Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?

Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites. Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 2
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?




Explanation
Multiple hereditary exostosis and enchondroma commonly present as multiple lesions in the hand. Multiple hereditary exostosis consists of cartilage capped bony exostoses arising from the metaphyseal end of rapidly growing bones. Osteosarcoma and chondrosarcoma rarely appear as multiple lesions. Fracture callus can exhibit enchondral ossification that is usually circumferential, but the radiographic findings are not consistent with fracture. Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Question 3
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
The mainstay of early treatment of open fractures includes irrigation and debridement. Prior to the development of antibiotics, this was traditionally accomplished with some form of detergent irrigation. Antibiotic irrigation has been in favor more recently but has mixed scientific results related to its use. Results of at least one major study show the use of a nonsterile liquid soap additive (castile soap) is at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, and shows a significant decrease in problems with soft-tissue healing.
Question 4
High Yield
What nerve is at greatest risk when developing the superficial plane between the tensor fascia lata and sartorious during the anterior (Smith-Peterson) approach to the hip?
Explanation
The lateral femoral cutaneous nerve pierces the fascia between the tensor fascia lata and the sartorius approximately 2.5 cm distal to the anterosuperior iliac spine and is at risk when the interval is defined. The superior gluteal and femoral nerves define the internervous plane between the tensor fascia lata and the sartorius and are not at risk for injury. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 302-316.
Question 5
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
Bisphosphonates are a class of drugs that act to inhibit osteoclast resorption of bone. It has been shown that patients with multiple myeloma who are treated with bisphosphonates have fewer pathologic fractures than patients who are not treated with bisphosphonates. Vitamin D and calcium are considered appropriate for patients who are at risk for the development of osteoporosis, as is estrogen in selected women. Chelating agents and progesterones have no use in the treatment of patients with multiple myeloma or osteoporosis. Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Question 6
High Yield
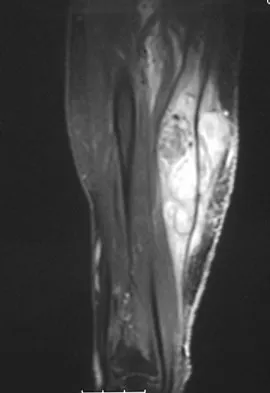
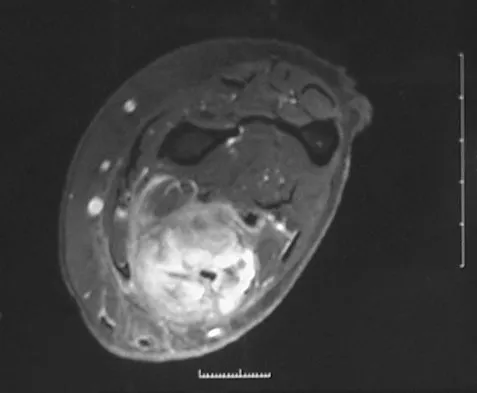
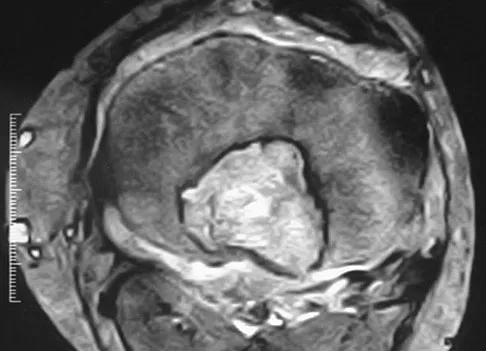
Figure 8a shows the clinical photograph of an 83-year-old woman who has an enlarging left forearm mass. MRI scans are shown in Figures 8b and 8c. What is the next most appropriate step in management?

Explanation
Any large (greater than 5 cm), deep, heterogeneous mass in the extremities should be considered a sarcoma until proven otherwise. Sarcomas are rare, and without a high index of suspicion, the lesions may be misdiagnosed or there may be a delay in diagnosis. Needle biopsies can obtain sufficient tissue for diagnosis and are associated with less morbidity than open biopsy. Marginal resections or excisional biopsies should be reserved for a few select benign lesions and locations. Damron TA, Beauchamp CP, Rougraff BT, et al: Soft-tissue lumps and bumps. Instr Course Lect 2004;53:625-637.
Question 7
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?

Explanation
Without stabilization, progressive kyphosis will develop between the spine and pelvis. The kyphosis progresses to the point that the child must use his or her hands to support the trunk, and therefore is unable to use his or her hands for other activities. Neck extension contracture does not usually develop. Neurologic deficit, including sexual dysfunction, is generally present at birth and static. Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Question 8
High Yield
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Question 9
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination. Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16. Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27. Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546. Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Question 10
High Yield
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
The musculocutaneous nerve travels through the conjoined tendon approximately 8 cm distal to the tip of the acromion. The musculocutaneous nerve innervates the biceps muscle and the bracialis muscle, both of which are responsible for elbow flexion. Shoulder flexion is facilitated by the anterior fibers of the deltoid muscle (axillary nerve) and the supraspinatus muscle (suprascapular nerve). The subscapular muscle facilitates internal rotation of the shoulder (upper and lower subscapularis nerve). Shoulder abduction is performed by the deltoid muscle (axillary nerve), and forearm pronation is facilitated by the pronator teres (median nerve). Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Question 11
High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?

Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 12
High Yield
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 13
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 14
High Yield
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
In review of 154 patients with nonrhabdomyosarcoma, Rao reported that histologic grade, tumor invasiveness, and adequate surgical margin were the most important prognostic factors. Histologic subtype, use of adjuvant chemotherapy, and patient age were not as important. Size related to degree of invasiveness was not statistically significant. Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531. Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 15
A 12-year-old girl has scoliosis at T5-T10 that measures 62 degrees. A clinical photograph of the axilla is shown in Figure 56. Management should consist of

Explanation
Neurofibromatosis type 1 (NF-1) is an autosomal-dominant disorder affecting about 1 in 4,000 people. NF-1 causes tumors to grow along various types of nerves and affects the development of non-nervous tissues, such as bone and skin. The gene for NF-1 is located on the long arm of chromosome 17 and codes the protein neurofibromin. Research indicates that NF-1 acts as a tumor-suppressor gene and, as such, plays an important role in the control of cell growth and differentiation. Axillary and inguinal freckling is considered a good diagnostic marker for NF-1. The hyperpigmented spots that measure from 2 mm to 4 mm may be congenital, but these typically appear and increase later in life. Scoliosis is the most common musculoskeletal disorder of NF-1. The curves are frequently dystrophic, kyphotic, and have a high risk of pseudarthrosis following spinal fusion. Anterior and posterior spinal fusion with rigid posterior segmental instrumentation is the treatment of choice. Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Question 16
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Explanation
Osteochondritis dissecans of the capitellum is seen most commonly in adolescent athletes. It should be distinguished from osteochondrosis of the capitellum (Panner's disease), a self-limiting condition seen in younger patients. Lesions are graded I through V based on radiographic and arthroscopic appearance. Grade I lesions show intact but soft cartilage. Grade II lesions show fissuring of the overlying cartilage. Grade III lesions show exposed bone or an attached osteoarticular flap that is not loose. Grade IV lesions show a loose but nondisplaced osteoarticular flap. Grade V lesions show a displaced fragment. Simple excision of the loose osteoarticular flap is the treatment of choice for grade IV and V lesions. More complex procedures such as drilling of the in situ lesion, bone grafting, or internal fixation are associated with significantly worse results. While some authors advocate abrasion chondroplasty, the long-term benefits of the procedure are yet to be proven. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 17
High Yield
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?


Explanation
The images show an epiphyseal lesion. The MRI scan shows extensive bone edema surrounding the lesion, consistent with chondroblastoma. Histology shows polygonal chondroblasts in a cobblestone-like pattern and areas of calcification consistent with chondroblastoma. Although some giant cells are seen, the age of the patient and the polygonal chondroblasts differentiate this lesion from giant cell tumor. Clear cell chondrosarcoma is an epiphyseal lesion that occurs in an older population, and the cells have clear cytoplasm. This lesion is not producing bone on imaging or histologic specimen, eliminating osteosarcoma. Tuberculous septic arthritis can be an epiphyseal lesion, but granulomas would be seen on histology. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 18
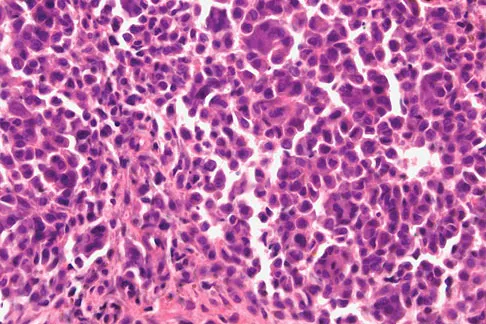
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of


Explanation
The histology shows small round blue cells that are uniform in appearance; these findings are consistent with Ewing's sarcoma. The MRI scan shows infiltration of the marrow and a large surrounding soft-tissue mass. Based on these findings, the management of choice is systemic chemotherapy. Local control of the primary lesion is addressed by either surgical resection or radiation therapy or a combination of the two after the patient receives systemic chemotherapy. The clinical, radiographic, and histologic presentation of Ewing's sarcoma often can be confused with osteomyelitis. The histology shows an absence of inflammatory cells. Grier HE: The Ewing family of tumors: Ewing's sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Question 19
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?

Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 20
High Yield
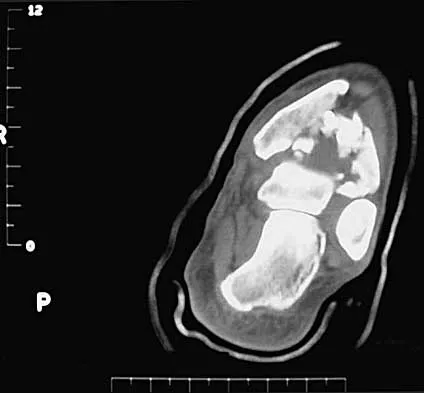
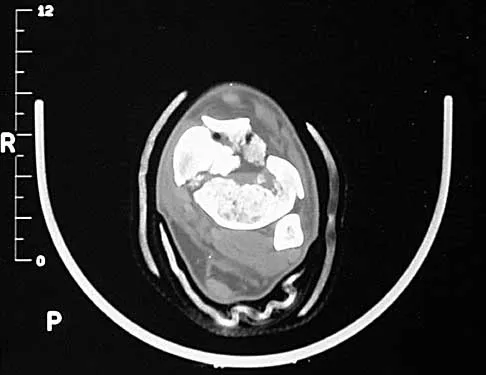
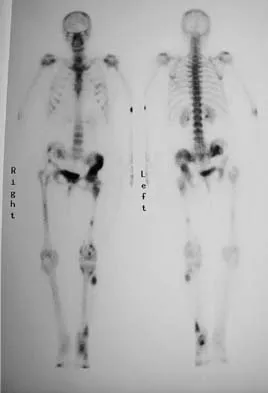
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of



Detailed Explanation
The studies reveal significant heterotopic ossification that appears to be mature. Following resection, the most reliable way to prevent recurrence is with low-dose external-beam radiation therapy. Bisphosphonate therapy can be considered; however, when terminated, heterotopic bone may reform. Heterotopic ossification is unrelated to the patient's endocrine status and is not associated with any metabolic abnormalities. Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Question 21
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
The patient sustained an injury to the long thoracic nerve, which supplies the serratus anterior. Branches of C5 and C6 enter the scalenus medius, unite in the muscle, and emerge as a single trunk and pass down the axilla. On the surface of the serratus anterior, the long thoracic nerve is joined by the branch from C7 and descends in front of the serratus anterior, providing segmental innervation to the serratus anterior.
Question 22
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.
Question 23
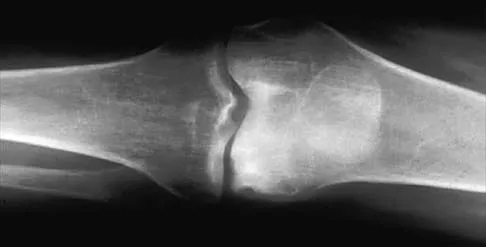
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of



Explanation
The radiographs reveal a malunited distal fibular fracture with shortening. Because there appears to be an adequate cartilage space within the ankle joint, the role of reconstruction would be to prevent arthrosis and the need for ankle arthrodesis, as well as to decrease symptoms. The treatment of choice is restoration of fibular length, alignment, and rotation with osteotomy plating, and bone grafting as needed. There is no indication for ligament reconstruction of a mechanically stable ankle, and tibial shortening osteotomy will not assist in correcting the deformity. Cast immobilization may assist with improvement of symptoms but will not correct the overall process. Determination of fibular length is best done by comparing the talocrural angle of the injured side with the uninjured side. The goal is to perfectly reduce the talus in the ankle mortise. Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713. Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Question 24
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?

Explanation
The pedigree documents involvement of male offspring only, and it also shows transmission through an uninvolved female carrier. This inheritance pattern is most consistent with a x-linked recessive inheritance. It would be inconsistent with a dominant inheritance pattern unless there was incomplete penetrance. Autosomal-recessive inheritance would be possible only if the family member labeled II.F was also a carrier of the same gene; however, this is unlikely. Mitochondrial inheritance is possible, but as with autosomal patterns, mitochondrial inheritance normally affects both male and female offspring. It is transmitted only through the maternal line.
Question 25
High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Detailed Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 26
A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?

Explanation
Proprionobacter acnes has been a leading cause of indolent shoulder infections. During shoulder arthroscopy, the arthroscopic fluid may actually dilute the shoulder preparation and lead to a higher rate of infection during subsequent mini-open rotator cuff repair surgery. The remaining bacteria listed are rarely associated with shoulder infections after arthroscopy. Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 27
High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of


Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 28
High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Detailed Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 29
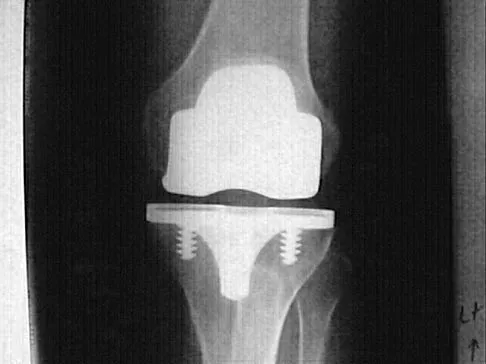
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 30
High Yield
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Detailed Explanation
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Question 31
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?


Explanation
An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 32
High Yield
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?

Detailed Explanation
The work-up for a patient with an unknown primary lesion that is metastatic to bone includes a search for the primary tumor and other sites of metastasis. This involves conducting a thorough history and physical examination, appropriate laboratory studies, bone scan, chest radiograph, and CT of the chest, abdomen, and pelvis. In women, a mammogram may be indicated. CT of the brain is not necessary in the early stages of a metastatic work-up. Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Question 33
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?

Explanation
Compression of the suprascapular nerve by a ganglion cyst is a well-documented cause of pain and weakness in the shoulder. Isolated involvement of the infraspinatus indicates that the area of entrapment is at the spinoglenoid notch and not the suprascapular notch. The majority of ganglion cysts found in the shoulder are related to tears of the labrum. When such a compressive lesion is found, decompression can be accomplished through either an open or arthroscopic approach. Several authors have shown the value of arthroscopy in the treatment of this condition. It has been shown that it is technically possible to decompress a paralabral ganglion cyst using arthroscopy; this method is usually followed by repair of the torn labrum. Alternatively, arthroscopic repair of the labrum can be performed and the cyst may be aspirated at the time of surgery. Open cyst excision through a posterior approach is also an acceptable method of treatment. Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114. Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Question 34
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 35
High Yield
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 36
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?

Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding. Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432. Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23. Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Question 37
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?




Explanation
Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients. Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 38
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
The plantar intrinsic muscles are divided into four layers with respect to depth from the plantar fascia. They are (from superficial to deep): 1) abductor hallucis, flexor digitorum brevis, abductor digiti minimi; 2) quadratus plantae, lumbricals; 3) flexor digiti minimi, flexor hallucis brevis, adductor hallucis brevis; and 4) dorsal and plantar interosseous muscles. The flexor hallucis brevis and adductor hallucis brevis originate from the midtarsal bones, encompass the sesamoids, and insert into the base of the proximal phalanx. The adductor hallucis brevis consists of two muscle bellies forming a conjoined tendon and inserting into the lateral portion of the proximal phalanx and the lateral sesamoid. The adductor hallucis brevis is stronger than the abductor hallucis brevis, which may contribute to hallux valgus. The flexor digitorum minimi travels under the fifth metatarsal, arising at the base and inserting into the lateral base of the fifth proximal phalanx.
Question 39
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?



Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 40
High Yield
What structure is most at risk with anterior penetration of C1 lateral mass screws?
Detailed Explanation
Posterior screw fixation of the upper cervical spine has gained a great deal of popularity due to its stable fixation, obviating the use of halo vest immobilization, and its high fusion rates. The use of screws in this location, however, has introduced a whole new set of potential complications. Vertebral artery injury is one of the most feared complications associated with screws in the C1/C2 region. This structure, however, is lateral and posterior at the C2 level and then penetrates the foramen transversarium of C1 to lie cephalad to the arch of C1 before entering the foramen magnum. It is the internal carotid artery that lies immediately anterior to the arch of C1 that is particularly at risk by anterior penetration of C1 lateral mass or C1-C2 transarticular screws as demonstrated by Currier and associates. The internal carotid artery lies posterior to the pharynx. The external carotid artery and the glossopharyngeal nerve are not at risk with this method of fixation. Currier BL, Todd LT, Maus TP, et al: Anatomic relationship of the internal carotid artery to the C1 vertebra: A case report of cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Spine 2003;28:E461-E467. Grant JC: Grant's Atlas of Anatomy, ed 6. Baltimore, MD, Williams & Wilkins, 1972.
Question 41
High Yield
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 42
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient's ability to heal the wound postoperatively?
Explanation
Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status. A transcutaneous oxygen level should be greater than 40 mm Hg for healing. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Question 43
Significant anterior tibial translation occurs during which of the following rehabilitation exercises?
Explanation
Terminal non-weight-bearing knee extension exercises from 60 degrees to 0 degrees of flexion increase anterior tibial translation. It is for this reason that this type of exercise should be avoided in the early phase of rehabilitation following anterior cruciate ligament reconstruction so as not to place a tensile strain on the graft. The other rehabilitation exercises either lead to posterior tibial translation in relation to the femur or have no significant effect on tibial translation. Grood ES, Suntay WJ, Noyes FR, et al: Biomechanics of the knee extension exercise: Effect of cutting the anterior cruciate ligament. J Bone Joint Surg Am 1984;66:725-734. Lutz GE, Palmitier RA, An KN: Comparison of tibiofemoral joint forces during open-kinetic-chain and closed-kinetic-chain exercises. J Bone Joint Surg Am 1993;75:732-739.
Question 44
High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 45
Stiffness relates the amount of load applied to a structure like a long bone or an intramedullary nail to the amount of resulting deformation that occurs in the structure. What is the most important material property affecting the axial and bending stiffness of a structure?
Explanation
The amount of deformation resulting in response to an applied load depends on the stress distribution that the load creates in the structure and the stress versus strain behavior of the material that makes up the structure. Axial and bending loads create stress distributions that involve normal stresses and normal strains. Although all five responses are indeed material properties, only one, elastic modulus, relates normal stresses to normal strains. In fact, axial and bending stiffness are directly proportional to modulus, so that a nail made from stainless steel will have nearly twice the stiffness of a nail made from titanium alloy (because their respective elastic moduli differ by about a factor of two). Hayes WC, Bouxsein ML: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 74-82. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 159-165.
Question 46
High Yield
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of

Explanation
The findings are classic for a pectoralis major tendon avulsion. Deformity of the anterior axillary fold is a classic finding, and ecchymosis down the arm suggests that the injury is at the humeral attachment rather than at the musculotendinous junction. Good external rotation strength indicates that function in the supraspinatus and infraspinatus has been preserved. The treatment of choice for a tendon avulsion in a young individual is early surgical repair. Conversely, if the injury is within the muscle or at the musculotendinous junction, initial nonsurgical management is recommended. If the location of the injury cannot be determined by physical examination, then MRI of the pectoralis major can be helpful. Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 47
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
The superficial peroneal nerve, which is adjacent to the location of the lateral arthroscopic portal is most commonly injured. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 48
In the upright standing position, approximately what percent of the vertical load is borne by the lumbar spine facet joints?

Explanation
Direct measurement and finite element modeling results show that approximately 20% of the vertical load is borne by the posterior structures of the lumbar spine in the upright position. Adams MA, Hutton WC: The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980;62:358-362.
Question 49
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?

Explanation
The MRI scan shows an acute complete tear of the posterior cruciate ligament. No evidence is seen of a quadriceps tendon rupture, a tibia fracture, or a bone contusion. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 50
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?




Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 51
High Yield
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 52
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 53
High Yield
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of

Detailed Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 54
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?

Explanation
Chronic anterior inferior tibiofibular ligament sprains can lead to thickening and synovitis that catches or impinges dorsiflexion; patients often note painful clicking with dorsiflexion eversion. The other structures are not affected by this injury. Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH: Syndesmosis sprains of the ankle. Foot Ankle 1990;10:325-330. Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50. Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Question 55
High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?

Detailed Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 56
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
Necrotizing fasciitis is an aggressive and rapidly spreading soft-tissue infection, usually caused by group A beta-hemolytic Streptococcus pyogenes. Presentation is typical of a rapidly ascending cellulitis, recalcitrant to antibiotic treatment. Differentiation between cellulitis and impetigo is difficult, and success depends on a high level of suspicion. The skin and subcutaneous tissues are affected, with sparing of the muscles. Septic shock and multi-organ system failure can be fatal. Treatment is aggressive surgical debridement with broad-spectrum antibiotics. Repeat irrigation and debridement may be necessary. Hyperbaric oxygen studies have shown inconsistent results. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 199-205.
Question 57
High Yield
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 58
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of

Explanation
Because the patient has a hallux valgus with increased intermetatarsal and hallux valgus angles and advanced degenerative arthritis of the joint, arthrodesis of the first metatarsophalangeal joint will provide the most predictable pain-free result. An attempt to correct the bunion with a bunionectomy or osteotomy would most likely fail. The hallux valgus and advanced degenerative changes put the foot beyond the indications for a cheilectomy. Long-term results with silicone arthroplasty have been disappointing. Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 59
High Yield
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?



Explanation
Chondrosarcomas associated with diffuse bone lesions (enchondromas) are characteristic of Ollier's disease. When accompanied by subcutaneous masses (hemangiomas), the condition is called Maffucci's syndrome. Multiple hereditary exostosis is characterized by diffuse osteochondromas. McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia with cafe-au-lait spots and precocious puberty. Neurofibromatosis can have associated bone lesions but is not associated with chondrosarcomas. Sun TC, Swee TC: Chondrosarcoma in Maffucci's syndrome. J Bone Joint Surg Am 1985;67:1214-1219. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Question 60
High Yield
A patient undergoes a proximal tibial resection that is reconstructed with a fresh frozen osteoarticular allograft. Eleven months later, the graft is retrieved. Histologically, the articular cartilage and subchondral bone retrieved would be expected to show evidence of
Explanation
Osteoarticular allografts are devoid of host chondrocytes but do contain "mummified" cellular debris left over from donor processing. The cartilage architecture is preserved in the first 2 to 3 years after transplantation. The articular surface is covered with a pannus of fibrocartilage maintaining the joint space radiographically; this pannus later contains islands of fibrocartilage containing host mesenchymal stem cells. Degenerative changes to the joint surface occur earlier and are more severe in joints that are unstable. Only with degenerative changes at the surface is there histologic evidence of subchondral revascularization. Often degenerative changes involving the articular cartilage reach the tidemark, but the tidemark itself remains structurally intact. Enneking WF, Campanacci DA: Retrieved human allografts: A clinicopathological study. J Bone Joint Surg Am 2001;83:971-986.
Question 61
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?



Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 62
High Yield
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 63
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?


Explanation
Osteoid osteoma is a round or oval, well-circumscribed lesion with a radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 64
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?

Explanation
Most soft-tissue sarcomas are treated with a combination of radiation therapy and wide resection. Rhabdomyosarcomas are an exception, where chemotherapy is included in all treatment plans. Chemotherapy for other soft-tissue sarcomas is controversial. Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Question 65
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
The median survival of patients after discovery of bone metastasis from primary lung carcinoma is shorter compared with other primary sites.
Question 66
High Yield
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?



Explanation
The radiographs reveal osteoarthritis and proximal humeral head migration. Integrity of the rotator cuff must be questioned based on these radiographic changes. The status of the rotator cuff is the most influential factor affecting postoperative function in shoulder hemiarthroplasty. The coracoacromial ligament provides a barrier to humeral head proximal migration in the face of a rotator cuff tear. The radiographs do not indicate significant humeral head or glenoid erosion. Acromioclavicular arthritis is often asymptomatic. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 67
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 68
A 1-year-old infant has the hand deformities shown in Figure 40. What pathologic process is the most likely cause of these deformities?

Explanation
Streeter's dysplasia is clearly related to rupture of the amnion in utero and is now most commonly referred to as premature amnion rupture sequence. The deformities arise from amniotic bands that wrap about protruding parts and from uterine packing because of the accompanying oligohydramnios. Clubfoot can develop as a result of the latter mechanism. Three limb involvement is most commonly seen, along with syndactyly. Treatment involves resection of bands and Z-plasty of skin. The disease is not genetic and has not been related to teratogen exposure or to iatrogenic influences such as amniocentesis. Developmental field disruption is not seen in this disease, and the growth potential of the involved parts is normal unless neurovascular disruption has arisen from band formation.
Question 69
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?

Explanation
Posttraumatic osteolysis of the distal portion of the clavicle is a condition that can be a complication of acute or repetitive trauma. The distal end of the clavicle is frayed and resorbed. Resorption may occur after weeks or months. The end of the clavicle may reconstitute over a period of months, or the acromioclavicular joint may remain widened. The differential diagnosis for distal clavicular erosion also includes rheumatoid arthritis, hyperparathyroidism, neoplastic destruction, cleidocranial dysplasia, and pyknodysostosis. Acutely, a type 2 acromioclavicular joint injury does not result in erosion or resorption of the clavicle. Periosteal sleeve injuries radiographically mimic acromioclavicular joint dislocation. Rickets occurs only in childhood.
Question 70
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?



Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
Question 71
High Yield
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
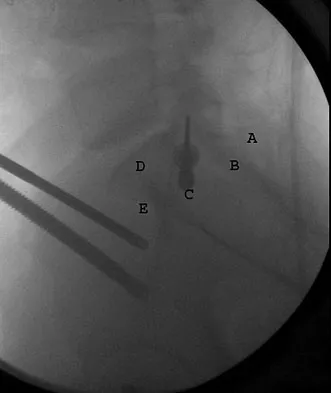
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 72
High Yield
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?


Explanation
The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically. Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Question 73
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 74
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
The patient has sustained a low-velocity, low-caliber gunshot wound to the foot. Because the injury occurred within a period of 8 hours, this is classified as a type I wound. Several studies support the use of surface debridement, cleansing, and sterile dressings as the treatment of choice. More aggressive measures are reserved for high-velocity injuries and shotgun injuries. Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31. Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Question 75
High Yield
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of


Detailed Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 76
High Yield
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?

Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 77
High Yield
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of

Explanation
Because the patient has a hallux valgus with increased intermetatarsal and hallux valgus angles and advanced degenerative arthritis of the joint, arthrodesis of the first metatarsophalangeal joint will provide the most predictable pain-free result. An attempt to correct the bunion with a bunionectomy or osteotomy would most likely fail. The hallux valgus and advanced degenerative changes put the foot beyond the indications for a cheilectomy. Long-term results with silicone arthroplasty have been disappointing. Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 78
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Both the AAOS and AdvaMed, the medical device manufacturer's trade organization, have written guidelines that address potential conflicts of interest regarding interactions between physicians and manufacturer's representatives when it comes to patients' best interest. The AAOS feels that the orthopaedic profession exists for the primary purpose of caring for the patient and that the physician-patient relationship is the central focus of all ethical concerns. When an orthopaedic surgeon receives anything of significant value from industry, a potential conflict of interest exists. The AAOS believes that it is acceptable for industry to provide financial and other support to orthopaedic surgeons if such support has significant educational value and has the purpose of improving patient care. All dealings between orthopaedic surgeons and industry should benefit the patient and be able to withstand public scrutiny. A gift of any kind from industry should in no way influence the orthopaedic surgeon in determining the most appropriate treatment for his or her patient. Orthopaedic surgeons should not accept gifts or other financial support with conditions attached. Subsidies by industry to underwrite the costs of educational events where CME credits are provided can contribute to the improvement of patient care and are acceptable. A corporate subsidy received by the conference's sponsor is acceptable; however, direct industry reimbursement for an orthopaedic surgeon to attend a CME educational event is not appropriate. Special circumstances may arise in which orthopaedic surgeons may be required to learn new surgical techniques demonstrated by an expert or to review new implants or other devices on-site. In these circumstances, reimbursement for expenses may be appropriate. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6, 9, 12-15. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf The Orthopaedic Surgeon's Relationship with Industry, in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. www.aaos.org/about/papers/ethics/1204eth.asp
Question 79
High Yield
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
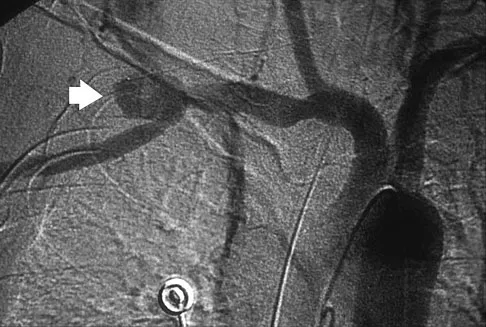
Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
Question 80
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?


Explanation
The history, examination, and radiographs are pathognomonic for Little League shoulder, a stress syndrome of the proximal humeral physis caused by overuse. Complete fracture rarely occurs, and recovery usually occurs with rest. Night pain is always a serious concern and further work-up is needed if the patient does not respond to activity modification. Occult instability is not a real concern in this patient, although it should be included in the differential diagnosis. Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Question 81
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 82
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
Shufflebarger and others have reported that the placement of anterior interbody structural support at the lumbosacral junction increases the overall construct stiffness and reduces the strain on posterior instrumentation, thereby reducing the risk of screw pull-out or fracture. The stiffness of the posterior instrumentation actually increases, whereas the actual strength of the instrumentation remains the same. Actual strain measured at an adjacent intervertebral disk to a fusion construct is expected to increase. Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393. Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Question 83
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



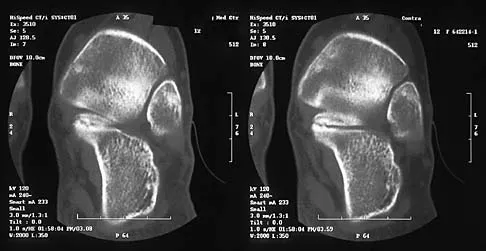
Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 84
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 85
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
Because the man is only recently removed from his injury and is judged capable of returning to work with some restrictions, the term that best describes his work status is temporary partial disability.
Question 86
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?

Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 87
High Yield
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 88
A 42-year-old woman reports that she has low back pain and had a transient loss of consciousness after falling off a horse. She denies having neck pain but notes that she was involved in a motor vehicle accident 2 years ago and had neck pain at that time. Examination reveals full range of motion of the neck and no localized tenderness. The neurologic examination is normal. A lateral radiograph of the cervical spine is obtained. Figures 41a and 41b show CT and MRI scans. What is the most likely diagnosis?


Explanation
The examination findings do not correlate with an acute injury (full range of cervical motion and the absence of pain). Radiographically, the fracture appears old based on the smooth contour of the fracture fragments and the absence of soft-tissue swelling. Flexion-extension radiographs can be obtained to determine potential instability; if present, stabilization and fusion should be considered. Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoid process: An experimental investigation. Clin Orthop 1975;108:127-137.
Question 89
High Yield
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?

Explanation
The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty. Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Question 90
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 91
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?

Explanation
The risk of Salmonella osteomyelitis is much greater in patients with sickle cell disease than the general population. The exact reason for this increased risk is still unclear, but it appears to be associated with an increased incidence of gastrointestinal microinfarcts and abscesses. Both Staphylococcus aureus and Salmonella have been mentioned as the most prevalent causative organisms. Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227. Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413. Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Question 92
High Yield
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of


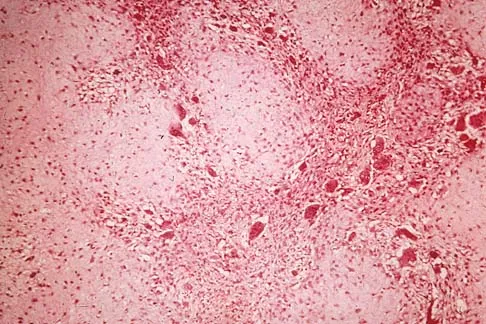
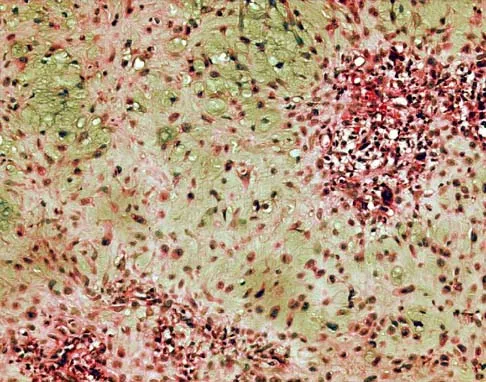
Explanation
The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially. Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Question 93
A 6-year-old boy with acute hematogenous osteomyelitis of the distal femur is being treated with intravenous antibiotics. The most expeditious method to determine the early success or failure of treatment is by serial evaluations of which of the following studies?

Explanation
Successful antibiotic treatment of osteomyelitis should lead to a rapid decline in the CRP. The CRP should decline after 48 to 72 hours of appropriate treatment. Imaging studies will take much longer to show resolution of bone infection. Unkila-Kallio L, Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Question 94
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of


Explanation
Because the patient has sustained a tarsometatarsal injury with midfoot sag, the treatment of choice is a tarsometatarsal arthrodesis. The cause of his flatfoot deformity is secondary to the tarsometatarsal injury and not from posterior tibialis tendon deficiency. Lateral column lengthening, double arthrodesis, and calcaneal osteotomy are not indicated. Although open reduction and internal fixation may be performed late when arthritis is present, these procedures are less likely to succeed. Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 95
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?

Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 96
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of



Explanation
The posttraumatic lumbar kyphotic deformity will not remodel and is likely to worsen with time because the central line of gravity lies anterior to the deformity and the ligamentous disruption will not heal. The worsening deformity also puts the patient at some risk for future neurologic damage. Ebraheim NA, Savolain ER, Southworth SR, et al: Pediatric lumbar seat belt injuries. Orthopedics 1991;14:1010-1013.
Question 97
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 98
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Long-term survivorship studies have attempted to clarify patient factors related to good outcomes in HTO. One particular study showed that a patient age of less than 50 years was related to good outcomes in those who had good preoperative knee flexion. The same study found no relation between HTO failure and the presence of postoperative infection or deep venous thrombosis. The presence of a lateral tibial thrust is a contraindication to performing this surgery. As expected, good patient selection is critical to obtaining good long-term results with HTO. Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 99
High Yield
A positive Froment sign indicates weakness of which of the following muscles?

Detailed Explanation
Thumb adduction is powered by the adductor pollicis (ulnar nerve). Testing involves having the patient forcibly hold a piece of paper between the thumb and radial side of the index proximal phalanx. When this muscle is weak or nonfunctioning, the thumb interphalangeal joint flexes with this maneuver, resulting in a positive Froment sign. The paper is held by action of the thumb flexion (flexor pollicis longus and flexor pollicis brevis; median innervated).
Question 100
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?

Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
