ilioinguinal and iliohypogastric nerves are the most superior branches of the lumbar plexus and emerge along the upper lateral border of the psoas muscle traveling toward the quadratus lumborum. Both the obturator and femoral nerves are deep and lateral to the psoas muscle. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107. Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 27
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 28
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must

Explanation
While it is recommended that a patient gain full range of motion, pain-free function, and symmetric strength prior to returning to vigorous activities, it is absolutely essential that radiographs of the fracture site reveal a circumferential external bridging callus to prevent refracture. This is particularly important for comminuted femoral fractures with various sized fragments. It is also recommended that a return to rodeo riding be postponed for at least 1 year. Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112. Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am 1991;73:1561-1566.
Question 29
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of

Explanation
An exercise program to strengthen the deltoid and remaining rotator cuff will most likely offer the best results. Revision rotator cuff surgery yields better results in decreasing pain than improving strength and function, and this patient has only minimal pain. Tendon transfers, involving the use of the latissimus dorsi or teres major, have been used when the rotator cuff is deemed irreparable but are not indicated in elderly patients with minimal symptoms. Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515. DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Question 30High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 31High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 32
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?




Explanation
The imaging studies show a permeative lesion of the left hemipelvis with a large soft-tissue mass. The photomicrograph demonstrates a small blue cell tumor with pseudorosettes. The most likely diagnosis is primitive neuroectodermal tumor (Ewing's sarcoma family of tumors). MIC-2 is a highly sensitive and specific marker for this family of tumors. Cytokeratin is an epithelial marker. Vimentin is a mesenchymal marker. Thus, Ewing's sarcomas are cytokeratin negative and vimentin positive. Before discovery of the MIC-2 antigen, PAS and reticulin stains were commonly used to help differentiate Ewing's sarcoma from lymphoma. In contrast to lymphoma, Ewing's sarcomas are typically PAS positive and reticulin negative. Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Question 33High Yield
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?

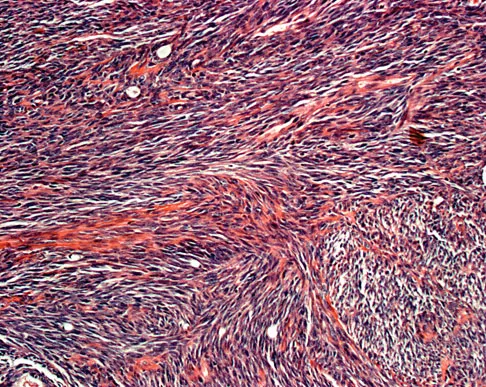
Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 34
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
The tibiofibular overlap is measured between the medial border of the fibula and the lateral border of the anterior tibial tubercle. Plain radiographic assessment of the distal tibiofibular syndesmosis requires AP and mortise views. The following criteria have been used as the normal limits in adults: a talocrural angle of + or - 83 degrees with up to 5 degrees of normal difference between both sides, a medial clear space of less than 4 mm, a talar tilt of less than 2 mm, a tibiofibular clear space of less than 5 mm, a tibiofibular overlap of greater than or equal to 0 mm, and a talar subluxation that is a subjective assessment of congruity of the tibial articular surface and the talar dome; any incongruity is abnormal. It has been recommended to obtain the first three measurements on the mortise view and the other three on the AP view. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 35High Yield
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
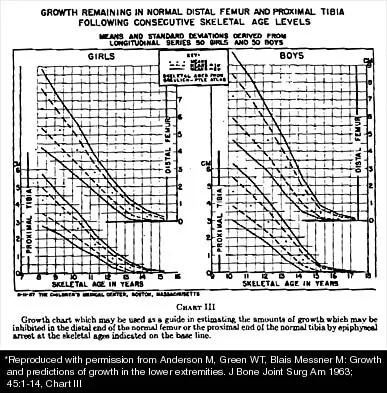
Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 36High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include

Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 37
Figure 18a shows the clinical photograph of a 2-year old boy who has a deformity of the right leg. Examination reveals eight cutaneous markings similar to those shown in Figure 18b. Radiographs are shown in Figure 18c. Management should consist of



Explanation
The diagnosis of neurofibromatosis may be based on the presence of at least six cafe-au-lait spots larger than 5 mm in diameter and the osseous lesion shown in Figure 18c. Neurofibromatosis occurs in 50% of patients who have an anterolateral bowing deformity of the tibia, and this bowing may be the first clinical manifestation of this disorder. The patient has anterolateral bowing of the tibia and fibula that warrants concern for a possible fracture and pseudarthrosis; therefore, the limb should be protected in a total contact orthosis to prevent fracture. In contradistinction to posteromedial bowing of the tibia and fibula, spontaneous remodeling of an anterolateral bowing deformity is not expected. Intramedullary nailing or the use of a vascularized fibula is reserved for the treatment of a congenital pseudarthrosis of the tibia. Crawford AH Jr, Bagamery N: Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72-88.
Question 38 High Yield
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include


Detailed Explanation
Comminuted, displaced radial head fractures (Hotchkiss type 3) require anatomic metallic radial head arthroplasty to regain function. Radial head excision has led to catastrophic sequelae including chronic wrist pain, elbow instability, and proximal radius migration. Immobilization, internal fixation, or anconeus arthroplasty are not recommended at this time because of the potentially poorer outcomes. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 39High Yield
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?

Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 40High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 41
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 42High Yield
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of


Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 43
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?

Explanation
The patient has not undergone a trial of foot-specific patient education and accommodative/therapeutic shoe wear. He must use therapeutic shoe wear at all times, as even the occasional use of pressure-concentrating shoe wear has a high likelihood of leading to the development of a diabetic foot ulcer. Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746. Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Question 44
A 25-year-old man has had an insidious onset of left hip pain over the past 11 months. A radiograph, coronal MRI scan, and histopathologic specimens are seen in Figures 2a through 2d. What is the most likely diagnosis?




Explanation
Ewing's sarcoma is the second most common primary sarcoma of bone in children and young adults. It is a malignant round cell tumor with uncertain histogenesis. Sheets of uniform small round blue cells with a high nuclear-to-cytoplasm ratio and the absence of osteoid formation differentiate this histologic diagnosis from the other conditions. Immunohistochemical staining and molecular diagnostic studies are useful to verify the diagnosis.
Question 45
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?


Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 46High Yield
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?

Explanation
In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
Question 47High Yield
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Question 48
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?



Explanation
Nodular fasciitis is a pseudosarcomatous, self-limiting reactive process composed of fibroblasts and myofibroblasts. Most patients give a history of a rapidly growing mass that has been present for only a few weeks. Many have pain associated with the mass and can recall a specific traumatic event predating the presence of the lesion. It can occur at any age but is most commonly seen in adults who are 20 to 40 years of age. Histologically, the lesion is composed of predominantly plump, immature-appearing fibroblasts that bear a close resemblance to the fibroblasts found in granulation tissue. Characteristically, the fibroblasts are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Question 49
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 50
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder "slip out" when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?



Explanation
The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert's. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 51High Yield
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T1-weighted MRI scan are shown in Figures 28a and 28b. Management should consist of


Explanation
The radiograph and MRI scan reveal a lytic lesion in the left femoral neck region that extends to the lesser trochanter. Although external beam radiation and radioactive iodine infusion may be helpful in controlling the local disease, the patient is at high risk for femoral neck fracture given the location of the lesion. Prophylactic surgery is indicated; therefore, the treatment of choice is a cemented bipolar hemiarthroplasty. The use of a compression hip screw and side plate or an intramedullary nail has a high likelihood of failure with disease progression. Postoperative treatment with radiation therapy and bisphosphonates is also indicated. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264. Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Question 52
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?

Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 53High Yield
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in

Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 54
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
Chronic or neglected Achilles tendon ruptures can present a surgical problem. Ideally, end-to-end apposition of tendon should be attempted, but this should be accomplished without placing the foot in marked equinus. A defect of greater than 5 cm requires the use of a tendon transfer either alone or in combination with a V-Y advancement of the gastrocnemius. Because of its proximity to the Achilles tendon and its strength as a plantar flexor, the flexor hallucis longus is an ideal choice for this task. Studies have shown that early active range-of-motion exercises after an Achilles tendon repair is beneficial for tendon healing and improved clinical outcomes. Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 55
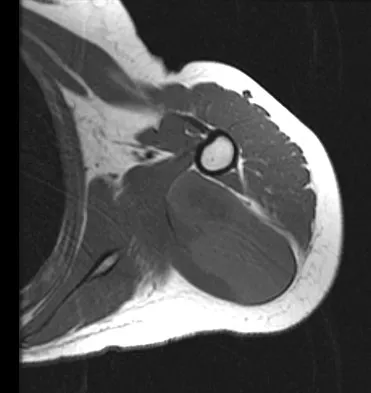
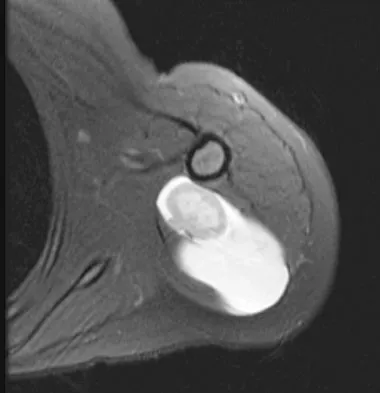
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 56
Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
Explanation
Denis divided the sacrum into three zones: zone 1 represents the lateral ala, zone 2 represents the foramina, and zone 3 represents the central canal. A fracture is classified according to its most medial extension. Those in zone 3 are typically bursting-type fractures or fracture-dislocations and are most prone to neurologic sequelae. Denis F, Davis S, Comfort T: Sacral fractures: An important problem. A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.
Question 57
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
Pain secondary to an osteochondroma is usually from soft-tissue irritation and bursal formation. This is particularly common for proximal medial tibia osteochondromas that irritate the pes anserine tendons. Malignant degeneration into a chondrosarcoma rarely occurs, is usually associated with multiple hereditary exostoses, and usually occurs after skeletal maturity. Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Question 58 High Yield
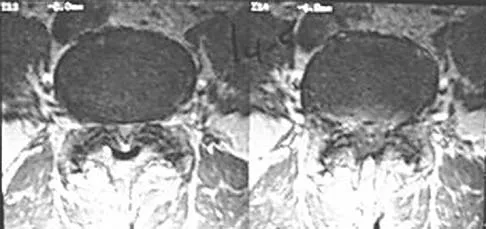
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?

Detailed Explanation
The MRI scan reveals a L4-L5 foraminal disk herniation originating from the L4-5 disk space that has migrated up into the foramen, compressing the left L4 nerve root. There is normal distribution of the roots in the cerebrospinal fluid, excluding arachnoiditis as a diagnosis, and disk herniation in this location would not result in cauda equina syndrome or myelopathy.
Question 59High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 60
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 61
Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
Explanation
Intradiskal electrothermal therapy (IDET) initial clinical results were reported in 2000. The early case series were quite encouraging with reported therapeutic success rates of 60% to 80%. Early enthusiasm was high as IDET provided a nonsurgical treatment option for an otherwise complex and difficult clinical entity, chronic diskogenic low back pain. The actual mechanism of action was not well understood, and while the theoretic explanation made good sense, it did not hold up under laboratory testing. Soon clinical results from the field did not meet the high expectations set by the developers of the technique. Since those early case studies, a few level I evidence studies have been conducted, one by Freeman and associates and one by Pauza and associates. These randomized, placebo-controlled trials demonstrated no significant benefit of IDET over the placebo. Freeman BJ, Fraser RD, Cain CM, et al: A randomized, double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-2377. Pauza KJ, Howell S, Dreyfuss P, et al: A randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.
Question 62
The major blood supply to the cruciate ligaments arises from which of the following structures?

Explanation
The major blood supply to the cruciate ligaments arises from the ligamentous branches of the middle genicular artery. Few terminal branches of the inferior genicular artery contribute to the blood supply. The synovial plexus and sheath covering the cruciate ligaments are also supplied by branches of the middle genicular artery. The blood supply to the cruciate ligaments is predominately of soft-tissue origin. There is no significant osseous vascular contribution to the ligaments. Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Question 63
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 64 High Yield
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?


Detailed Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 65
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0 degrees to 125 degrees of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of



Explanation
While many low-demand patients with injuries to the ulnar collateral ligament can be treated nonsurgically, Jobe and associates described two situations in which ulnar collateral ligament reconstruction is indicated: (1) an acute complete rupture in a competitive athlete who uses the upper extremities extensively and who wishes to remain active; and (2) chronic pain or instability that does not improve after at least 3 months of nonsurgical management. Rarely is direct surgical repair of the ligament possible or able to withstand the valgus stresses applied to the elbow. Most authors recommend surgical reconstruction of the ulnar collateral ligament using a palmaris longus, plantaris, or fourth toe extensor tendon from the fourth autograft. Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133. Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Question 66
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of


Explanation
The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Question 67 High Yield
A 32-year-old laborer reports left ankle pain and deformity. History reveals that he sustained a left ankle fracture 2 years ago and was treated with closed reduction and casting. Radiographs are shown in Figures 25a through 25c. What is the most appropriate management?



Detailed Explanation
Corrective osteotomy of fibular malunions, with appropriate lengthening, even in the presence of early arthritis, has been shown to decrease ankle pain and increase stability. Reduction and bone grafting of the medial malleolar nonunion is also needed. There is no evidence supporting the use of intra-articular steroids or hyaluronic acid in the ankle joint. Lateral talar displacement of even 1 mm has been reproducibly shown to decrease tibiotalar contact by 40% to 42%, causing a predisposition to arthritis. Weber D, Friederich NF, Muller W: Lengthening osteotomy of the fibula for post-traumatic malunion: Indication, technique and results. Int Orthop 1998;22:149-152. Lloyd J, Elsayed S, Hariharan K, et al: Revisiting the concept of talar shift in ankle fractures. Foot Ankle Int 2006;27:793-796. Offierski CM, Graham JD, Hall JH, et al: Later revision of fibular malunion in ankle fractures. Clin Orthop Relat Res 1982;171:145-149.
Question 68
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of


Explanation
Soft-tissue sarcomas generally are treated with radiation therapy and wide surgical resection. In this patient, involvement of most of the posterior calf compartment and circumferential involvement of the posterior tibial and peroneal neurovascular bundle makes limb salvage impractical. Any attempt at wide surgical resection would leave a poorly functioning limb with questionable surgical margins. A high below-knee amputation would be the best option. Radiation therapy alone is contraindicated. Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397. Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 69
What are the five most common tumors that metastasize to bone?
Explanation
The five most common primary carcinomas that metastasize to bone are breast, prostate, lung, renal, and thyroid in decreasing order of incidence. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 70 High Yield
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Detailed Explanation
The tenosynovium excised at the time of a carpal tunnel release for idiopathic carpal tunnel syndrome rarely shows signs of acute or chronic inflammation. Fibrosis, edema, and vascular sclerosis are the most common histologic findings. A tenosynovectomy with a carpal tunnel release usually is not necessary in the treatment of idiopathic carpal tunnel syndrome. Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225. Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Question 71High Yield
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
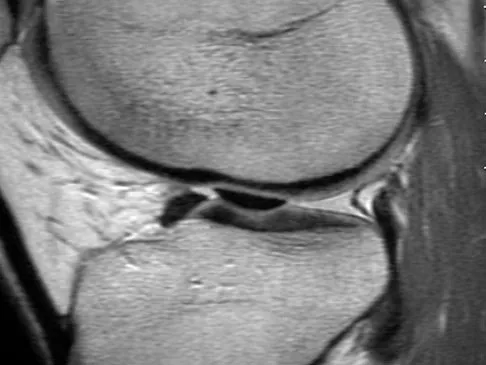
Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 72
Back pain and ipsilateral knee pain are common long-term sequelae of hip arthrodesis. To limit these problems, what position should be avoided during fusion of the hip?
Explanation
The recommended position for a hip fusion is flexion of 20 degrees to 30 degrees, slight adduction (5 degrees) or neutral, and 10 degrees of external rotation. In long-term follow-up, patients who underwent fusion in abduction had more ipsilateral knee and low back pain than patients who were positioned in adduction. Internal rotation should be avoided to prevent interference with the opposite foot during gait. External rotation facilitates the application of shoe wear. Callaghan JJ, Brand RA, Pederson DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 73
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?

Explanation
Thoracic outlet syndrome is thought to be caused by compression of the neurovascular supply to the upper limb in the supraclavicular and axillary regions of the shoulder. While typically progressive in onset, thoracic outlet syndrome may develop after acute injury. Injury or weakness of the scapular muscles, especially the trapezius, may result in descent of the scapula and cause compression of the thoracic outlet. In general, most symptoms are the result of neural compression. Typical symptoms include pain in the neck or shoulder and numbness or tingling that predominantly involves the ulnar side of the arm and hand. Exacerbation of these symptoms is typical when the arm is abducted. Initial management should consist of postural exercises aimed at restoring proper scapular stability. Severe recalcitrant symptoms may warrant surgical decompression. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 74
An 83-year-old woman with a long history of her foot slowly and progressively "turning out" now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
Question 75High Yield
The anticoagulant effect of the low-molecular-weight heparins (LMWH) is mediated by the binding affinity of antithrombin III to which of the following coagulation factors?

Explanation
Standard heparin mediates its anticoagulant effect largely through its interaction with antithrombin III. A conformational change in antithrombin III occurs that markedly accelerates its ability to inactivate the coagulation enzymes thrombin factor (II), factor Xa, and factor IXa. In contrast, LMWHs do not contain the necessary saccharide units to bind thrombin and antithrombin III simultaneously. The anticoagulant effect of LMWHs involves binding of antithrombin III to factor Xa.
Question 76
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of




Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 77High Yield
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of

Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 78
Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?


Explanation
The patient has a zone 1 base of the fifth metatarsal fracture (Pseudojones) that represents a less serious injury compared to zone 2 and 3 fractures with regard to healing potential. Treatment is symptomatic and casting is not necessary. These fractures are well treated with a hard-soled shoe for comfort and weight bearing as tolerated. Surgical intervention is not warranted. Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5-10. Wiener BD, Linder JF, Giattini JF: Treatment of fractures of the fifth metatarsal: A prospective study. Foot Ankle Int 1997;18:267-269.
Question 79
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of


Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 80
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of



Explanation
The imaging studies show a fracture-dislocation. Surgical treatment of this injury consists of a decompression reduction, stabilization, and fusion. A posterolateral decompression can also be performed as necessary. An isolated anterior procedure in this type of injury is contraindicated. The anterior longitudinal ligament is most likely intact; therefore, an anterior procedure further destabilizes the spine. Reduction by an anterior approach would also be difficult. Nonsurgical management of the neurologic injury in this patient is not indicated. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 81High Yield
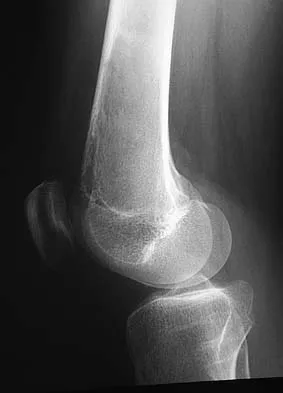
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include

Explanation
The radiograph shows bilateral flattening of the femoral heads with mottling and "fragmentation" suggestive of Legg-Calve-Perthes disease. However, when these changes occur bilaterally and are symmetric, multiple epiphyseal dysplasia or spondyloepiphyseal dysplasia should be suspected. Skeletal survey will show irregularity of the secondary ossification centers. With these conditions, there is no true osteonecrosis and no evidence that orthotic or surgical "containment" will alter the outcome of progressive degenerative arthritis. Cardiac anomalies and coagulopathies are not associated with the epiphyseal dysplasias. Crossan JF, Wynne-Davies R, Fulford GE: Bilateral failure of the capital femoral epiphysis: Bilateral Perthes disease, multiple epiphyseal dysplasia, pseudoachondroplasia, and spondyloepiphyseal dysplasia congenita and tarda. J Pediatr Orthop 1983;3:297-301.
Question 82
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?

Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 83High Yield
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Question 84
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 85 High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?

Detailed Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 86
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 87
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 88High Yield
Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?

Explanation
The first step in the treatment of an amputation residual limb (stump) ulcer is local wound care and adjustment of the residual limb-prosthetic interface, as well as adjusting prosthetic alignment. Surgical revision should be undertaken only when prosthetic modification is unsuccessful. Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.
Scientific References
- :
Question 89High Yield
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
The rhomboideus major and minor muscles are innervated by the dorsal scapular nerve, which is supplied entirely by the C5 nerve root. The dorsal scapular nerve arises just distal to the dorsal root ganglion of the C5 nerve root. A functioning rhomboid muscle indicates that an injury involving C5 nerve root fibers must be postganglionic or distal to the C5 dorsal root ganglion. Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Question 90
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome. Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Question 91High Yield
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
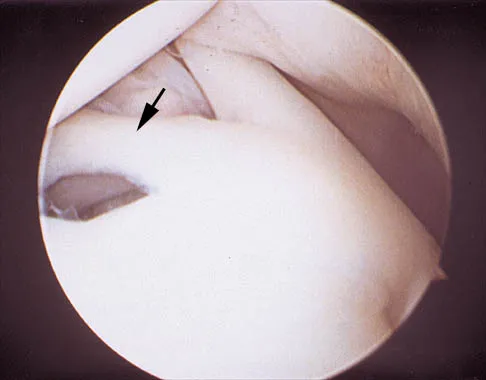
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 92
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 93
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?


Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 94
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?



Explanation
A chordoma is a malignant neoplasm originating from remnants of the notochord. It is usually localized to the midline with 50% at the sacrococcygeal area, 35% at the skull base, and 15% at the mobile portion of the spine. Large vacuolated cells (physaliferous cells) are a characteristic of the tumor. Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Question 95High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 96High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 97High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?

Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44. Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Question 98
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?

Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 99
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
While guidelines for predicting fracture risk are at best imprecise, the scoring system by Mirels (pain, anatomic location, and pattern of bony destruction) has been shown to be most predictive of fracture risk. Functional pain, peritrochanteric location, and lytic bone destruction are the greatest risk factors for pathologic fracture. The factors of patient weight, age, soft-tissue mass, and location within bone are all of lesser importance. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 100High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
