Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 2
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 3
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?

Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 4
High Yield
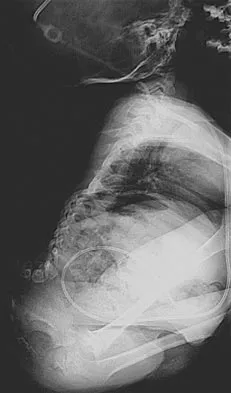
A 68-year-old woman stepped on a needle while walking barefoot 10 days ago. She is not certain but thinks it is imbedded in her foot, and she notes local tenderness at the puncture site and drainage. Her primary care physician has been treating her with oral antibiotics. A plain radiograph is shown in Figure 38. What is the best course of action?

Detailed Explanation
Based on the radiographic findings, the patient has a metallic foreign body in her foot that is consistent with a needle. She has local infection secondary to the continued presence of the foreign body. CT is not necessary to localize the foreign body as it is adequately visualized on the plain radiographs. The infection cannot be adequately treated until the foreign body is removed. Attempted removal of foreign bodies without proper anesthesia and fluoroscopy frequently results in frustration because of the inability to localize the foreign body. Removal in a surgical suite with proper anesthesia and fluoroscopy is the preferred option. Once the foreign body is removed, the local infection will resolve rapidly. Combs AH, Kernek CB, Heck DA: Orthopedic grand rounds: Retained wooden foreign body in the foot detected by computed tomography. Orthopedics 1986;9:1434-1435.
Question 5
High Yield
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?





Explanation
The patient has a fracture-dislocation of the radiocarpal joint. Attached to the large radial styloid fragment are the extrinsic wrist ligaments to the carpus. This injury should be treated with open reduction and internal fixation of the styloid fracture. Radiolunate fusion or extrinsic ligament repair is suggested when the extrinsic ligaments are ruptured, resulting in ulnar translocation of the carpus. Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Question 6
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Piriformis syndrome is best characterized by localized posterior hip pain and radicular symptoms in the sciatic distribution because of compression of the piriformis muscle on the sciatic nerve. Weakness in hip extension is not a characteristic finding, nor is pain with hip abduction or flexion. Hypesthesia of the lateral thigh would be more characteristic of a lesion of the lateral femoral cutaneous nerve. Radiating medial thigh pain would suggest hip joint pathology or upper lumbar nerve root irritation. Weakness in internal rotation is not a characteristic feature, and hypesthesia of the perineum would suggest possible involvement of the pudendal nerve. Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002, pp 114-139.
Question 7
High Yield
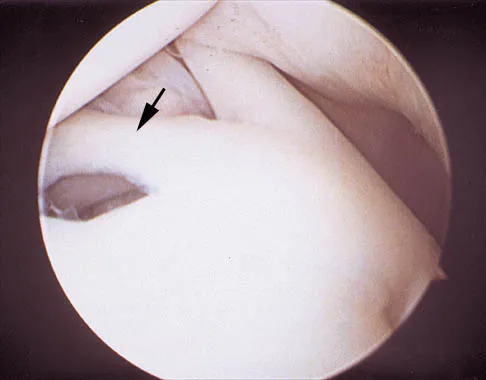
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 8
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 9
A 13-year-old boy has a painless "knot" over his left hip. History reveals that he injured his left hip playing soccer 4 months ago. A radiograph and MRI scan obtained at the time of injury are shown in Figures 7a and 7b. He is very active and is currently asymptomatic. A current radiograph is shown in Figure 7c. What is the next most appropriate step in management?



Explanation
The diagnosis is myositis ossificans resulting from an injury. The initial radiograph reveals a small amount of mineralization in the soft tissues overlying the left hip. The MRI scan shows signal abnormality of the entire gluteus minimus muscle with a mineralized mass in the center. The current radiograph shows a lesion within the abductor musculature with mature ossification peripherally. The imaging studies are diagnostic and the patient is asymptomatic; therefore, the management of choice is observation with no further evaluation or treatment indicated. Miller AE, Davis BA, Beckley OA: Bilateral and recurrent myositis ossificans in an athlete: A case report and review of treatment options. Arch Phys Med Rehabil 2006;87:286-290.
Question 10
High Yield
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?

Explanation
Although arthroscopic debridement with or without subacromial decompression is a reasonable response, the patient has positive impingement signs. Several recent studies regarding the surgical treatment of partial rotator cuff tears have demonstrated good to excellent results after repair of tears involving more than 50% of the tendon thickness. This was shown specifically for bursal-sided tears and joint-side tears. Biceps tenotomy is not indicated in a young patient. Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears. Am J Sports Med 2005;33:1405-1417.
Question 11
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of



Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 12
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
In symptomatic partial-thickness rotator cuff tears, a painful arc with active range of motion is common, impingement signs are usually positive, and the lift-off test is normal. Active and passive range of motion measurements are often equal, although active range of motion can be painful. External rotation lag signs are often seen with larger full-thickness tears. Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 13
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 14
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
In a patient with hemophilia, factor replacement followed by assessment of compartment pressures is essential. If the patient has inhibitors, the problem is more difficult. Porcine factor has been helpful in patients with inhibitory antibodies. Recent evidence points to using activated factor VII and bypassing the intrinsic pathway. Desmopressin is an adjunct to therapy but is not as effective as factor VII. Dumontier C, Sautet A, Man M, Bennani M, Apoil A: Entrapment and compartment syndromes of the upper limb in haemophilia. J Hand Surg Br 1994;19:427-429. Carr ME Jr, Loughran TP, Cardea JA, Smith WK, Kuhn JG, Dottore MV: Successful use of recombinant factor VIIa for hemostasis during total knee replacement in a severe hemophiliac with high-titer factor VIII inhibitor. Int J Hematol 2002;75:95-99.
Question 15
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of


Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 16
High Yield
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?



Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 17
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

Explanation
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Question 18
High Yield
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?



Explanation
Nonsurgical management of a symptomatic accessory navicular should be attempted prior to surgery. Good relief is often obtained with a semi-rigid orthosis with a medial arch support. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Question 19
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?


Explanation
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful. Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Question 20
High Yield
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of

Explanation
The patient has a moderately displaced distal diaphyseal fracture of the fifth metatarsal, and the most appropriate treatment is brief immobilization and symptomatic management. Attempts at closed reduction are unlikely to appreciably alter the position of the fracture. Surgical techniques for either reduction of the fracture or fixation have not been shown to result in improved functional outcomes. O'Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: "Dancer's Fracture." Am J Sports Med 1996;24:240-243. DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Question 21
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 22
High Yield
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Detailed Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 23
High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 24
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 25
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?


Explanation
The figures show a longitudinal split within the peroneus brevis tendon as it courses posterior to the fibula. The peroneus longus tendon has been driven between the medial and lateral components of the peroneus brevis tendon. Peroneal split syndrome is a cause of lateral ankle pain but may be less asymptomatic in the elderly. It may be associated with tendon subluxation following a tear of the superior peroneal retinaculum.
Question 26
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Urbaniak and Harvey reported donor site morbidity following free vascularized fibular graft in 198 consecutive patients. At a 5-year follow-up, they reported overall complications in 24% of the patients. The most common complication was a sensory deficit (11.8%), followed by motor weakness (2.7%), flexor hallucis longus contracture (2%), and deep venous thrombosis (less than 1%).
Question 27
High Yield
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 28
High Yield
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Detailed Explanation
Results have been satisfactory in many patients; however, at long-term follow-up, examination of the affected shoulder often shows some decrease in range of motion compared with the contralateral side. Although range of motion often improves over time, it does not return to normal in 60% of patients. Pain improves but is often increased compared with the contralateral side. Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Question 29
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?

Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 30
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of


Explanation
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Question 31
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced

Explanation
The literature supports similar clinical outcomes after surgical and nonsurgical methods. The chief difference lies in the complications between the groups. Surgical patients experience more wound problems but a significantly lower rerupture rate. Although suturing the tendon allows earlier mobility, the tendon healing time is unchanged. Nonsurgical methods are less expensive to provide. Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Question 32
High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Detailed Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 33
High Yield
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 34
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T1- and T2-weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?






Explanation
The imaging studies show a permeative lytic destructive lesion in the proximal radius with "hair-on-end" periosteal reaction and a large soft-tissue mass most consistent with Ewing's sarcoma. The pathology reveals monotonous sheets of "round blue" cells. This limits the differential diagnosis to primary lymphoma of bone versus Ewing's sarcoma. These are best differentiated by immunohistochemistry, cytogenetics, and flow cytometry. Lymphoma of bone is typically CD34 positive and CD99 negative; whereas, the reverse is true of Ewing's sarcoma, CD34 negative and CD99 positive. The most common cytogenetic translocation with Ewing's sarcoma is 11; 22; 21; 22 and 7; 22 translocations have also been reported in Ewing's sarcomas. The X; 18 translocation is most commonly associated with synovial cell sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Flow cytometry is used to characterize the cell types of lymphomas. Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21. Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing's sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Question 35
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of

Explanation
The patient has posttraumatic arthritis of the elbow; therefore, the treatment of choice is hardware removal and soft-tissue releases with splinting to avoid recurrence of contractures. The combination of pain and stiffness in an elbow that has sustained significant joint surface damage renders it unresponsive to simple soft-tissue releases and heterotopic bone excision. Joint distraction and interposition arthroplasty offer the possibility of maintaining motion and relieving pain as a later salvage procedure. Joint replacement should not be performed in young, active, strong individuals because the prosthesis will fail quickly and complications will develop. Synovectomy and radial head excision are not indicated. Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
Question 36
High Yield
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 37
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
Nondisplaced distal radial fractures have a higher rate of spontaneous rupture of the extensor pollicis longus tendon. The extensor mechanism is felt to impinge on the tendon following a nondisplaced fracture and causes either a mechanical attrition of the tendon or a local area of ischemia in the tendon. Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles' type of fracture. Hand 1982;14:41-47.
Question 38
High Yield
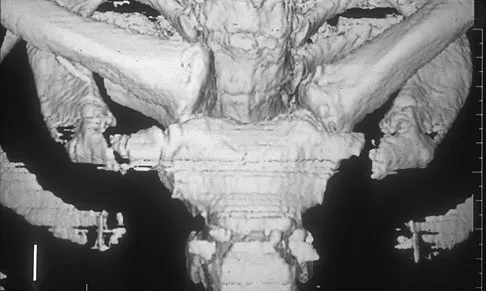
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?

Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 39
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?


Explanation
The overriding factor determining treatment in this case is the appearance of the surgical wound. Based on MacPhearson's work, this "C" wound is best managed with two-stage exchange. The functional outcome is markedly diminished following a knee arthrodesis compared to revision knee arthroplasty. Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22. Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 40
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 41
High Yield
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Explanation
Degenerative spondylolisthesis of the cervical spine is seen almost exclusively at C3-4 and C4-5; this is in contrast to degenerative changes, which are most commonly seen at C5-6 and C6-7. Tani T, Kawasaki M, Taniguchi S, et al: Functional importance of degenerative spondylolisthesis in cervical spondylotic myelopathy in the elderly. Spine 2003;28:1128-1134.
Question 42
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of


Explanation
The patient has symptoms of synovitis that are most likely the result of the release of particles from the tibial polyethylene. While observation may be warranted in a completely asymtomatic knee, some intervention is indicated for this patient as there is clear radiographic evidence of lysis in both the tibia and femur. The decision about the extent of the revision should be made at the time of surgery. A limited incision technique is not indicated. Grafting (or using graft substitute) the defect is the most appropriate approach for treating the osteolytic lesions. While a posterior stabilized prosthesis might be the solution, surgical findings might dictate otherwise.
Question 43
High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 44
High Yield
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?

Explanation
The radiograph shows three zones: an outer regenerated cortical layer, an interface zone consisting of viable trabecular bone and occasional particles of bone cement, and an inner layer of necrotic bone embedded in cement. No fibrous membrane is noted, and there is no direct contact of cement with native bone. Based on these findings, it is believed that the middle layer is the result of incorporation of the allograft with further remodeling. Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Question 45
High Yield
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of


Explanation
The patient has kyphosis in association with achondroplasia. The AP radiograph shows decreased interpedicular distance at the lower lumbar vertebrae, a feature considered to be a distinctive sign of achondroplasia. Most patients with achondroplasia have kyphosis, and this usually resolves spontaneously. When the fixed component is greater than 30 degrees, however, brace treatment is recommended. Spinal fusion is seldom required.
Question 46
High Yield
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of


Explanation
The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas. Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Question 47
High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 48
What is the most significant factor affecting long-term survival for a patient with bone sarcoma?

Explanation
The most significant impact on long-term survival is the presence or absence of identifiable metastatic disease on initial presentation. All of these factors have been shown to be predictive of long-term survival to varying degrees. Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 1980;153:106-120.
Question 49
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50 degrees only if the hip is allowed to externally rotate. Management should consist of


Explanation
The patient has radiographic signs of osteogenesis imperfecta, including osteopenia, mild acetabular protrusio, cortical thinning, and bowing associated with anterior stress fracturing. The treatment of choice is correction of the bow with osteotomies, followed by intramedullary fixation to prevent further deformity. Biphosphonates, such as pamidronate, may be useful in increasing bone density and preventing fractures. Large multicenter studies on biphosphonate efficacy are currently in progress. Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195. Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Question 50
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
Question 51
High Yield
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?
Explanation
Nonsurgical management of a symptomatic accessory navicular should be attempted prior to surgery. Good relief is often obtained with a semi-rigid orthosis with a medial arch support. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Question 52
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
Both myeloma and lymphoma are more responsive to radiation therapy. The other types of tumors are relatively more resistant to radiation. Doses of 25 to 50 Gy (2,500 to 5,000 cGy) are usually sufficient for myeloma and lymphoma, while carcinomas frequently require a higher dosage. Large cell lymphoma of bone is usually of B-cell origin and is treated with chemotherapy and radiation therapy. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Question 53
High Yield
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?

Explanation
The radiograph reveals a distal clavicle fracture. In children, a periosteal sleeve will remain attached to the intact coracoclavicular ligament, and as such, remodeling can be expected. Therefore, nonsurgical management with a sling is preferred. Surgical treatment is not necessary, and a shoulder spica cast offers no advantage over a simple sling.
Question 54
High Yield
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.
Question 55
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?

Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 56
High Yield
What is the main function of collagen found within articular cartilage?

Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 57
High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by


Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 58
High Yield
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 59
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel's sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly. Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Question 60
High Yield
Ganglion cysts about the wrist most commonly arise from what structure?
Detailed Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 61
High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of

Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 62
High Yield
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?

Detailed Explanation
The radiograph reveals a "bony mallet injury." As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate. Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Question 63
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include

Explanation
The patient has painful lateral and plantar keratoses with metatarsus quintus valgus deformity. This combination of problems is best addressed with an oblique mid-diaphyseal osteotomy that allows the distal metatarsal to be displaced medially and dorsally. Lateral eminence resection alone will not address the painful plantar keratosis. A distal chevron osteotomy has a more limited ability to address the plantar keratosis (if translated medially and slight dorsally). Proximal diaphyseal osteotomies of the fifth metatarsal are associated with an increased risk of delayed union or nonunion secondary to the relative hypovascularity in the proximal diaphysis. Excision of the fifth metatarsal head can result in a floppy fifth toe and transfer metatarsalgia. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 64
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?


Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 65
High Yield
Which of the following structures runs through the site indicated by the arrow in Figure 11?

Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 66
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 67
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include

Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 68
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 69
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?

Explanation
From proximal to distal, the brachial plexus is divided into roots, trunks, divisions, and cords before forming specific peripheral nerve branches. The structure marked Q is called the posterior cord because it lies posterior to the axially artery at the level of the cords. Its terminal branches are the upper subscapular (V), thoracodorsal (W), lower subscapular (X), axillary (F), and radial (G) nerves. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-24.
Question 70
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner's syndrome?

Explanation
The sympathetic chain approaches the lateral border of the longus coli muscle at C6 and is more vulnerable to injury at this level. Injury to the chain will cause Horner's syndrome, usually seen as unilateral ptosis.
Question 71
A 45-year-old man who underwent an open capsulolabral stabilization procedure 15 years ago now reports pain and has no external rotation on the affected side. Nonsurgical management has failed to provide relief. Examination reveals external rotation to -5 degrees compared with 50 degrees of external rotation on the contralateral side. Radiographs show a small inferior osteophyte and minimal posterior glenoid wear. Which of the following procedures will offer the best chance of restoring motion, decreasing pain, and preserving the native joint?

Explanation
Loss of external rotation following stabilization procedures can result in progressive degenerative joint disease. A tight anterior capsule results in posterior humeral translation and progressive posterior glenoid wear. Patients with early degenerative joint disease and pain can be treated with anterior release to restore more normal glenohumeral biomechanics. This procedure not only improves function but also decreases pain in most patients. Closed manipulation at 15 years after surgery is unlikely to be successful and carries the risk of complications. Acromioplasty, posterior release, and removal of osteophytes do not address the pathology. Arthroscopic releases are favored for intra-articular procedures that have addressed the pathology of instability. Open releases are recommended for nonanatomic extra-articular repairs that include subscapularis tightening procedures. MacDonald PB, Hawkins RJ, Fowler PJ, et al: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Question 72
High Yield
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Detailed Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 73
High Yield
What is the most common secondary malignancy arising in pagetic bone?

Explanation
The incidence of malignant transformation or the formation of a secondary malignancy in pagetic bone is estimated to be less than 1%. Osteosarcoma is the most common secondary malignancy, followed by fibrosarcoma and chondrosarcoma. Ewing's sarcoma arising in pagetic bone has not been reported. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Question 74
High Yield
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?

Explanation
The authors of several studies conducted in Europe have reported promising results in the short- and medium-term with use of a reversed or inverted shoulder implant. The most recent investigation, a multicenter study in Europe in which 77 patients (80 shoulders) with glenohumeral osteoarthritis and a massive rupture of the rotator cuff were treated with the Delta III prosthesis, described an improvement in the mean constant score of 42 points, an increase of 65 degrees in forward elevation, and minimal or no pain in 96% of the patients. Hemiarthroplasty, the "nonconstrained" option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform. Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 75
High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include

Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 76
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?


Explanation
The radiographs show ankylosing spondylitis with sclerosis of the sacroiliac joints and a "bamboo spine" in the lumbar region. HLA-B27 is positive in 80% to 90% of patients with ankylosing spondylitis and in about 8% of the general population. The findings do not represent diffuse idiopathic skeletal hyperostosis (DISH), which is a radiographic diagnosis in which there are three consecutive levels of nonmarginated osteophytes without disk degeneration. Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60. Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
Question 77
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?

Explanation
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Question 78
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 79
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
The patient has diskitis. Administration of IV antibiotics speeds resolution and minimizes recurrence. Bed rest and cast immobilization have been successfully used to treat this disorder but can be associated with prolonged recovery and frequent recurrence, even when oral antibiotics are administered. A perivertebral abscess seen in association with this condition usually resolves without surgery. Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop 1995;15:652-660.
Question 80
High Yield
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
Question 81
High Yield
Which of the following tumors is most likely to present with a pathologic fracture in a child?

Explanation
In nearly 50% of patients with a unicameral bone cyst, the lesion remains asymptomatic until a fracture occurs, usually as the result of relatively minor trauma. If the lesion expands, the bone is weakened and may cause pain. Fibrous cortical defects are usually an incidental finding and typically asymptomatic. Malignant bone tumors such as osteosarcoma and Ewing's sarcoma most commonly cause pain, and pathologic fracture occurs in less than 10% of patients. Giant cell tumors are uncommon in children and usually are painful. Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 82
High Yield
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 83
High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?

Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 84
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?


Explanation
The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age. Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259. Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Question 85
High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Detailed Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 86
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Vascular invasion, histologically similar to granulation tissue, has been noted between the columns in the zone of hypertrophy, leading to the theory of microtrauma as an etiology. SCFE is also associated with conditions that increase the height of the zone of hypertrophy, including the adolescent growth spurt and endocrinopathies. The perichondral ring has been shown to decrease in thickness with age. Normal undulations in the growth plate also decrease during this time, possibly further destabilizing the physis. Abnormal accumulations of proteoglycan have been reported. Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Question 87
High Yield
Which of the following anatomic structures is labeled 6 in Figure 27?
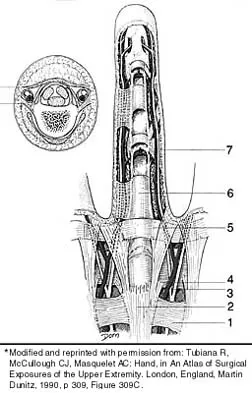
Explanation
The line labeled 6 points to the A2 pulley. This structure is the condensation of the digital flexor tendon sheath corresponding to the proximal aspect of the proximal phalanx. Grayson's ligament is volar to the digital nerve and artery. Cleland's ligament is dorsal to the digital nerve and artery. The sagittal band anchors the extensor tendons over the metacarpophalangeal joints. The triangular ligament connects the lateral bands just proximal to the terminal tendon inserting onto the base of the distal phalanx. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Question 88
A previously healthy 14-year-old boy now reports fatigue, and has a bilateral Trendelenburg gait, right hip pain, and bilateral knee and foot pain. Biopsy of a right sacral mass reveals intermediate grade osteosarcoma. There are no metastases. Laboratory studies reveal a serum calcium level of 7.7 mg/dL (normal 8.5 to 10.5), a phosphate level of 2.0 mg/dL (normal 2.7 to 4.5), a 1,25-dihydroxyvitamin D level of less than 10 pg/mL (normal 18 to 62), a parathyroid hormone level of 19 pg/mL (normal 10 to 60), and an alkaline phosphatase level of 428 U/L (normal 15 to 351). What is the most likely cause of the patient's symptoms?
Explanation
The laboratory findings are typical for rickets. Oncogenic rickets is a paraneoplastic syndrome that results from a substance secreted by the tumor that interferes with renal tubule reabsorption of phosphate. This substance previously had been called phosphatonin but recently has been identified as fibroblast growth factor 23. Nutritional rickets is rare in developed countries. Delayed onset familial hypophosphatemic rickets is possible, but the likelihood of having two rare diseases is unlikely. Osteosarcoma does not sequester calcium. Alkaline phosphatase levels can be elevated in osteosarcoma but does not cause muscle weakness. Tumor cachexia would occur only with advanced metastatic disease. A unilateral sacral mass would not cause a bilateral L5 neuropathy or the abnormal laboratory findings. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 29-2001. A 14-year-old with abnormal bones and a sacral mass. N Engl J Med 2001;345:903-908.
Question 89
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include

Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 90
High Yield
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
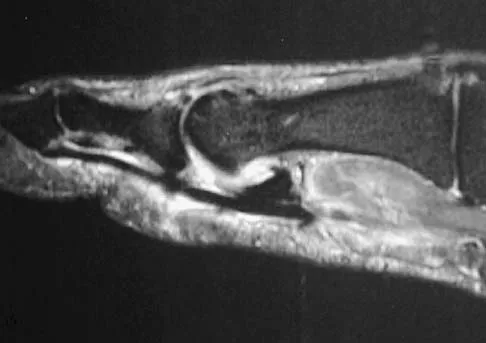
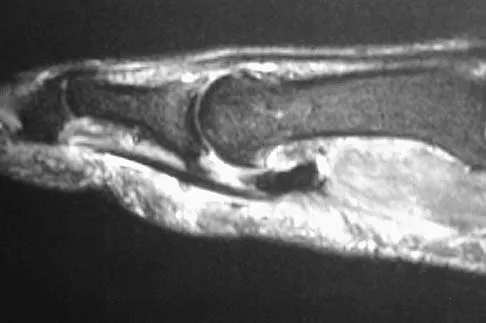
Explanation
The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 91
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?


Explanation
The radiographs show displacement of the prosthesis, and there has been large amounts of bone resected to insert the implant. Arthrodesis is indicated with interposition bone graft to stabilize the joint and restore length to the first ray.
Scientific References
-
:
Question 92
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?

Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 93
High Yield
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?


Detailed Explanation
The arrow is pointing to a cystic-appearing structure with high signal intensity on T2-weighted image sequencing. It appears to be contiguous with the hypertrophied right facet joint, which appears to also have high signal intensity. The mass significantly narrows the right lateral recess. The high signal intensity suggests that this is a fluid-filled mass. In addition, the facet joints are degenerative and there is a very mild degree of anterolisthesis on the sagittal image. These findings make a lumbar synovial cyst the most likely diagnosis. Most lumbar juxtafacet cysts are observed at the L4-5 level, extradurally and adjacent to the degenerative facet joint. They may contain synovial fluid and/or extruded synovium. Presentation is indistinguishable from that of a herniated disk. The etiology of spinal cysts remains unclear, but there appears to be a strong association between their formation and worsening spinal instability. They occasionally regress spontaneously and may respond to aspiration and injection of corticosteroids, though there is a high recurrence rate with nonsurgical management. Synovial cysts resistant to nonsurgical management should be treated surgically. If the patient's symptoms can be attributable to radicular findings, a microsurgical decompression that limits further destabilization should suffice. However, if there is significant low back pain attributable to spinal instability, decompression and fusion remains an appropriate option. Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972. Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Question 94
Which of the following tumors is most likely to present with a pathologic fracture in a child?

Explanation
In nearly 50% of patients with a unicameral bone cyst, the lesion remains asymptomatic until a fracture occurs, usually as the result of relatively minor trauma. If the lesion expands, the bone is weakened and may cause pain. Fibrous cortical defects are usually an incidental finding and typically asymptomatic. Malignant bone tumors such as osteosarcoma and Ewing's sarcoma most commonly cause pain, and pathologic fracture occurs in less than 10% of patients. Giant cell tumors are uncommon in children and usually are painful. Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 95
High Yield
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 96
What is the most likely primary cause of decreased success rates of bony fusion in smokers undergoing lumbar arthrodesis?

Explanation
A number of studies have shown a lower success rate of arthrodesis in smokers. Animal models also have shown that administration of nicotine can markedly decrease the rate of arthrodesis. Although it may not be possible to completely eliminate some of the other associated factors that contribute to the failure of arthrodesis, it does appear that nicotine is the primary factor. Andersen T, Christensen FB, Laursen M, et al: Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine 2001;26:2623-2628.
Question 97
A 42-year-old man undergoes right total hip arthroplasty for hip dysplasia. Postoperatively, he has a significant limb-length increase with a foot drop. A preoperative radiograph is shown in Figure 19. Which of the following should have been considered preoperatively to avoid this complication?

Explanation
In a patient with bilateral hip dysplasia, there are significant technical challenges that need to be addressed to ensure a successful total hip arthroplasty. Restoring the center of the hip may cause significant lengthening and require femoral shortening. Lengthening of greater than 4 cm can lead to sciatic nerve palsy that will present clinically as a foot drop. A high hip center can be used when there is inadequate bone stock in the acetabulum to achieve adequate host bone coverage. A modular femoral implant may be used for a dysplastic hip with significant rotational deformity. Although an anterolateral approach to the hip may decrease the incidence of sciatic nerve palsy during the exposure, it will not be helpful when there is more than 4 cm of limb lengthening. Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement: Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080. Papagelopoulos PJ, Trousdale RT, Lewallen DG: Total hip arthroplasty with femoral osteotomy for proximal femoral deformity. Clin Orthop 1996;332:151-162.
Question 98
High Yield
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of

Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 99
High Yield
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
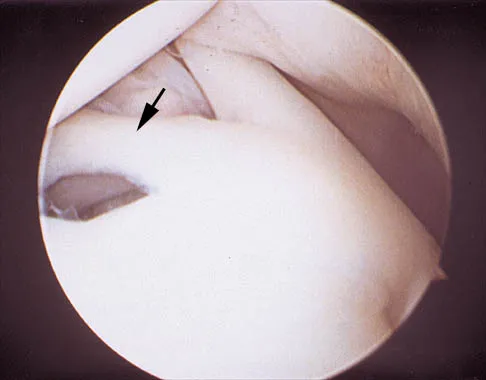
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 100
High Yield
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
The popliteal artery lies just posterior to the posterior cruciate ligament tibial insertion, separated only by the posterior capsule of the knee. When performing a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation of the tibial tunnel. Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
