Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient's symptoms?


Detailed Explanation
The MRI scans show Modic changes in the L4-L5 vertebral bodies due to spondylosis. There is no increased fluid signal or enhancement in the L4-L5 disk to suggest infection or any other pathologic process. Therefore, the patient's pain should be treated with a course of physical therapy and rehabilitation. There is no infection; therefore, IV antibiotics and debridement are not indicated. Similarly, a pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Question 2
High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 3
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 4
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of


Explanation
The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Question 5
High Yield
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of

Explanation
The radiograph reveals a reverse obliquely subtrochanteric/intertrochanteric fracture. Open reduction and internal fixation should be accomplished with a 95-degree fixed angle device. An intramedullary nail with screw fixation into the head is another possible technique. Either method should correct the varus deformity. Exchange of a high-angled screw and plate device to a longer side plate and bone grafting does not afford any improvement in the mechanical stability. Hardware removal and retrograde intramedullary nailing is not indicated for this level of a proximal femoral injury. Placement of an implantable bone stimulator may change local biologic factors but would not enhance mechanical stability. The patient's femoral head is intact without signs of collapse; therefore, hardware removal, proximal femoral resection, and total hip arthroplasty are not warranted. Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Question 6
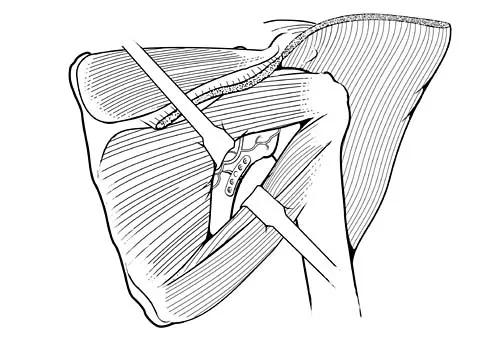
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of



Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 7
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 8
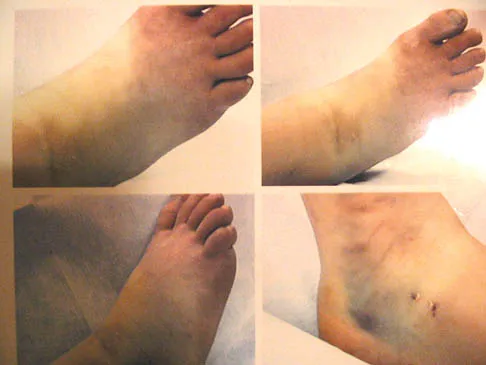
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?




Explanation
Pigmented villonodular synovitis often presents with intermittent swelling and minimal pain. It often occurs around joints but may be found around tendon sheaths and bursal linings. Periarticular erosions involving both sides of joints are typical, and multiple joint involvement has been described. Portions of low-signal intensity on T1- and T2-weighted images are characteristic of hemosiderin-laden processes. High-signal content is suggestive of high water content. The combination of low-signal intensity areas in intra-articular lesions with or without osseous destruction is diagnostic of pigmented villonodular synovitis. Aspiration reveals bloody or brownish fluid. The treatment of choice is synovectomy performed arthroscopically or open. Recurrence is common. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Question 9
High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 10
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
Improvement in the appearance of the hip joint on functional radiographic evaluation (abduction/adduction views) has been shown to be predictive of outcome following joint preserving surgery. CT and MRI findings have not been shown to be predictive of outcome.
Question 11
On MRI, a nonsanguinous effusion has what appearance?

Explanation
Nonbloody effusions that are greater than 1 mL are readily detected by MRI. They appear black on T1-weighted images and white on T2-weighted images. A sanguinous effusion is seen as white on T1-weighted images and black on T2-weighted images. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 12
High Yield
Figures 57a through 57c show the radiographs of a patient who has pain, discomfort, and a popping sensation localized to the posterior aspect of the knee after undergoing primary left total knee arthroplasty 6 months ago. Examination reveals that the patient is able to ambulate without a limp. There is no significant swelling, erythema, or effusion. Range of motion is 0 degrees to 115 degrees, and a palpable crepitation or snapping is detected at the posterior lateral joint line. What is the most likely diagnosis?



Detailed Explanation
Popliteal snapping syndrome represents the most likely diagnosis. Barnes and Scott noted that the popliteus tendon can be a potential source of internal derangement after total knee arthroplasty. They noted that it can be subluxated anteriorly and posteriorly over a retained lateral femoral condyle osteophyte. Allardyce and associates described the condition as a popliteus condition, snapping as it rolls over a retained lateral femoral condylar osteophyte. Patellar clunk syndrome is a distinct syndrome associated with the patella and has been reported in posterior stabilized knees. In addition to crepitation with range of motion, the patella literally snaps or jumps as the knee is taken from flexion to extension. Beight JL, Yao B, Hozack WJ, et al: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142. Barnes CL, Scott RD: Popliteus tendon dysfunction following total knee arthroplasty. J Arthroplasty 1995;10:543-545.
Question 13
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
In the patient who is neurologically intact or has an incomplete injury from a cervical facet dislocation, a closed reduction with weighted tong traction is appropriate when the patient is awake, alert, and cooperative. Although there is a risk that a cervical facet dislocation could occur with an underlying cervical disk herniation, Vaccaro and associates have shown that closed reduction can be safely carried out in the awake, responsive patient. Closed reduction can be performed in the emergency department with traction with skull tongs or a halo ring. A slow stepwise application of weight is added until a reduction is achieved. Any worsening of the neurologic status of the patient requires immediate termination of the closed reduction and further diagnostic imaging before proceeding with further treatment. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Question 14
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?

Explanation
Many clinical studies to date show that the extent of arthritis is the most common variable that has the greatest influence on outcome. The success rate of allograft transplantation is significantly diminished in patients who have grade IV chondromalacia of the knee or notable flattening and general joint incongruity. Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63. Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
Question 15
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?



Explanation
A destructive mixed lytic and blastic metaphyseal lesion with a large soft-tissue mass in an adolescent is most likely an osteosarcoma until proven otherwise. The epicenter of the tumor is on the surface of the bone, most likely involves the periosteum, and is more likely to be chondroblastic in nature. Parosteal osteosarcoma is a low-grade tumor, much more radiodense, usually smaller, and found in the posterior distal femur of middle-aged patients. Chondrosarcomas are distinctly rare in childhood.
Question 16
Plots of stress versus strain for four orthopaedic biomaterials are shown in Figure 3. Referring to the figure, what is the correct identification of the curves?

Explanation
Stress-strain plots allow easy comparison of a number of important mechanical properties, including elastic modulus (the slope of the initial straight line portion of the curve) and yield stress (the stress at the break in the curves for bone, steel, and titanium alloy). Important considerations here are much lower modulus and ultimate stress of bone and cement compared to the two metallic alloys, the fact that titanium is lower modulus but higher strength than stainless steel, and the identification of cement as the only brittle material among the four. Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 97-129.
Question 17
High Yield
Anabolic steroid use has which of the following effects on serum lipoprotein levels?

Explanation
The use of anabolic steroids causes a decrease in high-density lipoprotein levels but has no effect on low-density lipoprotein levels. An abnormally low high-density lipoprotein level should alert the physician to the possibility of steroid use in an athlete. Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Question 18
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm3, an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include



Explanation
This clinical picture is most consistent with periarticular erosions from gout. The patient has multiple periarticular lytic lesions in the hand. The laboratory studies show an elevated serum uric acid level, and the biopsy specimen demonstrates acute and chronic inflammation with prominent clefts. Therefore, the preferred treatment is systemic control of her gout. Radiation therapy, chemotherapy, and/or amputation should be considered for a malignancy; however, the pathology does not demonstrate any evidence of pleomorphism, high nuclear-to-cytoplasmic ratio, nuclear atypia, or mitotic activity. Antibiotics for an infectious process is a consideration, but the minimal elevation in the WBC count and erythrocyte sedimentation rate does not support an infectious process. Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Question 19
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of


Explanation
Surgery is not indicated in a patient who has a mild deformity and no pain. Shoe wear modifications should be recommended.
Question 20
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?

Explanation
Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Question 21
High Yield
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 22
In patients with neurofibromatosis, what is the most important sign of impending rapid progression of a spinal deformity?
Explanation
Neurofibromatosis can progress very rapidly. Rib penciling is the only singular prognostic factor. Significant progression has been observed in 87% of the curves with three or more penciled ribs. The other factors are often present but do not have a high correlation with rapid, severe progression. Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Question 23
What is the main function of collagen found within articular cartilage?

Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 24
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 25
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?

Explanation
The resultant spasticity and weakness (paresis) following a cerebrovascular accident leads to muscle imbalance that commonly results in contracture of the shoulder in adduction, internal rotation, and varying degrees of forward flexion. In addition, the elbow is usually flexed and the forearm pronated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 26
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis. Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Question 27
High Yield
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Detailed Explanation
Anteromedial displacement of the tibial tubercle unloads the distal and lateral facets of the patella and shifts the forces to the proximal and medial facets. Therefore, if findings indicate arthrosis predominately in the medial and proximal areas of the patella, this is considered a relative contraindication because it may accentuate arthritic symptoms. Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181. Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Question 28
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 29
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?

Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 30
High Yield
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 31
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 32
High Yield
Which of the following is considered the most common infectious organism causing osteochondritis in pediatric puncture wounds of the foot?
Explanation
Pseudomonas aeruginosa is the most common infectious organism causing osteochondritis in pediatric puncture wounds of the foot. Eikenella corrodens is found in human bites, and Pasteurella multocida is characteristically seen with animal bites. Serratia marcescens and Proteus mirabilis have been reported but are much less likely. Jacobs RF, Adelman L, Sack CM, et al: Management of pseudomonas osteochondritis complicating puncture wounds of the foot. Pediatrics 1982;69:432-435.
Question 33
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder "slipped out" and "went back in." The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?


Explanation
A hard fall on an outstretched arm often results in injury to the glenoid labrum. A significant tear of the anterior/inferior labrum often leads to instability, pain, and mechanical symptoms of the shoulder. The MRI scan shows no obvious labral tear or Hill-Sachs lesion to suggest an anterior dislocation. Recent clinical studies have suggested that early stabilization of initial anterior dislocations may lead to better results than nonsurgical management in young, athletic patients. However, there are no data to support early surgery for anterior labral tears resulting from traumatic subluxation without dislocation. Initial treatment should consist of a short period of rest and immobilization, followed by a physical therapy rehabilitation program designed to restore motion, strength, and dynamic stability to the shoulder. If the athlete cannot return to play following nonsurgical management, surgical repair of the labrum, either through an open or arthroscopic approach, is indicated. There is no role for immediate thermal capsular shift in this setting. Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
Question 34
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?

Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Question 35
High Yield
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
Most patients lose elbow range of motion after open reduction and internal fixation of a distal humeral fracture. Ulnar nerve dysfunction, nonunion, and infection all occur less commonly. Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
Question 36
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?



Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 37
High Yield
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of

Detailed Explanation
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis. Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Question 38
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?

Explanation
Most humeral fractures will heal with nonsurgical functional brace management. When the initial pain has subsided in a coaptation splint, the patient is converted to a functional brace and allowed to use the arm for activities. The fracture should heal within 6 weeks to 12 weeks with acceptable results. Surgery is indicated if there is vascular injury, open injury, floating elbow, chest injury, bilateral humeral fractures, or if a reduction cannot be obtained or maintained. The surgical treatment of choice is either antegrade reamed locked intramedullary nailing or plate osteosynthesis. Plate osteosynthesis appears to offer better results with respect to union, function, and risk of complications. Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Question 39
Based on the findings seen in the posteroanterior radiograph of the wrist shown in Figure 17, which of the following structures is torn?

Explanation
The radiograph shows widening between the scaphoid and lunate. The normal variance is up to 5 mm. Although several ligaments may be torn, the scapholunate interosseous ligament must be torn for this widening to occur. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 503-506.
Question 40
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include


Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 41
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30 degrees, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury. Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Question 42
High Yield
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Detailed Explanation
The tenosynovium excised at the time of a carpal tunnel release for idiopathic carpal tunnel syndrome rarely shows signs of acute or chronic inflammation. Fibrosis, edema, and vascular sclerosis are the most common histologic findings. A tenosynovectomy with a carpal tunnel release usually is not necessary in the treatment of idiopathic carpal tunnel syndrome. Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225. Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Question 43
High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?

Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 44
High Yield
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Detailed Explanation
It is important that the radii of a metal-on-metal head to cup articulation be such that there is polar contact. As the radii become closer to equal, conditions favor higher frictional torque and equatorial seizing. The "bedding in" of metal-on-metal surfaces and their stiffness are both components of the properties considered in the design of polar contact surfaces.
Question 45
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 46
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 47
High Yield
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation. Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 48
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength. Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172 Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Question 49
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 50
High Yield
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of


Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 51
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 52
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?

Explanation
The first rule of total knee arthroplasty is to restore the joint line to its original location. This will ensure optimal patellofemoral biomechanics and will facilitate ligament balancing. Changes on the tibial side affect both the flexion and extension gaps equally. Changes in femoral component sizing or position affect the flexion gap only. Tibial changes affect both the flexion and extension gaps. To convert a tight extension gap to a normal flexion gap, more distal femur needs to be resected. Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
Question 53
High Yield
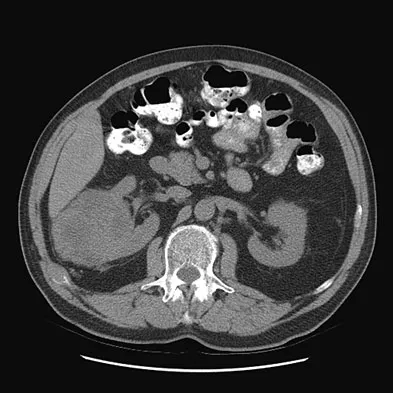
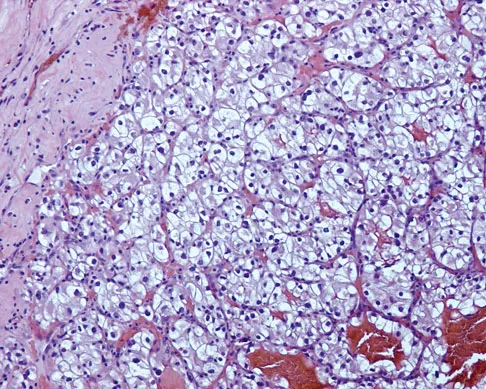
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?


Explanation
The histology shows findings consistent with metastatic renal cell carcinoma. Renal cell carcinoma metastases are extremely vascular. Preoperative embolization helps minimize the amount of blood loss during curettage of these lesions. Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Question 54
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?

Explanation
The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid. Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 55
High Yield
A 44-year-old recreational weight lifter reports chronic deep pain in his left shoulder that is aggravated by any pressing exercises. He also notes a painful catch in the shoulder occurring with rotational movements. Physical therapy and nonsteroidal anti-inflammatory drugs for 3 months have failed to provide relief. Examination reveals pain with O'Brien's test but no signs of instability. MRI scans are shown in Figures 4a and 4b. Treatment should now consist of


Detailed Explanation
The MRI scans show a large paralabral ganglion cyst in the spinoglenoid notch that communicates with an extensive tear of the glenoid labrum. Snyder and associates have classified superior labral tears into several subtypes that reflect the location and extent of the injury. Arthroscopic repair of the labral tear and aspiration of the ganglion cyst is the treatment of choice. Open excision of the cyst does not address the underlying problem of the labral tear. Snyder SJ, Karzel RP, Delpizzo W: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch cysts. J Shoulder Elbow Surg 2002;11:600-604. McFarland EG, Kim TK, Savino RM: Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
Question 56
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?

Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 57
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
BMPs signal through the activation of a transmembrane serine/threonine kinase receptor that leads to the activation of intracellular signaling molecules called SMADs. There are currently eight known SMADs, and the activation of different SMADs within a cell leads to different cellular responses. The other mediators are not believed to be directly involved with BMP signaling. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 58
A 24-year-old dancer reports posterior ankle pain when in the "en pointe" position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
Flexor hallucis longus tendinitis is a common cause of posterior ankle pain in dancers. It tends to be more posteromedial and is characterized by a clicking or catching sensation posteromedially with motion of the great toe. A painful os trigonum typically causes more posterolateral ankle pain and may occur after an ankle sprain or plantar flexion injury where there may be a fracture of the os trigonum. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Question 59
High Yield
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?

Detailed Explanation
The patient has a grade 4 spondylolisthesis. Optimal surgical management is posterior spinal fusion from L4 to the sacrum. The use of instrumentation is controversial. Vertebrectomy is typically reserved for spondylo-optosis (grade 5) cases. Spinal fusion from L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis. Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Question 60
High Yield
What is the most likely cause of the lesion shown in Figures 35a and 35b?

Explanation
The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Question 61
Examination of a 9-year-old boy reveals a right thoracic prominence on forward flexion. Neurologic examination is normal, and no other abnormalities are noted. AP radiographs reveal a 30-degree right thoracic curve. Initial management should consist of
Explanation
The patient has juvenile scoliosis. MRI has shown an association between juvenile scoliosis and intraspinal abnormalities, most often syringomyelia and Arnold-Chiari malformations. All juvenile curves greater than 20 degrees should be evaluated with MRI despite the absence of neurologic findings. Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 685-705 Nohria V, Oakes WJ: Chiari I malformation: A review of 43 patients. Pediatr Neurosurg 1990-91;16:222-227.
Question 62
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?


Explanation
The patient has a global loss of motion that has failed to improve with 6 months of nonsurgical treatment; because he has reached a plateau, further nonsurgical management will likely be ineffective. Revision in the form of an open release is indicated to lyse intra- and extra-articular adhesions; subscapularis lengthening may be done concurrently as needed. Revising to a smaller head can be considered if adequate motion is not achieved. The radiographs reveal an adequate neck cut with appropriate seating of the component. Removing the glenoid component will decrease capsular tension but will probably increase pain because of the lack of glenoid resurfacing. Increasing humeral retroversion will not improve motion. Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Question 63
High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 64
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?

Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 65
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
Question 66
High Yield
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients. Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Question 67
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as

Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 68
High Yield
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?



Detailed Explanation
The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
Question 69
High Yield
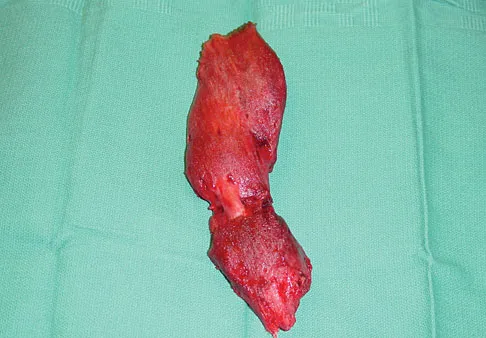
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?

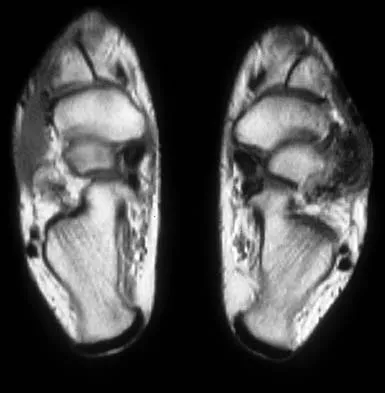
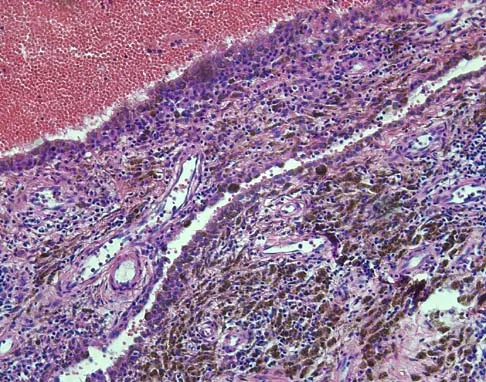
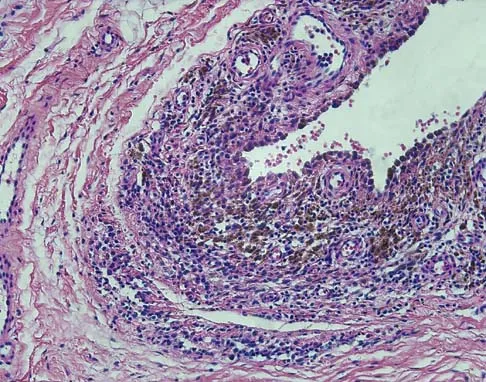
Explanation
Synovial sarcoma should always be considered in the differential diagnosis of a foot mass; however, the histopathology shows a typical example of PVNS, with hemosiderin, giant cells, and synovium. Synovial chondromatosis would have metaplastic cartilage in the synovium. The radiograph shows subtle erosion of the lateral cortex of the cuboid, and the MRI scan shows a soft-tissue mass. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830. Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Question 70
Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at mid-range follow-up (5-10 years) after lumbar fusion?
Explanation
The rate of symptomatic degeneration at an adjacent segment warranting either decompression or arthrodesis was predicted to be 16.5% at 5 years and 36.1% at 10 years based on a Kaplan-Meier analysis.
Question 71
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?

Explanation
The patient has nonunions of the metatarsal fractures and a hallux valgus deformity with arthritic changes. To address all of the findings, management should consist of open treatment of the metatarsal nonunions and hallux metatarsophalangeal arthrodesis. Cast immobilization and a bone stimulator are unlikely to be beneficial at this time. Isolated correction of the hallux valgus deformity will not address the metatarsal nonunions or the arthritis at the hallux metatarsophalangeal joint. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214. McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Question 72
High Yield
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?

Explanation
Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 73
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?

Explanation
Burks and Schaffer described an approach to the tibial insertion of the posterior cruciate ligament that uses the interval between the semimembranosus and the medial gastrocnemius. The medial gastrocnemius muscle is retracted laterally and protects the neurovascular bundle. This approach is used to repair an avulsion of the posterior cruciate ligament tibial attachment or for performing a posterior cruciate ligament tibial inlay reconstruction. Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Question 74
High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 75
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Explanation
Sodium deficiency is the cause of heat cramps. It is the principle electrolyte of sweat and is readily lost during training, especially in warmer temperatures. The condition can be avoided by adding extra table salt to food and maintaining good hydration before and after sports activities. Salt tablets are to be avoided when a patient has heat cramps because the high soluble load will cause gastric irritation. Bergeron MF, Armstrong LE, Maresh CM: Fluid and electrolyte losses during tennis in the heat. Clin Sports Med 1995;14:23-32.
Question 76
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of


Explanation
The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy. Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Question 77
A 16-year-old high school student undergoes a routine preparticipation physical examination at the beginning of the school year. Examination reveals marked laxity of both shoulders but only mild generalized laxity in other joints. The load and shift test allows for anterior humeral translation to the glenoid rim and posterior humeral translation beyond the glenoid rim. The sulcus sign is present. What is the next most appropriate step in management?
Explanation
This patient has shoulder laxity without apprehension. Because there is a wide range of normal laxity in asymptomatic shoulders, the physician should inform the student of these findings, recommend shoulder strengthening exercises, and allow unrestricted sports participation unless symptoms develop. Harryman DT, Sidles JA, Harris SL, Matsen FA III: Laxity of the normal glenohumeral joint: A quantitative in vivo assessment. J Shoulder Elbow Surg 1992;1:66-76. Hawkins RJ, Bokor RJ: Clinical evaluation of shoulder problems, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 186. McFarland EG, Campbell G, McDowell J: Posterior shoulder laxity in asymptomatic athletes. Am J Sports Med 1996;24:468-471.
Question 78
High Yield
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
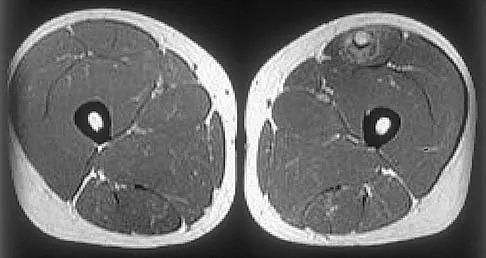


Explanation
The images reveal a region of increased signal within the rectus femoris muscle with mild, ill-defined surrounding edema. The presence of high intensity signal on the T1-weighted image favors acute blood, in this case associated with a rectus femoris muscle tear or fatty tissue. However, because of fat suppression, a fatty lesion or lipoma would be dark on STIR, rather than bright as in this image. Most foreign bodies are low intensity signal and if small, are difficult to evaluate with MRI. The lack of adjacent subcutaneous soft-tissue edema or surrounding fluid makes pyomyositis an unlikely diagnosis.
Question 79
High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 80
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T1-weighted MRI scan with fat suppression and an axial T2-weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?



Explanation
MRI findings of acute osteomyelitis include a decrease in the normally high signal intensity of bone marrow on T1-weighted imaging; however, a postgadolinium T1-weighted image with fat suppression will show osteomyelitis as a bright marrow signal compared to the surrounding fat. Osteomyelitis is also brighter than normal fat on T2-weighted imaging. There is no rim-enhancing lesion suggesting an abscess, although myositis is seen in the obturator internus and short external rotators. The clinical scenario and imaging studies do not support the diagnosis of septic hip, eosinophilic granuloma, or pelvic fracture. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 81
High Yield
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of "weeping" serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Detailed Explanation
Although not as common as arterial injury, venous thrombosis secondary to trauma of the subclavian or axillary vein can be problematic; therefore, venous duplex ultrasound scanning is the diagnostic study of choice. Arteriography may not show venous thrombosis in the venous run-off phase. The clinical history does not fit the usual presentation of a compartment syndrome or complex regional pain syndrome.
Question 82
High Yield
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?
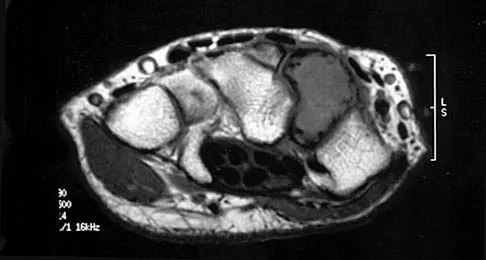
Explanation
The MRI scan reveals an abnormal signal in the trapezoid, which lies adjacent to the capitate in the distal carpal row. The tumor is a giant cell tumor of bone. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240. bar based on these measurements is shown in Figure 54d. Initial treatment should consist of 1- bony bar resection and distal fibula epiphysiodesis. 2- bony bar resection and corrective osteotomy. 3- bony bar resection and physiodesis of the opposite distal tibial physis. 4- corrective osteotomy and a limb-lengthening procedure. 5- corrective osteotomy and physiodesis of the opposite distal tibial physis. 2 54a 54b 54c 54d Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 83
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of


Explanation
A favorable prognosis can be expected in up to 70% of children with Legg-Calve-Perthes disease who are younger than age 6 years. Containment treatment has not been shown to alter the outcome in this age group. The goals of treatment in this patient are to reduce pain (synovitis), restore motion, and improve function. Symptomatic treatment modalities include bed rest, traction, crutches, activity modification, and nonsteroidal anti-inflammatory drugs. Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Question 84
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include

Explanation
The imaging studies reveal a navicular stress fracture. This condition is secondary to chronic overuse (often running on hard surfaces) and results in vague, ill-defined pain in the midfoot. These fractures can be missed on radiographs but are well-defined on CT or MRI. Tarsal navicular fractures are typically oriented in the sagittal plane. Surgery is typically indicated for the high-level athlete because of the high risk for nonunion and persistent symptoms following nonsurgical management. Internal fixation is the treatment of choice. Torg JS, Pavlov H, Cooley JH, et al: Stress fractures of the tarsal navicular. J Bone Joint Surg Am 1982;64:700-712.
Question 85
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
In children, the main route of infection in skeletal TB is through hematogenous spread from a primary source. The mycobacterium is deposited in the end arterials in the vertebral body adjacent to the anterior aspect of the vertebral end plate. Thus, the anterior portion of the vertebral body is most commonly involved. The lower thoracic region is the most common segment; next in decreasing order of frequency are the lumbar, upper thoracic, cervical, and sacral regions. Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Question 86
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of

Explanation
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis. Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Question 87
High Yield
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of

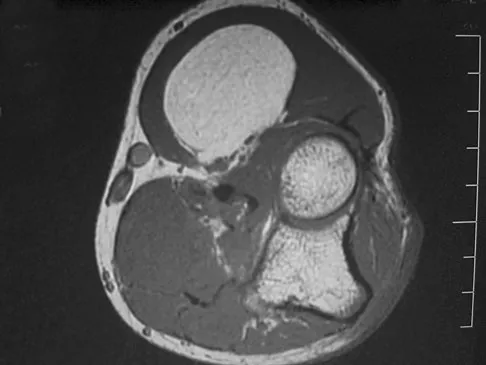
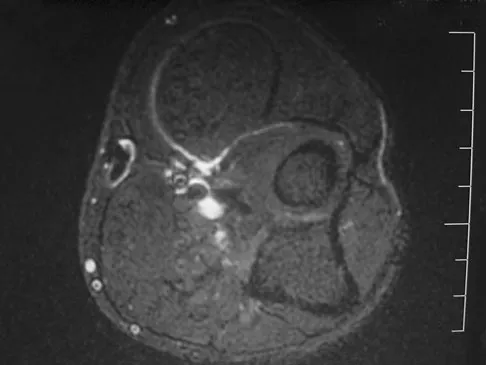
Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 88
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 89
High Yield
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 90
A 67-year-old man is requesting revision surgery because of continued pain in the knee after undergoing a total knee replacement 2 years ago. Examination reveals that the knee is not warm, the incision is well-healed, and the skin has normal coloration and hair formation. No varus or valgus instability is noted, and knee range of motion is 5 degrees to 100 degrees. Laboratory studies show an erythrocyte sedimentation rate of 15 mm/h and a WBC of 5,000/mm3. Aspiration of the knee reveals clear fluid that shows no growth on culture. Radiographs reveal an appropriately positioned cruciate-retaining cemented total knee arthroplasty that is well-fixed. What is the probability that the patient's pain will be improved with revision surgery?

Explanation
The patient has a well-fixed and aligned painful total knee replacement. The success rate of revision knee replacement for pain when no mechanical problem can be identified is approximately 40%. The critical step is to rule out the presence of infection with appropriate laboratory studies and aspiration. If no infection is detected, revision should be avoided. Rand JA: Planning for revision total knee arthroplasty, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 161-166.
Question 91
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?


Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 92
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 93
The fracture shown in Figure 32 is strongly indicative of what diagnosis?

Explanation
Fractures that occur through the primary spongiosa at the subphyseal region of the metaphysis are highly specific for child abuse. On radiographic studies, the metaphyseal lucency in these injuries may appear as either the so-called "bucket-handle" or "metaphyseal corner" fracture. These fractures are not typical features of osteogenesis imperfecta or vitamin D-resistant rickets. The ingestion of lead may lead to thick, transverse bands of increased density at the distal metaphysis. Fractures in the subphyseal region of the metaphysis are not typically seen in children who have osteomyelitis. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Question 94
High Yield
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Detailed Explanation
Low-molecular-weight heparin is highly bioavailable with a half-life of 3 to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin. Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding. Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62. Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Question 95
High Yield
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
In a traditional plate system, fracture security depends on the friction between the plate and the underlying bone. Bicortical fixation will decrease the toggle and improve stability. Locking plates absorb axial forces transmitted from the screws. Such plates do not require plate compression against the bone, thus preserving periosteal blood supply. Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.
Question 96
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of


Explanation
The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem. Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Question 97
High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 98
High Yield
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
After an osteoporotic vertebral compression fracture, the risk of subsequent fractures at adjacent levels increases. This is felt to be the result of a shifting of the sagittal alignment more anteriorly, putting more stress on the osteopenic vertebral bodies and their anterior cortices. Pain generally resolves with rest, but this may take weeks or months. It has been demonstrated experimentally that osteoporotic vertebral bodies are actually less stiff and weaker after a compression fracture; therefore, deformity predisposes to further deformity. The extensor musculature often fatigues over time and usually does not hypertrophy. Frontal plane deformity is a rare development. Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Question 99
High Yield
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?

Detailed Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 100
What type of nerve palsy is most common following elbow arthroscopy?

Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
