Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
Detailed Explanation
Kondrashov and associates noted stable good outcomes at 4 years in 14 of 18 patients treated with X-STOP interspinous process decompression as defined as an improvement over preoperative Oswestry scores of 15 points or more. Similar results were seen after 1 year in a European study by Siddiqui and associates. Exclusion and inclusion criteria for these studies varied somewhat, but cauda equina syndrome was the only exclusion criteria listed in both studies. All of the other choices did not represent exclusion criteria in either study. Kondrashov DG, Hannibal M, Hsu KY, et al: Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study. J Spinal Disord Tech 2006;19:323-327.
Question 2
High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?

Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44. Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Question 3
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?


Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 4
High Yield
When performing an arthroscopic subacromial decompression, bleeding can be encountered when dividing the coracoacromial ligament because of injury to what artery?
Detailed Explanation
The acromial branch of the thoracoacromial trunk courses along the coracoacromial ligament. This artery enters the ligament approximately 5 mm below the acromial edge. Division of the ligament at its insertion on the acromion minimizes the risk of bleeding. Esch JC, Baker CL: Arthroscopic anatomy and normal variations, in Whipple TL (ed): Surgical Arthroscopy: The Shoulder and Elbow. Philadelphia, PA, JB Lippincott, 1993, pp 63-76.
Question 5
High Yield
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Detailed Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 6
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of

Explanation
Because the patient's shoulders are overtensioned anteriorly, premature osteoarthritis may develop. This may create obligate translation posteriorly and increase the interarticular pressure of the humeral head against the glenoid. Patients should achieve 20 degrees to 30 degrees of external rotation with the elbow at the side. Late degenerative arthritis following a Putti-Platt procedure is associated with significant restriction of external rotation. This patient's shoulder has a reduced risk of anterior instability, rotator cuff tear, and internal impingement because of the limitation of motion. Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 7
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
Cadaveric studies have shown that external rotation of the tibia is most pronounced following transection of the posterior cruciate and lateral collateral ligaments with the knee at 90 degrees of flexion. Isolated release of the lateral collateral ligament results in increased external tibial rotation at 30 degrees. Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242. Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Question 8
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
The patient sustained an injury to the long thoracic nerve, which supplies the serratus anterior. Branches of C5 and C6 enter the scalenus medius, unite in the muscle, and emerge as a single trunk and pass down the axilla. On the surface of the serratus anterior, the long thoracic nerve is joined by the branch from C7 and descends in front of the serratus anterior, providing segmental innervation to the serratus anterior.
Question 9
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?


Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 10
High Yield
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?

Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 11
High Yield
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?



Explanation
The radiographs reveal osteoarthritis and proximal humeral head migration. Integrity of the rotator cuff must be questioned based on these radiographic changes. The status of the rotator cuff is the most influential factor affecting postoperative function in shoulder hemiarthroplasty. The coracoacromial ligament provides a barrier to humeral head proximal migration in the face of a rotator cuff tear. The radiographs do not indicate significant humeral head or glenoid erosion. Acromioclavicular arthritis is often asymptomatic. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 12
High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Detailed Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 13
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of


Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 14
High Yield
Turf toe typically involves injury to which of the following structures of the great toe?
Detailed Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 15
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?

Explanation
Isolated split posterior tendon transfer alone is best performed in a patient with cerebral palsy who is between the ages of 4 and 7 years and has a flexible equinovarus foot. Rigid deformities often must be managed with a combination of soft-tissue and bony procedures. Patients with out-of-phase activity may be best managed with a transfer of the posterior tibialis to the dorsum of the foot, while those with continuous activity are better candidates for an isolated split posterior tendon transfer. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Question 16
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?



Explanation
The epiphyseal location on the radiograph and MRI scan and the histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification all suggest chondroblastoma. Although giant cell tumors of bone typically occupy an epiphyseal location, they are rare in children and when present are often metaphyseal in skeletally immature patients. Enchondromas and osteoblastomas are generally metaphyseal and, along with giant cell tumors, have very different histology than seen here. Chondromyxoid fibromas are typically metaphyseal in location. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Question 17
A 19-year-old woman has a painful right knee. A radiograph, MRI scan, CT scan, and histopathologic specimen are shown in Figures 24a through 24d. What is the most likely oncologic stage of the lesion?




Explanation
The patient has a high-grade osteosarcoma of the distal femur with a skip lesion, and pulmonary metastasis is seen on the CT scan. This corresponds to a stage III lesion according to the Musculoskeletal Tumor Society System as adopted from Enneking.
Question 18
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of

Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 19
Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?

Explanation
Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy. Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.
Question 20
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
The patient has extensive degenerative changes in both the medial and lateral compartments within the knee; therefore, arthroscopic debridement or an osteotomy will not be helpful. A patellar arthroplasty will not address the medial and lateral compartments. Because the extensor mechanism provides a significant amount of anteroposterior stability, a posterior cruciate-substituting total knee arthroplasty is the treatment of choice for this patient. Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Question 21
High Yield
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
Repetitive subfailure strains have been shown to affect the mechanical behavior of the inferior glenohumeral ligament, producing dramatic declines in the peak load response and length increases that are largely unrecoverable. In another study, anteroinferior subluxation was found to result in nonrecoverable strain in the anteroinferior capsule, varying from 3% to 7% through a range of joint subluxation. Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Question 22
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of

Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 23
High Yield
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?



Explanation
The axial views show fusion of the talus and calcaneus at the medial facet (talocalcaneal coalition). Peroneal spastic flatfoot is a descriptive term applying to the symptoms of painful flatfoot associated with apparent peroneal spasm and is sometimes caused by tarsal coalition; however, this is not the most appropriate diagnosis for this patient. Flexible flatfoot with a short Achilles tendon often causes symptoms similar to the ones listed above, but subtalar motion should be normal. A diagnosis of calcaneonavicular coalition can be made based on plain oblique views of the foot but is not seen in these views. Posterior tibial tendon dysfunction in the absence of other pathology is uncommon in children. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 24
Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
Explanation
Arthrodesis of the talonavicular joint eliminates almost all hindfoot motion. Arthrodesis of the subtalar joint eliminates 74% of talonavicular motion and 44% of calcaneocuboid motion. Arthrodesis of the calcaneocuboid joint eliminates 33% of talonavicular motion and 8% of subtalar motion. Arthrodesis of the naviculocuneiform or cuboid-fifth metatarsal joint has limited effect on hindfoot motion. Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.
Question 25
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of


Explanation
The patient has lung cancer metastatic to the right proximal femur. The lesion is large, has destroyed a portion of the cortex, and involves the peritrochanteric region. All of these findings put the patient at high risk for pathologic fracture. The lesion is amenable to intramedullary fixation in the form of some type of reconstruction nail. Chemotherapy alone will not restore the bone stock. Given the extent of the lesion, radiation therapy, chemotherapy, or embolization will not prevent fracture. A proximal femoral replacement would be indicated in patients with bone destruction extending into the femoral head and neck. Bisphosphonates may diminish the risk of subsequent lesions but are not sufficient to treat this high-risk lesion. Radiation therapy should be given postoperatively to prevent further bone destruction.
Question 26
High Yield
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?

Detailed Explanation
The femoral nerve is the most lateral structure in the anterior neurovascular bundle. The femoral artery and vein lie medial to the nerve. Retractors placed in the anterior acetabular lip should be safe, although neurapraxia of the femoral nerve may occur if retraction is prolonged or forceful leading to quadriceps weakness. The femoral artery and nerve are well protected by the interposed psoas muscle. Damage to the lateral femoral cutaneous nerve, causing numbness over the anterolateral thigh, can occur while developing the interval between the tensor fascia latae and sartorious in the anterior (Smith-Petersen) approach but less likely in the Watson-Jones approach. Superior gluteal injury and accompanying abductor insufficiency may occur during excessive splitting of the glutei during the direct lateral (Hardinge) approach. Foot drop secondary to sciatic injury is more common with a posterior exposure or posterior retractor placement. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Question 27
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of


Explanation
The plain radiographs reveal a pedunculated osteochondroma with a fracture. There is a bony growth in the metaphysis of a long bone, on a stalk that is directed away from the nearby epiphysis. On the AP view, the host cortical and medullary bone are shown as "blending" with lesional bone. There is also a fracture through the lesion. Based on these radiographic findings, the diagnosis is an osteochondroma; therefore, initial management of an acute fracture of an osteochondroma is symptomatic treatment alone. Additional imaging studies are not indicated in this patient. At times it may be difficult to distinguish a sessile osteochondroma from a parosteal osteosarcoma. In the latter case, the host medullary bone and lesion bone are not confluent. A CT scan may be helpful to distinguish if the host medullary and cortical bone are confluent with the lesion.
Question 28
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed "quadriceps avoidance." This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45 degrees of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability. Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20. Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Question 29
Osteoclasts originate from which of the following cell types?
Explanation
Osteoclasts originate from the monocyte/macrophage lineage. Fibroblasts and osteoprogenitor cells originate from mesenchymal stem cells and do not form osteoclasts. Plasma cells reside in the bone marrow and are derivatives of the hematopoietic system. Megakaryocytes are also in the bone marrow and synthesize platelets. Zaidi M, Blair HC, Moonga BS, et al: Osteoclastogenesis, bone resorption, and osteoclast-based therapeutics. J Bone Miner Res 2003;18:599-609. Brinker MR: Bone (Section 1), in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 1-35.
Question 30
What are the five most common tumors that metastasize to bone?
Explanation
The five most common primary carcinomas that metastasize to bone are breast, prostate, lung, renal, and thyroid in decreasing order of incidence. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 31
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
In this age group of patients with arthrogryposis, open reduction through a medial approach is generally recommended. Open reduction through an anterior approach is reserved for patients in which a medial approach has failed or for older patients who require simultaneous femoral shortening and/or pelvic osteotomy. Closed treatment of unilateral hip dislocation in association with arthrogryposis is rarely successful. In bilateral hip dislocation associated with arthrogrypsis, the consensus is that the hips are best left unreduced because of the difficulty in obtaining excellent clinical and radiographic results bilaterally. Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685. Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Question 32
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient's pain. Treatment should now consist of
Explanation
Children with symptomatic severe torsional malalignment of the lower extremity and patellofemoral pathology show excessive femoral anteversion and external tibial torsion on physical examination and analysis of gait. The functional effect of this torsional malalignment is centered about the knee joint. If nonsurgical management fails to alleviate patellofemoral pain, definitive surgical treatment should consist of corrective osteotomies, including internal rotation of the distal part of the tibia or external rotation of the femur, or both. Patients with surgical correction by osteotomy show an improved gait pattern and appearance of the extremity and a marked decrease in knee pain. External rotation of the distal part of the tibia or internal rotation of the distal part of the femur worsens the torsional malalignment. No additional soft-tissue realignment procedures, including retinacular release or patellar realignment, are required.
Question 33
High Yield
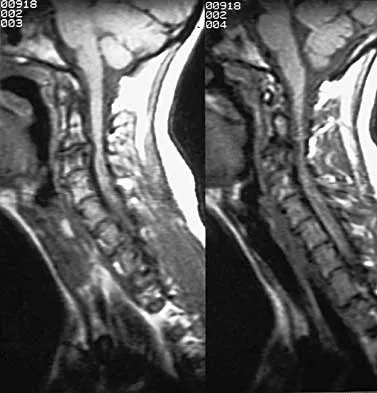
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?

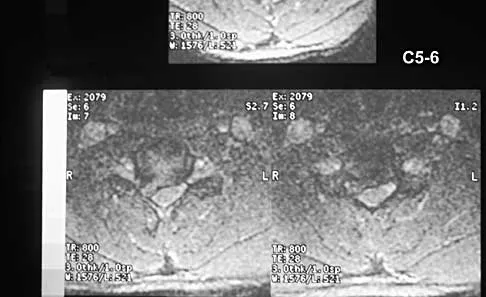
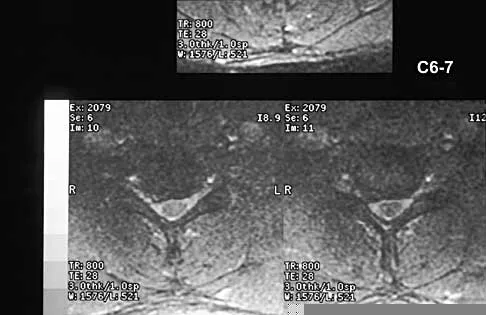
Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 34
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?

Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 35
High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 36
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches


Explanation
Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000. Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Question 37
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 38
High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?

Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 39
High Yield
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?


Explanation
The clinical photograph shows a rocker-bottom deformity, and the lateral radiograph suggests a congenital vertical talus deformity. A lateral radiograph of the foot in maximum plantar flexion is needed to demonstrate the fixed position of the deformity with malalignment of the talar-metatarsal axis. A fixed dislocation of the navicular on the talus differentiates a congenital vertical talus from the oblique talus with talonavicular subluxation. Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251. Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 40
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel's sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient's pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms. Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161. An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 41
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 42
High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 43
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 44
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
Using an infraspinatus-splitting incision allows for excellent exposure of the posterior capsule and minimizes the risk of injury to the axillary nerve which lies inferior to the teres minor in the quadrilateral space. Dreese J, D'Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207. Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Question 45
High Yield
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of

Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 46
High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 47
High Yield
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization. Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Question 48
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
It has been proposed that an imbalance in the proteolytic cascade involving matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) may play a role in the development or progression of malignancy. TIMP activity has been shown to be weak or nonexistent and MMP activity to be high in patients with soft-tissue sarcoma. The level of vascular endothelial growth factor is shown to be a negative prognostic indicator because the expression of this factor is associated with angiogenesis and aggressive growth of many tumors including Ewing' s sarcoma and chondrosarcoma. Stromelysin is a type of MMP. The biology of cytokines in malignancy is complex. A low level of interleukin-1 is not known to be associated with high-grade tumors.
Question 49
High Yield
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 50
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 51
High Yield
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 52
High Yield
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?
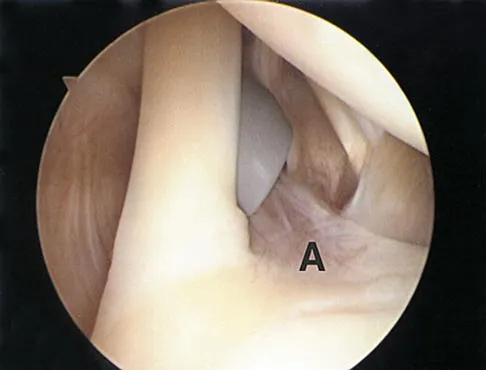
Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 53
High Yield
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis?

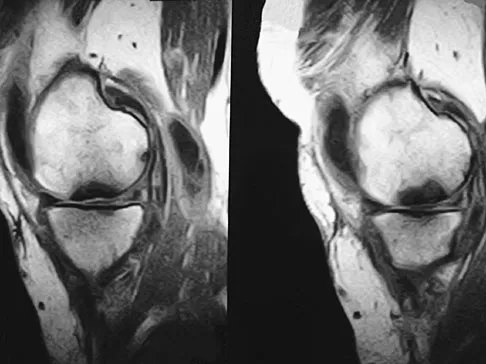
Explanation
Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial. Kidwai AS, Hemphill SD, Griffiths HJ: Spontaneous osteonecrosis of the knee reclassified as insufficiency fracture. Orthopedics 2005;28:236,333-336. Soucacos PN, Xenakis TH, Beris AE, et al: Idiopathic osteonecrosis of the medial femoral condyle: Classification and treatment. Clin Orthop 1997;341:82-89.
Question 54
Figure 16 shows the radiograph of a 7-year-old boy who sustained a pathologic fracture of the left humerus 1 day ago. Initial management should consist of

Explanation
The radiograph shows a pathologic fracture through a unicameral (simple) bone cyst (UBC). This is the most common location and presentation of a UBC. Less than 10% of UBCs heal spontaneously following a fracture. Urgent biopsy is not indicated because the lesion appears benign and the histology of fracture callus may be misinterpreted as osteosarcoma. After the fracture heals with the use of a sling and swathe, the UBC may be treated with a minimally invasive procedure such as injection of bone marrow and/or demineralized bone matrix. The chance for success is relatively low in an active cyst located adjacent to the physis. More invasive procedures, such as curettage, Rush rod fixation, or cannulated screw decompression, have been described but are rarely necessary for treatment of upper extremity cysts. Rougraff BT, Kling TJ: Treatment of active unicameral bone cysts with percutaneous injection of demineralized bone matrix and autogenous bone marrow. J Bone Joint Surg Am 2002;84:921-929. Robosch A, Saraph V, Linhart WE: Flexible intramedullary nailing for the treatment of unicameral bone cysts in long bones. J Bone Joint Surg Am 2000;82:1447-1453.
Question 55
High Yield
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 56
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.
Question 57
A 12 1/2-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of


Explanation
This skeletally immature patient has a small OCD lesion that appears stable, and he has not undergone any treatment. Therefore, a trial of immobilization until pain resolves is the best initial choice. Thereafter, cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients who have not shown radiographic evidence of healing and are still symptomatic after 6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture. Wall E, Von Stein D: Juvenile osteochondritis dissecans. Orthop Clin North Am 2003;34:341-353.
Question 58
High Yield
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 59
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 60
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in

Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 61
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%. Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294. Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Question 62
High Yield
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of

Explanation
The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment. Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650. Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737. Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am 1988;70:982-991.
Question 63
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 64
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?

Explanation
A DEXA scan is most appropriately used to establish a baseline score. Even if the bone mineral density is not within the osteoporotic range (T-score less than -2.5), a prior fragility fracture is a strong risk factor for a second fracture as a result of factors other than bone density, such as worsening vision or balance, confusion, or other predispositions to falls. The guidelines of the National Osteoporosis Foundation indicate that, following a fragility hip fracture, active anti-osteoporotic medication should be initiated, whether or not a DEXA scan is performed. A recent study showed that antiresorptive therapy following a hip fracture reduces not only the risk of a second fracture but also overall mortality.
Question 65
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a

Explanation
Complications of thermal capsule shrinkage or accelerated rehabilitation include capsule ablation. Since the original surgery did not include labral reattachment, findings of a Bankart lesion or a glenoid fracture from a nontraumatic injury are unlikely. Subscapularis detachment or biceps subluxation is a postoperative complication of open repairs. Failure of early postoperative instability treatment should not produce loose bodies. Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Question 66
High Yield
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include


Explanation
The radiographs show Ficat and Arlet stage 2 osteonecrosis. The femoral head remains round, and there are sclerotic changes in the superolateral quadrant. Patients with systemic lupus erythematosus are at risk for osteonecrosis because of prednisone use and the underlying metabolic changes associated with the condition (hypofibrinolysis and thrombophilia). MRI is the best diagnostic method for detecting osteonecrosis, with a greater than 98% sensitivity and specificity. For this patient, an MRI can assess the contralateral hip for any involvement and can quantify the extent of the lesion. Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 67
High Yield
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 68
High Yield
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
Surgical open reduction may increase the neurologic deficit if a disk herniation exists. Evidence from animal studies suggests that rapid decompression of the spinal cord may improve recovery. Serially increasing traction weight to reduce the dislocation has been shown to be safe when used in patients who are awake. Indications for MRI include patients who are unable to cooperate with serial examinations, the need for open reduction, and progression of deficit during awake reduction. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am 1995;77:1042-1049. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 69
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of
Explanation
Following a CVA, the muscular imbalance often leads to a fixed contracture of the shoulder in adduction, internal rotation, and flexion. The responsible muscles include the pectoralis major, subscapularis, teres major, and latissimus dorsi. If stretching cannot produce enough improvement for axillary hygiene, then surgery is an option. If the shoulder resists external rotation during examination with the arm at the side, as in this patient, then the subscapularis is spastic and contributing to the deformity as well and needs to be released along with the pectoralis. Phenol nerve blocks are most effective and best given within 6 months of the initial CVA to be effective. Lidocaine blocks may be helpful in determining whether a deformity is caused by a fixed soft-tissue contracture or by spasticity but play no role once the contracture is present. The modified L'Episcopo procedure is indicated in patients with contracture secondary to brachial plexus birth palsies. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 70
High Yield
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 71
A 70-year-old woman had poliomyelitis as a young child, and the residual weakness she has as an adult principally involves the lower extremities. She now notes progressive weakness in both legs and she tires easily. What is the best course of action?

Explanation
The most likely diagnosis is postpolio syndrome, which is characterized by increasing weakness in both the paretic and previously normal muscles. Fatigability, joint pain, muscle atrophy, respiratory insufficiency, dysphagia, and sleep apnea are also seen. Gentle exercise and modification in lifestyle demands are generally recommended. Vigorous rehabilitation is likely to be detrimental in this condition. Further diagnostic work-up is not indicated at this time. Dalakas MC, Elder G, Hallett M, et al: A long-term follow-up study of patients with post-poliomyelitis neuromuscular symptoms. N Eng J Med 1986;314:959-963.
Question 72
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of



Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 73
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 74
High Yield
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include


Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 75
High Yield
Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?

Detailed Explanation
The most common complication following acetabular or pelvic ring injury is deep venous thrombosis (DVT). Without prophylaxis, rates of DVT are as high as 70% to 80%. With prophylaxis, the rates are around 10%. Infection rates in surgical repair of acetabular fractures are relatively low but a history of diabetes mellitus and a significant Morel-Lavalle lesion certainly increase the risk. However, even with these two complicating factors, the rates of infection are still lower than 10%. Sciatic nerve palsy rates from the injury alone approach 20% and iatrogenic injury is usually less than 2%. Degenerative changes to the hip following this injury approach 20% to 25%, even with an anatomic reduction. Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.
Question 76
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 77
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?


Explanation
This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear. Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573. Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 78
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 79
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 80
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 81
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in

Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 82
High Yield
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?

Explanation
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
Question 83
High Yield
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Question 84
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
The rate of complications increases as the pin moves farther from the ideal position, which is the center of the head. This is the strongest argument for the use of a single pin. The highest rate of complications, primarily osteonecrosis and pin penetration, is associated with pin placement in the anterior superior quadrant. Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 85
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 86
High Yield
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
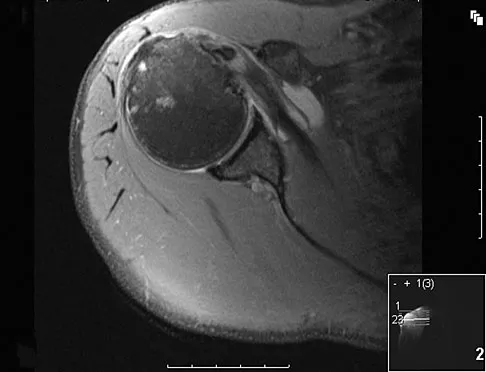
Explanation
The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 87
High Yield
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
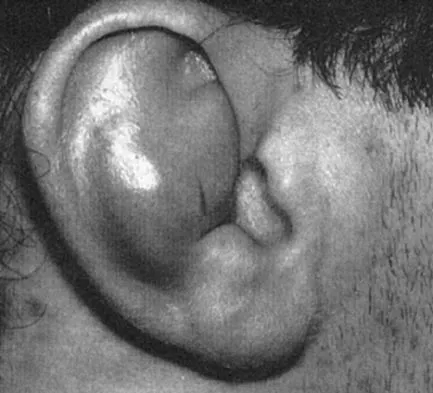
Explanation
Loss of internal rotation is common among overhead throwers and tennis players. Posterior capsular stretching can improve symptoms when accompanied by rest and gradual resumption of throwing. To avoid a false impression of improvement, cortisone injection is not recommended. Pitching through pain can cause further damage to the labrum and capsule. A sling and external rotator strengthening will not improve internal rotation. Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Question 88
High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?

Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 89
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 90
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of

Explanation
During the initial healing phases of a dural tear, pia and arachnoid from adjacent nerve roots migrate, fill the dural defect, and create a pia-arachnoid plug. It is this initial plugging of the defect that is believed to prevent further egress of cerebrospinal fluid through the defect. The plug has been shown to develop by the second postoperative day. Fibroblastic proliferation occurs within the dura itself and accounts for the bulbous ends of the dura seen in the photomicrograph. The appearance of the material within the dural edges is inconsistent with the appearance of neural elements, and scar tissue formation occurs later in the healing process. Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 91
High Yield
A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?

Detailed Explanation
The patient has gouty arthropathy of the first metatarsophalangeal joint. This definitive diagnosis is achieved with aspiration of the joint and polarized light microscopy that shows needle-shaped negatively birefringent monosodium urate crystals. Differential diagnoses of infectious arthritis and pseudogout are also definitively made through joint aspiration. Although rheumatoid arthritis is a possibility, a serum rheumatoid factor is not always diagnostic and a patient with rheumatoid arthritis may have concomitant gouty arthritis. The radiographic findings are not typical of diabetes mellitus or of a patient with Charcot arthropathy. Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.
Question 92
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
Curettage and bone grafting typically are the preferred treatment of chondroblastoma, yielding acceptable local recurrence rates of less than 10%. Some surgeons advocate adjuvant therapies such as phenol, liquid nitrogen, or argon beam coagulation. Untreated, these lesions can destroy bone and invade the joint to a significant degree. Large intra-articular lesions may require major joint reconstruction. Wide local excision is rarely required to control the tumor. Radiation therapy is indicated only in unresectable lesions. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Question 93
High Yield
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of

Detailed Explanation
Based on the mechanism of injury and findings of medial laxity, the most likely diagnosis is injury to either the growth plate or the medial collateral ligament. With the open physeal plate, this area of injury is presumed present until proven otherwise; therefore, stress radiographs should be obtained before implementing any treatment or ordering more extensive and expensive tests. DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 406-432. Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Question 94
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of

Explanation
Patients require prophylaxis for heterotopic bone after resection to prevent recurrence. The optimal management has been found to be a dose of 700 cGy in one dose delivered either pre- or postoperatively. A dose of 2,000 to 3,000 cGy is considered excessive. Radiation therapy consisting of 1,000 cGy in five doses is an acceptable prophylaxis; however, it will require an extended hospital stay of 3 to 4 days and is more problematic for the patient who must be transported for radiation therapy for 5 days. A dose of 400 cGy is not as effective in prophylaxis for heterotopic bone formation. Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595. Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Question 95
High Yield
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?




Detailed Explanation
The patient sustained a growth plate fracture of the distal radius and ulna. Although treated with closed reduction and casting, the follow-up radiographs demonstrate shortening of the radius in comparison to the ulna, and the MRI scan confirms thinning of the distal radius growth plate and bony bars consistent with a growth arrest. At this time, the discrepancy in length is too minor to consider lengthening of the radius; in addition, excision of a physeal bar with minimal growth potential is not likely to restore the gross discrepancy. Ulnar styloid fractures are rarely symptomatic and do not require treatment in the asymptomatic patient. Closure of the distal ulna growth plate will prevent further discrepancy between the radius and ulna. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Question 96
High Yield
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of

Explanation
Children have a much greater capacity to heal soft-tissue injuries than adults. Most crush or avulsion fingertip amputations in children, particularly those younger than age 2 years, can be treated with serial dressing changes, even with bone exposed. Das SK, Brown HG: Management of lost finger tips in children. Hand 1978;10:16-27.
Question 97
Optimal management of the injury shown in Figure 31 should include which of the following?

Explanation
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Question 98
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
Mild scoliosis is not a painful condition, but it usually presents during adolescence. Intermittent back pain is reported by 25% to 30% of adolescents whether or not scoliosis is present. Such pain is often attributed to muscle strain from tight muscles, poor posture, or heavy school backpacks. The clinician must distinguish typical pain (mild, intermittent, nonlimiting) from atypical pain. The latter requires more careful examination and imaging studies (bone scan or MRI) to determine the source of pain. The patient's age and right thoracic curve pattern are typical for idiopathic scoliosis; therefore, imaging of the neuroaxis is not necessary to look for cord syrinx, tethering, or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368. Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
Question 99
High Yield
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?


Detailed Explanation
The arrow is pointing to a cystic-appearing structure with high signal intensity on T2-weighted image sequencing. It appears to be contiguous with the hypertrophied right facet joint, which appears to also have high signal intensity. The mass significantly narrows the right lateral recess. The high signal intensity suggests that this is a fluid-filled mass. In addition, the facet joints are degenerative and there is a very mild degree of anterolisthesis on the sagittal image. These findings make a lumbar synovial cyst the most likely diagnosis. Most lumbar juxtafacet cysts are observed at the L4-5 level, extradurally and adjacent to the degenerative facet joint. They may contain synovial fluid and/or extruded synovium. Presentation is indistinguishable from that of a herniated disk. The etiology of spinal cysts remains unclear, but there appears to be a strong association between their formation and worsening spinal instability. They occasionally regress spontaneously and may respond to aspiration and injection of corticosteroids, though there is a high recurrence rate with nonsurgical management. Synovial cysts resistant to nonsurgical management should be treated surgically. If the patient's symptoms can be attributable to radicular findings, a microsurgical decompression that limits further destabilization should suffice. However, if there is significant low back pain attributable to spinal instability, decompression and fusion remains an appropriate option. Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972. Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Question 100
High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
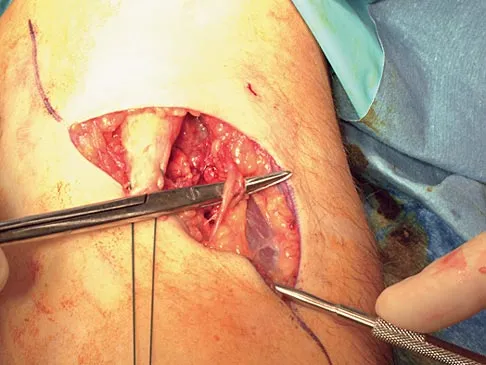
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
