Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?

Detailed Explanation
Multidisciplinary treatment combining systemic chemotherapy and adequate surgical resection has resulted in a 5-year survival rate of 70% in patients with nonmetastatic osteosarcoma of the extremity . The advent of effective chemotherapy has increased the overall survival rate from 20% to 70% in current studies. Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 2
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?

Explanation
Assessment of the acutely injured patient follows the Advanced Trauma Life Support protocol. Cervical cord injury is often associated with a disruption in sympathetic outflow. Absent sympathetic input to the lower extremities leads to vasodilatation, decreased venous return to the heart, and subsequent hypotension. With hypotension, the physiologic response of tachycardia is not possible because of the unopposed vagal tone. This results in bradycardia. Patient positioning, fluid support, pressor agents, and atropine are used to treat neurogenic shock.
Question 3
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 4
High Yield
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of


Detailed Explanation
The examination findings are consistent with subscapularis muscle weakness but normal supraspinatus and infraspinatus strength. The lift-off test and abdominal compression test are specific for subscapularis function. The MRI scan reveals a chronic avulsion and retraction of the subscapularis. The transverse image reveals a normal infraspinatus muscle, and the sagittal image reveals an atrophic subscapularis. Surgical repair of the isolated subscapularis tendon is indicated. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Question 5
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 6
High Yield
A 36-year-old woman is wearing an ankle-foot orthosis for a foot drop secondary to spastic hemiplegia following a postpartum stroke 2 years ago. Knee and hip motion and strength are within normal ranges. She has undergone multiple rounds of physical therapy but has seen no improvement over the past several months. No improvement has been recorded by electromyography (EMG) studies over the past year. Examination reveals a 5-degree plantar flexion contracture with clonus, heel varus, and compensatory knee hyperextension when standing. She has 4/5 power in the tibialis anterior and gastrocnemius soleus complex with resistance testing. Everters are 2/5 to resistance testing. EMG gait studies show that the tibialis anterior demonstrates activity during both swing and stance phase that is increased during swing phase. Premature firing of the triceps surae is noted when positioning the foot in equinus prior to floor contact. What is the most appropriate management?

Detailed Explanation
The patient has a dynamic varus deformity secondary to spasticity of the tibialis anterior during stance phase with inverter/everter imbalance. The patient still has active motion of the tibialis anterior; therefore, an out-of-phase posterior tibial tendon transfer should not be performed. The same is true of the Bridle procedure. Transfer of the posterior tibialis in this patient may also result in subsequent planovalgus deformity. Lengthening of the Achilles tendon through a percutaneous tenotomy will restore dorsiflexion and decrease clonus from the stretch response. If adequate dorsiflexion is not obtained intraoperatively, then posterior tibialis tendon lengthening may be considered. A split tibialis anterior tendon transfer to the lateral cuneiform, or, transfer of the entire tendon to the cuneiform should correct the varus component and compensate for the weakened peroneals. Yamamoto H, Okumura S, Morita S, et al: Surgical correction of foot deformities after stroke. Clin Orthop Relat Res 1992;282:213-218. Piazza SJ, Adamson RL, Moran MF, et al: Effects on tensioning errors in split transfers of tibialis anterior and posterior tendons. J Bone Joint Surg Am 2003;85:858-865.
Question 7
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?


Explanation
The patient has lumbar spinal stenosis and the MRI scans reveal the pathology at L4-5, which is secondary to posterior disk bulging and hypertrophy and infolding of the ligamentum flavum, as well as degenerative facet arthrosis. The degree of spinal stenosis is moderate and his symptoms are positional in nature. Tadokoro and associates reported on a prospective study of 89 patients older than 70 years of age who underwent nonsurgical management for lumbar spinal stenosis. They found the prognosis to be relatively good with patients scoring at "excellent" or "good" for activities of daily living at final follow-up. However, they did note that patients with a complete block on myelography did not respond favorably to nonsurgical management. Amundsen and associates reported on a 10-year prospective study comparing surgical care to nonsurgical management. They concluded that, while the long-term results largely favored surgical treatment, more than half of the nonsurgically managed patients had a satisfactory outcome. They also concluded that a delay of surgery for some months did not worsen the prognosis. Therefore, their recommendation was for an initial primarily nonsurgical approach. Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435. Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Question 8
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?

Explanation
The dual plate fixation construct is significantly stronger than single plate or "Y" plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis. Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Question 9
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow?
Explanation
Osteochondritis dissecans occurs in the older child or adolescent (typically older than age 13 years). It involves the lateral compartment. The etiology is felt to be microtraumatic vascular insufficiency from repetitive rotatory and compressive forces. MRI typically shows separation of cartilage from the capitellum and chondral fissuring. Panner's disease is usually seen in children younger than age 10 years, involves the entire capitellar ossific nucleus, and resolves typically with no residual deformity or late sequelae. There is no evidence of ligamentous injury. Defelice GS, Meunier MJ, Paletta GA: Elbow injury in the adolescent athlete, in Altchek DW, Andrews JR (eds): The Athlete's Elbow. New York, NY, Lippincott Williams & Wilkins, 2001, pp 231-248.
Question 10
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?


Explanation
The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient's age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement. Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
Question 11
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.
Question 12
High Yield
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Detailed Explanation
Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended. Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394. Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Question 13
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and

Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 14
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 15
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of


Explanation
The patient has a stress fracture of the olecranon that occurs with repetitive throwing motions. If the fracture is not displaced, the initial treatment of choice is rest and rehabilitation to maintain elbow motion, followed by aggressive strengthening at 6 to 8 weeks. A light throwing program generally can begin at 8 to 12 weeks. Complete recovery may require 3 to 6 months. If the fracture is displaced or if nonsurgical management fails, surgery is indicated for internal fixation of the stress fracture. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Question 16
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of


Explanation
Open reduction and internal fixation is the treatment of choice for accurate reduction of the disrupted intercarpal ligaments. In addition, the displaced scaphoid fracture will require open reduction and internal fixation and possible bone grafting. Closed reduction and long arm casting will not allow accurate reduction of the dislocated intracarpal intervals, and it is unlikely to allow accurate reduction of the scaphoid. The maneuver required to effect closed reduction of a displaced scaphoid fracture will most likely cause the scaphoid lunate interval to displace. Closed reduction with percutaneous pin fixation or with an external fixator is unable to effect anatomic reduction of the injury. Proximal row carpectomy is used as a salvage procedure for a variety of degenerative and posttraumatic problems of the wrist. Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120. Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Question 17
High Yield
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 18
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of


Explanation
The patient has lung cancer metastatic to the right proximal femur. The lesion is large, has destroyed a portion of the cortex, and involves the peritrochanteric region. All of these findings put the patient at high risk for pathologic fracture. The lesion is amenable to intramedullary fixation in the form of some type of reconstruction nail. Chemotherapy alone will not restore the bone stock. Given the extent of the lesion, radiation therapy, chemotherapy, or embolization will not prevent fracture. A proximal femoral replacement would be indicated in patients with bone destruction extending into the femoral head and neck. Bisphosphonates may diminish the risk of subsequent lesions but are not sufficient to treat this high-risk lesion. Radiation therapy should be given postoperatively to prevent further bone destruction.
Question 19
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?

Explanation
Because of the previously transferred bone block of coracoid and short arm flexors, the musculocutaneous nerve often scars along the anteroinferior glenohumeral capsule. Mobilization of this tissue places the nerve at greatest risk. The axillary nerve is also potentially at risk, but this is nonspecific to prior surgery, particularly the Bristow procedure. Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 98-116.
Question 20
High Yield
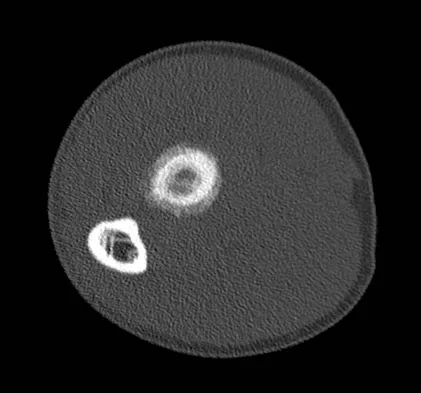
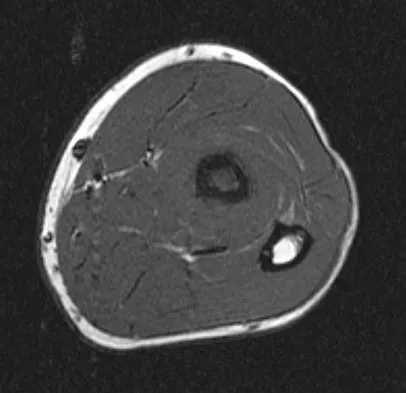
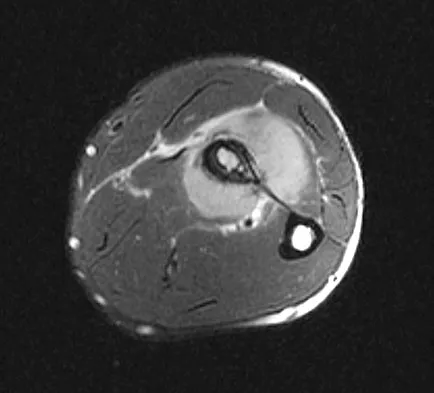
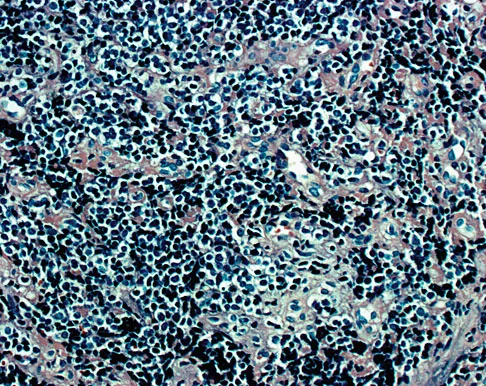
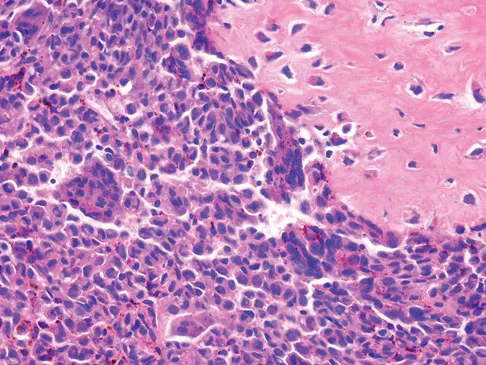
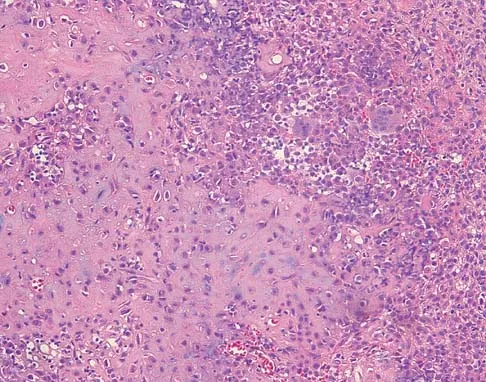
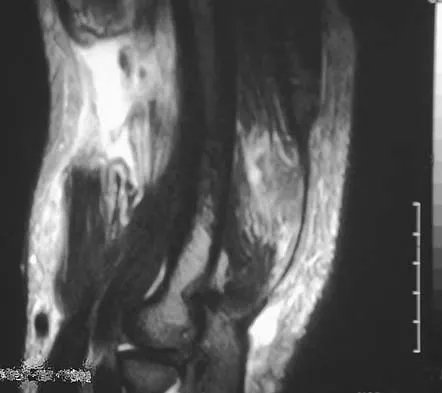
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T1- and T2-weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?


Explanation
The imaging studies show a permeative lytic destructive lesion in the proximal radius with "hair-on-end" periosteal reaction and a large soft-tissue mass most consistent with Ewing's sarcoma. The pathology reveals monotonous sheets of "round blue" cells. This limits the differential diagnosis to primary lymphoma of bone versus Ewing's sarcoma. These are best differentiated by immunohistochemistry, cytogenetics, and flow cytometry. Lymphoma of bone is typically CD34 positive and CD99 negative; whereas, the reverse is true of Ewing's sarcoma, CD34 negative and CD99 positive. The most common cytogenetic translocation with Ewing's sarcoma is 11; 22; 21; 22 and 7; 22 translocations have also been reported in Ewing's sarcomas. The X; 18 translocation is most commonly associated with synovial cell sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Flow cytometry is used to characterize the cell types of lymphomas. Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21. Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing's sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Question 21
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of

Explanation
The patient has a type IIIB patellar fracture (inferior pole fracture with an intact patellar tendon). Nonsurgical management is the treatment of choice if there is little displacement and the extensor mechanism is intact. Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Question 22
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?




Explanation
Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients. Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 23
Which of the following palpable bony landmarks is correctly matched with its corresponding vertebral level?

Explanation
The carotid tubercle is usually located at the level of C6. The angle of the mandible is at C1-C2; the hyoid is at C4; the superior portion of the thyroid cartilage is C4-C5; and the cricoid cartilage is at C6. Smith GW, Robinson RA: The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40:607.
Question 24
High Yield
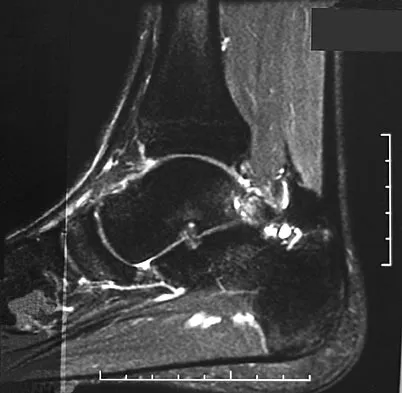
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?

Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 25
High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Detailed Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 26
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 27
High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 28
What is the structure indicated by the letter "A" in Figure 21?

Explanation
The ligaments shown are the components of the lateral collateral ligament complex, and the structure indicated by the letter "A" is the radial collateral ligament. The lateral ulnar collateral ligament is the structure indicated by the letter "C" and the annular ligament is indicated by the letter "B." The transverse ligament is a component of the medial collateral ligament complex. Morrey BF: Anatomy of the elbow joint, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 30.
Question 29
High Yield
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
The plantar-medial cutaneous nerve is at risk with the surgical approach to the medial sesamoid. It is found directly underlying an incision made at the junction of the glabrous skin of the hallux and must be identified before the approach can proceed. Transection will result in a painful neuroma that impinges on the plantar-medial surface of the toe and cause problems with shoe wear. The only other structure that lies near the surgical field is the abductor hallucis tendon which lies dorsal to the incision.
Question 30
High Yield
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of

Explanation
Most patients with a significant recurrent neuroma will not obtain relief with conservative methods. Pain results from a stump neuroma at the weight-bearing area from too short of a resection of the nerve or from regrowth of the remaining nerve end. Although steroid injection may be helpful in localizing symptoms or providing temporary relief, it rarely cures a stump neuroma. Orthotics with a metatarsal pad will likely increase pressure and pain at the neuroma site. Physical therapy could temporize the symptoms but will not address the underlying problem. Similarly, bone decompression alone will not alter the location of the neuroma stump. Revision of the nerve to a more proximal level off of the weight-bearing area is the most likely method to succeed. A plantar approach facilitates identification and ability to revise the nerve to a more proximal level. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657. Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Question 31
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 32
High Yield
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?

Explanation
To mobilize the common iliac vessels across the midline, the iliolumbar vein must be ligated. It has a short trunk and can be torn if mobilization is attempted without ligation. It is the only branch off the common iliacs (there are no arterial branches) prior to the terminal branches, the internal (hypogastric) and external iliacs. The middle sacral vessels run distally from the axilla of the bifurcation and are a factor when accessing the L5-S1 disk. Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
Question 33
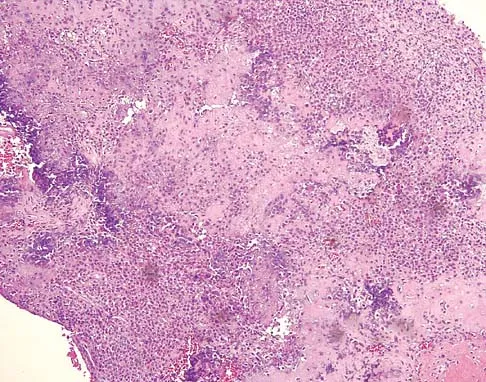
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 34
High Yield
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?



Explanation
The radiographs reveal osteoarthritis and proximal humeral head migration. Integrity of the rotator cuff must be questioned based on these radiographic changes. The status of the rotator cuff is the most influential factor affecting postoperative function in shoulder hemiarthroplasty. The coracoacromial ligament provides a barrier to humeral head proximal migration in the face of a rotator cuff tear. The radiographs do not indicate significant humeral head or glenoid erosion. Acromioclavicular arthritis is often asymptomatic. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 35
High Yield
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?


Explanation
The epiphyseal location on the radiograph and MRI scan and the histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification all suggest chondroblastoma. Although giant cell tumors of bone typically occupy an epiphyseal location, they are rare in children and when present are often metaphyseal in skeletally immature patients. Enchondromas and osteoblastomas are generally metaphyseal and, along with giant cell tumors, have very different histology than seen here. Chondromyxoid fibromas are typically metaphyseal in location. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Question 36
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?


Explanation
This radiolucent lesion with a "fallen leaf sign" is typical for a unicameral bone cyst(UBC). The most appropriate treatment is to allow the fracture to heal with clinical and radiographic observation. Curettage and bone grafting is not the best initial management for UBC. Wide resection is not indicated for UBC. The proximal humerus is the most common site for UBC. While staging studies consisting of MRI, bone scan, and CT of the chest are appropriate for lesions suspected of being malignant, the classical appearance of this UBC is such that this work-up is not necessary initially. Following fracture healing, aspiration and injection of the cyst may be indicated. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 37
High Yield
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?

Detailed Explanation
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Question 38
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of

Explanation
Femoral shortening osteotomy for a Crowe type IV hip dislocation has been shown to provide superior results with minimal complications. Cementless fixation of the stem allows for modular implants that greatly simplify the reconstruction.
Question 39
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
These finding indicate central cord syndrome, and injury that is more common in the older population who have some degree of spondylosis. The physiologic insult can be a central spinal hematoma with resultant hematomyelia. Bowel and bladder functional return has a good prognosis, unlike the upper extremity motor loss. Cauda equina syndrome generally involves injury at the lumbar levels, with some degree of lower extremity motor loss. Posterior cord syndrome is characterized by preservation of motor function below the level of injury and position/vibratory sensory loss. Brown-Sequard syndrome, which is often produced by a penetrating injury, results in contralateral hypalgesia and ipsilateral weakness. Anterior cord syndrome has a poor prognosis for functional return; lower extremity findings include loss of light touch, sharp/dull, and temperature sensations below the level of injury, as well as motor function. Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Question 40
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 41
High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?

Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Question 42
High Yield
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of

Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 43
High Yield
What is the most common bone tumor in the hand?

Detailed Explanation
The most common bone tumor in the hand is an enchondroma. Forty-two percent of these lesions occur in the small tubular bones. They frequently present with a fracture in these locations. Fractures are usually treated nonsurgically. Indications for surgery include patients with symptomatic lesions or those who are considered high risk for recurrent fracture. The histologic appearance of an enchondroma in the hand is more cellular than enchondromas found in the long bones. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Question 44
High Yield
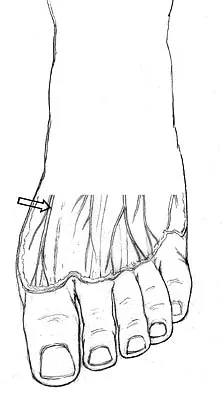
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 45
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
Epithelioid sarcoma is a rare soft-tissue sarcoma that most commonly arises in the hand or upper extremity, and it is frequently misdiagnosed as an infection or granuloma. It tends to have a higher incidence of lymph node metastasis than other soft-tissue sarcomas. The mainstay of treatment is wide surgical excision, even if amputation is necessary. Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Question 46
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?


Explanation
The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length. Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Question 47
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degree left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of

Explanation
The findings and radiographic appearance are most consistent with osteoid osteoma involving the medial pedicle. Scoliosis is commonly seen with this lesion and usually does not need surgical intervention. Excellent results have been reported with surgical excision as well as with percutaneous thermocoagulation. Nonsurgical treatment also has been described in peripheral osteoid osteoma but is not well described for lesions within the spine. Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 48
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?

Explanation
The patient's symptoms are typical for gouty arthropathy, and the diagnosis can only be confirmed with aspiration and visualization of the crystals. A concomitant infection also must be ruled out; therefore, it is important to obtain a cell count and culture. Colchicine may have a role in gouty management, but the diagnosis must be confirmed. Allopurinol is not effective in acute gouty arthropathy. Measurement of serum uric acid levels is often not helpful in making a definitive diagnosis. Steroid injections should be deferred until cell count and culture results indicate no accompanying infection. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 49
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 50
High Yield
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 51
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of


Explanation
The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Question 52
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 53
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?

Explanation
Although CPM machines are used widely in the United States for patients undergoing TKA, the benefit seems to be marginal, if any. Numerous randomized trials have shown that final outcomes after total knee arthroplasty are unaffected by the use of CPM machines postoperatively. Some studies have suggested that use of CPM may improve flexion in the first few weeks, but any short-term benefit from the machine was lost by intermediate-term follow-up. Aside from potential improvement in flexion within the first few postoperative weeks, there does not appear to be any benefit from the machines. There is no improvement in pain, ambulation, or extension. The cost-effectiveness of these machines has been questioned by many authors. Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293. McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Question 54
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?



Explanation
Schwannomas (neurilemomas) occur at all ages but are most frequently seen in persons between the ages of 20 and 50 years. MRI features of schwannomas are fairly nonspecific, but when they are associated with a large named nerve, the identification of a mass in continuity with that nerve is highly suggestive of a schwannoma. Most have a fairly homogeneous appearance with a high water content and often fusiform shape. Classically, the histology shows alternating Antoni A (dense spindle cell region) areas and Antoni B (loose myxoid tissue) areas. They also demonstrate uniform intense immunostaining with S-100 protein. Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Question 55
High Yield
A 17-year-old boy has had elbow pain for the past 6 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 65a through 65e. What is the most likely diagnosis?





Detailed Explanation
The findings are consistent with an osteoblastoma. The radiographs show a bone-forming lesion of the distal humerus. The lesion has an osseous component extending out of the native cortex with a thin sclerotic border. The T2-weighted MRI scan shows the lesion extending anteriorly beyond the native cortex. No fluid-fluid levels are seen. Histology shows large osteoblasts producing osteoid and woven bone. The tissue between the spicules of bone and osteoid contains thin fibrous tissue and capillaries. Osteoid osteoma is a smaller lesion usually with sclerotic reactive bone around a small nidus. The histology differentiates osteoblastoma from osteosarcoma because no malignant cells are seen. There is no cartilage production or chondroblasts in the histologic specimen, eliminating chondroblastoma. Giant cell tumors of bone typically occur in a epiphyseal metaphyseal location, most commonly after skeletal maturity, and contain numerus giant cells. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 87-102.
Question 56
High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 57
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
Question 58
High Yield
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Detailed Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 59
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 60
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 61
High Yield
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?


Explanation
Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 62
High Yield
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?

Explanation
The radiograph shows three zones: an outer regenerated cortical layer, an interface zone consisting of viable trabecular bone and occasional particles of bone cement, and an inner layer of necrotic bone embedded in cement. No fibrous membrane is noted, and there is no direct contact of cement with native bone. Based on these findings, it is believed that the middle layer is the result of incorporation of the allograft with further remodeling. Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Question 63
High Yield
A 62-year-old woman with soft-tissue calcifications and telangiectasia has severe pain in the left index, middle, ring, and little fingers. History reveals that she does not smoke. The clinical history and arteriogram shown in Figure 6 are consistent with which of the following conditions?

Explanation
The arteriogram shows generalized disease of all vascular structures. Even though the image was obtained following an infusion of nitroglycerin, little flow is present to the fingers. Based on the history of soft-tissue calcifications and telangiectasia, the most likely diagnosis is CREST (chondrocalcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly and telangiectasias). The arteriogram reveals Raynaud's phenomenon or the "R" component of CREST. Buerger's disease, or thromboangiitis obliterans, is strongly associated with a history of smoking. Hypothenar hammer syndrome involves repetitive trauma to the ulnar artery at the wrist, resulting in well-defined filling defects in the superficial palmar arch of the hand. Although not well visualized in this patient, the superficial arch is narrowed, showing no evidence of aneurysmal dilation. Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Question 64
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 65
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 66
Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?
Explanation
Surgical technique in patellar resurfacing has been found to be one of the critical factors in the success or failure of total knee arthroplasty. Theoretically, metal-backed patellar components are an excellent way of evenly distributing joint forces from the polyethylene button to bone (similar to the tibial component). However, despite this theoretical advantage, metal-backed patellae have been associated with a higher failure rate. Some of the observed problems include poor bone ingrowth, peg failure, dissociation of the metal plate and polyethylene button, and component fracture. Because of these factors, all-polyethylene patellae have proved to be the standard if patellar resurfacing is attempted. Medialization of the patellar component, a symmetrically thick patella, and external rotation of the femoral and tibial components improve patellar tracking. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Question 67
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 68
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?



Explanation
The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal. Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
Question 69
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 70
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of

Explanation
The radiograph shows excessive thoracic kyphosis (normal 20 degrees to 50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann's kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann's kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees. Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248. Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Question 71
High Yield
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of

Explanation
In a 6-year-old child with a physeal fracture, the healing response 10 days after injury is so advanced that manipulation would have to be very forceful to be successful. A forceful manipulation in a patient this age increases the risk of early growth arrest and a significant disability because 80% of the growth of the radius comes from the distal physis. Because of the large contribution of growth from the distal radial physis and the angulation being in the plane of wrist motion, the potential for remodeling of this fracture is great. It is highly probable that this fracture will completely remodel in 1 to 2 years of growth. In this patient, even a "gentle" open reduction would probably require enough force that the physis would be damaged. Dimeglio A: Growth in pediatric orthopaedics, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 33-62.
Question 72
High Yield
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?

Detailed Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness. Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Question 73
High Yield
What is the main function of collagen found within articular cartilage?

Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 74
High Yield
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
Recovery of upper extremity motor function after a cerebrovascular accident follows a predictable pattern. The greatest amount of recovery is seen within the first 6 weeks. Return of function proceeds from proximal to distal. Shoulder flexion occurs first, followed by return of flexion to the elbow, wrist, and fingers. Return of forearm supination follows the return of finger flexion.
Question 75
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 76
Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
Explanation
Arthrodesis of the talonavicular joint eliminates almost all hindfoot motion. Arthrodesis of the subtalar joint eliminates 74% of talonavicular motion and 44% of calcaneocuboid motion. Arthrodesis of the calcaneocuboid joint eliminates 33% of talonavicular motion and 8% of subtalar motion. Arthrodesis of the naviculocuneiform or cuboid-fifth metatarsal joint has limited effect on hindfoot motion. Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.
Question 77
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 78
High Yield
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
The term 'spinal shock' applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
Question 79
High Yield
An eversion mechanism of injury is associated with which of the following ankle conditions?
Detailed Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 80
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Question 81
High Yield
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?


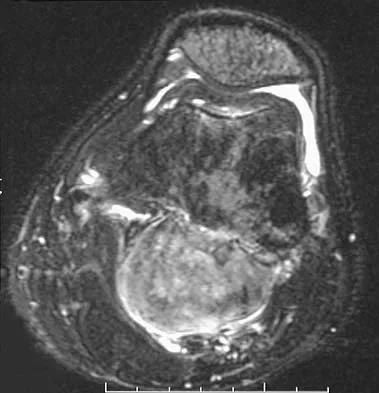
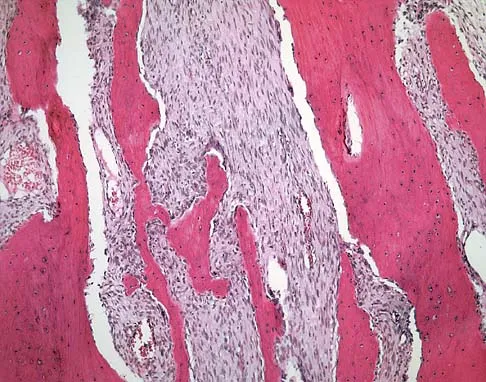
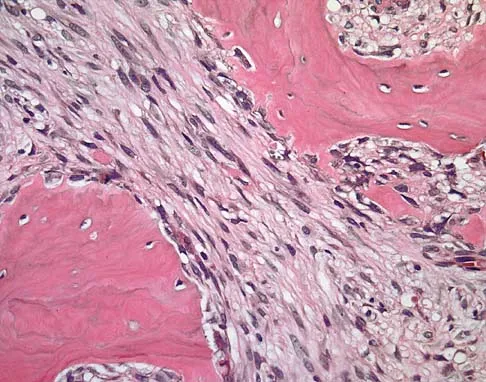
Explanation
The patient has parosteal osteosarcoma. The posterior aspect of the distal femur is the typical location for this variant of osteogenic sarcoma. The imaging studies indicate a surface lesion with no involvement of the adjacent intramedullary canal. The histologic appearance is that of a low-grade fibroblastic osteosarcoma, consisting of relatively mature bone and a bland fibroblastic stroma lacking cytologic atypia and mitotic activity. A cartilaginous component is also frequently seen. Classic osteosarcoma typically has a more aggressive radiologic and histologic appearance. Sessile osteochondromas, while common behind the knee, have a presence of hematopoietic marrow and fat. The cartilage found in the associated cartilaginous cap is oriented. Chondrosarcomas are more typical in an older age group and have a histologic pattern consisting of malignant chondroid. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Question 82
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?

Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 83
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?



Explanation
A discoid meniscus is a large disk-like meniscus. It is seen in the lateral meniscus in 3% of the population; a discoid medial meniscus is much less common. It can be identified on the coronal view by noting meniscal tissue extending into the tibial spine at the intercondylar notch. The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 84
High Yield
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?


Explanation
The patient has multiple hereditary exostoses and a secondary chondrosarcoma arising from a proximal femoral exostosis. The radiograph of the knee shows multiple osteochondromas typical in a patient with multiple hereditary exostoses. Patients with this diagnosis are at an increased risk for malignant degeneration of an osteochondroma. The lateral radiograph of the hip shows a bony lesion emanating from the anterior aspect of the femoral neck that is not well defined in the surrounding soft tissues. There are punctate calcifications and a large soft-tissue mass. The most likely diagnosis is a secondary chondrosarcoma developing from a benign osteochondroma. An enchondroma is an intramedullary benign cartilage lesion. Ollier's disease and Maffucci's syndrome involve multiple enchondromas. Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Question 85
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0 degrees to 125 degrees of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of



Explanation
While many low-demand patients with injuries to the ulnar collateral ligament can be treated nonsurgically, Jobe and associates described two situations in which ulnar collateral ligament reconstruction is indicated: (1) an acute complete rupture in a competitive athlete who uses the upper extremities extensively and who wishes to remain active; and (2) chronic pain or instability that does not improve after at least 3 months of nonsurgical management. Rarely is direct surgical repair of the ligament possible or able to withstand the valgus stresses applied to the elbow. Most authors recommend surgical reconstruction of the ulnar collateral ligament using a palmaris longus, plantaris, or fourth toe extensor tendon from the fourth autograft. Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133. Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Question 86
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?



Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 87
High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 88
High Yield
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
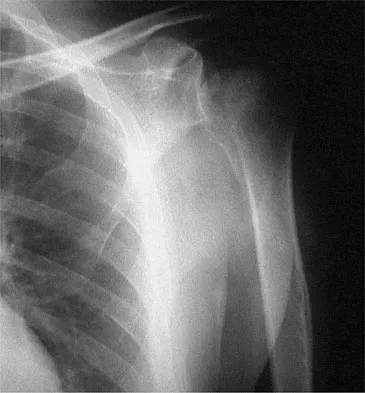
Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 89
High Yield
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?



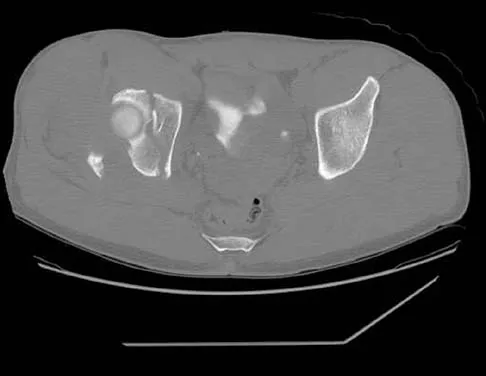
Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 90
High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?

Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 91
High Yield
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient's symptoms?


Detailed Explanation
The MRI scans show Modic changes in the L4-L5 vertebral bodies due to spondylosis. There is no increased fluid signal or enhancement in the L4-L5 disk to suggest infection or any other pathologic process. Therefore, the patient's pain should be treated with a course of physical therapy and rehabilitation. There is no infection; therefore, IV antibiotics and debridement are not indicated. Similarly, a pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Question 92
High Yield
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Detailed Explanation
Latissimus dorsi tendon transfer is considered a surgical option for treatment in patients with chronic supraspinatus and infraspinatus tendon tears. Preoperative subscapularis function is necessary for good clinical results. Additionally, men with active elevation to shoulder level and active external rotation to 20 degrees have predictably good results. Women with active shoulder elevation limited to below chest level have poor results from this procedure and should not be considered candidates. Postoperatively they lack pain control, active elevation, and active external rotation. Muscular atrophy in the latissimus dorsi does not occur, and glenohumeral arthritic changes frequently develop postoperatively. Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am 2006;88:113-120.
Question 93
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?

Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 94
High Yield
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type

Explanation
The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 95
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 96
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 97
High Yield
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
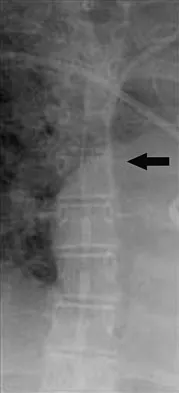
Explanation
In this patient, the radial nerve is most likely injured at the level of the radial neck. The radial nerve emerges from the posterior cord of the brachial plexus and travels along the spiral groove of the humerus. At the level of the lateral humeral condyle, the radial nerve branches into the posterior interosseous nerve after giving off two cutaneous branches, the superficial radial and the posterior cutaneous. The posterior interosseous nerve travels through the supinator muscle and winds around the radial neck. At this level, the posterior interosseous nerve is vulnerable to injury, particularly following fracture or penetrating trauma. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Question 98
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Question 99
High Yield
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?

Detailed Explanation
Cheilectomy has been shown to provide satisfactory pain relief and improved function in long-term studies. It is important to select patients appropriately when choosing a cheilectomy versus an arthrodesis. Pain at the midrange of motion and loss of more than 50% of the metatarsal head cartilage are predictors of a poor outcome following cheilectomy, and these patients should receive an arthrodesis. Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Question 100
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems. Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89. Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
