Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of

Explanation
With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
Question 2
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?


Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 3
A 19-year-old woman has had a painful prominence on the lateral border of her fifth metatarsal head since she was a young girl. Nonsurgical management, including the use of a wide toe box shoe, has failed to provide relief. Examination reveals a callus over the lateral prominence and on the plantar portion as well. A clinical photograph and a radiograph are shown in Figures 34a and 34b. Treatment should consist of


Explanation
The type of deformity described is a type 2 bunionette. There is often a congenital component to this deformity. The bowing of the fifth shaft differentiates a large intermetatarsal angle from a type 3 deformity. A distal chevron osteotomy corrects 1 degree in the intermetatarsal angle for every 1-mm shift. Because of limitations in the width of the fifth metatarsal neck, the allowable shift is generally 3 to 4 mm. This shift will not compensate for the large intermetatarsal angle. The floating osteotomy has a high rate of delayed union/nonunion and a low satisfaction rate. Metatarsal head excision has a high complication rate, including severe shortening, transfer metatarsalgia, stiffness, and pain. A more proximal procedure is necessary to correct the large intermetatarsal angle and the lateral bowing. The osteotomy of choice is a diaphyseal shaft osteotomy. Because this patient has a plantar callosity and a lateral callosity, the osteotomy is angled superiorly to elevate the fifth shaft with the shift, eliminating overload of the plantar metatarsal head and subsequent callus formation. Shereff MJ, Yang QM, Kummer FJ, Frey CC, Greenidge N: Vascular anatomy of the fifth metatarsal. Foot Ankle 1991;11:350-353. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 4
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of



Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 5
High Yield
For halo traction, what is the preferred site for anterior pin placement?
Detailed Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 6
High Yield
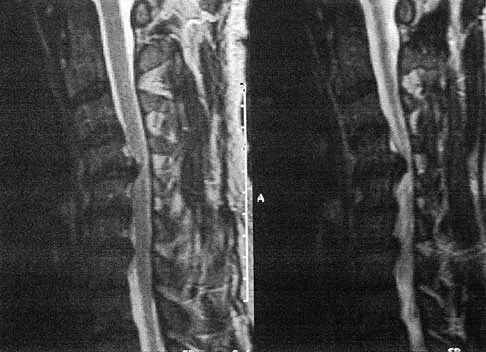
A 50-year-old man reports the onset of back pain and incapacitating pain radiating down his left leg posterolaterally and into the first dorsal web space of his foot 1 day after doing some yard work. He denies any history of trauma. Examination reveals ipsilateral extensor hallucis longus weakness. MRI scans are shown in Figures 19a through 19c. What nerve root is affected?



Detailed Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 root on the left side. In addition, the L5 root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot, and L4 affects the medial calf. An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, pp 98-100.
Question 7
High Yield
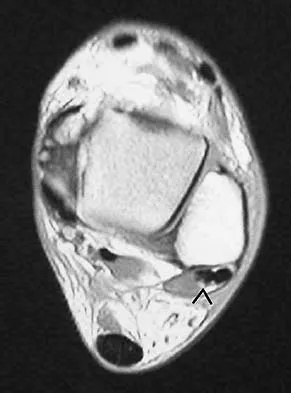
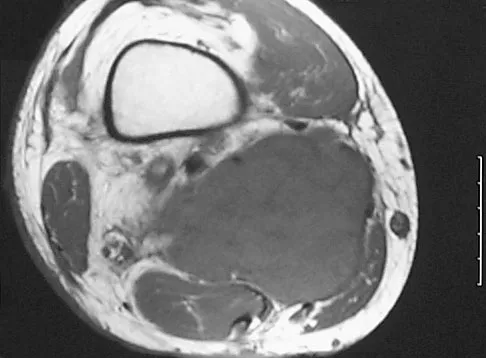
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel's sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of


Detailed Explanation
Neurilemoma is a benign tumor of nerve sheath origin, and peak incidence is in the third through sixth decades. The tumor is well encapsulated on the surface of a peripheral nerve. MRI findings may be significant for a "string sign." A positive Tinel's sign in the distribution of the nerve affected may be present. Grossly, the lesion is well encapsulated in a nerve sheath. Microscopically, there are structures referred to as Antoni A (a pattern of spindle cells arranged in intersecting bundles) and Antoni B (areas with less cellularity with loosely arranged cells). These lesions are benign, and treatment should consist of marginal excision. Nerve function may be preserved by careful dissection, excising the lesion parallel to the nerve fascicles so the lesion may be extruded. Recurrence is rare. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Question 8
High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?

Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 9
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 10
High Yield
An eversion mechanism of injury is associated with which of the following ankle conditions?
Detailed Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 11
A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?

Explanation
Proprionobacter acnes has been a leading cause of indolent shoulder infections. During shoulder arthroscopy, the arthroscopic fluid may actually dilute the shoulder preparation and lead to a higher rate of infection during subsequent mini-open rotator cuff repair surgery. The remaining bacteria listed are rarely associated with shoulder infections after arthroscopy. Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 12
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Scientific References
-
:
Question 13
An otherwise healthy 65-year-old man reports thigh pain of insidious onset. He states that the pain is increased with weight bearing and also occurs at night. He denies any history of cancer. Radiographs are shown in Figures 22a and 22b. A bone scan shows an isolated lesion. CT scans of the chest and abdominal are negative for any other lesions. Initial management should consist of


Explanation
The patient has a solitary lesion that is at high risk for fracture. While metastatic lesions are most common in this age group, a stabilization procedure is contraindicated until results of a biopsy confirm the presence of a metastasis. Because of the lytic lesion and the associated calcification shown on the radiograph, the most likely diagnosis is a chondrosarcoma. Therefore, any type of stabilization procedure with a rod or plate would compromise a wide surgical excision to remove the entire proximal femur. Radiation therapy and chemotherapy are also contraindicated until biopsy results are obtained. Because of these factors, obtaining a frozen section biopsy specimen is considered the next most appropriate step in management. If a metastatic lesion is confirmed on the frozen section, a stabilization procedure could then be performed under the same anesthetic. Therefore, it is important to have a pathologist available at the time of a biopsy. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 14
High Yield
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Question 15
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
Both myeloma and lymphoma are more responsive to radiation therapy. The other types of tumors are relatively more resistant to radiation. Doses of 25 to 50 Gy (2,500 to 5,000 cGy) are usually sufficient for myeloma and lymphoma, while carcinomas frequently require a higher dosage. Large cell lymphoma of bone is usually of B-cell origin and is treated with chemotherapy and radiation therapy. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Question 16
High Yield
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
SIS is a devastating but preventable complication of head injury. It occurs when return to activities is allowed prior to complete resolution of the symptoms of the first head injury. A second, sometimes trivial, head injury can lead to a devastating series of events that can result in sudden death. The symptoms tend to progress rapidly and often involve the brain stem. The prognosis is poor. Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44. Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Question 17
High Yield
What structure provides the major blood supply to the humeral head?
Explanation
The ascending branch of the anterior circumflex humeral artery provides the major blood supply to the humeral head. The posterior circumflex humeral artery supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 18
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 19
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?

Explanation
The CT scan reveals an avulsion of the dorsal beak of the anterior process of the calcaneus. This common fracture is an avulsion of the origin of the bifurcate ligament, which runs from the anterior calcaneal process to both the cuboid and the lateral aspect of the navicular. An inversion mechanism is common, and the fracture is often missed in evaluation for a suspected ankle sprain. MRI may be useful in the diagnosis of these occult injuries, and suspicion should be present when tenderness exists over the superior portion of the anterior process of the calcaneus.
Question 20
High Yield
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 21
High Yield
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 22
High Yield
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?



Explanation
The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair. Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28. Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528. Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Question 23
A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?


Explanation
The examination findings do not correlate with an acute injury (full range of cervical motion and the absence of pain). Radiographically, the fracture appears old based on the smooth contour of the fracture fragments and the absence of soft-tissue swelling. Flexion-extension radiographs can be obtained to determine potential instability; if present, stabilization and fusion should be considered. Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Question 24
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?

Explanation
The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used after surgery. Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
Question 25
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?


Explanation
The history, examination, and radiographs are pathognomonic for Little League shoulder, a stress syndrome of the proximal humeral physis caused by overuse. Complete fracture rarely occurs, and recovery usually occurs with rest. Night pain is always a serious concern and further work-up is needed if the patient does not respond to activity modification. Occult instability is not a real concern in this patient, although it should be included in the differential diagnosis. Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Question 26
A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
Explanation
Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel's sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient's pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms. Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161. An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 27
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Explanation
The terminal branch of the posterior interosseous nerve is contained in the fourth dorsal compartment. The contents of the various dorsal wrist compartments are as follows: 1st Compartment: Abductor pollicis longus, extensor pollis brevis; 2nd Compartment: Extensor carpi radialis brevis, extensor carpi radialis longus; 3rd Compartment: Extensor pollicis longus; 4th Compartment: Extensor digitorum comminus, extensor indicus proprius, posterior interosseous nerve; 5th Compartment: Extensor digiti minimi; 6th Compartment: Extensor carpi ulnaris. The extensor indicis proprius is also contained in the fourth dorsal compartment. The extensor digiti minimi is located in the fifth dorsal compartment. The extensor carpi radialis brevis is located in the second dorsal compartment. The extensor pollicis longus is located in the third dorsal compartment, and the abductor pollicis longus is located in the first dorsal compartment. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 150-151.
Question 28
High Yield
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?


Explanation
The lateral radiograph reveals a triceps avulsion with a small portion of bone. Triceps weakness and insufficiency can be a symptomatic problem after total elbow arthroplasty and is probably underreported. Ulnar nerve neuritis, aseptic loosening, instability, and infection are all complications of total elbow arthroplasty but would not account for the radiographic findings. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Question 29
High Yield
A healthy 52-year-old woman is seeking professional advice about management of osteoporosis. She has no risk factors for osteoporosis. What is the best recommendation for bone health for this patient?
Explanation
Women older than age 50 years should receive daily supplementation with calcium and vitamin D to help preserve bone density. Bone mineral density testing is recommended for women age 65 years or older and postmenopausal women with at least one risk factor for osteoporotic fractures: prior fragility fracture, low estrogen levels, premature menopause, long-term secondary amenorrhea, glucocorticoid therapy, maternal history of hip fracture, or low body mass index. Hormone therapy is not approved for the treatment of osteoporosis. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 30
High Yield
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?

Explanation
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus. Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque. Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Question 31
High Yield
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of

Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 32
High Yield
A 54-year-old woman sustained an elbow injury 3 months ago that was treated with open reduction and internal fixation. She now reports pain and limited elbow motion. Radiographs are shown in Figures 10a and 10b. Treatment should now consist of


Explanation
Radiographs reveal malunion of a Monteggia fracture-dislocation. Dislocation of the posterior radial head is caused by the malunited ulnar fracture. The deformity includes shortening with an apex posterior angulation. In the acute setting, open reduction of the radial head rarely is necessary; however, in chronic dislocations, open reduction is required. Without ulnar osteotomy, recurrent radial head dislocation is likely.
Question 33
High Yield
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Detailed Explanation
The placement of ACL graft with respect to its femoral and tibial attachments has a significant effect on its function. Evidence has shown that if the graft is placed in the over-the-top position, the graft will become lax in flexion and more taut with extension. Conversely, if the graft is placed too anterior on the femoral side, it will tighten in flexion and become lax in extension. Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342. Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Question 34
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 35
High Yield
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?

Explanation
The authors of several studies conducted in Europe have reported promising results in the short- and medium-term with use of a reversed or inverted shoulder implant. The most recent investigation, a multicenter study in Europe in which 77 patients (80 shoulders) with glenohumeral osteoarthritis and a massive rupture of the rotator cuff were treated with the Delta III prosthesis, described an improvement in the mean constant score of 42 points, an increase of 65 degrees in forward elevation, and minimal or no pain in 96% of the patients. Hemiarthroplasty, the "nonconstrained" option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform. Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 36
High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of


Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 37
A 35-year-old male laborer with isolated posttraumatic degenerative arthritis of the right hip undergoes the procedure shown in Figure 8. What is the most appropriate position of the right lower extremity?

Explanation
The primary indication for hip arthrodesis is isolated unilateral hip disease in a young, active patient. Avoiding abductor damage and preserving proximal femoral anatomy are imperative to allow conversion to a future total hip arthroplasty. Optimal positioning is 30 degrees of flexion to allow swing-through. Neutral abduction and adduction and slight external rotation allow the most efficient gait while allowing sufficient support in stance. A small degree of adduction is acceptable for a successful hip arthrodesis. Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 38
High Yield
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?

Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 39
High Yield
Which of the following body positions is associated with the highest intradiskal pressure?
Explanation
Intradiskal pressure is lowest when the patient is in the supine position. Sitting is associated with higher intradiskal pressures than standing. Flexion also increases intradiskal pressure. The combination of flexion and sitting produces the highest intradiskal pressure. Nachemson and Morris found that intradiskal pressure increases as position changes from lying supine, lying prone, standing, leaning forward, sitting, and sitting leaning forward. Twisting or straining in positions of relatively high intradiskal pressure may predispose patients to herniation of the intervertebral disk. Patients with a herniated disk may also notice their pain worsens with activities that increase the disk pressure, including the positions mentioned, or activities that increase intra-abdominal pressure (coughing, sneezing, straining). Nachemson A, Morris JM: In vivo measurements of intradiscal pressure. J Bone Joint Surg Am 1964;46:1077-1092.
Question 40
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
This child has the potential to walk and therefore should have all the contracted structures in the feet released as necessary to place the feet in a plantigrade position for fitting of ankle-foot orthoses. Physical therapy, manipulation, and casting may provide some benefit in a newborn with flexible feet but are not effective in an older infant with rigid clubfeet. Botulinum injections and tendon transfers are of no use because there are no muscles functioning below the knee. Tendon releases are more effective than tendon transfers in children with myelomeningocele. Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Question 41
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 42
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?

Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 43
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include

Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 44
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?




Explanation
The patient sustained a growth plate fracture of the distal radius and ulna. Although treated with closed reduction and casting, the follow-up radiographs demonstrate shortening of the radius in comparison to the ulna, and the MRI scan confirms thinning of the distal radius growth plate and bony bars consistent with a growth arrest. At this time, the discrepancy in length is too minor to consider lengthening of the radius; in addition, excision of a physeal bar with minimal growth potential is not likely to restore the gross discrepancy. Ulnar styloid fractures are rarely symptomatic and do not require treatment in the asymptomatic patient. Closure of the distal ulna growth plate will prevent further discrepancy between the radius and ulna. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Question 45
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 46
High Yield
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
Local control of osteosarcoma consists of wide resection and reconstruction. Radiation therapy is not recommended except in unresectable lesions or for palliation. Curettage and bone grafting result in intralesional resection with an unacceptable high rate of local recurrence. Chemotherapy alone is not adequate for local control. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Question 47
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35 degrees. Neurologic examination is normal. Management should consist of


Explanation
Because hydrosyringomyelia, with or without an Arnold-Chiari malformation, is now being recognized as the etiology of many infantile and juvenile idiopathic scolioses, management should consist of a neurosurgical consultation. Observation with follow-up radiographs is not an option in curves of this magnitude. A technitium Tc 99m bone scan is unnecessary because the etiology of the curve has been identified. Although spinal fusion may be needed in the future, it should not be undertaken before the neurosurgical problem has been addressed. Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767. Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 48
High Yield
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Detailed Explanation
Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 49
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include

Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 50
High Yield
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal


Detailed Explanation
The patient has a perilunate dislocation. A volar dislocation of the lunate is often associated with median nerve dysfunction. This injury to the wrist is often overlooked because of its benign clinical appearance and the presence of other injuries, as it is caused by high-energy mechanisms. Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Question 51
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?

Explanation
The risk of Salmonella osteomyelitis is much greater in patients with sickle cell disease than the general population. The exact reason for this increased risk is still unclear, but it appears to be associated with an increased incidence of gastrointestinal microinfarcts and abscesses. Both Staphylococcus aureus and Salmonella have been mentioned as the most prevalent causative organisms. Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227. Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413. Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Question 52
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of

Explanation
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery. Blazina ME, et al: Jumper's knee. Orthop Clin North Am 1973;4:665. Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper's knee. Am J Sports Med 1984;12:375-380. Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Question 53
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include


Explanation
Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Question 54
High Yield
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of

Explanation
Asymptomatic spondylolysis in a child or adolescent should be observed for the possible development of spondylolisthesis, but no other active intervention is needed. The initial treatment of choice for symptomatic spondylolysis includes rest and activity modifications, nonsteroidal anti-inflammatory drugs, physical therapy, bracing, and casting. Immobilization with a TLSO or pantaloon spica cast may permit healing of an acute pars fracture. Rarely, surgical treatment may be necessary. Surgical options include posterolateral L5-S1 fusion or direct repair of the pars defect. Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Question 55
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
Osteopenia, decreased bone mass without fracture risk as defined by the WHO criteria for diagnosis of osteoporosis, is when a woman's T-score is within -1 to -2.5 SD. The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
Question 56
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 57
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?


Explanation
The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern. Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
Question 58
High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season. Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Question 59
High Yield
What structure (arrow) is shown in Figure 24?

Detailed Explanation
The structure illustrated is the sympathetic chain viewed from an anterolateral view of the lower lumbar spine. It descends along the anterolateral aspect of the spine into the pelvis closely adherent to the vertebral column. The spinal nerves, including L5, can be seen exiting from the foramen. The ureters descend from the kidneys and cross anterior to the iliac vessels to the bladder. Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Question 60
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure. Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 61
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?

Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 62
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?

Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding. Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432. Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23. Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Question 63
High Yield
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
Continuous fluoroscopy and cine radiography expose the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Question 64
High Yield
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?

Explanation
The saphenous nerve follows the saphenous vein, giving off the infrapatellar branch that crosses the knee anteriorly to supply the peripatellar skin. A longitudinal incision can interrupt the nerve, leaving the terminal distribution without sensation.
Question 65
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes' disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?

Explanation
Several authors have reported good success in relieving pain with shelf acetabuloplasty. This patient's Perthes' disease is in the healed phase; therefore, proximal femoral varus and Salter innominate osteotomies aimed at improving containment are not indicated. The medial one half of the patient's femoral head is markedly deformed, and rotating it into a weight-bearing position with proximal femoral valgus osteotomy is unlikely to relieve pain. Hip arthrodesis can always be performed as a salvage procedure if the shelf acetabuloplasty fails. Daly K, Bruce C, Catterall A: Lateral shelf acetabuloplasty in Perthes' disease: A review of the end of growth. J Bone Joint Surg Br 1999;81:380-384.
Question 66
A 60-year-old man has pain at the tip of the index finger. A radiograph and biopsy specimen are shown in Figures 40a and 40b. Management should consist of


Explanation
The radiograph and histology findings are most consistent with squamous cell carcinoma. This tumor is best treated with wide surgical resection margins alone in the absence of metastasis; in this patient, management should consist of amputation through the distal interphalangeal joint. The other treatments are not indicated. Soltani K, Krunic A: Non melanoma skin neoplasms, in Vokes E, Golomb H (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, pp 646-647.
Question 67
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?


Explanation
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time. Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Question 68
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 69
High Yield
Stability at the atlanto-occipital joint is provided mainly by
Detailed Explanation
The atlanto-occipital joint is inherently unstable and would easily dislocate without the supporting ligaments. The apical ligament attaches to the basion and tip of the dens but does not provide adequate stability to the joint. Werne demonstrated that dividing the tectorial membrane and the alar ligaments resulted in gross joint instability. The anterior longitudinal ligament turns into the anterior atlanto-occipital membrane. This is called a membrane rather than a ligament because it is not strong enough to support these two structures. Werne S: Studies in spontaneous atlas dislocation. Acta Orthopaedica Scandinavica 1977;23(supplement).
Question 70
High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 71
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?

Explanation
Cheilectomy has been shown to provide satisfactory pain relief and improved function in long-term studies. It is important to select patients appropriately when choosing a cheilectomy versus an arthrodesis. Pain at the midrange of motion and loss of more than 50% of the metatarsal head cartilage are predictors of a poor outcome following cheilectomy, and these patients should receive an arthrodesis. Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Question 72
A 57-year-old man with type I diabetes mellitus has had a tender, erythematous right sternoclavicular joint for the past 2 weeks. Radiographs reveal mild osteolysis without arthritic changes, within normal limits. Management should consist of

Explanation
Sternoclavicular joint sepsis is a rare condition that is most often restricted to patients who are immunocompromised, diabetic, or IV drug abusers. Examination commonly reveals a tender, painful, and possibly swollen sternoclavicular joint. If suspicion remains high following a thorough history, physical examination, radiographs, and routine blood tests, joint aspiration should be performed prior to incision and drainage or administration of antibiotics. Bremner RA: Monarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 73
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?


Explanation
Based on her symptoms and prior shoe wear modifications, the treatment of choice is surgical correction of the hallux valgus with a chevron osteotomy. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Steroid injection would only risk infection, as well as joint and capsule damage. Extra-depth shoes are an option; however, the patient is interested in surgical options. Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584. Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Question 74
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?

Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 75
High Yield
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?

Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 76
High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 77
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of


Explanation
The patient has a stress fracture of the olecranon that occurs with repetitive throwing motions. If the fracture is not displaced, the initial treatment of choice is rest and rehabilitation to maintain elbow motion, followed by aggressive strengthening at 6 to 8 weeks. A light throwing program generally can begin at 8 to 12 weeks. Complete recovery may require 3 to 6 months. If the fracture is displaced or if nonsurgical management fails, surgery is indicated for internal fixation of the stress fracture. Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Question 78
High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

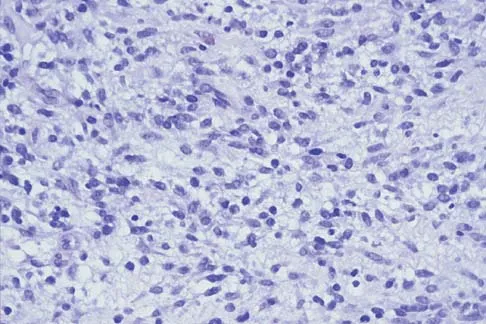
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 79
High Yield
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?



Detailed Explanation
The patient has degeneration of an adjacent segment with resultant kyphosis and stenosis. Because he is healthy, has responded well to previous surgery, and has a potentially correctable lesion, he is not a good candidate for an end-stage failed back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient's relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
Question 80
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 81
A 43-year-old man has had right groin pain for the past 3 months. A radiograph, CT scan, and biopsy specimen are shown in Figures 18a through 18c. What is the most likely diagnosis?



Explanation
The radiographic appearance of the lesion is lytic with calcifications in the supra-acetabular region. The CT scan shows bone destruction and periosteal reaction, which rules out an enchondroma. The histologic appearance is that of cellular cartilage, with a high cytoplasmic:nuclear ratio and basophilic appearance to the cytoplasm; these findings rule out chordoma and metastatic renal cell carcinoma. In addition, chordomas are most frequently found in the sacrum and base of the skull. Because there is no high-grade spindle cell component to suggest dedifferentiation, the most likely diagnosis is chondrosarcoma. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 82
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 83
High Yield
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of

Detailed Explanation
Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability. Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Question 84
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Question 85
High Yield
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?

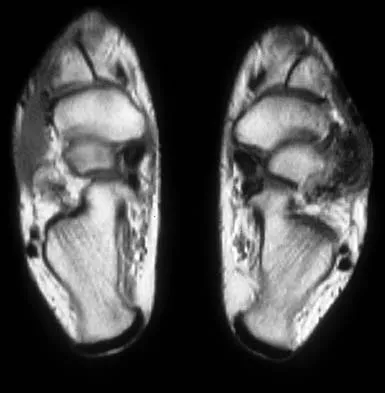
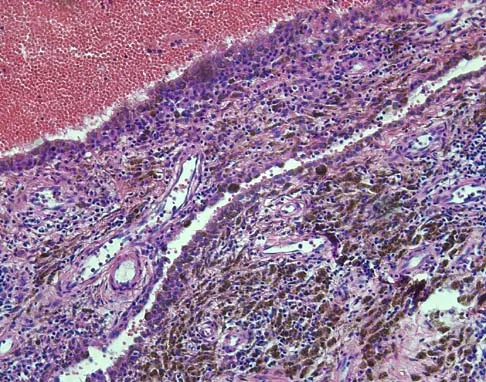
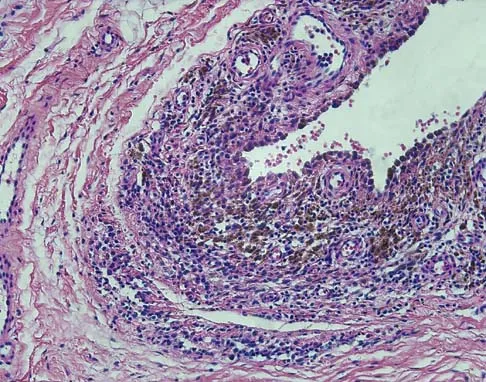
Explanation
Synovial sarcoma should always be considered in the differential diagnosis of a foot mass; however, the histopathology shows a typical example of PVNS, with hemosiderin, giant cells, and synovium. Synovial chondromatosis would have metaplastic cartilage in the synovium. The radiograph shows subtle erosion of the lateral cortex of the cuboid, and the MRI scan shows a soft-tissue mass. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830. Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Question 86
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?

Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 87
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?


Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 88
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 89
High Yield
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of

Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 90
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90 degrees of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90 degrees of flexion. Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Question 91
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?

Explanation
Rheumatoid arthritis commonly affects the metatarsophalangeal joints, which become destabilized with time resulting in hallux valgus and dislocated lesser claw toes. The result is metatarsalgia as the dislocated claw toes "pull" the fat pad distally. Severe hallux valgus reduces first ray load, which compounds the metatarsalgia because the load is transferred to the lesser metatarsal heads. First metatarsophalangeal arthrodesis restores weight bearing medially and corrects the painful bunion. Metatarsal head resection slackens the toe tendons to allow correction of the claw toes by whatever means necessary and decreases plantar load over the forefoot. Rheumatoid arthritis in the first metatarsophalangeal joint will continue to progress if osteotomies or a Lapidus procedure are performed. Keller resection arthroplasty increases transfer metatarsalgia and reduces push-off power during gait. Flexor-to-extensor tendon transfer of the lesser toes does not address the metatarsalgia and does not correct the dislocation of the metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Question 92
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?

Explanation
Fractures of the distal radius increase the relative risk of a subsequent hip fracture significantly more in men than in women. A previous spinal fracture has an equally important impact on the risk of a subsequent hip fracture in both genders.
Question 93
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 94
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
Evidence implicates an association, albeit unexplained, between Clostridium septicum infection and malignancy, particularly hematologic or intestinal malignancy. The malignancy is often at an advanced stage, compromising survival of the patients. A bowel portal of entry is postulated for most patients. In the absence of an external source in the patient with clostridial myonecrosis or sepsis, the cecum or distal ileum should be considered a likely site of infection. Increased awareness of this association between Clostridium septicum and malignancy, and aggressive surgical treatment, may result in improvement in the present 50% to 70% mortality rate. Other organisms associated with malignancy include group Clostridium streptococci that are occasionally associated with upper gastrointestinal malignancies. Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Question 95
High Yield
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 96
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 97
The vascularity of the digital flexor tendons is significantly richer in what cross-sectional region?
Explanation
The vascularity of the dorsal portion of the digital flexor tendons is considerably richer than the volar portion. The other regions are not preferentially more vascular. Hunter JM, Scheider LH, Makin EJ (eds): Tendon Surgery in the Hand. St Louis, MO, Mosby, 1987, pp 91-99.
Question 98
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include


Explanation
The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 99
High Yield
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of


Explanation
A favorable prognosis can be expected in up to 70% of children with Legg-Calve-Perthes disease who are younger than age 6 years. Containment treatment has not been shown to alter the outcome in this age group. The goals of treatment in this patient are to reduce pain (synovitis), restore motion, and improve function. Symptomatic treatment modalities include bed rest, traction, crutches, activity modification, and nonsteroidal anti-inflammatory drugs. Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Question 100
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
