Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 2
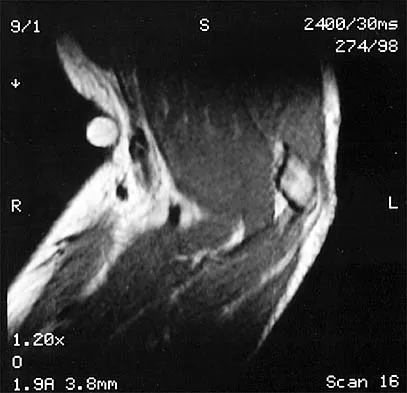
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?

Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 3
High Yield
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
Question 4
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems. Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89. Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Question 5
High Yield
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Detailed Explanation
Electromyography during walking reveals the tibialis anterior muscle is active during early swing, allowing the foot to clear the ground. All of the other muscles are quiet, as the limb moves forward through space with minimal muscular effort. The other muscles are primarily active during weight acceptance or push-off. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Question 6
High Yield
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative

Detailed Explanation
Boden and associates' recent article presents significant evidence that patients with rheumatoid arthritis, neurologic deterioration, and C1-2 instability are more likely to improve after surgery if the posterior alanto-odontoid interval is greater than 10 mm preoperatively. The accepted safe range for the posterior atlanto-odontoid interval is 14 mm. This measurement is believed to better represent the space available for the cord than the anterior alanto-odontoid interval. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 7
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?


Explanation
The radiographs show narrowing of the medial joint space, which indicates polyethylene wear and progressive varus alignment. Wear particles incite osteolytic lesions like the one seen on the lateral radiograph. O'Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Question 8
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 9
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?



Explanation
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
Question 10
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?

Explanation
The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207. Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079. Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Question 11
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
In this age group of patients with arthrogryposis, open reduction through a medial approach is generally recommended. Open reduction through an anterior approach is reserved for patients in which a medial approach has failed or for older patients who require simultaneous femoral shortening and/or pelvic osteotomy. Closed treatment of unilateral hip dislocation in association with arthrogryposis is rarely successful. In bilateral hip dislocation associated with arthrogrypsis, the consensus is that the hips are best left unreduced because of the difficulty in obtaining excellent clinical and radiographic results bilaterally. Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685. Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Question 12
High Yield
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 13
High Yield
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?

Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 14
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?

Explanation
The radiograph reveals complete loss of joint space with particulate metal debris consistent with total polyethylene failure and metal-on-metal articulation. The components appear to be well fixed and minimal osteolysis is evident. Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
Question 15
High Yield
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Detailed Explanation
The tenosynovium excised at the time of a carpal tunnel release for idiopathic carpal tunnel syndrome rarely shows signs of acute or chronic inflammation. Fibrosis, edema, and vascular sclerosis are the most common histologic findings. A tenosynovectomy with a carpal tunnel release usually is not necessary in the treatment of idiopathic carpal tunnel syndrome. Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225. Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Question 16
Which of the following is considered the most effective means of identifying an evolving motor tract injury during cervical spine surgery?
Explanation
In a study of 427 patients undergoing cervical spine surgery, 12 patients demonstrated substantial or complete loss of amplitude of the tceMEPs. Ten of those patients had complete reversal of the loss following prompt intraoperative intervention. SSEP monitoring failed to identify any changes in one of the two patients that awoke with a new motor deficit. SSEP changes lagged behind the tceMEP changes in patients in which major changes were detected by both modalities. TceMEP monitoring was 100% sensitive and 100% specific. SSEP monitoring was only 25% sensitive and 100% specific.
Question 17
High Yield
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of

Detailed Explanation
The hallmark of neurogenic shock is hypotension without tachycardia. It is associated most commonly with high cervical spinal cord injuries and results from loss of function of the sympathetic nervous system. Because the peripheral vasculature is dilated due to loss of its sympathetic tone, continued rapid administration of fluid corrects the hypotension and can quickly lead to fluid overload and congestive heart failure. Therefore, neurogenic shock is best treated by the use of pressors. Cardioversion or administration of antibiotics or systemic steroids is not appropriate treatment for this patient's hypotension. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Question 18
A cortisone injection in the subacromial space will most likely result in
Explanation
A cortisone injection in the subacromial space will most likely result in elevated blood glucose levels in patients with type I diabetes mellitus. Patients should be warned of this potential complication. Cortisone does not have an effect on instability or proprioception, and a single injection would not affect osteoporosis. Repetitive injections or injection into the tendon itself could accelerate rupture of the biceps tendon. Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Question 19
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 20
What is the most likely type of pathology seen in Figure 16?

Explanation
The figure shows the missing pedicle or "winking owl" sign that is characteristic of tumor involvement of the cortical bone of the pedicle. None of the other pathologic processes commonly gives this radiographic picture. Thinned, but not missing pedicles, have been described as a normal variant. McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Question 21
High Yield
An adult patient has an 8- x 4- x 10-cm soft-tissue mass located within the adductor compartment of the thigh. Staging studies should consist of

Detailed Explanation
The appropriate staging studies should consist of MRI and a radiograph of the primary lesion and CT of the chest. MRI is superior to CT for soft-tissue imaging. CT may be useful for evaluating the cortex of bone for invasion by tumor. Bone scans are not commonly used because soft-tissue sarcomas rarely metastasize to bone. CT of the abdomen and pelvis is not typically ordered except for possible liposarcoma. With liposarcoma, there may be a synchronous or metastatic retroperitoneal liposarcoma. Demetri GD, Pollock R, Baker L, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Question 22
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20 degrees of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked "A," the resulting ligament reconstruction will excessively

Explanation
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90 degrees. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20 degrees to 0 degrees of flexion. If the graft is tensioned in significant flexion (greater than 60 degrees), it will be excessively loose as the knee fully extends. Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Question 23
High Yield
In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?

Detailed Explanation
The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step. Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Question 24
A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the most likely diagnosis?



Explanation
The radiograph shows a benign-appearing cortically based lesion eroding the underlying cortex, producing a saucer-shaped defect typical of a periosteal chondroma. The histology shows benign-appearing neoplastic cartilage. Although enchondroma would have the same histologic appearance, radiographs generally show a lesion with a central medullary epicenter. The benign-appearing histology does not support chondrosarcoma. Chondromyxoid fibroma will generally show histologic elements of its fibrous and myxoid components. Chondroblastoma typically demonstrates histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification. Schajowicz F: Tumors and Tumorlike Lesions of Bone: Pathology, Radiology, and Treatment, ed 2. Berlin, Springer-Verlag, 1994, pp 147-151.
Question 25
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?

Explanation
Congenital dislocation of the radial head is often confused with posttraumatic dislocation. The distinguishing feature here is the dome-shaped radial head. Some patients with congenital anomalies fail to recognize their limitations until an injury occurs. Soft-tissue contractures do not cause radial head dislocation nor do they usually cause this pattern of motion restriction (mainly flexion and rotation without significant loss of extension). There is no deformity of the ulna to suggest an old Monteggia lesion. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Question 26
High Yield
What structure is most often injured in a volar proximal interphalangeal joint dislocation?

Explanation
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Question 27
High Yield
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Detailed Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 28
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk. Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 29
A 45-year-old recreational tennis player underwent arthroscopic decompression and mini-open repair of a small supraspinatus tendon tear 3 weeks ago after nonsurgical management failed to provide relief. He now has pain, swelling about the wound, erythema, and purulent drainage. The patient is returned to the operating room for irrigation, debridement, and cultures. What is the most common organism causing this infection?

Explanation
In a large series of mini-open rotator cuff repairs, an infection rate of at least 2% was found, with the majority of the infections caused by Propionibacterium acnes. To prevent this complication, the shoulder should be re-prepped before the mini-open incision is made to prevent bacterial contamination from the arthroscopic procedure. Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 30
High Yield
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?



Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 31
High Yield
The orthosis shown in Figure 47 is commonly used for
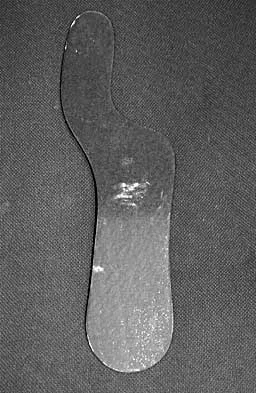
Explanation
The orthosis shown is a carbon reinforced Morton's extension, and it is commonly used for hallux rigidus. It decreases motion of the first metatarsophalangeal joint and subsequently decreases pain.
Question 32
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?





Explanation
Odontoid fractures can be classified based on the anatomic position of the fracture within the dens itself. Type I is an oblique fracture through the upper part of the odontoid process. Type II is a fracture that occurs at the base of the odontoid as it attaches to the body of C2; type III occurs when the fracture line extends through the body of the axis. Type 1 fractures typically can be treated nonsurgically with 6 to 8 weeks of immobilization with a semi-rigid cervical orthosis. Nondisplaced, deep type III fractures generally are treated with skeletal halo fixation. Deep, displaced, and angled type III fractures can be treated with closed reduction and skeletal halo fixation. Shallow type III fractures are sometimes amenable to anterior odontoid screw fixation. Type II fractures can be managed nonsurgically or surgically. Treatment options include halo immobilization, internal fixation (odontoid screw fixation), and posterior atlantoaxial arthrodesis. Management with the halo vest usually is considered if the initial dens displacement is less than 6 mm, the reduction is performed within 1 week of the injury and is able to be maintained, and the patient is younger than age 60 years. Halo vest immobilization can lead to a healing rate of more than 90%. Posterior surgical fusion techniques provide high fusion success rates but do so at the expense of cervical rotation. Up to 50% of rotation is lost with these techniques. Anterior odontoid single screw fixation is often tolerated better than skeletal halo fixation and also is noted to preserve the normal rotation at C1/C2. Studies have shown less of a malunion and nonunion rate in the treatment of type II odontoid fractures with anterior odontoid screw fixation. Osteoporosis, short neck and barrel-chested anatomy, and fractures that are more than 4 weeks old preclude anterior odontoid fixation. Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3. Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Question 33
High Yield
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of

Explanation
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate (greater than 50%) for treating MDI. Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am 2000;82:919-928.
Question 34
High Yield
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Detailed Explanation
Co-planing the distal clavicle may lead to painful acromioclavicular joints in up to 35% of patients; this is felt to be related to destabilizing the distal clavicle. Intra-articular diagnosis of synovitis, degenerative joint disease, and superior labrum anterior and posterior lesions would have been identified at initial arthroscopy (not necessarily seen in open surgery). Ganglions are seen on MRI. Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248. Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Question 35
High Yield
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
The obturator internus originates on the obturator membrane and adjacent bone, including the quadrilateral plate, and exits the lesser sciatic notch to insert on the posterior medial greater trochanter. The structure labeled C is the pectineus, B is the sartorius, and D is the gluteus medius. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Question 36
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
A muscle that lengthens as it is activated is an eccentric contraction. Isometric contraction involves no change in length. Concentric contraction occurs while the muscle is shortening. In isotonic contraction, the force remains constant through the contraction range. Isokinetic muscle contraction occurs at a constant rate of angular change of the involved joint. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 12-13.
Question 37
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
The etiology of hip fractures in the elderly is multifactorial, and intervention and prevention can occur at multiple points. Events leading to hip fracture from a fall include fall initiation (during which the individual's neuromuscular status, cognitive status, and vision come into play along with environmental hazards); fall descent (fall direction toward the side being the most influential, energy content of the fall, and fall height, along with muscle activity of the muscles of the thigh); impact (impact location, soft-tissue attenuation such as from trochanteric padding or from overlying fat, impact surface, and muscle activity); and the structural capacity of the femur (bone mineral density, bone geometry, and bone architecture). Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
Question 38
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include


Explanation
The radiographs do not show significant arthrosis of the hallux metatarsophalangeal joint; therefore, arthrodesis is unnecessary. Orthotics will not correct the deformity. A distally based osteotomy will not achieve sufficient correction of the incongruity of deformity, and a Keller resection is not indicated in the younger population. The treatment of choice is a proximal metatarsal osteotomy with second toe correction.
Question 39
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show


Explanation
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 40
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a

Explanation
The wound described indicates loss of soft tissue directly to the level of the tendon, precluding use of skin grafts if excursion of the tendon is desired. A cross-finger flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb. Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Question 41
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 42
High Yield
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of

Explanation
If the patient's medical condition and prognosis remain good in the presence of significant and progressive neurologic deficit from cord compression, then the most reliable means of restoring function is via surgical decompression and fusion. Decompression should be directed toward the compressing structure (eg, anteriorly if the compression is from the anterior side). This procedure can be done via a posterolateral technique, such as costotransversectomy in some cases.
Question 43
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?

Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 44
Figure 21 shows the radiograph of a 32-year-old patient with right hip pain that has failed to respond to nonsurgical management. What is the most appropriate surgical treatment at this time?

Explanation
The radiograph reveals developmental dysplasia of both hips. The patient has classic anterolateral undercoverage of the femoral head on the right side as demonstrated by a high acetabular index (measured at 27 degrees). Anterior undercoverage can be determined by drawing the marking for the anterior wall that fails to overlap the femoral head in this patient. Currently in North America, the most accepted surgical management for symptomatic dysplasia of the hip with good joint space is a Bernese (Ganz) periacetabular osteotomy. Surgical dislocation of the hip and femoroacetabular osteoplasty may be considered for patients with symptomatic femoroacetabular impingement of the hip. Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 45
High Yield
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
Uneven resection of bone, typically leaving a retained posterolateral corner of the distal clavicle, can lead to failure of arthroscopic distal clavicle excision. The amount of bone resected, the gender of the patient, or the diagnosis (osteoarthritis versus osteolysis) does not appear to affect the results.
Question 46
High Yield
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of


Explanation
The hallux varus seen in this patient is most likely the result of a combination of causes. Based on the degenerative changes and the significant shortening of the first metatarsal relative to the second metatarsal, a metatarsophalangeal arthrodesis is the treatment of choice. The other surgical approaches are not expected to provide a satisfactory result. Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Question 47
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?


Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 48
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of


Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 49
An otherwise healthy 75-year-old man has a painful mass in the popliteal fossa of his right knee. A lateral radiograph of the knee, a CT scan of the distal femur, and a histopathologic specimen are shown in Figures 13a through 13c. Management should consist of



Explanation
The patient has a parosteal osteosarcoma of the distal femur. The findings of mild knee pain, radiographic evidence of a radiodense mass involving the parosseous space or surface of the distal femur, and histologic findings of a spindle cell lesion forming immature osteoid with little to no necrosis most likely suggest a parosteal osteosarcoma. The treatment of choice is surgical resection. Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma: A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Scientific References
-
:
Question 50
Which of the following findings is considered a poor prognostic factor for postoperative neurologic recovery in patients with rheumatoid arthritis?
Explanation
When markedly diminished space available for the cord (demonstrated by a posterior atlantoaxial interval of less than 10 mm) is seen, there is a poor prognosis for recovery (25% of Ranawat class IIIb patients) following surgery. A posterior atlantoaxial interval of 14 mm or less is a predictor of increased risk of paralysis, but patients with an interval between 10 mm and 14 mm have a greater chance of recovery. Space available for the cord that is at least 14 mm is not associated with an increased risk of neurologic deficit. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 51
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of




Explanation
The patient has Ewing's sarcoma. Management options for local tumor control include radiation therapy, resection, or a combination; however, in this patient wide resection is preferred over radiation therapy. Radiation therapy is associated with damage to the growth plate, pathologic fracture, radiation-induced sarcomas, and a local recurrence rate of approximately 10% to 12%. Radiation therapy is used for positive margins, unresectable tumors, or for tumors that have a poor response to chemotherapy. Amputation is not necessary since the tumor is resectable. Chemotherapy has improved overall survival rates to over 60% of patients. Sailer SL: The role of radiation therapy in localized Ewing' sarcoma. Semin Radiat Oncol 1997;7:225-235. Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing's sarcoma. United Kingdom Children's Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704. Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Question 52
High Yield
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of


Explanation
The patient has extensor tendon ruptures at the level of the wrist that are the result of synovitis at the distal radioulnar joint (Vaughn-Jackson syndrome). Extensor indius proprius transfer appropriately matches strength and excursion of the ruptured extensor digiti quinti and extensor digitorum communis tendons. An extensor tenosynovectomy with distal radioulnar joint resection decreases the synovitis, which if left untreated may cause additional tendon ruptures. Radial head resection is used for posterior interosseous nerve compression secondary to radial head synovitis, and in this patient only two fingers are involved, which rules out this diagnosis. Dynamic splinting is not indicated for ruptured tendons. Metacarpophalangeal arthroplasties and imbrication of the sagittal bands are used for metacarpophalangeal arthritis and extensor tendon subluxation. If this was the problem, the patient should be able to maintain the fingers in extension after they are passively extended. Total wrist arthrodesis prevents the tenodesis effect, thus limiting effective tendon excursion and making the proposed transfer less effective. Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1669-1684. Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Question 53
High Yield
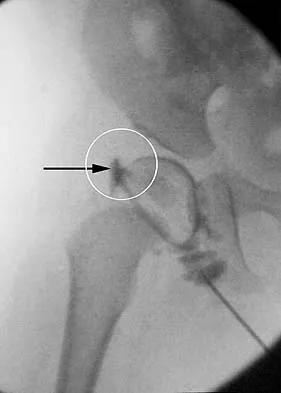
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
The structure enclosed by the circle is the acetabular labrum. It is visible as the white point of tissue outlined by the darkly radiopaque contrast. The appearance of the contrast surrounding the sharp white point of a normal labrum is called the "rose thorn sign." The limbus is the term reserved for a rounded, infolded labrum seen with arthrography. The pulvinar is the fatty tissue seen in the empty acetabulum when the hip is dislocated. The ligamentum teres is seen as a white stripe outlined by contrast coursing from the central acetabulum to the dislocated femoral head. The transverse acetabular ligament courses across the inferior portion of the acetabulum and is not clearly seen with arthrography. Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 532-533.
Question 54
High Yield
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of


Explanation
The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
Question 55
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?



Explanation
Malignant fibrous histiocytoma (MFH) is the most common soft-tissue sarcoma. MFH typically presents as a large mass, deep to the fascia with heterogeneous signal on MRI. The MRI scans show a heterogeneous lesion in the posterior thigh. There is significant high signal uptake on the T2-weighted image. The histology shows malignant histiocytic cells with marked atypia and pleomorphism. Histology of a hematoma would show only old hemorrhage and some granulation tissue. Lipoma and liposarcoma are both seen as a fat-containing lesion on histology. No significant fat tissue is seen in this histologic specimen. Histology of myositis ossificans would show bone formation. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 56
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome. Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Question 57
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 58
High Yield
What gene is expressed the earliest during the differentiation of a chondrocyte during endochondral ossification?
Detailed Explanation
Transcription factors regulate the activation or repression of cartilage-specific genes. Sox-9, considered a major regulator of chondrogenesis, regulates several cartilage-specific genes during endochondral ossification, including collagen types II, IV, and XI and aggrecan. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 59
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?


Explanation
The patient has a global loss of motion that has failed to improve with 6 months of nonsurgical treatment; because he has reached a plateau, further nonsurgical management will likely be ineffective. Revision in the form of an open release is indicated to lyse intra- and extra-articular adhesions; subscapularis lengthening may be done concurrently as needed. Revising to a smaller head can be considered if adequate motion is not achieved. The radiographs reveal an adequate neck cut with appropriate seating of the component. Removing the glenoid component will decrease capsular tension but will probably increase pain because of the lack of glenoid resurfacing. Increasing humeral retroversion will not improve motion. Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Question 60
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include

Explanation
Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 61
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?


Explanation
The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 62
A 2-year-old boy has been referred for musculoskeletal evaluation. Examination reveals shortened proximal limbs, hip and knee flexion contractures, an abducted thumb, and ear abnormalities. His parents are concerned about his deformed feet. What is the most common foot deformity associated with this patient's diagnosis?
Explanation
The patient has diastrophic dysplasia. Affected individuals have rhizomelic short stature, cauliflower ears, severe joint contractures (especially knees and hips), hitchhiker's thumb, and a cleft palate. The most common foot abnormality is a rigid equinovarus deformity. Surgical results are poorer than those for idiopathic clubfeet and often require bony procedures or talectomy. Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-444.
Question 63
What cell type causes the bone destruction in metastatic lesions?
Explanation
The main consequence of tumor invading the bone is activation of both osteoblasts and osteoclasts. However, the osteoclastic effect predominates in the majority of tumors early after the invasion of bone by tumor cells, causing resorption of bone. Cramer SF, Fried L, Carter KJ: The cellular basis of metastatic bone disease in patients with lung cancer. Cancer 1981;48:2649-2660.
Question 64
High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 65
High Yield
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 66
High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of


Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 67
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?

Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 68
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
Latissimus dorsi tendon transfer is considered a surgical option for treatment in patients with chronic supraspinatus and infraspinatus tendon tears. Preoperative subscapularis function is necessary for good clinical results. Additionally, men with active elevation to shoulder level and active external rotation to 20 degrees have predictably good results. Women with active shoulder elevation limited to below chest level have poor results from this procedure and should not be considered candidates. Postoperatively they lack pain control, active elevation, and active external rotation. Muscular atrophy in the latissimus dorsi does not occur, and glenohumeral arthritic changes frequently develop postoperatively. Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am 2006;88:113-120.
Question 69
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
Question 70
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman's test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
The patient has chronic posterolateral instability with a varus knee alignment; therefore, the most effective treatment is a valgus-producing HTO. A repeat soft-tissue reconstruction without correction of the varus alignment will most likely fail. An ACL reconstruction is not indicated with a normal Lachman's test. Physical therapy and bracing will have little effect. Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Question 71
High Yield
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?

Explanation
The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty. Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Question 72
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?



Explanation
The biopsy specimen is a low-power view of a soft-tissue sarcoma with a biphasic pattern of epithelial cells and fibrous spindle cells that are typical of a synovial sarcoma. A deep, painless soft-tissue mass greater than 5 cm in size is suspicious for a sarcoma. The imaging in this patient is indeterminate and the patient requires a biopsy for an accurate diagnosis. The biopsy reveals a tumor with a biphasic appearance consistent with a synovial sarcoma. These tumors are slow growing, occur primarily in the lower extremities, and are found in a younger demographic population compared to malignant fibrous histiocytoma and liposarcoma. They can occur in a biphasic pattern with clumps of epithelial cells and fibrous spindle cells or in a monophasic pattern. Synovial sarcomas stain positively for keratin. Keratin is positive in nearly all biphasic types and in many tumors of the monophasic fibrous type. Sixty percent of these tumors are found in the lower extremity. The area around the knee is the most common location, followed by the ankle and foot. Epithelioid and clear cell sarcomas are found associated with tendon sheaths of the hand and feet and are generally smaller in size. Epithelioid sarcoma may resemble granulomatous inflammation histologically; clear cell sarcoma is composed of nests of clear cells with occasional multinucleated giant cells. Pigmented villonodular synovitis is found within the synovium and is characterized by a villous histologic appearance with hemosiderin-laden macrophages. Malignant fibrous histiocytoma has a storiform histologic pattern with an abundance of pleomorphic cells. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 757.
Question 73
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 74
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of




Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 75
High Yield
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
The popliteal artery lies just posterior to the posterior cruciate ligament tibial insertion, separated only by the posterior capsule of the knee. When performing a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation of the tibial tunnel. Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Question 76
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 77
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.
Question 78
High Yield
What is the most common reason for reoperation in total knee arthroplasty?

Detailed Explanation
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 79
High Yield
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Detailed Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 80
High Yield
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient's family reports that he is a Jehovah's Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient's blood pressure becomes unstable. What is the most appropriate action?
Explanation
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah's Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah's Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open would is not recommended nor would there likely be enough from an open tibial fracture to salvage. The patient's family may be expressing their own beliefs rather than the patient's beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability. Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 81
A 62-year-old woman has back pain and right L2 radicular pain. MRI scans suggest a neoplastic lesion at L2, and a bone scan is negative except at L2. History reveals that she was treated for breast cancer without known metastatic disease 12 years ago and is thought to be free of disease. What is the next most appropriate step in management?
Explanation
Because of the long disease-free interval, it cannot be assumed that this is breast cancer. The lesion could represent metastasis from a new primary tumor or could itself be a primary tumor. CT-guided biopsy will most effectively identify the lesion and guide treatment options. Depending on the specific diagnosis, any of the other options may be appropriate.
Question 82
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 83
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?


Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 84
High Yield
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 85
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 86
High Yield
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of


Explanation
The patient has the findings of classic subacromial impingement. Initial management should consist of stretching exercises directed at the posterior capsule and a program of rotator cuff and deltoid strengthening exercises performed below the horizontal in a "safe" plane. The judicious use of subacromial cortisone injections (one or two) may be helpful. Anterior acromioplasty is reserved for patients who have failed to respond to nonsurgical management. Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737. Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Question 87
High Yield
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches


Detailed Explanation
Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000. Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Question 88
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 89
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?



Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
Question 90
High Yield
The arrow in Figure 39 is pointing to which of the following ligaments?

Detailed Explanation
The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The scapholunate interosseous ligament stabilizes the scapholunate joint. The ulnolunate ligament originates from the base of the ulnar styloid and inserts in the lunate. The ulnotriquetral ligament originates from the base of the ulnar styloid and inserts on the triquetrum. The ulnolunate and the ulnotriquetral ligaments are important stabilizers to the ulnar side of the wrist. The short radiolunate ligament originates on the volar ulnar margin of the distal radius and inserts in the ulnar margin of the lunate. Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 91
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?


Explanation
Alcohol abuse, steroids, Caisson disease, sickle cell disease, and radiation therapy are the leading causes of nontraumatic osteonecrosis of the femoral head. Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
Question 92
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?

Explanation
The patient has a failed Silastic implant. Nonsurgical management will not work at this point. A Keller resection will only exacerbate her metatarsalgia. Implant removal with structural bone grafting and MTP fusion is the most appropriate choice because restoration of length is needed to alleviate the forefoot pain and bone grafting is required to fuse the MTP joint because there is an abundance of osteolysis. Total toe implants do not offer good long-term outcomes and are very difficult to fit into the large exploded-out cavity of the proximal phalanx. Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Question 93
High Yield
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?

Detailed Explanation
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Question 94
High Yield
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?
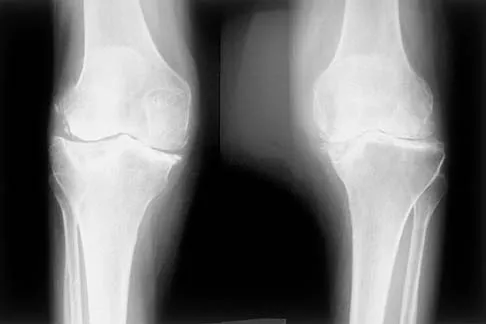
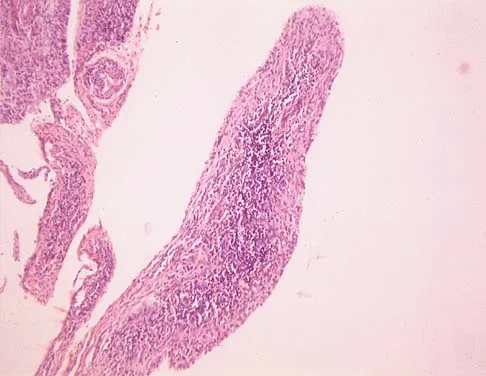
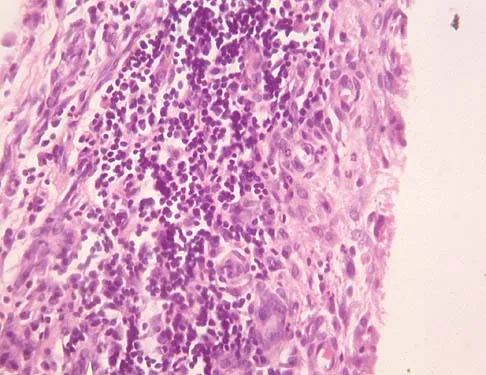
Explanation
Rheumatoid arthritis is an inflammatory arthritis that usually involves multiple joints. Radiologic findings of periarticular erosion, osteopenia, and minimal osteophyte formation favor rheumatoid arthritis over osteoarthritis. Pigmented villonodular synovitis and Charcot arthropathy are more often considered monoarticular diseases. There are no radiographic findings of Paget's disease.
Question 95
High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 96
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of


Explanation
The plain radiographs reveal a pedunculated osteochondroma with a fracture. There is a bony growth in the metaphysis of a long bone, on a stalk that is directed away from the nearby epiphysis. On the AP view, the host cortical and medullary bone are shown as "blending" with lesional bone. There is also a fracture through the lesion. Based on these radiographic findings, the diagnosis is an osteochondroma; therefore, initial management of an acute fracture of an osteochondroma is symptomatic treatment alone. Additional imaging studies are not indicated in this patient. At times it may be difficult to distinguish a sessile osteochondroma from a parosteal osteosarcoma. In the latter case, the host medullary bone and lesion bone are not confluent. A CT scan may be helpful to distinguish if the host medullary and cortical bone are confluent with the lesion.
Question 97
High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 98
High Yield
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 99
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?

Explanation
Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH ("athlete's heart") from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm). Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete's heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436. Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Question 100
High Yield
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization. Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
