Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
Numerous surgical approaches have been used for thoracic diskectomy, including the most recent VATS. One of the first approaches described, posterior laminectomy, involves manipulation of the spinal cord, which the other approaches avoid. The posterior approach had dismal results, including further neurologic deterioration and even paralysis. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864. Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg 1983;30:577-605. Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Question 2
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?

Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 3
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 4
High Yield
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?

Explanation
Rheumatoid arthritis commonly affects the metatarsophalangeal joints, which become destabilized with time resulting in hallux valgus and dislocated lesser claw toes. The result is metatarsalgia as the dislocated claw toes "pull" the fat pad distally. Severe hallux valgus reduces first ray load, which compounds the metatarsalgia because the load is transferred to the lesser metatarsal heads. First metatarsophalangeal arthrodesis restores weight bearing medially and corrects the painful bunion. Metatarsal head resection slackens the toe tendons to allow correction of the claw toes by whatever means necessary and decreases plantar load over the forefoot. Rheumatoid arthritis in the first metatarsophalangeal joint will continue to progress if osteotomies or a Lapidus procedure are performed. Keller resection arthroplasty increases transfer metatarsalgia and reduces push-off power during gait. Flexor-to-extensor tendon transfer of the lesser toes does not address the metatarsalgia and does not correct the dislocation of the metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Question 5
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?



Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
Question 6
High Yield
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?


Explanation
The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated. Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
Question 7
High Yield
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of

Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 8
High Yield
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Detailed Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 9
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?


Explanation
The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length. Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Question 10
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a "pencil in cup" distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?

Explanation
The patient's clinical picture is considered the classic presentation for psoriatic arthritis. The other answers are not applicable for the constellation of findings. Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1691-1693.
Question 11
High Yield
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?

Explanation
The patient needs to immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side. Sling immobilization without stretching for either 3 or 6 weeks will result in severe stiffness that will compromise her ultimate range of motion. Since she has a good quality subscapularis tendon, there is no need to avoid beginning external rotation to the side. However, starting a strengthening program at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal. Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Question 12
High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 13
High Yield
A 23-year-old man sustains a unilateral jumped facet with an isolated cervical root injury in a motor vehicle accident. Acute reduction results in some initial improvement of his motor weakness. Over the next 48 hours, examination reveals ipsilateral loss of pain and temperature sensation in his face, limbs, and trunk, as well as nystagmus, tinnitus, and diplopia. What is the most likely etiology for these changes?
Explanation
The patient is showing signs of vertebral artery stroke. The signs of Wallenberg syndrome include those listed above, as well as contralateral loss of pain and temperature sensation throughout the body, an ipsilateral Horner's syndrome, dysphagia, and ataxia. Vertebral artery injuries are not unusual in significant cervical facet injuries. A lesion in the cervical spinal cord is not associated with these symptoms, and an intracranial hemorrhage from trauma is unlikely to present in this manner. Young PA, Young PH: Basic Clinical Neuroanatomy. Baltimore, MD, Williams and Wilkins, 1997, pp 242-243. Hauop JS, et al: The cause of neurologic deterioration after acute cervical spinal cord injury. Spine 2001;26:340-346.
Question 14
High Yield
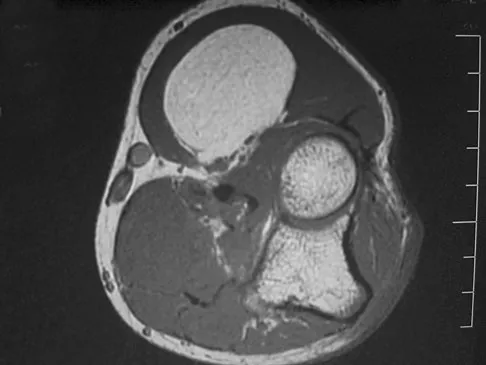
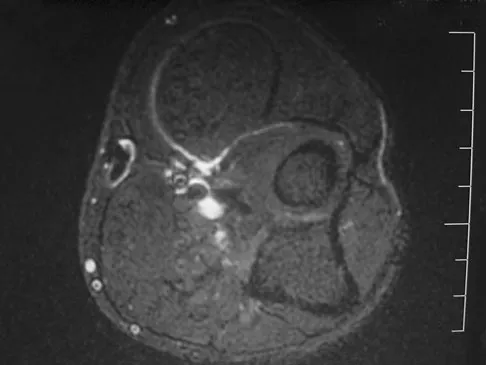
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?





Detailed Explanation
The imaging studies reveal a predominantly blastic lesion in the distal femur with posterolateral periosteal changes. The bone scan shows increased uptake in the distal femur, beyond that expected with radiography. Cross-sectional imaging confirms the presence of a soft-tissue mass extending from the lateral aspect of the femur, with diffuse intramedullary signal changes. This aggressive presentation, particularly in this location and in a patient of this age, is most consistent with osteosarcoma. The mineralization in the soft tissue strongly suggests neoplasm, not the reactive bony changes seen in an infectious process. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 15
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?

Explanation
The obturator internus originates on the obturator membrane and adjacent bone, including the quadrilateral plate, and exits the lesser sciatic notch to insert on the posterior medial greater trochanter. The structure labeled C is the pectineus, B is the sartorius, and D is the gluteus medius. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Question 16
High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Detailed Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 17
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 18
High Yield
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?

Explanation
Early mobilization and resumption of normal activities immediately after neck sprain has been shown to improve functional outcome and decrease subjective symptoms as measured 6 months after injury. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Question 19
High Yield
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of

Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 20
Which of the following methods best aids in diagnosis of an interdigital neuroma?

Explanation
History and physical examination are still the gold standard for diagnosis of an interdigital neuroma. Ultrasound and MRI may be helpful adjuncts but are dependent on equipment and operator expertise. Web space injection may be helpful for diagnostic and therapeutic purposes. Electromyography and nerve conduction velocity studies are of little benefit for distal lesions. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Question 21
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the



Explanation
The patient has a cavovarus deformity that has resulted in lateral foot overload and stressing of the lateral ligaments. Further treatment depends on the ability to correct the deformity. The Coleman block test indicates whether a deformity is fixed or supple. A supple deformity will respond to orthotic management or soft-tissue procedures, while a fixed deformity requires corrective osteotomy or fusion. Physical therapy, casting, and injection will not address the underlying pathophysiology. There is no indication that this is a neuropathic problem.
Question 22
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?


Explanation
Because the patient has chronic pain, a possible lateral recess stenosis of the C7 root, and no neurologic deficits, keyhole foraminotomy is the treatment of choice for decompressing the exiting nerve root and offering an early return to play, especially when using a muscle-splitting posterior approach. Henderson and associates reported excellent results with posterolateral foraminotomy in patients with radicular symptoms. Although anterior cervical diskectomy and fusion is equally effective in the long term, a period of 6 to 12 weeks is required to allow the anterior fusion to heal prior to a return to play. Chen and associates reported that keyhole foraminotomy maintains cervical motion segment dynamics better than compared to anterior limited diskectomy and foraminotomy or anterior diskectomy with fusion. Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512. Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Question 23
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 24
High Yield
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
Question 25
High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 26
High Yield
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The radiographs reveal a large femoral metaphyseal lytic lesion with well-defined borders. Joint space narrowing medially is consistent with polyethylene wear. The most likely diagnosis is particle-mediated osteolysis. Metastatic tumors and primary sarcomas adjacent to an arthroplasty are extremely rare. In addition, malignant tumors and infection would more likely reveal a destructive lesion with poorly defined borders and increased uptake on a bone scan. Stress shielding with massive bone loss has not been described in knee arthroplasty literature, although this entity has been observed in fully porous-coated femoral implants in total hip arthroplasty. Robinson EJ, Mulliken BD, Bourne RB, et al: Catastrophic osteolysis in total knee replacement: A report of 17 cases. Clin Orthop Relat Res 1995;321:98-105. Archibeck MJ, Jacobs JJ, Roebuck KA, et al: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Question 27
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren's contracture?
Explanation
The normal fascial components that become diseased and compose the spiral cord include the pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament. Cleland's ligament lies dorsal and is not involved with spiral cord formation. The intrinsic muscle and tendon, the natatory ligament, and the intermetacarpal ligament are well proximal to the digit and are not involved in spiral cord formation. McGrouther D: Dupuytren's contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 1, pp 565-569.
Question 28
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder "slip out" when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?



Explanation
The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert's. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 29
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 30
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of



Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 31
High Yield
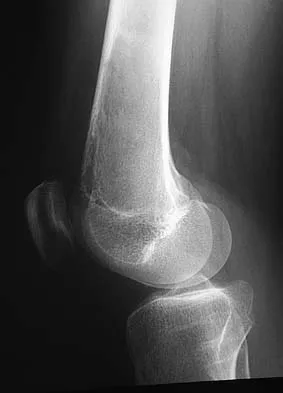
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 32
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?


Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 33
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Scientific References
-
:
Question 34
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?




Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 35
High Yield
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?


Detailed Explanation
Based on her symptoms and prior shoe wear modifications, the treatment of choice is surgical correction of the hallux valgus with a chevron osteotomy. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Steroid injection would only risk infection, as well as joint and capsule damage. Extra-depth shoes are an option; however, the patient is interested in surgical options. Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584. Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Question 36
High Yield
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Detailed Explanation
Ceramic-on-ceramic bearing surfaces have superior tribological properties and show lower linear wear than metal-on-metal implants. However, because of their lower strength and vulnerability to fracture, design considerations constrain the neck-length options available to ensure optimal taper fit.
Question 37
High Yield
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of


Explanation
The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 38
High Yield
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?

Explanation
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
Question 39
High Yield
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
EIP transfer results in no functional deficit. If the tendon is cut proximal to the sagittal band, there will be no extensor deficit. Browne EX, Teague MA, Snyder CC: Prevention of extensor lag after indicis proprius transfer. J Hand Surg Am 1979;4:168-172.
Question 40
High Yield
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Detailed Explanation
In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of "red flags" for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five "red flags" for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of "red flags" for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI. Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Question 41
High Yield
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of


Detailed Explanation
Fractures of the long bones are common in patients with myelodysplasia, and the frequency of fracture increases with higher level defects. Fractures also occur following surgery and immobilization secondary to disuse osteoporosis. The response to the fracture (swelling, fever, warmth, erythema) is often confused with infection, osteomyelitis, or cellulitis. Management should consist of a short period of immobilization in a well-padded splint. Long-term casting results in further osteopenia and repeated fractures. Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Question 42
High Yield
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?

Detailed Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 43
What is the most common problem seen following epiphysiodesis for limb-length discrepancy?

Explanation
Errors in timing are by far the most common in this technically safe procedure. Incomplete growth arrest has been reported in up to 15% of patients versus timing errors in 61%. Fracture through the site has been reported rarely. Neurovascular and cartilaginous injury are extremely uncommon but always need to be considered when performing surgery in the vicinity of these structures. Blair VP III, Walker SJ, Sheridan JJ, Schoenecker PL: Epiphysiodesis: A problem of timing. J Pediatr Orthop 1982;2:281-284.
Question 44
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
Cadaveric studies have shown that external rotation of the tibia is most pronounced following transection of the posterior cruciate and lateral collateral ligaments with the knee at 90 degrees of flexion. Isolated release of the lateral collateral ligament results in increased external tibial rotation at 30 degrees. Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242. Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Question 45
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin's lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?




Explanation
Radiation-associated sarcomas typically occur at least 5 years following radiation therapy, in the radiation therapy field, and with different histology than the original disease. The radiograph shows a lytic destructive lesion of the medial clavicle. The radiographic differential could include any of the above etiologies. The CT and MRI scans show this same reaction with extension into the adjacent soft tissue and periosteal reaction. These findings eliminate a degenerative process or radiation-induced osteonecrosis but do not distinguish between a neoplastic and infectious process. A PET scan showed marked uptake in the distal clavicle, which is more consistent with a malignant neoplastic process than a reactive process, like that of an infection. These findings, combined with the cellular atypia and bone formation on the biopsy specimen, confirm the diagnosis of radiation-associated sarcoma. In this older patient, radiation-associated sarcoma appears in an unusual location secondary to her previous radiation treatment in that region, which can occur 3 to 50 years after previous radiation therapy. Shaheen M, Deheshi BM, Riad S, et al: Prognosis of radiation-induced bone sarcoma is similar to primary osteosarcoma. Clin Orthop Relat Res 2006;450:76-81.
Question 46
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
Revision of a failed patellar component can be difficult because of bone loss and damage to the extensor mechanism. Several authors have advised against reinsertion of a patellar component if the residual patellar thickness is 10 mm or less. Leaving an unresurfaced bony remnant in place at the time of revision or reimplantation surgery has been shown to be a reasonable option; however, the results are of a lower quality when compared with revision surgery where the patellar component can be retained or revised. The other treatment options have not been shown to be effective approaches to this problem. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620. Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Question 47
High Yield
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?


Detailed Explanation
The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement. McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective. Am J Orthop 1999;28:21-26.
Question 48
High Yield
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?

Detailed Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion. Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Question 49
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?


Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 50
High Yield
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
Surgical open reduction may increase the neurologic deficit if a disk herniation exists. Evidence from animal studies suggests that rapid decompression of the spinal cord may improve recovery. Serially increasing traction weight to reduce the dislocation has been shown to be safe when used in patients who are awake. Indications for MRI include patients who are unable to cooperate with serial examinations, the need for open reduction, and progression of deficit during awake reduction. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am 1995;77:1042-1049. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 51
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Although management of shoulder pain in the throwing athlete is controversial, there are some general principles. Initial management generally includes rest from throwing, restoring normal joint function, specifically motion and strength as well as eliminating pain. In this patient, examination reveals excessive external rotation and decreased internal rotation. This pattern is common in pitchers; however, the total arc of motion should remain close to 180 degrees in abduction. In this patient, the total arc is 140 degrees. Treatment should first focus on restoring a 180-degree arc with posterior scapular stretching, as well as pain control and muscle rehabilitation. Injections and surgery are generally reserved for patients who fail to respond to rest and rehabilitation.
Question 52
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?


Explanation
This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 53
Optimal management of the injury shown in Figure 31 should include which of the following?

Explanation
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Question 54
At the level of the midcalf, the plantaris tendon is found at which of the following locations?
Explanation
The plantaris tendon is often harvested to augment a tendon reconstruction. The origin of the plantaris muscle is on the posterolateral aspect of the distal femur, and the muscle lies lateral to the tibial nerve and the posterior tibial artery. The tendon then courses posteriorly between the soleus and the medial head of the gastrocnemius. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 475.
Question 55
High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Detailed Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 56
For halo traction, what is the preferred site for anterior pin placement?
Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 57
High Yield
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 58
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?


Explanation
Because the radiographs demonstrate severe arthritis, hallux metatarsophalangeal arthrodesis is the treatment of choice. Cheilectomy alone will not relieve pain because the entire joint is degenerative. Joint replacement has not been shown to be a long-term solution. Keller resection arthroplasty is not indicated in younger active patients. Hallux valgus correction will not address arthritis of the joint and could stiffen the joint further. Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Question 59
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 60
High Yield
What is the mechanism of action of bisphosphonates?
Detailed Explanation
Bisphosphonates are stable analogues of pyrophosphate that have a strong affinity for bone hydroxyapatite; these agents inhibit bone resorption by reducing the recruitment and activity of osteoclasts and increasing apoptosis. Bone formed while patients are receiving bisphosphonate treatment is histologically normal. Bisphosphonates have been shown to be effective in decreasing pathologic fractures, bone pain, and the need for radiation therapy in patients with multiple myeloma and metastatic carcinoma to bone. The most effective method of administration is via monthly intravenous infusion. Osteonecrosis of the mandible is sometimes a complication of this treatment. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 61
High Yield
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?

Detailed Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 62
High Yield
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Detailed Explanation
The average location of the anterior portal is 6.3 cm distal to the anterior superior iliac spine. The lateral femoral cutaneous nerve typically has divided into three or more branches at the level of the anterior portal. The portal usually passes within several millimeters of the most medial branch. Injury to the nerve can lead to meralgia paresthetica. The femoral nerve lies an average minimum distance of 3.2 cm from the anterior portal. The ascending branch of the lateral circumflex artery lies approximately 3.7 cm inferior to the anterior portal. Neither the ascending branch of the medial circumflex artery nor the superior gluteal nerve are at risk. Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Question 63
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?


Explanation
A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
Question 64
High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 65
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by

Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Question 66
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 67
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
The patient has diskitis. Administration of IV antibiotics speeds resolution and minimizes recurrence. Bed rest and cast immobilization have been successfully used to treat this disorder but can be associated with prolonged recovery and frequent recurrence, even when oral antibiotics are administered. A perivertebral abscess seen in association with this condition usually resolves without surgery. Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop 1995;15:652-660.
Question 68
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?



Explanation
Tuberculosis is uncommon in the cervical spine but has a relatively greater incidence in young children. In a review of 40 patients with lower cervical spine involvement (C2 to C7), 24 were younger than age 10 years at presentation. In children, the disease is characterized by more extensive involvement with the formation of large abscesses. In older patients with lower cervical tuberculosis, the disease is more localized but is more likely to cause paraplegia. Four-drug antituberculosis therapy should be used. For patients with pain or neurologic dysfunction, anterior excision of diseased bone and grafting are indicated. Whether vertebral body excision and grafting should be done in an asymptomatic 10-year-old child is debatable. The CT scan shows a large "cold" abscess that is partially calcified. Hsu LC, Leong JC: Tuberculosis of the lower cervical spine (C2 to C7): A report on 40 cases. J Bone Joint Surg Br 1984;66:1-5.
Question 69
High Yield
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
Osteolysis of an otherwise well-functioning total hip arthroplasty is a recognized complication, and its radiographic appearance is typical, as shown here. Distal osteolysis, such as that shown here, is more prevalent when there is noncircumferential sealing of the proximal femoral canal. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 70
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of

Explanation
Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability. Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Question 71
A 5-year-old girl sustained a comminuted Salter-Harris type IV fracture of the left distal tibia 2 years ago. The AP radiograph shown in Figure 54a reveals a growth arrest and a 1.4-cm limb-length discrepancy. The ankle is in approximately 20 degrees of varus. Figure 54b shows a coronal reconstruction image of the distal tibial physis, and Figure 54c shows a sagittal reconstruction image of the same area. On the sagittal reconstruction image, the bar extends from the 9-mm mark to the 24-mm mark in 3-mm increments. On the coronal image, the bar extends from the 9-mm mark to the 24-mm mark, also in 3-mm increments. A map of the physeal bar based on these measurements is shown in Figure 54d. Initial treatment should consist of




Explanation
Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 72
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower's elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin. Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Question 73
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the

Explanation
The superior gluteal nerve is located approximately 7.82 cm above the tip of the greater trochanter as it courses through the gluteus medius. This anatomic consideration is relevant during a Hardinge approach to the hip, where excessive proximal dissection or retraction could result in nerve injury. A split of the gluteus medius of no more than 4 cm above the greater trochanter is considered safe. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Question 74
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 75
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include

Explanation
Achieving stability in chronic locked posterior dislocations of the shoulder remains a difficult challenge. Intraoperative measures include decreased humeral retroversion, anterior releases, and posterior capsular tightening. Postoperative rehabilitation is of equal importance. Immobilization in an external rotation brace (10 degrees to 15 degrees) with the arm at the side for 4 to 6 weeks is recommended to decrease tension in the posterior capsule. When passive range-of-motion exercises are instituted, they should be performed in the plane of the scapula to avoid stress posteriorly. Internal rotation and supine elevation should be avoided for similar reasons. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 76
High Yield
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of





Explanation
The initial fracture was an unstable reverse oblique intertrochanteric fracture with subtrochanteric extension. Initial fixation with a high-angled screw and side plate construct may not provide stability as well as a 95 degree fixed-angle device or a intramedullary hip screw device. The follow-up radiographs show loss of fixation and further propagation of the fracture distally. Reconstruction would best be accomplished with hardware removal and conversion to a long intramedullary nail with femoral head fixation or a 95 degree angled plate and screw device. Conversion to a longer plate does not improve the biomechanical situation at the primary fracture site. In situ bone grafting would not provide any additional stability and would not correct the deformity. The proximal femoral fracture is not amenable to retrograde nailing. Cerclage wiring will not sufficiently enhance stability and is not indicated. Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334. DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825. Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Question 77
High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Detailed Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 78
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include

Explanation
The patient has a displaced radial neck fracture. Displaced radial neck fractures with angulation of more than 30 to 45 degrees require reduction. Methods of attempted closed reduction include wrapping the arm with an Esmarch's bandage and applying direct pressure over the maximum deformity of the radial head. More aggressive methods include a Kirschner wire used as a joystick or intramedullary reduction as described by the Metaizeau technique. Open reduction should be avoided because of complications such as stiffness or osteonecrosis. Indications for open reduction are irreducible displacement of more than 45 degrees with severe restriction of forearm rotation. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Question 79
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 80
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?


Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 81
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 82
High Yield
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
When you are employed as a team physician, you are obligated to inform the players and the team organization of all athletically relevant medical issues. This differs significantly from the normal rule of patient confidentiality. If the player came to see you and you were not the team physician, you may not inform the team unless the player so desires. As the team physician, you are not obligated to inform the media. Tucker AM: Ethics and the professional team physician. Clin Sports Med 2004;23:227-241.
Question 83
Figure 24 shows the sitting AP and lateral spinal radiographs of a nonambulatory 12½-year-old boy with Duchenne muscular dystrophy who is being evaluated for scoliosis. The lumbar curve from T12 to L5 measures 36 degrees, and the thoracic curve from T3 to T12 measures 24 degrees on the AP radiograph. He has 5 degrees of pelvic obliquity. His forced vital capacity is 45% of predicted for height and weight. What is the most appropriate treatment for the spinal deformity?

Explanation
Posterior spinal fusion is the treatment of choice for scoliosis in patients with Duchenne muscular dystrophy once they are no longer able to walk. This treatment improves quality of life and upright wheelchair positioning. Its effect on pulmonary function is less clear, as pulmonary function will continue to decline because of the underlying muscle disease. While bracing and wheelchair modifications may slow the progression of the curve, progression will continue. Surgical intervention at this stage does not have to include the pelvis, which, in general, is indicated in curves of greater than 40 degrees, and when pelvic obliquity is greater than 10 degrees. Fixation to the pelvis should also be considered in lumbar curves where the apex is lower than L1. Surgical treatment usually can be safely performed if the vital capacity is greater than 35%. Hahn GV, Mubarak SJ: Muscular dystrophy, in Weinstein SL (ed): The Pediatric Spine, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 819-832.
Question 84
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
The long-term effect of transient quadriplegia is unknown. Based on a history of one brief episode of transient quadriplegia and normal examination and MRI findings, the risk of permanent spinal cord injury with a return to play is low. There is a risk of recurrent episodes of transient quadriplegia after the initial episode. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136. Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509. Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Question 85
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
As long as the dissection stays proximal to the annular ligament, the posterior interosseous nerve is not at risk for injury. However, to ensure that the nerve is as far removed from the surgical field as possible, the forearm should be placed in pronation. Forearm supination of any degree will bring the nerve toward the surgical field. A neutral position of the forearm or elbow extension with wrist extension will not protect the posterior interosseous nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 100.
Question 86
A 23-year-old man has pain and a callus beneath the second metatarsal head. Initial management should consist of

Explanation
The initial treatment of metatarsalgia with or without the presence of an intractable keratosis should be conservative. Simple paring of the callus with elevation of the metatarsals may suffice. A prefabricated "off-the-shelf" orthosis or felt pad can be used before investing in a custom orthosis. The use of medicated pads can lead to greater amounts of keratosis and should be avoided. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Question 87
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 88
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?

Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 89
High Yield
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?

Explanation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries. Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Question 90
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed "quadriceps avoidance." This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45 degrees of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability. Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20. Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Question 91
High Yield
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?

Explanation
Osteonecrosis of the femoral head is the most devastating complication of SCFE. There is a 47% incidence of ischemic necrosis associated with an unstable SCFE. By definition, the patient with an unstable SCFE is unable to bear weight even with crutches. Osteonecrosis is most likely associated with the initial femoral head displacement rather than the result of either tamponade from hemarthrosis or from gentle repositioning prior to stabilization. Age, sex, and obesity are not risk factors for osteonecrosis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 92
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 93
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative

Explanation
Boden and associates' recent article presents significant evidence that patients with rheumatoid arthritis, neurologic deterioration, and C1-2 instability are more likely to improve after surgery if the posterior alanto-odontoid interval is greater than 10 mm preoperatively. The accepted safe range for the posterior atlanto-odontoid interval is 14 mm. This measurement is believed to better represent the space available for the cord than the anterior alanto-odontoid interval. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 94
High Yield
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?



Explanation
Chondrosarcomas associated with diffuse bone lesions (enchondromas) are characteristic of Ollier's disease. When accompanied by subcutaneous masses (hemangiomas), the condition is called Maffucci's syndrome. Multiple hereditary exostosis is characterized by diffuse osteochondromas. McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia with cafe-au-lait spots and precocious puberty. Neurofibromatosis can have associated bone lesions but is not associated with chondrosarcomas. Sun TC, Swee TC: Chondrosarcoma in Maffucci's syndrome. J Bone Joint Surg Am 1985;67:1214-1219. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Question 95
High Yield
Back pain and ipsilateral knee pain are common long-term sequelae of hip arthrodesis. To limit these problems, what position should be avoided during fusion of the hip?
Detailed Explanation
The recommended position for a hip fusion is flexion of 20 degrees to 30 degrees, slight adduction (5 degrees) or neutral, and 10 degrees of external rotation. In long-term follow-up, patients who underwent fusion in abduction had more ipsilateral knee and low back pain than patients who were positioned in adduction. Internal rotation should be avoided to prevent interference with the opposite foot during gait. External rotation facilitates the application of shoe wear. Callaghan JJ, Brand RA, Pederson DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 96
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?


Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 97
High Yield
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?

Detailed Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 98
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
Open release allows lengthening of the shortened subscapularis and is preferred when there are extra-articular contractures. Arthroscopic release, combined with the use of an interscalene catheter postoperatively, is an excellent treatment for capsular contractures but is contraindicated after procedures that result in extracapsular shortening (ie, Magnuson-Stack, Putti-Platt). Additional physical therapy or manipulation under anesthesia is not likely to be helpful. Shoulder hemiarthroplasty is contraindicated with normal articular surfaces, but prosthetic arthroplasty is sometimes necessary for arthritis associated with instability or overly tight instability repairs. Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147. Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 99
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?



Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 100
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by

Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
