Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Detailed Explanation
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Question 2
High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 3
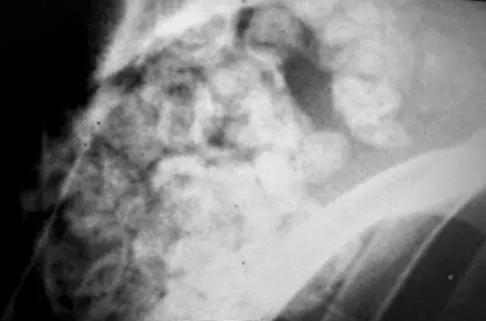
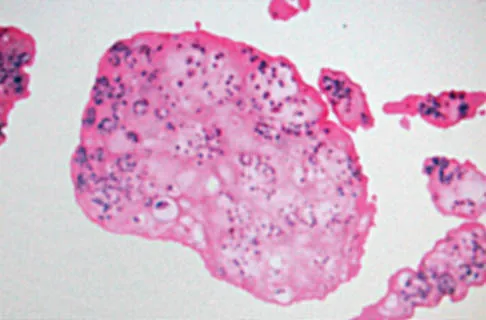
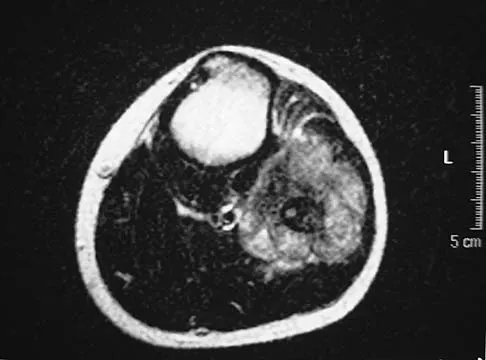
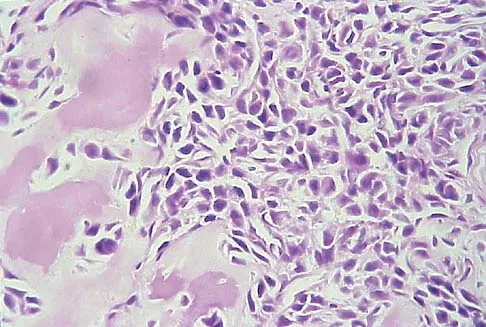
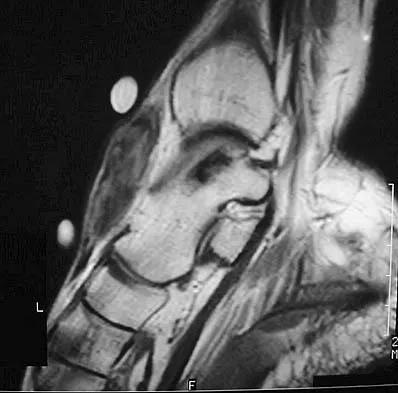
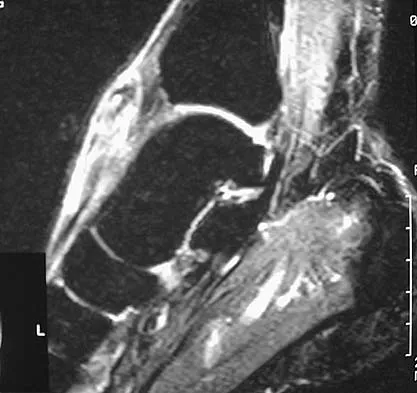
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include




Explanation
The patient has rhabdomyosarcoma. Axilliary node and bone marrow biopsy are part of the staging because about 12% of patients with rhabdomyosarcoma of the extremity have evidence of lymph nodes metastases at presentation. Bone marrow metastases have been shown to portend a worse prognosis. Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Question 4
Sudden cardiac death in the young athlete is most frequently caused by

Explanation
Hypertrophic cardiomyopathy is the leading cause of sudden cardiac death in athletes, accounting for 40% of reported cases. Most athletes have no previous symptoms, and sudden death may be the first clinical manifestation. The prevalence of hypertrophic cardiomyopathy in the general population is 1 in 500, with a mortality rate of 2% to 4% in young adults. Athletes with active myocarditis should not engage in sports for up to 6 months, and although they may be at risk for the development of chronic cardiomyopathy, it is rarely a cause of sudden cardiac death. Mitral valve prolapse with an accompanying systolic murmur is common in the general population, but infrequently a cause of sudden cardiac death. Weakening of the aortic wall associated with Marfan syndrome can result in abrupt rupture of the aorta. This accounts for 3% of sudden cardiac deaths in young athletes. Marfan syndrome usually can be detected on preparticipation screenings by its skeletal and ocular manifestations. Atherosclerotic coronary artery disease is the most common cause of sudden cardiac death in older athletes, accounting for 75% of reported cases. However, it is much less common in the young competitive athlete. Burke AP, Farb A, Virmani R, Goodin J, Smialek JE: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991;121:568-575.
Question 5
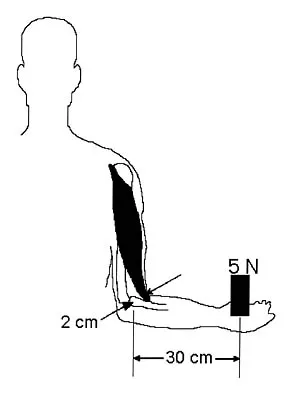
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?

Explanation
At the level of tibial bone resection in total knee arthroplasty, the common peroneal nerve lies superficial to the lateral head of the gastrocnemius and is therefore protected by this structure. In an MRI study of 60 knees, the mean distance from the bony posterolateral corner of the tibia to the nerve was 1.49 cm, with no distance less than 0.9 cm. The distance from the bone to nerve was greater in larger legs. Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the "pie crust" technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
Question 6
High Yield
The fracture shown in Figure 50 is most reliably treated with what form of fixation?

Detailed Explanation
The radiograph shows a comminuted proximal ulnar fracture. The most reliable fixation is a posterior plate, acting as a tension band plate. The fracture involves the proximal shaft of the ulna; therefore, a 3.5-mm compression plate or one of similar size should be used to provide adequate stability. Kirschner wires and tension band wires do not provide axial stability of the comminution of the ulna. Compression screws alone will most likely fail and will not provide axial rotational stability to the construct. A medial plate will not resist the distraction forces across this fracture. McKee MD, Seiler JG, Jupiter JB: The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive cases. Injury 1995;26:661-666.
Question 7
High Yield
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of

Detailed Explanation
Because nonsurgical managment has failed and a significant number of type II odontoid fractures will go on to a nonunion, the salvage treatment of choice is posterior fusion at C1-2. Odontoid screws are contraindicated in patients with a chronic nonunion, which this patient has at the end of 3 months. Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761. Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Question 8
High Yield
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 9
High Yield
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Detailed Explanation
Both autograft and allograft have been used for complex acetabular reconstructions. They have been shown to be successful in the short term. However, graft resorption with collapse and subsequent cup loosening have occurred at high rates for both types of grafts, especially if reinforcement rings or cages are not used. Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 10
High Yield
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of

Detailed Explanation
The radiograph shows calcific deposits within the substance of the supraspinatus tendon. Patients with this condition are prone to recurrent bouts of acute inflammation in the shoulder. While the response to cortisone injection is often dramatic, repeated injections are not recommended because of injury to the collagen fibers. Good results have been obtained with arthroscopic evacuation of the calcium deposits. In one study, the addition of a subacromial decompression did not improve the results. Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Question 11
High Yield
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?


Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled cal
Question 12
High Yield
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
Laminectomy is associated with the highest risk of iatrogenic paraplegia because retraction on the cord is necessary for visualization, but retraction is difficult because of tethering of the intradural dentate ligaments. All of the other approaches allow for access to the disk herniation through an angle that avoids the cord itself, although other limitations may exist. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Question 13
High Yield
The condition shown in Figures 9a and 9b is most likely the result of


Explanation
The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection. Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley's Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 14
High Yield
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?


Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 15
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?


Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 16
High Yield
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?

Detailed Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 17
High Yield
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?


Explanation
Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 18
A 77-year-old woman who underwent a cemented total hip arthroplasty 10 years ago now reports groin pain. Examination reveals a loosened acetabular component and a well-fixed femoral component. Treatment should consist of revision of
Explanation
Recent literature supports retention of well-fixed cemented femoral components when revising loosened cemented acetabular components. Current literature also supports the use of cementless components for revision of loosened cemented acetabular components. Peters CL, Kull L, Jacobs JJ, Rosenberg AG, Galante JO: The fate of well fixed cemented femoral components left in place at the time of revision of the acetabular component. J Bone Joint Surg Am 1997;79:701-706. Poon ED, Lachiewicz PF: Results of isolated acetabular revisions: The fate of the unrevised femoral component. J Arthroplasty 1998;13:42-49. Moskal JT, Shen FH, Brown TE: The fate of stable femoral components retained during isolated acetabular revision: A six- to twelve-year follow-up study. J Bone Joint Surg Am 2002;84:250-255.
Question 19
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?

Explanation
Adequate decompression of the cervical cord can be achieved in a variety of ways depending on the pathoanatomy of the compression, but kyphosis is a relative contraindication to laminectomy alone. For laminectomy to be effective, the lordosis must be maintained so the cord can displace posteriorly away from the anterior structures. In addition, removing the posterior tension band increases the probability that the kyphosis will progress, therefore increasing the force against the front of the cord as it tents across the kyphosis. Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745. Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Question 20
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia. Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Question 21
High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 22
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
Internal rotators of the shoulder include the subscapularis, pectoralis major, teres major, and latissimus dorsi muscles. The subscapularis has two portions, with the upper portion receiving its innervation from the upper subscapular nerve (C5) and the lower portion from the lower subscapular nerve (C5-6). The two tests commonly performed to isolate the internal rotation to the subscapularis muscle are the lift-off test and the belly press test. Electromyographic findings have shown the lift-off test to be more accurate for the lower portion of the subscapularis and the belly press test to be more sensitive for the upper portion. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Question 23
High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 24
High Yield
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?


Detailed Explanation
Aneurysmal bone cysts typically present as radiolucent lesions with an expansile remodeled cortex. The histologic appearance consists of blood-filled lakes surrounded by a benign lining that contains fibroblasts, giant cells, and hemosiderin. Although the other lesions are in the radiographic differential diagnosis, these histologic findings indicate an aneurysmal bone cyst. Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Question 25
High Yield
What region of the thoracic curve is most dangerous for pedicle screw insertion while performing a posterior fusion for adolescent idiopathic scoliosis?
Detailed Explanation
Morphologic and anatomic studies confirm the pedicle is smaller on the concave side of thoracic curves. The dura is also closer to the pedicle on the concave side of the curves. Liljenqvist U, Allkemper T, Hackenberg L, et al: Analysis of vertebral morphology in idiopathic scoliosis with use of magnetic resonance imaging and multiplanar reconstruction. J Bone Joint Surg Am 2002;84:359-368.
Question 26
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of




Explanation
The patient has Ewing's sarcoma. Management options for local tumor control include radiation therapy, resection, or a combination; however, in this patient wide resection is preferred over radiation therapy. Radiation therapy is associated with damage to the growth plate, pathologic fracture, radiation-induced sarcomas, and a local recurrence rate of approximately 10% to 12%. Radiation therapy is used for positive margins, unresectable tumors, or for tumors that have a poor response to chemotherapy. Amputation is not necessary since the tumor is resectable. Chemotherapy has improved overall survival rates to over 60% of patients. Sailer SL: The role of radiation therapy in localized Ewing' sarcoma. Semin Radiat Oncol 1997;7:225-235. Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing's sarcoma. United Kingdom Children's Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704. Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Question 27
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Question 28
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 29
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?

Explanation
When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures. McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522 McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707. Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop 2000;370:19-33.
Question 30
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?



Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
Question 31
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 32
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show


Explanation
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 33
High Yield
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include

Explanation
The patient has a cyclops lesion. This is a nodule of fibroproliferative tissue that originates from either drilling debris from the tibial tunnel or remnants of the ACL stump; more rarely it is the result of broken graft fibers. The treatment of choice is excision of the nodule and, if needed, additional notchplasty. Marked improvements in function and symptoms have been noted after removal of the extension block and resumption of a rehabilitation program. Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Question 34
High Yield
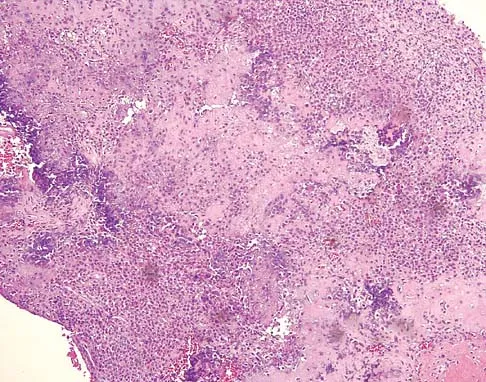
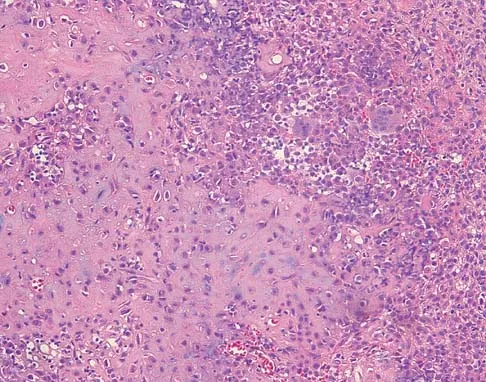
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?

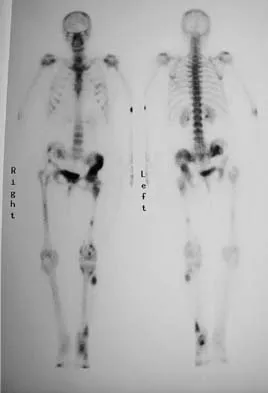


Explanation
Chondrosarcomas associated with diffuse bone lesions (enchondromas) are characteristic of Ollier's disease. When accompanied by subcutaneous masses (hemangiomas), the condition is called Maffucci's syndrome. Multiple hereditary exostosis is characterized by diffuse osteochondromas. McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia with cafe-au-lait spots and precocious puberty. Neurofibromatosis can have associated bone lesions but is not associated with chondrosarcomas. Sun TC, Swee TC: Chondrosarcoma in Maffucci's syndrome. J Bone Joint Surg Am 1985;67:1214-1219. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Question 35
High Yield
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of


Explanation
The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas. Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Question 36
High Yield
A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?

Detailed Explanation
Arthrodesis of any of the ankle or hindfoot joints should be reserved for fixed deformities or end-stage degenerative arthritis. Achilles tendon lengthening is necessary to correct the equinus and to improve dorsiflexion-plantar flexion balance. Similarly, transfer of the posterior tibialis tendon reduces both plantar flexion and inversion torque. Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.
Question 37
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?

Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion. Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Question 38
High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by

Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 39
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 40
High Yield
Storage of musculoskeletal allografts by cryopreservation is achieved by
Detailed Explanation
Cryopreservation uses chemicals to remove cellular water and controlled rate freezing to prevent ice crystal formation. The tissue is procured, cooled to wet ice temperature for quarantine, and then stored in a container with cryoprotectant solution of dimethyl sulfoxide or glycerol which displaces the cellular water. The controlled rate freezing is then done to prevent ice crystal formation. Fresh allografts are not frozen in order to maintain maximum cellular viability, and this process limits the shelf life of osteochondral allografts. Freeze-drying involves replacement of water in the tissue with alcohol to a moisture level of 5% and then uses a vacuum process to remove the alcohol from the tissue. Preparation of fresh frozen grafts involves freezing the graft twice and packaging the tissue without solution at minus 80 degrees C. American Association of Tissue Banks: Standards for Tissue Banking. MacLean, VA, American Association of Tissue Banks, 1999. Vangsness CT Jr, Triffon MJ, Joyce MJ, et al: Soft tissue allograft reconstruction of the human knee: A survey of the American Association of Tissue Banks. Am J Sports Med 1996;24:230-234.
Question 41
A previously healthy 13-year-old girl has had thigh pain for the past 3 weeks. The radiograph shown in Figure 47a reveals a lesion in the right femur. A bone scan and CT scan of the chest show no evidence of other lesions. A biopsy specimen is shown in Figure 47b. What is the most likely diagnosis?


Explanation
The patient has Langerhans cell histiocytosis that may be solitary (eosinophilic granuloma) or associated with systemic illness (Hand-Schuller-Christian disease and Letterer-Siwe disease). The solitary form of the disease, eosinophilic granuloma, typically affects patients in the first three decades of life. Radiographically, it is characterized as a well-defined, lytic, "punched out" intramedullary lesion. Histologically, two cell types, eosinophils and Langerhans cells, are seen. The Langerhans cells are seen as mononuclear histiocyte-like cells with oval nuclei with well-defined round or oval cytoplasm. A prominent nuclear groove can be seen in most of the nuclei (coffee bean nuclei). A mixture of inflammatory cells and lipid-laden foam cells with nuclear debris may be present as well. The lack of nuclear atypia and atypical mitoses excludes malignant conditions such as Ewing's sarcoma, lymphoma of bone, and metastatic neuroblastoma. The lack of acute inflammatory cells excludes the diagnosis of osteomyelitis. The eosinophils have bi-lobed nuclei and granular eosinophilic cytoplasm. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1988.
Question 42
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of

Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 43
High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 44
High Yield
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?

Explanation
Any of the above conditions is credible with a limited history. The MRI scan unequivocally shows the stress fracture in the distal tibia. Most tibial stress fractures can be managed with rest and immobilization. Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 45
High Yield
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Detailed Explanation
Loss of external rotation can lead to degenerative joint disease following an anterior stabilization procedure. A tight anterior capsule will prevent internal impingement. Risk of thoracic outlet syndrome should not be increased. Subscapularis detachment is a risk following open anterior repair; however, a gain in external rotation would be noted. In time, this patient's shoulder may show increased posterior glenohumeral wear but should not have symptoms of recurrent subluxation unless multidirectional instability is present. Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 46
What type of nerve palsy is most common following elbow arthroscopy?

Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 47
High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of



Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 48
High Yield
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?

Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 49
High Yield
For halo traction, what is the preferred site for anterior pin placement?
Detailed Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 50
The arrow in Figure 11 points toward a finding consistent with which of the following?

Explanation
The finding of a unilateral absent pedicle is often referred to as a winking owl sign and is a manifestation of pedicle destruction from metastatic disease. As the vertebral body is destroyed from the neoplastic process, it extends into the pedicle and destroys the cortical rim that normally creates the oval ring of the pedicle on an AP image. McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Question 51
High Yield
Turf toe typically involves injury to which of the following structures of the great toe?
Detailed Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 52
High Yield
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of

Explanation
Nonsurgical management such as a functional brace, hanging arm cast, or sugar tong splint is the treatment of choice for a fracture of the humeral shaft that is the result of throwing. The fracture surface typically is wide and the degree of displacement is not large; therefore, surgery is not indicated in most patients. Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Question 53
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of

Explanation
In most patients with symptomatic talocalcaneal coalition involving less than 50% of the subtalar joint, resection with fat graft interposition is preferred over a subtalar or triple arthrodesis, especially if reasonable range of motion can be achieved. This patient has a synchondrosis that is partially cartilaginous. Although patients may have a residual gait abnormality, most report pain relief after surgery. Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539. Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Question 54
A 14-year-old boy undergoes application of a circular frame with tibial and fibular osteotomy for gradual limb lengthening. He initiates lengthening 7 days after surgery. During the first week of lengthening, he reports that turning of the distraction devices is becoming increasingly difficult. On the 9th day of lengthening, he is seen in the emergency department after feeling a pop in his leg and noting the acute onset of severe pain. What complication has most likely occurred?

Explanation
Incomplete corticotomy may result from osteotomy with limited soft-tissue stripping and exposure. When the patient begins distraction, tension develops at all wire/half-pin and bone interfaces, leading to increasing difficulty in distraction and limb pain. Sudden spontaneous completion of the osteotomy with continued tension applied by the fixator results in acute distraction of the osteotomy with severe pain. Premature consolidation is unlikely this early following the initial surgery. Birch JG, Samchukov ML: Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J Am Acad Orthop Surg 2004;12:144-154.
Question 55
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?

Explanation
Many clinical studies to date show that the extent of arthritis is the most common variable that has the greatest influence on outcome. The success rate of allograft transplantation is significantly diminished in patients who have grade IV chondromalacia of the knee or notable flattening and general joint incongruity. Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63. Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
Question 56
High Yield
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate


Detailed Explanation
In the absence of vascular compromise, there has been no proven value to proceeding immediately to surgery, especially when the patient has a full stomach and runs a significant risk of perioperative aspiration. It would be more prudent to wait until the next morning with a surgical plan of closed reduction and pinning. Open reduction should be reserved for the unusual case of where closed treatment has not been successful. The implication that there may be a radial nerve injury associated with this fracture does not alter the treatment plan, and with a high level of certainty would be expected to resolve. Attempting closed reduction in the emergency department creates the opportunity for uncertain results and is not tolerated well by most patients. Skeletal traction, with its associated lengthy hospitalization and the technical difficulties associated with both the traction and radiographic evaluations, has fallen into disfavor for typical clinical situations. Iyengar SR, Hoffinger SA, Townsend DR: Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: A comparative study. J Orthop Trauma 1999;13:51-55.
Question 57
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 58
The failure of the acetabular component shown in Figure 15 is most likely the result of the use of a 32-mm head and

Explanation
Astion and associates analyzed 23 acetabular components, out of a total of 173 implanted, that had failed because of either migration or severe osteolysis. The radiographic appearance of osteolysis was positively associated with the duration that the implant had been in situ. The prevalence of osteolysis was also significantly greater in acetabular components with an outer diameter of 55 mm or less (a polyethylene thickness of 8.5 mm or less). Thirteen of the 23 components were revised at a mean of 70 months after the index operation. Examination of the retrieved acetabular components revealed extensive polyethylene damage on the articular and back surfaces of the liners. Cracks in the polyethylene rim of the liner and deformation of the antirotation notch in the polyethylene rim were common findings. The density of the polyethylene was greater than expected, and more particles than anticipated had not fused with the surrounding polyethylene. Factors related to both the design and the material contributed to the failure of these porous-coated anatomic acetabular components.
Question 59
High Yield
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity. Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Question 60
High Yield
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 61
High Yield
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 62
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?

Explanation
Retrograde ejaculation is the sequela of superior hypogastric plexus injury. This structure needs protection, especially during anterior exposure of the L5-S1 disk space. Only blunt dissection should be used, and use of monopolar electrocautery should be avoided. If possible, preserve and retract the middle sacral artery. Once the iliac veins are isolated, blunt dissection is begun along the course of the medial edge of the left iliac vein, reflecting the prevertebral tissues toward the patient's right side. The dissection goes from left to right because the parasympathetic plexus is more adherent on the right side.
Question 63
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)?

Explanation
The rotator cuff interval is located between the supraspinatus and subscapularis and the biceps tendon is deep to the interval. It is a triangular area where the base is the coracoid process and the apex is the transverse humeral ligament at the biceps sulcus. Closure or tightening of this area is often helpful in patients with shoulder instability. Conversely, this area is often contracted in patients with adhesive capsulitis and may need to be released. Selecky MT, Tibone JE, Yang BY, et al: Glenohumeral joint translation after arthroscopic thermal capsuloplasty of the rotator interval. J Shoulder Elbow Surg 2003;12:139-143.
Question 64
High Yield
A 60-year-old woman reports anterior knee pain 2 years after undergoing primary total knee arthroplasty for rheumatoid arthritis. A Merchant view of the patella is shown in Figure 16. What is the most likely cause of her pain?

Detailed Explanation
Patellar complications commonly occur after primary total knee arthroplasty; therefore, proper component positioning is critical in obtaining a successful result. This patient has lateral tilting and subluxation of the patellar component. Internal rotation of the femoral component has the most deleterious effect on patellar tracking. Lateral placement of the femoral component, medial placement of the patellar component, and external rotation of the tibial component have beneficial effects on patellar tracking. Elevation of the joint line, if not excessive, should not impact patellar tracking. Rand JA: Patellar resurfacing in total knee arthroplasty. Clin Orthop 1990;260:110-117.
Question 65
High Yield
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?

Explanation
Synovectomy of the knee prior to loss of articular cartilage has been shown to consistently relieve pain in patients with rheumatoid arthritis. Partial knee replacement will not arrest the process of joint destruction. Osteotomy of the hip has not been found to be a successful procedure in patients with rheumatoid arthritis. Hip arthrodesis should not be considered because of the multiarticular involvement in patients with rheumatoid arthritis. Core decompression of the hip has not been shown to save the femoral head because the necrosis appears to occur simultaneously with the inflammatory joint process. Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Question 66
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
The rapidly increasing prevalence of infection from Staphylococcus epidermidis has made this the most frequently cultured organism. In most patients, the infection occurred intraoperatively, thereby resulting in a chronic infection if not detected within the first 6 weeks after surgery. Irrigation of the joint may be successful during this time in 60% of patients, but the most successful treatment is extirpation for 6 weeks, followed by delayed reimplantation. This approach may result in a salvage rate of as high as 90% in some patients. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Question 67
High Yield
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 68
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include

Explanation
The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure. Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238. Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 69
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of


Explanation
Because the patient has sustained a tarsometatarsal injury with midfoot sag, the treatment of choice is a tarsometatarsal arthrodesis. The cause of his flatfoot deformity is secondary to the tarsometatarsal injury and not from posterior tibialis tendon deficiency. Lateral column lengthening, double arthrodesis, and calcaneal osteotomy are not indicated. Although open reduction and internal fixation may be performed late when arthritis is present, these procedures are less likely to succeed. Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 70
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?

Explanation
Recurrent posterolateral rotatory instability of the elbow is difficult to diagnose. Such instability can be demonstrated only by the lateral pivot-shift test. The cause for this condition is laxity of the ulnar part of the lateral collateral ligament, which allows a transient rotatory subluxation of the ulnohumeral joint and a secondary dislocation of the radiohumeral joint. The annular ligament remains intact, so the radioulnar joint does not dislocate. Treatment consists of surgical reconstruction of the lax ulnar part of the lateral collateral ligament. The anterior band is the most important part of the medial collateral which is lax in valgus instability of the elbow. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 71
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 72
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 73
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 74
High Yield
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
Numerous causes of tarsal tunnel syndrome have been reported. The most favorable outcomes from release of the tarsal tunnel are in patients who have a space-occupying lesion (eg, ganglion, lipoma, or neurilemoma). While electrodiagnostic studies may be abnormal preoperatively, there is a low correlation between clinical outcome and electromyographic findings. Intrinsic weakness is a late finding in long-standing nerve dysfunction. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 75
High Yield
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?


Detailed Explanation
The patient has an abnormal neurologic exam as shown by the abnormal abdominal reflexes. Furthermore, she has a significant curve and is younger than age 10 years. These findings are not consistent with idiopathic scoliosis. MRI will best rule out syringomyelia or an intraspinal tumor. Bracing and surgery are not indicated for this small curvature prior to obtaining an MRI scan. Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
Question 76
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 77
High Yield
Which of the following is the most relevant clinical factor in the maturation assessment of an adolescent female athlete contemplating anterior cruciate ligament (ACL) reconstruction?
Detailed Explanation
Age of menarche is the most accurate clinical factor to assess the degree of skeletal maturity in the female athlete. Such an assessment is necessary prior to ACL reconstruction in a skeletally immature female because of the risk of damage to the distal femoral and proximal tibial physes. Height of an older male sibling is not relevant to the female athlete. Parental height and recent change in shoe size are only moderately useful in predicting final growth, and hence, skeletal maturity. The presence of breast buds occurs early in adolescent development; therefore, its presence suggests a high likelihood of future growth. Micheli LJ, Foster TE: Acute knee injuries in the immature athlete. Instr Course Lect 1993;42:473-481. Stanitski CL: Anterior cruciate ligament injury in the skeletally immature patient: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:146-158.
Question 78
High Yield
In a patient who has rheumatoid arthritis with acetabular protrusion, what is the best biomechanical position for the cup with respect to the preoperative center of rotation?

Explanation
Acetabular protrusion in patients with rheumatoid arthritis moves the center of hip rotation medially and posteriorly. Positioning of the acetabular component in a patient with protrusion is best accomplished in the normal (anterior and inferior) position and not in a protruded position. This has been shown both clinically and in a finite-element analysis. Any medial positioning will produce impingement of the prosthesis neck on the rim, and superior placement produces improper hip mechanics. Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of acetabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am 1983;65:495-499.
Question 79
High Yield
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?

Detailed Explanation
Severely displaced acromioclavicular injuries disrupt the deltotrapezial fascia and muscular origin in addition to the ligaments (acromioclavicular and coracoclavicular or trapezoid and conoid). When the deltoid is still attached to the clavicle, an isometric shoulder shrug will tend to reduce the displacement. When the deltoid is detached but the trapezius is attached, this manuever will increase the deformity and surgery may be indicated.
Question 80
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of


Explanation
The best results after dislocations of the tarsometatarsal joints are seen with anatomic reduction; this is best achieved by open reduction and maintained with internal fixation with either pins or screws. Open reduction provides a means of debriding small bony fragments from the joint and allowing direct inspection of the reduction. Associated crush or shearing fractures of the cuboid or tarsal navicula are signs that suggest a Lisfranc injury. Because patients can function quite well despite the development of arthrosis in the Lisfranc joint, primary arthrodesis is not indicated in the management of this injury. Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123. Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Question 81
High Yield
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?

Detailed Explanation
Ample evidence supports an increased rate of degenerative arthritis in the ACL-deficient knee. Several variables play a role in the development of the arthritis, but the integrity of the meniscus has been shown to be the single most important factor. O'Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118. Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
Question 82
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include


Explanation
IV broad-spectrum antibiotics should be administered for 7 days. This regimen, when compared to fragment removal or other antibiotic regimens, has been shown to reduce the incidence of spinal infections and reduce the need for metallic fragment removal with perforation of a viscus. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 83
High Yield
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?


Explanation
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis. Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Question 84
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 85
High Yield
Figures 47a and 47b show the CT scans of a patient who reports persistent pain in the sinus tarsi following a fall. The avulsion fracture fragment remains attached to what ligament?
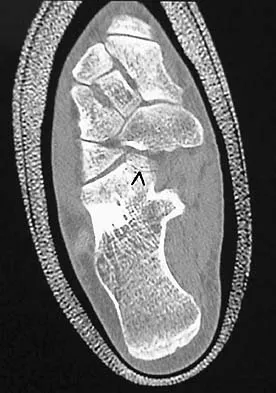

Explanation
The bifurcate ligament bifurcates to connect the dorsal aspect of the anterior process of the calcaneus to both the cuboid and the navicular. Inversion injuries on the side of the foot can result in avulsion fractures (arrow) of the anterior process of the calcaneus. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, p 192.
Question 86
High Yield
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?

Explanation
The peroneus tertius, although absent in 10% of the population, originates on the distal third of the extensor surface of the fibula and inserts onto the base of the fifth metatarsal, possibly extending to the fascia over the fourth interosseous space. The muscle is located in the anterior compartment of the leg and is innervated by the deep peroneal nerve. The tendon produces dorsiflexion and eversion when walking and can be used as an insertion point during tendon transfers to assist dorsiflexion. This tendon is peculiar to humans and is a proximally migrated deep extensor of the fifth toe. Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle. Clin Anat 2006;19:611-614. Williams PL, Bannister LH, Berry MM, et al (eds): Gray's Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Question 87
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner's syndrome?

Explanation
The sympathetic chain approaches the lateral border of the longus coli muscle at C6 and is more vulnerable to injury at this level. Injury to the chain will cause Horner's syndrome, usually seen as unilateral ptosis.
Question 88
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
Most authors recommend an initial trial of nonsurgical management in the treatment of adult-acquired flatfoot deformity such as posterior tibial tendon dysfunction. Chao and associates found that there is high patient satisfaction with ankle-foot orthoses and UCBL-type inserts in elderly patients with a relatively sedentary lifestyle. Alternatively, there was a higher dissatisfaction rate in young active patients, those with balance and ambulation difficulties (Parkinson's, severe arthritis of the hip or knee), and patients with inflammatory systemic disorders. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Question 89
High Yield
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of


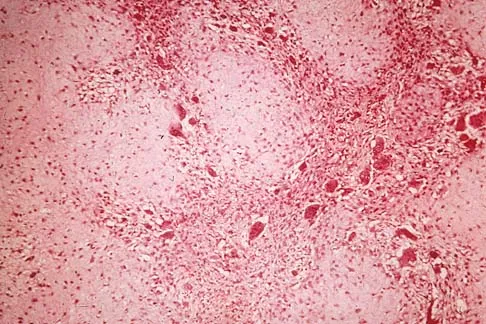
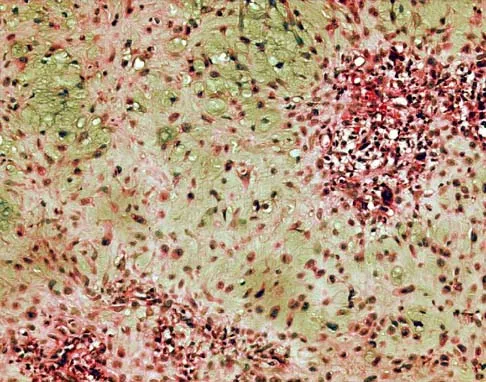
Explanation
The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially. Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Question 90
High Yield
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of


Detailed Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 91
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?



Explanation
Dickman and associates classified injuries of the transverse atlantal ligament into two categories. Type I injuries are disruptions through the substance of the ligament itself. Type II injuries render the transverse ligament physiologically incompetent through fractures and avulsions involving the tubercle of insertion of the transverse ligament on the C1 lateral mass. Type I injuries are incapable of healing without supplemental internal fixation. Type II injuries can be treated with a rigid cervical orthosis with a success rate of 74%. Surgery may be required for type II injures that fail to heal with 3 to 4 months of nonsurgical management. Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Question 92
High Yield
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
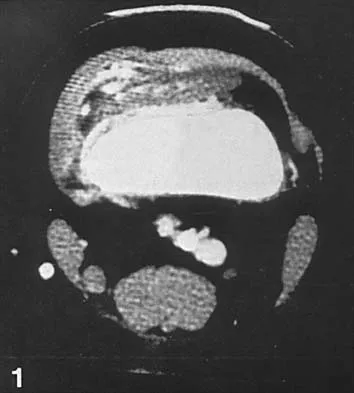
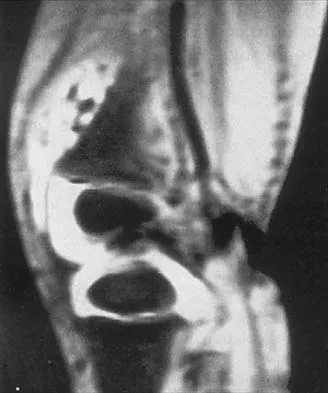
Explanation
In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
Question 93
High Yield
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?

Explanation
In a review of the practical applications of antibiotic-loaded bone cement for the treatment of the infected total joint arthroplasties, Hanssen and Spangehl described commercially available antibiotic-loaded bone cement as low-dose antibiotic cements. These cements generally contained 0.5 g of either tobramycin or gentamicin per 40 g of cement. They are indicated for use in prophylaxis and not for treatment of infected total joint arthroplasties. High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics. Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Question 94
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?

Explanation
The patient has a posterior dislocation. The radiograph reveals marked internal rotation, but fails to show whether the humeral head is posteriorly displaced. Therefore, an axillary radiograph should be obtained to help confirm the diagnosis. Transverse view CT or MRI scans also may be useful. The other studies will not help confirm the diagnosis. In addition to a direct posterior blow, a shoulder dislocation may be caused by a seizure disorder or electrocution. Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Question 95
High Yield
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?

Detailed Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 96
High Yield
A 6-year-old boy with spastic diplegic cerebral palsy has a crouched gait. Examination reveals hip flexion contractures of 15 degrees and popliteal angles of 70 degrees. Equinus contractures measure 10 degrees with the knees extended. Which of the following surgical procedures, if performed alone, will worsen the crouching?

Detailed Explanation
Children with spastic diplegic cerebral palsy often have contractures of multiple joints. Because the gait abnormalities can be complex, isolated surgery is rarely indicated. To avoid compensatory deformities at other joints, it is preferable to correct all deformities in a single operation. Isolated heel cord lengthening in the presence of tight hamstrings and hip flexors will lead to progressive flexion at the hips and knees, thus worsening a crouched gait. Split posterior tibial tendon transfer is used for patients with hindfoot varus, which is not present in this patient. Gage JR: Distal hamstring lengthening/release and rectus femoris transfer, in Sussman MD (ed): The Diplegic Child. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 324-326.
Question 97
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 98
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
In a recent study on restoration of motion following zone I and zone II flexor tendon repairs in children, age was found to have no effect on the results of zone II tendon repairs. Early passive motion offered no better results than immobilization for 3 weeks. Immobilization for more than 4 weeks correlated with poorer results.
Question 99
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
The radial nerve is only 4 mm from the anterolateral portal, while the median nerve is 11 mm away from the anteromedial portal. The ulnar nerve is only at risk on the medial side of the elbow. Anterior and posterior interosseous nerves are more distal within the forearm and are not in danger during portal placement. O'Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Question 100
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
