Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?

Detailed Explanation
The eccentric metaphyseal location, skeletal maturity, narrow zone of transition, and lack of symptoms suggest a benign process and are consistent with a healed nonossifying fibroma. These lesions typically fill in (ossify) with skeletal maturity, eventually remodeling and disappearing. Radiographic monitoring is indicated. Biopsy is not recommended unless the lesion changes radiographically. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393. Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Question 2
High Yield
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
The compaction of FDBA is faster than that of fresh-frozen bone. The maximal stiffness reached by both materials when tested was the same (55 MPa), but the FDBA required fewer impactions to achieve that stiffness. Because it is easier to impact, the FDBA may be mechanically more efficient than the fresh-frozen bone in surgical conditions. The brittleness of irradiated FDBA, caused by loss of the capacity to absorb energy in a plastic way, increases the compactness and stiffness of morcellized grafts. The failure rate of fusion in adolescent idiopathic scoliosis has been shown to be much higher in FDBA than in either iliac crest bone graft or composite autograft with demineralized bone matrix. There is a greater erosive surface response to allograft when compared to autograft or frozen allograft, with a larger number of osteoclast and osteoblast nuclei seen microscopically. Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand 2004;75:309-314. Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Question 3
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of


Explanation
The radiographs show increased density and reactive bone formation. A faint nidus can be seen on the radiograph but is obvious on the CT scan. The initial therapy for an osteoid osteoma should be oral anti-inflammatory drugs. A biopsy or SPECT bone scan is not indicated because the osteoid osteoma is clearly seen on the CT scan. If the patient fails to respond to nonsurgical therapy, CT-guided radiofrequency ablation or surgical excision is indicated depending on the anatomic location. Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 4
High Yield
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?

Explanation
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
Question 5
High Yield
A 42-year-old patient has had a fever and low back pain for several days. Laboratory studies show an elevated erythrocyte sedimentation rate and a WBC count of 9,500 mm3 with 75% neutrophils. A CT scan is shown in Figure 15. Examination will most likely reveal what other findings?

Detailed Explanation
The CT scan reveals a left-sided psoas abscess. Irritation of the saphenous division of the femoral nerve can cause paresthesias along the medial aspect of the knee. Pain is usually improved with hip flexion. Cellier C, Gendre JP, Cosnes J, et al: Psoas abscess complication Crohn's disease. Gastroenterol Clin Biol 1992;16:235-238.
Question 6
High Yield
An 18-year-old boy reports increasing pain with weight bearing on his right leg and at night. Examination reveals swelling around the right midcalf. Radiographs and an MRI scan are shown in Figures 13a through 13c, and a biopsy specimen is shown in Figure 13d. What is the preferred treatment?


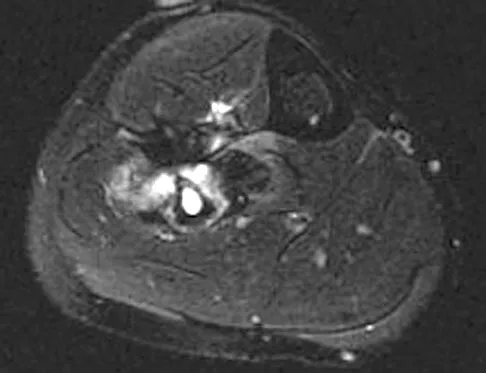
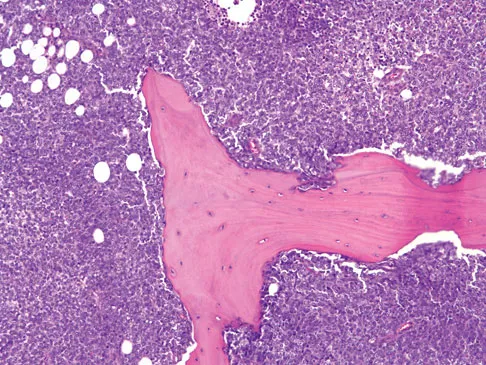
Explanation
The findings are consistent with Ewing's sarcoma. The radiographs reveal a lytic lesion in the diaphysis of the right fibula. There is elevation of the periosteum and evidence of a surrounding soft-tissue mass. The biopsy specimen shows diffuse small round blue cells surrounding the lamellar bone. It is the second most common malignant bone tumor in children. The most common treatment regimen consists of chemotherapy followed by surgical resection and/or radiation therapy. Surgical resection is employed when the lesion can be removed with wide margins and causes less morbidity than radiation therapy. McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 258.
Question 7
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 8
High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of

Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 9
High Yield
A 20-year-old patient has foot pain. A radiograph and T1-weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of


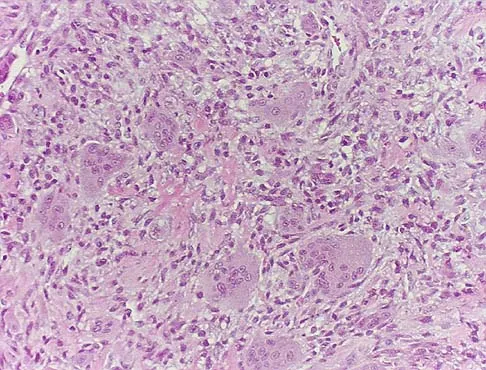
Explanation
Giant cell tumors occur near articular surfaces in young adults. The histology shows abundant giant cells with nuclei resembling the surrounding cells. Although the MRI scan shows soft-tissue involvement, curettage is still the preferred treatment. Chemotherapy is not necessary for benign lesions, and amputation is too aggressive. Cementation, phenol, and cryosurgery (liquid nitrogen) are all acceptable local adjuvants to curettage. Packing the cavity with bone graft rather than cement is also acceptable. Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Question 10
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 11
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 12
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?

Explanation
It is critical for graft isometry and knee stability that the femoral tunnel be placed as far posterior as possible on the lateral femoral condyle. Superiorly, the graft should be at the one o'clock position on the left knee. Resident's ridge is a false posterior shelf that often seems like the extreme posterior cortex. Abnormal tunnel placement results in a variety of complications, including an unstable knee, early graft failure, and joint stiffness. Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Question 13
Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?

Explanation
Sudden death during total hip arthroplasty has been reported. In a report from the Mayo Clinic, intraoperative death occurred during cemented total hip arthroplasty in 23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries. Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.
Question 14
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?

Explanation
The dual plate fixation construct is significantly stronger than single plate or "Y" plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis. Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Question 15
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?

Explanation
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Question 16
High Yield
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 17
High Yield
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
The traditional treatment of a reduced type II fracture is a halo vest. A 20-year-old man will tolerate a halo vest better than the elderly or women. Anterior screw fixation has gained increasing support; however, it too has risks and requires a significant learning curve. More recently, C1 lateral mass screws have become more popular. The long-term results and benefits have not yet been determined. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193. Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Question 18
Figure 53a shows the AP radiograph of a 70-year-old patient who is scheduled to undergo unicompartmental knee arthroplasty. Figure 53b shows the immediate postoperative radiograph, and the radiograph shown in Figure 53c, obtained 6 months after surgery, shows a medial tibial plateau fracture. The etiology of the fracture is best related to



Explanation
While all of the above may contribute to the etiology of a tibial plateau fracture following unicompartmental knee arthroplasty, the recent literature has clearly noted that pin placement for fixation of tibial resection guides is the most critical factor associated with a tibial plateau fracture following unicompartmental knee arthroplasty. Vince and Cyran suggest that fractures associated with unicompartmental knee arthroplasty might be avoidable by limiting the number and paying attention to the location of the pin holes that are created to secure the tibial resection guides. Brumby and associates suggest avoiding multiple guide pin holes in the proximal tibia for unicompartmental knee arthroplasty. They currently recommend the use of one centrally placed pin and an ankle clamp to stabilize the resection guide. Yang and associates note that a medial tibial plateau fracture in association with minimally invasive unicompartmental knee arthroplasty can be eliminated by avoiding fixation pins close to the medial tibial cortex. Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809-812. Yang KY, Yeo SJ, Lo NN: Stress fracture of the medial tibial plateau after minimally invasive unicompartmental knee arthroplasty: A report of 2 cases. J Arthroplasty 2003;18:801-803.
Question 19
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 20
High Yield
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include
Explanation
Unwitnessed spiral fractures should raise the possibility of child abuse, especially prior to walking age. With nonaccidental trauma being considered in the differential diagnosis, a skeletal survey is indicated to determine if there are other fractures in various stages of healing. Kempe CH, Silverman FN, Steele BF, et al: The battered-child syndrome. JAMA 1962;181:17-24.
Question 21
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?


Explanation
Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 22
High Yield
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 23
High Yield
A patient with no history of patellar instability sustains a traumatic lateral patellar dislocation. What structure most likely has been torn?

Detailed Explanation
Any of the above structures may be involved in a lateral patellar dislocation. However, biomechanic studies have found that the medial patellofemoral ligament is the major soft-tissue static restraint of lateral patellar displacement, providing at least 50% of this function. Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65. Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Question 24
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?

Explanation
Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Question 25
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk. Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 26
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
This child has the potential to walk and therefore should have all the contracted structures in the feet released as necessary to place the feet in a plantigrade position for fitting of ankle-foot orthoses. Physical therapy, manipulation, and casting may provide some benefit in a newborn with flexible feet but are not effective in an older infant with rigid clubfeet. Botulinum injections and tendon transfers are of no use because there are no muscles functioning below the knee. Tendon releases are more effective than tendon transfers in children with myelomeningocele. Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Question 27
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of

Explanation
Most patients with a significant recurrent neuroma will not obtain relief with conservative methods. Pain results from a stump neuroma at the weight-bearing area from too short of a resection of the nerve or from regrowth of the remaining nerve end. Although steroid injection may be helpful in localizing symptoms or providing temporary relief, it rarely cures a stump neuroma. Orthotics with a metatarsal pad will likely increase pressure and pain at the neuroma site. Physical therapy could temporize the symptoms but will not address the underlying problem. Similarly, bone decompression alone will not alter the location of the neuroma stump. Revision of the nerve to a more proximal level off of the weight-bearing area is the most likely method to succeed. A plantar approach facilitates identification and ability to revise the nerve to a more proximal level. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657. Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Question 28
Which of the following palpable bony landmarks is correctly matched with its corresponding vertebral level?

Explanation
The carotid tubercle is usually located at the level of C6. The angle of the mandible is at C1-C2; the hyoid is at C4; the superior portion of the thyroid cartilage is C4-C5; and the cricoid cartilage is at C6. Smith GW, Robinson RA: The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40:607.
Question 29
High Yield
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?

Explanation
The prognosis of Legg-Perthes disease in children younger than age 6 years is good. There is no indication that surgical treatment will improve the outcome. Range-of-motion exercises to prevent contracture may be helpful. Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Question 30
High Yield
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?

Explanation
A ganglion cyst compressing the suprascapular nerve results in poorly localized pain in the shoulder girdle. Sensation is intact, with weakness of external rotation and abduction. Supraspinatus and infraspinatus atrophy is often noted when viewed from behind. These cysts are typically associated with labral tears. Deltoid weakness is associated with an axillary nerve injury, and scapular winging results from injury to the long thoracic nerve. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 31
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of

Explanation
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis. Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Question 32
High Yield
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of


Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 33
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?

Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 34
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
Question 35
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 36
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?





Explanation
The radiograph reveals a metaphyseal lesion with some stippled mineralization suggesting a chondroid tumor. The bone scan shows increased uptake, beyond what is expected for a simple enchondroma, and beyond the limits of the lesion. The MRI sequences shows a lobular lesion on the T1- and T2-weighted (bright on the T2 sequence) images with inhomogeneous uptake of gadolinium; both findings are typical for a chondroid lesion. The history of pain, the positive bone scan, the age of the patient, the size of the lesion, and the central location (enostotic) of the lesion all suggest a malignant cartilage tumor. The images are not consistent with the other diagnoses. In particular, plasmacytoma is more uniformly bright on T2-weighted images and often has a negative bone scan. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-194.
Question 37
High Yield
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with

Explanation
The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival. Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587. Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Question 38
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?

Explanation
The classic MRI findings of osteomyelitis are a decrease in the normally high signal intensity of marrow on T1-weighted images and normal or increased signal intensity on T2-weighted images. This is the result of replacement of marrow fat by inflammatory cells and edema, which causes lower signal intensity than fat on T1-weighted images and higher signal intensity than fat on T2-weighted images. The addition of gadolinium to a T1-weighted sequence reveals increased signal intensity in the hyperemic marrow. Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 39
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?



Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 40
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of


Explanation
Because the patient has sustained a tarsometatarsal injury with midfoot sag, the treatment of choice is a tarsometatarsal arthrodesis. The cause of his flatfoot deformity is secondary to the tarsometatarsal injury and not from posterior tibialis tendon deficiency. Lateral column lengthening, double arthrodesis, and calcaneal osteotomy are not indicated. Although open reduction and internal fixation may be performed late when arthritis is present, these procedures are less likely to succeed. Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 41
High Yield
What structure provides the most static stability for valgus restraint in the elbow?
Detailed Explanation
The anterior band of the ulnar collateral ligament provides the greatest restraint to valgus stress in the elbow. The posterior band is taut in flexion and resists stress between 60 degrees and full flexion. The annular ligament stabilizes the radial head. The flexor/pronator mass are important dynamic stabilizers of the medial elbow. Ahmad CS, ElAttrache NS: Elbow valgus instability in the throwing athlete. J Am Acad Orthop Surg 2006;14:693-700. Regan WD, Korinek SL, Morrey BF, et al: Biomechanical study of ligaments around the elbow joint. Clin Orthop Relat Res 1991;271:170-179.
Question 42
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
Numerous surgical approaches have been used for thoracic diskectomy, including the most recent VATS. One of the first approaches described, posterior laminectomy, involves manipulation of the spinal cord, which the other approaches avoid. The posterior approach had dismal results, including further neurologic deterioration and even paralysis. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864. Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg 1983;30:577-605. Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Question 43
High Yield
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?

Explanation
The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement. Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748. Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Question 44
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had "burners" in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
The player's symptoms represent more than the mere "burner syndrome," which leads to unilateral symptoms that typically last less than 1 minute. Return to play following a burner is allowed following nonsurgical management and once the symptoms have subsided and the player exhibits normal strength and motion of the neck and upper extremities. This player has the history, symptoms, and examination findings that are consistent with cervical neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine. CT of the brain is indicated with a history of loss of consciousness or other symptoms suggestive of a concussion. Torg JS, Sennett B, Pavlov H, et al: Spear tackler's spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649. Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Question 45
High Yield
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?

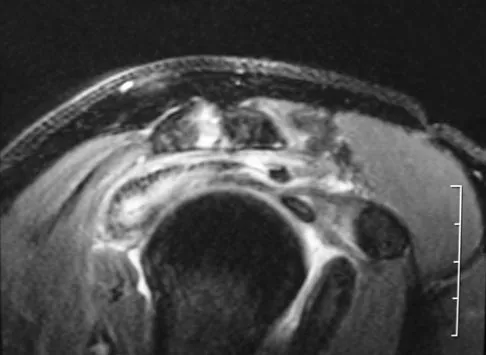
Explanation
The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Question 46
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of

Explanation
The MRI scan demonstrates a grade III MCL tear. Basic science and clinical studies have shown that nonsurgical management is preferred for MCL tears. Functional rehabilitation and early motion have led to consistently better results than has surgical repair.
Question 47
High Yield
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of

Detailed Explanation
Fractures of the hook of the hamate frequently are not identified in the acute phase. Because the fracture can be difficult to see on plain radiographs, the lack of findings can lead to a painful nonunion. A carpal tunnel view may show the fracture, but a CT scan will best detect the injury. Immobilization is the treatment of choice and will result in union in most patients unless the diagnosis is delayed. However, excision of the fragment may be necessary for patients who have nonunion, persistent pain, or ulnar nerve palsy. Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Question 48
High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 49
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Recent evidence has shown that the position of immobilization of the shoulder after a dislocation influences the reduction of the Bankart lesion. In an MRI study in patients who sustained an anterior dislocation, the Bankart lesion was reduced to the glenoid anatomically with the arm in 30 degrees of external rotation. Subsequently, a clinical follow-up study has shown a reduction in recurrence rates when the arm is immobilized in external rotation compared to internal rotation. Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Question 50
High Yield
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Detailed Explanation
Radiographic fusion success rates are best described as slightly rather than substantially improved. Hospital stay and time to fusion also are not substantially decreased. Use of BMP does eliminate the need for autograft harvest for anterior lumbar interbody fusion/cage. The need for postoperative bracing is not altered based on graft choice. Early studies of posterolateral fusion applications appear to show a greater potential benefit of rhBMP-2 over autograft. Not all BMP formulations perform the same with regard to safety and effectiveness. Other osteoinductive proteins in clinical trials (BMP-7, GDF-5) will require individual analysis of these properties.
Question 51
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?

Explanation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries. Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Question 52
High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by


Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 53
High Yield
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of


Explanation
The radiographs show localized diffuse cortical thickening that is characteristic of melorheostosis. The condition may be monostotic or it may involve many bones in one extremity (monomelic) in the distribution of a sclerotome. Bone scans will show increased uptake at the site or sites of skeletal involvement. Long tubular bones are most commonly involved. Melorheostosis is usually asymptomatic and requires no treatment. On rare occasions, there may be associated soft-tissue contractures. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 54
High Yield
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
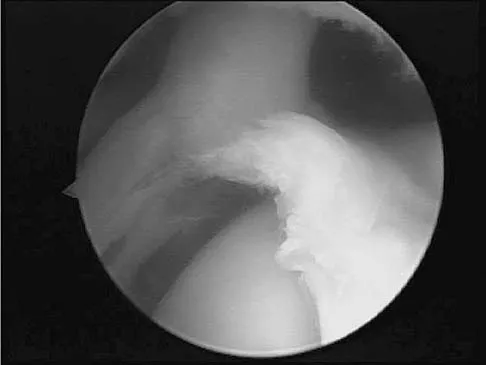
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 55
High Yield
What is the primary role of superficial zone protein (SZP) in articular cartilage?
Explanation
Lubricin and SZP share a similar primary structure but may differ in posttranslational modifications with O-linked oligosaccharides. The primary physiologic function of SZP appears to be boundary lubrication. SZP does not influence interleukin-1, collagenase, or TIMP directly because these proteins are associated with articular cartilage turnover. Hlavacek M: The influence of the acetabular labrum seal, intact articular superficial zone and synovial fluid thixotropy on squeeze-film lubrication of a spherical synovial joint. J Biomech 2002;35:1325-1335.
Question 56
High Yield
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 57
High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 58
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient's program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study. Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Question 59
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?



Explanation
The images reveal a region of increased signal within the rectus femoris muscle with mild, ill-defined surrounding edema. The presence of high intensity signal on the T1-weighted image favors acute blood, in this case associated with a rectus femoris muscle tear or fatty tissue. However, because of fat suppression, a fatty lesion or lipoma would be dark on STIR, rather than bright as in this image. Most foreign bodies are low intensity signal and if small, are difficult to evaluate with MRI. The lack of adjacent subcutaneous soft-tissue edema or surrounding fluid makes pyomyositis an unlikely diagnosis.
Question 60
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?

Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 61
High Yield
Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?

Detailed Explanation
Although all of these factors may influence the decision to perform surgery, the most important is the position of the talus in the mortise. The goal of treatment of ankle fractures is to maintain the talus centered in the mortise. If it is in this position, the other factors do not enter into the decision to intervene surgically. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Question 62
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?


Explanation
The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 63
High Yield
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 64
High Yield
Which of the following factors can contribute to patellar subluxation following routine total knee arthroplasty?

Explanation
Excessive resection of the lateral facet of the patella can lead to subluxation. Rotational alignment of the components can have a significant impact on patellar tracking. Internal rotation of the femoral component leads to more lateral alignment of the patella within the trochlear groove. Internal rotation and medial placement of the tibial component results in lateralization of the tibial tubercle with an increase in the Q angle. Excessive valgus alignment of the mechanical axis, or insufficient correction of preoperative valgus, has a similar effect on the Q angle, and both can result in a higher rate of tracking problems.
Question 65
What is the most common bone tumor in the hand?

Explanation
The most common bone tumor in the hand is an enchondroma. Forty-two percent of these lesions occur in the small tubular bones. They frequently present with a fracture in these locations. Fractures are usually treated nonsurgically. Indications for surgery include patients with symptomatic lesions or those who are considered high risk for recurrent fracture. The histologic appearance of an enchondroma in the hand is more cellular than enchondromas found in the long bones. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Question 66
What is the most common complication following surgical fixation of a distal humeral fracture?

Explanation
In most series, elbow stiffness is the most common complication and can be overcome by achieving stable fixation and initiating early motion after surgery. All of the other complications are seen but to a lesser degree than elbow stiffness. Sanders RA, Raney EM, Pipkin S: Operative treatment of bicondylar intra-articular fractures of the distal humerus. Orthopedics 1992;15:159-163.
Question 67
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
Transfer of the latissimus dorsi and teres major to the posterior rotator cuff will restore external rotation and some abduction. The procedure should be performed in children who are approximately age 4 years, following spontaneous recovery and prior to significant stiffness. External rotation osteotomy is more appropriate for an older child. Fusion should not be performed until skeletal maturity. Distal biceps rerouting restores pronation for a supination deformity. Latissimus dorsi and teres major transfer to the subscapularis would accentuate the internal rotation. In younger patients without significant bony deformity, a subscapularis slide or lengthening can restore external rotation. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Question 68
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
Epithelioid sarcoma is a rare soft-tissue sarcoma that most commonly arises in the hand or upper extremity, and it is frequently misdiagnosed as an infection or granuloma. It tends to have a higher incidence of lymph node metastasis than other soft-tissue sarcomas. The mainstay of treatment is wide surgical excision, even if amputation is necessary. Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Question 69
Figures 40a and 40b show the pre- and postoperative radiographs of an 82-year-old woman with bilateral hip pain who has had staged total hip arthroplasties. To minimize potential injury to the sciatic nerve at the time of surgery, the surgeon should


Explanation
To improve hip biomechanics and secure more suitable bone for acetabular fixation, the true acetabulum is often resurfaced in patients who have developmental dysplasia of the hip, thus lowering the hip center and lengthening the leg. Acute lengthening of more than 3 cm will place excessive tension on the sciatic nerve and require a femoral shortening to avoid sciatic nerve injury. The other maneuvers will not relieve sciatic nerve tension because of limb lengthening. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 430-431.
Question 70
High Yield
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?

Detailed Explanation
The patient has a grade 4 spondylolisthesis. Optimal surgical management is posterior spinal fusion from L4 to the sacrum. The use of instrumentation is controversial. Vertebrectomy is typically reserved for spondylo-optosis (grade 5) cases. Spinal fusion from L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis. Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Question 71
High Yield
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T1-weighted MRI scan with fat suppression and an axial T2-weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?

Explanation
MRI findings of acute osteomyelitis include a decrease in the normally high signal intensity of bone marrow on T1-weighted imaging; however, a postgadolinium T1-weighted image with fat suppression will show osteomyelitis as a bright marrow signal compared to the surrounding fat. Osteomyelitis is also brighter than normal fat on T2-weighted imaging. There is no rim-enhancing lesion suggesting an abscess, although myositis is seen in the obturator internus and short external rotators. The clinical scenario and imaging studies do not support the diagnosis of septic hip, eosinophilic granuloma, or pelvic fracture. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 72
High Yield
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
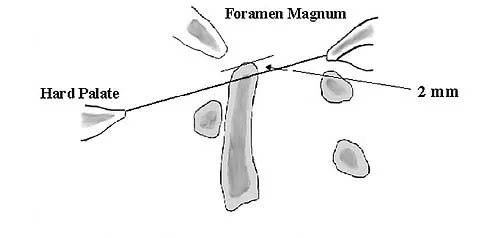
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 73
High Yield
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include

Explanation
Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 74
High Yield
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Detailed Explanation
Insufficient caloric intake caused by either a poor diet or an eating disorder is the most common cause for the loss of menses in a female athlete. In the face of adequate caloric intake, stress is unlikely to cause amenorrhea. Oral contraceptives control menses but do not eliminate it. Diabetes mellitus does not cause the new onset of amenorrhea. Pregnancy can be a cause in a sexually active athlete. Chromosomal abnormalities can result in delayed or absent menarche but not the onset of amenorrhea in a postmenarchal female. Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Question 75
High Yield
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
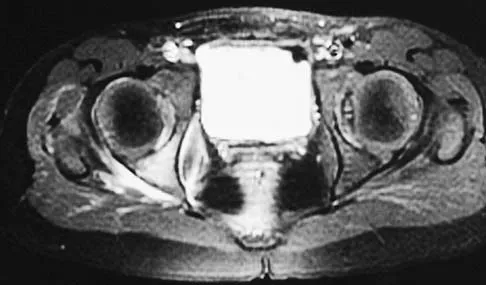
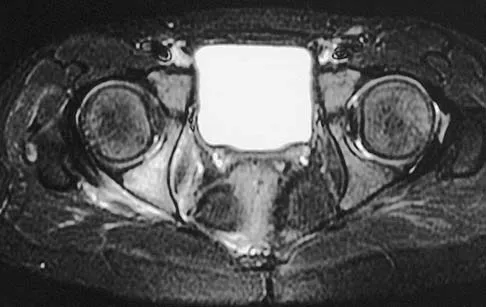
Question 76
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal



Explanation
The patient will most likely exhibit ipsilateral weakness of the tibialis anterior. Gaenslen's test is designed to detect sacroiliac inflammation as a source of low back pain. Beevor's sign tests the innervation of the rectus abdominus and paraspinal musculature (L1 innervation). The extensor hallucis longus is predominantly innervated by L5. The peroneals are predominantly innervated by S1. Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Question 77
High Yield
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?

Explanation
Anatomic positioning of the acetabular component has been shown to be the optimal position for reconstruction of the acetabulum in total hip arthroplasty for DDH. The use of medialized component positioning has been shown to be successful at maximizing the host bone coverage and minimizing the use of bone graft to structurally support the acetabular component. A small acetabular component can be used successfully as long as the femoral head is also reduced in size to maintain the thickness of the acetabular polyethylene. High and lateral positioning for the acetabular reconstruction will result in an increase in the joint reaction forces. In addition, a high and lateral placement will not provide adequate bone to stabilize the reconstruction. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360. Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Question 78
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the

Explanation
The Watson-Jones approach to the hip uses the intermuscular interval between the gluteus medius and the tensor fascia lata. This is not a true internervous plane, as both muscles are supplied by the superior gluteal nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 316-332.
Question 79
High Yield
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of

Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
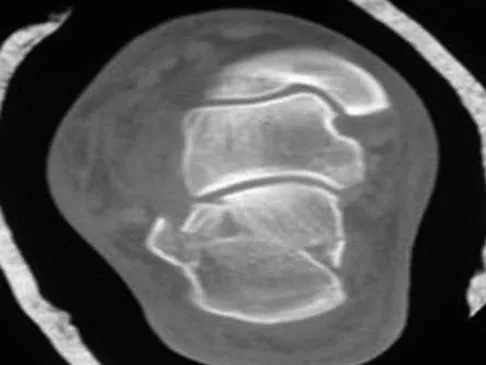
Question 80
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?



Explanation
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
Question 81
High Yield
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of

Explanation
The radiograph shows developmental dysplasia of the hip with the hip reduced and congruent. The treatment of choice is a periacetabular osteotomy because it can improve hip biomechanics and prolong the function of the hip joint. This procedure should be performed prior to the development of severe degenerative changes. Observation will not alter the patient's natural history or the biomechanics of the hip. A total hip arthroplasty should be delayed until severe degenerative changes are present. A Chiari osteotomy is a salvage osteotomy used for a noncongruent subluxated hip. A Pemberton osteotomy requires an open triradiate cartilage; therefore, it is not an option in an adult. Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Question 82
High Yield
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule. Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Question 83
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited. Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Question 84
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Explanation
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism. Tencer AF, Johnson KD: Biomechanics in Orthopaedic Trauma: Bone Fracture and Fixation. Philadelphia, PA, JB Lippincott, 1994. Gonza ER: Biomechanical long bone injuries, in Gonza ER, Harrington IJ (eds): Biomechanics of Musculoskeletal Injury. Baltimore, MD, Williams & Wilkins, 1982, pp 1-30.
Question 85
High Yield
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?

Explanation
The knee is the most common location of spontaneous bleeding in children with hemophilia. Treatment generally requires replacement to 40% to 50% of normal. For surgery, the replacement should be to 100%. The plasma level generally rises 2% for every unit (per kg body weight) of factor VIII administered. Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
Question 86
A 12-year-old girl has had increasing left knee pain for the past 3 months. A radiograph is shown in Figure 75a, and low- and high-power photomicrographs are shown in Figures 75b and 75c. What is the most appropriate treatment?



Explanation
The radiograph reveals an aggressive purely lytic lesion of the distal femoral metaphysis. There is no apparent matrix mineralization or periosteal reaction. The photomicrographs show a malignant spindle cell neoplasm in a storiform pattern. Based on these findings, the diagnosis is malignant fibrous histiocytoma of bone. At most institutions, patients with this tumor are treated similar to patients with osteosarcoma with multi-agent chemotherapy and surgery with wide margins (resection or amputation). Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 203-209.
Question 87
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?


Explanation
The radiographs demonstrate a rapid erosion of the bipolar component into the acetabulum. Although acetabular erosion is more common with unipolar hip arthroplasties, it can occur with bipolar components. Haidukewych and associates noted a very low erosion rate but none in the first 2 years. The second finding on the radiographs is the linear radiolucency progressing from the joint toward the end of the stem at the cement-bone interface suggesting chronic infection or diffuse loosening. The persistent pain since implantation also suggests chronic infection. High activity levels and osteoporosis do not lead to acetabular erosion in the first 2 years after hemiarthroplasty. While the cement technique is suboptimal, loosening and erosion should not be expected from this alone. An oversized bipolar head would extrude and not erode. Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126. Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Question 88
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and

Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 89
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?


Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 90
High Yield
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?

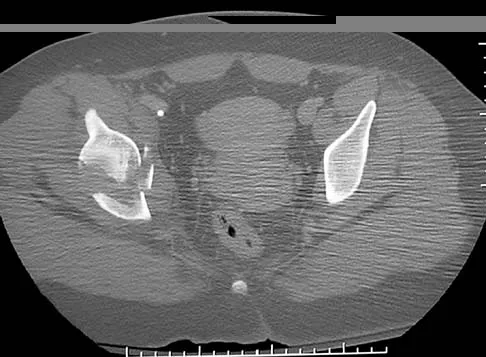

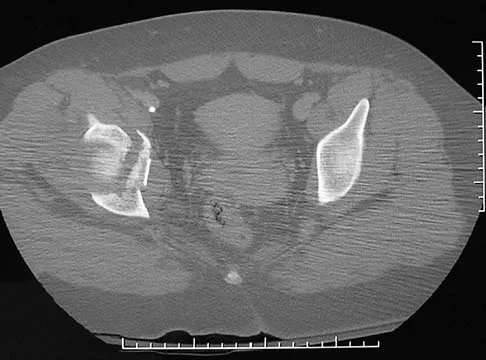
Explanation
The patient has a very low T-type acetabular fracture; however, the head is not congruent under the dome so surgical reduction is necessary. The anterior and posterior columns are displaced and will move independent from each other. The extended iliofemoral is the only approach allowing for visualization and reduction of each column. A combined anterior and posterior approach may also be used. The timing of surgery should be within the first 3 weeks of injury to optimize chances of obtaining an accurate reduction because this is an important factor in determining outcome. Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer-Verlag, 1991.
Question 91
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be


Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 92
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient's ability to heal the wound postoperatively?
Explanation
Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status. A transcutaneous oxygen level should be greater than 40 mm Hg for healing. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Question 93
High Yield
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Question 94
Which of the following definitions best describes Batson's vertebral vein system?

Explanation
The venous plexus was described by Batson and helps to explain the common distribution of metastatic cells to the vertebrae, skull, ribs, and proximal long bones. Batson studied the vertebral vein system extensively by using contrast agents in human cadavers and live monkeys. Batson's plexus is a valveless system that allows retrograde embolism from the major organs such as the breast, prostate, lung, kidney, and thyroid. It is located within the thoracoabdominal cavity and has connections to the proximal long bones and an intercommunicating network of thin-walled veins with a low intraluminal pressure. Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Question 95
High Yield
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 96
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of



Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 97
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
The superficial peroneal nerve, which is adjacent to the location of the lateral arthroscopic portal is most commonly injured. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 98
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 99
High Yield
In performing an opening wedge high tibial osteotomy at the tibial tubercle, the osteotome extends 5 mm posteriorly and centrally out of the bone as shown in Figures 17a and 17b. What is the first structure it enters?


Detailed Explanation
The major risk of performing a high tibial osteotomy is neurovascular injury. The new version of the high tibial osteotomy makes a transverse osteotomy at the level of the tibial tubercle. The osteotome is protected by the oblique belly of the popliteus muscle. The popliteal artery and vein and tibial nerve all lie posterior to the muscle. The soleus muscle originates below this level. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 422.
Question 100
High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
